Back to Journals » International Journal of General Medicine » Volume 11
In vitro biofilm formation by Staphylococcus aureus isolated from wounds of hospital-admitted patients and their association with antimicrobial resistance
Authors Neopane P, Nepal HP, Shrestha R ![]() , Uehara O
, Uehara O ![]() , Abiko Y
, Abiko Y
Received 4 October 2017
Accepted for publication 25 November 2017
Published 18 January 2018 Volume 2018:11 Pages 25—32
DOI https://doi.org/10.2147/IJGM.S153268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Puja Neopane,1,2 Hari Prasad Nepal,3 Rojeet Shrestha,4 Osamu Uehara,5 Yoshihiro Abiko2
1Department of Microbiology, Chitwan Medical College and Teaching Hospital, Bharatpur, Nepal; 2Division of Oral Medicine and Pathology, Department of Human Biology and Pathophysiology, School of Dentistry, Health Sciences University of Hokkaido, Tobetsu, Japan; 3Department of Microbiology, Trinity School of Medicine, Kingstown, St. Vincent and the Grenadines; 4School of Medicine, Washington University of Barbados, St. Philip, Barbados; 5Division of Disease Control and Molecular Epidemiology, Department of Oral Growth and Development, Health Sciences University of Hokkaido, Tobetsu, Japan
Introduction: Staphylococcus aureus including methicillin-resistant S. aureus (MRSA) has the propensity to form biofilms, and causes significant mortality and morbidity in the patients with wounds. Our aim was to study the in vitro biofilm-forming ability of S. aureus isolated from wounds of hospitalized patients and their association with antimicrobial resistance.
Materials and methods: Forty-three clinical isolates of S. aureus were obtained from 150 pus samples using standard microbiological techniques. Biofilm formation in these isolates was detected by tissue culture plate (TCP) method and tube adherence method (TM). Antimicrobial susceptibility test was performed using the modified Kirby–Bauer disk diffusion method as per Clinical and Laboratory Standards Institute guidelines. MRSA was detected using the cefoxitin disk test.
Results: Biofilm formation was observed in 30 (69.8%) and 28 (65.1%) isolates of S. aureus via TCP method and TM, respectively. Biofilm-producing S. aureus exhibited a higher incidence of antimicrobial resistance when compared with the biofilm nonproducers (P<0.05). Importantly, 86.7% of biofilm-producing S. aureus were multidrug resistant (MDR), whereas all the biofilm nonproducers were non-MDR (P<0.05). Large proportions (43.3%) of biofilm producers were identified as MRSA; however, none of the biofilm nonproducers were found to be MRSA (P<0.05).
Conclusion: Both the in vitro methods showed that S. aureus isolated from wound infection of hospitalized patients have high degree of biofilm-forming ability. Biofilm-producing strains have very high tendency to exhibit antimicrobial resistance, multidrug resistance and methicillin resistance. Regular surveillance of biofilm formation by S. aureus and their antimicrobial resistance profile may lead to the early treatment of the wound infection.
Keywords: biofilm, multidrug resistant, methicillin-resistant Staphylococcus aureus
Introduction
Biofilms are the aggregation of bacteria embedded in a self-produced extracellular matrix of exopolysaccharides (EPSs), proteins and some micromolecules such as DNA. They can form on both biotic and abiotic surfaces.1 Studies have confirmed using scanning electron microscopy and other molecular techniques that wounds are colonized by biofilms.2,3 Biofilm protects the microorganism from host defenses and impedes delivery of antibiotics which may cause impairment in wound healing.4,5
Staphylococcus aureus is an opportunistic pathogen implicated as the most common agent of skin and soft tissue infections. It exists in the nasopharynx, skin, eye, intestine and urogenital tract as normal flora. However, it can breach the skin barriers through the wound or surgical incision and cause infection. Furthermore, it has the ability to adhere to and form a biofilm on tissues or medical indwelling devices. S. aureus initially adheres to a solid substrate, after which cell–cell adhesion occurs; the bacteria then multiply to form a multilayered biofilm encased in EPS. In fact, biofilm formation involves the production of polysaccharide intercellular adhesin,6 which depends on the expression of the intercellular adhesion (IcaADBC) operon that encodes three membrane proteins (IcaA, IcaD and IcaC) and one extracellular protein (IcaB).7 In addition, several surface proteins have been involved in the biofilm formation process, including biofilm-associated protein,8 S. aureus surface protein G,9 fibronectin-binding proteins or staphylococcal protein A.10 Biofilm formation by S. aureus can lead to a delay in reepithelialization of the infected tissues, ultimately increasing healing time. S. aureus biofilms have been associated with chronic wounds like diabetic foot ulcer, pressure sores and venous ulcers.3 Detachment of matured biofilm of S. aureus is a prerequisite for the dissemination of wound infection.11
Methicillin-resistant S. aureus (MRSA) poses a great risk to patients with wounds; significant increase in both mortality and morbidity in humans has been reported in patients infected with MRSA due to the development of biofilms.12 MRSA are frequently resistant to a wide variety of antibiotics, and this is more pronounced in those having ability to form a biofilm. The S. aureus infections and biofilm formations, in addition to an increase in the length of hospital stay, are associated with more clinically important pathologies such as pneumonia, polyarthritis, necrotizing fasciitis, endocarditis and septicemia. Therefore, our aim was to study the in vitro biofilm-forming ability of S. aureus isolated from wounds of hospitalized patients and their association with antimicrobial resistance.
Materials and methods
This cross-sectional observational study was conducted in the Department of Microbiology, Chitwan Medical College and Teaching Hospital (CMCTH), Bharatpur, Nepal. A total 150 routine pus samples were obtained from wounds at various body sites of patients admitted in CMCTH. The samples were inoculated onto nutrient agar, blood agar and mannitol salt agar. Of the total samples, 43 grew S. aureus, which was identified by a standard microbiological techniques including Gram stain, catalase, coagulase, phosphatase and DNAase tests.13 Biofilm formation by these isolates was detected by two in vitro methods: tissue culture plate (TCP) method and tube adherence method (TM).
TCP method
This quantitative, gold standard method for biofilm detection was carried out as described by Christensen et al.7 In brief, a colony of S. aureus was isolated from a fresh agar plate and inoculated in 2 mL of trypticase soy broth. The broth was incubated overnight at 37 °C. The culture was then diluted to 1:100 with fresh medium. A sterile individual plate with 96 flat-bottom polystyrene wells was filled with 200 μL of the diluted culture. The control organisms were also processed in a similar manner. The plate was incubated at 37 °C for 24 hours. After incubation, the contents of each well were removed by gentle tapping. The wells were washed with 200 μL of phosphate buffer saline (pH 7.3) to remove free-floating bacteria. Biofilms formed by bacteria adherent to the wells were fixed by 99% methanol and stained with 0.1% crystal violet (CV). Excess stain was washed gently, and the plate was kept for drying. The optical density of the stained adherent biofilm was measured using a micro-ELISA auto-reader (HUMAN) at a wavelength of 570 nm. The experiment was performed in triplicate. Interpretation of biofilm production was performed as per the criteria described by Stepanovic et al,14 and the bacteria were categorized into biofilm nonproducers, or weak, moderate or strong biofilm producers.
Tube adherence method
The isolated organisms were inoculated in 5 mL trypticase soy broth in test tubes and incubated overnight at 37 °C along with the control organism.15 After incubation, the tubes were decanted, dried and stained with 0.1% CV. Subsequently, the tubes were washed gently and placed upside down for drying. Visible lining of the wall and bottom of the tube by a film was considered as positive. The results were scored visually as nonproducers, or weak, moderate or strong biofilm producers.
S. aureus ATCC 25923 and S. aureus ATCC 35556 were used as negative and positive controls, respectively, for the biofilm assay.
Antimicrobial susceptibility test
Antimicrobial susceptibility tests of the clinical isolates against different antimicrobials were performed in Müller–Hinton agar (MHA) using the standard disk diffusion technique (modified Kirby–Bauer method) and interpreted as per Clinical and Laboratory Standards Institute guidelines.16 The following antimicrobial agents were tested: ampicillin (10 µg), cefoxitin (30 µg), ciprofloxacin (5 µg), chloramphenicol (30 µg), clindamycin (2 µg), cotrimoxazole (25 µg), doxycycline (30 µg), erythromycin (15 µg), gentamicin (10 µg), minocycline (30 µg), rifampicin (5 µg), teicoplanin (30 µg), tetracycline (30 µg) and vancomycin (30 µg) (HiMedia Laboratories, Mumbai, Maharashtra, India). S. aureus ATCC 25923 was used as the control organism.
Isolates were considered multidrug resistant (MDR) based on the guidelines recommended by the joint initiative of the European Centre for Disease Prevention and Control (ECDC) and the Centers for Disease Control and Prevention (CDC).17 According to those guidelines, the isolates showing non-susceptibility to at least one agent in three or more antimicrobial categories were identified as MDR.
S. aureus isolates showing positive D zone test were considered as resistant to clindamycin.
Screening of MRSA
All the isolates identified as S. aureus were further screened for methicillin resistance using the cefoxitin disk.
Test inoculum (0.5 McFarland standards) was inoculated onto MHA by lawn culture. Cefoxitin disk (30 µg) was placed on the agar plate and incubated overnight at 37 °C. On the following day, the zones of inhibition were measured, and those ≤21 mm in diameter were considered to be MRSA.12
S. aureus ATCC 25923 and ATCC 43300 were used as negative and positive controls, respectively.
Ethical approval
This study was approved by the Institutional Review Committee (IRC) of CMCTH, Bharatpur, Chitwan, Nepal (Ref. No. CMC-IRC-64). Written informed consent was obtained from each of the patients from whom samples were collected.
Statistical analysis
SPSS software (version 17; SPSS, Chicago, IL, USA) was used for data analysis. Chi-square test was used for analysis of categorical data. A P-value of <0.05 was considered statistically significant.
Results
Detection of biofilm by two methods
Among 43 clinical isolates of S. aureus obtained from the wounds, biofilm formation was observed in 30 (69.8%) isolates by the TCP method and in 28 isolates (65.1%) by TM (Table 1). Of the total S. aureus isolates, 3 (6.97%) demonstrated strong biofilm production, 12 (27.90%) showed moderate production and 15 (34.88%) demonstrated weak biofilm production by the TCP method; on the other hand, the TM revealed strong production in 2 (4.65%) isolates, and moderate and weak production in 10 (23.25%) and 16 (37.20%) isolates, respectively. The use of both methods revealed 2 (4.65%) strong, 10 (23.25%) moderate and 13 (30.23%) weak biofilm producers (Table S1).
 | Table 1 Detection of biofilm producers by two different methods |
Considering TCP as the gold standard method, the sensitivity, specificity, positive predictive value, negative predictive value and accuracy were found to be 83.3%, 77%, 89.3%, 66.7% and 81.4%, respectively.
Antimicrobial resistance patterns
As shown in Table 2, the biofilm-producing S. aureus were associated with higher incidence of antimicrobial resistance when compared to the nonproducers: ampicillin (86.7% vs 76.9%, P=0.427), cefoxitin (43.3% vs 0%, P=0.007), cotrimoxazole (66.7% vs 30.8%, P=0.029), ciprofloxacin (60% vs 23.1%, P=0.026), erythromycin (50% vs 0%, P=0.002), clindamycin (20% vs 7.7%, P=0.315), gentamicin (50% vs 0%, P=0.002), tetracycline (10% vs 0%, P=0.237), chloramphenicol (3.3% vs 0%, P=0.505) and teicoplanin (6.7% vs 0%, P=0.340). All the isolates were sensitive to doxycycline, minocycline, rifampicin and vancomycin.
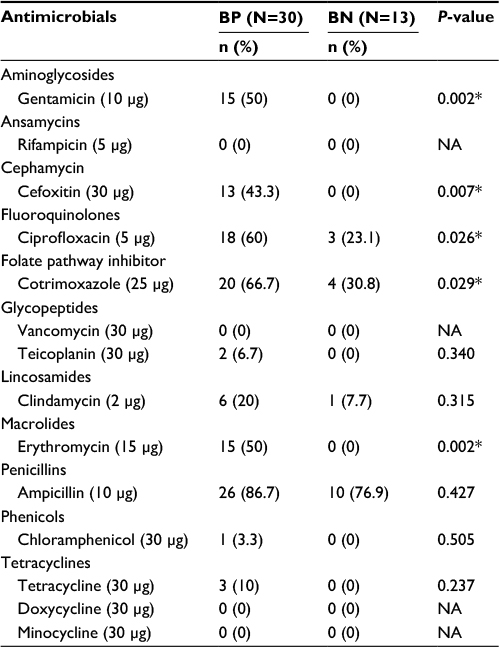 | Table 2 Antimicrobial resistance pattern of Staphylococcus aureus Note: *Statistically significant (P<0.05). Abbreviations: BP, biofilm producer; BN, biofilm nonproducer; NA, not applicable. |
Comparison of multidrug resistance and methicillin resistance in biofilm-positive and biofilm-negative S. aureus isolates
Of the total isolates, 26 (60.5%) were MDR; interestingly, out of 30 biofilm-positive isolates, 26 (86.7%) were MDR, whereas 4 (13.3%) were non-MDR. In contrast, no MDR isolates were noted among any of the biofilm nonproducers; in other words, all the biofilm nonproducers were non-MDR isolates (P<0.05; Table 3).
 | Table 3 Comparison of multidrug resistance and methicillin resistance in biofilm-positive and biofilm-negative Staphylococcus aureus isolates Abbreviations: MDR, multidrug resistant; MRSA, methicillin-resistant S. aureus; MSSA, methicillin-sensitive S. aureus. |
Furthermore, 13 (30.2%) of the total isolates were MRSA. Remarkably, 43.3% of biofilm producers were MRSA, whereas no MRSA isolates were noted among the biofilm nonproducers (P<0.05; Table 3).
Discussion
In spite of the various antimicrobial therapies available, the management of bacterial wound infections remains problematic.3 In the present study, we detected the in vitro biofilm-forming ability of S. aureus isolated from wounds of hospitalized patients and their association with antimicrobial resistance.
In this study, the detection and comparison of biofilm-forming ability were performed using two in vitro methods, TCP and TM, respectively. TCP has been used as a gold standard method, whereas TM is used as a screening test.18 Although TM is one of the simplest methods used, the presence of visible errors should be considered with the method.19 In the present study, the prevalence of biofilm formation was very similar in the two methods (69.8% and 65.1% biofilm formation was detected using the TCP and TM methods, respectively). In addition, we confirmed the accuracy of TM by measuring the sensitivity, specificity, positive predictive value and negative predictive value. Moreover, TM is cost effective and easily available which has to be taken under consideration in a developing country like Nepal. Therefore, TM may be used for the screening of biofilms during routine laboratory work at the general hospital.
Differences in the prevalence of biofilm formation have been reported, with data ranging from <50% to >70%.20–22 The prevalence of biofilm formation in the present study (69.8% was detected by TCP and 65.1% by TM) was in the higher range. Our data, using samples isolated from wound and pus, are similar to that of a previous report that showed 66.67% biofilm formation in the blood samples.23 The potential for biofilm formation in wounds and pus may be similar to that in the blood. Biofilm formation depends on many factors such as environment, availability of nutrients, geographical origin, types of specimen, surface adhesion characteristics and genetic makeup of the organism.24 These factors may have affected the data and contributed to the high prevalence observed in the present study. However, it is not known as to how these factors are involved. Biofilms can form on any wound when planktonic bacteria are not eliminated by the host’s immune system or by exogenous antimicrobial agents.25 In addition, mutations in Ica and regulatory genes have been associated with reduced capacity of S. aureus to form biofilms.26 Taken together, these factors may have affected the results in the present study. Further studies are needed to clarify these phenomena.
Identification of the adherence property of S. aureus has shown associations between biofilm formation and degree of pathogenicity, wherein the virulence property of the organism was found to vary with its ability to adhere to the surface.27 Therefore, the adherence property of biofilm producers was graded as strong, moderate and weak in both methods used in this study (TM and TCP). In the present study, 6.97% of the S. aureus were highly virulent showing strong adherence. Our result was consistent with another study from Algeria,28 which showed 4 (8%) strongly adherent, 10 (20%) moderately adherent, 20 (40%) weakly adherent and 16 (32%) nonadherent strains. Environmental factors like sugars (glucose or lactose) or proteases present in the growth medium, surface area, type of surface (rough/smooth), porosity, charge of the surface and the genetic makeup of the S. aureus isolate affect biofilm formation.29 The genes that are essential for biofilm formation are a subset of those involved in the pathogenesis.28 According to another report,30 IcaA-positive S. aureus can form a strong biofilm; however, MRSA isolates are Ica gene-independent, and even IcaA-negative isolates demonstrate weak biofilm production.31
Biofilm infections are clinically important because bacteria in biofilms exhibit recalcitrance to antimicrobial compounds.32 The biofilm-producing S. aureus were more resistant to various antimicrobials than the biofilm nonproducers.19,33 To eradicate the biofilm producers, high concentrations of antimicrobials may be necessary. However, this may not always be practical in vivo due to the risk of toxicity and related side effects. Therefore, low-concentration combination therapies may be effective to eradicate biofilm-related staphylococcal infections, including those by MRSA.34 The early detection and screening of biofilm producers followed by their antimicrobial susceptibility tests is important for the selection of an appropriate antimicrobial agent.
In our study, biofilm producers were resistant to erythromycin, gentamicin, tetracycline, cefoxitin, chloramphenicol and teicoplanin, whereas none of the biofilm nonproducers was resistant to these antibiotics (P<0.05). The resistant rates of biofilm producers to cotrimoxazole and ciprofloxacin were significantly higher than those of biofilm nonproducers (P<0.05). The higher rate of resistance in biofilm-producing Gram-positive bacteria toward erythromycin, cotrimoxazole and ciprofloxacin has been reported earlier.32 Our result provides support to those from a previous study in Nepal,35 which reported that resistance toward erythromycin and cotrimoxazole was increased due to the excessive use of these drugs for the treatment of both minor and more serious staphylococcal infections. Therefore, the antimicrobial resistance seen in the present study was higher among biofilm-producing S. aureus than among the nonproducers. These results indicate that biofilm formation may be one of the crucial factors for increasing resistance toward commonly used antibiotics.
Vancomycin is reported to be the most effective antibiotic for Gram-positive bacteria, including MRSA.36 Accordingly, our data also showed that all the isolates including biofilm producers were sensitive to vancomycin. This finding is consistent with the previously proposed suggestion that vancomycin is the last reserve antibiotic and one of the most expensive drugs that is sparingly used in Nepal.37
The multidrug resistance to most of the antimicrobials used in wound infections caused by S. aureus is an increasing problem.37 Therefore, surveillance of the antimicrobial resistance pattern of S. aureus is of utmost importance in the management of wound infections.35 According to the guidelines by the ECDC and CDC,17 we determined 86.7% of the biofilm-producing S. aureus as MDR. MDR was significantly higher in biofilm producers when compared with the biofilm nonproducers (P<0.05). The mechanism of multidrug resistance in biofilm-forming organisms is described as a direct result of close cell–cell contact in the biofilm, which facilitates easy transfer of plasmids containing MDR genes among one another.38 According to our data, only the biofilm producers were MDR; nevertheless, further investigations should be conducted in a larger numbers of samples.
MRSA strains are one of the MDR organisms that pose a great risk to wounded patients.35 In Nepal, incidence of MRSA was reported to be 20–43.1% by previous studies conducted between 2001 and 2013.35 In the present study, 30.2% of total S. aureus and 43.3% of biofilm-forming S. aureus were methicillin resistant which were recovered from wounds of hospitalized patients. The high incidence reported in this study may be attributed to the fact that MRSA is usually spread by direct contact via infected wound samples or contaminated hands of the health care providers.39
Another study showed that 3 of 11 biofilm-positive isolates obtained from indwelling medical devices were MRSA.18 The difference in the result between the two studies may be due to the limited number of samples used or the different sources of specimens in the previous study. In other study, 97.5% of biofilm producers from burn wound samples were MRSA.40 This may be due to the large area involved for the multiplication of S. aureus in burn wounds. Further, transmissions of MRSA are more common in burn wounds.
Conclusion
The clinical isolates of S. aureus recovered from wound infection of hospitalized patients exhibit a high degree of biofilm formation. Higher rate of antimicrobial resistance is demonstrated by biofilm producers than by biofilm nonproducers. The biofilm-positive strains have a higher tendency to exhibit multidrug resistance and methicillin resistance compared to biofilm-negative strains. This may lead to the high risk of impairment in the wound healing and dissemination of the infection enhancing morbidity and mortality of the admitted patients. Therefore, we recommend regular surveillance of biofilm formation in S. aureus wound isolates and their antimicrobial resistance profiles. This may help us to formulate an effective antimicrobial policy for the early treatment of wound infection.
Acknowledgments
The authors are grateful to the laboratory staff and management of CMCTH for their help and cooperation during the study.
Author contributions
P Neopane and Y Abiko conceived the design of the study. P Neopane and O Uehara were involved in laboratory procedure, data collection and analysis. P Neopane, Y Abiko, R Shrestha and HP Nepal prepared the manuscript. Y Abiko and O Uehara did interpretation of data and statistical analysis. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Gowrishankar S, Duncun Mosioma N, Karutha Pandian S. Coral-associated bacteria as a promising antibiofilm agent against methicillin-resistant and susceptible Staphylococcus aureus biofilms. Evid Based Complement Alternat Med. 2012;2012:862374. | ||
James GA, Swogger E, Wolcott R, et al. Biofilms in chronic wounds. Wound Repair Regen. 2008;16(1):37–44. | ||
Schierle CF, De la Garza M, Mustoe TA, Galiano RD. Staphylococcal biofilms impair wound healing by delaying reepithelialization in a murine cutaneous wound model. Wound Repair Regen. 2009; 17(3):354–359. | ||
Stewart PS. Mechanisms of antibiotic resistance in bacterial biofilms. Int J Med Microbiol. 2002;292(2):107–113. | ||
Gurjala AN, Geringer MR, Seth AK, et al. Development of a novel, highly quantitative in vivo model for the study of biofilm-impaired cutaneous wound healing. Wound Repair Regen. 2011;19(3):400–410. | ||
Ziebuhr W, Loessner I, Krimmer V, Hacker J. Methods to detect and analyze phenotypic variation in biofilm-forming Staphylococci. Methods Enzymol. 2001;336:195–205. | ||
Christensen GD, Simpson WA, Younger JJ, et al. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: a quantitative model for the adherence of staphylococci to medical devices. J Clin Microbiol. 1985;22(6):996–1006. | ||
Cucarella C, Solano C, Valle J, Amorena B, Lasa Í, Penadés JR. Bap, a Staphylococcus aureus surface protein involved in biofilm formation. J Bacteriol. 2001;183(9):2888–2896. | ||
Montanaro L, Speziale P, Campoccia D, et al. Scenery of Staphylococcus implant infections in orthopedics. Future Microbiol. 2011;6(11):1329–1349. | ||
Vergara-Irigaray M, Valle J, Merino N, et al. Relevant role of fibronectin-binding proteins in Staphylococcus aureus biofilm-associated foreign-body infections. Infect Immun. 2009;77(9):3978–3991. | ||
Otto M. Staphylococcal biofilms. Curr Top Microbiol Immunol. 2008;322:207–228. | ||
Doebbeling B. The epidemiology of methicillin-resistant Staphylococcus aureus colonisation and infection. J Chemother. 1995;7(Suppl 3):99–103. | ||
Baird D. Staphylococcus: cluster forming gram positive cocci. In: Collee JG, Fraser AG, Marmion BP, Simmons A, editors. Mackie and McCartney Practical Medical Microbiology. 14th ed. Vol. 2. London: Churchill Livingstone; 1996:245–261. | ||
Stepanovic S, Vukovic D, Hola V, et al. Quantification of biofilm in microtiter plates: overview of testing conditions and practical recommendations for assessment of biofilm production by staphylococci. APMIS. 2007;115(8):891–899. | ||
Christensen GD, Simpson WA, Bisno AL, Beachey EH. Adherence of slime-producing strains of Staphylococcus epidermidis to smooth surfaces. Infect Immun. 1982;37(1):318–326. | ||
Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; Seventeenth Informational Supplement. Document M100-S17. Wayne, PA: CLSI; 2007. | ||
Magiorakos AP, Srinivasan A, Carey R, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. | ||
Mishra SK, Basukala P, Basukala O, Parajuli K, Pokhrel BM, Rijal BP. Detection of biofilm production and antibiotic resistance pattern in clinical isolates from indwelling medical devices. Curr Microbiol. 2015;70(1):128–134. | ||
Mathur T, Singhal S, Khan S, Upadhyay D, Fatma T, Rattan A. Detection of biofilm formation among the clinical isolates of Staphylococci: an evaluation of three different screening methods. Indian J Med Microbiol. 2006;24(1):25–29. | ||
Samie A, Shivambu N. Biofilm production and antibiotic susceptibility profiles of Staphylococcus aureus isolated from HIV and AIDS patients in the Limpopo Province, South Africa. Afr J Biotechnol. 2011;10(65):14625–14636. | ||
Khan F, Shukla I, Rizvi M, Mansoor T, Sharma SC. Detection of biofilm formation in Staphylococcus aureus. Does it have a role in treatment of MRSA infections. Trends Med Res. 2011;6(2):116–123. | ||
Cha JO, Yoo JI, Yoo JS, et al. Investigation of biofilm formation and its association with the molecular and clinical characteristics of methicillin-resistant staphylococcus aureus. Osong Public Health Res Perspect. 2013;4(5):225–232. | ||
Poudel P, Adhikari N, Shah PK. Multi-drug resistant bacterial isolates associated with blood stream infection. ASRJETS. 2015;14(2):23–52. | ||
Kokare CR, Chakraborty S, Khopade AN, Mahadik KR. Biofilm: importance and applications. Indian J Biotechnol. 2009;8:159–168. | ||
Hurlow J, Couch K, Laforet K, Bolton L, Metcalf D, Bowler P. Clinical biofilms: a challenging frontier in wound care. Adv Wound Care (New Rochelle). 2015;4(5):295–301. | ||
Beenken KE, Dunman PM, McAleese F, et al. Global gene expression in Staphylococcus aureus biofilms. J Bacteriol. 2004;186(14):4665–4684. | ||
Baddour LM, Christensen GD, Hester MG, Bisno AL. Production of experimental endocarditis by coagulase-negative staphylococci: variability in species virulence. J Infect Dis. 1984;150(5):721–727. | ||
Lotfi G, Hafida H, Nihel K, et al. Detection of biofilm formation of a collection of fifty strains of Staphylococcus aureus isolated in Algeria at the University Hospital of Tlemcen. J Bacteriol Res. 2014;6(1):1–6. | ||
Christensen BB, Sternberg C, Andersen JB, et al. Establishment of new genetic traits in a microbial biofilm community. Appl Environ Microbiol. 1998;64(6):2247–2255. | ||
Moretro T, Schirmer BCT, Heir E, Fagerlund A, Hjemli P, Langsrud S. Tolerance to quaternary ammonium compound disinfectants may enhance growth of Listeria monocytogenes in the food industry. Int J Food Microbiol. 2017;241:215–224. | ||
Ando E, Monden K, Mitsuhata R, Kariyama R, Kumon H. Biofilm formation among methicillin-resistant Staphylococcus aureus isolates from patients with urinary tract infection. Acta Med Okayama. 2004;58(4):207–214. | ||
Hassan A, Usman J, Kaleem F, Omair M, Khalid A, Iqbal M. Detection and antibiotic susceptibility pattern of biofilm producing Gram positive and Gram negative bacteria isolated from a tertiary care hospital of Pakistan. Malays J Microbiol. 2011;7(1):57–60. | ||
CharanKaur D, Khare AS. Biofilm formation and antibiotic susceptibility pattern in MRSA strains in a tertiary care rural hospital. IJAR. 2013;3(1):37–44. | ||
Wu WS, Chen CC, Chuang YC, et al. Efficacy of combination oral antimicrobial agents against biofilm-embedded methicillin-resistant Staphylococcus aureus. J Microbiol Immunol Infect. 2013;46(2):89–95. | ||
Ansari S, Nepal HP, Gautam R, et al. Threat of drug resistant Staphylococcus aureus to health in Nepal. BMC Infect Dis. 2014;14:157. | ||
Lundstrom TS, Sobel JD. Antibiotics for gram-positive bacterial infections. Infect Dis Clin North Am. 2000;14(2):463–474. | ||
Percival SL, McCarty SM, Lipsky B. Biofilms and wounds: an overview of the evidence. Adv Wound Care (New Rochelle). 2015;4(7):373–381. | ||
Mah TF, O’Toole GA. Mechanisms of biofilm resistance to antimicrobial agents. Trends Microbiol. 2001;9(1):34–39. | ||
Lee BY, Bartsch SM, Wong KF, et al. The importance of nursing homes in the spread of methicillin-resistant Staphylococcus aureus (MRSA) among hospitals. Med Care. 2013;51(3):205–215. | ||
Moghadam SO, Pourmand MR, Aminharati F. Biofilm formation and antimicrobial resistance in methicillin-resistant Staphylococcus aureus isolated from burn patients, Iran. J Infect Dev Ctries. 2014;8(12):1511–1517. |
Supplementary material
 | Table S1 Grading of biofilm producers by two different methods Abbreviations: S, strong; M, moderate; W, weak. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.