Back to Journals » Advances in Medical Education and Practice » Volume 17
Improving Representation and Knowledge of Dermatological Conditions in Skin of Colour in Undergraduate Dermatology Teaching: An Educational Intervention
Authors Gore A, Satchwell F, Barfei M, Burden-Teh E
Received 6 February 2026
Accepted for publication 24 April 2026
Published 13 May 2026 Volume 2026:17 596942
DOI https://doi.org/10.2147/AMEP.S596942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Alice Gore,1 Francesca Satchwell,1,2 Maryam Barfei,1 Esther Burden-Teh1,2
1Department of Dermatology NHS Treatment Centre, Nottingham University Hospitals NHS Trust, Nottingham, UK; 2Centre of Evidence Based Dermatology School of Medicine, University of Nottingham, Nottingham, UK
Correspondence: Alice Gore, Email [email protected]
Background: Nottingham University medical students undergo a two-week rotation in dermatology which incorporates teaching sessions, including didactic lecture presentations, tutorial seminars on skin cancers and acute dermatological conditions and patient simulations. Many studies highlight the need to improve skin of colour teaching in medical school curricula globally, as low representation can negatively affect physician knowledge throughout their career.
Methods: Using a pre-post intervention study design, Nottingham University Hospitals NHS Trust (NUH) teaching materials were adapted by adding clinical images of dermatological conditions in skin of colour to existing teaching sessions (obtained from DermNetNZ). Four new learning objectives were set relating to skin of colour in four common skin conditions in the curriculum: acne, eczema, psoriasis and skin cancer. Teaching materials were added to cover this content, and knowledge acquisition was assessed before and after the dermatology rotation using a pre/post-attachment questionnaire. Data were analysed using descriptive analysis.
Results: Ninety-nine medical students completed pre- and post-dermatology attachment questionnaires. Students’ confidence in recognising skin conditions in patients with skin of colour improved, with 71% reporting confidence ≤ 5/10 pre-attachment and 74.7% reporting confidence > 5/10 post-attachment. The post-attachment questionnaire showed that 97% of students identified increased risk of post-inflammatory hyperpigmentation and scarring in acne in skin of colour, 94.9% recognised psoriatic plaques differed in darker skin tones, 100% recognised erythema can be challenging to identify in eczema of darker skin tones, and 97% identified that melanoma is diagnosed later and is associated with poorer survival in patients with skin of colour.
Conclusion: Adaptations to the NUH dermatology teaching materials demonstrate the feasibility and educational benefits of incorporating skin of colour content into existing undergraduate dermatology teaching. Data collection is ongoing to increase sample size and assess inclusivity. Results are preliminary and may be limited by methods used to assess knowledge gain and confidence.
Keywords: dermatology, inclusivity, skin of colour, medical education, medical students
Introduction
Healthcare professionals often see patients with skin conditions, with studies showing that 36% of patients presenting to general practice have at least one skin problem.1 Beyond localised healthcare services, the high prevalence of skin disease also extends globally and is currently the fourth-biggest cause of illness-related disability internationally.2 This indicates that skin disease is a significant contributor to disability worldwide. Furthermore, this burden of skin disease on healthcare services is increasing globally due to modifiable factors, such as smoking, alcohol and sun exposure increasing the incidence of dermatological disease.3 This emphasises the need for healthcare professionals to be confident in the management of dermatological conditions. Moreover, the large diversity of the general population,4 including skin type and ethnicity, results in a wider variety of skin tones that require examination and treatment. The skin can be graded into six different types, according to the Fitzpatrick scale,5 which was historically created to describe an individual’s response to phototherapy, referencing their capability to burn or tan in relation to ultraviolet exposure. The large variety of skin types and tones can affect the clinical presentation of skin conditions, with “typical” skin disease features presenting differently depending on skin tone.6 This highlights the need for healthcare professionals to have good awareness and knowledge of the presentation of skin disease in Skin of Colour (SoC). A lack of knowledge of how skin diseases may present in different skin tones could lead to misdiagnosis and delayed treatment of conditions.
Despite the high volume of skin disease encountered by healthcare professionals, there remains a lack of dermatology teaching within the medical school curricula.7 Currently, medical schools typically offer a dermatology placement lasting a maximum of 2 weeks,8 providing little time for students to fully understand the fundamentals of skin disease. This could contribute to doctors feeling inadequately trained to treat skin disease.8 Studies have found that general practitioners (GPs) feel that they lack sufficient training or education in the skills required to identify and diagnose specific skin lesions.9
In addition, there is a notable lack of representation and diversity in the resources used to deliver the dermatology curriculum in medical schools.10 This was recognised as a global issue by an expert panel of consultant dermatologists representing six different countries.11 Through literature search using the key word “skin of colour”, they highlighted the disproportionate representation of this population within medical textbooks.11 Photographs used to teach students how to recognise skin diseases are rarely of darker skin tones, with very common skin conditions (eg. acne vulgaris) often depicted on lighter skin.12 On average, approximately only four percent of images from medical and anatomy textbooks have dark skin tones.10 This immediately limits medical students’ exposure to skin conditions in SoC and their varied presentation. Inadequate education can result in disparities in patient management based on their skin tone.13 Students have a lower diagnostic accuracy for patients with non-white skin tones, proving how the current teaching materials are negatively impacting overall knowledge.14 Consequently, this leads to future doctors’ knowledge and confidence in this area being impacted.
Lack of awareness of skin disease in patients with SoC could lead to higher rates of morbidity and mortality in these patients. Poor recognition of disease can lead to misdiagnosis,15 creating an inequality within healthcare. Evidence has shown that SoC patients with hidradenitis suppurativa are more likely to see a dermatologist 5 years after the first presentation, in contrast to patients with white skin where it takes approximately 3 years to seek specialist treatment after initial presentation.15 The diagnostic challenges are further highlighted by the fact that skin conditions in darker skin tones are also more likely to appear brown/black, as well as having textural changes compared to lighter skin tones.16 This creates a huge disparity in the quality of healthcare that different patients receive, caused by a lack of understanding and education of diversity in patient presentation.
If these issues relating to students and doctors’ knowledge of skin diseases in SoC are not addressed, the problem is only likely to be exacerbated in the future. Medical educators have identified that for an adequate change to occur this issue must be addressed from a training level,17 for example by tackling the current lack of diversity within medical school curricula. Improving dermatology medical school teaching to be more inclusive of skin of colour has the potential to improve clinical accuracy of future doctors. Adequate teaching and training in this underrepresented area will more likely improve future patient outcomes, hopefully reducing this disparity currently shown in our healthcare system.
Dermatologists and medical educators are recognising the current gaps in medical education and has resulted in recommendations for increasing the diversity of teaching materials from specialists.18 Yet despite this awareness, the underlying problem remains largely unaddressed. This requires action and change from the undergraduate medical education level to determine the effects of change on future doctors. This potential gap in the dermatology medical school curricula at the University of Nottingham (UoN) and dermatology clinical placement at the Nottingham University Hospitals (NUH) NHS Trust was identified, with the previous dermatology teaching materials showing gaps for improving inclusivity in representing skin disease in SoC.
This teaching improvement project investigates whether adapting existing teaching materials and introducing skin of colour-specific learning objectives improves medical student knowledge and confidence of skin disease in patients with skin of colour. It is anticipated that students who are taught about skin disease with more inclusive teaching materials will have better knowledge and confidence compared to their pre-study levels. Students at the UoN medical school undertake a two-week dermatology clinical placement during their third or fourth year of study. Informal feedback from current students and clinical teaching fellow doctors highlighted the need for more inclusivity and diversity within the current dermatology teaching materials. However, the question remains as to how best to implement changes within the teaching materials, and their effectiveness in improving students’ knowledge.
Previous studies have attempted to improve inclusivity within medical school dermatology teaching materials, including introducing additional one-off seminars which have shown to improve student confidence in recognising conditions in skin of colour.19 However, these interventions have often required additional time, extra resources and have not been integrated into existing teaching materials. Despite the growing number of studies highlighting the underrepresentation of SoC in dermatology teaching materials,20 the current literature lacks research on minimal-resource, targeted teaching material adjustments, such as SoC-specific teaching materials and learning objectives, on students’ confidence and understanding. This highlights the need for minimal resource teaching material-integrated strategies that can be included within current dermatology placements for students.
This teaching improvement project therefore seeks to adapt existing teaching materials to be more inclusive of SoC and assess the overall impact on student knowledge and confidence, aiming to provide guidance for future teaching material development.
Methods
This teaching improvement project was conducted on 99 medical students at UoN during their two-week dermatology clinical attachment between March and September 2025. This study used a prospective, non-randomised, pre-post intervention study design. No control group was included as all medical students received teaching from the adapted teaching materials to ensure equitable learning experiences. Thus, an absolute causal relationship could not be identified, and evaluation was limited to pre- and post-attachment changes. Medical students involved were either in their third or fourth year, depending on where their dermatology placement occurred within their clinical placement rotation. Participation in the teaching improvement project was voluntary for medical students. Before this educational intervention, dermatology resources in the UoN dermatology teaching programme primarily featured lighter skin tones, with minimal representation of darker skin tones and skin conditions in SoC.
Four new specific learning objectives were added to the teaching material which focused on enhancing awareness and understanding of how the following skin conditions present in patients with SoC: eczema, psoriasis, acne and malignant melanoma. The learning objectives were as follows:
- Identify that there is a higher risk of hyperpigmentation and scarring in acne in people with SoC.21
- Recognise that psoriatic plaques can present differently in darker skin tones: including a lack of obvious erythema and plaques may be purplish, reddish, white or greyish colour.22,23
- Recognise that erythema can be more challenging to identify in patients with eczema and darker skin tones.24
- Identify that malignant melanoma is diagnosed at more advanced stages and associated with worse survival rates among individuals with SoC.25,26
These objectives were highlighted to students particularly in placement inductions and session objectives. Acne, psoriasis and eczema were chosen due to their high incidence in primary care and dermatology clinics,27 and their notable difference in presentation in SoC patients. Furthermore, melanoma was chosen due to the high burden skin cancers pose on healthcare services,28 and due to its typical late-stage presentation in patients with SoC.25,26 These skin conditions are also consistent with the existing teaching curriculum and GMC’s “Outcomes for Graduates”.29
Existing dermatology teaching materials were adapted to be more inclusive of SoC by adding images of different skin tones throughout existing teaching materials. Clinical images incorporated were obtained from DermNetNZ, ensuring that a diverse range of skin tones were included. DermNetNZ was chosen as an image source as they were high-quality images, non-identifiable with a declaration of patient consent obtained.
The adapted two dermatology teaching programme included a two-hour induction session, two two-hour interactive tutorials with lectures and case-based discussions and a four-hour expert patient simulation activity. The two-hour induction session focused on history taking and rash/lesion description terminology and introduced a total of nine new images of skin disease in SoC. The first interactive tutorial focused on skin cancer diagnosis and breaking bad news and incorporated three new images of skin disease in SoC. The second interactive tutorial focused on acute dermatology and emergencies and introduced two new images of skin disease in SoC. The expert patient session involved real-life patient actors and students taking a history and examining the patient. Peer and teacher feedback was applied using the Pendleton model. A PowerPoint was then used to teach each condition an expert patient presented and included nine new images of SoC, with at least one new image per condition. Patient cases in the expert patient session included malignant melanoma, psoriasis, urticaria, acne vulgaris and scabies. Overall, a total of 23 SoC images were added across all teaching sessions. Clinical images of the following conditions in SoC were included: malignant melanoma, psoriasis, eczema, acne, urticaria and scabies. The four skin conditions in the new learning objectives were the focus and highlighted due to their common presentation within clinical practice and curriculum, however the additional skin conditions stated were included to provide broader clinical context. Verbal teaching delivery alongside the adapted teaching materials was tailored to highlight awareness of the different conditions in skin of colour. All students received the same teaching materials and observed the same updated patient images. Outside of these structured sessions, which included the adapted teaching materials, students were assigned to regular dermatology hospital clinics in a variety of sub-specialties.
The effectiveness of the adapted teaching materials was assessed using a pre- and post-dermatology placement online questionnaire accessed via a QR code. This aimed to evaluate changes in students’ knowledge and confidence in SoC patients. All responses received were anonymous. The pre-attachment questionnaire focused on assessing students’ confidence and included one single question asking students to rate their ability in recognising skin disease in SoC using a Likert scale (0 being low confidence and 10 being high confidence). The post-attachment questionnaire focused on assessing students’ confidence and knowledge and included five questions, one question assessing confidence and four questions assessing knowledge. The first question assessed confidence and asked students to re-rate their ability to recognise skin disease in SoC post-attachment using the same Likert scale as the pre-attachment questionnaire. A single best answer (SBA) multiple-choice question format was used to assess student knowledge, with each of the four questions covering a different condition highlighted in the learning objectives. These specific questions are shown in Figure 1.
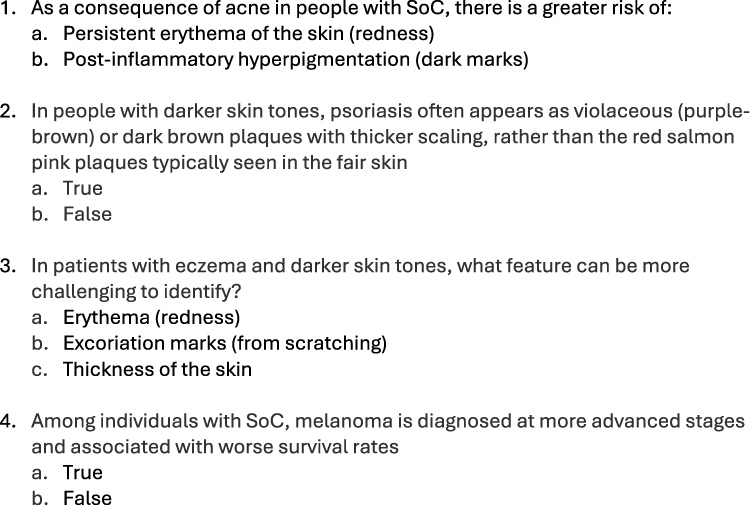 |
Figure 1 Single best answer (SBA) questions used in post-attachment questionnaire to evaluate knowledge of skin conditions in SoC. |
Confidence levels were assessed in this teaching improvement project as they can portray how capable students feel in a certain medical subject area. Studies have shown that confidence can affect a person’s engagement in medical tasks and their willingness to make decisions in a clinical environment.30 Thus, confidence levels could show the change pre- and post-attachment in students’ perceived ability to recognise conditions and manage patients who have skin disease in SoC. Furthermore, a Likert scale was chosen to enable numerical data to be gathered, enabling easy comparison pre- and post-attachment. Four SBA questions were included to directly assess each of the four newly introduced learning objectives. Each SBA question aligned with one learning objective, ensuring the question assessed exactly what was intended for students to learn. This also allowed results to be recorded per objective and made it easy to assess which specific learning objectives were achieved.
Data was analysed by comparing student answers from the pre- and post-attachment questionnaires. Confidence ratings pre- and post-attachment were interpreted by calculating the percentage of each score given by students, and the percentage change in students reporting confidence of >5 etc. Post-attachment student knowledge was analysed by calculating the percentage of students who were able to correctly answer questions about that specific skin disease in SoC. Microsoft Excel was used to gather the data, and descriptive statistics were used only in this project. There was deemed not to be scope for inferential statistics in this study due to small cohort size (n=99) and lack of control group, thus it would not be informative or appropriate. In addition, the exploratory nature of this teaching improvement meant descriptive analytics were useful in presenting initial findings when evaluating the intervention. Furthermore, this study was designed to assess initial feasibility and educational benefit of this intervention rather than a formal hypothesis. Thus, descriptive analysis was considered most informative in reporting results and advising future more detailed evaluation.
Results
A total of 99 responses were received from the pre- and post-dermatology attachment questionnaires throughout the period of March–September 2025. One hundred percent of students who completed the pre-attachment questionnaire also completed the post-attachment questionnaire (n=99).
Initially, the majority of students reported low confidence in recognising skin conditions in patients with SoC, with 71.7% rating their confidence at 5 out of 10 or lower in the pre-attachment questionnaire (see Figure 2). Post-attachment questionnaires revealed an improvement in student confidence, with 74.7% rating their confidence above 5 out of 10 post-attachment (see Figure 3).
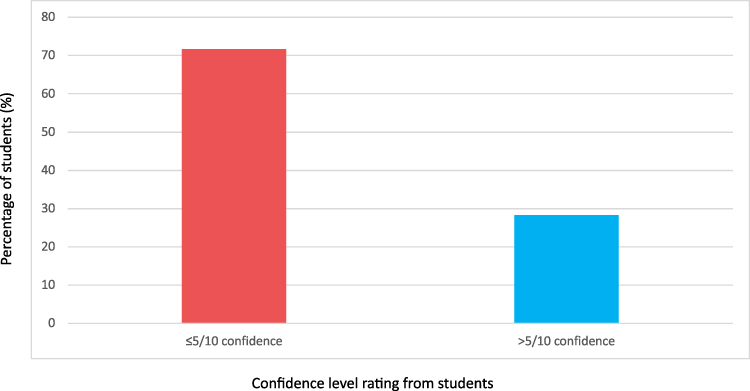 |
Figure 2 A bar graph showing students’ self-reported confidence levels in recognising skin conditions in SoC pre-attachment. |
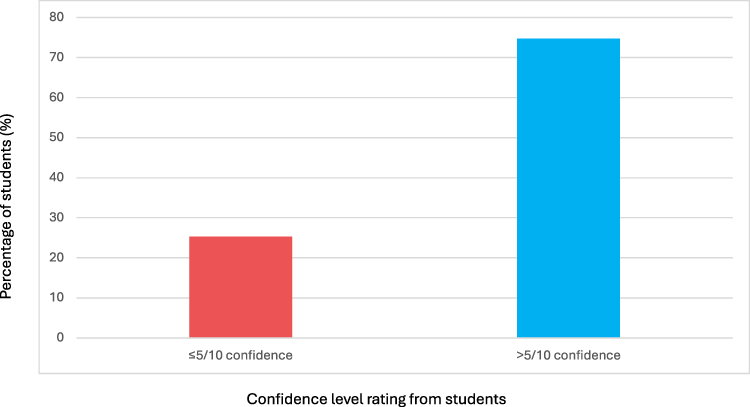 |
Figure 3 A bar graph showing students’ self-reported confidence levels in recognising skin conditions in SoC post-attachment. |
In the post-attachment multiple-choice questions, 97% of students were able to identify the increased risk of post-inflammatory hyperpigmentation and scarring in acne in SoC. Additionally, 94.9% of students were able to correctly recognise that psoriatic plaques could present differently in darker skin tones. Furthermore, 100% of students were able to recognise that erythema can be more challenging to identify in eczema of darker skin tones. Finally, 97% of the students could correctly identify that malignant melanoma is diagnosed at more advanced stages and associated with worse survival rates among individuals with SoC.
Discussion
This teaching improvement project aimed to adapt existing teaching materials to enhance student knowledge of skin disease in SoC, introduce dedicated learning objectives, and evaluate the impact the adaptations have on students’ overall confidence and knowledge in patients with SoC. The project’s findings offer insight into the strength of this specific educational intervention in enhancing diversity and inclusivity within dermatology teaching materials.
The increase in confidence level reported by students after undertaking the adapted dermatology teaching materials shows that these changes were beneficial in equipping students to identify skin disease in patients with SoC. Although reported confidence levels do not directly correlate with the accuracy of diagnosis, they are a contributing factor to students’ general willingness and competency to manage patients with different skin tones. Most students were able to correctly answer the multiple-choice questions presented to them to assess their knowledge of skin conditions in patients with SoC, with no less than 94% being able to accurately select the correct answer for each question. The high accuracy level across all four skin diseases potentially demonstrates effective learning of the updated teaching materials, especially considering it was a short clinical placement in which the students undertook. Improved knowledge across these four common skin conditions is key in students having a good awareness of skin disease in SoC as they are all very common yet often underrepresented in patients with different skin tones.
Previous studies have highlighted the lack of diversity and inclusion of SoC within dermatology curricula,10 resulting in a disparity in the healthcare received by patients depending on their skin tone. The initial low confidence reported by students in this project (71.7% of students rating 5/10 or lower) emphasises how SoC is underrepresented within medical education. The results of this educational intervention are supported by previous studies, which also demonstrate that targeted educational interventions can improve students’ confidence in recognising skin conditions in SoC.12,19,31 Related studies introducing an additional one-off skin-type diversity seminars or cross-sectional improvement projects demonstrated increased competence and confidence in knowledge of disease in skin of colour, aligning with the findings of this project.30,31
Whilst previous studies have assessed standalone educational interventions, this project evaluates an embedded teaching material change without increasing teaching time. Unlike one-off sessions, our project was fully integrated within existing teaching materials to ensure adequate exposure throughout clinical placements. In comparison to earlier research, which shows the potential for improved SoC teaching, this project demonstrates how this can be established within existing medical school teaching materials. What makes this teaching enhancement project novel is the feasibility of integrating inclusive SoC content into existing materials without extending teaching hours, whilst also improving students’ knowledge and confidence. The study has contributed to current literature by evaluating a low-cost and easy-access approach to improving diversity within dermatology teaching, which could improve clinical competence of future doctors treating a diverse population. The approaches used in this project could offer broader applicability across UK medical school curricula, and provides a practical, scalable and low-resource model to which medical schools could improve inclusivity within their teaching resources. Most importantly, this project was created as a pilot with the aim to call for more studies and integration of inclusive study material throughout UK medical schools.
The main strength of this project was the educational intervention’s integration into the current medical school teaching materials – making it more reflective of how the changes could work practically in the curriculum and likely promoting student engagement. Another strength is that the use of DermNetNZ provided the opportunity to use images from real-life patients. This allowed the students to properly visualise presentation of skin disease in a variety of skin tones, as they may appear in clinical practice. The project was further strengthened by using four key conditions in the learning objectives. Students are more likely to encounter these skin diseases in clinical practice, and this project has increased their knowledge of diagnosis and management of them. The use of pre- and post-attachment questionnaires enabled a comparison to be formed of confidence levels during this attachment. The different questions used allowed for both student knowledge and confidence to be assessed, enabling a wide range of modalities to be evaluated.
By improving teaching material inclusivity and diversity, this project has also potentially had a broader impact by preparing students to treat and manage more diverse populations in their future medical careers. This will inevitably hopefully improve the disparity in healthcare patients receive depending on their skin type.6 The improved confidence and knowledge seen could potentially translate to better clinical practice for patients with SoC in the future. Repeated exposure of skin disease in SoC means medical students are more likely to accurately diagnose, overall improving patient safety. By addressing this issue at a training level, it is hoped that the next generation of doctors will be more experienced in treating a variety of skin types and will have improved clinical competence in this area. Thus, there is potential for a longer-term educational outcome by improving diagnostic accuracy for a larger variety of patients. Overall, this could potentially contribute to addressing the issue of physicians lacking exposure to skin disease in SoC. Furthermore, this project will hopefully encourage students to be more inclusive in their diagnostic reasoning, a skill which is a useful habit to develop early on in a clinical career and can be applied to a wide variety of specialities.14 This will positively impact medical students’ diagnostic accuracy amongst a diverse population in real-life clinical scenarios when they eventually qualify as doctors in the future.
The project was limited by its relatively small sample size (n=99), with a larger sample size more likely to capture a wider variety of knowledge among medical students. Furthermore, because this project did not include a control group, it is difficult to determine whether the improvements seen in student knowledge and confidence were directly caused by the educational intervention itself, or if they might have resulted from other factors such as prior experience. Additionally, the absence of inferential statistics means it is not possible to evaluate that the changes seen post-attachment was due to the adapted teaching materials alone. Therefore, no causal relationship can be identified. The use of confidence ratings enabled students to self-report their assumed confidence post-attachment, however it is not an accurate measure of diagnostic certainty and performance in clinical settings. Confidence ratings could be subjective between different students which further makes it difficult to assess the true impact the adapted teaching materials had on the students’ learning and self-perceived ability. Additionally, students may potentially overestimate their perceived ability which does not correlate with their clinical practice. The small number of SBA questions used in the post-attachment questionnaire means it is difficult to fully assess knowledge retention post-attachment. SBA questions are short and may limit the assessment of students’ deeper clinical reasoning as if in real hospital settings. Having a larger number and variety of questions tested would have enabled more understanding into the overall student knowledge gained in this study. Although self-reported confidence levels and SBA questions present good initial analysis, they do not offer full insight into students’ ability to clinically reason and accurately diagnose patients. Thus, these results need to be interpreted with caution when evaluating the full impact this teaching enhancement project had on knowledge and confidence. Furthermore, this project measured the short-term outcome of acquired student knowledge, rather than long-term retention. This means it is difficult to assess the true impact this teaching improvement project would have had on long-term learning, therefore also the impact it would have when these students are working as clinical doctors in the future.
Future work could involve assessing clinical knowledge retained in this study through different types of exams, such as a clinical OSCE environment. This would evaluate students’ diagnostic competence and whether the new teaching materials have benefited their clinical skills. Other directions for further research could involve piloting increased inclusivity within teaching materials across a wider variety of specialities, including working towards making changes throughout the entire medical curriculum to ensure that all students are mandated to learn this. This would promote an improvement in the management of diverse patients across the entire healthcare system, and not just within dermatology. Additionally, this project could be replicated at other universities to improve diversity of teaching materials on a national scale. A wider variety of clinical images used would also further enhance diversity by including more skin conditions in different skin types (eg. hidradenitis suppurativa, lupus and scabies).
Conclusion
Overall, this project demonstrated the feasibility and educational benefits of incorporating inclusive skin of colour content in to existing undergraduate dermatology teaching. Adaptations to the NUH dermatology teaching materials have potentially improved students’ awareness of skin conditions in patients with SoC and increased their confidence in recognition. Although these findings have offered good initial insight, it is noted that findings should be carefully considered within context. This is due to the limitations of the study surrounding subjectivity of self-reported confidence and the modest SBA knowledge testing. Inclusive teaching materials are essential if future doctors are going to be able to treat and manage an increasingly diverse population. This has the potential to reduce inequalities in healthcare and improve clinical competence in the treatment of a large variety of patients. Further work is ongoing to increase the sample size of this project and assess the true long-term impact of this intervention on inclusivity within medical student teaching and healthcare.
Abbreviations
SoC, skin of colour; NUH, Nottingham University Hospital; UoN, University of Nottingham; GP, general practitioner; SBA, single best answer; OSCE, objective structured clinical examination; MCQ, multiple choice questionnaire; NHS, National Health Service; GMC, General Medical Council.
Data Sharing Statement
All data sets can be made available from the corresponding author on request. The online questionnaire used can also be shared on request.
Ethics Approval and Consent to Participate
This project was supervised by Dr. Burden-Teh, a clinical associate professor and consultant dermatologist from the Centre of Evidence-Based Dermatology, School of Medicine, University of Nottingham, UK. Participation in this project was voluntary, and no identifiable data was collected.
Ethical approval was not required for this study as it involved non-interventional educational research using voluntary anonymous questionnaires and did not involve patients or the use of identifiable personal data. This was confirmed by local institutional guidance. The study was conducted in accordance with the principles of the Declaration of Helsinki. All participants gave informed consent before participation. Inferred consent was taken with completion of the questionnaire.
Consent for Publication
This is not applicable as no identifiable data is gathered. DermNetN images using state patient consent were obtained.
Acknowledgments
The authors would like to thank the students at the University of Nottingham for their participation in this project. We thank the NUH Dermatology Department and clinical teaching fellows for enabling the adapted teaching materials. We thank DermNetNZ for providing open access, patient-consented images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project received no external funding.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Le Roux E, Edwards PJ, Sanderson E, Barnes RK, Ridd MJ. The content and conduct of GP consultations for dermatology problems: a cross-sectional study. British J General Prac. 2020;70(699):e723–10. doi:10.3399/bjgp20X712577
2. Karimkhani C, Dellavalle P, Coffeng E, et al. Global skin disease morbidity and mortality: an update from the global burden of disease study 2013. JAMA Dermatol. 2017;153(5):406–412. PMID: 28249066;PMCID: PMC5817488. doi:10.1001/jamadermatol.2016.5538
3. Williams HC. Epidemiology of skin disease. In: Williams HC, Langan SM editors. Reducing the Global Burden of Skin Disease. Wiley-Blackwell;2016:Chapter RTD0005. doi:10.1002/9781118441213.rtd0005
4. Catney G. The changing geographies of ethnic diversity in England and Wales, 1991–2011. Popul Space Place. 2016;22(8):750–765. doi:10.1002/psp.1954
5. Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124(6):869–871. doi:10.1001/archderm.1988.01670060015008
6. Hutchison E, Yoseph R, Wainman H. Skin of colour: essentials for the non-dermatologist. Clin Med. 2023;23(1):2–8. doi:10.7861/clinmed.2022-0335
7. Hansra NK, O’Sullivan P, Chen CL, Berger TG. Medical school dermatology curriculum: are we adequately preparing primary care physicians? J Am Acad Dermatol. 2009;61(1):23–29.e1. doi:10.1016/j.jaad.2008.11.912
8. Sharma M, Murphy R, Doody GA. DT01: barriers to and facilitators of implementation of the dermatology curriculum across UK medical schools: results of a national survey and recommendations. Br J Dermatol. 2021;185(Suppl 1):157. doi:10.1111/bjd.20154
9. Fee JA, McGrady FP, Hart ND. Dermoscopy use in primary care: a qualitative study with general practitioners. BMC Prim Care. 2022;23(1):47. doi:10.1186/s12875-022-01653-7
10. Louie P, Wilkes R. Representations of race and skin tone in medical textbook imagery. Soc Sci Med. 2018;202:38–42. doi:10.1016/j.socscimed.2018.02.023
11. Lim HW, Zhang C, Taylor M, et al. International expert consensus on knowledge gaps in care for dermatologic disorders in skin of color. Int J Dermatol. 2026;65(1):41–56. doi:10.1111/ijd.70101
12. Adelekun A, Onyekaba G, Lipoff JB. Skin color in dermatology textbooks: an updated evaluation and analysis. J Am Acad Dermatol. 2021;84(1):194–196. doi:10.1016/j.jaad.2020.04.084
13. Buster KJ, Stevens EI, Elmets CA. Dermatologic health disparities. Dermatol Clin. 2012;30(1):53–59,viii. doi:10.1016/j.det.2011.08.002
14. Dodd RV, Rafi D, Stackhouse AA, et al. The impact of patient skin colour on diagnostic ability and confidence of medical students. Adv Health Sci Educ. 2023;28(4):1171–1189. doi:10.1007/s10459-022-10196-6
15. Serrano L, Ulschmid C, Szabo A, Roth G, Sokumbi O. Racial disparities of delay in diagnosis and dermatologic care for hidradenitis suppurativa. J Natl Med Assoc. 2022;114(6):613–616. doi:10.1016/j.jnma.2022.08.002
16. Barzallo DA, Ofori-Darko AA, Perez AM, DiSano K. Diversifying skin tone representation in medical school dermatology curriculum. Med Sci Educ. 2024;35(1):37. doi:10.1007/s40670-024-02159-w
17. Kaundinya T, Kundu RV. Diversity of skin images in medical texts: recommendations for student advocacy in medical education. J Med Educ Curric Dev. 2021;8:23821205211025855. doi:10.1177/23821205211025855
18. Perlman KL, Williams NM, Egbeto IA, et al. Skin of color lacks representation in medical student resources: a cross-sectional study. Int J Women’s Dermatol. 2021;7(2):195–196. doi:10.1016/j.ijwd.2020.12.018
19. Abeck F, Heinen I, Sommer R, et al. Effects of a skin type diversity seminar on undergraduate medical students’ self-assessed competence in managing skin diseases in patients with skin of color. BMC Med Educ. 2024;24(1):848. doi:10.1186/s12909-024-05828-x
20. Creamer K, Javadzadeh S, Ferguson L, Pinder V, Jiyad Z. Is skin of colour appropriately represented in undergraduate resources for dermatological conditions covered in the new national medical licensing assessment? Br J Dermatol. 2022;187(S1):175. doi:10.1111/bjd.21477
21. Perkins AC, Cheng CE, Hillebrand GG, Miyamoto K, Kimball AB. Comparison of the epidemiology of acne vulgaris among Caucasian, Asian, Continental Indian and African American women. J Eur Acad Dermatol Venereol. 2011;25(9):1054–1060. doi:10.1111/j.1468-3083.2010.03919.x
22. Khanna R, Khanna R, Desai SR. Diagnosing psoriasis in skin of color patients. Dermatol Clin. 2023;41(3):431–434. doi:10.1016/j.det.2023.02.002
23. Lytvyn Y, Sachdeva M, Mufti A, Yeung J. Dermatology: how to manage psoriasis and recognize differences in pathophysiology and presentation in patients with skin of colour. Drugs in Context. 2022;11:2021–2029. doi:10.7573/dic.2021-9-3
24. Gan C, Mahil S, Pink A, Rodrigues M. Atopic dermatitis in skin of colour. Part 2: considerations in clinical presentation and treatment options. Clin Exp Dermatol. 2023;48(10):1091–1101. doi:10.1093/ced/llad162
25. Brunsgaard EK, Wu YP, Grossman D. Melanoma in skin of color: part I. Epidemiology and clinical presentation. J Am Acad Dermatol. 2023;89(3):445–456. doi:10.1016/j.jaad.2022.04.056
26. Brunsgaard EK, Jensen J, Grossman D. Melanoma in skin of color: part II. Racial disparities, role of UV, and interventions for earlier detection. J Am Acad Dermatol. 2023;89(3):459–468. doi:10.1016/j.jaad.2022.04.057
27. Richard MA, Paul C, Nijsten T, et al. EADV burden of skin diseases project team. Prevalence of most common skin diseases in Europe: a population-based study. J Eur Acad Dermatol Venereol. 2022;36(7):1088–1096. doi:10.1111/jdv.18050
28. Arnold M, Singh D, Laversanne M, et al. Global burden of cutaneous melanoma in 2020 and projections to 2040. JAMA Dermatol. 2022;158(5):495–503. doi:10.1001/jamadermatol.2022.0160
29. General Medical Council. Outcomes for graduates. London: GMC; 2020. Available from: https://www.gmc-uk.org/education/standards-guidance-and-curricula/standards-and-outcomes/outcomes-for-graduates.
30. Fry M, MacGregor C. Confidence and impact on clinical decision-making and behaviour in the emergency department. Australas Emerg Nurs J. 2014;17(3):
31. Peterknecht E, Reid E, Cheung K, Rajasekaran A. Improving recognition among undergraduate and postgraduate trainees of dermatological conditions in skin of colour: a cross-sectional quality improvement project. Clin Exp Dermatol. 2022;47(12):2261–2264. doi:10.1111/ced.15374
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Faculty and Students’ Perceptions About Online Teaching Styles of Faculty in Large Group Lectures
Malay J, Kassab SE, Merghani TH, Rathan R, Sreejith A
Advances in Medical Education and Practice 2022, 13:1261-1266
Published Date: 6 October 2022
Impact of a Preclinical Medical Student Anesthesiology Elective on the Attitudes and Perceptions of Medical Students Regarding Anesthesiology
Walsh KL, Yadav A, Cradeur M, Huang H, Lee D, Owusu-Dapaah H, Ji C, Kendall MC, Asher S
Advances in Medical Education and Practice 2023, 14:1347-1355
Published Date: 29 November 2023
What Matters Most: Determinants Associated with the Selection of Medical Residencies in Qatar
Kane T, Ford J, Al Saady RM, Vranic S, Musa OAH, Suliman S
Advances in Medical Education and Practice 2024, 15:141-151
Published Date: 28 February 2024
Crafting Tomorrow’s Medical Leaders: Insights from Medical Students and Interns in Saudi Arabia
Albednah FA, Albishri SB, Alnader RY, Alwazzan L
Journal of Healthcare Leadership 2024, 16:141-156
Published Date: 13 March 2024
Integrating Psychological Care Training in Trauma Care for Medical Students: the Need and the Strategies
Shrivastava SR, Shrivastava PS, Joshi A
Advances in Medical Education and Practice 2024, 15:447-450
Published Date: 27 May 2024