Back to Journals » Patient Preference and Adherence » Volume 15
Improving Quality of Service Among Antiretroviral Therapy Users Through Strategic Problem-Solving Approach at Bure Primary Hospital, Northwest Ethiopia
Authors Yeshiwas Y, Debie A ![]() , Worku N
, Worku N ![]() , Yazachew L
, Yazachew L ![]()
Received 13 March 2021
Accepted for publication 24 June 2021
Published 5 July 2021 Volume 2021:15 Pages 1497—1504
DOI https://doi.org/10.2147/PPA.S310945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Yirga Yeshiwas,1 Ayal Debie,2 Nigusu Worku,2 Lake Yazachew2
1Bure Primary Hospital, Amhara National Regional State, Bure, Ethiopia; 2Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Lake Yazachew
University of Gondar, PO Box: 196, Gondar, Ethiopia
Tel +251-918084747
Email [email protected]
Background: Globally, an estimated 1.7 million new human immunodeficiency virus (HIV) infections occurred in 2018. Although significant progress has been made still, it remained a public health threat. Thus, this capstone project aimed to improve the quality of services among anti-retroviral therapy (ART) users through a strategic problem-solving approach at Bure Primary Hospital, northwest Ethiopia, 2020.
Methods: A before–after study design was employed among 357 people living with HIV (PLWH) clients on ART from December 2019 to January 2020 and from April to May 2020 pre and post capstone project. The capstone project involved regular internal mentorship, availing supplies, and providing refresher training. Data were entered using EPI data version 3.1 and exported to SPSS version 23 statistical for analysis. Paired t-test was used for comparing the mean scores before and after the capstone project. A mean score with 95% CI and a P-value < 0.05 were used to determine the effect of the capstone project on the quality of the service.
Results: The overall quality of ART service was improved as evidenced by the presence of a positive gap score (+0.0164) according to the SERVQAUL model. Receiving first CD4 count was improved from 65% to 85.1% and screening for TB from 90% to 97% with 95% CI at a p-value of 0.001. Whereas, viral load measurement at six months is 78% to 89.75% and IPT uptake is 62% to 71% with 95% CI at a p-value of 0.013 and 0.004, respectively.
Conclusion: Ensuring regular internal mentorship, availing supplies, and providing refresher training have a significant effect on the quality of ART service. Therefore, adhering to national guidelines and fulfilling the availability of the recommended infrastructures helps to improve the quality of ART service.
Keywords: ART, service quality, Ethiopia
Introduction
The human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) is one of the most destructive epidemics and a major threat to the world population.1 It is a devastating disease that affects almost 37.9 million persons globally, and an estimated 1.7 million new HIV infections occur in 20182,3 In Ethiopia, the presence of the disease was recognized in the early 1980s, with the first two AIDS cases reported in 1986 and has rapidly spread throughout the country. However, anti-retroviral therapy has dramatically reduced the rates of morbidity and mortality.4,5
Quality improvement covers the actual activities conducted in facilities to close observed service gaps client perceptions of service quality result from comparing their before-service expectations with their actual service experience.6–8 The Health Sector Transformation in Quality (HSTQ) guideline incorporated HIV as one of the prioritized communicable diseases and planned to have a standard of practice for HIV care on the quality of the HIV prevention, care and treatment services.9 The provision of quality health services is essential to maintain health, prevent disease, and minimize morbidity and mortality, ensuring a prosperous nation.
Despite remarkable achievements in health infrastructure expansion, increments in volume, and a mix of trained and deployed human resources for health in Ethiopia, steady access to quality health care across the various levels of the healthcare delivery system are observed.10 Although the care for individuals with HIV/AIDS has advanced greatly in the last decade, the struggle to consistently deliver high-quality care to each patient still exists for many providers across the country.11
Although significant progress has been made towards ending AIDS as a public health threat, many gaps in service access and quality remain, poor quality of antiretroviral therapy (ART) service can lead to poor adherence, which increases the risk of HIV-related morbidity and mortality.12–14
A cross-sectional study conducted in the United States showed that the quality of ART service was a major problem.15 In the past decades, tremendous improvements have occurred in measuring and monitoring the quality of medical care in the United States. Despite these achievements and the Joint United Nations Programme on HIV/AIDS (UNAIDS) endeavor to combat HIV, serious HIV/AIDS service quality issues exist.16,17 In a similar study, just 34% of PLWHIV in South Africa had their viral load tested.18 In Tanzania showed that early initiation of ART treatment was 53%, enrolling in CPT was 69%, receiving IPT was 46%.19 In Ethiopia, studies showed that low CD4 count and body mass index, as well as poor adherence for ART treatment, predicts virological failure.20–22
Even though, preventive activities that enhance the quality of HIV care for PLWHIV are international strategies which are complemented by national guidelines, evidence shows that early initiation of ART and enrolling to Isoniazid preventive therapy was a challenge.23 Though IPT is recommended to PLWHA for TB prevention on the package, compliance of patients with IPT is expectedly a practical challenge on implementation.24–27
The Mortality of people living with HIV/AIDS has declined at the national level. However still, there is a gap in the quality of ART service provided to ART users. Therefore, this pre-post interventional study is important to identify root causes for that compromised quality of ART service among ART users and to take an appropriate intervention timely.
At Bure Primary Hospital, ART clients chart review findings show that the overall performance or quality of clinical care provided to clients on ART at Bure Primary Hospital is not in line with the recommendation of national ART treatment guidelines. Hence applying a strategic problem-solving approach to improve the quality of ART service provided to clients in Bure Primary Hospital was important in improving ART service outcomes.
After a thorough discussion and verification, root causes were identified for poor ART service at Bure Primary Hospital. The root causes were irregularity of internal mentorship, stock out of supplies and lack of refreshment training. Thus, launching regular internal mentorship, availing supplies and provide ART refresher training for ART unit health-care providers were the selected strategies to address the root causes. They were implemented to quantify their outcome on ART service quality:
Even though the mortality of people living with HIV/AIDS has declined at the national level, there is still a gap in ART service quality provided to ART users. Therefore, this pre-post ART service quality improving capstone project is important to identify root causes for that compromised quality of ART service among ART users and to take any appropriate measure timely.
Methods
Study Design and Settings
Bure Primary Hospital provides highly active anti-retroviral therapy (HAART) for people living with HIV/AIDS (PLWHA) since 2017. Since then, there were 415 ever enrolled in ART at Bure Primary Hospital. Currently, there were 357 clients on ART, of which 346 and 11 were adults and paediatrics, respectively. The study was conducted from December 2019 to May 2020 (the baseline data was collected from December 1 to 30, 2019. The capstone project was implemented from January to March, and after the capstone project, data were collected from April to May 2020)
Nature of the Capstone Project
A capstone project is a comprehensive endeavour designed to help investigators address difficult problems. The goal of capstone projects is to inspire investigators and tackle difficult issues. Therefore, on December 12, 2019, a multi-disciplinary team was organized to improve the quality of services among ART users. The team includes clinical nurses, laboratory, pharmacy, medical doctors, and all department heads. All the team members were involved in searching for the root causes and developing strategies. A strategic problem-solving approach was used to define the problem, set an objective, conduct a root cause analysis (using fishbone), generate alternative methods, compare strategies, select a strategy, implement the system, and evaluate its impact on the problem.28
The team defined the problem as poor ART service quality and set objectives to increase service quality indicators score from the current state to the national target within seven months after implementing the capstone project. Next, the team spent five months conducting a root cause analysis, designing the best intervention, and implementing the selected strategies. People-related factors, process, policy-related factors, equipment, and supply-related factors were analyzed in the root cause analysis. Finally, based on the identified root causes, the team proposed all possible strategies.
To prioritize strategies, criteria were used, such as the cost, impact, time to implement, and the strategy’s feasibility. Score 5 for the ideal strategy and score 1 for the least ideal strategy. Finally, rank was given based on the total score out of 20 for each strategy. Accordingly, providing training on ART for health-care workers in the ART unit, launching regular mentorship schedules, and availing necessary materials and supplies for ART service provision. Then, the team deployed the plan, do, study, and act (PDSA) cycle to determine whether a change leads to an improvement or not,29 which focuses on planning it, trying it, observing the results, and acting on what is learned.
Strategies and Activities
Introducing regular internal mentorship, availing supplies and medical devices, and providing ART refresher training for ART unit health-care providers were the selected strategies. A three-day ART training was given for clinicians working at the ART unit. The training was given by two general practitioners trained on ART. Preparing training materials from the national ART service guideline, invite trainers, book training hall, selecting training participants was done in advance. The other activities were, availing CD4 cartilage, supplies like co-trimoxazole, isoniazid, HIV test kit, preparing mentorship checklist.
Population and Sampling Procedures
All PLWHA clients who were ever enrolled in ART care at Bure Primary Hospital were the source population. In contrast, all PLWHA clients, who were currently on follow-up for anti-retroviral therapy at Bure Primary Hospital were considered the study population. All PLWHA clients who were currently on follow-up for anti-retroviral therapy and unable to communicate were excluded from the study.
The sample size was determined by using a single population proportion formula: n =z2 (1-p)/d2, Where n= the required sample size, Z = standardized normal distribution value at the 95% CI, which is 1.96, P=50%, d = the margin of error, taken as 5%, substituting the value, in the formula, = 1.962* (0.5) (0.5) 0.052 =384. Even though the required sample size was 384, the number of ART clients currently on ART in Bure primary hospital was 357. Therefore, all 357 PLWHA who were on ART were included in the sample size. Data was collected two times, ie, pre and post-intervention. Two data collectors were BSc nurses in their profession and trained in basic ART training but not working at ART clinic at the time of the data collection period.
Variables and Measurement
SERVQUAL is a multidimensional research instrument designed to measure service quality. The SERVQUAL captures respondents’ expectations and perceptions along the five dimensions of service quality. The five dimensions are tangible, reliability, responsiveness, assurance and empathy comparing four, five, four, four and five items, respectively.29,30 According to SERVQUAL Model, service quality is calculated as the perception score minus the expectation score (Q = P-E). Thus, a positive gap score signifies the good quality of ART service, and negative gap scores show that service quality is perceived as poor.32 Hence average gap scores of each SERVQAL dimension and the overall quality of ART service were computed as follows:
Tangibility (TA) – the appearance of physical facilities, equipment, and personnel of the hospital.30,31 Average gap score for tangible items = (TA1+TA2+TA3+TA4)/4. Reliability (RL) – the ability to perform the promised service dependably and accurately.30,31 Average gap score for reliability items = (RL1+RL2+RL3+RL4+RL5)/5. Responsiveness (RN) – the willingness of employees to help customers and to provide prompt service.30,31 Average gaps score for responsiveness items = (RN1+RN2+RN3+RN4)/4. Assurance (AS) – the knowledge and courtesy of employees and their ability to convey trust and confidence for the client.30,31 Average gaps score for assurance items = (AS1+AS2+AS3+AS4)/4. Empathy (EM) – the provision of caring, individualized attention to customers.31 Average gap score for empathy items = (EM1+EM2+EM3+EM4+EM5)/5. OSQ – Overall service quality = (TA+RL+RN+AS+EM)/5.
Good adherence: if the adherent status of ARV clients is≥95%. That is, the percentage of missed dose is <2 doses of 30 doses or <3 doses of 60 doses according to ART national treatment guidelines. Viral load suppression: when the viral load of clients is <1000 copies/mL or when the viral RNA is undetectable by the test. Good ART service quality: the presence of positive gap scores when perception score minus expectation score. Poor ART service quality: the presence of negative gap scores when perception score minus expectation score.
Data Collection Tools and Procedures
A structured interview administered the questionnaire, and data extraction checklists were used. ART users’ charts and documents of registration book review were done to identify the service provided. Besides this, an exit interview of ART users using SERVQUAL quality measurement questionnaires was conducted to measure respondents’ expectation and perception of the quality of ART service. Previous studies confirmed the reliability and validity of the questionnaire.32 The principal investigator had provided one-day training for data collectors and supervisors on how to collect data. The principal investigator and the supervisor evaluated the completeness of the collected data daily. To minimize data entry error, the collected data were entered using Epi data.
Data Processing and Analysis
Data were cleaned, coded, and entered using EPI data version 3.1 and exported to SPSS version 23 statistical for analysis. The data were analyzed using descriptive statistics, and the results were presented using textual narration, tables. Paired t-test was used for comparing the mean score indicators before and after the capstone project. To determine statistical significance, a 95% confidence level or p-value <0.05 was used.
Results
Socio-Demographic Characteristics
A total of 357 ART users took part in the study before the capstone project with a response rate of 100% whereas, 350 ART user took part in the study after the capstone project with a response rate of 98%. The mean age of the study participants was 39.61 years ± (11.73 SD). More than half of the respondents, 186 (53.1%), were females, and 134 (38.2%) were aged from 30 to 39 years. About 203 (58%) participants were rural residents (Table 1).
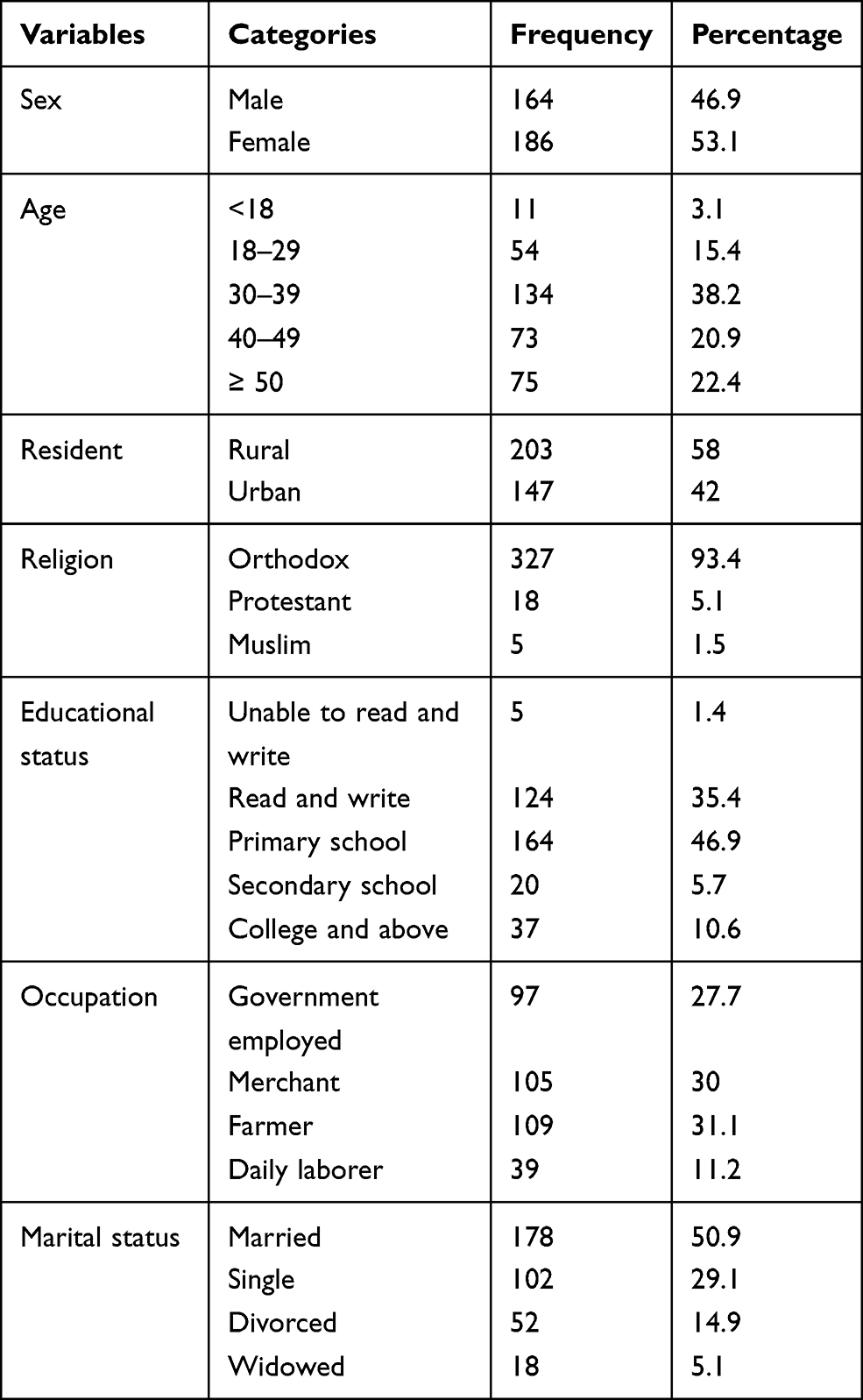 |
Table 1 Socio-Demographic Characteristics of Study Participants in Bure Primary Hospital, 2020 |
Overall Compliance of HIV Clinical Care Practice Based on Selected Indicators
The overall clinical care practice among users was 67% in the before capstone project and 83.37% after the capstone project. Receiving first CD4 count was improved from 65% to 85.1% (20.1% pre-post difference with 95% CI and at a p-value of 0.001), CPT uptake 75% to 90.3% (15.3% pre-post difference with 95% CI and p-value of 0.002), viral load measurement at six months 78% to 89.75% (11.75% pre-post difference with 95% CI at the p-value of 0.013), IPT uptake 62% to 71% (9.7% pre-post difference with 95% CI at a p-value of 0.004), screening for TB 90% to 97% (7% pre-post difference with 95% CI at a p-value of 0.001) and reporting of good adherence status 96.9% to 98.3% (1.4% pre-post difference with 95% CI and at a p-value of 0.014) (Table 2).
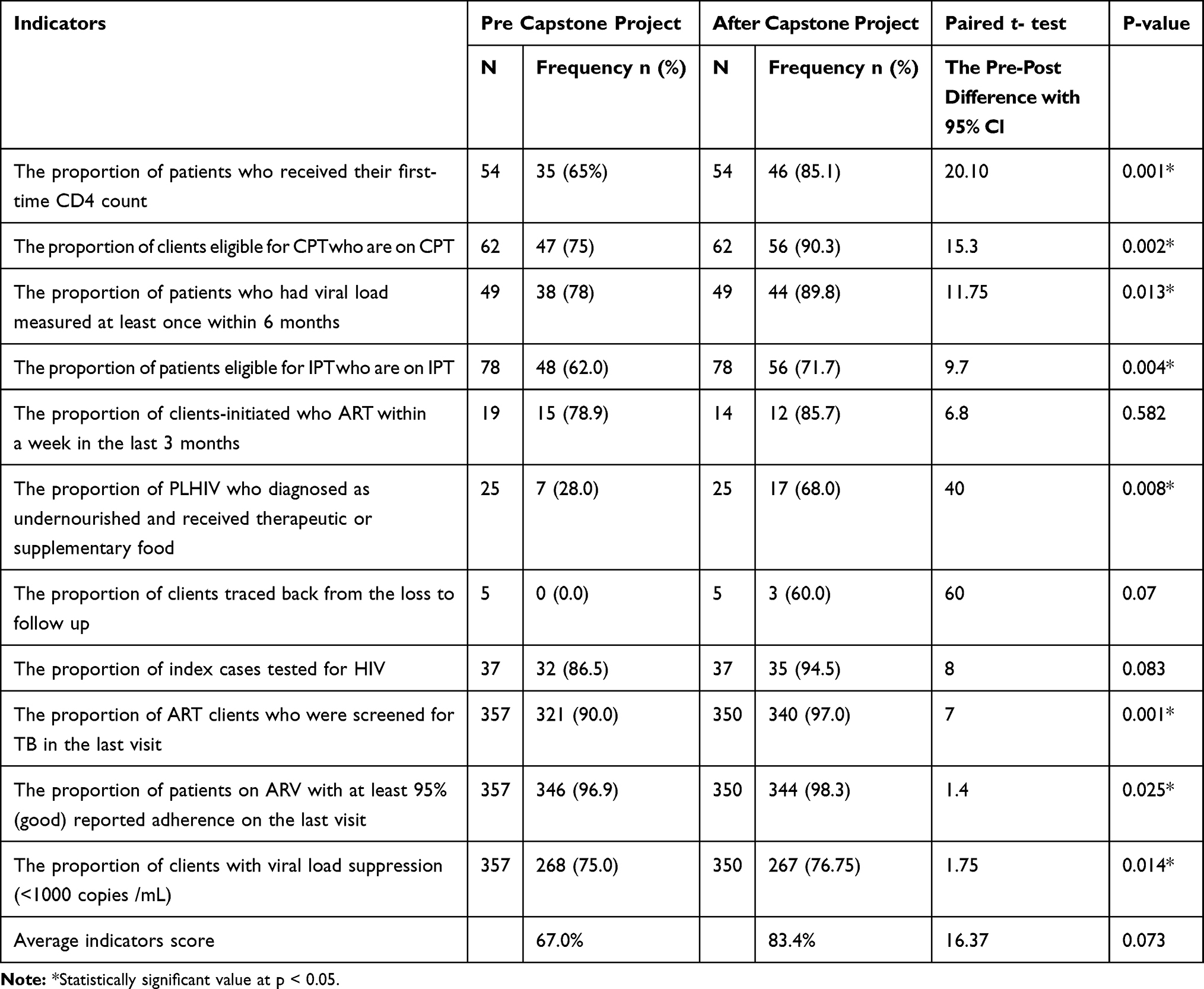 |
Table 2 Output of Pre- and After Capstone Project Compliance of HIV Clinical Care Practice with National Guidelines Based on Chart Review Data at Bure Primary Hospital, Northwest, Ethiopia, 2020 |
Average Gap Scores of Participants Expectation and Perception
The tangibility, reliability, and assurance dimensions of the SERVQUAL model provided positive scores. On the contrary, the empathy and responsiveness dimensions showed negative values. Supplementary Table 1
Overall Scores of Participants Expectation and Perception
The overall score shows a positive value which indicates good quality ART service (Table 3).
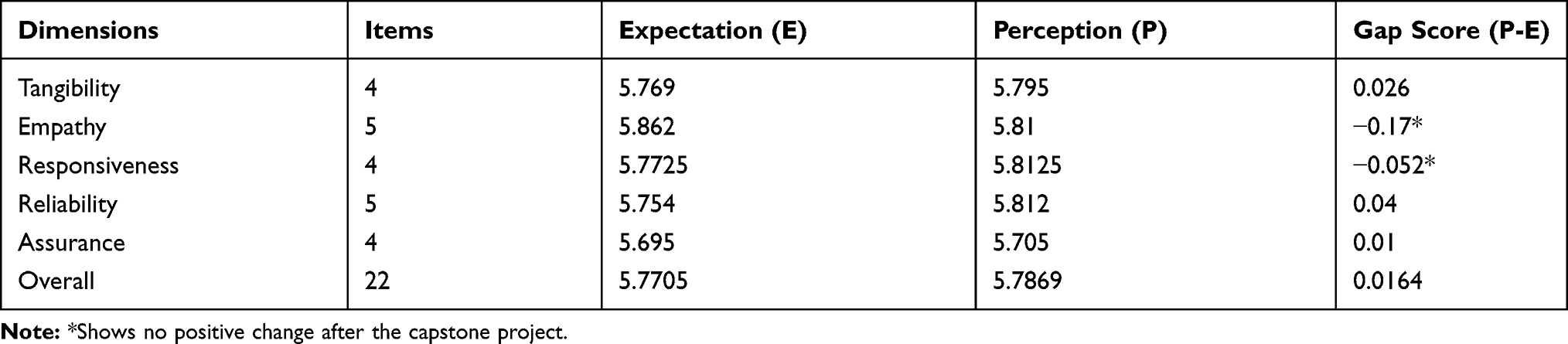 |
Table 3 Summary of Average Gap Scores of SERVQAL Dimensions at Bure Primary Hospital, 2020 |
Discussion
Based on the finding, the average compliance of clinical care practice indicators score improves from 67% to 83.37% before and after the capstone project, respectively. Thus, even though the magnitude of change of compliance of clinical care practice score after the capstone project varies, there was a significant change in all clinical care practice indicators score. This finding might show that the effect of the capstone project on the identified root causes was important to improve the quality of ART service. But there is no significant change in the initiation of ART within a week after the capstone project.
Receiving the first time, CD4 count improved from 65% to 85.1% (20.1% increment). This post-interventional finding is greater than a study conducted in South Africa to know the uptake of CD4 count determination at public health facilities which is only 57% of people living with HIV had CD4 count done.18 Here, the difference might be due to the capstone project. According to this study finding, CPT intake among eligible is improved from 75% to 90.3%. On the other hand, a cross-sectional study conducted in Felege Hiwot referral hospital to evaluate HIV/AIDS clinical care quality showed that only 45.9% of patients eligible for co-trimoxazole prophylactic therapy (CPT) were taking CPT.
In a study conducted in the Yangon Region of Myanmar, only 34% of PLWHIV received viral load testing due to programmatic challenges in adhering to routine visceral leishmaniasis (VL) monitoring protocol.33 But in this particular capstone project study finding by the routine collection of samples and sending it for viral load testing, viral load measurement improves from the baseline of 75% to 89.75%. Furthermore, in this before-after study, viral load suppression is almost the same (75% and 76.75) before and after capstone project periods, respectively. This finding contradicts the findings of the UNAIDS 2014 report, which set performance targets for the elimination of HIV by reaching 90% viral suppression among individuals who started treatment. Patient-related factors such as co-morbidities, incomplete medication adherence, missed clinic appointments, and interruption of or intermittent access to ART, as well as ARV regimen-related factors such as adverse drug effects and suboptimal pharmacokinetics, cause virological non-suppression in HIV patients.17 Even though preventive activities that enhance the quality of HIV care among PLWHA individuals enrolling eligible clients in IPT are international strategies that are complemented by national guidelines, a study conducted in health facilities of Addis Ababa showed that gab enrolling in IPT were observed.23 This finding is observed in this capstone project in which only 75% of eligible clients are enrolled in IPT.
ART initiation within a week improved from 78.9% to 85.7%, showed a 6.8% increment after the capstone project. Based on this finding, early initiation is still a problem due to different reasons. However, this before-after study finding is similar to that of a study conducted in Tanzania and Mozambique.20 This similarity might be due to being similar in the socio-economic status of respondents.
By ensuring the availability of supplementary food, the percentage of receiving supplementary food improves from 28% to 68%, and by strengthening of lost follow-up tracing mechanism, three clients are traced back to their treatment out of 5 lost to follow-up patients who make the percentage of lost to follow up was 60%.
In this before-after study, the overall quality of ART service was measured in the design by capturing respondents’ expectations and perceptions along the five dimensions of service quality. In this case, there is the poor quality of ART service along empathy and responsiveness dimensions, evidenced by the negative gap score. In contrast, the gap score on tangibility, reliability, and assurance dimension is positive, indicating good quality of ART service according to the SERVQUAL model.32 In general, the overall ART service quality was computed to be a positive value. This shows that the presence of positive gap scores signifies higher service quality.
Limitation of the Study
This study used a pre-post study design, which has the merit of showing that the intervention has an impact on the outcome; however, pre-post studies lack control over other confounders that are changing at the same time the intervention is being implemented. Therefore, the changes attained in the service quality improvement during the study period cannot be entirely attributed to the specific intervention.
Conclusion
Ensuring regular internal mentorship, availing supplies, and providing refresher training has a significant effect on the quality of ART service. Thus, adhering to national guidelines and fulfilling the availability of the recommended infrastructures helps to improve the quality of ART service. Therefore, the clinical care provider should adhere to national guidelines to keep the quality of ART service. In addition, the clinical care provided to PLWHA clients should regularly monitor through internal mentorship.
Data Sharing Statement
All the data were included in the study, and data will be available upon a reasonable request from the corresponding author.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Ethical Committee of the Institute of Public Health, College of Medicine and Health Sciences, the University of Gondar (Ref. No. IPH/837/2020). Before the actual data collection was started, an official permission letter was obtained from Bure Primary Hospital. After a brief description of the study’s purpose, risk, and benefits, written consent was obtained from participants, and for <18 years, parental informed consent was obtained. Data were anonymous and held on a secure password-protected system. Confidentiality during all phases of research activities was kept. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
Our gratitude goes to the University of Gondar, College of Medicine and Health Sciences, Institute of Public Health, Department of Health Systems and Policy to conduct this capstone project on the selected topic. Furthermore, our in-depth gratitude goes to data collectors and supervisors who helped us a lot and study participants for their valuable time spent in the interview. Finally, we would like to express our in-depth gratitude to Bure Primary Hospital senior management team for their support on any occasion.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The University of Gondar sponsored this study. However, it has no role in the decision to publish, manuscript preparation, and publication.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. UNAIDS/WHO. Global report: UNAIDS report on the global AIDS epidemic 2012; 2013.
2. World Health Organization. HIV/AIDS. Key facts. WHO; 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
3. Dias SS, Andreozzi V, Martins RO. Analysis of HIV/AIDS DRG in Portugal: a hierarchical finite mixture model. Eur J Health Econ. 2013;14(5):715–723. doi:10.1007/s10198-012-0416-5
4. Paterson DL, Swindells S, Mohr J, et al. adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30. doi:10.7326/0003-4819-133-1-200007040-00004
5. Bangsberg DR, Hecht FM, Charlebois ED, et al. adherence to protease inhibitors, HIV-1 viral load, and development of drug resistance in an indigent population. AIDS (London, England). 2000;14(4):357–366. doi:10.1097/00002030-200003100-00008
6. World Health Organization. Maintaining and improving quality of care within HIV clinical services. World Health Organization; 2019.
7. Naik CK, Gantasala SB, Prabhakar GV. Service quality (SERVQUAL) and its effect on customer satisfaction in retailing. Eur J Soc Sci. 2010;16(2):231–243.
8. Sohail MS. Service quality in hospitals: more favourable than you might think. Manag Serv Qual. 2003.
9. Wilson IB, Landon BE, Marsden PV, et al. Correlations among measures of quality in HIV care in the United States: cross sectional study. BMJ. 2007;335(7629):1085. doi:10.1136/bmj.39364.520278.55
10. Ababa A. Federal Democratic Republic of Ethiopia Ministry of Health. Ethiopia: Postnatal Care; 2003.
11. Kubacka RT. A primer on drug utilization review. J Am Pharm Assoc. 1996;NS36(4):257–61, 79. doi:10.1016/s1086-5802(16)30049-3
12. Hirschhorn LR. Ensuring quality of care in the scale-up of HIV care and treatment in resource-limited settings: a challenge for all. Clin Pract. 2007;4(6):737.
13. McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635–2645. doi:10.1056/NEJMsa022615
14. Stein MD, Piette J, Mor V, et al. Differences in access to zidovudine (AZT) among symptomatic HIV-infected persons. J Gen Intern Med. 1991;6(1):35–40. doi:10.1007/BF02599388
15. Gallant JE, Adimora AA, Carmichael JK, et al. Essential components of effective HIV care: a policy paper of the HIV Medicine Association of the Infectious Diseases Society of America and the Ryan White Medical Providers Coalition. Clin Infect Dis. 2011;53(11):1043–1050. doi:10.1093/cid/cir689
16. Seid M, Wasie B, Admassu M. Disclosure of HIV positive result to a sexual partner among adult clinical service users in Kemissie district, northeast Ethiopia. Afr J Reprod Health. 2012;16(1):97–104.
17. Manosuthi W, Ongwandee S, Bhakeecheep S, et al. Guidelines for anti-retroviral therapy in HIV-1 infected adults and adolescents 2014, Thailand. AIDS Res Ther. 2015;12(1):12. doi:10.1186/s12981-015-0053-z
18. Rispel L. Analyzing the progress and fault lines of health sector transformation in South Africa. S Afr Health Rev. 2016;2016(1):17–23.
19. Malawi’s Option B+ 2011–2015: the impact of rapid ART decentralization.
20. Ahmed M, Merga H, Jarso H. Predictors of virological treatment failure among adult HIV patients on first-line anti-retroviral therapy in Woldia and Dessie hospitals, Northeast Ethiopia: a case-control study. BMC Infect Dis. 2019;19(1):305. doi:10.1186/s12879-019-3924-4
21. Rosenthal EL, Brownstein JN, Rush CH, et al. Community health workers: part of the solution. Health Aff. 2010;29(7):1338–1342. doi:10.1377/hlthaff.2010.0081
22. Alemayehu YK, Bushen OY, Muluneh AT. Evaluation of HIV/AIDS clinical care quality: the case of a referral hospital in North West Ethiopia. Int J Qual Health Care. 2009;21(5):356–362. doi:10.1093/intqhc/mzp030
23. Kassa A, Teka A, Shewaamare A, et al. Incidence of tuberculosis and early Mortality in a large cohort of HIV infected patients receiving anti-retroviral therapy in a tertiary hospital in Addis Ababa, Ethiopia. Trans R Soc Trop Med Hyg. 2012;106(6):363–370. doi:10.1016/j.trstmh.2012.03.002
24. Denegetu AW, Dolamo BL. HIV screening among TB patients and co-trimoxazole preventive therapy for TB/HIV patients in Addis Ababa: facility based descriptive study. PLoS One. 2014;9(2):e86614. doi:10.1371/journal.pone.0086614
25. World Health Organization. WHO report on the tuberculosis epidemic, 1997: use dots more widely. Geneva; 1997.
26. Melaku B, Biruk M, Abegaz TM, et al. Evaluation of co-trimoxazole use as a preventive therapy among patients living with HIV/AIDS in Gondar University Referral Hospital, northwestern Ethiopia: a retrospective cross-sectional study; 2016.
27. Morowatisharifabad M-A, Movahed E, Nikooie R, et al. Adherence to medication and physical activity among people living with HIV/AIDS. Iran J Nurs Midwifery Res. 2019;24(5):397. doi:10.4103/ijnmr.IJNMR_205_18
28. Binagwaho A, Kyamanywa P, Farmer PE, et al. The human resources for health program in Rwanda—a new partnership. N Engl J Med. 2013;369(21):2054–2059. doi:10.1056/NEJMsr1302176
29. Langley GJ, Moen RD, Nolan KM, et al. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. John Wiley & Sons; 2009.
30. Parasuraman A, Berry L, Zeithaml V. Refinement and reassessment of the SERVQUAL scale. J Retail. 2002;67(4):114.
31. Parasuraman A, Zeithaml VA, Berry LL. Servqual: a multiple-item scale for measuring consumer perc. J Retail. 1988;64(1):12.
32. Parasuraman A, Zeithaml VA, Berry LL. A conceptual model of service quality and its implications for future research. J Mark. 1985;49(4):41–50. doi:10.1177/002224298504900403
33. Thinn KK, Thekkur P, Kyaw NTT, et al. Uptake of routine viral load testing among people living with HIV and its implementation challenges in Yangon Region of Myanmar: a mixed-methods study. BMJ Open. 2019;9(12):e032678. doi:10.1136/bmjopen-2019-032678
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.