Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Incidence of Pneumonia and Predictors Among Human Immunodeficiency Virus Infected Children at Public Health Institutions in the Northwest Part of Ethiopia: Multicenter Retrospective Follow-Up Study
Authors Mengesha T ![]() , Embiale T, Azmeraw M
, Embiale T, Azmeraw M ![]() , Kerebeh G, Mulatu S
, Kerebeh G, Mulatu S ![]() , Meseret F
, Meseret F ![]() , Birhanu M
, Birhanu M ![]()
Received 21 October 2021
Accepted for publication 29 January 2022
Published 11 February 2022 Volume 2022:13 Pages 13—25
DOI https://doi.org/10.2147/PHMT.S345638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Teshale Mengesha,1 Tsegasew Embiale,1 Molla Azmeraw,2 Gashaw Kerebeh,3 Sileshi Mulatu,4 Fentahun Meseret,5 Minyichil Birhanu4
1Department of Pediatrics and Child Health Nursing, College of Medicine and Health Sciences, Dire Dawa University, Dire Dawa, Ethiopia; 2Department of Nursing, College of Health Sciences, Woldia University, Woldia, Ethiopia; 3Department of Pediatrics and Child Health Nursing, College of Medicine and Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 4Department of Pediatrics and Child Health Nursing, School of health Sciences, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 5Department of Pediatrics and Child Health Nursing, School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Teshale Mengesha, Pediatrics and Child Health Nursing at Dire Dawa University, Dire Dawa, Ethiopia, Email [email protected]
Introduction: Pneumonia is an inflammation of the lung parenchymal structure secondary to hematogens spread of pathogens, inhalation, or aspiration. It is also one of the most frequently occurring opportunistic infections in HIV-infected children. In Ethiopia, data on the incidence and predictors of opportunistic infection, especially pneumonia, among HIV-infected children is very limited. Hence, this study aimed to assess the incidence of pneumonia and predictors among HIV-infected children at public health institutions in the Northwest part of Ethiopia.
Methods: An institution-based retrospective cohort study was conducted among 342 HIV-infected children at public health institutions from January 1, 2013 to December 30, 2020. Log rank test was used to compare the survival curves between different explanatory variables. Bivariable Cox proportional hazards regression model was employed for each explanatory variable to check the association with the outcome variable. Variables found to have a p-value of < 0.25 in the bivariable analysis were candidates for the multi-variable proportional hazard model. Cox proportional hazards model was used at 5% level of significance to identify predictors of pneumonia.
Results: This study included 342 records of HIV-infected children who started antiretroviral therapy between the periods of January 1, 2013 to December 30, 2020. The overall incidence rate of pneumonia during the follow-up time was 5.57 (95% CI: 4.4, 7.0) per 100 child-years of observation. Those children who did not take cotrimoxazole preventive therapy (AHR: 3, 95% CI: 1.40, 6.44), being underweight at baseline (AHR: 2.6, 95% CI: 1.41, 4.86), having baseline advanced disease (clinical stages III and IV) (AHR: 2.8, 95% CI: 1.30, 6.04), and presenting with recently detected viral load (AHR: 5.9, 95% CI: 2.53, 14.06), were more likely to develop pneumonia.
Conclusion: Pneumonia incidence rate was high. Providing prophylaxis and nutritional supplementation for those children with baseline advanced disease stage, low weight for age and detectable viral load would reduce pneumonia occurrence.
Keywords: pneumonia, incidence, HIV, children, Ethiopia
Background
Pneumonia is one of the most frequently occurring opportunistic infections in human immunodeficiency virus (HIV) infected children. Bacterial respiratory tract infections occur more frequently in HIV-positive children and HIV-exposed infant than in HIV-negative children.1 Pneumonia continues to be the leading cause of morbidity and mortality in children worldwide.2 In 2017, pneumonia caused an estimated 6.3 million deaths globally; 1 million of these occurred in 5 to 14 year old children.3 Globally, 1.4 million episodes of clinical pneumonia were attributable to HIV in 2015.4 In 2010, 88,000 pneumonia deaths occurred in HIV-infected children, and 93% of deaths were among children under 5 years of age in Africa.5 Acute and chronic respiratory illnesses are the most common presenting complaint of morbidity in HIV-infected children.6 HIV-infected children are 6.5 times more at risk of hospitalization and at higher risk of death from pneumonia when compared to HIV-uninfected children, especially in African countries.7 In the highest HIV burden countries in sub-Saharan Africa, 60% of pneumonia deaths occur in HIV-infected children.5,8 The proportionate contribution of sub-Saharan Africa to the global estimates of pneumonia among HIV-infected children was 72%.4 HIV-infected children carry a high burden of lower respiratory zone infection usually caused by viruses, bacteria, and mycobacterium tuberculosis. Bacteria are an important cause of childhood pneumonia. Haemophilus influenzae type b and Streptococcus pneumonia are the most common causes and vaccines against them have been introduced to reduce the mortality from childhood pneumonia.9 Streptococcus pneumonia is part of normal flora in the upper part of the respiratory system but it can cause severe invasive diseases like meningitis, septicemia, and pneumonia.10 Pneumocystis pneumonia was one of the most frequent opportunistic infections before the widespread use of antiretroviral drugs and effective prevention of mother-to-child transmission. It commonly occurs when a patient’s immunity is significantly suppressed.11
As evidence shows from study in Ethiopia, pneumonia is one of the leading opportunistic infections that predict nearly 60% of hospitalizations among HIV-infected children in the six months following antiretroviral therapy (ART) initiation.12 A study in the United States revealed that there were 87 community acquired pneumonia (CAP) episodes among HIV-infected children, with an incidence of 3.32 cases per 100 PY of follow-up.13 Another study, in Latin America, showed that the incidence of overall opportunistic infection among HIV-infected children was 23.5 per 100 PY; of these, the overall incidence of pneumonia was 8.1 per 100 person years.14
Evidence from other studies shows that young age, malnutrition, low immunity, smoking or air pollution exposure, high viral load and low hemoglobin level are risk factors for pneumonia among HIV-infected patients.11,15,16 Although sufficient studies are done about pneumonia among children, there is a scarcity of information on children infected with HIV, especially in sub-Saharan Africa where the HIV burden is high.17 Even though pneumonia was the first common opportunistic infection among HIV-infected children in Ethiopia,18 data on the incidence and predictors of pneumonia among HIV-infected children is very limited.
Therefore, this study is intended to fill this information gap. Moreover, for better intervention and treatment, up-to-date information regarding the occurrence of pneumonia among HIV-infected children is important. So, the aim of this study is to assess the incidence of pneumonia and predictors among HIV-infected children at public health institutions in the northwest parts of Ethiopia. The results of this study provide evidence-based information for decision makers, health care workers, and researchers to develop general or specific effective preventive strategies and programs to reduce the burden of pneumonia in HIV-infected children.
Methods
Study Design, Setting and Period
An institution-based retrospective cohort study was conducted at public health institutions in the northwest parts of Ethiopia from January 1, 2013 to December 30, 2020. Bahir Dar city was the selected study area; it is the capital city of Amhara regional state, located in the northwest of Ethiopia. It is found 565 km away from Addis Ababa, the capital city of Ethiopia. According to the Bahir Dar city administration report, estimated total population in 2020 was 389,177, of which 183,984 were male and 205,193 were female. Additionally, the estimated number of children under 15 years of age is 147,983. Currently, the total number of pediatric population on ART at public health facilities in Bahir Dar city is 763. The city has two referral hospitals, one primary hospital, and ten health centers, of which only one health center does not provide ART service.
Study Participants
The source population for this study was all HIV-infected children age < 15 years who started ART enrollment at public health institutions in Bahir Dar city. The study population included all HIV-infected children who started ART follow-up at public health institutions from January 1, 2013 to December 30, 2020.
Eligibility Criteria
All HIV-infected children aged less than 15 years who started ART follow-up from January 1, 2013 to December 30, 2020 were included in this study. But all HIV-infected children with incomplete baseline records such as CD4 cell count, WHO clinical stage and the first date of occurrence of event as well as transfer in from other facilities and having pneumonia at the time of ART initiation were excluded.
Sample Size Determination and Sampling Procedures
To determine the required sample size, the authors considered both objectives to calculate the largest sample size needed. For the first objective, the single-population proportion formula was used to calculate the sample size by considering the estimated incidence proportion of pneumonia among HIV-infected children taken from a study done in Debre Markos referral hospital (30%),18 which yielded 356. For the second objective of this study, sample size was determined using double population proportion formula considering predictor variables (CD4 count, ART adherence, WHO clinical stage, past OI prophylaxis) from a study conducted at Debre Markos referral hospital.18 By using Epi info version 7.2.4.0 statistical calculator computer software assuming 95% confidence interval, power of 80% and one-to-one ratio of exposed and unexposed group and gave the maximum sample size of 92. Therefore, 356 from the first objective was considered as the final sample size for this study. After identifying the list of 530 pediatric population who started ART at public health facilities in Bahir Dar city from January 1, 2013 to December 30, 2020, all their medical registration numbers were extracted from SMART care of the selected health institutions and a sampling frame was constructed. Finally, study unit from the frame was selected by simple random sampling using a computer generated system.
Study Variables
The dependent variable was incidence of pneumonia and independent variables were baseline sociodemographic predictors (age, sex, residence, family size, the live status of the parents, and occupation of the parent or caregiver), baseline clinical and laboratory-related predictors (functional status, developmental status, weight for age, BMI for age, weight for height, height for age, WHO clinical stage, CD4 count or %, recent viral load, and Hgb level), and treatment-related predictors (history of CPT, ART adherence, immunization status, and treatment failure).
Operational Definition
Events
Pneumonia cases were identified based on EFMOH guidelines for pediatric HIV/AIDS care and treatment.
Censored
Lost, transferred out, dropped out, died due to another cause, and completed the follow-up time before the occurrence of an event.
According to this study, pneumonia was defined as at least two of the following signs and symptoms with or without chest x-ray confirmation.
Bacterial Pneumonia
Chest in-drawing, tachypnea, grunting and presence of danger signs in young children. In older children: sudden onset of cough, sputum production, chest pain, fever and/or shortness of breath. History of acute symptoms presented over days to a few weeks and consolidation in the affected lung or lungs.19
Pneumocystis Pneumonia
In infants 2 to 6 months: abrupt onset of fever, tachypnea, dyspnea and cyanosis. In older children: insidious onset of low grade fever, dry cough, dyspnea exacerbated by exertion, tachypnea, tachycardia and scattered rales in the lungs. Typical chest x-ray findings revealing a perihilar interstitial infiltration with tendency to spread outwards.19
Level of ART Adherence
Adherence can be classified according to the percentage calculated from the number of missed pills out of the supplied pills as good, fair, and poor.
Good (≥ 95% adherence) or ≤ 3 missed pills out of 60 pills supply. Fair (85–94% adherence) or between 4 and 8 missed pills out of 60 pills supply. Poor (< 85% adherence) or ≥ 9 missed pills out of 60 pills supply.20
CD4 Cell Count or % Below the Threshold
CD4 cell count < 1500/mm3 or 25% for children aged under 12 months, CD4 cell count < 750/ mm3 or 20% for children aged 12 to 35 months, CD4 cell count < 350/mm3 or 15% for children aged 36 to 59 months, and CD4 cell count < 200/ mm3 or 15% for children aged ≥ 60 months, respectively.21
Underweight
According to WHO curve, weight for age Z score <-2 standard deviation.
Data Collection Tools and Procedures
The data collection tool was based on the Federal Ministry of Health’s ART follow-up and intake form, which is currently in use at ART clinics of Ethiopian hospitals. First, the appropriate data extraction format was prepared in an English version. The data extraction form included sociodemographic characteristics, treatment, clinical, laboratory-related characteristics, and outcome-related information. The children’s chart was retrieved from the chart room after having their MRN from the electronic database. The occurrence of pneumonia was ascertained by reviewing health professionals’ diagnoses or reporting on the patient’s chart. Any laboratory results and other clinical-related tests done at the time of ART initiation were taken as a baseline.
Data Quality Control
One day training was given to data collectors and a supervisor before the actual data collection period. A pretest was performed on 5% of the sample size one week before the actual data collection time at Felege Hiwot Comprehensive Specialized Hospital. Based on pretest experience,the variables that do not present were avoided. The data were collected by three Bsc nurses. One health officer who has experience in HIV care and follow-up was recruited to continuously supervise the data collectors. Additionally, the data were checked for completeness and consistency by the principal investigator.
Data Processing and Analysis
After the completeness and consistency were checked, the collected data were coded and entered into EPI data version 4.6. Next, they were exported to STATA version 14 for analysis. The assumption of the Cox proportional hazard regression model was checked by running a global test based on the scaled Schoenfeld residuals test. Model goodness of fit was also checked by the Cox–Snell residual test. Multi-collinearity was computed using variance inflation factor and correlation coefficient. Descriptive statistics were computed as frequency, percentage, and median and results were displayed using tables and graphs. Outcomes of each participant were dichotomized into censored or pneumonia and incidence rate was calculated for the entire period. The pneumonia-free survival time was estimated by using the Kaplan–Meier (KM) survival curve. Pneumonia-free survival time between different categorical variables was compared using KM plot and log rank test. The bivariable Cox PH model was employed to check variables that have P-value < 0.25. Then, variables with this value were selected for multivariable Cox PH regression model. Hazard ratio with a 95% confidence interval and p-value < 0.05 was used to measure association and to consider statistically significant predictors of pneumonia. WHO Anthro and Anthroplus software programs were used to assess nutritional status of the participants.
Missing data analysis for some variables was computed. After the pattern of missing data was checked and Little’s test was done, missing mechanism of data was identified. Next, by using multiple imputations the data were imputed and pooled into a new complete dataset.
Results
Baseline Sociodemographic Characteristics of the Child and Parents or Child’s Caregiver Information
In this study, among HIV-infected children on ART from January 1, 2013 to December 30, 2020, a total of 356 medical records of children were retrieved. Of these, 14 charts were excluded due to the exclusion criteria and the remaining 342 charts of the children were included in this study. Among those children, slightly more than half (51.46%) of the children were male. Majority (40.35%) of the children were in the age group of 5 to 9 years. The median age of the participants at the ART initiation was 8 years (IQR=5, 11). The highest proportion of pneumonia (10.23%) was seen among the 10 to 14 year age group and among children living in urban areas (17.25%) (Table 1).
 |
Table 1 Baseline Sociodemographic Characteristics of HIV-Infected Children at Public Health Institutions in Bahir Dar City, Northwest Ethiopia from January 1, 2013 to December 30, 2020 (n=342) |
Baseline Clinical and Laboratory Related Information
The majority (71.35%) and 80.12% of children were classified as normal weight and CD4 cell count above the threshold, respectively. The incidence rates of pneumonia among children categorized as underweight, WHO clinical stages III and IV, and detected viral load were 13.88, 15.65, and 17.48 per 100 PY of observation, respectively (Table 2).
 |
Table 2 Baseline Clinical and Laboratory Related Information of HIV-Infected Children at Public Health Institutions in Bahir Dar City, Northwest Ethiopia from January 1, 2013 to December 30, 2020 (n=342) |
Treatment Related Information
The highest proportion (81.87%) of the children had no treatment failure during the follow-up period. Children who did not receive co-trimoxazole preventive therapy had an incidence rate of 21.81 cases per 100 PY of observation (Table 3).
 |
Table 3 Treatment-Related Information of HIV-Infected Children at Public Health Institutions in Bahir Dar City, Northwest Ethiopia from January 1, 2013 to December 30, 2020 (n=342) |
Incidence of Pneumonia During Follow-Up
The study participants were followed for a minimum of 0.96 months and a maximum of 86.3 months. The total person month of the cohort was 15,300.067 child-months of observation and the total person year of the cohort was also 1256.679 child-years of observation. From 342 study participants, 70 (20.47%) developed pneumonia and the remaining 272 (79.5%) were censored observation. Of these, 60 (85.71%) pneumonia cases were bacterial pneumonia and the remaining were pneumocystis pneumonia.
From all participants followed, about 59.9%, 3.8% and 14.6% were alive beyond the study period, deceased and transferred out, respectively (Figure 1). This study found that the incidence of pneumonia among HIV-infected children was 5.57 (95% CI: 4.4, 7.0) per 100 child-years of observation. As this study indicated, the incidence of pneumonia among HIV-infected children within the first year was 8.5 (95% CI: 5.8, 12.4) per 100 child-years of observation.
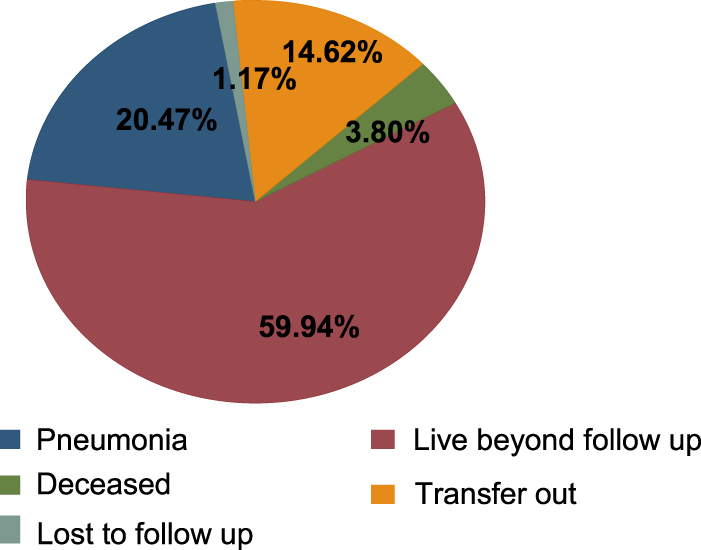 |
Figure 1 Outcome status of HIV-infected children at public health institutions in Bahir Dar city, Northwest Ethiopia from January 1, 2013 to December 30, 2020 (n=342). |
The overall pneumonia-free probability among HIV-infected children remained 68% (95% CI: 54.4, 78) and survival was above the median (Figure 2).
 |
Figure 2 Overall Kaplan–Meier curve of pneumonia-free survival probability of HIV-infected children at public health institutions in Bahir Dar city, from January 1, 2013 to December 30, 2020 (n=342). |
Predictors of Pneumonia Among HIV-Infected Children on ART
The Cox proportional hazard model was used to identify predictors of pneumonia among HIV-infected children. In bivariable Cox regression, sex of the child, family number, level of ART adherence, history of cotrimoxazole preventive therapy, immunization, WHO clinical stage, CD4 cell count, weight for age, height for age, hemoglobin level, treatment failure, recent viral load, and live status of the parents were variables eligible for multivariable Cox regression at p-value < 0.25. In multivariable analysis, history of cotrimoxazole preventive therapy, baseline WHO clinical stage, baseline weight for age, and recent viral load were found to be significant predictors of pneumonia among HIV-infected children. This study found that HIV-infected children who did not take cotrimoxazole preventive therapy during follow-up were 3 times (AHR: 3, 95% CI: 1.40, 6.44) more likely to develop pneumonia than those children who took cotrimoxazole preventive therapy. Children presenting with WHO clinical stages III and IV were nearly 3 times (AHR: 2.8, 95% CI: 1.30, 6.04) more likely to develop pneumonia as compared to those children with stages I and II. The risk of developing pneumonia among children who started ART underweight was 2.5 times (AHR: 2.6, 95% CI: 1.41, 4.86) higher as compared to those children who started ART with normal weight. This study also found that the hazard of developing pneumonia among children with detected viral load was about 6 times (AHR: 5.9, 95% CI: 2.53, 14.06) higher as compared to those children with recent undetected viral load (Table 4).
 |
Table 4 Bivariable and Multivariable Cox Regression Analysis of Predictors of Pneumonia Among HIV-Infected Children at Public Health Institutions in Bahir Dar City, Northwest Ethiopia from January 1, 2013 to December 30, 2020 (n=342) |
Discussion
This retrospective cohort study was conducted to assess the incidence and predictors of pneumonia among HIV-infected children who started ART at public health institutions in Bahir Dar city. This study showed that the proportion of pneumonia among HIV-infected children who started ART at public health institutions in Bar Dar City was 20.47% (95% CI: 16.5, 25). This finding was lower than the study conducted in Debre-Markos referral hospital that revealed the proportion of pneumonia was 30%.18 The difference might be due to the previous study’s length of follow-up period, which was 14 years, single study setting and sample size difference. As this study revealed, bacterial pneumonia is higher proportion than pneumocystis pneumonia, which is in agreement with the study conducted in India.22 This is perhaps because bacterial pneumonia is the most frequent opportunistic infection due to lower immunity in HIV-patients and increased bacteria in the blood. In addition to this, the incidence of pneumocystis pneumonia has declined with the wide use of combined antiretroviral therapy and prophylaxis. The declined incidence of PCP might be also due to limited diagnostic options.
The overall incidence of pneumonia among HIV-infected children in this study was 5.57 per 100 child-years of observation, which was consistent with the study done in Northern India23 but higher than the studies from the United States (3.32 per 100 person-years)13 and Europe (0.54 per 100 person-years).24 The possible explanations for this difference might be due to developed countries having more advanced technologies for diagnosis, prevention, and management of infections than developing countries. However, this finding is lower than the studies conducted in Spain (13.7 per 100 child-years)25 and Latin America (8.1 per 100 person-years).14 The reason for variation with the study in Spain might be due to study population difference since it included HIV-infected children less than 17 years of age and the study included a arger sample size (1307) than the current study. The difference with the study in Latin America might be due to the time period of the study and the longitudinal behavior of the study. Moreover, the current well-organized HIV prevention, treatment and care for HIV-infected children might make a difference. According to this study the incidence of pneumonia among HIV-infected children was higher within the first year of ART initiation, which was in-line with the study done in Uganda,26 in resource-limited settings,27 and in Asia.28 This may be due to the fact that patients have low immunity and low awareness about adherence to HAART at ART initiation time.
This study found that the risk of developing pneumonia among HIV-infected children who took cotrimoxazole preventive therapy prophylaxis was low as compared to those HIV-infected children who did not take CPT. Retrospective study in Ethiopia indicated that cotrimoxazole preventive therapy is a feasible, cost-effective, and safe way of using cotrimoxazole to reduce the incidence of opportunistic infections.29 Another prospective study, conducted in South Africa, revealed that CPT reduces HIV-related morbidity and hospitalization not only by preventing pneumocystis pneumonia but also reducing the incidence of bacterial infection.30 According to Ethiopian ART guideline, early initiation of CPT for HIV-infected children is recommended to prevent pneumocystis pneumonia, bacterial infections, toxoplasmosis gondii and protozoal infections.31
As the current study indicated, children who started ART with the baseline WHO stages III and IV were more likely to develop pneumonia as compared to those children who started ART with the baseline WHO clinical stages I and II. This was similar to the studies done in Asia28 and India.23 Another similar study also observed in Nigeria showed that advanced baseline WHO clinical stage is an independent risk factor for the occurrence of infections.32 This could be because of lower immunity with advanced WHO staging which increases the occurrence and recurrence of opportunistic infections.33 This is explained by as the immune status of the patient living with HIV infection becomes weaker, the HIV clinical stage gets higher.34 Therefore, stage I and II patients have stronger immunity than stage III and IV patients who have moderate and severe opportunistic infections, respectively.
This study also found that the risk of developing pneumonia among HIV-infected children who started ART underweight was higher as compared to those HIV-infected children who started ART with normal weight. This finding is supported by studies done in Kenya,35 Uganda,36 and in Asia.28 This could be due to the fact that malnutrition is the major cause of immune deficiency. It elicits dysfunctions in the immune system and promotes increased vulnerability of the host to infections.37 In other words, it might be due to the fact that infection also contributes to malnutrition due to appetite loss, which leads to inadequate dietary intake resulting in weight loss, lowered immunity, mucosal damage, invasion by pathogens and impaired growth and development in children.
Moreover, the hazard of developing pneumonia among children with detected viral load was much higher as compared to children with undetected viral load. This was similar to the studies done in Denmark38 and the United States.13 The study in Brazil has shown that detectable viral load doubled the risk of pneumonia among HIV-infected children (AHR: 2.2).16 This could be explained by the fact that the higher the viral load, then the faster the CD4 cell count will fall, resulting in the greater risk of infections.39
A surprising result of this study was the absence of significant association between CD4 cell count and pneumonia. This finding is consistent with the study conducted in Indonesia.40 In contrast to this, various studies have shown worse disease severity and an increased frequency of opportunistic infections when CD4 cell levels are below the threshold.41,42 This discrepancy might be attributable to the presence of high levels of sustained adherence to HAART necessary to improve the immunological and clinical outcomes of the HIV-infected children.
Therefore, this study implies that even though the government strives to ensure healthy lives and promote well-being of all HIV-infected patients by preventing, diagnosing, and treating opportunistic infections, pneumonia remains to be a cause of morbidity among HIV-infected children.
Limitation
This study is not without limitations. The data for this study was obtained from charts. Therefore, some variables could not be found such as parents’ educational status, income, and cigarette smoking behavior that could be potential predictors of the event. As is common in resource-limited settings, the diagnostic options such as bacteriologic confirmation were limited, which may potentially lead to misclassification. A limited previous study done in Ethiopia makes comparison and discussions difficult in the local context.
Conclusion
This study found that among HIV-infected children who started ART at public health facilities in Bahir Dar city, two from ten children developed pneumonia during follow-up time. As this study showed, predictors such as not taking past cotrimoxazole preventive therapy, being underweight at baseline, baseline advanced WHO clinical stage (III and IV), and detected viral load were predictors of pneumonia among HIV-infected children.
Abbreviations
ART, Antiretroviral Therapy; BMI, Body Mass Index; CAP, Community Acquired Pneumonia; CMV, Cytomegalo Virus; CPT, Cotrimoxazole Preventive Therapy; EFMOH, Ethiopian Federal Ministry of Health; FU, Follow-Up; HAART, Highly Active Antiretroviral Therapy; Hgb, Hemoglobin; HIV, Human Immunodeficiency Virus; IPD, Invasive Pneumococcal Disease; KM, Kaplan–Meier; LRTI, Lower Respiratory Tract Infection; MRN, Medical Recording Number; NGOs, Non-Governmental Organizations; OIs, Opportunistic Infections; PCP, Pneumocystis Pneumonia; PH, Proportional Hazard; PMTCT, Prevention of Mother to Child Transmission; PY, Person-Year; SARI, Severe Acute Respiratory Infection; SDG, Sustainable Development Goal; SMART, Strategies for Management of Antiretroviral Therapy.
Data Sharing Statement
Data will be available upon request from the corresponding author.
Ethical Considerations
In order to conduct this research, the authors tried to address the Declaration of Helsinki Ethical principles for medical research. First, ethical clearance was obtained from Bahir Dar University, College of Medicine and Health Sciences, school of health sciences with Ethical Review Board number (CMHS/IRB 01-008) decided on the date February 26, 2021. Then, a letter was written to each study institution in Bahir Dar city by Bahir Dar University. A supporting letter was obtained from each selected health facilities general manager, health centers head and coordinators. As this was a retrospective study, informed consent from an individual patient was not requested because the authors had no physical contact with them and the data were collected from their medical charts after their discharge from the health institutions. Information in the data extraction was anonymous. The confidentiality of the information was kept throughout the study process and the information was used only for the study purpose.
Acknowledgments
Authors would like to acknowledge Bahir Dar University and Dire Dawa University. Authors also thank data collectors, supervisors, data clerks, and head of health institutions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no competing interests in this work.
References
1. Jeena PM. Respiratory Diseases Amongst HIV Infected Children. HIV Infection in Children and Adolescents: Springer; 2020:55–72.
2. Pandey A, Galvani AP. The burden of childhood pneumonia in India and prospects for control. Lancet Child Adolescent Health. 2020;4(9):643–645. doi:10.1016/S2352-4642(20)30238-8
3. Macpherson L, Ogero M, Akech S, et al. Risk factors for death among children aged 5–14 years hospitalised with pneumonia: a retrospective cohort study in Kenya. BMJ Global Health. 2019;4(5):e001715. doi:10.1136/bmjgh-2019-001715
4. McAllister DA, Liu L, Shi T, et al. Global, regional, and national estimates of pneumonia morbidity and mortality in children younger than 5 years between 2000 and 2015: a systematic analysis. Lancet Global Health. 2019;7(1):e47–e57. doi:10.1016/S2214-109X(18)30408-X
5. Theodoratou E, McAllister DA, Reed C, et al. Global, regional, and national estimates of pneumonia burden in HIV-infected children in 2010: a meta-analysis and modelling study. Lancet Infect Dis. 2014;14(12):1250–1258. doi:10.1016/S1473-3099(14)70990-9
6. Ayuk AC, Ubesie AC, Iloh KK, et al. Pattern of respiratory diseases among human immunodeficiency virus-infected children in Enugu, Nigeria. Indian J Child Health. 2019;2:287–291.
7. Rabie H, Marais BJ. Tuberculosis and Other Opportunistic Infections in HIV-Infected Children. Viral Infections in Children, Volume I. Springer; 2017:101–124.
8. Punpanich W, Groome M, Muhe L, Qazi SA, Madhi SA. Systematic review on the etiology and antibiotic treatment of pneumonia in human immunodeficiency virus-infected children. Pediatr Infect Dis J. 2011;30(10):e192–e202. doi:10.1097/INF.0b013e31822d989c
9. Dembele BPP, Kamigaki T, Dapat C, et al. Aetiology and risks factors associated with the fatal outcomes of childhood pneumonia among hospitalised children in the Philippines from 2008 to 2016: a case series study. BMJ open. 2019;9(3):e026895. doi:10.1136/bmjopen-2018-026895
10. Dayie NT, Baffuor-Asare M, Labi A-K, et al. Epidemiology of pneumococcal carriage among HIV-infected individuals in the conjugate vaccine era: a study in Southern Ghana. Biomed Res Int. 2019;1:2019.
11. Marangu D, Zar HJ. Childhood pneumonia in low-and-middle-income countries: an update. Paediatr Respir Rev. 2019;32:3–9. doi:10.1016/j.prrv.2019.06.001
12. Haileamlak A, Hagos T, Abebe W, Abraham L, Asefa H, Teklu AM. Predictors of Hospitalization among Children on ART in Ethiopia: a Cohort study. Ethiop J Health Sci. 2017;27(1):53–62. doi:10.4314/ejhs.v27i1.6S
13. Steenhoff AP, Josephs J, Rutstein RM, et al. Incidence of and risk factors for community acquired pneumonia in US HIV-infected children, 2000–2005. AIDS. 2011;25(5):717. doi:10.1097/QAD.0b013e3283440583
14. Alarcón JO, Freimanis-Hance L, Krauss M, et al. Opportunistic and other infections in HIV-infected children in Latin America compared to a similar cohort in the United States. AIDS Res Hum Retroviruses. 2012;28(3):282–288. doi:10.1089/aid.2011.0057
15. Mussini C, Galli L, Lepri AC, et al. Incidence, timing, and determinants of bacterial pneumonia among HIV-infected patients: data from the ICONA Foundation Cohort. JAIDS J Acquired Immune Deficiency Syndromes. 2013;63(3):339–345. doi:10.1097/QAI.0b013e318295ab85
16. Lamas CC, Coelho LE, Grinsztejn BJ, Veloso VG. Community-acquired lower respiratory tract infections in HIV-infected patients on antiretroviral therapy: predictors in a contemporary cohort study. Infection. 2017;45(6):801–809. doi:10.1007/s15010-017-1041-0
17. Huson MA, Stolp SM, van der Poll T, Grobusch MP. Community-acquired bacterial bloodstream infections in HIV-infected patients: a systematic review. Clin Infect Dis. 2014;58(1):79–92. doi:10.1093/cid/cit596
18. Melkamu MW, Gebeyehu MT, Afenigus AD, et al. Incidence of common opportunistic infections among HIV-infected children on ART at Debre Markos referral hospital, Northwest Ethiopia: a retrospective cohort study. BMC Infect Dis. 2020;20(1):1–12. doi:10.1186/s12879-020-4772-y
19. Ethiopian Federal Ministery of Health. Guidelines for Paediatric HIV/AIDS Care and Treatment in Ethiopia. Ethiopian Federal Ministery of Health; 2014.
20. Ethiopian Ministry Of Health(EMOH). National Comprehensive HIV Care and Treatment Training for Health Care Providers. Ethiopian Ministry Of Health(EMOH); 2014.
21. World Health Organization. Antiretroviral Therapy of HIV Infection in Infants and Children: Towards Universal Access: Recommendations for a Public Health Approach-2010 Revision. World Health Organization; 2010.
22. Mehta AA, Kumar VA, Vithalani K, Patel K. Clinico epidemiological profile of HIV in Patients with respiratory infections and Tuberculosis in Western India. J Clinic Diag Res. 2011;5:206–209.
23. Dhaka G, Sherwal B, Saxena S, Rai Y, Chandra J. Current trends in opportunistic infections in children living with HIV/AIDS in a tertiary care hospital in northern India. Indian j Sex Trans Dis AIDS. 2017;38(2):142. doi:10.4103/2589-0557.216992
24. Søgaard O, Reekie J, Ristola M, et al. Severe bacterial non-aids infections in HIV-positive persons: incidence rates and risk factors. J Infection. 2013;66(5):439–446. doi:10.1016/j.jinf.2012.12.012
25. Micheloud D, Álvaro-meca A, Jensen J, Díaz A, Resino S. Trend of pneumonia incidence among children infected with HIV in the era of highly active antiretroviral therapy. Pediatr Infect Dis J. 2012;31(6):599–601. doi:10.1097/INF.0b013e3182501cd4
26. Weissberg D, Mubiru F, Kambugu A, et al. Ten years of antiretroviral therapy: incidences, patterns and risk factors of opportunistic infections in an urban Ugandan cohort. PLoS One. 2018;13(11):e0206796. doi:10.1371/journal.pone.0206796
27. Curtis AJ, Marshall CS, Spelman T, et al. Incidence of WHO stage 3 and 4 conditions following initiation of anti-retroviral therapy in resource limited settings. PLoS One. 2012;7(12):e52019. doi:10.1371/journal.pone.0052019
28. Prasitsuebsai W, Kariminia A, Puthanakit T, et al. Impact of antiretroviral therapy on opportunistic infections of HIV-infected children in the TREAT Asia pediatric HIV observational database. Pediatr Infect Dis J. 2014;33(7):747. doi:10.1097/INF.0000000000000226
29. Sisay M, Bute D, Edessa D, et al. Appropriateness of Cotrimoxazole prophylactic therapy among HIV/AIDS patients in public hospitals in eastern Ethiopia: a retrospective evaluation of clinical practice. Front Pharmacol. 2018;9:727. doi:10.3389/fphar.2018.00727
30. Zar HJ, Workman L, le Roux SM, et al. A randomized controlled trial of intermittent compared with daily cotrimoxazole preventive therapy in HIV-infected children. Aids. 2010;24(14):2225–2232. doi:10.1097/QAD.0b013e32833d4533
31. Ethiopian Ministry Of Health(EMOH). National Guidelines for Comprehensive HIV Prevention, Care and Treatment. Ethiopian Ministry Of Health(EMOH); 2017.
32. Iroezindu M, Ofondu E, Hausler H, Van Wyk B. Prevalence and risk factors for opportunistic infections in HIV patients receiving antiretroviral therapy in a resource-limited setting in Nigeria. J AIDs Clin Res. 2013;3:002.
33. Bhuvana KB, Hema NG, Patil RT. Prevalence and risk factors for opportunistic infections in HIV patients who developed adverse drug reactions (ADRs) to antiretroviral therapy (ART) in a tertiary-care teaching hospital. National J Physiol Pharm Pharmacol. 2015;5(3):200–206. doi:10.5455/njppp.2015.5.0301201517
34. Praharaj BR, Agarwalla S. Opportunistic infections in HIV infected children and its correlation with CD4 count. Int J Contemporary Pediatrics. 2017;4(5):1743. doi:10.18203/2349-3291.ijcp20173777
35. Ásbjörnsdóttir KH, Slyker JA, Weiss NS, et al. Breastfeeding is associated with decreased pneumonia incidence among HIV-exposed, uninfected Kenyan infants. AIDS. 2013;27(17):2809. doi:10.1097/01.aids.0000432540.59786.6d
36. Tam P-YI, Wiens MO, Kabakyenga J, Kiwanuka J, Kumbakumba E, Moschovis PP. Pneumonia in HIV-exposed and infected children and association with malnutrition. Pediatr Infect Dis J. 2018;37(10):1011. doi:10.1097/INF.0000000000001971
37. Duggal S, Chugh TD, Duggal AK. HIV and malnutrition: effects on immune system. Clin Dev Immunol. 2012;2012.
38. Harboe ZB, Larsen MV, Ladelund S, et al. Incidence and risk factors for invasive pneumococcal disease in HIV-infected and non-HIV-infected individuals before and after the introduction of combination antiretroviral therapy: persistent high risk among HIV-infected injecting drug users. Clin Infect Dis. 2014;59(8):1168–1176. doi:10.1093/cid/ciu558
39. Brennan AT, Maskew M, Sanne I, Fox MP. The interplay between CD 4 cell count, viral load suppression and duration of antiretroviral therapy on mortality in a resource‐limited setting. Trop Med Int Health. 2013;18(5):619–631. doi:10.1111/tmi.12079
40. Masri SH. CD4 T-lymphocyte cell counts and pneumonia in HIV children. Qanun Medika Med J Med Muhammadiyah Surabaya. 2018;2:1. doi:10.30651/qm.v2i01.654
41. Jadhav VM, Gabhale YR, Lala MM, Shah ND, Manglani MV. A study of clinical spectrum of opportunistic infections in HIV infected children and its correlation with CD4 count and anti-retroviral therapy. Int J Contemporary Pediatrics. 2017;4(4):1485. doi:10.18203/2349-3291.ijcp20172691
42. Borle M, Sunkoj Y. Opportunistic Infection among HIV Infected Children and Their CD4 Cell Correlates. IOSR J Dent Med Sci. 2016;15(3):584.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.