Back to Journals » Infection and Drug Resistance » Volume 12
In Vitro Activity Of Ceftaroline And Comparators Against Staphylococcus aureus Isolates: Results From 6 Years Of The ATLAS Program (2012 To 2017)
Authors Zhang Z, Chen M, Yu Y, Liu B, Liu Y
Received 9 August 2019
Accepted for publication 8 October 2019
Published 24 October 2019 Volume 2019:12 Pages 3349—3358
DOI https://doi.org/10.2147/IDR.S226649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Zhijie Zhang,1 Meng Chen,2 Ying Yu,3 Beini Liu,3 Yong Liu1
1Department of Clinical Laboratory, Shengjing Hospital, Shenyang, People’s Republic of China; 2Department of Rheumatology, Affiliated Hospital of Hebei University, Baoding, People’s Republic of China; 3Medical Affairs Department, Pfizer Investment Co., Ltd, Shanghai, People’s Republic of China
Correspondence: Yong Liu
Department of Clinical Laboratory, Shengjing Hospital, 36 Sanhao Street, Heping District, Shenyang, Liaoning, People’s Republic of China
Tel +86 189 0401 0918
Fax +86 24 96615 72115
Email [email protected]
Background: Ceftaroline is effective against methicillin-resistant Staphylococcus aureus (MRSA), but the resistance patterns still need to be defined. This study aimed to investigate the susceptibility of S. aureus to ceftaroline and comparator antimicrobial agents in patients hospitalized due to infection and to observe the patterns among different regions and over the years.
Methods: The Antimicrobial Testing Leadership And Surveillance (ATLAS) program includes medical centers located in five geographical regions (Europe, Asia-Pacific, South America, Africa-West Asia, and the United States). The isolates were collected from different specimens from patients hospitalized between 2012 and 2017 due to documented complicated skin and soft tissue infection, complicated intra-abdominal infection, complicated urinary tract infection, lower respiratory tract infection, and bloodstream infection.
Results: During the study period, 61,045 isolates were tested, including 35,837 MRSA isolates (58.7%) and 25,208 methicillin-sensitive S. aureus (MSSA) isolates (41.3%). For MRSA, the minimal inhibitory concentration (MIC)50, MIC90, and MIC range of ceftaroline were 0.5, 2, and 0.015–64 μg/mL. The proportion of susceptible MRSA strains was 89.3%. The proportion of resistant MRSA strains was 0.7%. The susceptibility of all S. aureus, MRSA, and MSSA strains to ceftaroline remained relatively constant from 2012 to 2017. The susceptibility to ceftaroline of S. aureus, MRSA, and MSSA strains from the United States, Europe, South America, and Africa/West Asia was high, while the susceptibility of the strains from Asia-Pacific was lower, especially for MRSA.
Conclusion: This study reveals the patterns of ceftaroline susceptibility of MRSA and MSSA around the world and over 6 years.
Keywords: methicillin-resistant Staphylococcus aureus, ceftaroline, antibiotics, resistance, sensitivity
Introduction
The increasing resistance of Staphylococcus aureus to antibiotics is a serious challenge for clinicians. Methicillin-resistant S. aureus (MRSA) is defined as S. aureus with a minimum inhibitory concentration (MIC) to oxacillin of ≥4 µg/mL, as opposed to methicillin-sensitive S. aureus (MSSA), which is sensitive to penicillins and cephalosporins.1 In addition to β-lactam antibiotics, MRSA also shows resistance to macrolides, aminoglycosides, and fluoroquinolones.2 The multidrug resistance often encountered in MRSA strains greatly limits the treatment options.2 An environment with high antibiotic selection pressure (like hospitals) is conducive to the development and propagation of MRSA,2 and the reported incidence of hospital-acquired MRSA ranges from 11.5% to 60%.3–5 MRSA is associated with significant morbidity, mortality, increased length of stay, and higher costs.1 Continuous surveillance of drug resistance helps improve the management of patients with infection and provide guidance for the optimal selection of effective antimicrobial agents.6
Ceftaroline is a fifth-generation broad-spectrum cephalosporin, and it is active against MRSA and Gram-positive bacteria, and, to a lesser extent, against Gram-negative bacteria.7 It is used for community-acquired pneumonia and complicated skin infections.8–11 Against MRSA, it is reported to be non-inferior to vancomycin.12–14
The patterns of ceftaroline resistance against MRSA around the globe still remain to be defined exactly. This study aimed to investigate the susceptibility of S. aureus to ceftaroline and comparator antimicrobial agents in patients hospitalized due to infection and to observe the variation among different regions and years.
Materials And Methods
Bacterial Isolates
The Antimicrobial Testing Leadership And Surveillance (ATLAS) program includes medical centers and microbiological labs located in five geographical regions (Europe, Asia-Pacific, South America, Africa-West Asia, and the United States). The isolates were collected from different specimens from patients who were hospitalized between 2012 and 2017 due to: 1) complicated skin and soft tissue infection; 2) complicated intra-abdominal infection; 3) complicated urinary tract infection; 4) lower respiratory tract infection; 5) bloodstream infection such as sepsis. All isolates were identified by each participating center, stored in tryptic soy broth with glycerol at −70°C, and shipped to International Health Management Associates, Inc. (IHMA; Schaumburg, IL, USA) for susceptibility testing. Only isolates considered to be the potential pathogen of the patient’s infection were included in this study. Only the testing of the first isolate was performed per patient per infectious episode. Ethical approval was not required because the isolates were collected for routine diagnostic testing.
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed by IHMA using the broth microdilution method. MICs were interpreted using both the Clinical and Laboratory Standards Institute (CLSI) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints.15,16 The breakpoint for ceftaroline is ≤1 μg/mL for CLSI and EUCAST. There is no breakpoint for oxacillin in the EUCAST file, leading to blank oxacillin results in the present study. The EUCAST file defined MIC >2 μg/mL as MRSA, which is the same as MIC ≥4 μg/mL in the CLSI file, showing equivalence.
Comparator antimicrobial agents included those representing the most common classes of drugs used for the treatment of S. aureus. Ceftaroline and the following comparator agents were tested: clindamycin, daptomycin, erythromycin, gentamicin, levofloxacin, linezolid, minocycline, moxifloxacin, oxacillin, teicoplanin, tigecycline, trimethoprim-sulfamethoxazole (TMP-SMX), and vancomycin. The S. aureus ATCC 29213 quality control strain was concurrently tested.
Results
Sample Retrieval
A total of 226 centers from five geographical regions (Europe, Asia-Pacific, South America, Africa-West Asia, and the United States) participated in the ATLAS program. The susceptibility testing of gentamicin and TMP-SMX was not performed in 2012 and 2013.
In Vitro Activity Of Ceftaroline Against S. aureus
During the study period, 61,045 isolates were tested, including 35,837 MRSA isolates (58.7%) and 25,208 MSSA isolates (41.3%) (Table 1). For S. aureus, the MIC50, MIC90, and MIC range of ceftaroline were 0.5, 1, and 0.015–64 μg/mL, respectively. According to the CLSI and EUCAST MIC interpretations, the proportions of susceptible strains were both 93.7%, and the proportions of resistant strains were both 0.4%. For MRSA, the MIC50, MIC90, and MIC range of ceftaroline were 0.5, 2, and 0.015–64 μg/mL, respectively. According to the CLSI and EUCAST MIC interpretations, the proportions of susceptible strains were both 89.3%, and the proportions of resistant strains were both 0.7%. For MSSA, the MIC50, MIC90, and MIC range of ceftaroline were 0.25, 0.25, and 0.015–2 μg/mL, respectively. According to the CLSI and EUCAST MIC interpretations, the proportions of susceptible strains were both >99.9%, and the proportions of resistant strains were both 0%.
 |
Table 1 In Vitro Activity Of Ceftaroline Tested Against Isolates Of Staphylococcus aureus |
Susceptibilities Of S. aureus To Ceftaroline And Comparators From 2012 To 2017
The susceptibility of all S. aureus, MRSA, and MSSA strains to ceftaroline were 92.5–95.1%, 86.8–91.8%, and 99.9–100% from 2012 to 2017, respectively (Table 2). In S. aureus, the susceptibility to all 14 tested antibiotics remained stable over time.
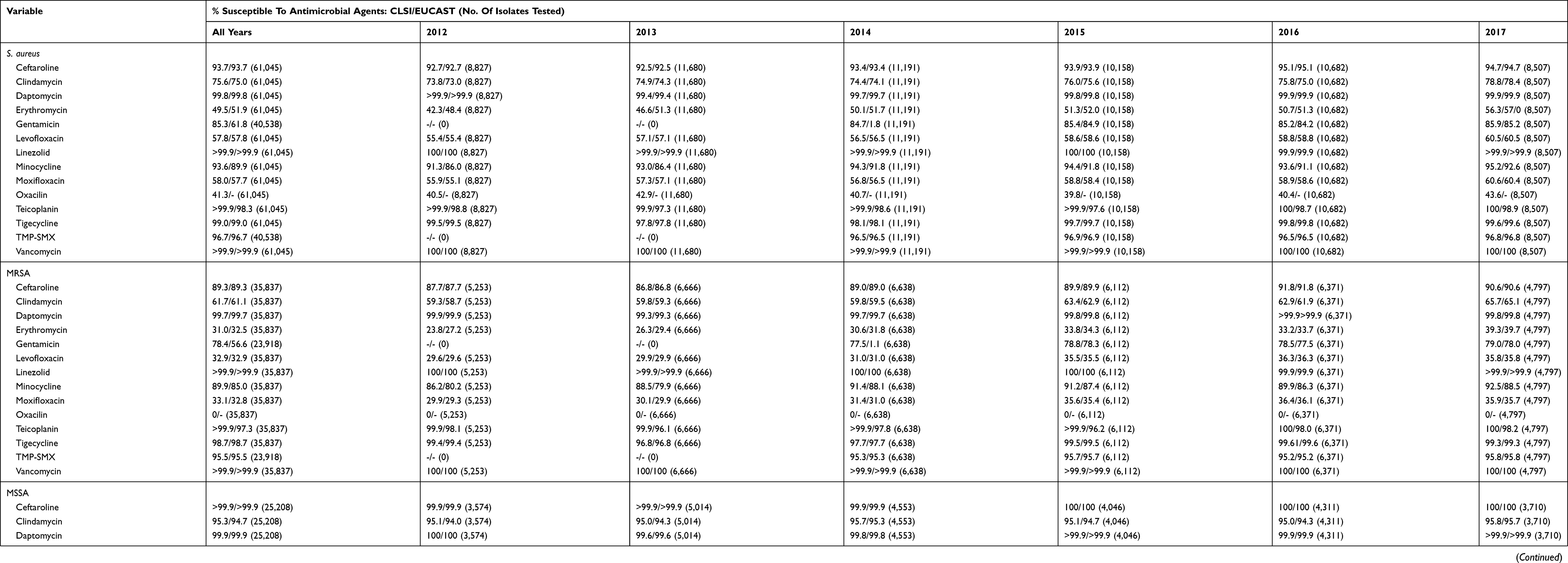 |
Table 2 Susceptibilities Of Staphylococcus aureus To Ceftaroline And Comparators From 2012 To 2017 |
The activities of daptomycin, linezolid, teicoplanin, tigecycline, TMP-SMX, and vancomycin against MRSA remained unchanged over the years. The activities of all other antimicrobial agents against MRSA, except for oxacillin, showed steady improvement during the 6-year period. Vancomycin (>99.9% susceptible), linezolid (>99.9% susceptible), teicoplanin (>99.9% susceptible), daptomycin (99.7% susceptible), tigecycline (98.7% susceptible), and TMP-SMX (95.5% susceptible) were the effective agents (>90% susceptible) against MRSA.
The activities of ceftaroline, clindamycin, daptomycin, gentamicin, linezolid, minocycline, oxacillin, teicoplanin, tigecycline, TMP-SMX, and vancomycin against MSSA were unchanged over the years. The activities of levofloxacin and moxifloxacin against MSSA slightly decreased over the years. Although the activity of erythromycin against MSSA showed steady improvement (69.5% to 78.4% susceptible) during the 6-year period, it was a suboptimal option considering the useful activities of all other antimicrobial agents (>90% susceptible).
Susceptibilities Of S. aureus To Ceftaroline And Comparators In Different Regions
Table 3 shows that the susceptibility to ceftaroline of S. aureus, MRSA, and MSSA strains from the United States (99.7%, 99.5%, and 100%), Europe (96.6%, 94.0%, and >99.9%), South America (91.3%, 84.4%, and 100%), and Africa/West Asia (95.7%, 92.3%, and 100%) was high, while the susceptibility of the strains from Asia-Pacific was markedly lower (85.0%, 75.9%, and 99.9%), especially for MRSA. In other words, the susceptibility of S. aureus and MRSA to ceftaroline was the highest in the United States, followed by Europe, Africa/West Asia, South America, and Asia-Pacific. Regarding MSSA, the susceptibility to ceftaroline was ≥99.9% in all regions of the world.
 |
Table 3 Susceptibilities Of Staphylococcus aureus To Ceftaroline And Comparators In Different Regions |
When examining the susceptibility of MRSA to comparator agents, the susceptibility among the five geographic regions was comparable and remarkable for vancomycin (>99.9–100%), linezolid (>99.9–100%), teicoplanin (99.9–100%), and daptomycin (99.6–99.9%). The activity of tigecycline against MRSA was favorable but relatively low in Asia-Pacific (95.8% susceptible), compared with other regions (99.2–99.9% susceptible). Minocycline and TMP-SMX were effective (>90% susceptible) against MRSA in all regions, except for Asia-Pacific with minocycline (72.4% susceptible) and Africa-West Asia with TMP-SMX (89.5% susceptible). The activities of daptomycin, linezolid, minocycline, oxacillin, teicoplanin, tigecycline, and vancomycin against MSSA showed similar trends with ceftaroline. Levofloxacin and moxifloxacin had relatively poor activity in the United States (86.3% and 86.5% susceptible, respectively), compared with other regions (>90% susceptible). Erythromycin was not an optimal option in any region.
Characteristics Of Ceftaroline-Resistant S. aureus
Table 4 shows the distribution of ceftaroline MICs for isolates of ceftaroline-resistant S. aureus. These isolates were all MRSA. The MIC50, MIC90, and MIC range of ceftaroline were 4, 4, and 4–64 μg/mL, respectively. Table 5 shows the susceptibility/resistance pattern of these strains against the comparators. The susceptibility of ceftaroline-resistant MRSA against clindamycin, erythromycin, gentamicin, levofloxacin, and moxifloxacin was dramatically lower than overall MRSA.
 |
Table 4 Distribution Of Ceftaroline MICs For Isolates Of Ceftaroline-Resistant Staphylococcus aureus |
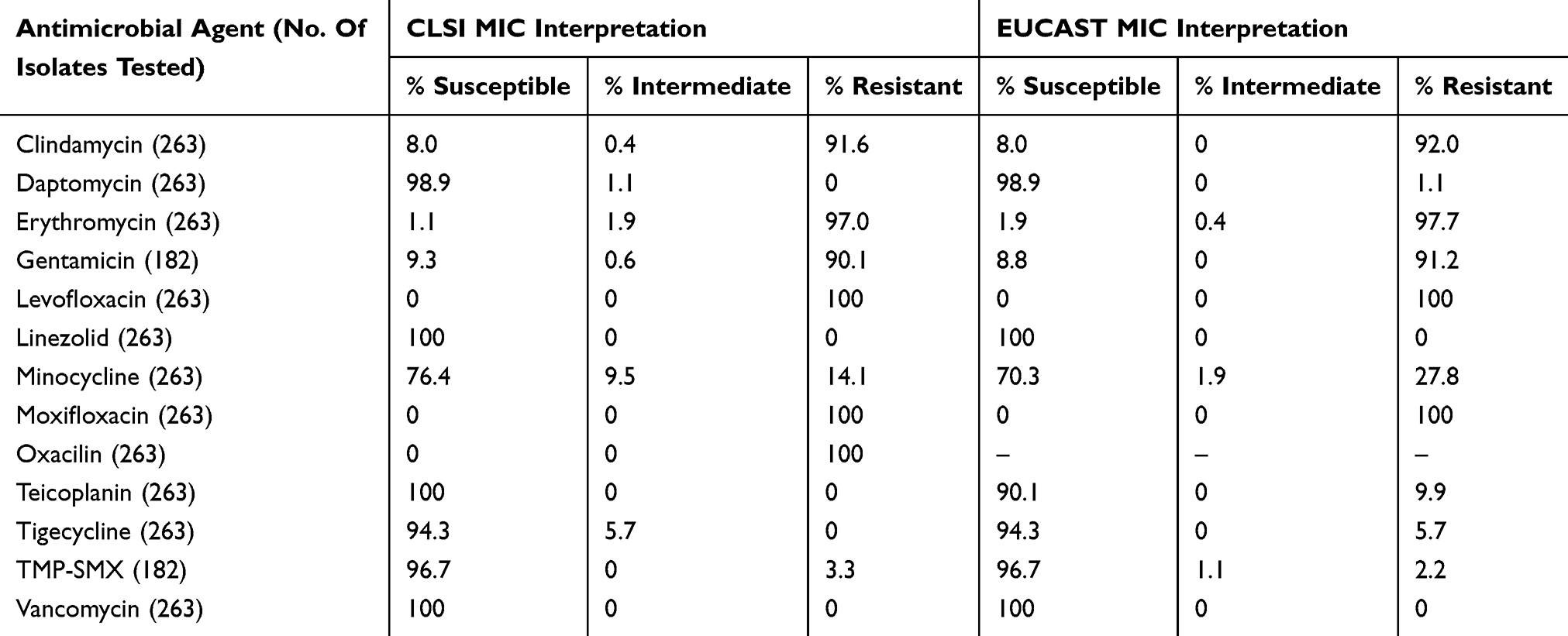 |
Table 5 Susceptibilities Of Ceftaroline-Resistant MRSA To Comparators |
Discussion
There is a plea for worldwide, automated, and comprehensive surveillance of antimicrobial resistance patterns.17 The ATLAS program provides the comprehensive susceptibility profile of ceftaroline and other antimicrobial agents against S. aureus. It involves data from different years and regions of the world and helps provide certain help for global surveillance of bacterial resistance. The ATLAS program also includes other Gram-positive or -negative bacteria, but this study only focused on S. aureus, which is of greater clinical attention to the important threat level of MRSA. The resistance of other pathogenic bacteria will be analyzed in future studies.
During the study period and across the five geographical regions covered by ATLAS, MRSA represented 58.7% of S. aureus isolates. This rate is higher than that of the Tigecycline Evaluation and Surveillance Trial (TEST) (40.2%)18 and TEST study specific to blood-borne infections (33.0%).19 The SENTRY surveillance report for Asia-Pacific and Latin America showed MRSA rates of 37.0% and 44.7%, respectively,20,21 which are lower than in the ATLAS study. These differences might come from the time period covered by the different studies, as well as from the source of patients/samples. In the present study, the frequencies of MRSA across the years were 59.5% in 2012, 57.1% in 2013, 59.3% in 2014, 60.2% in 2015, 59.6% in 2016, and 56.4% in 2017, suggesting a relatively stable frequency during this period.
Previous studies reported that the lowest antibiotic susceptibility of blood-borne infections from S. aureus was to penicillin (around 15%).18,19 A surveillance study from the Antimicrobial Resistance Surveillance Network in Germany reported that the susceptibility of MRSA to linezolid, teicoplanin, tigecycline, and vancomycin was high.22 The SENTRY program indicates that the susceptibility of MRSA to vancomycin remains high around the globe and that newer agents also show good susceptibility profiles.23 The report from the German surveillance network did not examine ceftaroline,22 but the SENTRY program reported that the susceptibility of MSSA to ceftaroline was 100% and that of MRSA was 91.6%.23 For skin and soft tissue infections with suspected MRSA, the guidelines usually recommend oral TMP-SMX, doxycycline, minocycline, and clindamycin, as well as newer agents like linezolid and tedizolid; intravenous vancomycin is the first choice for hospitalized patients, followed by daptomycin when vancomycin cannot be given.1,24–26 For bacteremia of suspected MRSA origin, vancomycin and daptomycin are the first choices, followed by ceftaroline combination regimens and teicoplanin.1,27,28 Ceftaroline is a rapid-acting agent and is a treatment option for S. aureus infection, especially for MRSA.29 The present study showed that both MRSA and MSSA are susceptible to ceftaroline. The present study revealed that the susceptibility of MRSA to ceftaroline was higher than for clindamycin and similar to that of minocycline. On the other hand, susceptibility of MRSA to daptomycin, vancomycin, TMP-SMX, and linezolid was higher than that of ceftaroline. Therefore, daptomycin, vancomycin, TMP-SMX, and linezolid should not be used empirically in the presence of infections in general, but should be kept as empiric therapy for critical cases who cannot afford the time to fail to a first line of therapy, or kept as definitive treatment for patients who fail to other antibiotics. The other antibiotics recommended by the guidelines were not tested in the present study. Regarding MSSA, the susceptibility to the 14 agents studied here was high.
Of note, of the ceftaroline-resistant strains (263/61,045, 0.4%), most (242/263, 92.0%) were from Asia, including Thailand (168 strains), China (35 strains), and Korea (35 strains). As ceftaroline was not approved in these countries between 2012 and 2017, we consider that these ceftaroline-resistant strains were naturally circulant strains. These isolates were all MRSA. The results also show that the susceptibility/resistance pattern of these ceftaroline-resistant MRSA strains was different than that of overall MRSA. The susceptibility of ceftaroline-resistant MRSA against clindamycin, erythromycin, gentamicin, levofloxacin, and moxifloxacin was dramatically lower than overall MRSA.
The results showed that the resistance of MRSA to ceftaroline, clindamycin, gentamicin, and minocycline in the Asia-Pacific region was much higher than in the rest of the world. A report from the World Health Organization highlighted that antibiotic resistance has increased all over the world, but that the increase was particularly alarming in Asia because of antibiotic over-prescription, poor infection control, poor waste management, overuse of antibiotics in farming, food security, and restricted access to the newest antibiotics,30 as supported by a number of studies.31,32 Asia-Pacific is the most populous region of the world, but many of its countries are among the poorest per capita, leading to poor health infrastructure.33 The rates of resistance of S. aureus to oxacillin (82.1%), ciprofloxacin (78.2%), clindamycin (64.2%), erythromycin (76.5%), and tetracycline (70.9%) are high in Asian countries.34 MRSA significantly affects the outcomes of Asian patients with S. aureus infection.35 The TEST study showed that Africa and Asia were the two regions of the world with the highest occurrence of S. aureus resistant to multiple antibiotics among blood-borne infections.19
A surveillance study from the Antimicrobial Resistance Surveillance Network in Germany reported that the resistance pattern for tobramycin, ciprofloxacin, moxifloxacin, clindamycin, erythromycin, tetracyclines, and gentamicin evolved from 2010 to 2015.22 In the present study, when considering all five regions together, the susceptibility to ceftaroline showed a rising tendency from 2012 to 2017, while the susceptibility to daptomycin, linezolid, teicoplanin, tigecycline, TMP-SMX, and vancomycin remained stable.
Conclusions
The present study examined the susceptibility of S. aureus to ceftaroline and comparator antimicrobial agents in patients hospitalized due to infection. For MRSA, the MIC50, MIC90, and MIC range of ceftaroline were higher than for MSSA. The susceptibility of S. aureus, MRSA, and MSSA strains to ceftaroline from the United States, Europe, South America, and Africa/West Asia is high, while the susceptibility of the strains from Asia-Pacific is markedly lower, especially for MRSA.
Ethics Approval And Informed Consent
Ethical approval was not required because the isolates were collected for routine diagnostic testing.
Abbreviations
methicillin-resistant Staphylococcus aureus (MRSA), Antimicrobial Testing Leadership And Surveillance (ATLAS), methicillin-sensitive S. aureus (MSSA), minimum inhibitory concentration (MIC), International Health Management Associates (IHMA), European Committee on Antimicrobial Susceptibility Testing (EUCAST), trimethoprim-sulfamethoxazole (TMP-SMX), Tigecycline Evaluation and Surveillance Trial (TEST), Clinical and Laboratory Standards Institute (CLSI).
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors contributed to conception and design, acquisition and analysis of data; drafting and critically revising the paper; final approval of the version to be published; and agreement to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siddiqui AH, Koirala J. Methicillin Resistant Staphylococcus Aureus (MRSA). Treasure Island (FL): StatPearls; 2019.
2. Lee AS, de Lencastre H, Garau J, et al. Methicillin-resistant Staphylococcus aureus. Nat Rev Dis Primers. 2018;4:18033. doi:10.1038/nrdp.2018.33
3. Tracy LA, Furuno JP, Harris AD, Singer M, Langenberg P, Roghmann MC. Staphylococcus aureus infections in US veterans, Maryland, USA, 1999-2008. Emerg Infect Dis. 2011;17(3):441–448. doi:10.3201/eid1703.100502
4. Lakhundi S, Zhang K. Methicillin-resistant Staphylococcus aureus: molecular characterization, evolution, and epidemiology. Clin Microbiol Rev. 2018;31(4):e00020–18.
5. Miao J, Wang W, Xu W, et al. The fingerprint mapping and genotyping systems application on methicillin-resistant Staphylococcus aureus. Microb Pathog. 2018;125:246–251. doi:10.1016/j.micpath.2018.09.031
6. Chipolombwe J, Torok ME, Mbelle N, Nyasulu P. Methicillin-resistant Staphylococcus aureus multiple sites surveillance: a systemic review of the literature. Infect Drug Resist. 2016;9:35–42. doi:10.2147/IDR.S95372
7. Duplessis C, Crum-Cianflone NF. Ceftaroline: a new cephalosporin with activity against methicillin-resistant Staphylococcus aureus (MRSA). Clin Med Rev Ther. 2011;3:a2466.
8. El Hajj MS, Turgeon RD, Wilby KJ. Ceftaroline fosamil for community-acquired pneumonia and skin and skin structure infections: a systematic review. Int J Clin Pharm. 2017;39(1):26–32. doi:10.1007/s11096-016-0417-z
9. Pawluk SA, Wilby KJ. Ceftaroline fosamil for community-acquired pneumonia. Lancet Infect Dis. 2015;15(9):999. doi:10.1016/S1473-3099(15)00139-5
10. Carreno JJ, Lodise TP. Ceftaroline fosamil for the treatment of community-acquired pneumonia: from FOCUS to CAPTURE. Infect Dis Ther. 2014;3(2):123–132. doi:10.1007/s40121-014-0036-8
11. Mpenge MA, MacGowan AP. Ceftaroline in the management of complicated skin and soft tissue infections and community acquired pneumonia. Ther Clin Risk Manag. 2015;11:565–579. doi:10.2147/TCRM.S75412
12. Dryden M, Zhang Y, Wilson D, Iaconis JP, Gonzalez J. A Phase III, randomized, controlled, non-inferiority trial of ceftaroline fosamil 600 mg every 8 h versus vancomycin plus aztreonam in patients with complicated skin and soft tissue infection with systemic inflammatory response or underlying comorbidities. J Antimicrob Chemother. 2016;71(12):3575–3584. doi:10.1093/jac/dkw333
13. Friedland HD, O’Neal T, Biek D, et al. CANVAS 1 and 2: analysis of clinical response at day 3 in two phase 3 trials of ceftaroline fosamil versus vancomycin plus aztreonam in treatment of acute bacterial skin and skin structure infections. Antimicrob Agents Chemother. 2012;56(5):2231–2236. doi:10.1128/AAC.05738-11
14. Corey GR, Wilcox M, Talbot GH, et al. Integrated analysis of CANVAS 1 and 2: phase 3, multicenter, randomized, double-blind studies to evaluate the safety and efficacy of ceftaroline versus vancomycin plus aztreonam in complicated skin and skin-structure infection. Clin Infect Dis. 2010;51(6):641–650. doi:10.1086/655827
15. Clinical and Laboratory Standards Institute(CLSI). Performance Standards for Antimicrobial Susceptibility Testing: 29thed. CLSI Document M100-S29. Wayne, PA.CLSI; 2019.
16. The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 9.0. 2019. Available from: http://www.eucast.org.
17. O’Brien TF, Clark A, Peters R, Stelling J. Why surveillance of antimicrobial resistance needs to be automated and comprehensive. J Glob Antimicrob Resist. 2019;17:8–15. doi:10.1016/j.jgar.2018.10.011
18. Hoban DJ, Reinert RR, Bouchillon SK, Dowzicky MJ. Global in vitro activity of tigecycline and comparator agents: Tigecycline Evaluation and Surveillance Trial 2004-2013. Ann Clin Microbiol Antimicrob. 2015;14:27. doi:10.1186/s12941-015-0113-1
19. Zhang Z, Chen M, Yu Y, Pan S, Liu Y. Antimicrobial susceptibility among gram-positive and gram-negative blood-borne pathogens collected between 2012-2016 as part of the Tigecycline Evaluation and Surveillance Trial. Antimicrob Resist Infect Control. 2018;7:152. doi:10.1186/s13756-018-0441-y
20. Mendes RE, Mendoza M, Banga Singh KK, et al. Regional resistance surveillance program results for 12 Asia-Pacific nations (2011). Antimicrob Agents Chemother. 2013;57(11):5721–5726. doi:10.1128/AAC.01121-13
21. Sader HS, Castanheira M, Farrell DJ, Flamm RK, Mendes RE, Jones RN. Tigecycline antimicrobial activity tested against clinical bacteria from Latin American medical centres: results from SENTRY Antimicrobial Surveillance Program (2011-2014). Int J Antimicrob Agents. 2016;48(2):144–150. doi:10.1016/j.ijantimicag.2016.04.021
22. Walter J, Noll I, Feig M, et al. Decline in the proportion of methicillin resistance among Staphylococcus aureus isolates from non-invasive samples and in outpatient settings, and changes in the co-resistance profiles: an analysis of data collected within the Antimicrobial Resistance Surveillance Network, Germany 2010 to 2015. BMC Infect Dis. 2017;17(1):169. doi:10.1186/s12879-017-2757-2
23. Diekema DJ, Pfaller MA, Shortridge D, Zervos M, Jones RN. Twenty-year trends in antimicrobial susceptibilities among staphylococcus aureus from the SENTRY antimicrobial surveillance program. Open Forum Infecti Dis. 2019;6(Suppl 1):S47–S53. doi:10.1093/ofid/ofy270
24. Kavanagh KT, Abusalem S, Calderon LE. View point: gaps in the current guidelines for the prevention of Methicillin-resistant Staphylococcus aureus surgical site infections. Antimicrob Resist Infect Control. 2018;7:112. doi:10.1186/s13756-018-0407-0
25. Lewis PO, Heil EL, Covert KL, Cluck DB. Treatment strategies for persistent methicillin-resistant Staphylococcus aureus bacteraemia. J Clin Pharm Ther. 2018;43(5):614–625. doi:10.1111/jcpt.12743
26. Eisenschenk M. A concern with the clinical consensus guidelines on meticillin-resistant staphylococci. Vet Dermatol. 2018;29(2):174. doi:10.1111/vde.2018.29.issue-2
27. Sirijatuphat R, Sripanidkulchai K, Boonyasiri A, et al. Implementation of global antimicrobial resistance surveillance system (GLASS) in patients with bacteremia. PLoS One. 2018;13(1):e0190132. doi:10.1371/journal.pone.0190132
28. Remschmidt C, Schneider S, Meyer E, Schroeren-Boersch B, Gastmeier P, Schwab F. Surveillance of antibiotic use and resistance in intensive care units (SARI). Dtsch Arztebl Int. 2017;114(50):858–865. doi:10.3238/arztebl.2017.0858
29. Saravolatz LD, Stein GE, Johnson LB. Ceftaroline: a novel cephalosporin with activity against methicillin-resistant Staphylococcus aureus. Clin Infect Dis. 2011;52(9):1156–1163. doi:10.1093/cid/cir147
30. World Health Organization. Antimicrobial Resistance in the Asia Pacific Region: A Development Agenda. Geneva: World Health Organization; 2017.
31. Kakkar M, Chatterjee P, Chauhan AS, et al. Antimicrobial resistance in South East Asia: time to ask the right questions. Glob Health Action. 2018;11(1):1483637. doi:10.1080/16549716.2018.1483637
32. Chereau F, Opatowski L, Tourdjman M, Vong S. Risk assessment for antibiotic resistance in South East Asia. Bmj. 2017;358:j3393. doi:10.1136/bmj.j3393
33. Jean SS, Hsueh PR. High burden of antimicrobial resistance in Asia. Int J Antimicrob Agents. 2011;37(4):291–295. doi:10.1016/j.ijantimicag.2011.01.009
34. Chung DR, Song JH, Kim SH, et al. High prevalence of multidrug-resistant nonfermenters in hospital-acquired pneumonia in Asia. Am J Respir Crit Care Med. 2011;184(12):1409–1417. doi:10.1164/rccm.201102-0349OC
35. Kang CI, Song JH, Chung DR, et al. Clinical impact of methicillin resistance on outcome of patients with Staphylococcus aureus infection: a stratified analysis according to underlying diseases and sites of infection in a large prospective cohort. J Infect. 2010;61(4):299–306. doi:10.1016/j.jinf.2010.07.011
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.