Back to Journals » Infection and Drug Resistance » Volume 14
In Vitro Activity of Vancomycin, Teicoplanin, Linezolid and Daptomycin Against Methicillin-Resistant Staphylococcus aureus Isolates Collected from Chinese Hospitals in 2018–2020
Authors Xu Y, Wang B, Zhao H, Wang X, Rao L, Ai W, Yu J, Guo Y, Wu X, Yu F, Chen S
Received 5 October 2021
Accepted for publication 23 November 2021
Published 16 December 2021 Volume 2021:14 Pages 5449—5456
DOI https://doi.org/10.2147/IDR.S340623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yanlei Xu,1 Bingjie Wang,1 Huilin Zhao,1 Xinyi Wang,1 Lulin Rao,2 Wenxiu Ai,2 Jingyi Yu,1 Yinjuan Guo,1 Xiaocui Wu,1 Fangyou Yu,1 Shuying Chen2
1Department of Clinical Laboratory Medicine, Shanghai Pulmonary Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China; 2Department of Laboratory Medicine, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
Correspondence: Fangyou Yu
Department of Clinical Laboratory Medicine, Shanghai Pulmonary Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China
Email [email protected]
Shuying Chen
Department of Laboratory Medicine, the First Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
Email [email protected]
Introduction: Vancomycin, teicoplanin, linezolid and daptomycin are four major antibacterials used for methicillin-resistant Staphylococcus aureus (MRSA) infection treatment. However, with the increasing failure of clinical MRSA anti-infective treatment, it is urgent to investigate the status of MRSA sensitivity to these four drugs.
Methods: In the present study, 407 non-duplicated MRSA isolates from 6 provinces in China were collected from January 2018 to August 2020. The minimum inhibitory concentrations (MICs) of vancomycin, teicoplanin, linezolid and daptomycin were determined by broth microdilution method, and their MIC50, MIC90, and geometric mean MIC were calculated.
Results: All 407 MRSA strains were sensitive to these four antibacterials. MIC range of vancomycin, teicoplanin, linezolid and daptomycin was 0.25 to 2 mg/L, 0.125 to 4 mg/L, 0.25 to 4 mg/L and 0.06 to 1 mg/L, respectively. Between 2018 and 2020, there was no “MIC creep” in vancomycin, teicoplanin and daptomycin. The geometric mean MIC of linezolid was not increased, but both MIC50 and MIC90 in 2019 and 2020 MRSA isolates were higher than 2018 isolates.
Conclusion: All MRSA isolates remained sensitivity to vancomycin, teicoplanin, linezolid and daptomycin. The linezolid MIC50 and MIC90 increased have been found in this study.
Keywords: methicillin-resistant Staphylococcus aureus, vancomycin, teicoplanin, linezolid, daptomycin, MICs
Introduction
Staphylococcus aureus (S. aureus) is an important pathogen of humans which can cause a series of infections, such as skin and soft tissue infections, pneumonia, septic arthritis, endocarditis, osteomyelitis, endovascular infections, foreign-body infections and sepsis.1 Methicillin, a β-lactam antibiotic, was introduced to treat S. aureus infections in 1959. Within 2 years of its introduction, in 1961, the United Kingdom reported the first methicillin-resistant S. aureus (MRSA) strain.2 Worryingly, compared with methicillin sensitive S. aureus (MSSA), infections caused by MRSA are associated with higher mortality, higher healthcare costs, and longer hospital stays.3,4
In the fight against MRSA, glycopeptide antibiotics (GPAs) are key weapons, especially vancomycin still a mainstream therapy against MRSA infections more than 50 years after it was first introduced.5 Teicoplanin is also a common glycopeptide antibiotic for treating severe MRSA infections. In some cases, teicoplanin can become an alternative to vancomycin because of the low incidence of adverse effects like nephrotoxicity and remains active against some vancomycin-resistant strains, such as vanB-type vancomycin-resistant strains.6,7 In addition to vancomycin and teicoplanin, linezolid (an oxazolidinone antibiotic) and daptomycin (a cyclic lipopeptide antibiotic) were also last resort antibiotics to treat MRSA infections.
However, with the extensive use of these drugs, reports on the emergence of drug non- susceptible strains have also increased. The first vancomycin-intermediate S. aureus (VISA) and the first vancomycin-resistant S. aureus (VRSA) strain were detected in Japan in 1997 and in the United States in 2002, respectively.8,9 The prevalence of VRSA has increasing in recent years, particularly in Africa/Asia.10 Although VRSA has not been reported in China, but cases of heterogeneous vancomycin-intermediate S. aureus (hVISA) and VISA were frequently reported, and even included patients with no vancomycin administration history.11,12 Currently, resistance to daptomycin has rarely been reported, while it is thought to be easier to develop drug resistance during the treatment.13 Linezolid resistance is mainly mediated by strains carrying the cfr gene, which leads to transferable linezolid resistance, and has been sporadically isolated in China.14,15
Some investigations observed the shift phenomenon of vancomycin MICs, and this phenomenon was also present in other three antibacterials.16,17 Although this is still a disputed concept. To investigate the current situation of MRSA susceptibility to these drugs in China, and whether the four drugs have “MIC creep” phenomenon. We collected 407 MRSA isolates from 6 provinces including Shanghai, Jiangxi, Zhejiang, Hubei, Sichuan and Guangdong to evaluate the MICs of vancomycin, teicoplanin, linezolid and daptomycin in China.
Materials and Methods
MRSA Clinical Isolates
A total of 407 MRSA isolates (single isolate per patient) isolated from 3 different specimens were randomly collected from 6 hospitals located in 6 provinces, between January 2018 and August 2020. The proportions of MRSA isolates isolated from 3 specimens were as follows: 32.43% (132/407), blood; 28.75% (117/407), pus; 38.82% (158/407), sputum. And the proportions of 3 years were 33.17% (135/407), 2018; 34.64% (141/407), 2019; 32.19 (131/407), 2020. S. aureus identification was performed using MALDI-TOF-MS (Bruker Daltonics, Bremen, Germany). MRSA was rechecked by cefoxitin susceptibility test (broth microdilution method and disk diffusion method), and further confirmed by mecA polymerase chain reaction (PCR).
Antimicrobial Susceptibility Testing
Vancomycin (MCE, USA), teicoplanin (MCE, USA), linezolid (MCE, USA) and daptomycin (MCE, USA) MICs for MRSA isolates were determined by broth microdilution (BMD) method according to the CLSI (2020) recommendation. When testing linezolid MIC, trailing growth can make end-point determination difficult, read the MIC at the lowest concentration where the trailing begins. And daptomycin MIC was performed in MHB (BD, USA), with a calcium supplement to a final concentration of 50 μg/mL, tiny buttons of growth were ignored. Interpretive standards for antimicrobial susceptibility followed criteria established by the CLSI. The susceptibility breakpoint for vancomycin, teicoplanin, linezolid and daptomycin were MIC ≤ 2 mg/L, MIC ≤ 8 mg/L, MIC ≤ 4 mg/L and MIC ≤ 1 mg/L, respectively. And vancomycin MIC ≥ 16 mg/L, teicoplanin MIC ≥ 32 mg/L, and linezolid MIC ≥ 4 mg/L were defined as resistance. S. aureus strain ATCC 29213 was used for quality control.
Data Treatment
The MIC-related parameters geometric mean MIC (geometric mean of MIC values, GM MIC), MIC50 (MICs required to inhibit the growth of 50% of bacteria), MIC90 (MICs required to inhibit the growth of 90% of bacteria), and MIC range were evaluated. The geometric mean is suitable for ratios and exponential, and the MIC value is exponential amplification.18 We used χ 2 test to compare categorical variations. The statistical analyses were accomplished using SPSS software (SPSS, Chicago, IL, USA). A P-value of < 0.05 was considered statistically significant.
Results
MIC-Related Parameters Among MRSA Isolates
For all of the 407 tested MRSA isolates, 100% were susceptible to vancomycin, teicoplanin, linezolid and daptomycin according to 2020 CLSI guidelines. The vancomycin MICs for 407 MRSA clinical isolates tested range from 0.25 mg/L to 2 mg/L, with the GM MIC of 0.54 mg/L, MIC50 of 0.5 mg/L, and MIC90 of 1 mg/L. The teicoplanin MICs range from 0.125 mg/L to 4 mg/L, with the GM MIC of 0.40 mg/L, MIC50 of 0.25 mg/L, and MIC90 of 1 mg/L. The linezolid MICs range from 0.25 mg/L to 4 mg/L, with the GM MIC of 0.89 mg/L, MIC50 of 1 mg/L, and MIC90 of 2 mg/L. The daptomycin MICs range from 0.06 mg/L to 1 mg/L, with the GM MIC of 0.25 mg/L, MIC50 of 0.25 mg/L, and MIC90 of 0.5 mg/L. The proportion of isolates MIC reaching the high end of vancomycin, teicoplanin, linezolid and daptomycin CLSI susceptibility range MIC = 2 mg/L, MIC = 8 mg/L, MIC = 4 mg/L, MIC = 1 mg/L were 0.49%, 0%, 1.72%, 5.90%, respectively. These four antibacterials MIC-related parameters among MRSA isolates from different clinical specimens are exhibited in Table 1. The MIC-related parameters of vancomycin, linezolid and daptomycin were similar for blood, pus and sputum MRSA isolates. However, the teicoplanin GM MIC for sputum isolates (0.47 mg/L) were remarkably higher than blood isolates (0.36 mg/L) and pus isolates (0.33 mg/L), and it also had higher teicoplanin MIC50 and MIC90.
 |
Table 1 MIC-Related Parameters from Different Specimens |
Comparison of MIC-Related Parameters for MRSA Isolates in Different Regions
Comparing the MICs of these four antibacterials in the six provinces, we found that the MRSA isolated from Zhejiang had the lowest GM MIC for each drug, and it also had the lowest daptomycin MIC50 (0.125 mg/L) and vancomycin MIC90 (0.5 mg/L) than other regions. Furthermore, the teicoplanin GM MIC (0.60 mg/L) and MIC90 (2 mg/L) were highest for Hubei isolates. Sichuan and Shanghai isolates had higher linezolid MICs, with GM MIC of 1.08 mg/L and 1.05 mg/L, respectively, with MIC90 both were 2 mg/L. Guangdong MRSA isolates had the highest daptomycin GM MIC (0.36 mg/L) and MIC50 (0.5 mg/L) (Table 2).
 |
Table 2 MIC-Related Parameters from Different Regions |
MIC Decline for Vancomycin, Teicoplanin and Daptomycin Was Exhibited in MRSA Isolates
The MIC-related parameters GM MIC, MIC50, MIC90, and MIC range of 2018–2020 for these four antibacterials are exhibited in Table 3. Compared with 2018, the GM MIC of vancomycin, teicoplanin and daptomycin had declined. Although linezolid GM MIC of 2019 (0.84 mg/L), 2020 (0.88 mg/L) were also decreased compared with 2018 (0.90 mg/L), the linezolid MIC90 of 2019 (2 mg/L) and 2020 (2 mg/L) were higher than 2018 (1 mg/L). Mostly due to the percentage of linezolid MIC ≥ 2 mg/L MRSA isolates in 2019 and 2020 were increased. The MICs distribution for each drug from 2018 to 2020 are shown in Figure 1. The proportion of isolates with higher MICs decreased in 2019 and 2020, such as that of vancomycin MIC = 1 mg/L, teicoplanin MIC = 1 mg/L, 2 mg/L, daptomycin MIC = 0.5 mg/L.
 |
Table 3 MIC-Related Parameters, 2018–2020 |
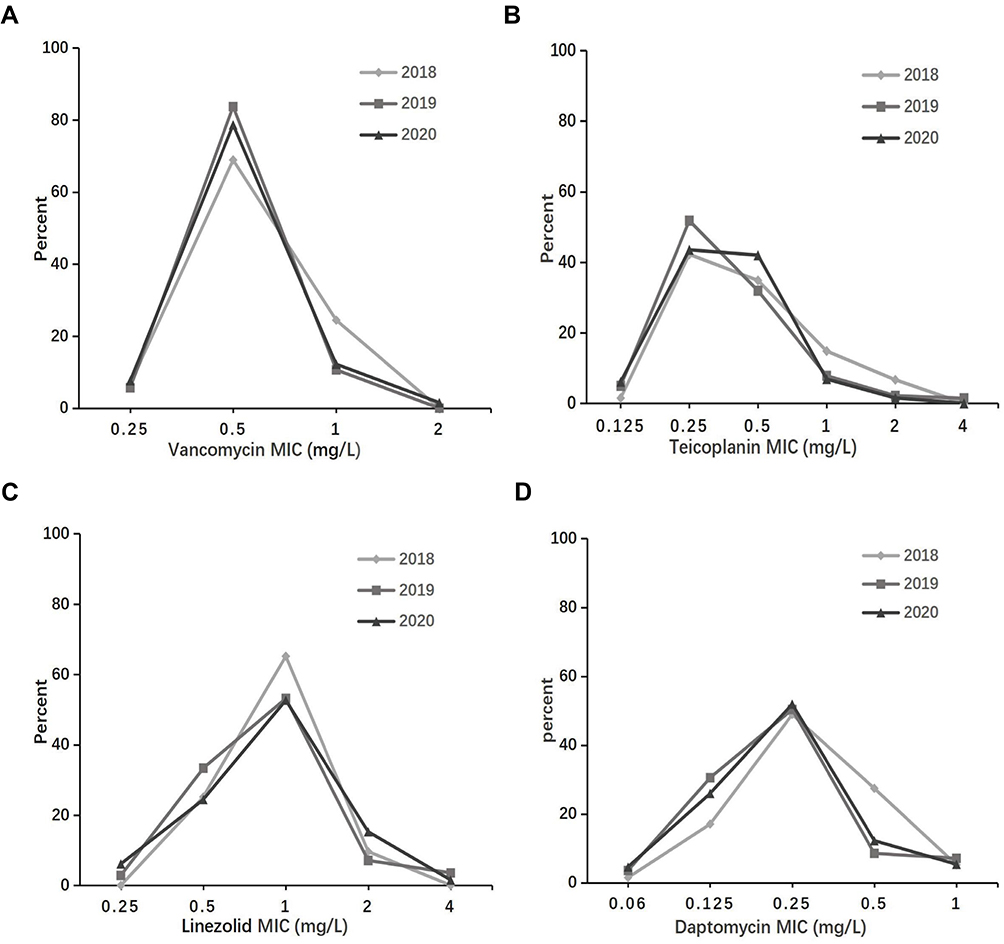 |
Figure 1 Trend over time of antimicrobial susceptibility of MRSA isolates in 2018 (n = 135), in 2019 (n = 141), and 2020 (n = 131) against vancomycin (A) teicoplanin (B) linezolid (C) and daptomycin (D). |
Stratified Analysis of Susceptibility of Teicoplanin, Linezolid and Daptomycin by Vancomycin MIC Values
Compared to the in vitro activities of these three drugs against MRSA stratified by vancomycin MIC values (<1 mg/L versus ≥1 mg/L) (Table 4). The MIC50, MIC90 and GM MIC of teicoplanin for isolates with vancomycin MIC ≥1 mg/L were higher than isolates with vancomycin MIC <1 mg/L. With regard to MIC50 and MIC90 values for linezolid and daptomycin, there were no differences between MRSA isolates with vancomycin MIC <1 mg/L and ≥1 mg/L. However, the GM MIC of teicoplanin and daptomycin were both higher. And data analysis showed that strains with a high vancomycin MIC were significantly more likely to have higher teicoplanin and daptomycin MIC values (≥2 and ≥0.5 mg/L, respectively) than those with vancomycin MIC of <1 mg/L (P = 0.0023, P = 0.0149, respectively).
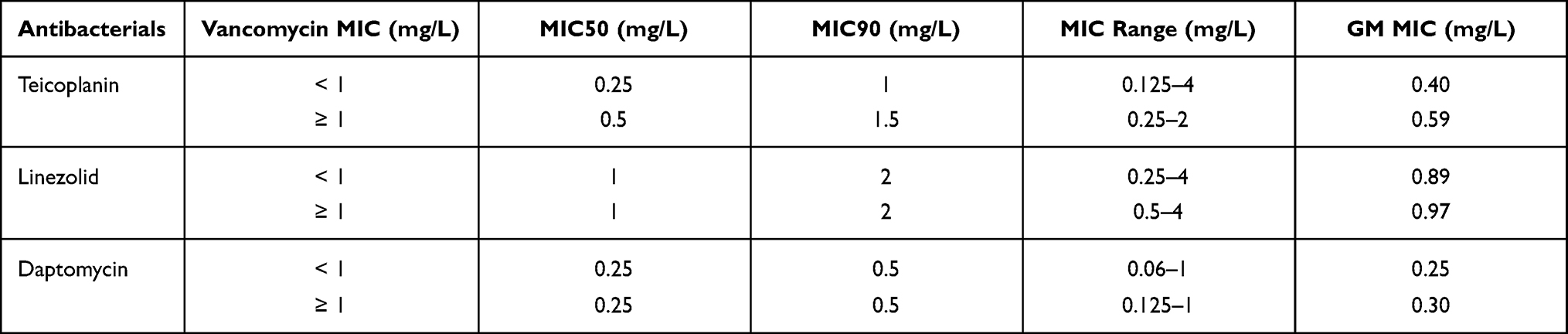 |
Table 4 MIC Values of Teicoplanin, Linezolid and Daptomycin Stratified by MIC Values of Vancomycin |
Discussion
Although the separation rate of MRSA has declined in recent years, MRSA remains a common and devastating pathogen that requires frequent monitoring of its resistance, especially for those antibacterials commonly used for its treatment.19 For this purpose, in this study, we collected 407 MRSA isolates from different parts of China to evaluate the MICs of vancomycin, teicoplanin, linezolid and daptomycin.
For all the MRSA isolates we collected, we did not find any MRSA isolates resistant to these drugs. The MIC values of the drugs in this study was lower compared to other studies in China. A study conducted in one of Shanghai's hospitals, from 2008 to 2018, showed that the vancomycin GM MIC (0.87–1.19 mg/L), MIC50 (1 mg/L), and MIC90 (1.5 mg/L) were all higher than our results, and the same result was observed in teicoplanin.20 One study performed in Chongqing also showed higher vancomycin, teicoplanin, and daptomycin MIC-related parameters compared to this study.21 The emergence of this result may be responsible for the MIC test method we used, or indeed due to the relatively high sensitivity of these MRSA to the four drugs. They measured the MIC using E-test methods. For vancomycin MIC, one study indicated that the MIC measured by the E-test method is higher than the BMD method.22 Both BMD and E-test method are recommended for MIC testing according to the guidelines published by CLSI, however, BMD remains the gold standard for the MIC test.
The sensitivity of MRSA to these drugs in each region was different, such as MRSA isolated from Zhejiang had the lowest GM MIC for each drug, and it also had the lowest daptomycin MIC50 and vancomycin MIC90 compared to other regions. Several studies have demonstrated that increased drug use may be leading to the drug's “MIC creep”.20,23 Whether the difference in MIC values in these regions was related to the different drug usage or the different dominant strains requires further inquiry. The MIC-related parameters of vancomycin, linezolid and daptomycin were similar for the three specimens. However, the teicoplanin GM MIC for sputum isolates were remarkably higher than the blood and pus isolates. This finding differs from one of our previous studies, which indicated that vancomycin has a higher GM MIC in sputum specimens.24
Some researches indicated that higher vancomycin MICs relate to more complicated courses, higher relapse rates and mortality rates in S. aureus infections.24–26 A study demonstrated that, infections with susceptible strains with MICs ≥1 mg/L to be more likely to fail on vancomycin therapy (success rates of 7/42) than those strains with MICs <1 mg/L (success rates of 10/21).27 Therefore, when vancomycin MIC ≥1 mg/L, it is better to use other antimicrobial agents to replace vancomycin for treatment.28,29 To observe MRSA sensitivity to other anti-MRSA drugs when its vancomycin MIC value is relatively high, we performed a stratified analysis between MRSA isolates with vancomycin MIC <1 mg/L and MIC ≥1 mg/L. It was observed that the GM MIC of teicoplanin, linezolid and daptomycin were all higher in vancomycin MIC ≥1 mg/L isolates. This was consistent with the results of another study, that the activities of anti-MRSA antibacterials stratified by vancomycin showed similar trends in MICs of vancomycin with daptomycin and linezolid.30 And we found MRSA strains with a high vancomycin MIC were significantly more likely to have higher teicoplanin and daptomycin MIC values.
Different studies have different definitions of “MIC creep”. A slight but statistically significant increase in percentage of strain MIC reaching the high end of CLSI susceptibility range, or higher MIC50 and MIC90, or shifts in geometric mean MIC can be considered “MIC creep”.31–33 For “MIC creep”, this was a controversial concept, both in China and other countries.16,24,32,34 In this study, vancomycin, teicoplanin and daptomycin GM MIC had declined compared with 2018. Although linezolid GM MIC for 2019 and 2020 were also lower compared with 2018, the MIC50 and MIC90 of 2019 and 2020 isolates were both increased. “MIC creep” was thought to be associated with study periods, drug usage densities and geographic locations.35 Whether the increase of linezolid MIC50 and MIC90 were related to the increased use of linezolid in recent years needs further monitoring. Perhaps these antibacterials indeed had “MIC creep” in some regions, but due to the limited isolates collected in each region, we were unable to analyze the case in individual regions, which is our limitation.
In summary, through our experiments, none of the MRSA strains were found resistant to these four antibacterials. The phenomenon of vancomycin, teicoplanin and daptomycin “MIC creep” was not found from 2018 to 2020 in a wide range of China. Linezolid GM MIC was not increased, but MIC50 and MIC90 of 2019 and 2020 had both increased compared with 2018.
Ethics Statement
This study was approved by the Ethics Committee of Shanghai Pulmonary Hospital, Shanghai Tongji University. The Review Board waived the requirement for informed consent because this retrospective study only focused on bacteria and had no impact on patients.
Acknowledgments
We are grateful to the Department of Clinical Laboratory Medicine, Shanghai Pulmonary Hospital for providing an experimental platform for this study.
Author Contributions
All authors have made a significant contribution to this study, all the way through the conception, study design, execution, acquisition of data, data analysis and interpretation to drafting, revising or critically reviewing stages of the article. The authors also gave final approval of the version to be published, agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Shorr AF. Epidemiology and economic impact of meticillin-resistant Staphylococcus aureus: review and analysis of the literature. Pharmacoeconomics. 2007;25(9):751–768. doi:10.2165/00019053-200725090-00004
2. Barber M. Methicillin-resistant staphylococci. J Clin Pathol. 1961;14(4):385–393. doi:10.1136/jcp.14.4.385
3. Thampi N, Showler A, Burry L, et al. Multicenter study of health care cost of patients admitted to hospital with Staphylococcus aureus bacteremia: impact of length of stay and intensity of care. Am J Infect Control. 2015;43(7):739–744. doi:10.1016/j.ajic.2015.01.031
4. Whitby M, McLaws ML, Berry G. Risk of death from methicillin-resistant Staphylococcus aureus bacteraemia: a meta-analysis. Med J Aust. 2001;175(5):264–267. doi:10.5694/j.1326-5377.2001.tb143562.x
5. Blaskovich MAT, Hansford KA, Butler MS, Jia Z, Mark AE, Cooper MA. Developments in glycopeptide antibiotics. ACS Infect Dis. 2018;4(5):715–735. doi:10.1021/acsinfecdis.7b00258
6. Dong SD, Oberthur M, Losey HC, et al. The structural basis for induction of VanB resistance. J Am Chem Soc. 2002;124(31):9064–9065. doi:10.1021/ja026342h
7. Vellappally S, Divakar D, Al Kheraif A, et al. Occurrence of vancomycin-resistant Staphylococcus aureus in the oral cavity of patients with dental caries. Acta Microbiol Immunol Hung. 2017;64(3):343–351. doi:10.1556/030.64.2017.033
8. Centers for Disease C, Prevention. Update: staphylococcus aureus with reduced susceptibility to vancomycin–United States, 1997. MMWR Morb Mortal Wkly Rep. 1997;46(35):813–815.
9. Centers for Disease C, Prevention. Staphylococcus aureus resistant to vancomycin–United States, 2002. MMWR Morb Mortal Wkly Rep. 2002;51(26):565–567.
10. Wu Q, Sabokroo N, Wang Y, Hashemian M, Karamollahi S, Kouhsari E. Systematic review and meta-analysis of the epidemiology of vancomycin-resistance Staphylococcus aureus isolates. Antimicrob Resist Infect Control. 2021;10(1):101. doi:10.1186/s13756-021-00967-y
11. Shen P, Zhou K, Wang Y, et al. High prevalence of a globally disseminated hypervirulent clone, Staphylococcus aureus CC121, with reduced vancomycin susceptibility in community settings in China. J Antimicrob Chemother. 2019;74(9):2537–2543. doi:10.1093/jac/dkz232
12. Zhu X, Liu C, Gao S, Lu Y, Chen Z, Sun Z. Vancomycin intermediate-resistant Staphylococcus aureus (VISA) isolated from a patient who never received vancomycin treatment. Int J Infect Dis. 2015;33:185–190. doi:10.1016/j.ijid.2014.12.038
13. Sharma M, Riederer K, Chase P, Khatib R. High rate of decreasing daptomycin susceptibility during the treatment of persistent Staphylococcus aureus bacteremia. Eur J Clin Microbiol Infect Dis. 2008;27(6):433–437. doi:10.1007/s10096-007-0455-5
14. Jian J, Chen L, Xie Z, Zhang M. Dissemination of cfr-mediated linezolid resistance among Staphylococcus species isolated from a teaching hospital in Beijing, China. J Int Med Res. 2018;46(9):3884–3889. doi:10.1177/0300060518781636
15. Li S, Zhou Y, Li L, et al. cfrCharacterization of the multi-drug resistance gene in Methicillin-Resistant (MRSA) strains isolated from animals and humans in China. Front Microbiol. 2018;9:2925. doi:10.3389/fmicb.2018.02925
16. Hsieh Y, Lin Y, Huang Y. Vancomycin, teicoplanin, daptomycin, and linezolid MIC creep in methicillin-resistant Staphylococcus aureus is associated with clonality. Medicine. 2016;95(41):e5060. doi:10.1097/MD.0000000000005060
17. Zhuo C, Xu Y, Xiao S, Zhang G, Zhong N. Glycopeptide minimum inhibitory concentration creep among meticillin-resistant Staphylococcus aureus from 2006–2011 in China. Int J Antimicrob Agents. 2013;41(6):578–581. doi:10.1016/j.ijantimicag.2013.02.014
18. Wang L, Zhang M, Guo J, et al. CryptococcusIn vitro activities of the tetrazole VT-1161 compared with itraconazole and fluconazole against and non- species. Mycologia. 2021;29(9):1–8. doi:10.1080/00275514.2021.1913949
19. Diekema D, Pfaller M, Shortridge D, Zervos M, Jones R. Staphylococcus aureusTwenty-year trends in antimicrobial susceptibilities among from the SENTRY Antimicrobial Surveillance Program. Open Forum Infect Dis. 2019;6:S47–S53. doi:10.1093/ofid/ofy270
20. Jian Y, Lv H, Liu J, et al. Staphylococcus aureusDynamic changes of susceptibility to vancomycin, teicoplanin, and linezolid in a central teaching hospital in Shanghai, China, 2008–2018. Front Microbiol. 2020;11:908. doi:10.3389/fmicb.2020.00908
21. Jiang B, Yin S, You B, et al. Staphylococcus aureusA 5-year survey reveals increased susceptibility to glycopeptides for methicillin-resistant isolates from bacteremia patients in a Chinese burn center. Front Microbiol. 2017;8:2531. doi:10.3389/fmicb.2017.02531
22. Phillips C, Wells N, Martinello M, Smith S, Woodman R, Gordon D. Optimizing the detection of methicillin-resistant Staphylococcus aureus with elevated vancomycin minimum inhibitory concentrations within the susceptible range. Infect Drug Resist. 2016;9:87–92. doi:10.2147/IDR.S107961
23. Chang W, Ma X, Gao P, Lv X, Lu H, Chen F. Vancomycin MIC creep in methicillin-resistant Staphylococcus aureus (MRSA) isolates from 2006 to 2010 in a hospital in China. Indian J Med Microbiol. 2015;33(2):262–266. doi:10.4103/0255-0857.148837
24. Lu C, Guo Y, Wang S, et al. Staphylococcus aureusDecreased vancomycin MICs among methicillin-resistant clinical isolates at a Chinese tertiary hospital over a 12-year period. Front Microbiol. 2016;7:1714. doi:10.3389/fmicb.2016.01714
25. Choi E, Huh J, Lim C, et al. Relationship between the MIC of vancomycin and clinical outcome in patients with MRSA nosocomial pneumonia. Intensive Care Med. 2011;37(4):639–647. doi:10.1007/s00134-011-2130-7
26. Miller C, Batra R, Cooper B, et al. An association between bacterial genotype combined with a high-vancomycin minimum inhibitory concentration and risk of endocarditis in methicillin-resistant Staphylococcus aureus bloodstream infection. Clin Infect Dis. 2012;54(5):591–600. doi:10.1093/cid/cir858
27. Sakoulas G, Moise-Broder P, Schentag J, Forrest A, Moellering R, Eliopoulos G. Relationship of MIC and bactericidal activity to efficacy of vancomycin for treatment of methicillin-resistant Staphylococcus aureus bacteremia. J Clin Microbiol. 2004;42(6):2398–2402. doi:10.1128/JCM.42.6.2398-2402.2004
28. Fu X, Lin Z, Chen S, Hong L, Yu X, Wu S. Staphylococcus epidermidisTreatment of intracranial infection caused by methicillin-resistant with linezolid following poor outcome of vancomycin therapy: a case report and literature review. Infect Drug Resist. 2021;14:2533–2542. doi:10.2147/IDR.S319013
29. Maraolo A, Giaccone A, Gentile I, Saracino A, Bavaro D. Daptomycin versus vancomycin for the treatment of methicillin-resistant bloodstream infection with or without Endocarditis: a systematic review and meta-analysis. Antibiotics. 2021;10(8):1014.
30. Cojutti P, Scarparo C, Sartor A, Coato P, Rigoli R, Pea F. A 5-year survey of antimicrobial susceptibility profiles of methicillin-resistant Staphylococcus aureus (MRSA) isolated from patients with bloodstream infections in Northeast Italy. Diagn Microbiol Infect Dis. 2015;81(1):53–56. doi:10.1016/j.diagmicrobio.2014.09.016
31. Yang X, Liu Y, Wang L, et al. Staphylococcus aureusClonal and drug resistance dynamics of methicillin-resistant in pediatric populations in China. Pediatr Invest. 2019;3(2):72–80. doi:10.1002/ped4.12129
32. Arshad F, Saleem S, Jahan S, Tahir R. Staphylococcus aureusAssessment of vancomycin MIC creep phenomenon in methicillin-resistant isolates in a Tertiary care hospital of Lahore. Pak J Med Sci. 2020;36(7):1505–1510. doi:10.12669/pjms.36.7.3273
33. Khurana S, Mathur P, Malhotra R. Staphylococcus aureus at an Indian tertiary hospital: antimicrobial susceptibility and minimum inhibitory concentration (MIC) creep of antimicrobial agents. J Glob Antimicrob Res. 2019;17:98–102. doi:10.1016/j.jgar.2018.10.021
34. Aljohani S, Layqah L, Masuadi E, et al. Occurrence of vancomycin MIC creep in methicillin resistant isolates in Saudi Arabia. J Infect Public Health. 2020;13(10):1576–1579. doi:10.1016/j.jiph.2020.07.008
35. Kehrmann J, Kaase M, Szabados F, et al. Vancomycin MIC creep in MRSA blood culture isolates from Germany: a regional problem? Eur J Clin Microbiol Infect Dis. 2011;30(5):677–683. doi:10.1007/s10096-010-1140-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.