Back to Journals » Clinical Interventions in Aging » Volume 18
Incidence, Causes, and Risk Factors of Unplanned Readmissions in Elderly Patients Undergoing Hip Fracture Surgery: An Observational Study
Authors Tian M ![]() , Wang Z, Zhu Y, Tian Y
, Wang Z, Zhu Y, Tian Y ![]() , Zhang K, Li X
, Zhang K, Li X ![]()
Received 24 November 2022
Accepted for publication 17 February 2023
Published 1 March 2023 Volume 2023:18 Pages 317—326
DOI https://doi.org/10.2147/CIA.S395012
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Miao Tian,1,* Zhijia Wang,2,* Yanbin Zhu,1,3 Yunxu Tian,1 Kexin Zhang,1 Xiuting Li1
1Department of Orthopedic Surgery, the Third Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China; 2Department of Joint Surgery, Huai ‘an Hospital of Huai‘an City, Huai‘an, People’s Republic of China; 3Hebei Orthopedic Research Institute, Key Laboratory of Biomechanics of Hebei Province, Shijiazhuang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiuting Li; Yanbin Zhu, Email [email protected]; [email protected]
Aim: The purpose of this study was to examine the incidence and cause of unplanned readmission after Surgically Treated Hip Fractures in Elderly Patients and identify the associated risk factors.
Methods: This study retrospectively collected the data on elderly patients who underwent hip fracture surgery at two institutions from January 2020 to December 2021, and identified those who were readmitted within 12 months postoperatively. Based on the presence or not of postoperative readmission, they were divided into readmission and non-readmission groups. Demographics, surgery-related variables, and laboratory parameters were compared between groups. The specific causes for documented readmission were collected and summarized. Multivariate logistic regression analysis was performed to identify the associated risk factors.
Results: There were 930 patients including 76 (8.2%) patients who were readmitted within 12 months postoperatively. Overall, cardiac and respiratory complications and new-onset fractures were the first three common causes of readmission, taking an overwhelming proportion of 53.9% (41/76). Over 60% (61.8%, 47/76) of readmissions occurred within 30 days after surgery, with medical complications taking a predominance (89.4%, 42/47). New-onset fractures accounted for a proportion of 18.4% (14/76), occurring at different time points; especially, at 90– 365 days, it accounted for 44.4% (8/18). Multivariate analysis revealed that age ≥ 80 years (OR, 1.0, 95% CI, 1.0 to 1.1; P=0.032), preoperative albumin level ≤ 21.5 g/L (OR, 1.1, 95% CI, 1.0 to 1.2; P=0.009), the postoperative occurrence of DVT (OR, 4.2, 95% CI, 2.5 to 7.2; P=0.001), and local anesthesia (OR, 2.1, 95% CI, 1.1 to 4.0; P=0.029) were independent risk factors for unplanned readmissions.
Conclusion: This study identified several risk factors for unplanned readmissions after elderly hip fractures, and provided detailed information about unplanned readmissions.
Keywords: hip fracture, the elderly, unplanned readmissions, cause, risk factors
Introduction
It has been estimated that about 6.26 million people will suffer from hip fractures every year globally by 2050.1 For most hip fractures, surgery is recommended as the treatment of choice.2 Unplanned readmission rate, an indicator used to measure the quality of healthcare and surgical outcome, often was associated with poor outcomes.3 It was estimated that each unplanned readmission increased the postoperative 1-year mortality risk by 23.1% to 34.4%,4,5 prolonged the hospitalization stay by an average of 8.7 days, and increased medical cost by 14,191 to 25,035 dollars.6
According to the available literature, the incidence of readmission after surgically treated hip fractures in elderly patients was 8.3% to 19.0% within 6 months, and high as 30.1% within 1 year after discharge.7–9 Recently, a systematic review involving 22 original studies suggested that medical causes more common than surgical causes were responsible for the readmission, with pneumonia consistently being the most common individual complication.10 In an original study of complications within 30 days after surgery, Kate et al6 reported that 18.6% of the readmissions were for surgical complications and 81.4% for medical complications. Specified at examining the causes for readmission, Andrea et al9 found that cardiac disease, infection, and cerebrovascular events were the first most common causes of readmission. However, these studies did not list detailed information about the causes for readmission at different time points after surgery, thus not facilitating precise prevention and management.11,12 In addition, the findings of these studies may have been somewhat affected by limitations, eg, limited sample size, inadequate adjustment for covariates, or the relatively short follow-up period (eg, post-operative 30 days). Another point that was easily overlooked was that these findings, mostly from western countries, might be less applicable to Chinese hip fracture patients, due to the differences in patient characteristics, health insurance system and coverage, and health care strategies.
Given the above, we conducted this study, with aims, first, to explore the incidence rate of unplanned readmission in elderly hip fracture patients; second, to describe the detailed and specific causes for unplanned readmission at different time points after surgery; and third, to identify the risk factors independently associated with unplanned readmission.
Methods
Study Design and Study Population
Before the commencement, the study protocol was approved by the Ethical Committee of the Third Hospital of Hebei Medical University and Huai’an Hospital of Huai’an City. Because no patient identity information was included, the requirement for informed consent was waived. This was a retrospective study based on data collected between January 2020 and December 2021 in these two institutions. The inclusion criteria were patients aged 60 or older presenting with hip fractures that were surgically treated within 21 days after injury. The exclusion criteria were high-energy trauma, old fracture (>21 days), polytrauma, multiple fractures, pathological fractures, or planned readmission (eg, planned removal of internal fixation device or removal of lower limb thrombus filter), incomplete variables of interest, or lost to follow-up due to any reasons.
Identification of Unplanned Readmission
The unplanned readmission was identified by inquiring about the hospitalization electronic medical records, and this work was completed by the two primary investigators (M.T. and Z.W.). Any cause for unplanned readmission was included, involving medical (hematologic, respiratory, cardiovascular, gastrointestinal, renal, neurologic, and others) complications or surgical ones (incisional complications, internal fixation, bone fracture nonunion/delayed union, and others). According to the time when unplanned readmission occurred, three categories were divided, ie, ≤30 days, 31 to 90 days, and 91 to 365 days. Any discrepancy or disagreement was addressed by a discussion with the senior author (X.L.). The definition for the cause of unplanned readmission in our study refers to reason and medical diagnosis for patient’s unplanned readmission.
Variables of Interest
Variables of interest were collected by the same two investigators (M.T. and Z.W.). A total of 42 variables related to demographics, comorbidities, fracture-related variables, surgery-related variables, and laboratory parameters were included. Demographic variables included age, sex and body mass index (BMI); comorbidities included age-adjusted Charlson Comorbidity Index (ACCI), diabetes, hypertension, coronary disease, cerebrovascular disease, respiratory disease, renal disease and so on; fracture-related variables included fracture type, injury mechanism and the time from injury to admission, and surgery-related variables included preoperative waiting time, operative time, anesthesia pattern, American Society of Anesthesiologists (ASA, categorized as either I–II or III–IV) classification, and perioperative blood transfusion volume; laboratory parameters included hemoglobin (HB) at admission, preoperative HB value, albumin at admission, preoperative albumin value, B-type natriuretic peptide (BNP) at admission, D-dimer at admission, serum potassium levels at admission, serum sodium levels at admission, serum creatine kinase (CK) at admission, C-reactive protein (CRP) levels at admission; others like length of stay, perioperative onset of complications (anemia, hypoproteinemia, deep venous thrombosis (DVT) of lower limb, cardiac events, cerebral infarction). Meanwhile, we also collected the time and medical diagnosis of unplanned readmission of elderly patients with hip fractures within 1 year after the operation by inquiring about the medical record system.
Statistical Analysis
Statistical analysis was carried out using IBM SPSS Statistics 26.0 (IBM Corporation, Armonk, NY, USA). Continuous variables with normal distribution were described as mean ± standard deviation ( ), and the continuous variables with non-normal distribution were presented with a median or interquartile (IQR). Categorical variables were expressed as frequency and percentage. The normal distribution of continuous variables was tested using the Shapiro–Wilk test, and those distributed normally were tested by two independent sample t-tests, otherwise, by the Mann–Whitney U-test. Pearson chi-square test or Fisher's exact test was applied to evaluate the between-group difference for categorical variables, as appropriate. For continuous variables tested with statistical significance, the optimal cut-off value was determined by receiver operating characteristic (ROC) when Youden index was maximized and the area under the curve (AUC) was used to evaluate their discriminating ability.
), and the continuous variables with non-normal distribution were presented with a median or interquartile (IQR). Categorical variables were expressed as frequency and percentage. The normal distribution of continuous variables was tested using the Shapiro–Wilk test, and those distributed normally were tested by two independent sample t-tests, otherwise, by the Mann–Whitney U-test. Pearson chi-square test or Fisher's exact test was applied to evaluate the between-group difference for categorical variables, as appropriate. For continuous variables tested with statistical significance, the optimal cut-off value was determined by receiver operating characteristic (ROC) when Youden index was maximized and the area under the curve (AUC) was used to evaluate their discriminating ability.
Variables that were tested with P < 0.10 were further entered into the multivariate logistic regression model to detect their independent effect on unplanned readmission. The association magnitude for potential risk factors was indicated by the odds ratio (OR) with its corresponding 95% confidence interval (95% CI). Variables with P < 0.10 were retained in the multivariate model. P < 0.05 was set as the significance threshold. The Hosmer–Lemeshow test was used to evaluate the goodness-of-fit of the multivariate model and the result was quantified as the adjusted R2 value, with P above 0.05 and R2 value <0.05 indicating the acceptable result.13
Result
Baseline Characteristics
During the study period, a total of 1054 patients were included, and 124 patients were excluded due to incomplete data (30), multiple injuries (43), old fractures (34), pathological fractures (2), and planned readmission (15). As is shown in Figure 1, a total of 930 patients were finally included.
 |
Figure 1 The flowchart illustrating the selection of the participants for this research. |
Univariate analysis revealed that age, BMI, ACCI, albumin at admission, preoperative albumin level, CRP at admission, respiratory diseases, anesthesia pattern, postoperative hypoproteinemia, the postoperative occurrence of DVT, and postoperative cerebral infarction were significant risk factors for readmission (Table 1). The ROC analysis showed that the AUC of age, BMI, ACCI, albumin at admission, preoperative albumin level, and CRP at admission were 0.62, 0.44, 0.59, 0.44, 0.38, and 0.59, respectively. The cut-off values were 80 years old, 15.2kg/m2, 7.0, 28.5g/L, 21.4g/L, and 46.6mg/L, respectively (Table 2).
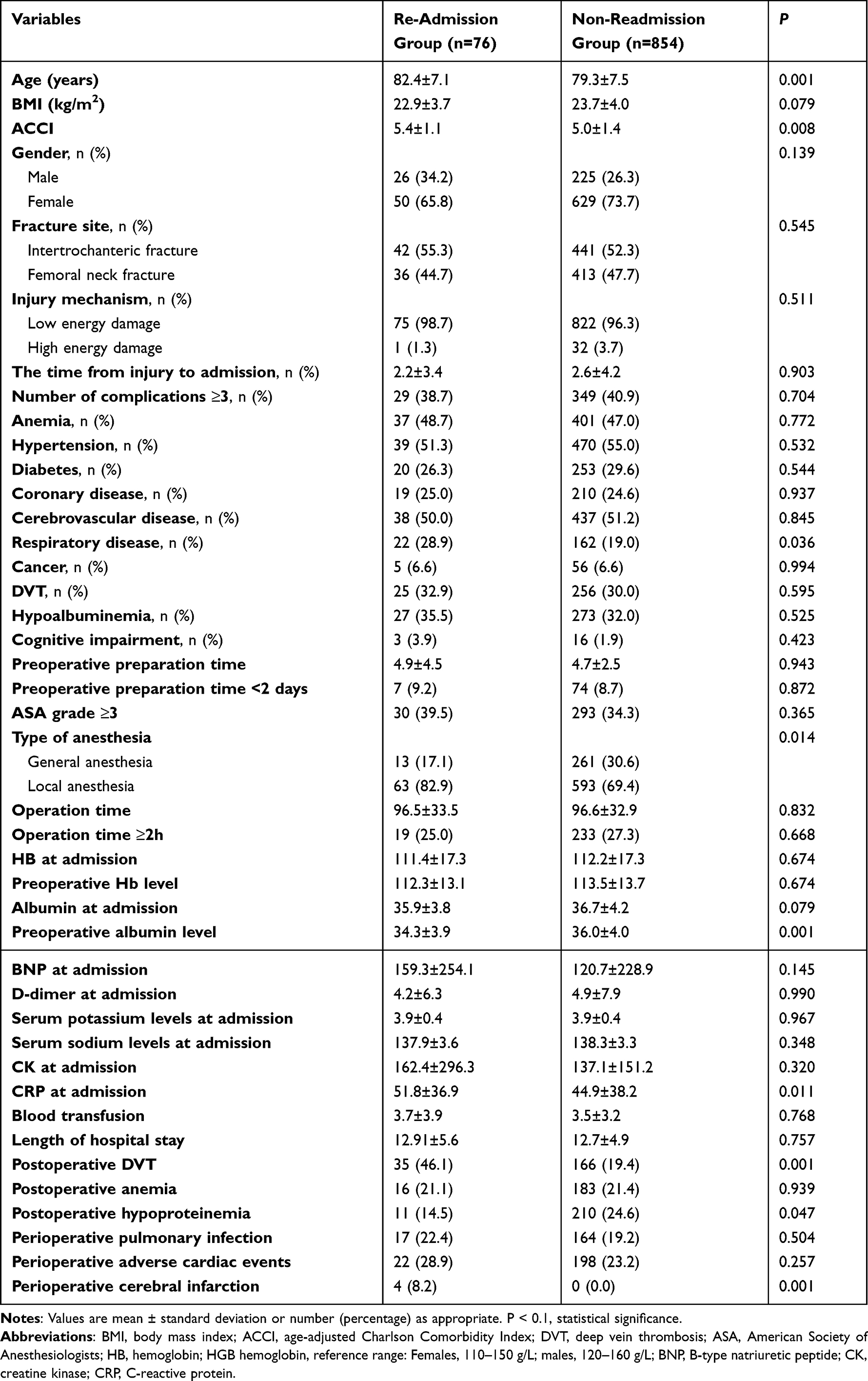 |
Table 1 The Comparison Between the Two Groups |
 |
Table 2 ROC Curve Analysis Results of Statistically Significant Continuous Variables |
The result of multivariate analysis showed age ≥80 years (OR, 1.0, 95% CI, 1.0 to 1.1; P=0.032), preoperative albumin level ≤21.5 g/L (OR, 1.1, 95% CI, 1.0 to 1.2; P=0.009), Postoperative occurrence of DVT (OR, 4.2, 95% CI, 2.5 to 7.2; P=0.001), and local anesthesia (OR, 2.1, 95% CI, 1.1 to 4.0; P=0.029) were independent risk factors (Table 3).
 |
Table 3 Multivariate Logistic Regression Analysis of Unplanned Transfer and Readmissions |
The Hosmer–Lemeshow test showed the acceptable goodness-of-fit of the final model (P=0.374, adjusted Nagelkerke R2=0.446).
We can see that 76 (8.2%) patients were readmitted within 1 year after discharge. Forty-seven (5.1%) patients required readmission within 30 days, predominantly caused by respiratory complications (19.1%, 9/47), cardiovascular complications (21.2%, 10/47), cerebral infarction (12.8%, 6/47), incisional complications (10.6%, 5/47) and DVT of bilateral lower extremities (10.6%, 5/47). Besides, there are nine patients had respiratory complications, of which pulmonary infection (66.7%, 6/9) was the most common. Eleven (1.18%) patients were readmitted 1–3 months after discharge, and new-onset fractures (36.4%, 4/11) were the common cause, including 2 cases of ipsilateral femoral shaft fracture, 2 humerus fractures, and 1 hip fracture at the contralateral limb, respectively. During the postoperative 3 to 12 months, 18 unplanned readmissions occurred, indicating an incidence of 1.9%; new onset of fractures (44.4%, 8/18) was predominant, and 75% were hip fractures occurring at the contralateral limb. The other two cases of fracture were periprosthetic fractures and supracondylar femoral fractures, respectively. One month after the operation is the peak time of readmission. With the prolongation of postoperative time, the rate of readmission decreased (Table 4).
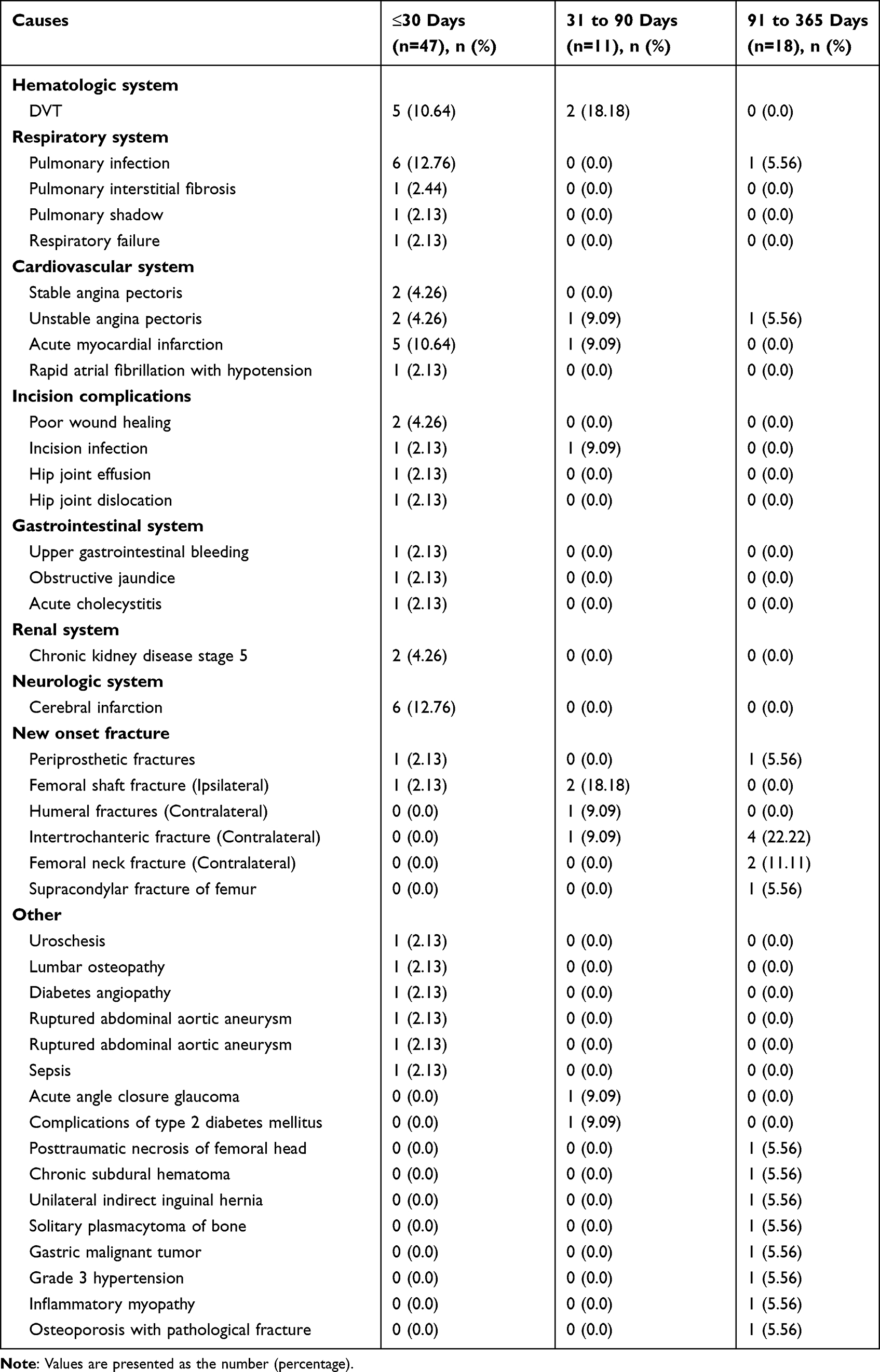 |
Table 4 The Cause and Medical Diagnosis of Unplanned Readmission |
Discussion
In this study, we found that the incidence rate of unplanned readmission within 12 months after surgery of hip fractures in the elderly was 8.2%, the medical complications and new onset of fractures were major causes and the older age, lower preoperative albumin level, regional anesthesia technique applied, and postoperative presence of DVT of bilateral lower extremities were identified as independent risk factors associated with unplanned readmission. To the best of our knowledge, this was the first study to exhibit very comprehensive and detailed data on unplanned readmission after elderly hip fracture, especially the specific causes at sequential time points postoperatively.
Postoperative 30 days after discharge was a key period for complication prevention and management, which was also a major reason for most previous studies focusing on complications at this time window, including the National Surgical Quality Improvement Program (NSQIP) studies. In this study, we found a similar trend that 61.8% (47/76) of unplanned readmission occurred within 30 days after discharge. It was also notable that most readmissions were related to medical complications (89.4%, 42/47) over than procedure-related complications (10.6%, 5/47), with cardiac complications, respiratory complications, and cerebrovascular complications accounting for a large proportion (53.2%, 25/47). These findings were comparable to that of Lizaur’s study,14 which found a readmission rate of 8.3% within 30 days after elderly hip fractures and the medical reason was 13 times more frequent than surgical reasons. Accordingly, optimized management of comorbidities remains a high priority, especially in the context of the existence of hemodynamic instability and low immunity caused by hip fracture itself and operative trauma.
After the first 1 month, there was no significant central trend to one certain complication, except for the fracture caused by a low-energy fall. In our data analysis, 12 new-onset fractures occurred at this time window, accounting for 41.4% of the total complications (n=29). In particular, seven cases of contralateral hip fractures were found, representing an incidence rate of 0.8%, which would be greater than the initial hip fracture healthy and morbidity burden. That meant a substantially increased risk of mortality and post-surgery functional independence loss.15–17 Therefore, postoperative rehabilitation exercises, especially including neuromuscular coordination, muscle strength, and balance, should be strengthened to prevent or improve bone mass loss or muscle loss due to long-term postoperative limb immobilization, after the bone union has been achieved (generally at 8–12 weeks).
The finding of advanced age identified as an independent risk factor for readmission reflected the decline of functional reserve of the organism with age, including the resistance to fracture trauma and operative trauma, and the higher susceptibility to change of homeostasis,18 which thus were more likely to cause early-period medical complications. Additionally, patients with older age were generally having higher odds of falls due to muscle weakness and poorer neuromuscular coordination, and this phenomenon was more remarkable in the post-operative recovery period, leading to a higher risk of falls or related fractures.19
Serum albumin, not only an indicator of nutritional status but also a predictor of surgical outcomes or systemic adverse events,20,21 provided a similarly important predictive value on readmission in this study. Elderly hip fracture patients with low serum albumin levels are more prone to develop perioperative complications, such as aspiration pneumonia and urinary retention.22,23 In this study, we found that patients with low albumin levels are more likely to be readmitted. Despite that multi-aspect factors (eg, nutritional status, surgical trauma, bacterial infection, and inflammation) may affect the serum albumin level, enhancing perioperative nutrition demonstrated to be beneficial in improving postoperative complications and the risk of readmission.
The relative advantages of general over local anesthesia remain controversial. A systematic review based on 13 original studies of 196,646 patients undergoing surgeries for hip fractures concluded that general anesthesia was associated with prolonged hospitalization and increased in-hospital mortality and readmission rates.24 However, in individual studies, no significant difference in readmission rate was observed between patients using regional and general anesthesia modes.25,26 In this study, we found the opposite conclusion that regional anesthesia was associated with a significant risk of readmission, and we inferred this result was associated with the fact that patients with local anesthesia had stronger immune suppression, inflammatory reactions, and hemodynamic instability than those with general anesthesia.27,28
Our study found the strongest association magnitude of postoperative presence of DVT with the unplanned readmission with an adjusted OR of 4.2, which was consistent with a previous finding that DVT increased the risk of postoperative admission within 30 days by 1.9 times in geriatric general surgery patients.29 In another study of 9441 patients undergoing primary total hip arthroplasty, Mednick et al30 also observed the same result that postoperative DVT was associated with an increased risk of 30-day readmission. Considering the still very high prevalence rate (21.6%, 201/930) of DVT after surgeries in this study, the strongest association with readmission, and the inadequate prophylaxis rate in previous studies,31 we suggest routine preoperative prophylaxis, early detection, and adequate treatment.
The merits of this study included a relatively large sample and data sources from two medical institutions. In addition, the collected variables are relatively comprehensive, and the detailed description of the specific causes for readmission at different periods is given. Several potential limitations should be noted. First, the retrospective design inherited the bias in patient selection and precision in data collection. Second, some variables that may affect the results have not been collected, such as the discharge destination, common geriatric syndromes, patient’s annual household income and the postoperative exercises (starting time, frequency, strength, duration), fracture occurrence place, the medications (number, type, and frequency), activities of the daily living level at admission. Due to that most patients had at least one comorbidity, and even some have multiple ones, the medications (number, patterns, and frequency) might have affected the result, but the relevant data were not available. Therefore, the residual confounding effects remain. Third, the readmission was identified only by inquiring about the electronic medical records, thus leaving a possibility that patients who were admitted to other hospitals were missed. Thus, we might have underestimated the true rate of readmission after surgeries for hip fractures in elderly patients.
Conclusions
In summary, we found that the unplanned readmission rate within 1 year after discharge in elderly hip fracture patients was 8.2%, and also presented the detailed specific causes at different time points. Most readmissions were caused by medical complications. Cardiac complications, respiratory complications, and new-onset fractures were the first three common readmission diagnoses. Advanced age, preoperative lower albumin level, postoperative presence of DVT, and local anesthesia mode were identified as independent risk factors. Despite in context of limitations, these findings provide detailed information about the unplanned readmissions after elderly hip fractures, facilitating individual risk evaluation and stratification, and implementation of the targeted prevention measures.
Abbreviations
BMI, body mass index; ACCI, age-adjusted Charlson Comorbidity Index; DVT, deep vein thrombosis; ASA, American Society of Anesthesiologists; HB, hemoglobin; BNP, B-type natriuretic peptide; CK, creatine kinase; CRP, C-reactive protein.
Data Sharing Statement
All the data used and/or analyzed during the current study are available from Xiuting Li upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of the Third Hospital of Hebei Medical University and informed consent was waived due to its retrospective nature. The study complied with the Helsinki Declaration.
Consent for Publication
We have obtained consent for publication from all participants.
Acknowledgments
We are grateful to the medical record query system of the Third Hospital of Hebei Medical University and Huai’an Hospital of Huai’an City for providing data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors declare that they do not have a conflict of interest.
References
1. Kannus P, Parkkari J, Sievänen H, Heinonen A, Vuori I, Järvinen M. Epidemiology of Hip fractures. Bone. 1996;18(1 Suppl):57s–63s. doi:10.1016/8756-3282(95)00381-9
2. Tan CMP, Park DH, Chen YD, Jagadish MU, Su S, Premchand AXR. Mortality rates for Hip fracture patients managed surgically and conservatively in a dedicated unit in Singapore. Arch Orthop Trauma Surg. 2022;142(1):99–104. doi:10.1007/s00402-020-03605-1
3. Coatsworth-Puspoky R, Duggleby W, Dahlke S, Hunter K. Unplanned readmission for older persons: a concept analysis. J Adv Nurs. 2021;77(11):4291–4305. doi:10.1111/jan.14893
4. Khan MA, Hossain FS, Dashti Z, Muthukumar N. Causes and predictors of early re-admission after surgery for a fracture of the Hip. J Bone Joint Surg Br. 2012;94(5):690–697. doi:10.1302/0301-620X.94B5.28933
5. Kates SL, Behrend C, Mendelson DA, Cram P, Friedman SM. Hospital readmission after Hip fracture. Arch Orthop Trauma Surg. 2015;135(3):329–337. doi:10.1007/s00402-014-2141-2
6. Kates SL, Shields E, Behrend C, Noyes KK. Financial implications of hospital readmission after Hip fracture. Geriatr Orthop Surg Rehabil. 2015;6(3):140–146. doi:10.1177/2151458515578265
7. Riggs RV, Roberts PS, Aronow H, Younan T. Joint replacement and Hip fracture readmission rates: impact of discharge destination. PM R. 2010;2(9):806–810. doi:10.1016/j.pmrj.2010.05.008
8. Hahnel J, Burdekin H, Anand S. Re-admissions following Hip fracture surgery. Ann R Coll Surg Engl. 2009;91(7):591–595. doi:10.1308/003588409X432374
9. Giusti A, Barone A, Razzano M, Pizzonia M, Oliveri M, Pioli G. Predictors of hospital readmission in a cohort of 236 elderly discharged after surgical repair of Hip fracture: one-year follow-up. Aging Clin Exp Res. 2008;20(3):253–259. doi:10.1007/BF03324779
10. Ali AM, Gibbons CE. Predictors of 30-day hospital readmission after Hip fracture: a systematic review. Injury. 2017;48(2):243–252. doi:10.1016/j.injury.2017.01.005
11. Shen Y, Hao Q, Wang Y, et al. The association between preoperative modified frailty index and postoperative complications in Chinese elderly patients with Hip fractures. BMC Geriatr. 2021;21(1):370. doi:10.1186/s12877-021-02330-7
12. Chen X, Shen Y, Hou L, Yang B, Dong B, Hao Q. Sarcopenia index based on serum creatinine and cystatin C predicts the risk of postoperative complications following Hip fracture surgery in older adults. BMC Geriatr. 2021;21(1):541. doi:10.1186/s12877-021-02522-1
13. Prabhakaran K, Gogna S, Lombardo G, Latifi R. Venous thromboembolism in geriatric trauma patients-risk factors and associated outcomes. J Surg Res. 2020;254:327–333. doi:10.1016/j.jss.2020.05.008
14. Lizaur-Utrilla A, Serna-Berna R, Lopez-Prats FA, Gil-Guillen V. Early rehospitalization after Hip fracture in elderly patients: risk factors and prognosis. Arch Orthop Trauma Surg. 2015;135(12):1663–1667. doi:10.1007/s00402-015-2328-1
15. Liu S, Zhu Y, Chen W, Sun T, Cheng J, Zhang Y. Risk factors for the second contralateral Hip fracture in elderly patients: a systematic review and meta-analysis. Clin Rehabil. 2015;29(3):285–294. doi:10.1177/0269215514542358
16. Chen M, Du Y, Tang W, et al. Risk factors of mortality and second fracture after elderly Hip fracture surgery in Shanghai, China. J Bone Miner Metab. 2022;40(6):951–959. doi:10.1007/s00774-022-01358-y
17. Park YG, Jang S, Ha YC. Incidence, morbidity and mortality in patients older than 50 years with second Hip fracture in a Jeju Cohort Study. Hip Pelvis. 2014;26(4):250–255. doi:10.5371/hp.2014.26.4.250
18. van der Ven MJ, Schoon Y, Olde Rikkert MG. Ongeplande heropnames bij kwetsbare ouderen: Retrospectieve analyse van opnames in een academisch ziekenhui[Unplanned readmissions of frail elderly patients: a retrospective analysis of admissions in a teaching hospital]. Ned Tijdschr Geneeskd. 2015;159:A9211. Dutch.
19. Turrentine FE, Zaydfudim VM, Martin AN, Jones RS. Association of geriatric-specific variables with 30-day hospital readmission risk of elderly surgical patients: a NSQIP analysis. J Am Coll Surg. 2020;230(4):527–533.e521. doi:10.1016/j.jamcollsurg.2019.12.032
20. Ohba T, Yokomichi H, Koyama K, Tanaka N, Oda K, Haro H. Factors affecting postoperative mortality of patients with insufficient union following osteoporotic vertebral fractures and impact of preoperative serum albumin on mortality. BMC Musculoskelet Disord. 2020;21(1):528. doi:10.1186/s12891-020-03564-z
21. Yagi T, Oshita Y, Okano I, et al. Controlling nutritional status score predicts postoperative complications after Hip fracture surgery. BMC Geriatr. 2020;20(1):243. doi:10.1186/s12877-020-01643-3
22. Higashikawa T, Shigemoto K, Goshima K, et al. Risk factors for the development of aspiration pneumonia in elderly patients with femoral neck and trochanteric fractures: a retrospective study of a patient cohort. Medicine. 2020;99(7):e19108. doi:10.1097/MD.0000000000019108
23. Higashikawa T, Shigemoto K, Goshima K, et al. Urinary retention as a postoperative complication associated with functional decline in elderly female patients with femoral neck and trochanteric fractures: a retrospective study of a patient cohort. Medicine. 2019;98(24):e16023. doi:10.1097/MD.0000000000016023
24. Chen DX, Yang L, Ding L, Li SY, Qi YN, Li Q. Perioperative outcomes in geriatric patients undergoing Hip fracture surgery with different anesthesia techniques: a systematic review and meta-analysis. Medicine. 2019;98(49):e18220. doi:10.1097/MD.0000000000018220
25. Le-Wendling L, Bihorac A, Baslanti TO, et al. Regional anesthesia as compared with general anesthesia for surgery in geriatric patients with Hip fracture: does it decrease morbidity, mortality, and health care costs? Results of a single-centered study. Pain Med. 2012;13(7):948–956. doi:10.1111/j.1526-4637.2012.01402.x
26. Basques BA, Bohl DD, Golinvaux NS, Samuel AM, Grauer JG. General versus spinal anaesthesia for patients aged 70 years and older with a fracture of the Hip. Bone Joint J. 2015;97-b(5):689–695. doi:10.1302/0301-620X.97B5.35042
27. Ye XF, Wang S, Wu AM, et al. Comparison of the effects of general and local anesthesia in lumbar interlaminar endoscopic surgery. Ann Palliat Med. 2020;9(3):1103–1108. doi:10.21037/apm-20-623
28. Chen Y, Liu W, Gong X, Cheng Q. Comparison of effects of general anesthesia and combined spinal/epidural anesthesia for cesarean delivery on umbilical cord blood gas values: a double-blind, randomized, controlled study. Med Sci Monit. 2019;25:5272–5279. doi:10.12659/MSM.914160
29. Dieterich JD, Divino CM. Postoperative complications predict 30-day readmission in geriatric general surgery patients. Am Surg. 2017;83(4):365–370. doi:10.1177/000313481708300423
30. Mednick RE, Alvi HM, Krishnan V, Lovecchio F, Manning DW. Factors affecting readmission rates following primary total hip arthroplasty. J Bone Joint Surg Am. 2014;96(14):1201–1209. doi:10.2106/JBJS.M.00556
31. Okuhara A, Navarro TP, Procópio RJ, Bernardes RC, Oliveira Lde C, Nishiyama MP. Incidence of deep vein thrombosis and quality of venous thromboembolism prophylaxis. Rev Col Bras Cir. 2014;41(1):2–6. doi:10.1590/S0100-69912014000100002
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Preliminary Screening Tool for High-Risk Frailty in Older Adults Patients with Pulmonary Tuberculosis
Li HJ, Zhou YY, Yu HH, Jiang J, Cai YW
Clinical Interventions in Aging 2025, 20:57-68
Published Date: 22 January 2025
Clinical and Genomic Characteristics of Carbapenem-Resistant Klebsiella pneumoniae Bloodstream Infections in Older Adults: A Single-Center Study from Changsha, China
Qin F, Liu Y, Jian Z, Yan Q, Liu W
Infection and Drug Resistance 2025, 18:6167-6177
Published Date: 26 November 2025