Back to Journals » International Journal of Women's Health » Volume 10
Incidence, characteristics, maternal complications, and perinatal outcomes associated with preeclampsia with severe features and HELLP syndrome
Authors Kongwattanakul K ![]() , Saksiriwuttho P, Chaiyarach S, Thepsuthammarat K
, Saksiriwuttho P, Chaiyarach S, Thepsuthammarat K ![]()
Received 18 March 2018
Accepted for publication 11 May 2018
Published 17 July 2018 Volume 2018:10 Pages 371—377
DOI https://doi.org/10.2147/IJWH.S168569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Kiattisak Kongwattanakul,1 Piyamas Saksiriwuttho,1 Sukanya Chaiyarach,1 Kaewjai Thepsuthammarat2
1Department of Obstetrics and Gynecology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Clinical Epidemiology Unit, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Objective: To determine the incidence of preeclampsia with severe features among pregnant women and evaluate the characteristics, maternal complications, and perinatal outcomes between nonsevere preeclampsia versus preeclampsia with severe features and hemolysis, elevated liver enzyme levels, and low platelet levels (HELLP) syndrome.
Materials and methods: A retrospective descriptive study was conducted at Khon Kaen University’s Srinagarind Hospital, a tertiary care facility in northeast Thailand. The pregnant women who had been diagnosed with preeclampsia according to American College of Obstetricians and Gynecologists guidelines from January 1, 2012 to December 31, 2016 were identified and their medical records were reviewed. Various characteristics were examined to compare maternal complications and perinatal outcomes.
Results: There was a total of 11,199 deliveries during the study period, out of which 213 preeclamptic women were identified. One hundred and seven women (9.6 per 1,000 deliveries) were diagnosed with nonsevere preeclampsia, 90 (8 per 1,000 deliveries) had preeclampsia with severe features, and 16 (1.4 per 1,000 deliveries) had HELLP syndrome. Twenty-one women (9.9%) experienced postpartum hemorrhage; 11 (10.3%) in the nonsevere features preeclampsia group and 10 (9.4%) in the preeclampsia with severe features and HELLP syndrome group. Placental abruption (3 women; 1.4%) and heart failure (1 women; 0.4%) only occurred among women in the preeclampsia with severe features group. Neonatal complications were significantly higher in the preeclampsia with severe features and HELLP syndrome group (low birth weight =35.1% versus 74.3%, p<0.001; birth asphyxia =4.4% versus 18.2%, p=0.001; neonatal intensive care unit admission =7.0% versus 30.9%, p<0.001; neonatal resuscitation =15.8% versus 42.7%, p<0.001). Stillbirths only occurred in cases of preeclampsia with severe features and HELLP syndrome (3 cases, 1.4%). Intrapartum death was higher in cases of preeclampsia with severe features and HELLP syndrome, but without statistical significance (2.6% versus 6.4%, p=0.190).
Conclusion: The incidence of preeclampsia with severe features and HELLP syndrome was 9.5 per 1,000 deliveries. Severe maternal and perinatal outcomes were more commonly observed.
Keywords: preeclampsia, HELLP syndrome, pregnancy induced hypertension, perinatal outcome, preeclampsia with severe features
Introduction
Preeclampsia is a common complication during pregnancy and is also a cause of ~10%–15% of cases of maternal morbidity and mortality,1 such as those involving cardiovascular and cerebrovascular diseases, liver and kidney failure, placental abruption, disseminated intravascular coagulation, and hemolysis, elevated liver enzyme levels, and low platelet levels (HELLP) syndrome.2 Additionally, neonatal morbidity and mortality can result from this condition, as it can cause fetal growth restriction with oligohydramnios, nonreassuring fetal status, preterm birth, low birth weight, severe birth asphyxia, stillbirth, and intrapartum death. The pathophysiology is not yet known. However, it is believed to be caused by placental insufficiency and generalized endothelial dysfunction.3,4
The global incidence of hypertensive disorders in pregnant women during 2002–2012 was ~4.6%, a figure that varied from 2.7%–8.2% by region,5 and the worldwide incidence rate of preeclampsia was ~2.16%.6 These numbers vary according to differences in population characteristics, definitions, and criteria of diagnosis. In Thailand, the incidence of preeclampsia was 2.2% and severe preeclampsia 10.1 per 1,000 deliveries.6 Over the past few decades, there has been an increase in the amount of relevant literature, as well as knowledge, regarding hypertension in pregnancy. In 2013, The American College of Obstetricians and Gynecologists (ACOG) changed the standard diagnostic criteria and definitions of preeclampsia with or without severe features.7 These changes in criteria may result in changes to the incidence rates, perinatal outcomes, and magnitude of difference between preeclampsia with or without severe features.
The primary objective of this study was to determine the incidence of preeclampsia with severe features and HELLP syndrome among pregnant women. Characteristics, maternal complications, and perinatal outcomes were also evaluated to compare with nonsevere preeclampsia, as assessed by the ACOG standard diagnostic criteria and definitions.
Materials and methods
A retrospective descriptive study was conducted at Khon Kaen University’s Srinagarind Hospital, which is a tertiary care facility for northeast Thailand. The pregnant women who had been diagnosed with preeclampsia according to ACOG guidelines from January 1, 2012 to December 31, 2016 were identified and their medical records were reviewed. Pregnant women with uncertain gestational age, fetal abnormalities, incomplete data, or whose data had been lost were excluded from this study. Data were collected and reviewed to confirm diagnosis from medical and labor records. The data collected included baseline characteristics, obstetric data, diagnosis, management, and perinatal outcomes. Incidence of preeclampsia was determined. Various characteristics regarding maternal complications and perinatal outcomes, as well as associated risk factors were compared between women with nonsevere preeclampsia and those with preeclampsia with severe features accompanied by HELLP syndrome.
According to ACOG guidelines, preeclampsia is diagnosed as new-onset hypertension (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg on 2 occasions at least 4 hours apart) after 20 weeks of gestation with or without proteinuria (≥300 mg per 24-hour urine collection, protein/creatinine ratio ≥0.3, or dipstick reading of 1+).
In the absence of proteinuria, preeclampsia with severe features is diagnosed if any of the following conditions are present: 1) severe hypertension (systolic blood pressure of 160 mmHg or higher or diastolic blood pressure of 110 mmHg or higher on 2 occasions at least 4 hours apart while the patient is on bed rest, unless antihypertensive therapy is initiated before this time); 2) thrombocytopenia (platelet count <100,000/μL); 3) impaired liver function (elevated blood levels of liver transaminases to twice the normal concentration); 4) new development of renal insufficiency (elevated serum creatinine >1.1 mg/dL or a doubling of serum creatinine in the absence of other renal disease); 5) pulmonary edema; or 6) new-onset cerebral or visual disturbances. The presence of hemolysis, impaired liver function, and thrombocytopenia is referred to as HELLP syndrome.7 Various characteristics regarding maternal complications (postpartum hemorrhage, blood transfusion, placental abruption, heart failure, and intensive care unit admission) and perinatal outcomes (low birth weight, birth asphyxia, neonatal intensive care unit admission, resuscitation, stillbirth, and intrapartum death), as well as associated risk factors were compared between women with nonsevere preeclampsia and those with preeclampsia with severe features accompanied with HELLP syndrome.
Descriptive statistics including number, percentage, mean, or median with SD were used to describe various characteristics as appropriate, Wilcoxon rank-sum test was performed if data were not normally distributed. The incidence of preeclampsia was reported as per 1,000 deliveries. Various characteristics were compared between patients with nonsevere preeclampsia versus those with preeclampsia with severe features and HELLP syndrome using a chi-square test and Student t-test. A p-value of <0.05 was considered statistically significant. Statistical analysis was carried out by using STATA version 10 (StataCorp LP, College Station, TX, USA). The protocol of this study has been reviewed and approved, and patient consent to review their medical records was not required by the Ethics Committee of Khon Kaen University, as patient data confidentiality was covered based on the Declaration of Helsinki (HE591307).
Results
There were a total of 11,199 deliveries during the study period, from which 213 preeclamptic women were identified. Table 1 shows the baseline characteristics of the pregnant women. Thirty-three of the women (15.5%) were 35 years or older. Approximately half (49.8%) of the women were nulliparous, 23 (11.1%) were obese, 11 (5.2%) were diagnosed preeclampsia during a previous pregnancy, and 47 (22.6%) had family histories of hypertension in first-degree relatives.
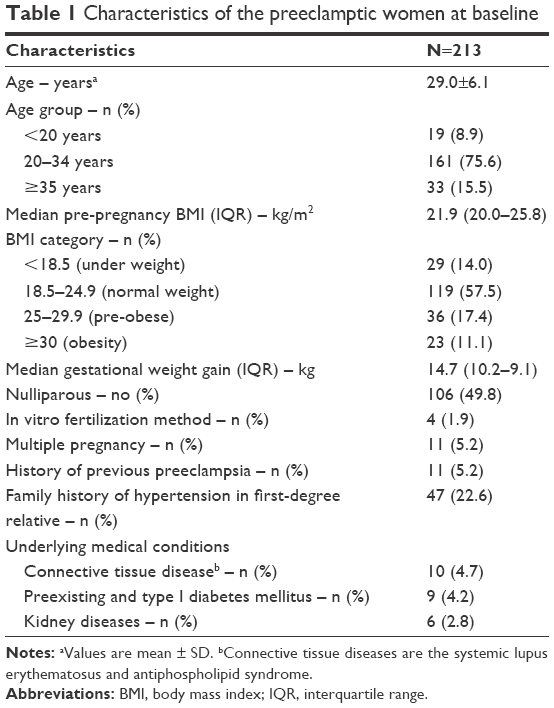 | Table 1 Characteristics of the preeclamptic women at baseline |
Table 2 displays the diagnoses and delivery characteristics of the pregnant women with preeclampsia in this study. The overall incidence of preeclampsia was 19.2 per 1,000 deliveries during the 5-year period of the study. Of the 213 women who were diagnosed with preeclampsia, 107 (50.2%, 9.6 per 1,000 deliveries) were diagnosed with nonsevere feature preeclampsia, 90 (42.3%, 8 per 1,000 deliveries) were diagnosed with preeclampsia with severe features, and 16 (7.5%, 1.4 per 1,000 deliveries) were diagnosed with HELLP syndrome. Fifty-eight women (27.2%) were diagnosed with early-onset preeclampsia (prior to 34 weeks of gestation), and 97 (45.5%) delivered before 37 weeks of gestation. The majority of the women included in this study (139, 65.3%) underwent primary cesarean section. Thirty-four (16%) had nonreassuring fetal status during the intrapartum period. In the preeclampsia with severe features group, 14 women (15.6%) had no proteinuria, 9 had acute renal insufficiency, 3 (3.3%) had impaired liver function, and 2 (2.2%) had new-onset cerebral or visual disturbances.
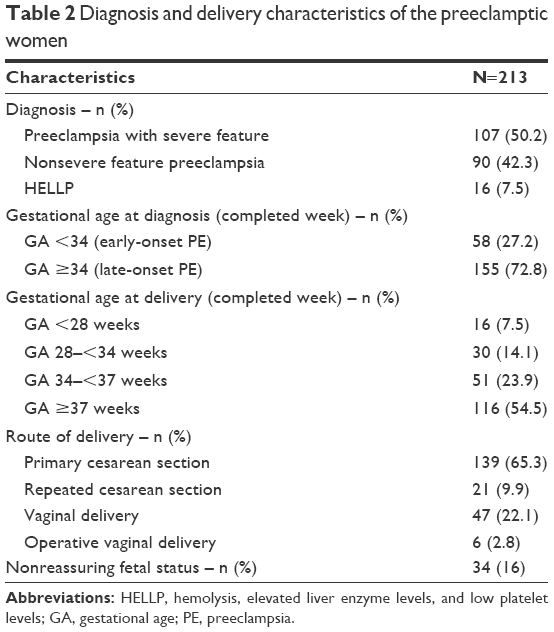 | Table 2 Diagnosis and delivery characteristics of the preeclamptic women |
Table 3 compares various characteristics between nonsevere preeclampsia versus preeclampsia with severe features and HELLP syndrome. The median gestational ages at diagnosis and delivery were different in the nonsevere feature preeclampsia group compared with the preeclampsia with severe features and HELLP syndrome group: 37 versus 34 weeks and 37 versus 35 weeks, respectively. Early-onset preeclampsia occurred in 11.2% of the nonsevere feature preeclampsia cases and 43% of the preeclampsia with severe features and HELLP syndrome cases. Preterm delivery occurred in 23.4% of the nonsevere feature preeclampsia cases and 67.9% of the preeclampsia with severe features and HELLP syndrome cases. Primary cesarean section (64 women, 59.8% in nonsevere feature preeclampsia and 75 women, 70.8% in preeclampsia with severe features and HELLP syndrome) and nonreassuring fetal status (15 women; 20% in nonsevere feature preeclampsia and 29 women; 22.9% in preeclampsia with severe features and HELLP syndrome) did not differ significantly between the 2 groups. Mean birth weight was significantly higher in the nonsevere feature preeclampsia group (2,747.9 versus 1,858.7 g, p<0.001).
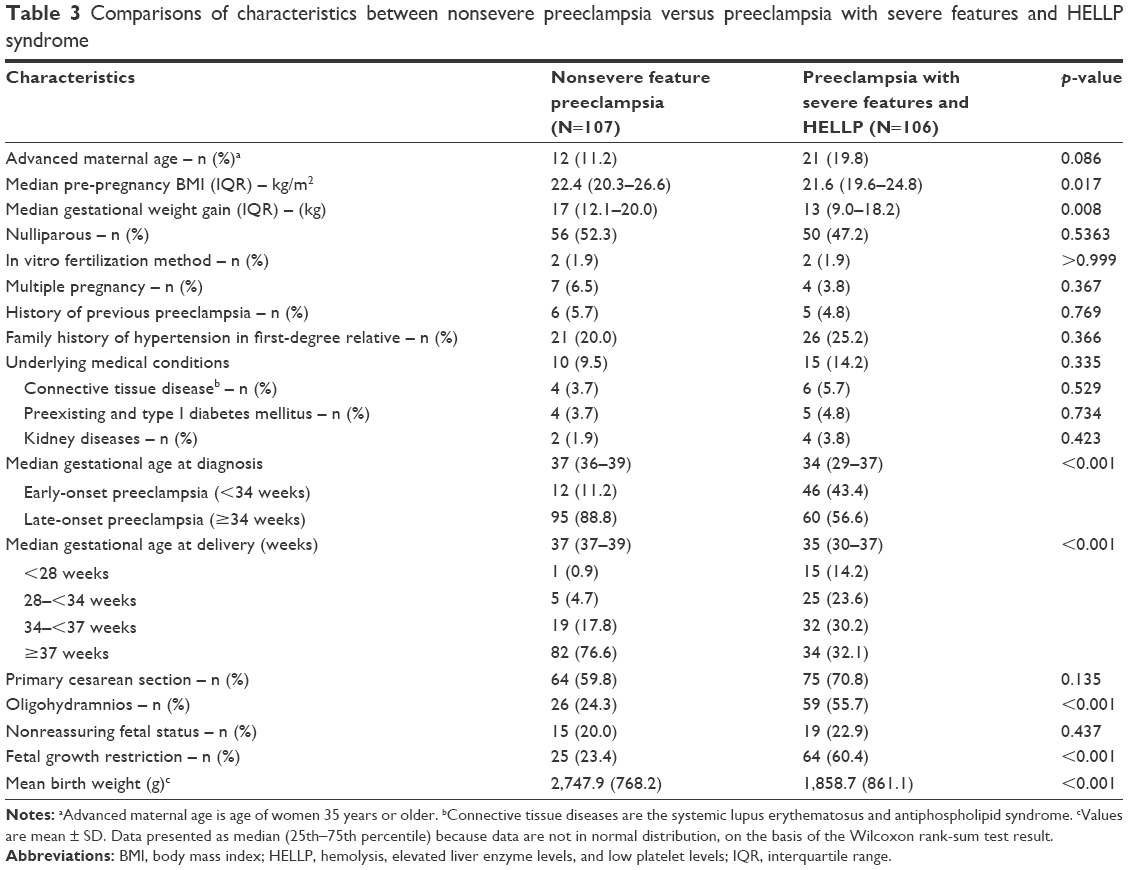 | Table 3 Comparisons of characteristics between nonsevere preeclampsia versus preeclampsia with severe features and HELLP syndrome |
Comparison of maternal complications between the nonsevere preeclampsia group versus preeclampsia with severe features and HELLP syndrome group is shown in Table 4. Twenty-one women (9.9%) had postpartum hemorrhage, 11 (10.3%) in the nonsevere feature preeclampsia group and 10 (9.4%) in the preeclampsia with severe features and HELLP syndrome group. Almost all of the women who received blood transfusions (12 of 13 women, 92.3%) had preeclampsia with severe features and HELLP syndrome. Placental abruption (3 women, 1.4%) and heart failure (1 woman, 0.4%) only occurred in cases of preeclampsia with severe features with HELLP syndrome. Intensive care unit admission (7 of 8 women, 87.5%) was more common among women with preeclampsia with severe features and HELLP syndrome, but this difference was not statistically significant.
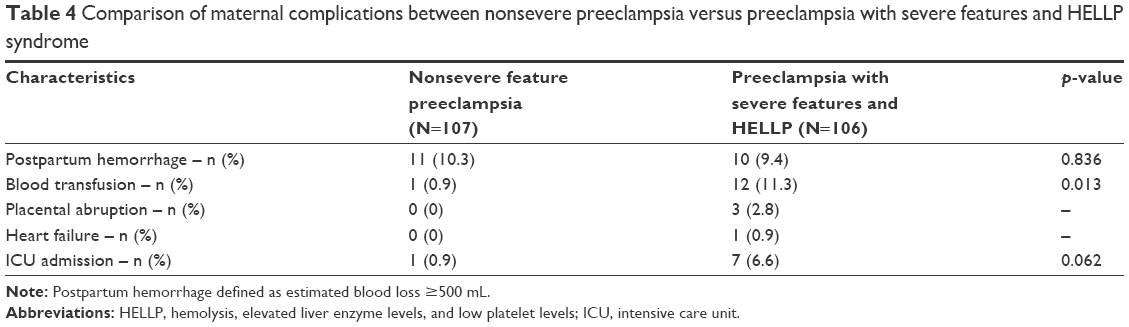 | Table 4 Comparison of maternal complications between nonsevere preeclampsia versus preeclampsia with severe features and HELLP syndrome |
Table 5 provides a comparison of neonatal complications between patients with nonsevere feature preeclampsia versus those with preeclampsia with severe features and HELLP syndrome. The rates of neonatal complications were significantly higher in women with preeclampsia with severe features and HELLP syndrome (low birth weight =35.1% versus 74.3%, p<0.001; birth asphyxia =4.4% versus 18.2%, p=0.001; neonatal intensive care unit admission =7.0% versus 30.9%, p<0.001; neonatal resuscitation =15.8% versus 42.7%, p<0.001). Stillbirths only occurred in women with preeclampsia with severe features and HELLP syndrome (3 cases, 1.4%), and intrapartum death was more common among women with preeclampsia with severe features and HELLP syndrome, but without statistical significance (2.6% versus 6.4%, p=0.190).
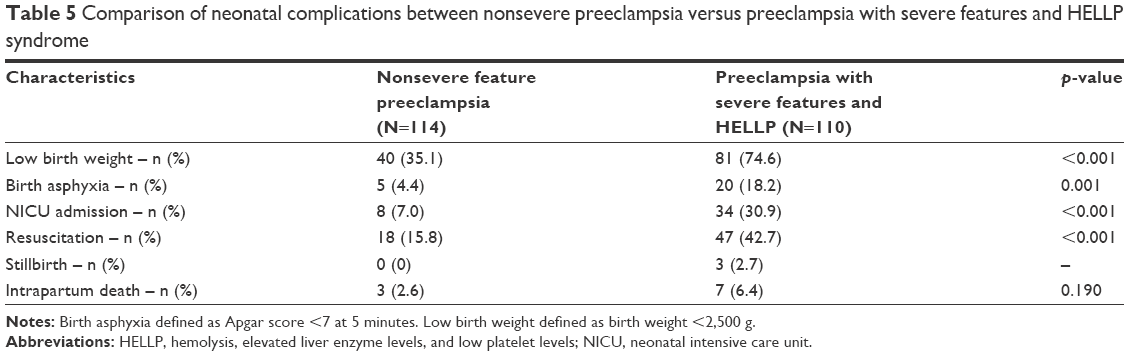 | Table 5 Comparison of neonatal complications between nonsevere preeclampsia versus preeclampsia with severe features and HELLP syndrome |
Discussion
The incidence of preeclampsia with severe features in this study (8 per 1,000 deliveries) was similar to those found in previous studies conducted prior to the changes to the ACOG diagnostic criteria for and definitions of preeclampsia mentioned earlier. These studies included a secondary analysis of hospital-based data retrieved from the 2014 database of the Thailand National Health Security Office (10.1 per 1,000 deliveries), a study from the UK (5 per 1,000 deliveries), and a study from the USA (10 per 1,000 deliveries).8,9 However, the incidence of HELLP syndrome in this study was 1.4 per 1,000 deliveries, which is considerably low when compared with that found in a previous report, 4 per 1,000 deliveries.10 Consistent with the literature,11,12 the HELLP syndrome rate among patients with preeclampsia with severe features in our study was 15.1%. The incidence of early-onset severe preeclampsia in this study was 0.4%, which is compatible with that found in a previous report (0.3%).13
Advanced maternal age, primiparity, multiple gestation, chronic hypertension or chronic renal disease, in vitro fertilization, diabetes mellitus, obesity, and systemic lupus erythematosus have also been associated with increased probability of preeclampsia.7,14,15 Nonetheless, risk factors such as advanced maternal age, underlying medical diseases, parity, in vitro fertilization method, multiple pregnancy, history of previous preeclampsia, and family history of hypertension in a first-degree relative did not differ between patients with nonsevere features preeclampsia and those with preeclampsia with severe features and HELLP syndrome in this study.
Delivery is usually promptly induced in patients with preeclampsia with severe features and HELLP syndrome in order to prevent maternal and fetal complications, as prolonging pregnancy increases the risk of perinatal mortality and morbidity.13,16 In this study, women with preeclampsia with severe features and HELLP syndrome had an increased risk of blood transfusion, rate of intensive care unit admission, and probability of postpartum hemorrhage. Previous studies have reported the rate of placental abruption to be 7.1%–8.8% in women with preeclampsia.17,18 In this study, only 2.8% of preeclamptic women developed placental abruption, all of whom belonged to the preeclampsia with severe features and HELLP syndrome group. In general, the rate of cesarean delivery has been shown to be higher in patients with hypertensive disorders during pregnancy.19 In this study, women with preeclampsia with severe features and HELLP syndrome were more likely to deliver by cesarean section. Nonreassuring fetal status was the most common indication for cesarean section, a finding that is similar to those of a previous study.17
Yet another study20 found oligohydramnios to be an independent risk factor for early neonatal morbidity in preeclamptic patients. However, although women with preeclampsia with severe features and HELLP syndrome in this study were more likely to experience oligohydramnios and fetal growth restriction than women with nonsevere features preeclampsia, there was no difference in terms of nonreassuring fetal status. In another study,17,21 women with severe preeclampsia had an increased risk of fetal growth restriction (50%–53%). However, the neonatal outcomes in this study were less severe than those found in that study,17 in which intrauterine fetal death occurred in 11% of cases (compared to the 6.1% of cases found in our study) and was considerably worse in women with preeclampsia with severe features and HELLP syndrome.
However, this study had several limitations. First, ACOG changed its standard diagnostic criteria and definitions of preeclampsia in 2013. Thus, it should be noted that studies published before the change in terminology used different features to characterize the features of the severe preeclampsia spectrum. Second, this study was based on retrospective data collection, which means that some data might be inaccurate or incomplete and difference in outcomes might be due to differences in baseline data. Finally, the incidence of preeclampsia in this study might be higher than in other settings in Thailand due to our data having been gathered from a tertiary care institution. In addition, we do not yet have an incidence rate for the overall population in our country, which might limit the generalizability of the results to other settings.
Despite these limitations, this was the first study that evaluated the incidence, characteristics, complications, and perinatal outcomes of preeclampsia with severe features and HELLP syndrome according to the ACOG standard diagnostic criteria in Thailand, and so it might be helpful for estimating the incidence, risk factors, and burden of disease severity for improving the standard practice guideline. Moreover, such knowledge can pave the way for further study or intervention, which will allow for appropriate prevention and management in order to minimize adverse pregnancy outcomes.
Conclusion
In conclusion, incidence of preeclampsia with severe features and HELLP was 9.5 per 1,000 deliveries. Common maternal and perinatal outcomes were placental abruption, cesarean delivery, oligohydramnios, and fetal growth restriction. Early detection and prevention of adverse maternal and perinatal outcomes in women with hypertensive disorders are essential.
Acknowledgments
We would like to thank the patients for their participation and the staff at Srinagarind Hospital for their assistance. We would also like to thank Dylan Southard, the English Consultant at the Khon Kaen University Faculty of Medicine Research Affairs division for his assistance with the English-language presentation of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–e333. | ||
Backes CH, Markham K, Moorehead P, Cordero L, Nankervis CA, Giannone PJ. Maternal preeclampsia and neonatal outcomes. J Pregnancy. 2011;2011:1–7. | ||
Visser W, Wallenburg HC. Maternal and perinatal outcome of temporizing management in 254 consecutive patients with severe pre-eclampsia remote from term. Eur J Obstet Gynecol Reprod Biol. 1995;63(2):147–154. | ||
Ganzevoort W, Rep A, de Vries JIP, Bonsel GJ, Wolf H, PETRA-investigators. Prediction of maternal complications and adverse infant outcome at admission for temporizing management of early-onset severe hypertensive disorders of pregnancy. Am J Obstet Gynecol. 2006;195(2):495–503. | ||
Abalos E, Cuesta C, Grosso AL, Chou D, Say L. Global and regional estimates of preeclampsia and eclampsia: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2013;170(1):1–7. | ||
Abalos E, Cuesta C, Carroli G, et al. Pre-eclampsia, eclampsia and adverse maternal and perinatal outcomes: a secondary analysis of the World Health Organization Multicountry Survey on Maternal and Newborn Health. BJOG. 2014;121(Suppl 1):14–24. | ||
American College of Obstetricians and Gynecologists. Hypertension in Pregnancy. Washington, DC: American College of Obstetricians and Gynecologists; 2013:89. | ||
Zhang J, Meikle S, Trumble A. Severe maternal morbidity associated with hypertensive disorders in pregnancy in the United States. Hypertens Pregnancy. 2003;22(2):203–212. | ||
Liabsuetrakul T, Thida T. Geographical Distribution of Hypertensive Disorders in Pregnancy and their Adverse Maternal and Perinatal Outcomes in Thailand. Int J Pregn & Chi Birth. 2017;2(2):42–43. | ||
Zuberi NF, Arif K, Khan FM, Pal JA. A comparison of severe pre-eclampsia/eclampsia in patients with and without HELLP syndrome. J Pak Med Assoc. 1998;48(2):29–32. | ||
Turgut A, Demirci O, Demirci E, Uludoğan M. Comparison of maternal and neonatal outcomes in women with HELLP syndrome and women with severe preeclampsia without HELLP syndrome. J Prenat Med. 2010;4(3):51–58. | ||
Vigil-De Gracia P. Pregnancy complicated by pre-eclampsia-eclampsia with HELLP syndrome. Int J Gynaecol Obstet. 2001;72(1):17–23. | ||
Publications Committee, Society for Maternal-Fetal Medicine, Sibai BM. Evaluation and management of severe preeclampsia before 34 weeks’ gestation. Am J Obstet Gynecol. 2011;205(3):191–198. | ||
Duckitt K, Harrington D. Risk factors for pre-eclampsia at antenatal booking: systematic review of controlled studies. BMJ. 2005;330(7491):565. | ||
Carr DB, Epplein M, Johnson CO, Easterling TR, Critchlow CW. A sister’s risk: family history as a predictor of preeclampsia. Am J Obstet Gynecol. 2005;193(3 Pt 2):965–972. | ||
Hauth JC, Ewell MG, Levine RJ, et al. Pregnancy outcomes in healthy nulliparas who developed hypertension. Calcium for Preeclampsia Prevention Study Group. Obstet Gynecol. 2000;95(1):24–28. | ||
Yildirim G, Güngördük K, Aslan H, Gül A, Bayraktar M, Ceylan Y. Comparison of perinatal and maternal outcomes of severe preeclampsia, eclampsia, and HELLP syndrome. J Turk Ger Gynecol Assoc. 2011;12(2):90–96. | ||
Saadat M, Nejad SM, Habibi G, Sheikhvatan M. Maternal and neonatal outcomes in women with preeclampsia. Taiwan J Obstet Gynecol. 2007;46(3):255–259. | ||
Gofton EN, Capewell V, Natale R, Gratton RJ. Obstetrical intervention rates and maternal and neonatal outcomes of women with gestational hypertension. Am J Obstet Gynecol. 2001;185(4):798–803. | ||
Rabinovich A, Holtzman K, Shoham-Vardi I, Mazor M, Erez O. Oligohydramnios is an independent risk factor for perinatal morbidity among women with pre-eclampsia who delivered preterm. J Matern Fetal Neonatal Med. 2017:1–7. | ||
Liu CM, Cheng PJ, Chang SD. Maternal complications and perinatal outcomes associated with gestational hypertension and severe preeclampsia in Taiwanese women. J Formos Med Assoc. 2008;107(2):129–138. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.