Back to Journals » Journal of Pain Research » Volume 11
Incidence and association factors for the development of chronic post-hysterectomy pain at 4- and 6-month follow-up: a prospective cohort study
Authors Sng BL ![]() , Ching YY, Han NLR, Ithnin FB, Sultana R, Assam PN, Sia ATH
, Ching YY, Han NLR, Ithnin FB, Sultana R, Assam PN, Sia ATH
Received 14 August 2017
Accepted for publication 12 February 2018
Published 27 March 2018 Volume 2018:11 Pages 629—636
DOI https://doi.org/10.2147/JPR.S149102
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Ban Leong Sng,1,2 Yin Ying Ching,3 Nian-Lin R Han,4 Farida Binte Ithnin,1 Rehena Sultana,5 Pryseley Nkouibert Assam,6 Alex Tiong Heng Sia1,2
1Department of Women’s Anaesthesia, KK Women’s and Children’s Hospital, Singapore, Singapore; 2Duke-NUS Medical School, Singapore, Singapore; 3Ministry of Health Holdings, Singapore, Singapore; 4Division of Clinical Support Services, KK Women’s and Children’s Hospital, Singapore, Singapore; 5Centre for Quantitative Medicine, Duke-NUS Medical School, Singapore, Singapore; 6Singapore Clinical Research Institute, Singapore, Singapore
Abstract: Chronic pain has major adverse effects on health-related quality of life and contributes to significant socioeconomic burden. Hysterectomy is a very common gynecological surgery, resulting in chronic post-hysterectomy pain (CPHP), an important pain syndrome. We conducted a prospective cohort study in 216 Asian women who underwent abdominal or laparoscopic hysterectomy for benign conditions. Demographic, psychological, and perioperative data were recorded. Postoperative 4- and 6-month phone surveys were conducted to assess the presence of CPHP and functional impairment. The incidence rates of CPHP at 4 and 6 months were 32% (56/175) and 15.7% (25/159), respectively. Women with CPHP at 4 and 6 months had pain that interfered with their activities of daily living. Independent association factors for CPHP at 4 months were higher mechanical temporal summation score, higher intraoperative morphine consumption, higher pain score in the recovery room, higher pain score during coughing and itching at 24 hours postoperatively, and preoperative pain in the lower abdominal region. Independent association factors for CPHP at 6 months were preoperative pain during sexual intercourse, higher mechanical temporal summation score, and higher morphine consumption during postoperative 24 and 48 hours. In a majority of cases, CPHP resolved with time, but may have significant impact on activities of daily living.
Keywords: chronic pain, hysterectomy, mechanical temporal summation score, postsurgical pain, central sensitization, morphine
Introduction
Chronic pain has major adverse effects on health-related quality of life and contributes to significant socioeconomic burden.1 The severity of pain leads to usage of health care and absence from work.2,3 Chronic postsurgical pain (CPSP) is defined as persistent pain that develops after a surgical procedure and lasts for at least 3 months with other causes of pain excluded.4 The incidence of CPSP could be up to 50%–60% depending on the type of surgery.4,5 High-risk surgeries, such as thoracic, amputation, mastectomy, and cardiac surgery,6–9 commonly lead to CPSP. Unfortunately, even simple minor procedures, for example, hernia repair and cholecystectomy have marked risk of developing CPSP.5
Hysterectomy is a commonly performed gynecological procedure that is associated with chronic post-hysterectomy pain (CPHP), with a reported incidence of 14%–50%.10–12 Risk factors have been suggested for the development of CPSP, including surgical technique, genetic susceptibility, significant perioperative pain, psychological factors, age, and female gender.13,14
Central sensitization is widely recognized as one of the major risk factors associated with chronic pain development. Central sensitization is defined as the increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input.15 Difference in the central process of peripheral tissue damages was believed to be one of the factors responsible for wide variability in pain perception. Higher mechanical temporal summation had been shown to predict acute provoked pain after thoracotomy, suggesting central pain augmentation or sensitization.16,17 However, few studies have associated preoperative physical testing with CPSP.18
In this study, we aimed to investigate women who were scheduled for elective abdominal or laparoscopic hysterectomy. Spielberger’s State–Trait Anxiety Inventory (STAI), Pain Catastrophizing Scale (PCS), preoperative surveys, and mechanical temporal summation physical pain test were conducted prior to the surgery. Phone surveys at 4 and 6 months after hysterectomy were also performed to identify demographic, psychological, and perioperative association factors for the development of CPHP.
By identifying the association factors for CPHP, the results of this study could elucidate potential mechanisms of CPSP development that will guide us in risk stratification and targeted therapy, such as minimizing injuries to peripheral sensory nerves by laparoscopic surgeries, cognitive behavior therapy or counseling for psychosocial factors, and ensuring adequate perioperative pain control.19
Materials and methods
This is a prospective cohort study involving women who were scheduled for elective abdominal or laparoscopic hysterectomy for benign conditions at KK Women’s and Children’s Hospital, Singapore. The SingHealth Centralized Institutional Review Board approved the study (CIRB ref.: 2013/512/D), and informed written consent was obtained. This trial is registered at Clinical.trials.gov. (NCT02025153).
The inclusion criteria were American Society of Anesthesiologists status 1 and 2 women between 21 and 70 years of age who underwent abdominal or laparoscopic hysterectomy for benign conditions (fibroids, adenomyosis). The exclusion criteria included vaginal hysterectomy, failure to adequately determine mechanical temporal summation, gynecological conditions such as uterine prolapse, endometriosis, malignant disease, or any other with the main indication being pelvic pain, and history of drug dependence or recreational drug use.
Patients were asked to complete STAI, PCS, preoperative surveys, and mechanical temporal summation physical pain testing prior to the surgery. The STAI is a self-reported tool for assessing anxiety and consists of two subscales, each containing 20 items on a four-point rating scale. The state anxiety subscale measures transient anxiety at the moment of scoring. Trait anxiety measures dispositional anxiety or anxiety in general.20 PCS contains 13 items which assess three components of catastrophizing: rumination, magnification, and helplessness, on a five-point scale.21 Preoperative survey comprised questions related to demographic data, history of lower abdominal pain, previous surgical history, and medical comorbidities (hypertension, diabetes mellitus, hyperlipidemia, pre-existing depression, thyroid diseases).22 Mechanical temporal summation is a dynamic test for central sensitization, associated with postoperative pain.17,23 Evoked mechanical temporal summation has been shown to predict acute provoked postoperative pain after thoracotomy, suggesting central pain augmentation or sensitization.
Intraoperative data such as use of analgesia were also recorded. After surgery, patients were asked to rate their pain scores (numerical rating scale: 0–10; 0=no pain, 10=worst pain imaginable) around the surgical scar at rest, when sitting at the edge of bed, and/or coughing, in the recovery area. The pain scores at postoperative 24, 48, and 72 hours were also collected in the ward.
Four- and 6-month postoperative phone surveys were conducted to assess the presence of CPHP and functional impairments. Each survey asked about pain duration in terms of “I don’t know/I don’t remember”, “less than 1 month”, “1–3 months”, “more than 3 months, but not now”, “I still have pain, ever since the operation”, “I still have pain, it started sometime after the operation”. In the 4-month pain survey, the primary outcome “patient is still in pain” was defined as follows: a patient mentioned any one of the last three options and with pain scores ≥3. Similarly, primary outcome in the 6-month survey was defined as a patient who selected any of the two above-mentioned options and with pain scores ≥3. Both outcomes of interest were treated as binary data with categories “yes” or “no”.
Statistical analysis
All categorical variables were presented as frequency with corresponding proportion, while all continuous variables were presented as mean±SD. The associations between outcomes and other categorical variables were evaluated using Fisher’s exact test, while the associations between outcomes and continuous variables were assessed using Student’s t-test. Univariate and multivariate logistic regression models were used to quantify the association between the potential covariates and the outcome of interest. The association from the logistic regression was characterized using odds ratio (OR) and corresponding 95% CI. Significance level was set at 0.05, and all tests were two-tailed. SAS version 9.3 software (SAS Institute, Cary, NC, USA) was used for the analysis.
Multivariate imputation using chained equations (MICE) is a practical approach to handle missing data.24,25 The imputation process has been described.25 We assumed that missing data being missing at random (MAR). A polytomous regression imputation method was also used for the variables with more than two categories. MICE method imputes missing values in different steps. All missing values were filled at random and multiple imputed data sets were generated. For each one of the imputed variables, an imputation model was built, considering all variables that were included in the subsequent analysis, as well as those that might be predictive of the missing values. The imputed data sets were analyzed separately and all the independent estimations were combined into an overall estimate. We created 500 imputed data for each 4- and 6-month outcome of interest. MICE package in R-software was used to perform the imputation of pain at 4- and at 6-month.21
Results
Two hundred sixteen women were recruited from September 2013 to January 2016 in this study (Figure 1). Two hundred and fifty-five women were screened, 30 women did not give consent for this study, and nine women did not meet the inclusion criteria. The response rates on the phone surveys at 4- and 6-months were 81.0% (175/216) and 73.6% (159/216), respectively. A total of 175 and 159 patients were included in the final analysis at 4- and 6-month phone surveys, respectively. Figure 1 shows the flow chart of the study.
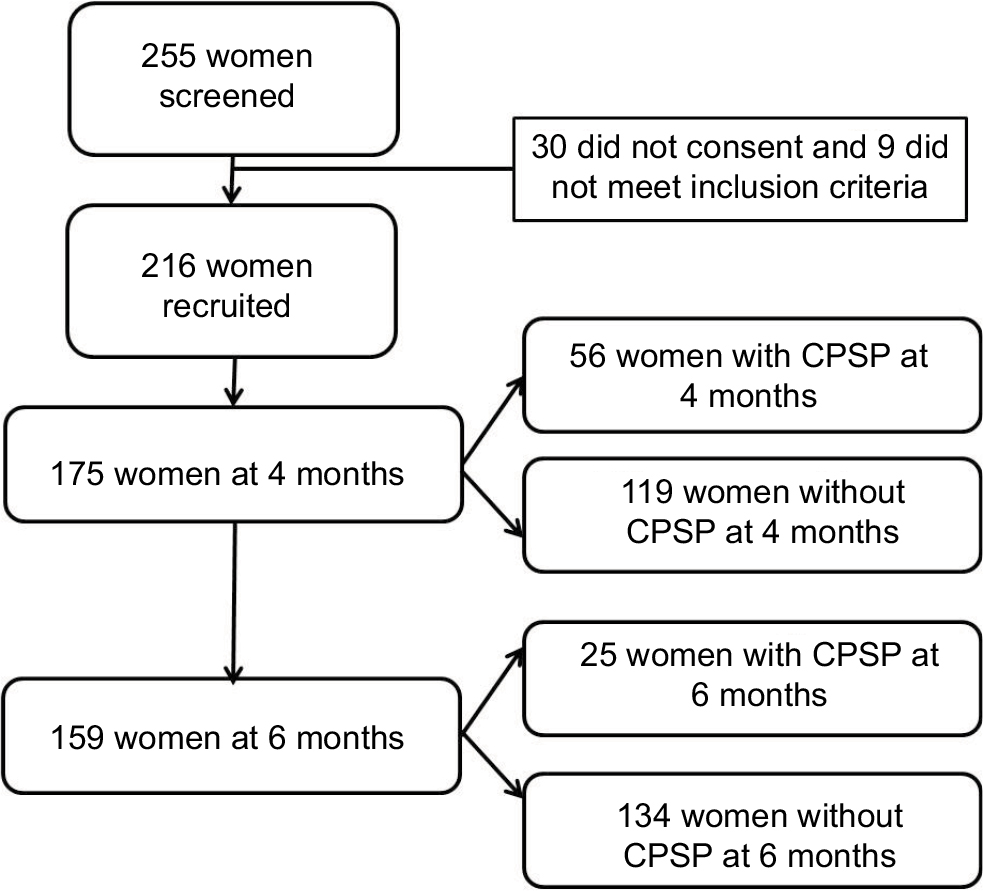 | Figure 1 Flow chart of the study subjects. Abbreviation: CPSP, chronic postsurgical pain. |
Baseline characteristics and comparisons are summarized in Table 1. Age, race, educational level, housing type, alcohol use, smoking, history of previous surgery (cesarean section, laparotomy, or laparoscopy), comorbidity (hypertension, diabetes mellitus, hyperlipidemia, pre-existing depression, thyroid diseases), types of surgery (laparotomy or laparoscopic hysterectomy), and postoperative complications were not associated with CPHP at 4- and 6-month follow-up (Table 1).
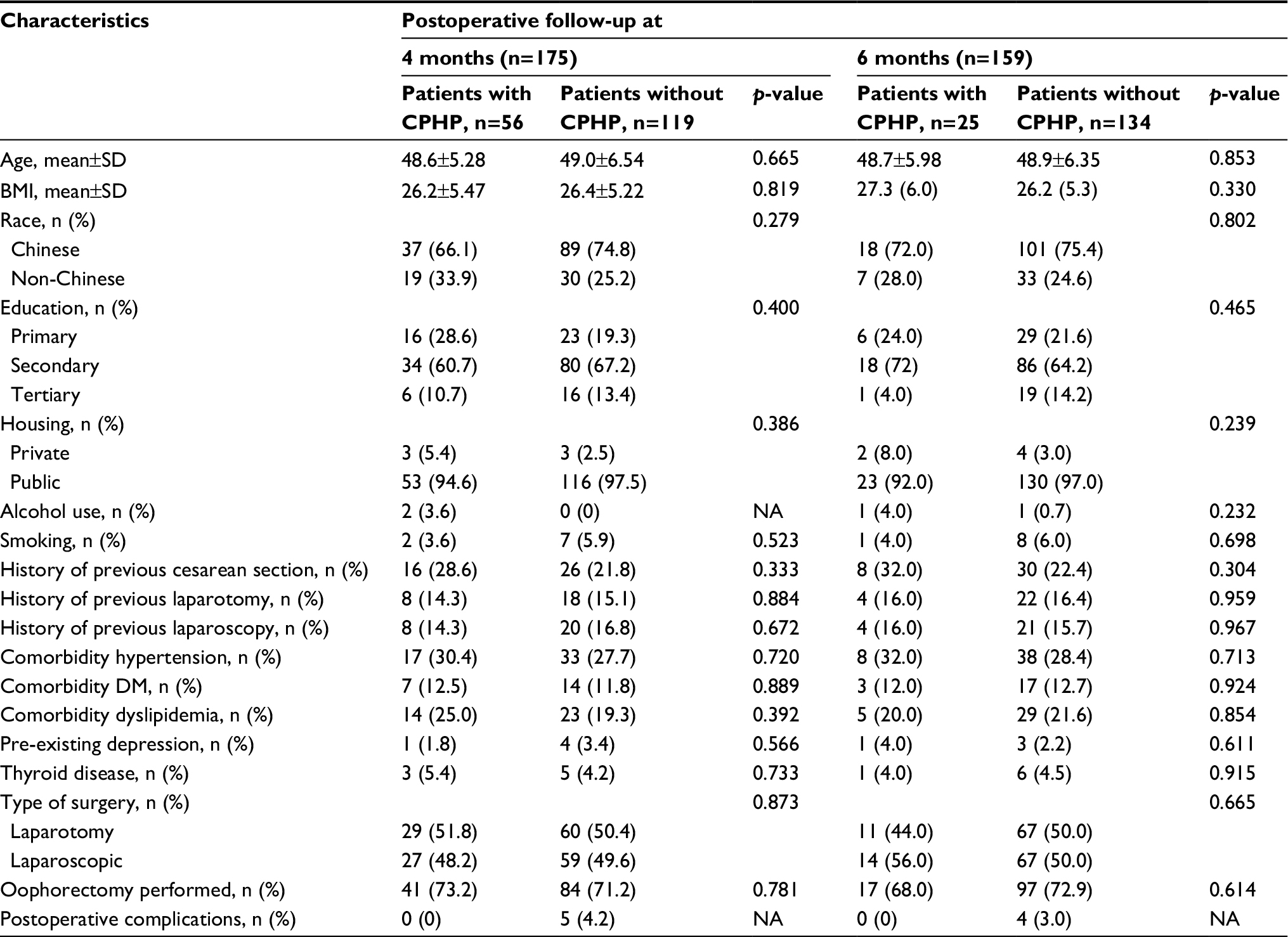 | Table 1 Comparison of baseline characteristics at 4 and 6 months Note: p-values are based on Student’s t-test for continuous variables and Fisher’s exact test for categorical variables. Abbreviations: BMI, body mass index; CPHP, chronic post-hysterectomy pain; DM, diabetes mellitus; NA, not applicable. |
Table 2 shows the comparison of perioperative events between patients with CPHP and those without CPHP at postoperative 4 and 6 months. Of the 175 patients who responded to the 4-month phone survey, 32% (56/175) reported persistent post-hysterectomy (CPHP) pain (numerical rating scale ≥3) for at least 4 months. The incidence of CPHP at 6 months was decreased to 15.7% (25/159). Based upon univariate analysis, patients with CPHP at 4 months were associated with higher pain score at the recovery room (p=0.001) and at 24 hours postoperatively when resting (p=0.015), higher PCS scores (p=0.011), especially rumination (p=0.020) and helplessness (p=0.017) subscores, as well as higher STAI total score (p=0.031) and trait anxiety scores (p=0.029). Women with CPHP at 6 months were associated with higher pain scores at the recovery room (p=0.008) and higher PCS scores (p=0.008), especially rumination (p=0.027) and helplessness (p=0.015) scores (Table 2).
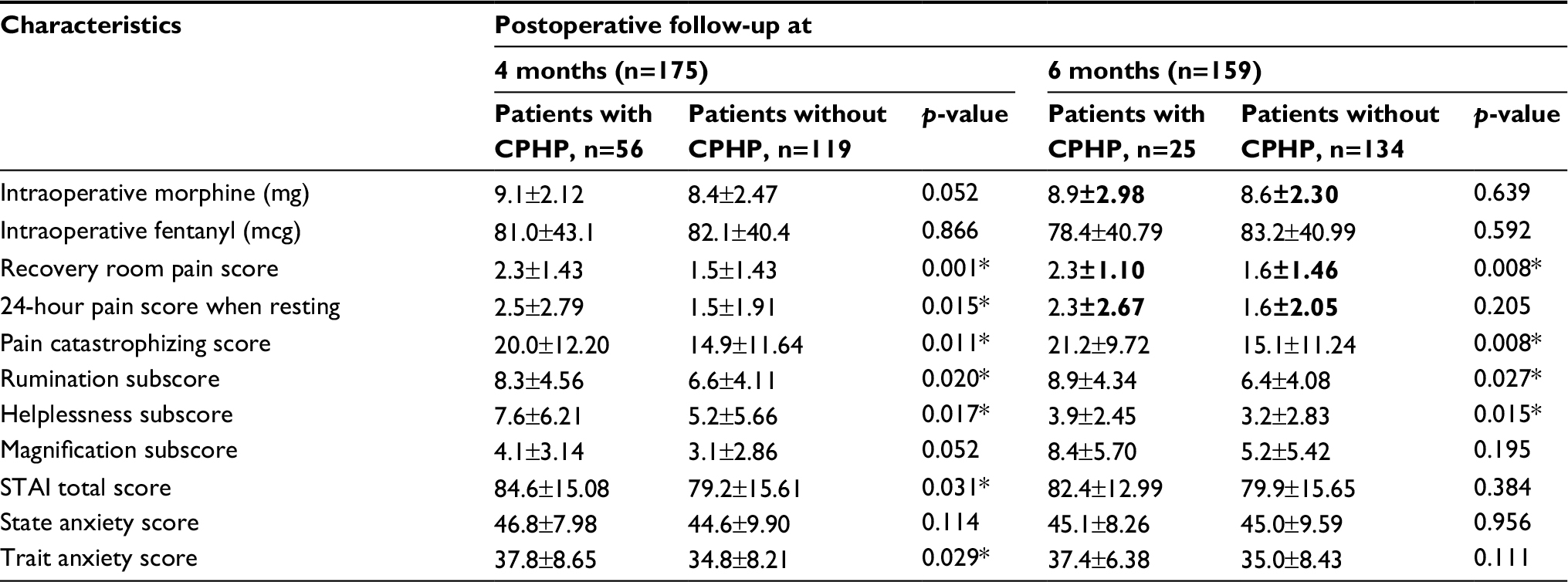 | Table 2 Comparison of perioperative events at 4 and 6 months Notes: All the values are expressed in terms of mean±SD. p-values are based on two-sample Student’s t-test. *p-value<0.05. Abbreviations: CPHP, chronic post-hysterectomy pain; STAI, State–Trait Anxiety Inventory. |
Women who developed CPHP at 4 and 6 months had pain that caused significant functional impairment in daily living. As shown in Table 3, of the 56 patients who reported persistent pain at 4-month survey, 38.2% reported pain affecting certain daily activities (p<0.001) such as getting up from a chair, prolonged sitting or standing, walking up or down stairs, and carrying heavy objects (Table 3). At the 6-month survey, of the 25 women who reported persistent pain, 24% reported pain that interfered with their sleep (p=0.031) and 44% reported pain affecting their daily activities (p<0.001) such as getting up from a chair and carrying heavy objects (Table 3).
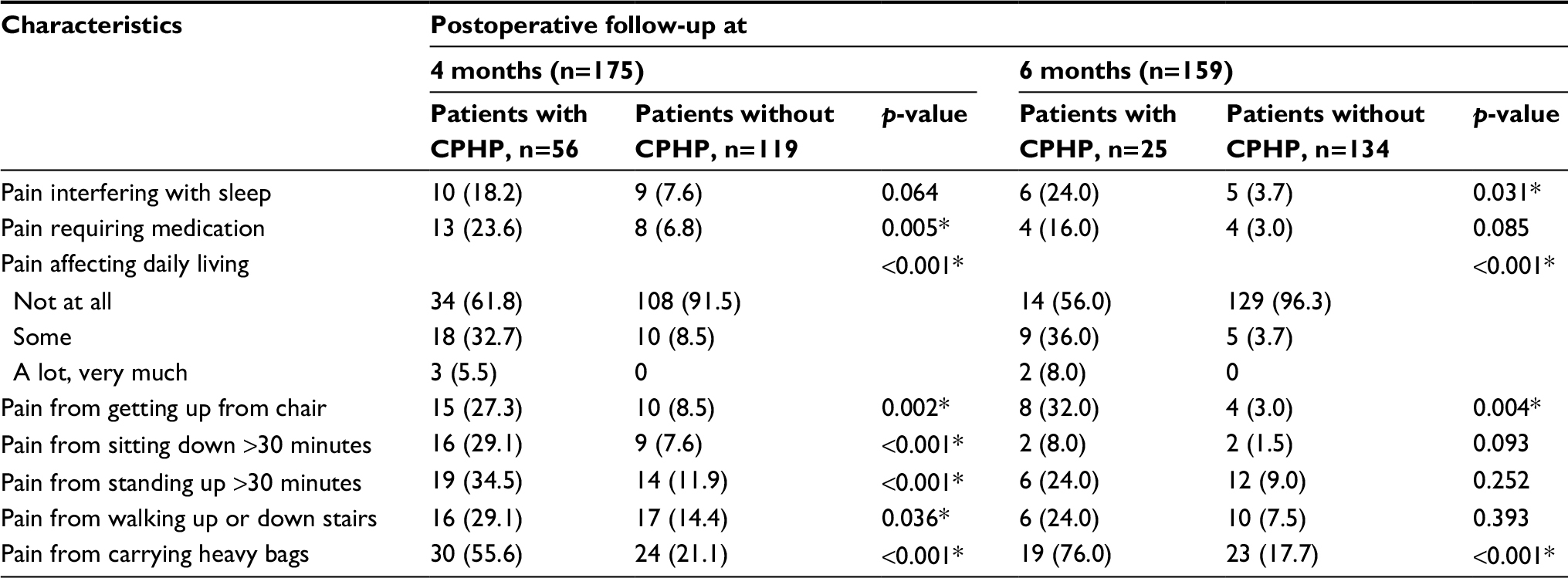 | Table 3 Functional impairment comparison at 4 and 6 months Notes: Values are expressed in terms of frequency (%). p-values are based on two-sample Fisher’s test. *p-value<0.05. Abbreviation: CPHP, chronic post-hysterectomy pain. |
Possible risk factors were considered in the multivariate logistic regression model to identify independent risk factors for persistent post-hysterectomy pain. The analysis results based on complete case data showed that higher mechanical temporal summation (OR 1.064, p=0.0002), higher pain score at the recovery room (OR 1.389, p=0.0153), 24-hour pain score while coughing (OR 1.135, p=0.0201), postoperative 24-hour itching (OR 3.327, p=0.0273), and preoperative lower abdominal pain (OR 8.546, p=0.0044) were associated with CPHP at 4 months (Table 4). Similarly, the independent risk factors for CPHP at 6 months on multivariate logistic regression based on complete data were higher mechanical temporal summation score (OR 1.078, p<0.001), preoperative experience of pain during sexual intercourse (OR 5.312, p=0.0158), and postoperative morphine consumption during 24-48 hours postoperatively (OR 1.172, p=0.0196; Table 5). Multivariate analysis based on the imputed data set produced similar results in terms of association between post-hysterectomy pain at 4 and 6 months, respectively.
 | Table 4 Multivariate logistics regression analysis at 4 months Notes: *p-value<0.05. Complete case refers to patients with complete baseline assessment and 4-month postoperative survey. Abbreviation: OR, odds ratio. |
 | Table 5 Multivariate logistics regression analysis at 6 months Notes: *p-value<0.05. Complete case refers to patients with complete baseline assessment and 6-month postoperative survey. Abbreviation: OR, odds ratio. |
Discussion
In our prospective cohort study in the Asian population, we investigated the development of CPHP at 4 and 6 months and found the incidence of CPHP to be 32% (56/175) and 15.7% (25/159), respectively. Women with CPHP at 4 and 6 months had pain that interfered with their activities of daily living. Several independent association factors were found, and most of the patients with CPHP had resolution of their pain at 6 months.
CPSP is an underappreciated chronic pain condition that has gained increasing attention, and several studies have reported varying incidence rates. Brandsborg et al previously reported that the incidence of CPHP at 4 months was 16.7%, which is lower than our result (32.0% [56/175]).12,18 It is interesting that Pokkinen et al found the incidence of CPHP at 6 months to be 26.0%, which is higher than our result (15.7%).10 Han et al described the incidence of CPHP at 3 months to be 27.7%, comparable with our finding.26 However, these studies only conducted a post-hysterectomy pain survey at one time point. Nevertheless, this study found that the incidence of CPHP decreased with time, suggesting the resolution of CPHP over time.
Women with CPHP reported significant functional limitations affecting their activities of daily living and sleep. This study also identified several significant association factors of CPHP development, such as experience of pain during sexual intercourse, higher mechanical temporal summation score, higher pain catastrophizing helplessness subscores preoperatively, higher intraoperative morphine consumption, and higher pain score in the immediate postoperative period. Hence, pain and psychological vulnerability could be important association factors with CPHP.
Higher mechanical temporal summation score and higher morphine consumption were independently associated with CPHP at 4 and at 6 months. Mechanical temporal summation is a dynamic test for central sensitization, which is associated with postoperative pain. Higher mechanical temporal summation has been shown to predict acute provoked pain after thoracotomy, suggesting central pain augmentation or sensitization.17,27 Such sensitization could be associated with nerve injury following surgical intervention. However, there is currently limited evidence of the association between mechanical temporal summation and chronic pain development.16 Our study suggests that the use of mechanical temporal summation could be associated with CPSP development, though more studies would be needed to validate this.
The roles of psychological factors such as anxiety, depression, and dysfunctional pain coping mechanism in the development of CPSP have been controversial.28–31 Pinto et al also found that pain catastrophizing, particularly helplessness subscore, could play an important role in pain development.11 This suggests that cognitive-affective therapy (cognitive behavior therapy, mindfulness therapy) could be an important target for treatment for CPHP. Of note, our study did not find an association of anxiety with CPHP.
Surgical nerve injury and neuropathic pain development could be one of the underlying causes of CPSP, thus leading to efforts to minimize nerve injury during surgery.13 Laparoscopic inguinal herniotomy and cholecystectomy are associated with lower CPSP, compared to the open approach.32–34 However, our study did not demonstrate this. Meltomaa et al35 also found that laparoscopy or laparotomy hysterectomy did not differ in CPHP incidence, suggesting deep visceral surgical injury to be the predominant factor. The association of acute postoperative pain intensity with chronic pain development was consistent with several previous studies;36–38 therefore, implementation of early, aggressive therapy for acute postoperative pain could reduce CPHP. Alternative therapy avoiding surgery could be considered for benign conditions.39,40 The minimally invasive uterine artery embolization has shown a good clinical success rate in reducing fibroid size.41
There are several limitations in this study. The assessment of possible confounding factors could be limited. We used available potential confounders such as diabetes mellitus, hypertension, dyslipidemia, and mood disorders that could be potential confounders. However, there could be unknown association factors not accounted for in our study design. The second limitation is that endometriosis, which is one of the most common gynecological diseases, was not studied.42,43 We felt that since endometriosis is associated with existing chronic pelvic pain condition, this could make the interpretation of our data difficult. Only females were recruited in this study; therefore, the effect of gender difference on CPSP cannot be evaluated. However, hysterectomy is a very common surgical procedure, making the disease burden very high. In addition, our study population was mainly Asian and this might not represent other populations, as pain could be influenced by ethnic and cultural differences.
In summary, the majority of CPHP cases recovered with time, but CPHP is associated with significant impact on activities of daily living. Independent association factors for CPHP include higher mechanical temporal summation scores and increased pain scores in the immediate postoperative period. Hence, these could be further investigated and modification in therapy could be targeted in these higher risk patients.
Acknowledgments
The authors would like to thank the clinical research coordinators (Agnes Teo, Liu Juan, Yvonne Yong), medical student (Tan Ze Yan), and the staff of the major operating theaters at KK Women’s and Children’s Hospital, Singapore for their support. They would like to acknowledge the NMRC Transition Award (NMRC/TA/017/2013) and the Centre Grant (NMRC/CG/006/2013) for the research funding.
A part of the results from this study were presented as:
Conference presentation at the 16th World Congress of Anaesthesiologists, 28 August–2 September 2016, Hong Kong (Abstract PR288). The abstract was published in “Anesthesia & Analgesia”, 2016;123(Issue 3S_Suppl):p. 373. doi: 10.1213/01.ane.0000492685.52766.e8.
Conference presentation at the Australian Pain Society 35th Annual Scientific Meeting on 15–18 March 2015, Brisbane, Australia. The abstract was published in “Anaesthesia & Intensive Care”, 2015;43(3):397.
Disclosure
The authors report no conflicts of interest in this work.
References
Harker J, Reid KJ, Bekkering GE, et al. Epidemiology of chronic pain in Denmark and Sweden. Pain Res Treat. 2012;2012:371248. | ||
Langley P, Muller-Schwefe G, Nicolaou A, Liedgens H, Pergolizzi J, Varrassi G. The societal impact of pain in the European Union: health-related quality of life and healthcare resource utilization. J Med Econ. 2010;13(3):571–581. | ||
Langley P, Muller-Schwefe G, Nicolaou A, Liedgens H, Pergolizzi J, Varrassi G. The impact of pain on labor force participation, absenteeism and presenteeism in the European Union. J Med Econ. 2010;13(4):662–672. | ||
Macrae WA. Chronic pain after surgery. Br J Anaesth. 2001;87(1):88–98. | ||
Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth. 2008;101(1):77–86. | ||
Peng Z, Li H, Zhang C, Qian X, Feng Z, Zhu S. A retrospective study of chronic post-surgical pain following thoracic surgery: prevalence, risk factors, incidence of neuropathic component, and impact on qualify of life. PLoS One. 2014;9(2):e90014. | ||
Nikolajsen L, Jensen TS. Phantom limb pain. Br J Anaesth. 2001;87(1):107–116. | ||
Jung BF, Ahrendt GM, Oaklander AL, Dworkin RH. Neuropathic pain following breast cancer surgery: proposed classification and research update. Pain. 2003;104(1–2):1–13. | ||
Kalso E, Mennander S, Tasmuth T, Nilsson E. Chronic post-sternotomy pain. Acta Anaesthesiol Scand. 2001;45(8):935–939. | ||
Pokkinen SM, Nieminen K, Yli-Hankala A, Kalliomaki ML. Persistent posthysterectomy pain: a prospective, observational study. Eur J Anaesthesiol. 2015;32(10):718–724. | ||
Pinto PR, McIntyre T, Nogueira-Silva C, Almeida A, Araujo-Soares V. Risk factors for persistent postsurgical pain in women undergoing hysterectomy due to benign causes: a prospective predictive study. J Pain. 2012;13(11):1045–1057. | ||
Brandsborg B, Dueholm M, Nikolajsen L, Kehlet H, Jensen TS. A prospective study of risk factors for pain persisting 4 months after hysterectomy. Clin J Pain. 2009; 25(4):263–268. | ||
Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. | ||
Reddi D, Curran N. Chronic pain after surgery: pathophysiology, risk factors and prevention. Postgrad Med J. 2014;90(1062):222–227; quiz 226. | ||
Loeser JD, Treede RD. The Kyoto protocol of IASP basic pain terminology. Pain. 2008;137(3):473–477. | ||
Yarnitsky D, Crispel Y, Eisenberg E, et al. Prediction of chronic post-operative pain: pre-operative DNIC testing identifies patients at risk. Pain. 2008;138(1):22–28. | ||
Landau R, Kraft JC, Flint LY, et al. An experimental paradigm for the prediction of Post-Operative Pain (PPOP). J Vis Exp. 2010;35:1671. | ||
Brandsborg B. Pain following hysterectomy: epidemiological and clinical aspects. Dan Med J. 2012;59(1):B4374. | ||
Thompson AR. Recognizing chronic postsurgical pain syndromes at the end of life. Am J Hosp Palliat Care. 2007;24(4):319–322. | ||
Spielberger CD, Gorssuch RL, Lushene PR, Vagg PR, Jacobs GA. Manual for the State-Trait Anxiety Inventory. Consulting Psychologists Press: Palo Alto, CA, USA; 1983. | ||
Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7:524–32. | ||
Sng BL, Sia AT, Quek K, Woo D, Lim Y. Incidence and risk factors for chronic pain after caesarean section under spinal anaesthesia. Anaesth Intensive Care. 2009;37(5):748–752. | ||
Weissman-Fogel I, Granovsky Y, Crispel Y, et al. Enhanced presurgical pain temporal summation response predicts post-thoracotomy pain intensity during the acute postoperative phase. J Pain. 2009;10(6):628–636. | ||
Acock AC. Working with missing values. J Marital Fam Ther. 2005; 67:1012–1028. | ||
White JR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat in Med. 2011;30:377–399. | ||
Han C, Ge Z, Jiang W, Zhao H, Ma T. Incidence and risk factors of chronic pain following hysterectomy among Southern Jiangsu Chinese Women. BMC Anesthesiol. 2017;17:103. | ||
Herrero JF, Laird JM, Lopez-Garcia JA. Wind-up of spinal cord neurones and pain sensation: much ado about something? Prog Neurobiol. 2000;61(2):169–203. | ||
Gerbershagen HJ, Dagtekin O, Rothe T, et al. Risk factors for acute and chronic postoperative pain in patients with benign and malignant renal disease after nephrectomy. Eur J Pain. 2009;13(8):853–860. | ||
Taillefer MC, Carrier M, Belisle S, et al. Prevalence, characteristics, and predictors of chronic nonanginal postoperative pain after a cardiac operation: a cross-sectional study. J Thorac Cardiovasc Surg. 2006;131(6):1274–1280. | ||
Riddle DL, Wade JB, Jiranek WA, Kong X. Preoperative pain catastrophizing predicts pain outcome after knee arthroplasty. Clin Orthop Relat Res. 2010; 468(3):798–806. | ||
Forsythe ME, Dunbar MJ, Hennigar AW, Sullivan MJ, Gross M. Prospective relation between catastrophizing and residual pain following knee arthroplasty: two-year follow-up. Pain Res Manag. 2008;13(4):335–341. | ||
Stiff G, Rhodes M, Kelly A, Telford K, Armstrong CP, Rees BI. Long-term pain: less common after laparoscopic than open cholecystectomy. Br J Surg. 1994;81(9):1368–1370. | ||
Liem MS, van der Graaf Y, van Steensel CJ, et al. Comparison of conventional anterior surgery and laparoscopic surgery for inguinal-hernia repair. N Engl J Med. 1997; 336(22):1541–1547. | ||
Laparoscopic versus open repair of groin hernia: a randomised comparison. The MRC Laparoscopic Groin Hernia Trial Group. Lancet. 1999;354(9174):185–190. | ||
Meltomaa SS, Makinen JI, Taalikka MO, Helenius HY. One-year cohort of abdominal, vaginal, and laparoscopic hysterectomies: complications and subjective outcomes. J Am Coll Surg. 1999; 189(4):389–396. | ||
Bisgaard T, Rosenberg J, Kehlet H. From acute to chronic pain after laparoscopic cholecystectomy: a prospective follow-up analysis. Scand J Gastroenterol. 2005; 40(11):1358–1364. | ||
Katz J, Jackson M, Kavanagh BP, Sandler AN. Acute pain after thoracic surgery predicts long-term post-thoracotomy pain. Clin J Pain. 1996;12(1):50–55. | ||
Tasmuth T, Kataja M, Blomqvist C, von Smitten K, Kalso E. Treatment-related factors predisposing to chronic pain in patients with breast cancer–a multivariate approach. Acta Oncol. 1997;36(6):625–630. | ||
Vitale SG, Padula F, Gulino FA. Management of uterine fibroids in pregnancy: recent trends. Curr Opin Obstet Gynecol. 2015;27(6):432–437. | ||
Vitale SG, Tropea A, Rossetti D, Carnelli M, Cianci A. Management of uterine leiomyomas in pregnancy: review of literature. Updates Surg. 2013;65(3):179–182. | ||
Vitale SG, Rosa VLL, Rossetti D, Rapisarda AMC, Laganà AS. Sexual function and psychological well-being after uterine artery embolization. It J Gynaecol Obstet. 2017; 29(2):7–9. | ||
Laganà AS, La Rosa VL, Rapisarda AMC, et al. Anxiety and depression in patients with endometriosis: impact and management challenges. Int J Womens Health. 2017; 9:323–330. | ||
Vitale SG, La Rosa VL, Rapisarda AM, Laganà AS. Comment on: “Impact of endometriosis on quality of life and mental health: pelvic pain makes the difference”. J Psychosom Obstet Gynaecol. 2017; 38(1):81–82. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.