Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Increased Antidepressant Prescriptions for Children and Adolescents with Major Depressive Disorder in Japan Based on a Claims Database
Authors Nomoto K ![]() , Inagaki A
, Inagaki A ![]() , Yamauchi K
, Yamauchi K
Received 28 April 2025
Accepted for publication 12 September 2025
Published 23 October 2025 Volume 2025:21 Pages 2385—2400
DOI https://doi.org/10.2147/NDT.S537251
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Taro Kishi
Keisuke Nomoto,1,2 Ataru Inagaki,3 Keita Yamauchi1
1Graduate School of Health Management, Keio University, Fujisawa, Kanagawa, Japan; 2Medical Affairs, Viatris Pharmaceuticals Japan G.K., Minato-ku, Tokyo, Japan; 3College of Education, Psychology and Human Studies, Aoyama Gakuin University, Shibuya-ku, Tokyo, Japan
Correspondence: Keisuke Nomoto, Medical Affairs, Viatris Pharmaceuticals Japan G.K., 1-3-1 Azabudai, Minato-ku, Tokyo, 106-0041, Japan, Email [email protected]
Purpose: Currently, no therapeutic antidepressants are approved for pediatric patients with major depressive disorder (MDD) in Japan. In addition, few longitudinal studies have been conducted in Japan on antidepressant prescriptions for children and adolescents with MDD. The purpose of this study is to clarify the actual pharmacotherapy for child and adolescent patients with MDD during fiscal year (FY) 2010–FY2017.
Patients and Methods: We investigated trends in the prescription of antidepressants and concomitant psychotropic drugs for child and adolescent patients aged ≤ 18 years with MDD from FY2010 to FY2017 using a large-scale Japanese health insurance claims database.
Results: From FY2010 to FY2017, the database recorded claims for an average of 443,977 patients annually. Antidepressant prescriptions increased year by year, with particularly large increases in the 13– 18 age group (4.72/1000 persons in FY2010; 6.14/1000 persons in FY2017). By drug class, a higher proportion of selective serotonin reuptake inhibitors, especially sertraline and escitalopram, were prescribed in any given FY, with an increasing trend in the 13– 18 age group (2.64/1000 persons in 2010, 3.55/1000 persons in 2017). However, the overall antidepressant prescription rate among patients with MDD declined gradually, particularly among those in the 13– 18 age group (68.7% in FY2010, 57.0% in FY2017).
Conclusion: The rate of child and adolescent patients prescribed antidepressants increased, while the antidepressant prescription rate among child and adolescent patients with MDD declined, indicating that Japanese physicians have become more cautious about the use of antidepressants. It is critical to generate new clinical data on the efficacy and safety of antidepressants for Japanese child and adolescent patients with MDD and to consider the development of additional pediatric indications for antidepressant therapy.
Keywords: depression, pediatric, prescribed drug, trend, psychotropic drug, longitudinal study
Introduction
Classically, it was believed that there was no depression in children and adolescents that could be diagnosed using the same criteria used for adults. However, since the late 1970s, it has become clear that some depression in children and adolescents meets the adult diagnostic criteria.1 Major depression disorder (MDD) was introduced as a new diagnostic category in 1980, and the diagnostic criteria have since been revised. According to the definitions in the DSM-IV-TR and DSM-5, MDD is diagnosed when a cluster of symptoms—including depressed mood or loss of interest or pleasure lasting at least 2 weeks—is accompanied by a required number of additional symptoms such as changes in appetite, sleep disturbances, fatigue, reduced concentration, feelings of guilt, and suicidal ideation.2,3
Previous epidemiological studies have suggested that the prevalence of first-episode MDD rises rapidly from around age 12, and from that point onward, the prevalence of depressive episodes approaches that seen in adults.4,5 In the United States, the 12-month prevalence of major depressive episodes in adolescents aged 12–17 years increased from 8.7% in 2005 to 11.3% in 20146 and 15.8% in 20197 based on National Surveys on Drug Use and Health. Meanwhile, in Japan, the point and lifetime prevalence of depression among adolescents aged 12–14 years are reported to be 4.9% and 8.8%, respectively.8 The number of patients with mood disorders (including depression) among children and adolescents in Japan also tended to increase year-on-year, especially in the 15–19 age group, and has increased greatly since the beginning of the 2000s.9
In Japan, the annual number of suicides exceeded 30,000 in 1998, peaked in 2003, and then tended to decline to below 22,000 by 2022. The downward trend was more pronounced in the older age groups. However, the number of suicides among adolescents has remained unchanged,10 and suicide is the leading cause of death among children and adolescents in Japan. The situation, along with the increasing number of patients with psychiatric disorders related to suicide, including depression, are critical issues that should be taken seriously by the government.
Major international guidelines for the treatment of depression recommend psychotherapy, such as cognitive behavior therapy or combination therapy with pharmacotherapy for the treatment of moderate to severe child and adolescent depression.11,12 The first-line drug for pharmacotherapy is fluoxetine, which is an FDA-approved drug for depression in children and adolescents aged 8 years and older. In the Japanese guidelines of the Japanese Society of Mood Disorders (JSMD), a chapter on depression treatment for children and adolescents was added for the first time in 2016.13 Medication recommendations are also described, with sertraline recommended for children aged 6 years and older and escitalopram recommended for children aged 12 years and older. Although fluoxetine is most commonly used for pediatric depression worldwide, it is not available in Japan. Because the efficacy and safety of sertraline and escitalopram have not been sufficiently verified in clinical trials in Japanese subjects, the recommendation is based on the results of clinical trials in non-Japanese subjects and the approval status in other countries.13 In Japan, fluvoxamine was approved for an additional indication in 2017 for children aged 8 years and older with obsessive-compulsive disorder (OCD). However, no antidepressants are indicated for the treatment of depression in children in Japan, so these drugs are used off-label.
When antidepressants are prescribed to children and adolescents, a comprehensive diagnosis of the psychiatric condition requiring pharmacotherapy should be made, and the risks and benefits, including the use of off-label therapy, should be explained to the parents and child before obtaining their consent and assent.14,15 Surveys of antidepressant prescriptions for children and adolescents suggest that the number of antidepressant prescriptions for children and adolescents is increasing worldwide and that selective serotonin reuptake inhibitors (SSRIs), mainly fluoxetine, are predominantly being prescribed. In Japan, a survey conducted using claims data up to 2010 revealed that psychotropic drugs, including antidepressants, were used regardless of the lack of established efficacy and safety for use in children and that the antidepressant prescription rate among adolescents increased between 2002 and 2010.16 A 2014 cross-sectional survey of Japanese physicians reported that an estimated 64% of adolescents with depression were on medication, with the most common first-line drugs among participating physicians being sertraline (23%), anxiolytics (17%), fluvoxamine (13%), and antipsychotics (7%).17
In Japan, escitalopram was launched in 2011, and venlafaxine in 2015 as new antidepressants, neither of which are indicated for pediatric use. Additionally, few longitudinal studies have been conducted on the prescribing of antidepressants to children and adolescents with MDD since the previously mentioned claims data–based study.16 If antidepressants are used for a substantial number of children and adolescents with MDD due to medical needs, it will be important to generate clinical data on the efficacy and safety of antidepressants in the Japanese population and to obtain insurance coverage for them in Japan. In this study, we investigated trends in the prescription of antidepressants and concomitant psychotropic drugs for child and adolescent patients with MDD from April 2010 to March 2018 from the claims database. Claims data include diagnoses by physicians regardless of expertise and often prioritize insurance requirements over clinical diagnostic accuracy, which can result in significant misclassification. However, since no other available data can provide such extensive and long-term information, many studies outside Japan have used claims data.18,19 The purpose of this study was to clarify the actual pharmacotherapy used for child and adolescent patients with MDD based on real-world data and to contribute to the evaluation of the medical need for antidepressants for additional pediatric indications and new clinical data in Japan, as well as to the development of clinical guidelines based on actual prescribing practices.
Materials and Methods
Data Source
This study was conducted using a longitudinal, large-scale Japanese health insurance claims database developed by MinaCare Co., Ltd. (Tokyo, Japan). The data were used in accordance with a database usage agreement. The database contains anonymized insurance claims data for company employees and their dependent family members, covering a wide age range up to 74 years, and is provided by multiple diverse corporate health insurance associations across Japan. As of January 2021, it covered approximately 6.3 million individuals across Japan. The use of anonymized data does not require explicit consent under Act on the Protection of Personal Information in Japan.
The study used monthly administrative claims data, including pharmacy, medical, and Diagnosis Procedure Combination (DPC) claims, collected from April 2010 to March 2018 by health insurance associations covering the entire study period. The DPC claims were generated by the DPC-introducing hospital (DPC hospitals) based on the DPC system, a diagnosis- and procedure-specific case-mix payment system consisting of a flat per diem payment and a reimbursement payment for inpatients only. The database included information on patient characteristics (encrypted personal identifiers, age, and sex), diagnosis, medical treatment, and prescribed medications.
Pharmacy claims included information on out-of-hospital prescriptions for outpatients dispensed by community pharmacies, and DPC claims included information on in-hospital prescriptions for inpatients hospitalized in DPC hospitals. Medical claims included information on in-hospital prescriptions for outpatients and in-hospital prescriptions for inpatients admitted to hospitals other than DPC hospitals dispensed by pharmacies inside the hospitals.
Study Population and Outcome Measures
The study subjects were patients aged 18 years or younger at the end of each fiscal year (FY, April 1 to March 31). If a patient was under 18 years old in a given FY, the same patient may have also been investigated in the following FY.
MDD was defined using the International Classification of Diseases, Tenth Revision (ICD-10) codes F32 (major depressive disorder, single episode) and F33 (major depressive disorder, recurrent).18,19 Individuals with at least one record of either code were included in the analysis population.
The primary outcome was the annual rate of patients with MDD prescribed antidepressant medications. The secondary outcomes included the annual rate of patients with MDD, the rate of patients with comorbid psychiatric disorders, the annual rate of patients with MDD prescribed each antidepressant by age group, the antidepressant prescription rates among patients with MDD, and the rates of the concomitant use of medications (use of multiple antidepressants and the use of antidepressants and other psychotropic drugs).
Prescriptions of psychotropic drugs, including antidepressants, for patients with MDD were defined as drug prescription in the same month as the diagnosis of MDD or drug dispensation in the month following the diagnosis (because prescriptions in Japan are valid for four days, including the prescription date) to cover cross-month cases.
Drugs were classified into the following established categories based on previous studies,16,17 current therapeutic agents,20 and the Ministry of Health, Labour and Welfare’s classification:21 “antidepressants”, “antipsychotics”, “mood stabilizers”, “attention-deficit/hyperactivity disorder (ADHD) medications”, “hypnotics”, and “anxiolytics”. Although oral sulpiride is generally classified as an antipsychotic, it was classified as an antidepressant in this study because it has an indication of “depression and depressive state” in Japan and is used to treat depression in daily medical practice (Supplementary Table 1). Even if a patient was diagnosed with MDD and ICD-10 code G40 (epilepsy) or G41 (status epilepticus) in the same month and was prescribed carbamazepine, lamotrigine, or sodium valproate, these drugs were not treated as “mood stabilizers”. Likewise, in the same case, phenobarbital was not treated as a “hypnotic”.
Statistical Analysis
The subjects were classified into three age groups based on a previous study conducted in Japan: 0–5 years (0–5 age group), 6–12 years (6–12 age group, children), and 13–18 years (13–18 age group, adolescents).
The comorbidity rate of other psychiatric disorders with MDD was calculated for each group of ICD-10 codes for each FY and expressed as the percentage of patients with MDD who also had comorbidities out of the total number of patients with MDD. This study had no exclusion criteria for psychiatric disorders to cover all patients with a diagnosis of MDD in the database.
The rate of patients with MDD and the rate of patients with MDD prescribed antidepressants were calculated per 1000 persons for each FY and for each age group using as follows:
Rate per 1000 persons = ([Number of patients with MDD or number of patients with MDD prescribed antidepressants] / [Total number of persons who had at least one claims data in the database]) × 1000
People with any claims data accounted for approximately 90% of the health insurance enrollees in the database for each FY.
The prescription rate of each antidepressant among patients with MDD (the percentage of antidepressant prescriptions for patients with MDD) was calculated for each FY and age group as follows:
Prescription rate (%) = ([Number of patients with MDD for whom each antidepressant was prescribed] / [Total number of patients with MDD]) × 100.
The prescription rate of the combined use of multiple antidepressants was calculated by FY and was defined as the percentage of patients prescribed at least two antidepressants for at least one month in each FY among patients with MDD. The rate of concomitant use of antidepressants and additional psychotropic drugs was calculated by drug class for each FY and was defined as the percentage of patients prescribed at least one antidepressant and psychotropic drug(s) for at least one month in each FY for which antidepressant was prescribed among patients with MDD.
JMP® Pro 17.2.0 and Microsoft Excel 2021 were used to conduct the calculations and produce the graphs.
Results
Characteristics of the Claims and Subjects
The characteristics of the claims and subjects included in the analysis are shown in Table 1. Over the 8 years from FY2010 to FY2017, the mean annual claims included 2,008,682 dispensing claims per year, 2,995,508 medical claims per year, and 18,223 DPC claims per year. In each FY, claims occurred for a mean of 443,977 patients per year, including duplicate patients across the years.
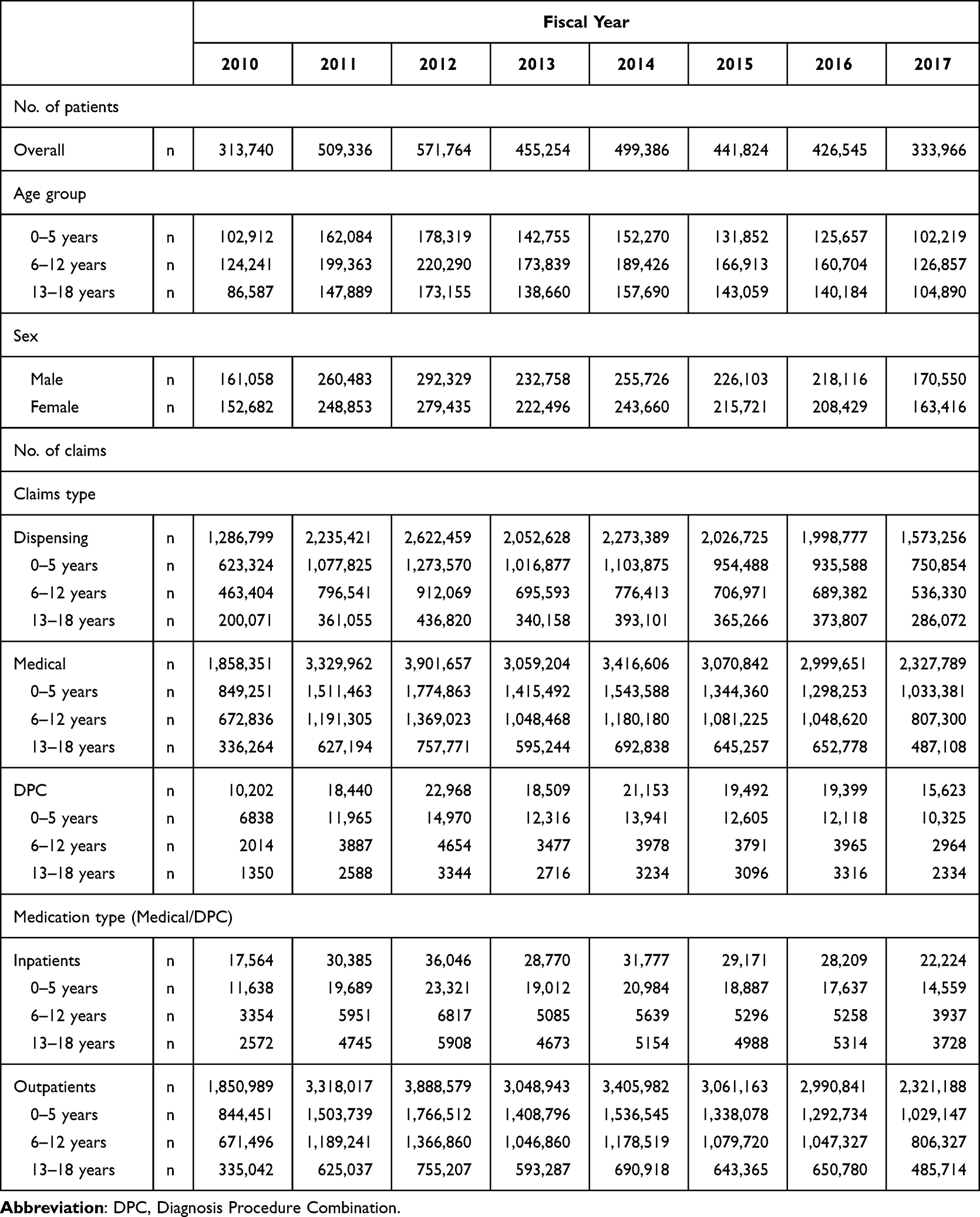 |
Table 1 The Characteristics of the Claims and Subjects for Analysis |
Rate of Patients with MDD
The rate of patients with MDD out of all persons with any claims included in the analysis is shown for each age group in Table 2. The overall rate of patients diagnosed with MDD increased year by year, and the mean annual rate of patients diagnosed with MDD from FY2010 to FY2017 was 3.17/1000 persons. The 13–18 age group (adolescence) accounted for a dominant proportion in each FY, with large increases between FY2010 and FY2017 (6.87/1000 persons in FY2010, 10.77/1000 persons in FY2017).
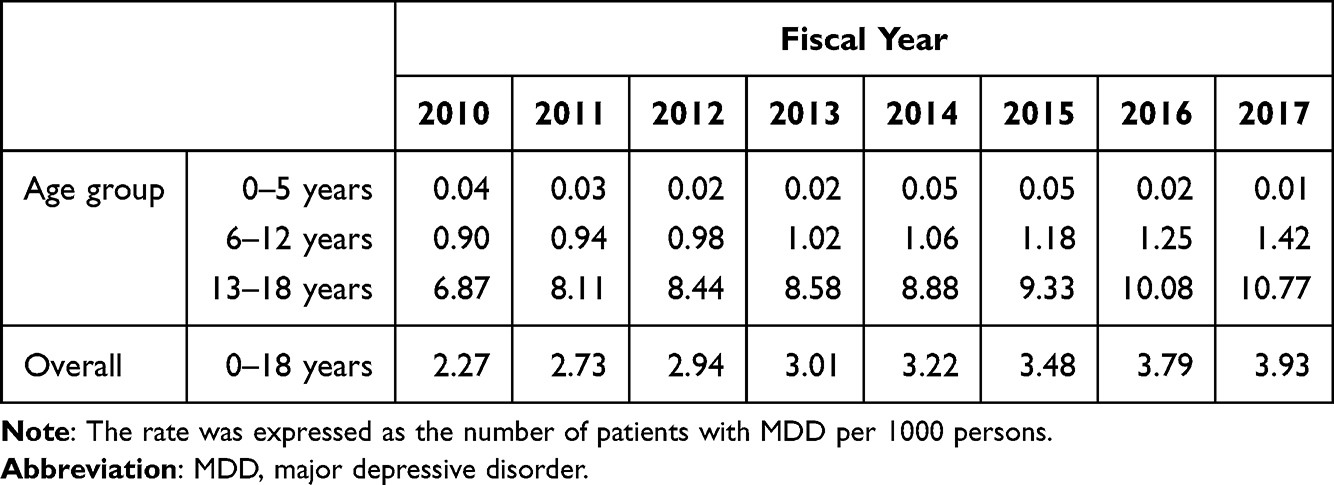 |
Table 2 The Rate of Patients with MDD (per 1000 Persons) |
Comorbidity with Other Psychiatric Disorders
The comorbidity rate of MDD with other psychiatric disorders is shown in Table 3. Some psychiatric disorders that may not be diagnostically comorbid with MDD were also included and were described according to the disorder named on the claims. “Neurotic, stress-related, and somatoform disorders” (ICD-10 code: F4) was the most common comorbidity in patients with MDD as a disease group throughout all the FYs.
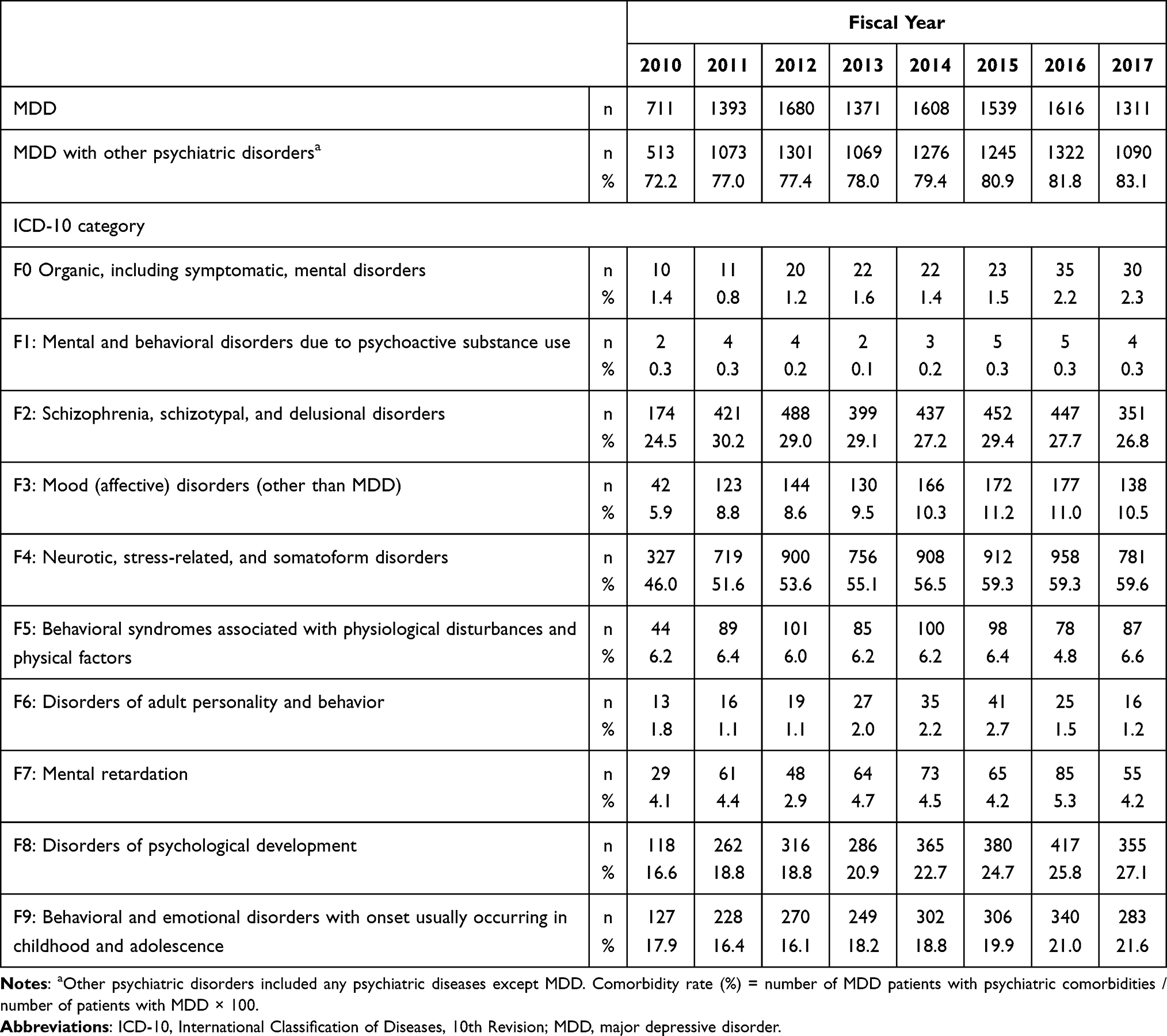 |
Table 3 Comorbidity with Other Psychiatric Disorders |
Antidepressants Prescription
The annual trends in the rate of patients with MDD prescribed antidepressants per 1000 persons are shown in Table 4. The rate of antidepressant prescriptions showed an increasing trend year by year, with particularly large increases in the 13–18 age group (4.72/1000 persons in FY2010; 6.14/1000 persons in FY2017, Table 4). The rate of antidepressant prescriptions in the 0–5 age group was generally below 0.01/1000 persons in all FYs, while the rate of antidepressant prescriptions in the 6–12 age group was between 0.53 and 0.68/1000 persons. Among the different drug classes, SSRIs accounted for a higher proportion of prescriptions in every FY, with an increasing trend observed in the 13–18 age group (from 2.64/1000 persons in FY2010 to 3.55/1000 persons in FY2017). In particular, among the SSRIs, sertraline and escitalopram had a higher rate in FY2017. Among all antidepressants, sulpiride had the highest prescription rate in the 13–18 age group in FY2017 (1.60/1000 persons). Since escitalopram’s launch in FY2011, its prescription has steadily increased in the 13–18 age group, whereas the rate of fluvoxamine prescriptions showed a decreasing trend. The rates of other SSRIs and sulpiride prescriptions showed no significant fluctuations (Figure 1).
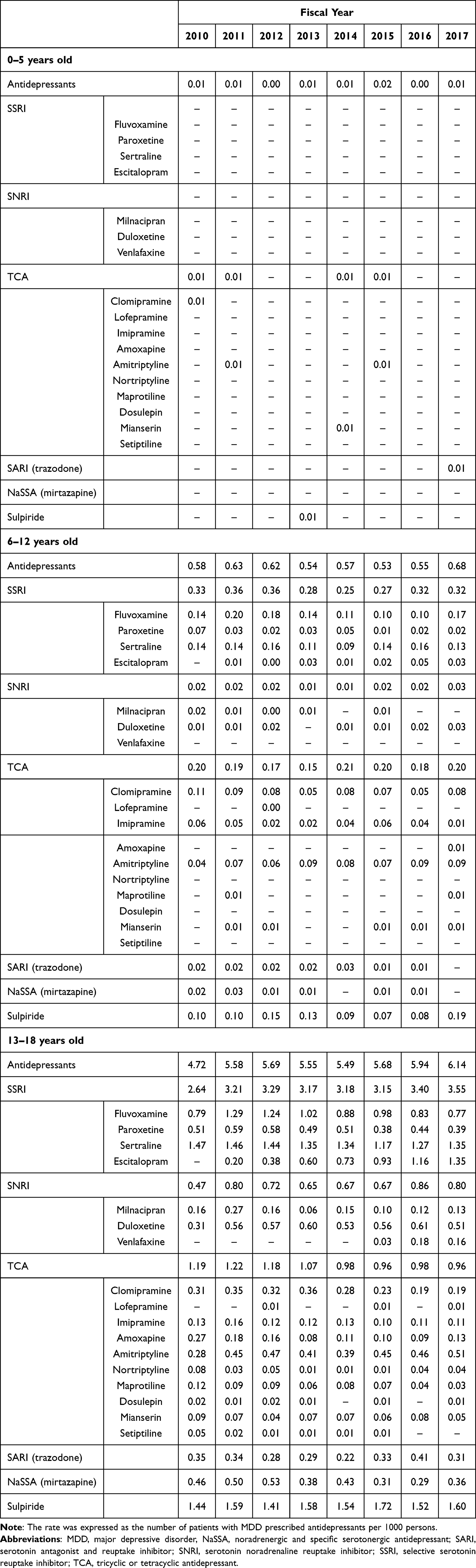 |
Table 4 The Rate of Patients with MDD Prescribed Antidepressants (per 1000 Persons) |
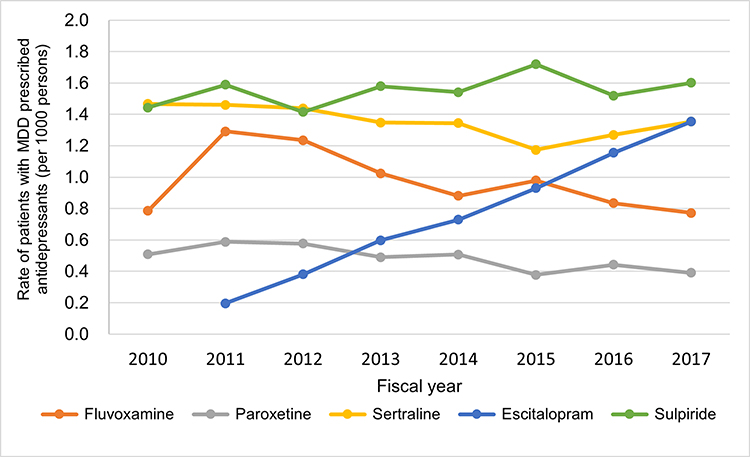 |
Figure 1 Trends in the rate of patients with MDD aged 13–18 years prescribed SSRIs or sulpiride. Abbreviations: MDD, major depressive disorder; SSRIs, selective serotonin reuptake inhibitors. |
The annual trends in the prescription rate of all antidepressants among patients with MDD are shown in Table 5. The antidepressant prescription rate declined gradually from FY2010 to FY2017, particularly in the 6–12 age group (64.3% in FY2010, 47.8% in FY2017, Table 5) and also in the 13–18 age group (68.7% in FY2010, 57.0% in FY2017, Table 5).
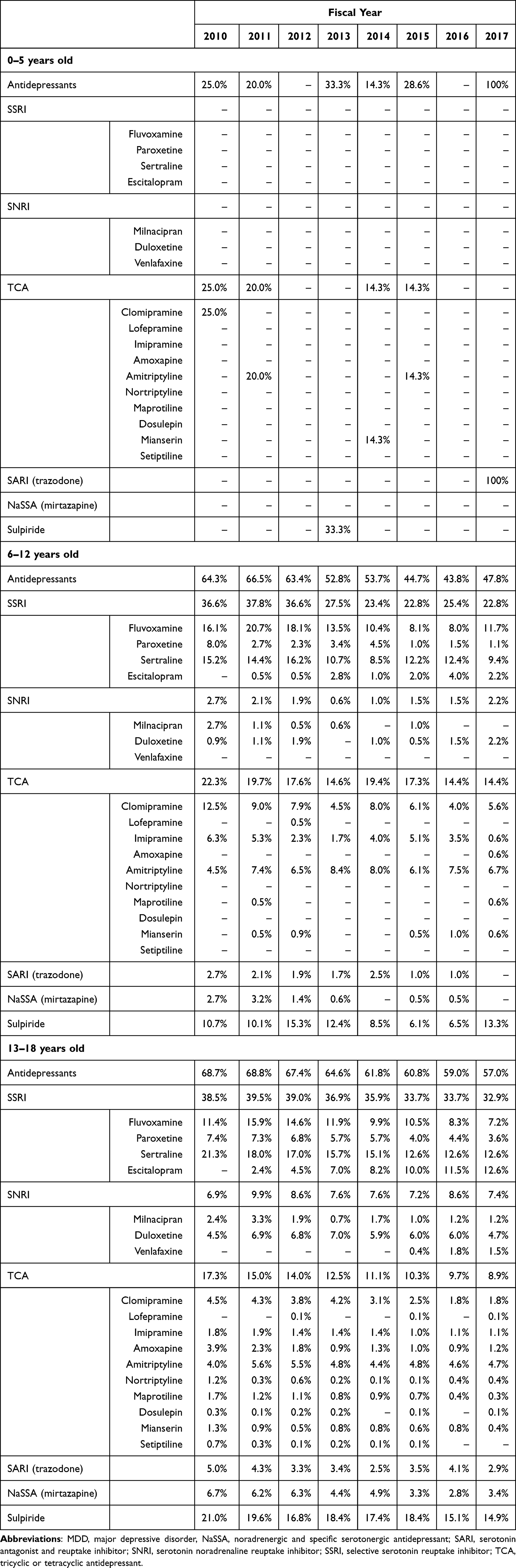 |
Table 5 Antidepressant Prescription Rates Among Patients with MDD |
Combined Use of Different Antidepressants and Concomitant Use of Antidepressants with Other Psychotropic Drugs
The prescription rate of the combined use of different antidepressants in patients with MDD showed a decreasing trend (24.5% in FY2010; 17.1% in FY2017) (Figure 2).
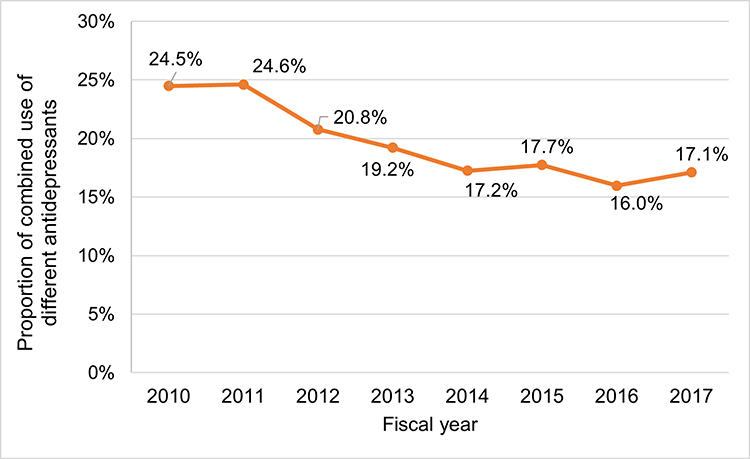 |
Figure 2 Combined use of different antidepressants for patients with MDD. Abbreviation: MDD, major depressive disorder. |
Regarding the concomitant use of antidepressants and other psychotropic drugs (Figure 3), a decreasing trend for anxiolytics (45.4% in FY2010 and 32.4% in FY2017) was observed. Meanwhile, the prescription of antipsychotics increased between FY2010 and FY2017 (21.8% in FY2010, 32.1% in FY 2017), with a significant rise observed for aripiprazole within this drug category (6.8% in FY2010, 21.1% in FY2017), accounting for approximately two-thirds of the antipsychotics prescribed in FY2017.
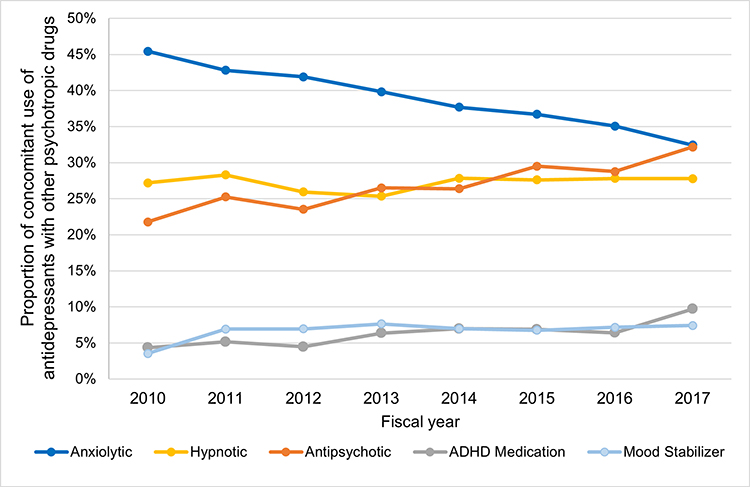 |
Figure 3 Concomitant use of antidepressants and psychotropic drugs for patients with MDD. Abbreviations: ADHD, attention-deficit/hyperactivity disorder; MDD; major depressive disorder. |
For hypnotics, there was almost no change (FY2010: 27.2%, FY2017: 27.8%). However, by drug category, the percentage of benzodiazepines prescribed decreased, while that of melatonin receptor agonists (3.1% in FY2010, 9.2% in FY2017) and orexin receptor antagonists (launched in 2014, 5.9% in FY2017) increased. Meanwhile, the rate of prescription of non-benzodiazepine hypnotics (ie, Z-drugs) remained constant.
The prescription rate of ADHD medications was low, but it was on the rise (4.4% in FY2010, 9.7% in FY2017). The prescription rate of mood stabilizers increased slightly from FY2010 (3.5%) to FY2011 (6.9%) but remained constant thereafter (7.4% in FY2017).
Discussion
This study is the first to examine the real-world clinical situation of antidepressant prescriptions specifically focusing on child and adolescent patients diagnosed with MDD. From FY2010 to FY2017, an increasing trend was observed in the overall rate of child and adolescent patients with MDD prescribed antidepressants. Analysis by age group revealed no change in the 0–5 and 6–12 age groups, and this trend occurred only in the 13–18 age group (adolescents). Among antidepressant classes, a high and increasing rate of prescriptions was found for SSRIs, especially sertraline and escitalopram, which are recommended in the Japanese MDD treatment guidelines.13 In contrast, fluvoxamine is not included in the recommendation of the Japanese guidelines. Although the additional approval of fluvoxamine for children with OCD in FY2017 may have had a marginal impact, the downward trend in its prescription since FY2012 continued. Therefore, antidepressant prescriptions may have followed the recommendations for the treatment of child and adolescent patients in the international guidelines. In addition, since the JSMD added a new chapter on children and adolescents to the Japanese guidelines for MDD treatment in July 2016,13 the recommendations may have influenced the 2017 prescription rates.
Notably, the prescription rate of sulpiride was the highest among the drug products. Although sulpiride is indicated in Japan for the treatment of depression and depressive states, the Japanese guidelines recommend that it should be used with caution in pediatric patients due to potential side effects, such as Parkinson’s syndrome and hyperprolactinemia.13 The reasons for the selection of sulpiride might include its relative safety compared with other antidepressants and the legal risk aversion in the treatment of a patient experiencing a suicide-related event because the package insert of general antidepressants indicates increased suicide-related behavior when used in young people. However, there is still a lack of evidence that sulpiride is safe for use in pediatric patients, and safety monitoring for Parkinson’s syndrome, hyperprolactinemia, and extrapyramidal symptoms should be conducted.
In contrast to the overall rate of antidepressant prescriptions, the percentage of antidepressant prescriptions for patients with MDD decreased over the years. This decline was particularly significant in the 6–12 age group; thus, the younger the patient, the higher priority was given to non-pharmacological approaches, such as environmental adjustment, before attempting pharmacotherapy, which is recommended in the MDD treatment guidelines of the JSMD.13 This suggests that although antidepressant prescription has increased over time, it is not an increase in indiscriminate antidepressant prescribing, and physicians are becoming more cautious about prescribing antidepressants to children. In an environment in which the appropriate treatment steps recommended in the guidelines are becoming more widespread, the results suggest that a certain number of pediatric patients with MDD require antidepressant medications.
A decreasing trend was observed for the concomitant use of different antidepressants, which was consistent in all age groups. We considered that this was likely due to physicians’ adherence to Japanese and international guidelines that recommend prescribing antidepressants as monotherapy and/or the 2014 revision of medical reimbursement in Japan to reduce the drug cost, prescription fees, and prescription dispensing fee for the prescription of multiple (≥4) antidepressants. In contrast, the prescription rate of antipsychotics used in combination with antidepressants increased. The approval of aripiprazole, an antipsychotic agent, for the treatment of “depression and depressive states” in Japan in 2013 may have contributed to its increased use as an augmentation therapy for MDD.
For hypnotics, although no trend in prescription rate was observed, these drugs are likely being replaced with melatonin agonists and orexin receptor antagonists, which are considered to be safer than traditional hypnotics. Concerning ADHD medications, they are possibly prescribed for patients with comorbid MDD and ADHD or depression secondary to ADHD rather than for patients with only MDD. The increased prescription rate of ADHD medications is likely due to the growing trend in the number of diagnosed ADHD patients.22
This study has several limitations. First, the database used was limited to members of Japanese health insurance societies and did not include self-employed individuals, employees of small and medium-sized enterprises, or recipients of public assistance (Japan’s protection program) and their family members. This restricts the generalizability of the findings to the broader Japanese population. Second, because the exact number of individuals by age group is not disclosed, we used the total number of individuals with at least one claim in the database as the denominator to calculate prescription rates per 1000 persons. While this may introduce some degree of error, the total number of individuals with claims is likely close to the actual population, and any resulting inaccuracies are unlikely to significantly affect the interpretation of long-term trends. Third, because the database used in this study was a medical claims database, the diagnostic names included in the database are likely to prioritize insurance claims, and the diagnostic names may not necessarily correspond to actual clinical practice. As an example, there were patients in this study with comorbid bipolar disorder, which diagnostically cannot be comorbid with MDD. Therefore, it is possible that mood stabilizer prescriptions included not only augmentation therapy for MDD but also a certain number of prescriptions for bipolar disorder. Similarly, the number of patients with MDD may have been overestimated because some diseases/conditions that should be excluded when diagnosing MDD may have been included. Fourth, since MDD is a common indication for antidepressants, even when antidepressants were prescribed for conditions other than MDD, MDD may have been selected preferentially as the insurance claim for administrative convenience, leading to an overestimation of MDD diagnoses. Fifth, even if unintentional, misdiagnoses may have been included, especially given that diagnostic agreement rates for MDD in adolescents are known to be low.23 The impact of the overestimation of MDD patients on the results of this study is unclear. Therefore, caution should be exercised when interpreting the data. Sixth, the database used in this study is limited to the period up to March 2018 and cannot anticipate the actual conditions after that date. Lastly, the present analysis does not provide information on the order of prescriptions. Additional analysis should be conducted to determine the prescribing patterns of individual patients.
Conclusion
This study is the first retrospective study to investigate the actual prescription rates of antidepressants to child and adolescent patients with MDD in Japan. The important finding is that while the rate of patients with MDD under the age of 18 prescribed antidepressants increased from FY2010 to FY2017, the antidepressant prescription rate among child and adolescent patients with MDD declined. This finding may be in accordance with the content of Japanese and international guidelines for drug selection and treatment procedures, which recommend that pharmacological treatment for child and adolescent patients with MDD should be approached with caution. In addition, psychotropic drugs were used in combination with antidepressants. This also aligned with the recommendations of the guidelines to treat patients more cautiously in consideration of their safety.
Although Japanese physicians have become more cautious about the use of antidepressants, there continues to be a certain number of child and adolescent patients with MDD who require antidepressant treatment. Therefore, there is a need to establish the efficacy and safety of antidepressants for Japanese child and adolescent patients with MDD and to consider the development of additional pediatric indications for antidepressant treatment. The observed use of antidepressants among a subset of child and adolescent patients with MDD, along with the upward trend in prescribing, may encourage further efforts to generate efficacy and safety data specific to Japanese children and adolescents. These findings are also expected to inform future updates to clinical guidelines, supporting the appropriate use of antidepressants in this population based on real-world prescribing practices.
Abbreviations
ADHD, attention-deficit/hyperactivity disorder; DPC, Diagnosis Procedure Combination; FY, fiscal year; ICD-10, International Classification of Diseases, Tenth Revision; JSMD, Japanese Society of Mood Disorders; MDD, major depressive disorder; OCD, obsessive-compulsive disorder; SSRIs, selective serotonin reuptake inhibitors.
Data Sharing Statement
Data supporting the results of this study were provided by MinaCare Co., Ltd. under license for this study. Although the data are not available publicly, they are obtained from the corresponding author on reasonable request with the permission of MinaCare Co., Ltd.
Ethics Approval and Informed Consent
The MinaCare database used in this study contained only already anonymized information. Approval from an ethical review committee and the informed consent of subjects were not required because research using only anonymized data is outside the scope of the Ethical Guidelines for Medical and Health Sciences Research Involving Human Subjects set by the Japanese government.
Acknowledgments
MinaCare Co., Ltd. provided the claims data. The authors acknowledge Yuji Yamamoto, MD, MBA (MinaCare Co., Ltd.) for his valuable advice on this study. Editorial support was provided by Takahiko Murata, PhD, at WysiWyg Co., Ltd. and was funded by Viatris Pharmaceuticals Japan G.K.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was sponsored and funded by Viatris.
Disclosure
KN is a full-time employee of Viatris Pharmaceuticals Japan G.K. AI has received a consulting fee/honorarium from Mitsubishi Tanabe Pharma Corporation, IQVIA Services Japan G.K., Meiji Seika Pharma Co., Ltd., Janssen Pharma K.K., Creativ-Ceutical K.K., and KnowledgeWire Corporation. AI is also involved in research projects funded by six companies: Otsuka Pharmaceutical Co., Ltd., Shionogi & Co., Ltd., Dainippon Sumitomo Pharma Co., Ltd. (now Sumitomo Pharma Co., Ltd.), Takeda Pharmaceutical Company Limited, Meiji Seika Pharma Co., Ltd., and Janssen Pharmaceutical K.K. However, AI has not been allocated any research funding from these companies. KY has no conflicts of interest to declare for this work.
References
1. Puig-Antich J, Blau S, Marx N, Greenhill LL, Chambers W. Prepubertal major depressive disorder: a pilot study. J Am Acad Child Psychiatry. 1978;17(4):695–707. doi:10.1016/s0002-7138(09)61021-9
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
3. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5). Arlington, VA: American Psychiatric Association; 2013.
4. Zisook S, Lesser I, Stewart JW, et al. Effect of age at onset on the course of major depressive disorder. Am J Psychiatry. 2007;164(10):1539–1546. doi:10.1176/appi.ajp.2007.06101757
5. Hasin DS, Goodwin RD, Stinson FS, Grant BF. Epidemiology of major depressive disorder: results from the national epidemiologic survey on alcoholism and related conditions. Arch Gen Psychiatry. 2005;62(10):1097–1106. doi:10.1001/archpsyc.62.10.1097
6. Mojtabai R, Olfson M, Han B. National trends in the prevalence and treatment of depression in adolescents and young adults. Pediatrics. 2016;138(6):e20161878. doi:10.1542/peds.2016-1878
7. Fox DJ, Hanes D. Prevalence and correlates of unmet mental health services need in adolescents with major depressive episode in 2019: an analysis of national survey on drug use and health data. J Adolesc Health. 2023;72(2):182–188. doi:10.1016/j.jadohealth.2022.10.001
8. Sato H, Shimotsu H, Ishikawa S. Prevalence rate of depressive disorders in a community sample of adolescents in Japan. Seishin Igaku/Clin Psychiatry. 2008;50(5):439–448. In Japanese. doi:10.11477/mf.1405101205
9. e-Stat/Statistics of Japan, patient survey, 2022. Tokyo, Japan: Official Statistics of Japan. Available from: https://www.e-stat.go.jp/stat-search/files?page=1&toukei=00450022&tstat=000001031167.
10. Nakamura K. The Guidelines for Pharmacological Treatment for Mental Disorders in Childhood and Adolescence. Tokyo, Japan: Jiho; 2018. In Japanese.
11. Depression in children and young people: identification and management NICE guideline [NG134]. London, United Kingdom: National Institute for Health and Care Excellence. Available from: https://www.nice.org.uk/guidance/ng134.
12. Taylor DM, Barnes TRE, Young AH. Children and adolescents. In: The Maudsley Prescribing Guidelines in Psychiatry:14th Edition. Hoboken, NJ, United States: Wiley-Blackwell; 2021:539–599.
13. Treatment guidelines of the Japan society of mood disorders II. depression (DSM-5)/major depressive disorder 2016. Tokyo, Japan: Japanese Society of Mood Disorders. Available from: https://www.secretariat.ne.jp/jsmd/iinkai/katsudou/data/20190724-02.pdf.
14. Usami M. Current practice of pharmacotherapy in child and adolescent psychiatry 2: antidepressants. Jpn J Child Adolesc Psychiatry. 2017;58(1):146–156. In Japanese. doi:10.20615/jscap.58.1_146
15. APA clinical practice guideline for the treatment of depression across three age cohorts. Washington, DC, United State: American Psychological Association. Available from: https://www.apa.org/depression-guideline/guideline.pdf.
16. Okumura Y, Fujita J, Matsumoto T. Trends of psychotropic medication use among children and adolescents in Japan data from the national insurance claims database between 2002 and 2010. Seishin Shinkeigaku Zasshi/Psychiat Neurol Jap. 2014;116(11):921–935. In Japanese.
17. Saito T, Reines EH, Florea I, Dalsgaard MK. Management of depression in adolescents in Japan. J Child Adolesc Psychopharmacol. 2019;29(10):753–763. doi:10.1089/cap.2019.0023
18. Bode K, Vogel R, Walker J, Kröger C. Health care costs of borderline personality disorder and matched controls with major depressive disorder: a comparative study based on anonymized claims data. Eur J Health Econ. 2017;18(9):1125–1135. doi:10.1007/s10198-016-0858-2
19. Lee JW, Lee H, Kang HY. Association between depression and antibiotic use: analysis of population-based national health insurance claims data. BMC Psychiatry. 2021;21(1):536. doi:10.1186/s12888-021-03550-2
20. Izutsu K, Imai Y, Kuwana M, Terada T, Tateda K. Today’s Drug Therapy in 2024. Tokyo, Japan: Nankodo Co. Ltd; 2024. In Japanese.
21. HIB/MED Notification No. 0717-1. Partial revision of Practical considerations regarding partial revisions to methods for calculating payments for medical services. Tokyo, Japan: Ministry of Health, Labour and Welfare; 2020. Available from: https://www.mhlw.go.jp/content/12400000/000650099.pdf.
22. Uchiyama Y, Tanaka T. Research on actual condition of ADHD and medical treatment. J Natl Inst Public Health. 2005;54(2):94–100.
23. Clarke DE, Narrow WE, Regier DA, et al. DSM-5 field trials in the United States and Canada, Part I: study design, sampling strategy, implementation, and analytic approaches. Am J Psychiatry. 2013;170(1):43–58. doi:10.1176/appi.ajp.2012.12070998
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.