Back to Journals » Clinical Ophthalmology » Volume 17
Incidence and Management of Epithelial-Related Complications After SMILE
Authors Moshirfar M ![]() , Zhang S, Pandya S, Stoakes IM, Hoopes PC
, Zhang S, Pandya S, Stoakes IM, Hoopes PC ![]()
Received 12 July 2023
Accepted for publication 30 August 2023
Published 20 September 2023 Volume 2023:17 Pages 2777—2789
DOI https://doi.org/10.2147/OPTH.S426547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Majid Moshirfar,1– 3 Stephanie Zhang,4 Shreya Pandya,5 Isabella M Stoakes,1,6 Phillip C Hoopes1
1Hoopes Vision Research Center, Hoopes Vision, Draper, UT, USA; 2John A. Moran Eye Center, University of Utah School of Medicine, Salt Lake City, UT, USA; 3Utah Lions Eye Bank, Murray, UT, USA; 4University of Arizona College of Medicine Phoenix, Phoenix, AZ, USA; 5University of Louisville School of Medicine, Louisville, KY, USA; 6Pacific Northwest University of Health Sciences, Yakima, WA, USA
Correspondence: Majid Moshirfar, Hoopes Vision Research Center, Hoopes Vision, 11820 S. State St., Ste. 200, Draper, UT, 84020, USA, Tel +1 801-568-0200, Fax +1 801-563-0200, Email [email protected]
Purpose: To investigate the incidence and management of only epithelial-related complications following small incision lenticule extraction (SMILE).
Patients and Methods: A retrospective, single-site study analyzed patients who underwent SMILE at Hoopes Vision Clinic in Draper, Utah, from June 2017 to February 2023. Demographic data and preoperative parameters were reviewed. Postoperatively, patients were assessed for visual acuity and complications at different time points. Statistical analyses were conducted between the control and complication groups.
Results: Four hundred and thirty-two eyes of 220 patients received SMILE. Postoperative epithelial-related complications were indicated in 68 (15.7%) eyes, including anterior basement membrane (ABM) changes (five [1.2%]) eyes), epithelial ingrowth (nine [2.1%] eyes), erosion (two [0.5%] eyes), rough epithelium (18 [4.2%] eyes), epithelial defect (12 [2.8%] eyes), diffuse lamellar keratitis (DLK) secondary to epitheliopathy (two [0.5%] eyes), microstriae secondary to epitheliopathy (four [0.9%] eyes), interface debris (21 [4.9%] eyes), and incisional fibrosis (one [0.2%] eye). There was a statistically significant difference in age, with older patients more likely to develop epitheliopathy postoperatively (P = 0.001). Additionally, patients with epithelial-related complications were more likely to receive photorefractive keratectomy (PRK) enhancement after SMILE than the control (P = 0.001). However, there was no statistical difference in uncorrected distance visual acuity (UDVA) better than 20/20 and corrected distance visual acuity (CDVA) between the complications group and the control at the last postoperative visit (P = 0.974 and 0.310, respectively). There was no statistically significant difference in the safety and efficacy indices between the complications and control group (P = 0.281 and 0.617, respectively).
Conclusion: In our study, epithelial-related complications were more prevalent in older patients and predisposed patients to require PRK enhancements after recovery from SMILE. Despite the incidence of epithelial-related complications, visual prognoses were favorable and achieved through various management strategies.
Keywords: ReLEx, epithelial ingrowth, DLK, diffuse lamellar keratitis, microstriae, LASIK
Introduction
Small incision lenticule extraction (SMILE) is a laser refractive surgery to correct myopia. Using a femtosecond laser, a small intrastromal lenticule is created and manually extracted through a small incision.1,2 Unlike other refractive surgical techniques, SMILE does not involve the creation of a corneal flap, providing several advantages over laser-assisted in situ keratomileusis (LASIK) with respect to managing postoperative corneal-related complications.1 Although epithelial-related complications after LASIK have been described in several studies, the incidence of epithelial-related complications following SMILE is not as well documented.3–7 This study reports a single-site five-year experience with the incidence and management of only epithelial-related complications after SMILE.
Methods
This study was a retrospective chart review of patients who underwent SMILE at Hoopes Vision Clinic, Draper, Utah, between June 2017 and February 2023. Informed consent was obtained from patients prior to performing all procedures. This study was approved by The Biomedical Research Alliance of New York (BRANY) Institutional Review Board (#A20-12-547-823) and adhered to the tenets of the Declaration of Helsinki. Preoperative age, sex, keratometry, and pachymetry measurements were collected from each patient. Postoperatively, any complications and their respective management regimens were documented. Uncorrected visual acuity (UCVA), corrected distance visual acuity (CDVA), and manifest refraction, measured as best-spectacle corrected visual acuity, were documented before and after SMILE. Patients were scheduled to be examined on day one, week one, month one, month three, and year one postoperatively, with additional examinations if complications arose.
Surgical Technique
SMILE was conducted with a VisuMax 500 kHz femtosecond laser system (Carl Zeiss Meditec, Jena, Germany). For patients undergoing SMILE bilaterally, the right eye was always performed first before the left. Further measurements were taken for patients receiving treatment for myopic astigmatism. Preoperatively, a surgical marker was used for limbal markings at the three and nine o’clock positions while the patient sat upright. The patient was then moved to the operating room, and while in the supine position, the markings were accentuated again with a caliper. The limbal markings were then aligned with the horizontal reticle through the laser scope, with additional maneuvers taken to adjust the alignment as needed. For all patients, the thickness of the cap was set at 120 µm. The lenticule diameter measured 6.5 mm for simple myopic treatment and 6.0 mm to 6.5 mm transition for myopic astigmatic treatment. A 3.0 mm incision was made with an angle of 90 degrees at the 12 o’clock position. The energy of the laser applied during SMILE was 125 nJ, with a spot spacing of 3.70 µm for the lenticule, 3.80 µm for the cap, and 2.00 µm for the lenticule side cut and cap side. The lenticule was removed through the incision with a blunt spatula. After surgery, ofloxacin 0.3% or moxifloxacin 0.5% was administered four times a day for one week and prednisolone acetate 1.0% four times a day for one week, tapering weekly over the course of one month.
Data Collection
Epithelial-related complications were classified into the following categories: anterior basement membrane (ABM) changes, epithelial ingrowth, epithelial erosion, rough epithelium, epithelial defect, diffuse lamellar keratitis (DLK) secondary to epitheliopathy, microstriae secondary to epitheliopathy, interface debris, and fibrosis at the SMILE incision. Other intraoperative and postoperative complications of SMILE, such as decentration, suction loss, inability to dissect the lenticule, black spots, incisional bleeding, cap tear, lenticule remnant, and residual refractive error, were not discussed, as the primary objective in this study was to only analyze epithelial-related complications following SMILE.
Statistical Analysis
Records of patients with epithelial-related complications were gathered and inputted into Datagraph-Med (Wendelstein, Germany). This data was then exported into Microsoft Excel 2023 (Microsoft Corporation, Redmond, WA, USA), where all statistical analyses were performed. Visual acuity was measured with logarithm of the minimum angle of resolution (logMAR) units. Clinical measurements were recorded as mean ± SD. SPSS software (version 29.0.1.0; IBM Inc., Armonk, NY, USA) was used for data analysis. Data were first analyzed for normality using the Shapiro–Wilk test. Comparisons between the epithelial-related complications group and control group were evaluated with an independent t-test for means of normally distributed data. The Mann–Whitney U-test or the Kruskal–Wallis test were used to compare data that were not normally distributed. For the comparison of categorical variables, a Chi-square test of independence was implemented. A P-value less than 0.05 was considered statistically significant. Additionally, the power of this study was calculated using G*Power (version 3.1, Franz Faul, Universitӓt Kiel, Germany). For an alpha value of 0.05, a minimum sample size of 245 for the control and 47 for the epithelial-related complications group was needed to obtain a power of 0.80.
Results
Patient Cohort
This study examined 432 eyes of 220 patients. Out of the 220 patients, 212 (96.4%) received bilateral SMILE. Of the eight (3.6%) patients who underwent unilateral SMILE, four received surgery in the right eye, and four received surgery in the left eye. Thus, SMILE was performed in 216 (50.0%) right eyes and 216 (50.0%) left eyes. None of the preoperative parameters concerning patient demographics and visual outcomes (Table 1) were statistically significant except for age, indicating that the group with epithelial-related complications was older than the control (P = 0.001). A post hoc analysis, with a sample size of 364 for the control and 68 for the epithelial-related complications group revealed a power of 0.92. Of 432 eyes, 68 (15.7%) had epithelial-related complications after SMILE (Table 2).
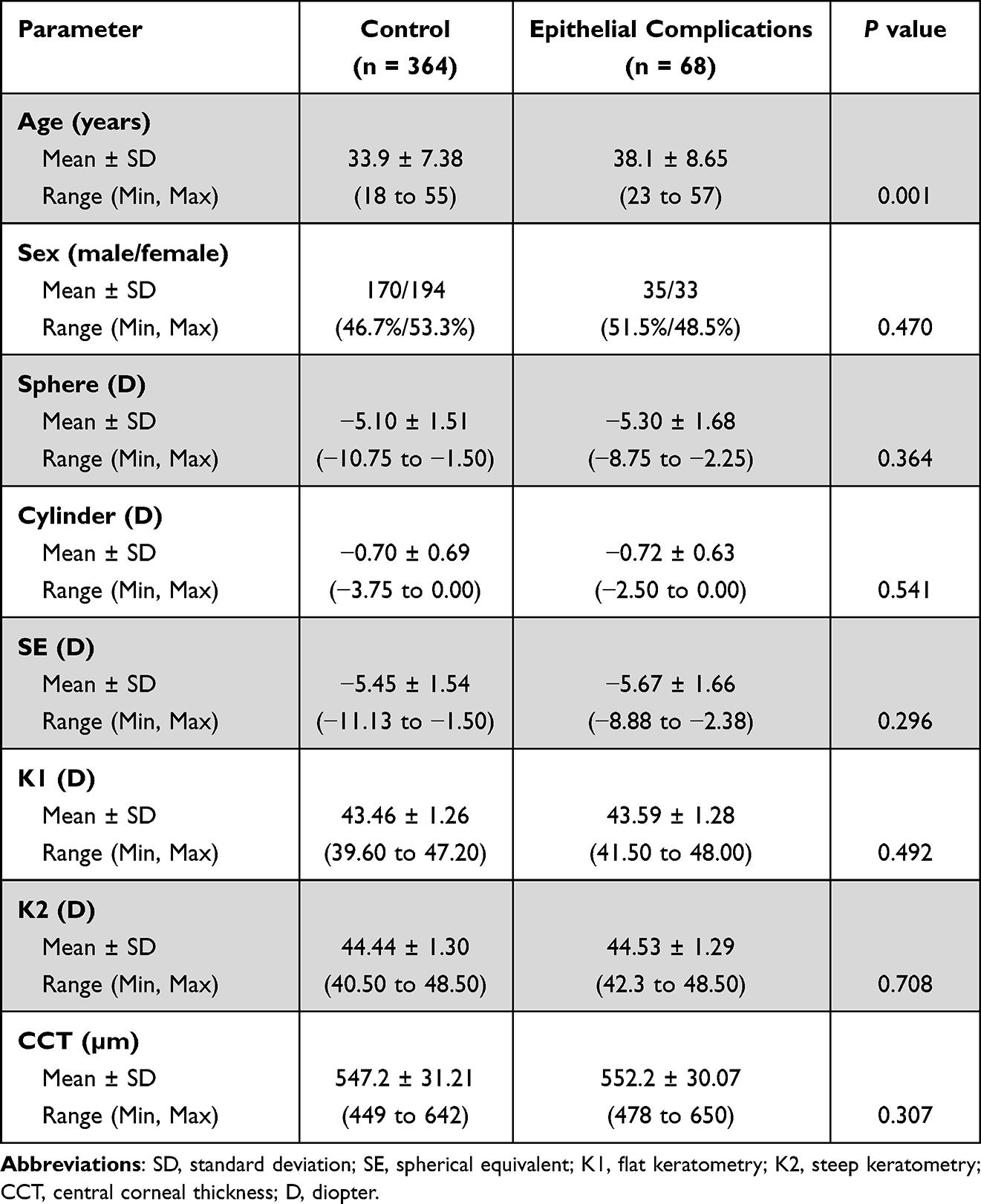 |
Table 1 Preoperative Patient Demographics (n = 432 Eyes) |
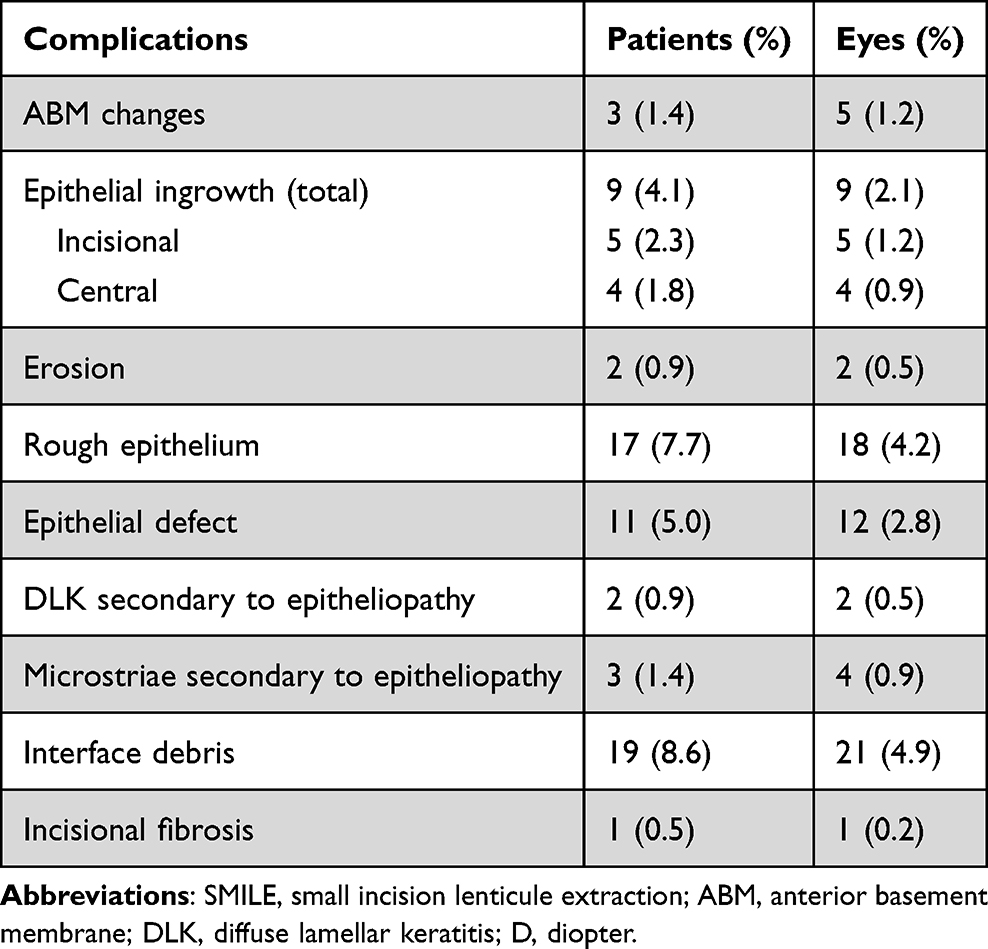 |
Table 2 Epithelial-Related Complications After SMILE |
Anterior Basement Membrane Changes
ABM changes following SMILE surgery were defined as microcysts within the epithelial tissue and irregular lines consisting of thickened basement membrane that extended into the epithelium. Five (1.2%) eyes from three (1.4%) patients presented with ABM changes. Of the three patients with ABM changes, two patients presented bilaterally, and one patient presented unilaterally in the left eye. In three eyes, ABM changes were noted from day one or day two, resolving by weeks three to seven after surgery. The remaining two eyes, from a single patient, were observed later in the postoperative period, first emerging at week two but still present at month six. All eyes attained a 20/20 or better UCVA at the last postoperative visit.
Epithelial Ingrowth
Epithelial ingrowth was classified here into two groups: incisional or central. An incisional ingrowth was attributed to the migration of epithelial cells through the SMILE incision, maintaining a connection with the incision. A central ingrowth was defined as the proliferation of epithelial cells secondary to the inadvertent introduction of these cells into the interface during the surgical procedure (Figure 1). It should be noted that ingrowths have been seen without a fistula to the incision after SMILE (Figure 2). Nine (2.1%) eyes presented unilaterally, with three in the right eye and six in the left eye. Four (44.4%) epithelial ingrowths were centrally isolated, and five (55.6%) were incisional. Each ingrowth was monitored for progression into the interface pocket. Of the nine eyes observed, seven epithelial ingrowths were self-limiting and resolved on their own, and two required intervention, with one ingrowth located centrally and the other near the incision. In the patient with the centrally located ingrowth, two areas of mild ingrowth at the interface were identified on day one. By week three, the two aforementioned areas had grown further, and by month one, the decision was made to remove the ingrowth due to increasing size. The other patient presented with an epithelial nest of cells, measuring 1.0 mm x 1.0 mm, noted near the incision, which grew over the course of one year and required attention. There was no recurrence of ingrowth noted in these patients. From the last postoperative visit, seven (77.8%) eyes achieved a UDVA of 20/20, and all eyes attained a CDVA of 20/20.
 |
Figure 1 Slit lamp images depicting various epithelial ingrowths after SMILE. White arrows point to red circled area of involvement; both speckled (A) and pooled (B) appearances are considered epithelial ingrowths. |
 |
Figure 2 Slit lamp image of an epithelial ingrowth without a fistula to the incision after SMILE. Green arrow points to an epithelial ingrowth that was self-limiting, while the black arrow points to the incision and absent fistula. |
Rough Epithelium
Rough epithelium was defined as irregular, loose, or not smooth epithelium. Eighteen (4.2%) eyes from 17 patients presented with rough epithelium immediately after surgery or on day one postoperatively. Of the 17 patients with rough epithelium after surgery, one patient presented bilaterally, and 16 patients presented unilaterally, with seven (43.8%) in the right eye and nine (56.3%) in the left eye. Out of the 17 eyes with incisional rough epithelium, the surgeon described 11 (64.7%) as rough and six (35.3%) as loose. Additionally, out of the 18 eyes, one (5.6%) presented with rough epithelium involving the central and paracentral aspects of the visual axis.
In two (11.1%) of these 18 eyes, intervention was indicated immediately after the completion of the surgery due to an epithelial remnant as well as loose epithelium that would likely increase the chance of developing an ingrowth or fibrosis at the incision site. Prompt action was warranted to improve visual outcomes. In both eyes, the epithelial defect was removed. By the last postoperative visit, 15 (83.3%) eyes achieved a UDVA of 20/25 or better, and all eyes attained a CDVA of 20/20.
Epithelial Defect
Epithelial defects were defined as focal areas with loss of the corneal epithelium. In 12 (2.8%) eyes from 11 patients, epithelial defects were noted. Of the 11 patients, one patient presented bilaterally, and 10 patients presented unilaterally, with nine (90.0%) defects in the right eye and one (10.0%) defect in the left eye. Eleven (91.7%) defects were located near the incision, and one (8.3%) defect was located centrally. Of these nine eyes, six (66.7%) had a bandage contact lens (BCL) inserted at the completion of the surgery and removed the following day. All epithelial defects were identified at the end of the surgery or on the first postoperative day. However, only one patient presented with a recurrent epithelial defect in one eye on postoperative week two, which required a BCL for several days to heal. All patients attained a UDVA of 20/25 or better by their last postoperative visit.
Corneal Erosion
Corneal erosion was attributed to poor adherence of the corneal epithelium to the underlying basement membrane presenting after the first postoperative week and outside the window of acute postoperative care. There were two cases (0.5%) of unilateral corneal erosion observed at postoperative week two and week six, respectively. It was important to emphasize that the latter patient did not have epitheliopathy prior to the corneal erosion. Both patients attained a UDVA of 20/25 or better at the last postoperative visit.
DLK Secondary to Epitheliopathy
DLK was defined by inflammatory infiltrates in the corneal flap interface (Figure 3). Although DLK can result from various etiologies, DLK associated with epitheliopathy was primarily analyzed in this study. There were two (0.5%) unilateral cases detected, but they occurred at different time points postoperatively. In one eye, DLK presented on the first day and resolved without any consequences by month one. In the other eye, DLK did not present until month six. Both eyes achieved a UDVA of 20/25 or better by the most recent postoperative visit.
 |
Figure 3 Slit lamp image of DLK observed after SMILE. White arrow indicates DLK, while yellow arrow indicates the SMILE incision; (B) illustrates a magnified depiction of (A). Abbreviation: DLK, diffuse lamellar keratitis. |
Microstriae Secondary to Epitheliopathy
Surface-level wrinkles of the epithelium were observed near the incision site in four (0.9%) eyes. In one eye, microstriae were documented on the first postoperative day. In the other three eyes, microstriae were not documented until three months after surgery. All eyes attained a UDVA of 20/25 or better by the last postoperative visit.
Interface Debris
Interface debris was composed of particles from the operating room and other minuscule foreign materials, including lint and fibers. There were 21 (4.9%) instances of debris detected. In four (19.0%) of these eyes, the debris was observed immediately following the conclusion of the surgery and removed then. Fifteen (71.4%) eyes obtained a UDVA of 20/25 or better, and all eyes achieved a CDVA of 20/20 at the last postoperative visit.
Incisional Fibrosis
Fibrosis was defined as an intense subepithelial scarring at the site of the corneal SMILE incision. In one (0.2%) eye, aggressive incision fibrosis was detected one year after surgery. This patient achieved a UDVA of 20/20 at their last postoperative visit.
Visual Acuity Overall
Of the 68 eyes with epithelial-related complications, 53 (78.6%) eyes achieved 20/40, 37 (55.7%) eyes achieved 20/25, and 16 (25.7%) eyes achieved 20/20 UDVA on the first day after surgery. From the eyes examined at three months postoperatively, 37 (84.1%) eyes achieved a UDVA of 20/25 or better, and no eyes lost two or more lines of CDVA. At six months after surgery, four eyes did not achieve a UDVA of 20/25 but achieved a UDVA of 20/25 or better at their last postoperative visit (Figures 4–6). Overall, 15 eyes (3.5%) underwent a PRK enhancement after SMILE (Table 3).
 |
Table 3 Postoperative Visual Outcomes from the Last Postoperative Visit |
 |
Figure 4 (A) Cumulative UDVA for the control and epithelial-related complications group at the last postoperative visit, (B) Cumulative CDVA for the control and epithelial-related complications group at the last postoperative visit. Abbreviations: UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity. |
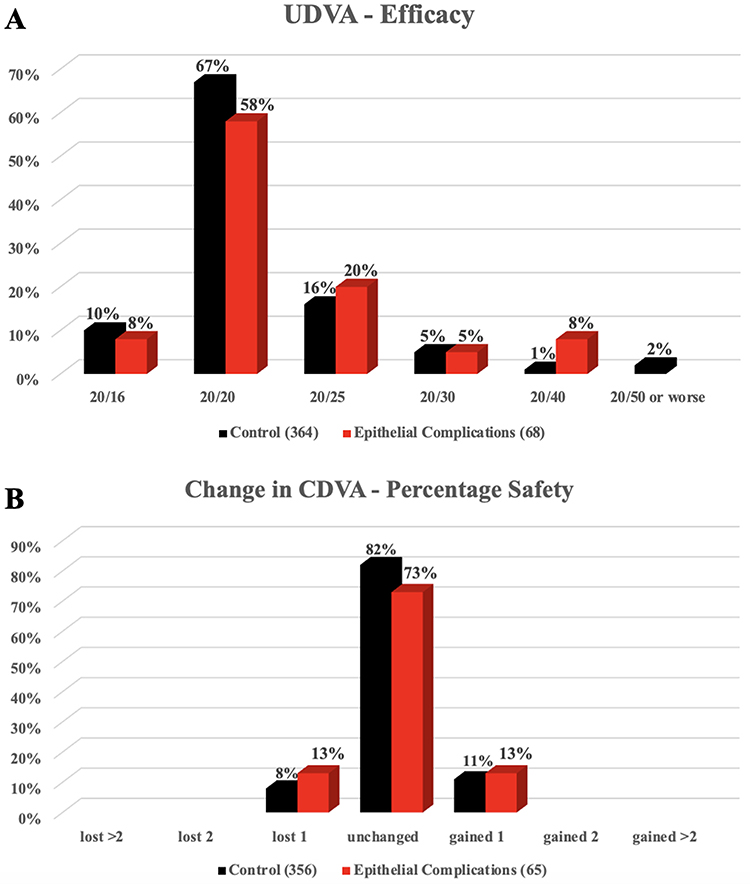 |
Figure 5 (A) UDVA (efficacy) of the control and epithelial-related complications group at the last postoperative visit, (B) Change in CDVA (safety) of the control and epithelial-related complications group at the last postoperative visit. Abbreviations: UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity. |
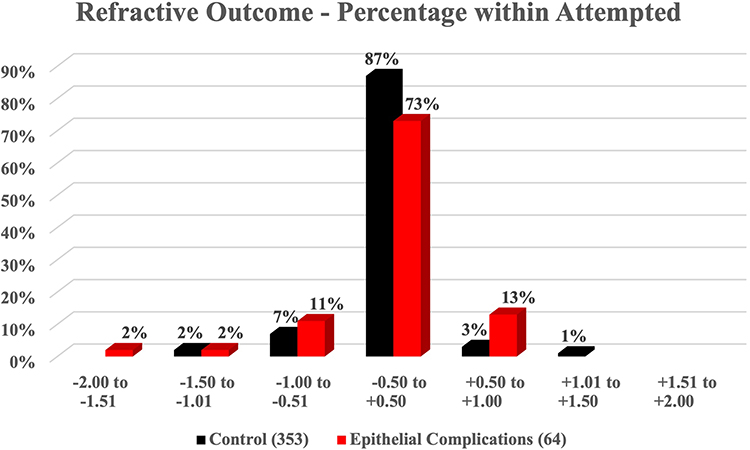 |
Figure 6 Refractive outcome between the control and epithelial-related complications group at the last postoperative visit. |
There was a statistically significant difference in UDVA on day one postoperatively (P = 0.023), which indicated that patients without epithelial-related complications had better visual acuity. However, no statistical difference was noted at three and six months and one year postoperatively (P = 0.064, 0.073, and 0.124). There was no statistically significant difference between the safety and efficacy indices of the epithelial-related complications group and the control at the last post-operative visit, with P-values of 0.261 and 0.617, respectively (Table 3).
Discussion
In this retrospective chart review, various epithelial-related complications following SMILE were analyzed. Of the 10 complication groups, these four were the most cited: interface debris, rough epithelium, epithelial defect, and epithelial ingrowth.
Interface debris was identified in 21 (4.9%) eyes in our study, corresponding with other sources reporting an incidence of 0.0% to 8.8%.1,8 In our patients, interface debris was accounted for in patients that had lint or fibers introduced during the surgery. Though careful attention was given to prevent the introduction of debris, the highly prevalent nature of debris made it difficult to avoid this epithelial-related complication. The authors speculate that the higher incidence observed in our case was because the stromal bed was not irrigated at the completion of the lenticule extraction to minimize manipulation during the surgical procedure. This method was traditionally recommended to reduce postoperative edema and achieve quicker satisfactory uncorrected visual acuity but may lead to a greater incidence of debris. Oftentimes, debris is asymptomatic as it does not impair visual acuity or cause inflammation. Management of these cases includes observation to monitor for progression. Nevertheless, significant amounts of debris can introduce inflammation or disrupt the central visual axis.9 In these situations, it is recommended to carefully but vigorously irrigate the region where the debris is located, as performed for patients in which debris was identified immediately after surgery.4
Studies have reported signs of rough epithelium, including epithelial sloughing, epithelial irregularity, and map-dot-fingerprint dystrophy, occurring after LASIK, with incidences of 0.32%,10 0.12%,11 and 0.36%,11 respectively. Our study noted rough epithelium in 18 (4.2%) eyes. These abnormalities are common symptoms of epithelial basement membrane disease, predisposing patients to loose epithelium that can be more easily dislodged and result in further complications.10 Pérez-Santonja et al and Oruçoğlu et al report that the development of such epithelial-related complications after LASIK may be a diagnostic marker for underlying epithelial basement membrane disease that was not diagnosed prior to the procedure.10,12 This is also an important consideration when evaluating patients for SMILE. Our study reported incidences of 1.2% for ABM changes and 0.2% for corneal erosion. Two (66.7%) patients presented with ABM changes bilaterally compared to one (33.3%) presenting unilaterally, a finding supported by literature that describes corneal dystrophy generally presenting bilaterally.13 In cases where there is suspicion of ABM changes, the utilization of optical coherence tomography (OCT) can be valuable for further examination. However, the diagnosis of ABM changes in our cohort was established with a thorough slit-lamp examination. In our experience, these changes did not manifest visually on OCT imaging. The incidence of these complications after SMILE is not well documented in medical literature, as SMILE is still considered a relatively recent refractive surgical procedure. Corneal erosion was treated with the insertion of a BCL and the administration of topical corticosteroid and topical broad-spectrum fluoroquinolone antibiotic therapy, resulting in a good visual prognosis. For all other cases, no intervention was required for recovery.
Epithelial defects occurred in 12 (2.8%) eyes, with one patient presenting bilaterally. Incidence for epithelial defects and abrasions after SMILE range from 0.17%6 to 7.4%.14 In another study, Ramirez-Miranda et al reported an incidence of 11.25% of epithelial defects after SMILE; however, the surgeons performing SMILE in this study were recently introduced to the SMILE surgical technique.15 This technique included the use of a spatula to remove the lenticule; however, it is noted that forceps can also be used for this process while performing the surgery. In comparison, the incidence of epithelial defects after LASIK surgery is observed to be 0.6% to 14%.16–18 Furthermore, two (0.46%) eyes were noted to have an epithelial defect after several weeks postoperatively. In one case, an acute epithelial defect was observed on the first day after surgery but recurred at postoperative week 2.5. In the other case, an abrasion was noted at postoperative month 1.5. These two patients were classified into the corneal erosion category, with an incidence of 0.46%, compared to 0.05–0.14% in LASIK, as reported by various studies.11,12,19
The corneal epithelium is composed of various structures, including hemidesmosomes, which contribute to adhesion mechanisms between the epithelium and the underlying basement membrane.20 When the hemidesmosomal connection is compromised, patients are predisposed to disturbances of the epithelium. The incidence of epithelial defects after SMILE in our study was within the range of incidence reported after LASIK. However, this complication was the third most common epithelial-related complication after SMILE observed from our retrospective review. In a study of epithelial fragility after LASIK performed with a mechanical keratome, Bashour reported that most epithelial defects were found at the superior region of the cornea, particularly close to the superior hinge.20 This study provides support for our hypothesis that there are weaker hemidesmosomal connections in the superior corneal epithelium, where the incision site for SMILE is located, increasing the likelihood of developing an epithelial defect or other basement membrane epitheliopathies in that region during the healing process. Most of the epithelial defects (11 [91.7%] eyes) observed in our study were at the site of SMILE incision, where the epithelium is looser, placing these patients at a higher risk for developing subsequent ingrowth. Only one (8.3%) eye had a central and paracentral epithelial defect, away from the incision site, likely attributed to loose ABM dystrophy, which increases the risk of recurrent corneal erosion.21 Thus, the authors recommend a low threshold for the placement of a BCL at the conclusion of such surgeries for any epitheliopathy involving the incision to prevent other complications from arising. BCLs are frequently used to alleviate discomfort after various laser refractive surgeries, especially PRK, but few studies have examined their use after SMILE.22 However, Wang et al explored this question and found that short-term use of BCL after SMILE provides comfort and pain relief, supporting our recommendation.22
Presentations of epithelial defects in our retrospective review included sections of the epithelium with a break or loose cells larger than an area of 2.0 mm x 2.0 mm.9 Previous studies have shown that epithelial defects after refractive surgery are heightened by certain risk factors, such as anterior basement membrane dystrophy and recurrent corneal erosion.9 Preventative measures to reduce the incidence of epithelial defect include sufficient hydration of the epithelium to prevent dry eye before surgery and limiting excessive corneal manipulation during the operation.23 Our treatment of an epithelial defect involves the use of topical corticosteroids and topical antibiotic therapy, placement of a BCL, and frequent lubrication of the eyes. These recommendations are supported by prior studies.9,23
Epithelial ingrowth was found in nine (2.1%) eyes following SMILE. Wang et al observed one case of epithelial ingrowth out of 6373 eyes, for an incidence of 0.02%.7 As reported in our study, epithelial ingrowths are often stable and only require monitoring, as they often resolve on their own.4 In cases of significant growth, management involves interface debridement with thorough irrigation, placement of a BCL, and topical corticosteroid and topical antibiotic therapy. Other studies treated an epithelial ingrowth using a neodymium:yttrium-aluminum-garnet (Nd:YAG) laser, a less invasive method.24,25 Careful examination of the patient immediately after SMILE should be conducted to prevent the development of epithelial ingrowths. Although the occurrence of an epithelial ingrowth is less likely to manifest at an early time point, typically becoming apparent around the 15-day mark, it is worth noting that ingrowths can also be observed on the first day following refractive surgery.26,27 Thus, surgeons should evaluate for any signs of epithelial cells at the incision or within the lenticule, predisposing patients to develop epithelial ingrowths. Likewise, a comparable phenomenon has been noted among individuals with a higher preoperative refractive error.28 This propensity may be attributed to factors including surgical trauma and modified healing responses, potentially facilitating the entry of epithelial cells.28 The authors believe this mechanism may be similar to what is observed in SMILE.
The incidence of microstriae in this study was 0.9%, which was higher than the incidence of 0.14% reported in a study by Wang et al7 Furthermore, patients who have undergone SMILE for high myopic correction are hypothesized to have a greater likelihood of developing microstriae postoperatively due to alterations in the corneal contour after SMILE.9 There was also variability in the timing of the identification of the microstriae. Nonetheless, these cases did not require intervention, as their CDVA was not affected and the microstriae were not as discernable over the course of the postoperative period over time. The authors speculate that the microstriae were less discernable due to the reduction of SMILE cap edema and epithelial hyperplasia. Striae are a very common complication observed after LASIK but often do not compromise visual outcomes after refractive surgery.29 However, if striae become visually significant, leading to the development of irregular astigmatism and a significant decline in visual acuity, further treatment options should be considered.30 In one case of striae after SMILE, Ganesh et al irrigated the interface and debrided the epithelium in the area of striae, then irrigated the exposed stroma and repositioned the striae into the proper alignment.31 This process is similar to the management of striae following LASIK.30
DLK associated with epitheliopathy was noted in two (0.5%) patients, both presenting unilaterally. The incidence of DLK after SMILE ranged from 0.45% to 2.2%, but the incidence of DLK secondary to an epithelial defect was lower at 0.10%.7,32 In our study, DLK in one patient was secondary to a corneal abrasion and occurred on the first day after surgery, similar to studies that report the emergence of DLK within the first five days postoperatively.32 However, for the second patient, DLK associated with epitheliopathy presented at month six postoperatively and was secondary to Staphylococcus marginal keratitis infection after the initiation of continuous positive airway pressure (CPAP) therapy. These patients were treated with topical corticosteroid therapy, a recommendation reinforced by previous studies.3,33
It is important to note that there was a significant difference in age between patients presenting with epithelial-related complications and the control group (P = 0.001). In analyzing different parameters between patients in the control group and those with epithelial-related complications, it was noted that the mean age for the epithelial-related complication group was older than that of the control. Thus, our data suggest that post-SMILE complications increase with age. This finding is supported by Min et al and Primavera et al, who also reported age as a contributing factor delaying corneal recovery when investigating nerve regeneration and refractive outcomes, respectively.34,35 However, to the best of the authors’ knowledge, our study is the first to examine the effect of age on various epithelial-related complications. Other studies have reported older age as a significant risk factor for intraoperative epithelial-related complications during LASIK, likely secondary to basement membrane changes that damage the adhesive connections with hemidesmosomes in the corneal epithelium.19 In addition, older individuals have been cited to have a higher risk of postoperative complications, including epitheliopathy-related complications, after LASIK.36
From the entire cohort, 15 (3.5%) eyes underwent a PRK enhancement after SMILE. Eight (2.2%) of these eyes were included in the control group, while seven (10.3%) of these experienced epithelial-related complications. There was a statistically significant difference in the rate of PRK enhancement, with a higher rate in patients in the epithelial-related complications group compared to the control (P = 0.001). Reports of PRK enhancement after SMILE note an incidence of 2.7%–3.7%.37,38 Patients who underwent enhancement exhibited suboptimal refractive outcomes subsequent to SMILE, characterized by residual refractive errors and an absence of UDVA of 20/20 or better.38 The frequency of epithelial-related complications in these patients led to a lack of spontaneous improvement in visual acuity, which served as a motivating factor to pursue PRK.5 Further studies should evaluate if patients who present with epitheliopathy-related complications after SMILE have a predilection for PRK enhancements. Overall, the visual prognosis of patients with epithelial-related complications was good. Despite a higher rate of PRK enhancement in this group, there was no significant difference in the cumulative UDVA, loss of CDVA, safety index, and efficacy index compared to the control at the last postoperative visit (Table 3).
Conclusion
This study examined the incidence and management of epithelial-related complications after SMILE. Despite the development of such complications, satisfactory visual prognoses could be achieved with various strategies. Our study found that epithelial-related complications were more prevalent in older patients and predisposed patients to require future PRK enhancements after recovery from SMILE. We encourage further studies to provide additional data to expand the literature on the postoperative epithelial-related complications of SMILE.
Acknowledgments
We would like to thank the patients that were involved in this retrospective study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol. 2011;95(3):335–339. doi:10.1136/bjo.2009.174284
2. Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: all-in-one femtosecond laser refractive surgery. J Cataract Refract Surg. 2011;37(1):127–137. doi:10.1016/j.jcrs.2010.07.033
3. Sahay P, Bafna RK, Reddy JC, Vajpayee RB, Sharma N. Complications of laser-assisted in situ keratomileusis. Indian J Ophthalmol. 2021;69(7):1658–1669. doi:10.4103/ijo.IJO_1872_20
4. Iskander NG, Peters NT, Penno EA, Gimbel HV. Postoperative complications in laser in situ keratomileusis. Curr Opin Ophthalmol. 2000;11(4):273–279. doi:10.1097/00055735-200008000-00009
5. Ivarsen A, Asp S, Hjortdal J. Safety and complications of more than 1500 small-incision lenticule extraction procedures. Ophthalmology. 2014;121(4):822–828. doi:10.1016/j.ophtha.2013.11.006
6. Wang Y, Ma J, Zhang J, et al. Incidence and management of intraoperative complications during small-incision lenticule extraction in 3004 cases. J Cataract Refract Surg. 2017;43(6):796–802. doi:10.1016/j.jcrs.2017.03.039
7. Wang Y, Ma J, Zhang L, et al. Postoperative corneal complications in small incision lenticule extraction: long-term study. J Refract Surg. 2019;35(3):146–152. doi:10.3928/1081597X-20190118-02
8. Xu Y, Yang Y. Small-incision lenticule extraction for myopia: results of a 12-month prospective study. Optom Vis Sci. 2015;92(1):123–131. doi:10.1097/OPX.0000000000000451
9. Shah DN, Melki S. Complications of femtosecond-assisted laser in-situ keratomileusis flaps. Semin Ophthalmol. 2014;29(5–6):363–375. doi:10.3109/08820538.2014.959194
10. Pérez-Santonja JJ, Galal A, Cardona C, Artola A, Ruíz-Moreno JM, Alió JL. Severe corneal epithelial sloughing during laser in situ keratomileusis as a presenting sign for silent epithelial basement membrane dystrophy. J Cataract Refract Surg. 2005;31(10):1932–1937. doi:10.1016/j.jcrs.2005.06.041
11. Mirshahi A, Bühren J, Kohnen T. Clinical course of severe central epithelial defects in laser in situ keratomileusis. J Cataract Refract Surg. 2004;30(8):1636–1641. doi:10.1016/j.jcrs.2004.02.052
12. Oruçoğlu F, Kenduşim M, Ayoglu B, Toksu B, Goker S. Incidence and management of epithelial loosening after LASIK. Int Ophthalmol. 2012;32(3):225–228. doi:10.1007/s10792-012-9557-x
13. Moshirfar M, Bennett P, Ronquillo Y. Corneal Dystrophy. In: StatPearls. StatPearls Publishing; 2023.
14. Ramirez -miranda A, Mangwani -mordani S, Hernandez -bogantes E, et al. Visual and refractive outcomes following SMILE to correct myopia performed by surgeons in training. J refract Surg. 2022;38(1):28–34. doi:10.3928/1081597X-20211209-01
15. Ramirez-Miranda A, Ramirez-Luquin T, Navas A, Graue-Hernandez EO. Refractive lenticule extraction complications. Cornea. 2015;34:S65. doi:10.1097/ICO.0000000000000569
16. Randleman JB, Lynn MJ, Banning CS, Stulting RD. Risk factors for epithelial defect formation during laser in situ keratomileusis. J Cataract Refract Surg. 2007;33(10):1738–1743. doi:10.1016/j.jcrs.2007.05.038
17. Moshirfar M, Gardiner JP, Schliesser JA, et al. Laser in situ keratomileusis flap complications using mechanical microkeratome versus femtosecond laser: retrospective comparison. J Cataract Refract Surg. 2010;36(11):1925–1933. doi:10.1016/j.jcrs.2010.05.027
18. Stephen MT, Farley ND, Tomasko KR, Amin SR. Intraoperative LASIK complications. Int Ophthalmol Clin. 2016;56(2). doi:10.1097/IIO.0000000000000110
19. Chen YT, Tseng SH, Ma MC, Huang FC, Tsai YY. Corneal epithelial damage during LASIK: a review of 1873 eyes. J Refract Surg. 2007;23(9):916–923. doi:10.3928/1081-597X-20071101-09
20. Bashour M. Risk factors for epithelial erosions in laser in situ keratomileusis. J Cataract Refract Surg. 2002;28(10):1780–1788. doi:10.1016/s0886-3350(02)01328-7
21. Fogle JA, Kenyon KR, Stark WJ, Richard Green W. Defective epithelial adhesion in anterior corneal dystrophies. Am J Ophthalmol. 1975;79(6):925–940. doi:10.1016/0002-9394(75)90674-1
22. Wang J, Xi S, Wang B, Chen Z, Zheng K, Zhou X. Clinical observation of silicon hydrogel contact lens fitted immediately after Small Incision Lenticule Extraction (SMILE). J Ophthalmol. 2020;2020:2604917. doi:10.1155/2020/2604917
23. Shah MN, Misra M, Wihelmus KR, Koch DD. Diffuse lamellar keratitis associated with epithelial defects after laser in situ keratomileusis. J Cataract Refract Surg. 2000;26(9):1312. doi:10.1016/S0886-3350(00)00570-8
24. Ayala MJ, Alió JL, Mulet ME, Hoz FDL. Treatment of laser in situ keratomileusis interface epithelial ingrowth with neodymium:yytrium–aluminum–garnet laser. Am J Ophthalmol. 2008;145(4):630–634.e2. doi:10.1016/j.ajo.2007.11.022
25. Lindfield D, Ansari G, Poole T. Nd:YAG laser treatment for epithelial ingrowth after laser refractive surgery. Ophthalmic Surg Lasers Imaging Retina. 2012;43(3):247–249. doi:10.3928/15428877-20120102-02
26. Srivatsa S, Sood S. Epithelial ingrowth following small incision lenticule extraction. Indian J Ophthalmol. 2020;68(12):3062–3064. doi:10.4103/ijo.IJO_941_20
27. Awad R, Awad K, Bakry A, Abdalla M. Femto-SMILE after photo-therapeutic keratectomy in an eye with failed LASIK flap: a case report. Am J Ophthalmol Case Rep. 2023;30:101852. doi:10.1016/j.ajoc.2023.101852
28. Friehmann A, Mimouni M, Nemet AY, Sela T, Munzer G, Kaiserman I. Risk factors for epithelial ingrowth following microkeratome-assisted LASIK. J Refract Surg. 2018;34(2):100–105. doi:10.3928/1081597X-20180105-01
29. Ambrósio R, Wilson SE. Complications of laser in situ keratomileusis: etiology, prevention, and treatment. J Refract Surg. 2001;17(3):350–379. doi:10.3928/1081-597X-20010501-09
30. Wallerstein A, Gauvin M, Adiguzel E, et al. Clinically significant laser in situ keratomileusis flap striae. J Cataract Refract Surg. 2017;43(12):1523–1533. doi:10.1016/j.jcrs.2017.09.023
31. Ganesh S, Ganesh SS, Gaster R, Brar S. Management of cap striae following challenging small incision lenticule extraction surgery – a case report. Indian J Ophthalmol. 2020;68(12):3060–3061. doi:10.4103/ijo.IJO_1487_20
32. Reinstein DZ, Stuart AJ, Vida RS, Archer TJ, Carp GI. Incidence and outcomes of sterile multifocal inflammatory keratitis and diffuse lamellar keratitis after SMILE. J Refract Surg. 2018;34(11):751–759. doi:10.3928/1081597X-20181001-02
33. Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: diagnosis and management. J Cataract Refract Surg. 2000;26(7):1072. doi:10.1016/S0886-3350(00)00468-5
34. Li M, Liu L, Shi Y, Sun L, Ma X, Zou J. Age-related differences in corneal nerve regeneration after SMILE and the mechanism revealed by metabolomics. Exp Eye Res. 2021;209:108665. doi:10.1016/j.exer.2021.108665
35. Primavera L, Canto-Cerdan M, Alio JL, Alio Del Barrio JL. Influence of age on small incision lenticule extraction outcomes. Br J Ophthalmol. 2022;106(3):341–348. doi:10.1136/bjophthalmol-2020-316865
36. Albietz JM, Lenton LM. Management of the ocular surface and tear film before, during, and after laser in situ keratomileusis. J Refract Surg. 2004;20(1):62–71. doi:10.3928/1081-597X-20040101-11
37. Liu YC, Rosman M, Mehta JS. Enhancement after small-incision lenticule extraction: incidence, risk factors, and outcomes. Ophthalmology. 2017;124(6):813–821. doi:10.1016/j.ophtha.2017.01.053
38. Moshirfar M, Parsons MT, Chartrand NA, et al. Photorefractive Keratectomy Enhancement (PRK) after Small-Incision Lenticule Extraction (SMILE). Clin Ophthalmol Auckl NZ. 2022;16:3033–3042. doi:10.2147/OPTH.S381319
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.