Back to Journals » Clinical Ophthalmology » Volume 17
Incidence of Epiretinal Membrane Formation After Pars Plana Vitrectomy for Giant Retinal Tear-Associated Retinal Detachment
Authors Lee IJ ![]() , Benjamin JE, Ghorayeb GR
, Benjamin JE, Ghorayeb GR
Received 8 February 2023
Accepted for publication 11 May 2023
Published 17 May 2023 Volume 2023:17 Pages 1415—1420
DOI https://doi.org/10.2147/OPTH.S407699
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ivan J Lee, James E Benjamin, Ghassan R Ghorayeb
Department of Ophthalmology, West Virginia University Eye Institute, Morgantown, WV, USA
Correspondence: Ivan J Lee, Department of Ophthalmology, West Virginia University Eye Institute, 1 Medical Center Drive, Morgantown, WV, 26506, USA, Tel +1 304-598-4820, Email [email protected]
Objective: To report the incidence of postoperative epiretinal membrane (ERM) formation after primary pars plana vitrectomy (PPV) for giant retinal tear associated retinal detachment (GRT-RD) repair as well as its clinical characteristics and visual outcomes at a level one trauma and tertiary referral academic center.
Patients and Methods: Patients with primary RD repair for GRT-RD at West Virginia University from September 2010 to July 2021 were identified using the ICD-10 codes (H33.031, H33.032, H33.033 and H33.039). Imaging studies including optical coherence tomography (OCT) were manually reviewed pre- and post-operatively for ERM formation after PPV for GRT-RD repair in patients who underwent PPV or combined PPV and scleral buckle (SB). Univariate analysis was performed to analyze clinical factors for ERM formation.
Results: The study included 17 eyes of 16 patients who underwent PPV for GRT-RD. Postoperative ERM was observed in 70.6% (13 of 17 eyes) of the patients. Anatomic success was achieved in all patients. The mean (range) preoperative and final best corrected visual acuity (BCVA) in logMAR units by macula status was 0.19 (0– 0.5) and 0.28 (0– 0.5) for macula-on and 1.7 (0.5– 2.3) and 0.7 (0.2– 1.9) for macular-off GRT-RDs. Clinical variables including use of medium-term tamponade with perfluorocarbon liquid (PFCL), cryopexy, endodiathermy, number of tears or total clock hours of tears did not correlate with an increased risk of ERM formation.
Conclusion: Post-vitrectomized eyes for GRT-RD repair have a significantly higher incidence of ERM formation, nearing 70% in our study. Surgeons may consider prophylactic ILM peel at the time of removal of tamponade agents or weigh in ILM peel at the time of primary repair, a more challenging surgical technique in our opinion.
Keywords: giant retinal detachment, post-operative epiretinal membrane formation
Plain Language Summary
What is already known on this topic: Incidence of epiretinal membrane (ERM) formation has been reported in literature after pars plana vitrectomy (PPV) for a routine rhegmatogenous retinal detachment (RRD) repair, but not for giant-retinal tear associated retinal detachment (GRT-RD).
What this study adds: Incidence of ERM after PPV for GRT-RD is higher than a routine RRD repair.
How this study might affect research, practice or policy: ILM peeling at the time of primary repair for GRT-RD can be more strongly considered to prevent post-operative ERM formation in patients with GRT-RD.
Introduction
A giant retinal tear (GRT) is a full-thickness circumferential retinal break that involves more than three clock hours or 90 degrees of the retina associated with posterior vitreous detachment.1 The annual incidence of GRTs is estimated to be between 0.094 and 0.15 per 100,000 people, comprising about 1.5% of all rhegmatogenous retinal detachments (RRD).2 Most GRTs are idiopathic,3 but are also associated with trauma, high myopia, Marfan syndrome, Ehlers–Danlos syndrome and hereditary vitreoretinopathies including Stickler syndrome.4–6
GRT-associated rhegmatogenous retinal detachments (GRT-RD) are surgically challenging to manage due to the frequently rolled posterior edge of the retinal flap and high incidence of proliferative vitreoretinopathy (PVR) that increases the chance of redetachment.7,8 With the advent of small-gauge pars plana vitrectomy (PPV), perfluorocarbon liquids (PFCL), silicone oil (SO), faster-speed cutters and wide-field visualization system,9–12 the final anatomic success has been reported to be between 81.8% and 100%.2 Despite the high anatomic success, final visual outcome may be limited due to postoperative complications of PPV for RD repair including epiretinal membrane (ERM).13–15
An ERM is a semitransparent membranous tissue that may occur after the retinal pigment epithelial cells migrate through a retinal break, on a scaffold of internal limiting membrane (ILM) composed of the footplate of Muller cells.13,15 The incidence of ERM formation after PPV for a routine RRD repair is reported between 6% and 28.5% and primary ILM peeling at the time of RRD repair has been shown to prevent ERM formation.12,14–17 While previous studies have shown that a large retinal tear may correlate with an ERM formation,17,18 a report on the incidence of postoperative ERM formation after primary vitrectomy for GRT-RD repair is scarce and yet to be highlighted. We report a retrospective, single-institution, consecutive case series evaluating the incidence of postoperative ERM after primary PPV for GRT-RD repair as well as clinical characteristics and visual outcomes at a level-one trauma and tertiary referral academic center.
Methods
Patients with primary RD repair for GRT-RD at West Virginia University from September 2010 to July 2021 were identified using the ICD-10 codes (H33.031, H33. 032, H33.033 and H33.039). Patient who had been followed for at least 90 days since the initial repair were included in this study. Patients with history of prior vitrectomy, scleral buckle, presence of ERM at diagnosis, GRT without associated RD, membrane peel at the time or prior to the initial repair, diabetic retinopathy, retinal vein occlusion, vitreous hemorrhage, vitreoretinopathy including Stickler syndrome, retinopathy of prematurity (ROP), intravitreal injection of any medication and prior intraocular inflammation or infection were excluded.
Data collected included age at diagnosis, gender, laterality, macula status (on/off), type of repair (primary PPV or combined PPV and scleral buckling (SB)), lens status, location of tears, number of tears, total clock hours of GRT, presence of proliferative vitreoretinopathy (PVR), use of medium-term PFCL, choice of tamponade (SO or perfluoropropane (C3F8)), presence of cystoid macula edema (CME), anatomic success, history of membrane peel when applicable, time in days between the first PPV or PPV/SB and ERM formation when applicable, best-corrected visual acuity (BCVA) at diagnosis, and final BCVA at the most recent visit were collected. A total of 78 patients were reviewed and 17 eyes of 16 patients met the inclusion criteria. Imaging studies including widefield fundus photography and optical coherence tomography (OCT, Spectralis; Heidelberg Engineering, Heidelberg Germany) were manually reviewed pre- and post-operatively. ERM was staged per Govetto et al.19 SPSS 23 software (IBM Corp., Armonk, NY) was used for all statistical analysis including 2-tailed Student’s t-test and chi-square test depending on the nature of the variable. The current study adhered to the tenets of the Declaration of Helsinki. The Institutional Board Review at the West Virginia University did not require patient consent for retrospective review of medical records and all patient data were deidentified during the review.
Results
A total of 17 eyes (right, 11 eyes; left 6 eyes) of 16 patients met the inclusion criteria. The mean age ± standard deviation of patients was 53.1 ± 8.38. The majority of the patients were male (88.2%), and the right eye was more frequently involved with a GRT (64.7%). The mean preoperative BCVA was 0.99 ± 0.89 logarithm of the minimum angle of resolution units (logMAR). Table 1 shows the differences in clinical characteristics of the eyes with and without postoperative ERM. Clinical variables including age, gender, lens status, macula status, PVR at presentation, total clock hours of tears, and number of tears have not shown to be statistically significant for an increased risk of ERM formation in our univariate analysis.
 |
Table 1 Difference in Clinical Variables of the Eyes with and without Postoperative Epiretinal Membrane |
In regard to surgical variables, about two-thirds of the eyes underwent primary PPV without SB, while the other third had a combined PPV with SB. Intraoperative PFCL was used for the majority of cases, but medium-term tamponade with PFCL was employed in about a third of the cases. SO was used as intraoperative tamponade for about 70% of cases, while C3F8 was used for the rest of the eyes. Anatomic success was achieved in all cases. Intraoperative cryopexy and endodiathermy (23.5% and 35.3% of cases, respectively) did not correlate with an increased risk of ERM formation.
In this study, postoperative ERM was observed in 70.6% (13 of 17 eyes) of the patients who were treated with either primary vitrectomy or combined PPV and SB for GRT-RD repair without primary ILM peel. The average time in days for ERM formation after primary repair was 191.08 ± 144.94. Of the 13 patients with ERM, 7 patients (58.3%) had subsequent membrane peel for visually significant ERM and the mean final BCVA was 0.50 ± 0.49 logMAR units. For visual outcome by the macula status at the time of presentation, the mean preoperative/final BCVA (range) was 0.19 (0–0.5)/0.28 (0–0.5) and 1.7 (0.5–2.3)/0.7 (0.2–1.9) for macula-on and macula-off GRT-RDs, respectively (Table 2 and Figure 1).
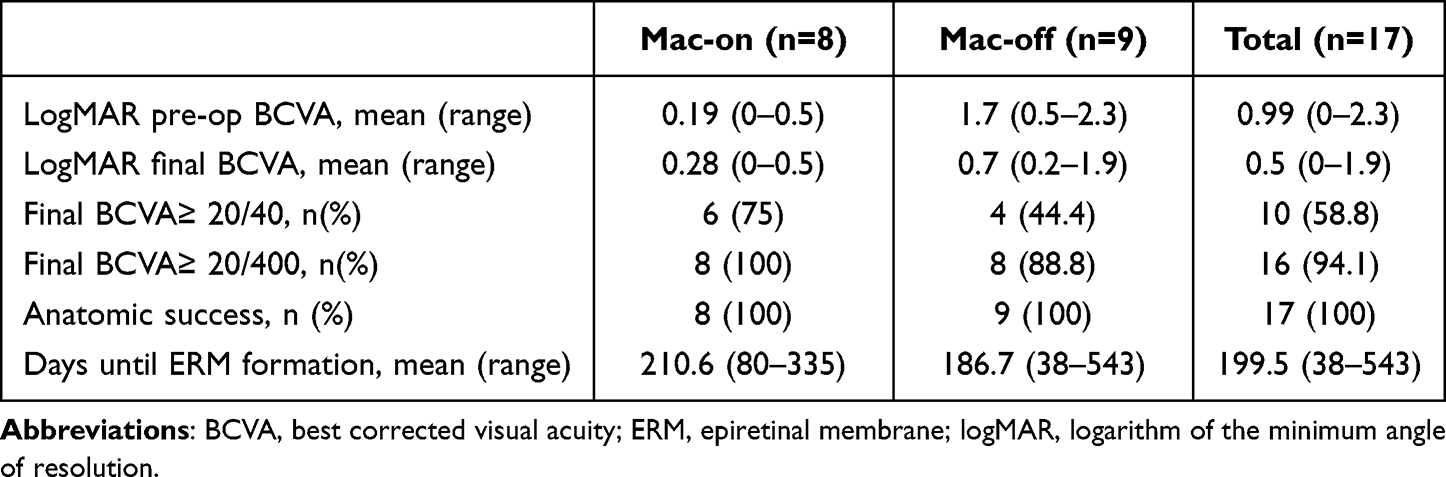 |
Table 2 Anatomic and Functional Visual Outcomes in Patients with Giant Retinal Tear Associated-RD Repair |
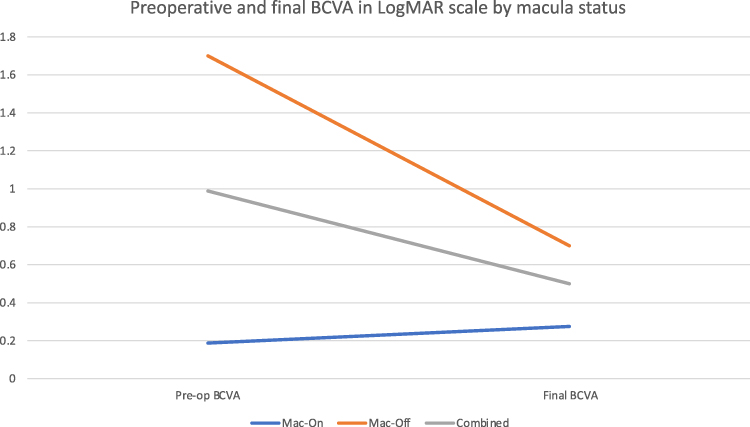 |
Figure 1 Preoperative and final BCVA by macula status. Final BCVA was the visual acuity obtained at the most recent visit. More than half of the patients with ERM required subsequent membrane peel to achieve their final BCVA. |
Discussion
The management of GRT-RD is challenging both intraoperatively and postoperatively. Despite a successful anatomic repair of the detachment, visual recovery may still be undermined due to postoperative complications, the most common of which is ERM formation. The current study finds that postoperative ERM after PPV or combined PPV/SB for GRT-RD repair is 70.6%, a significantly higher incidence when compared to a routine RRD repair with a reported incidence of 12.1% to 30.8%.14,15,17,18,20 One study has shown that the incidence of ERM after PPV for a routine RRD could be as high as 70.3% using en face OCT,21 likely due to its high sensitivity, whereas the current and most of the other studies14,15,17,18,20 have analyzed spectral-domain OCT for presence of ERM. Studies have suggested that epiretinal proliferation has multiple etiologies including RPE cell migration through a full-thickness retinal break, retinal glial cells as well as vitreous components including platelet-derived growth factors, cytokines and blood cells.22–24
The high incidence of ERM formation after PPV for GRT-RD repair in this study corroborates prior studies on the association between giant retinal tear and postoperative ERM formation.17,18 This is likely due to the larger size of the break, allowing the varying types of cells to be released into the vitreous cavity. In addition, GRT’s frequent association with trauma, vitreous hemorrhage and intraoperative cryopexy/endodiathermy use may contribute to more significant intraoperative inflammation. In our study, the size of the retinal break, macula status, number of retinal breaks, intraoperative cryopexy or endodiathermy use did not correlate with higher incidence of ERM formation, while prior studies have shown that older age, use of cryopexy, macular involvement, vitreous hemorrhage and multiple breaks may increase the risk of ERM formation.17,25–27
The current study finds that neither the type of tamponade (SO and C3F8) nor the use of medium-term tamponade with PFCL is associated with postoperative ERM formation despite the necessity for reoperations for removal that may potentially increase the risk of ERM formation.28 More than half of the patients with postoperative ERM have undergone membrane peel (58.3%) for visually significant ERM formation, the rate comparable to prior studies for eyes without primary ILM peel at the time of primary repair with vitrectomy.18,29,30 Primary ILM peel at the time of RRD repair has been shown to protect against ERM formation in multiple studies13,16–18,30 with the average dollars saved by conducting a primary ILM peel to be $615 in a facility setting.30 However, it is the author’s opinion that such primary peel is often challenging to execute in the settings of GRT-RD. When SO or medium-term tamponade with PFCL is used, peeling the ILM at the time of removal of the tamponade agent may be favorable. When the gas tamponade is pursued without primary ILM peel at the time of initial repair, closer monitoring of the ERM progression may be warranted. In our review of patients, two patients had undergone primary ILM peel at the time of GRT-RD repair and therefore excluded from the series to best estimate the incidence of postoperative ERM formation. Neither of the two patients has developed ERM.
There are several limitations to the current study including the nature of a retrospective study and surgical procedures performed by multiple surgeons without predefined criteria. A small sample size lowered the statistical power of the study with strict inclusion criteria in order to estimate the incidence of ERM as best as possible. Additionally, follow-up appointments after the primary repair could be standardized (1 day, 1 week, 1, 3, 6, 12, 24 months after primary repair and OCT obtained at each visit) in order to follow the presence of ERM at specific intervals.
Conclusion
In conclusion, post-vitrectomized eyes for GRT-RD repair have a significantly higher incidence of ERM formation nearing 70% in our study. Surgeons may consider prophylactic ILM peel at the time of removal of tamponade agents (SO or medium term PFCL) or weigh in ILM peel at the time or primary repair, a more challenging surgical technique in our opinion.
Funding
There is no funding to report.
Disclosure
No conflicting relationship exists for any author.
References
1. Kanski JJ. Giant retinal tears. Am J Ophthalmol. 1975;79(5):846–852. doi:10.1016/0002-9394(75)90746-1
2. Shunmugam M, Ang GS, Lois N. Giant retinal tears. Surv Ophthalmol. 2014;59(2):192–216. doi:10.1016/J.SURVOPHTHAL.2013.03.006
3. Ang GS, Townend J, Lois N. Interventions for prevention of giant retinal tear in the fellow eye. Cochrane Database Syst Rev. 2009;(2). doi:10.1002/14651858.CD006909.PUB2
4. Ang GS, Townend J, Lois N. Epidemiology of giant retinal tears in the United Kingdom: the British giant retinal tear epidemiology eye study (BGEES). Investig Ophthalmol Vis Sci. 2010;51(9):4781–4787. doi:10.1167/IOVS.09-5036
5. Ghosh YK, Banerjee S, Savant V, et al. Surgical treatment and outcome of patients with giant retinal tears. Eye. 2004;18(10):996–1000. doi:10.1038/SJ.EYE.6701390
6. Asaria RHY, Kon CH, Bunce C, et al. Adjuvant 5-fluorouracil and heparin prevents proliferative vitreoretinopathy: results from a randomized, double-blind, controlled clinical trial. Ophthalmology. 2001;108(7):1179–1183. doi:10.1016/S0161-6420(01)00589-9
7. Glaser BM. Treatment of giant retinal tears combined with proliferative vitreoretinopathy. Ophthalmology. 1986;93(9):1193–1197. doi:10.1016/S0161-6420(86)33597-8
8. Rodriguez M, Lin J, Townsend JH, et al. Giant retinal tears: clinical features and outcomes of vitreoretinal surgery at a university teaching hospital (2011–2017). Clin Ophthalmol. 2018;12:2053. doi:10.2147/OPTH.S180353
9. Al-Khairi AM, Al-Kahtani E, Kangave D, Abu El-Asrar AM. Prognostic factors associated with outcomes after giant retinal tear management using perfluorocarbon liquids. Eur J Ophthalmol. 2008;18(2):270–277. doi:10.1177/112067210801800216
10. Chang S, Lincoff H, Zimmerman NJ, Fuchs W. Giant retinal tears. Surgical techniques and results using perfluorocarbon liquids. Arch Ophthalmol. 1989;107(5):761–766. doi:10.1001/ARCHOPHT.1989.01070010779046
11. Scott IU, Murray TG, Flynn HW, Feuer WJ, Schiffman JC. Outcomes and complications associated with giant retinal tear management using perfluoro-n-octane. Ophthalmology. 2002;109(10):1828–1833. doi:10.1016/S0161-6420(02)01184-3
12. Goezinne F, La Heij EC, Berendschot TTJM, et al. Low redetachment rate due to encircling scleral buckle in giant retinal tears treated with vitrectomy and silicone oil. Retina. 2008;28(3):485–492. doi:10.1097/IAE.0B013E318150D879
13. Nam KY, Kim JY. Effect of internal limiting membrane peeling on the development of epiretinal membrane after pars plana vitrectomy for primary rhegmatogenous retinal detachment. Retina. 2015;35(5):880–885. doi:10.1097/IAE.0000000000000421
14. Forlini M, Date P, Ferrari LM, et al. Comparative analysis of retinal reattachment surgery with or without internal limiting membrane peeling to prevent postoperative macular pucker. Retina. 2017;38(9):1770–1776. doi:10.1097/IAE.0000000000001775
15. Rao RC, Blinder KJ, Smith BT, Shah GK. Internal limiting membrane peeling for primary rhegmatogenous retinal detachment repair. Ophthalmology. 2013;120(5):1102–1103.e2. doi:10.1016/J.OPHTHA.2012.12.010
16. Ishikawa Y, Hashimoto Y, Saito W, Ando R, Ishida S. Blood flow velocity and thickness of the choroid in a patient with chorioretinopathy associated with ocular blunt trauma. BMC Ophthalmol. 2017;17(1). doi:10.1186/s12886-017-0480-9
17. Ishida Y, Iwama Y, Nakashima H, Ikeda T, Emi K. Risk Factors, Onset, and Progression of Epiretinal Membrane after 25-Gauge Pars Plana Vitrectomy for Rhegmatogenous Retinal Detachment. Ophthalmol Retin. 2020;4(3):284–288. doi:10.1016/J.ORET.2019.10.004
18. Fu Y, Xie T-H, Gu Z-H, Li L-Y, Chen Q, Zhang Y-L. The development of epiretinal membrane following rhegmatogenous retinal detachment repair: incidence, risk factors, and outcomes. Arq Bras Oftalmol. 2021;85:370–376. doi:10.5935/0004-2749.20220032
19. Govetto A, Lalane RA, Sarraf D, Figueroa MS, Hubschman JP. Insights Into Epiretinal Membranes: presence of Ectopic Inner Foveal Layers and a New Optical Coherence Tomography Staging Scheme. Am J Ophthalmol. 2017;175:99–113. doi:10.1016/J.AJO.2016.12.006
20. Gharbiya M, Visioli G, Iannetti L, et al. COMPARISON BETWEEN SCLERAL BUCKLING AND VITRECTOMY IN THE ONSET OF CYSTOID MACULAR EDEMA AND EPIRETINAL MEMBRANE AFTER RHEGMATOGENOUS RETINAL DETACHMENT REPAIR. Retina. 2022;42(7):1268. doi:10.1097/IAE.0000000000003475
21. Matoba R, Kanzaki Y, Doi S, et al. Assessment of epiretinal membrane formation using en face optical coherence tomography after rhegmatogenous retinal detachment repair. Graefes Arch Clin Exp Ophthalmol. 2021;259(9):2503–2512. doi:10.1007/S00417-021-05118-Y
22. Pastor JC, Rojas J, Pastor-Idoate S, Di Lauro S, Gonzalez-Buendia L, Delgado-Tirado S. Proliferative vitreoretinopathy: a new concept of disease pathogenesis and practical consequences. Prog Retin Eye Res. 2016;51:125–155. doi:10.1016/J.PRETEYERES.2015.07.005
23. Feng K, Hu Y, Wang C, et al. Risk factors, anatomical, and visual outcomes of injured eyes with proliferative vitreoretinopathy: eye injury vitrectomy study. Retina. 2013;33(8):1512–1518. doi:10.1097/IAE.0B013E3182852469
24. Cardillo JA, Stout JT, LaBree L, et al. Post-traumatic proliferative vitreoretinopathy. The epidemiologic profile, onset, risk factors, and visual outcome. Ophthalmology. 1997;104(7):1166–1173. doi:10.1016/S0161-6420(97)30167-5
25. Cacioppo V, Govetto A, Radice P, Virgili G, Scialdone A. Premacular membrane formation after scleral buckling for primary rhegmatogenous retinal detachment: prospective study and pathophysiological insights. Br J Ophthalmol. 2019;103(4):481–487. doi:10.1136/BJOPHTHALMOL-2017-311787
26. Katira RC, Zamani M, Berinstein DM, Garfinkel RA. Incidence and characteristics of macular pucker formation after primary retinal detachment repair by pars plana vitrectomy alone. Retina. 2008;28(5):744–748. doi:10.1097/IAE.0B013E318162B031
27. Bonnet M, Fleury J, Guenoun S, Yaniali A, Dumas C, Hajjar C. Cryopexy in primary rhegmatogenous retinal detachment: a risk factor for postoperative proliferative vitreoretinopathy? Graefes Arch Clin Exp Ophthalmol. 1996;234(12):739–743. doi:10.1007/BF00189354
28. Lobes LA, Burton TC. The incidence of macular pucker after retinal detachment surgery. Am J Ophthalmol. 1978;85(1):72–77. doi:10.1016/S0002-9394(14)76668-1
29. Martínez-Castillo V, Boixadera A, Distéfano L, Zapata M, García-Arumí J. Epiretinal membrane after pars plana vitrectomy for primary pseudophakic or aphakic rhegmatogenous retinal detachment: incidence and outcomes. Retina. 2012;32(7):1350–1355. doi:10.1097/IAE.0B013E318242B965
30. Yannuzzi NA, Callaway NF, Sridhar J, Smiddy WE. Internal limiting membrane peeling during pars plana vitrectomy for rhegmatogenous retinal detachment cost analysis, review of the literature, and meta-analysis. Retina. 2018;38(10):2081–2087. doi:10.1097/IAE.0000000000002248
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.