Back to Journals » Cancer Management and Research » Volume 17

Improving Patient Education Materials for HPV Self-Collection: Insights from Women at High Risk of Developing Cervical Cancer
Authors Mkuu RS, Tohme S ![]() , Rivero-Mendoza D, Salloum RG, Goede D, Bruggeman B, Nicholson K, Hall JM, Bylund C, Woodard JN, Hensley J, Shenkman EA, Donahoo WT, Mulugeta A
, Rivero-Mendoza D, Salloum RG, Goede D, Bruggeman B, Nicholson K, Hall JM, Bylund C, Woodard JN, Hensley J, Shenkman EA, Donahoo WT, Mulugeta A ![]() , Hernandez M, Staras SA
, Hernandez M, Staras SA
Received 11 July 2025
Accepted for publication 29 November 2025
Published 24 December 2025 Volume 2025:17 Pages 3273—3284
DOI https://doi.org/10.2147/CMAR.S552282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bilikere Dwarakanath
Rahma S Mkuu,1 Sara Tohme,1 Daniela Rivero-Mendoza,1 Ramzi G Salloum,1 Dianne Goede,2 Bradley Bruggeman,3 Kaitlin Nicholson,3 Jaclyn M Hall,1 Carma Bylund,1 Jennifer N Woodard,4 Jamie Hensley,4 Elizabeth A Shenkman,1 William T Donahoo,5 Aman Mulugeta,1 Melody Hernandez,1 Stephanie A Staras1
1Department of Health Outcomes and Biomedical Informatics, University of Florida, Gainesville, FL, USA; 2Department of Internal Medicine, University of Florida, Gainesville, FL, USA; 3Department of Obstetrics and Gynecology, University of Florida, Gainesville, FL, USA; 4Office of Community Outreach and Engagement, University of Florida, Gainesville, FL, USA; 5Department of Medicine, Endocrinology, Diabetes, and Metabolism, University of Florida, Gainesville, FL, USA
Correspondence: Rahma S Mkuu, Department of Health Outcomes and Biomedical Informatics, University of Florida, 1889 Museum Road, Suite 7000, Gainesville, FL, 32611, USA, Email [email protected]
Purpose: Women living with chronic conditions and/or living in poverty have a higher risk of developing cervical cancer compared to the general population due to lower rates of cervical cancer screening (CCS). Human papillomavirus (HPV) self-collection tests improve CCS rates in under-screened populations by reducing barriers. However, some women are concerned about the ability to adequately perform self-collected sampling for CCS. This study examined how existing HPV self-collection patient education materials can be enhanced to increase self-efficacy in self-collecting samples.
Methods: We conducted three focus groups with 13 women living in zip codes associated with high poverty rates or chronic conditions in north central Florida. The Information-Motivation Behavioral Skills Model (IMB model) and the Patient Education Material Assessment Tool for Printable Materials (PEMAT-P) guided the focus group discussions. Focus group interviews were recorded and transcribed, and thematic analysis was used to analyze the data.
Results: Opportunities for improvement included: (1) Information: Using simplified language, including HPV and cervical cancer information, clear explanations about mailing procedures, information on access and interpretation of results, and visual elements to increase user confidence in medical soundness and safety, (2) Motivation: offering the materials in various languages and balancing design for inclusion of all women, and (3) Behavioral Skills: enhancing visual aids through clear directions to instructional videos, use of zoomed-in images, and projecting variable female anatomy figure positions to illustrate proper device insertion to encourage actionability.
Discussion: This study helps to bridge the gap in studies aimed at enhancing participation in HPV self-collection by examining opportunities to improve current HPV self-collection printed patient education materials and instructions among women with increased cervical cancer risk. Participants identified opportunities to enhance language, visual aids, and inclusivity – factors that may improve women’s confidence in self-collection and ultimately increase rates of CCS in underserved women.
Keywords: HPV self-collection, cervical cancer screening, underscreened population, chronic diseases, patient education material
Introduction
Each year, approximately 11,500 women in the United States are diagnosed with cervical cancer, of whom 4,000 die of the condition. The disease is highly preventable through screening.1,2 The 5-year survival rate of cervical cancer prior to metastasis is 91%, and drops to 60% once the cancer has spread to nearby tissues, organs, or lymph nodes.3 Therefore, screening is the cornerstone for reducing cervical cancer mortality. Primary screening methods include the Pap test, which screens for precancerous lesions of the cervix that can be treated to prevent cancer development; and/or the cervical human papillomavirus (HPV) test, which detects the virus responsible for 99% of cervical cancer.4,5 The American Cancer Society recommends screening for cervical cancer primarily via HPV testing as the most sensitive strategy to detect cervical cancer risk,5 allowing for surveillance of positive HPV cases to maximize timely intervention.
Women living in poverty6,7 and women with chronic conditions such as obesity8 and type 2 diabetes (T2D)9 have a high risk of developing cervical cancer. For example, the cervical cancer screening rate among women with type 2 diabetes is 66.5% compared to women without T2D, 73.3%.10 Women living in poverty or with chronic conditions often experience multiple barriers to screening, including cost, limited access to care, and time constraints.11–15 Additionally, research shows that women living with substance use or mental health conditions also have lower screening rates for cervical cancer.16 These obstacles to screening contribute to higher rates of late-stage diagnoses,17–20 which in turn are associated with higher mortality rates in these patients.9,21,22
HPV-based screening is preferred to cytology-based Pap screening by the American Cancer Society and many international society guidelines based on randomized controlled trials demonstrating the improved sensitivity and specificity of this method to detect cervical cancer.5 Self-collection is a primary HPV-based method, and for some patients, this option is preferable to Pap tests performed in the clinic because it allows women to collect a sample in privacy and return it to a lab for analysis.23 In recent years, HPV self-collection has gained attention as a strategy that mitigates barriers to cervical cancer screening.24–28 In a study conducted among infrequently screened women in North Carolina, up to 98% of participants who self-collected a sample for HPV testing found it acceptable enough to repeat it, citing convenience, ease of use, and privacy inherent to self-collection testing as motivating factors.23
While the opportunity to perform HPV self-collection significantly increases screening rates,24–28 some testing barriers need to be addressed.27 A qualitative study of women in the southeastern US concluded that women report concern about the ability to adequately collect their own sample despite being receptive to the test.27 Participants conceded that while physician-collected screening is inconvenient and uncomfortable, the experience of a trained professional alleviated some of these concerns.27 These findings have also been observed in other studies, highlighting the need to improve instructions to meet the information needs of women to collect their own samples adequately.24
Underserved and low-literacy communities often struggle to access, comprehend, and engage with cancer-related patient education materials.29,30 The US government’s “Healthy People 2030” initiative emphasizes health organizations’ responsibility for addressing health literacy, facilitating access, and allowing people to utilize health information rather than just understanding it.31 Thus, there is an increasing recognition of the need to tailor educational resources and communication tactics in order to meet diverse community needs and promote health equity.32 Resources can range from simple written instructions to an in-depth series of videos, covering every step from the self-collection procedure to the logistics of sample shipping. Patient education materials addressing health literacy needs for cancer screening have shown potential to improve patient uptake, adherence, and self-efficacy. For instance, research on fecal immunochemical test (FIT) use for colorectal cancer screening has highlighted that patient preferences for kit characteristics significantly influence test acceptability and completion rates.33 These lessons can be applied to HPV self-collection kits in order to maximize effective utilization among hard-to-reach women.
The Information-Motivation-Behavioral Skills model (IMB model)34 explains how constructs of information, motivation, and behavioral skills help to explain individuals’ HIV risk-related behaviors. The construct of information includes not only knowledge about the behavior but also factors such as myths/heuristics that may influence behavior change. Motivation includes personal beliefs about a particular intervention and associated attitudes in engaging in that behavior. Lastly, behavioral skills include the necessary elements or tools needed to facilitate behavior change for performing a specific health behavior.34 The model has been applied to cancer contexts and has been found to accurately predict participation in cervical cancer screening.35
For many years, patient education materials were predominantly designed by healthcare professionals, who often relied on tools such as the Patient Education Materials Assessment Tool for Print Materials (PEMAT-P) to evaluate the understandability and actionability of these resources.36 The PEMAT-P provides a systematic framework for assessing whether diverse patient populations can comprehend key messages and identify actionable steps based on the information presented. One example of a patient education material is the Evalyn Brush™ test, an HPV self-collection test from Rovers Medical Devices that uses animated films and graphics.
The development process of patient education materials has historically excluded direct patient involvement, resulting in materials that may not fully address patient priorities or lived experiences.37 Additionally, there has been a notable lack of systematic collection and integration of patient feedback, potentially limiting the patient-centeredness aspect of these resources. Although research shows that the effectiveness of patient education materials is not dependent upon whether they are developed by experts or co-created with patient engagement,38 it is important to tailor patient education materials by actively soliciting and incorporating patient feedback and input throughout their development and revision. This participatory approach not only aligns with best practices for person-centered care but may ensure that educational materials resonate with patients’ real-world needs and foster improved engagement and health outcomes.
This study aimed to identify the HPV self-collection information needs of women with increased cervical cancer risk. The secondary objective was to tailor the existing instructions for the HPV self-collection kit, using the Evalyn Brush™ test. We conducted focus groups to examine the opinions of women at high risk for developing cervical cancer. The feedback was obtained to guide the modification of printed patient education materials to increase patient understanding and actionability.
Methods
Study Design
This cross-sectional study gathered qualitative data through focus group discussions with women living in North Central Florida with high-risk factors for developing cervical cancer. The study utilized focus groups to explore the collective dialogue and social interactions that shape participants’ knowledge and attitudes, while also facilitating the discussion of diverse viewpoints in a supportive environment.39 The focus groups were conducted at a local church’s community room, a known community resource open to all members regardless of religious affiliation. This location regularly hosts non-religious activities, including research, youth, adult activities, Girl Scout meetings, and Anonymous Support Groups. Each focus group was conducted during the weekday, starting at 5:30 pm to reduce time barriers related to work hours.
Recruitment and Participants
Recruitment flyers were posted in various locations, including gyms, clinics, and parks throughout North Central Florida. Recruitment was also conducted via social media, and the study was highlighted on a large university in the Southeastern United States’ Facebook page designed for recruitment for research studies. Flyers were also displayed on media designed for local news, announcements, and support groups (eg, local social media mom groups). Information about the study was included, and a linked survey was utilized to screen patients for eligibility.
Eligibility/Inclusion criteria included women who met the following: 1) 25–65 years of age; 2) assigned sex of female at birth; 3) history of diagnosis of any of the following chronic conditions: mental health conditions, diabetes, substance use disorders, or obesity; 4) willingness and ability to participate in both study components (survey and focus group); and if the women had any of the following high-risk factors for cervical cancer: live in a census tract area representing the highest two quartiles of high social vulnerability score or live in a rural area or identify with minority race (Black, Hispanic) or have no insurance, or have Medicaid or Medicare insurance. We excluded women who had ever been diagnosed with cervical cancer.
Study procedures were described to each participant during the consent process. Women who agreed to participate were subsequently provided with a survey that collected their demographic characteristics and assessed their HPV testing knowledge. Participants received a $10 gift card as compensation for their time and effort. After completing the survey, participants were invited to a scheduled in-person focus group discussion. Participants received an additional $35, a light meal, and a $5 transportation allowance for the in-person focus group attendance. This study complies with the Declaration of Helsinki40 and was approved by the Institutional Review Board at the University of Florida, IRB# ET00023594.
Measures
Pre-Focus Group Survey
REDCap was used to collect demographic information and questions to establish a participant’s preexisting knowledge of HPV and HPV testing. The survey included 32 closed-ended questions regarding socioeconomic status, cervical cancer screening history, and responses to provided HPV statements, allowing researchers to achieve a baseline understanding of how each participant may be under-screened and/or under-represented. By exposing participants to topics that would be revisited later in focus groups, researchers were able to evaluate trends in HPV knowledge.
Focus Group Interviews
The research team developed a structured focus group discussion guide. The PEMAT scoring tool,36 which evaluates women’s understandability and actionability of existing material, was used to inform the development of this guide. The guide included general information on HPV and cervical cancer, such as transmission, symptoms, and collection practices. The guide first elicited women’s opinions on the self-collection kit. The questions focused on the instructions’ aesthetics, ease of understanding, word choice/style, organization/layout, and the visual aids they contained. Additional questions focused on the instructions’ ability to increase their desire to take their sample, self-collection confidence, and whether the participants found the product culturally acceptable.
Focus Group Procedures
Three audiotaped focus groups were conducted from June to October 2024. Each session lasted approximately 90 minutes. The size of the focus group ranged from three to six participants. Each participant was provided a light meal at the beginning of the focus group. After introductions at each interview, the study coordinator then reviewed the informed consent, addressed any questions, and reminded participants of the voluntary nature of the focus group and that their anonymized responses, including direct quotes, may be included in research reports, presentations, and publications. Following this, a warm-up activity was conducted in which participants wrote and read aloud an alias to be used for the purpose of recording the session.
The principal investigator then explained topics related to HPV, including how it spreads, the associated risks, and how healthcare providers perform Pap and HPV testing. Participants were then given information about the self-collection test, and sample kits were given out. Women were given time to familiarize themselves with the HPV self-collection kit and its instructions. The investigators facilitated the focus group, and interviews were recorded and field notes taken. Some participants returned the HPV-self collection kit instructions with notes they had taken while participating in the discussion. Each focus group discussion lasted approximately 90 minutes.
Data Management and Analysis
The audio recordings were uploaded to a secure, password-protected Google Document using an institutional Google Account. Within this platform, transcription features were employed to convert the audio content into text. To ensure the accuracy and reliability of the transcripts, a member of the research team (DRM) reviewed each transcription by listening to its corresponding recording and edited as necessary. The transcripts were then uploaded to Atlas.ti for analysis.41
Transcriptions were subjected to thematic analysis using a priori or deductive coding42 informed by the Information Motivation Behavioral Skills Model (IMB Model)43 and the Patient Education Material Assessment Tool for Printable Materials (PEMAT-P).36 Three members of the research team (AG, JO, KE) coded the transcripts using the operationalized codebook with clearly defined codes, which ensured that codes were structured and consistently defined. The transcripts were first coded using line-by-line coding, and the team met bi-weekly to discuss any discrepancies in the coding assigned to the transcripts. The codes with the highest frequency were then identified as the most important factors to be considered in modifying the instructional materials.
Results
Demographic Characteristics
Thirteen women participated in three focus groups with 3–6 participants in each session (Table 1). Most participants were between 25 and 39 years of age (92.3%) and non-Hispanic (84.6%). Five participants held a bachelor’s degree (38.5%), and six were never married (46.2%). Most participants had health insurance (92.3%). All participants reported having been screened for cervical cancer previously. Of the questions surrounding HPV general knowledge,44 no participant correctly answered all questions. Approximately half (53.8%) were aware that most sexually active people will encounter HPV at some point in their lives. Only 45.5% of participants (n=5) reported knowledge that a woman’s cervical cancer risk is low if an HPV test is negative.
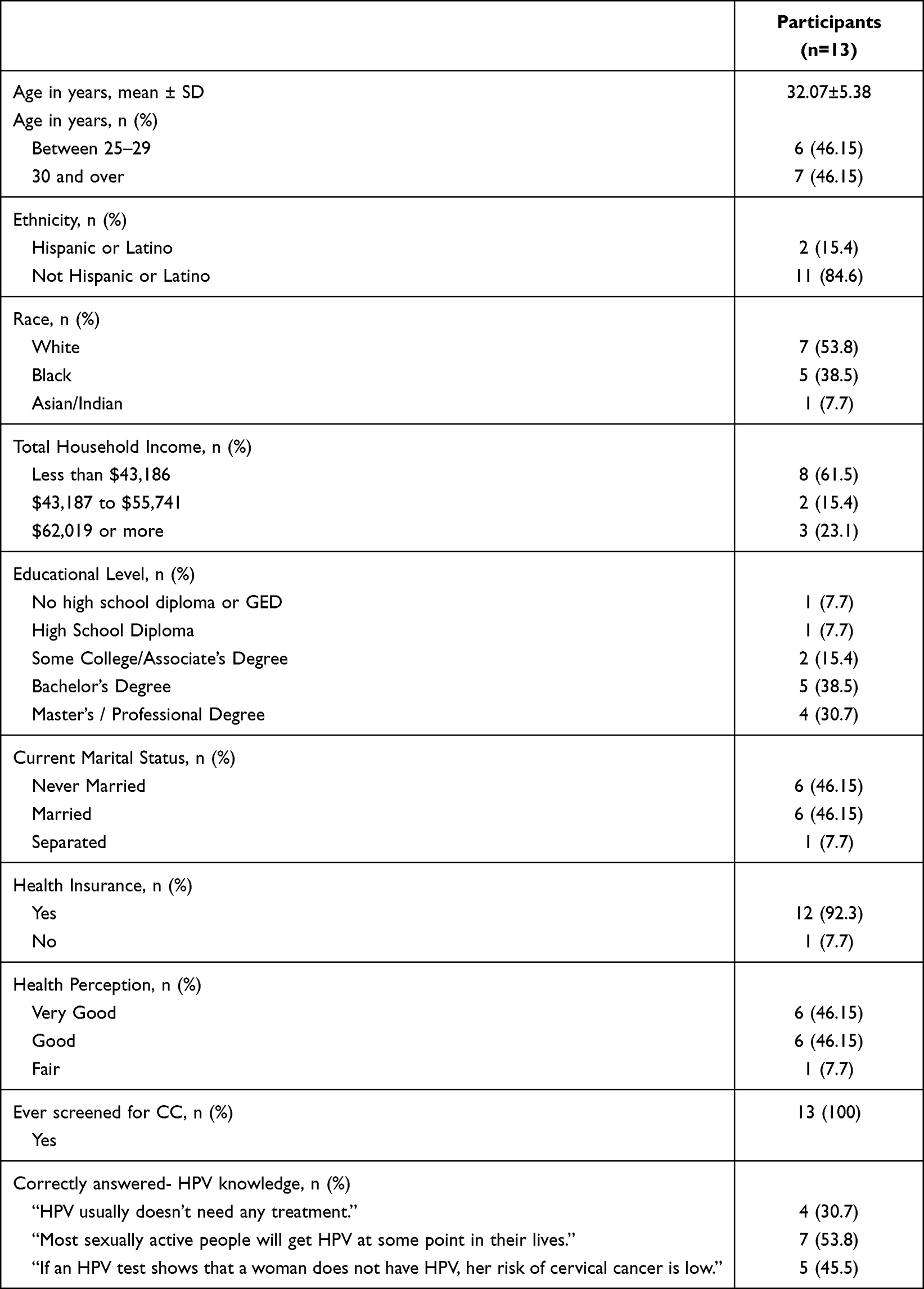 |
Table 1 Demographic Characteristics of Study Participants |
Qualitative Findings
According to the IMB model, “information” refers to the accuracy and relevance of specific behavior, condition, or prevention strategies. Two themes from the constructs of the PEMAT-P fit the “information” construct of the IMB model: (1) Content: need to have HPV and cervical cancer information, and (2) Word choice and style: need to simplify and use common language and reduce medical terms. Two themes from the constructs of the PEMAT-P fit the “motivation” construct of the IMB model: (1) offering materials in various languages, and (2) balancing design for inclusion of all women. The main PEMAT-P themes that emerged that fit the “behavioral skills” construct of the IMB model were (1) enhancing visual aids, and (2) breaking down instructions into manageable, explicit steps, and encouraging HPV self-collection actionability. Findings and example quotes are summarized in Table 2.
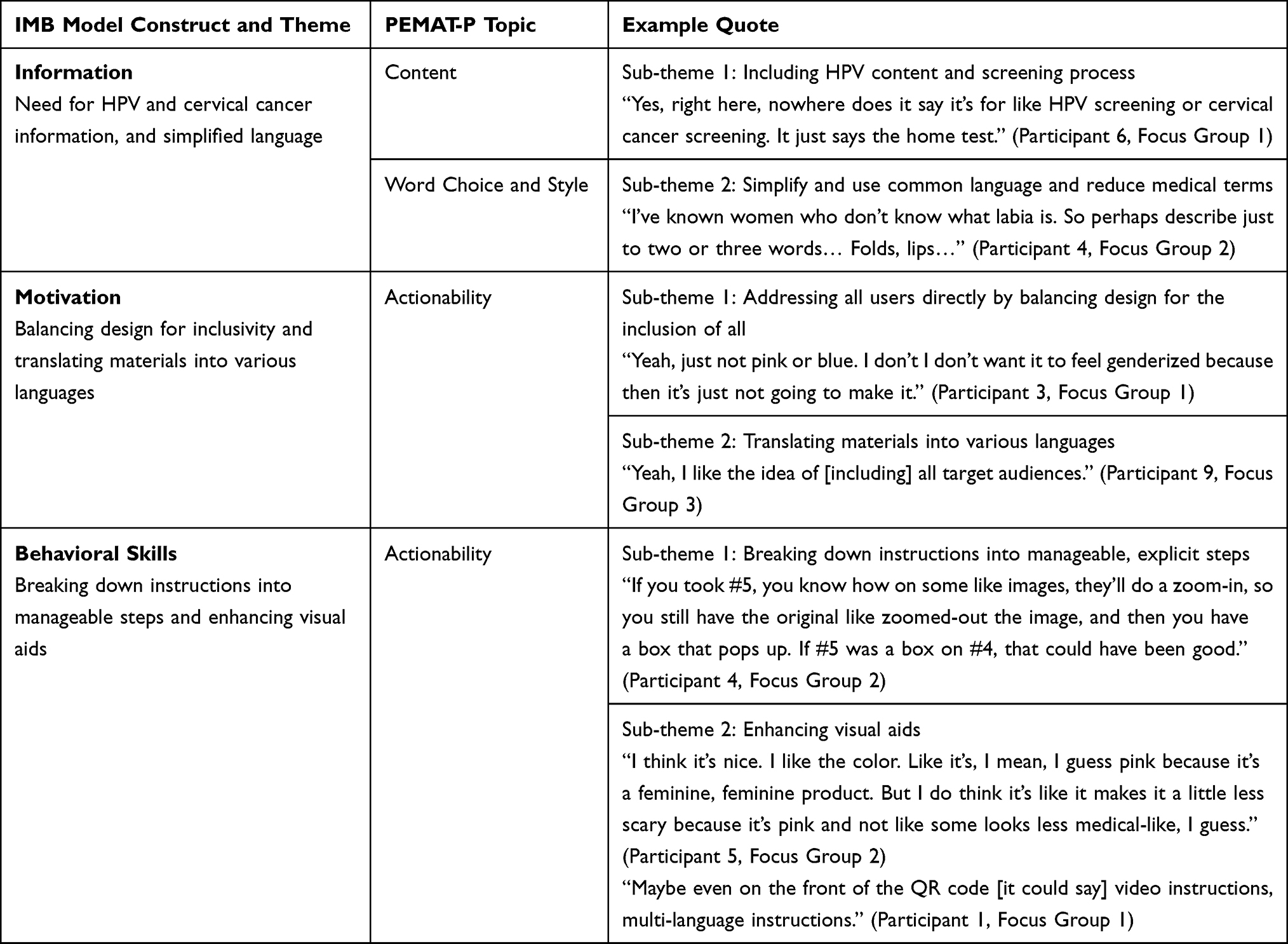 |
Table 2 Summary of Qualitative Results |
Information - Need for HPV and Cervical Cancer Information, and Simplified Language
Participants shared that the instructions were mainly focused on the self-collection of the sample and were missing information on HPV and cervical cancer. Participants shared that having information about HPV and cervical cancer would stress the importance of HPV testing and would provide women with more knowledge of the virus and cancer. The research team infers that the instruction guide for the Evalyn Brush™ may have been deliberately designed to be used for purposes other than HPV testing. Nevertheless, participants reported the need to have information about HPV and its association with cervical cancer as part of the content.
Sub-Theme 1: Include HPV Content and Screening Process Details
Participants suggested clarification on the recommended avoided vaginal products prior to use of the Evalyn Brush™ test. Specifically, they wanted to know if the avoidance of menstruation cups and tampons was required. In addition, one participant shared that the title of the instruction pamphlet did not precisely reflect the purpose of the instructions:
Yes, right here, nowhere does it say it’s for like HPV screening or cervical cancer screening. It just says the home test. (Participant 6, Focus Group 1)
Although women shared that after reading the instructions, they felt it was relatively simple to understand what steps to take while obtaining the sample, they expressed concerns regarding the shipping procedures, underscoring the importance of discretion in transporting such materials.
I think discreteness in terms of how it’s shipped to you would be a benefit. I don’t know like how it comes like in terms of envelope box or something like that, but it, it’s not something you necessarily want your roommates or your family to see that you’re getting because it’s a little bit like taboo. (Participant 5, Focus Group 2)
Similarly, women expressed uncertainty regarding the procedures for access and interpretation of results. They noted that the contact information provided on the back of the pamphlet was not local, which left them unaware of whom to approach with any questions. Furthermore, they recommended the inclusion of information detailing where to obtain additional resources. One participant stated:
Like give you know your, your readers like… if this happens, then maybe we could just put like a link of like a resource that they could go to. You know, that way, you’re not just leaving them hanging. Well, what happens when I get my test results back? You know, for positive HPV results, you can, you know, see your doctor. See whoever or visit this site for additional resources. (Participant 11, Focus Group 3)
Sub-Theme 2: Use Simplified, Common Language and Reduce Medical Jargon
Another participant described the number of adjectives as overwhelming and suggested simplifying sentences.
They’ve got all of the words for each item here on the stick. But then, in the instructions, they put more detailed information for it. Like the transparent casing, the pink plunger, the um, Evalyn Brush above the wings. You could have just told me to grab above the wings. The more words there are the more overwhelming it’s going to be. (Participant 3, Focus Group 1)
Participants reported overall satisfaction with the word selection used in the instructions. When discussing the appropriateness and comprehension of the words used in the instructions, one participant shared:
“Yeah, I think it was really well thought … like they really worded this very well. Even with like the vaginal terms. I think it was very, very, very, very thoughtful when they made this. I like it. (Participant 11, Focus Group 3)
Some participants thought that the language was overly formal and repetitive. Some participants emphasized the need to avoid medical jargon and instead use words that are more common for the general population. Several participants suggested adding a disclaimer stating that the collection should not be painful. They mentioned that the inclusion of adjectives such as “soft” to describe the brush could decrease women’s anxiety about potential pain. One participant shared:
Maybe it could just say like the soft brush or the flexible brush or flexible bristles or some sort of. adjective to kind of tell you… (Participant 5, Focus Group 2)
Motivation - Balancing Design for Inclusivity and Translating Materials into Various Languages
When asked about how to make the instruction materials more motivating to inspire behavior change, participants recommended that making the instructions more relatable to different types of women may motivate more engagement. Participants shared that the instructions should be available in different languages, and the design should be balanced to include women with diverse backgrounds.
Sub-Theme 1: Addressing All Users Directly by Balancing Design for the Inclusion of All
A majority of participants perceived the instructions to be welcoming and respectful of diverse cultural backgrounds. The instruction included a photo of three women who appeared to be culturally diverse, and the women were of different age groups. One participant shared:
They have like 3 different [women in the picture]. It shows that you know it can be used across the spectrum. (Participant 10, Focus Group 2)
Sub-Theme 2: Translate Materials into Various Languages
Participants shared that printed instructions should be available in multiple languages to enhance accessibility. Participants were shown the English version of the printed instructions. One participant stated:
It would be helpful for it to be. translated into multiple languages so that it can be… accessible to different cultures across places. (Participant 10, Focus Group 2)
Some participants suggested making the material available to individuals with disabilities. One participant shared:
I know in this kind of product it’s not easy to get some link to sign language, but it would be great to get like an explanation. Also, for blind people, an audio explanation of how to do this could be more accessible to those communities. (Participant 12, Focus Group 3)
Behavioral Skills - Breaking Down Instructions into Manageable Steps and Enhancing Visual Aids
Participants were asked whether the content was displayed in a way that encouraged actionability and behavioral change. A majority of participants shared that the content was clear on encouraging HPV self-collection and provided clear directions with explicit steps. While other participants suggested that the instruction guide could be improved by providing clear directions and enhancing some visual aids. Enhancements include enlarging images, showing different positions to illustrate proper insertion, and zooming in on images.
Sub-Theme 1: Organize Instructions into Manageable, Explicit Steps
The participants were queried about the actionability of the instructions, specifically the material’s capacity to delineate the actions that must be undertaken. Participants generally found that the instructions were easy to understand and the procedural steps with pictures to be helpful. Despite their overall satisfaction, participants commented on the clarification of some of the instructions. For instance, one participant stated:
I had to reference back to #4 from #5 because the hand with the leg up initially confused me… OK, so it’s it is her right hand. Using the insertion and then the left leg is up, so I had more pause on that. So, it wasn’t a barrier, but it was like, oh, I need to understand this. I need to go back at #4. (Participant 4, Focus Group 2)
Another participant expressed concern about the depiction of a single position for self-collection. One participant exclaimed:
It says standing position, but I know how my cervix is. I wouldn’t be able to stand to do it. So, I don’t know if there are other options to put other types of positions because it says like also like if you were to insert a tampon, but that never worked for me either. (Participant 3, Focus Group 1)
Other suggestions included illustrations of female anatomy. One participant acknowledged that reaching a balance between providing several options and keeping it simple can be challenging:
Because then it’s like when you when you give people too many options, they get confused. Yeah. So, it’s best to keep it simple. Best to keep it simple. (Participant 11, Focus Group 3)
Sub-Theme 2: Enhance Visual Aids
Participants offered suggestions for improvement, including changing the front picture to a more appealing image, such as one featuring women or a design conveying a message of self-care. Interestingly, participants had diverse opinions regarding the colors used for the instructions. Some participants were concerned about the excessive use of colors associated with femininity, such as pink, and suggested making the instruction more gender-neutral. Participants shared:
Like trans-friendly. I’m not trans myself, but I have friends who are trans, and they have. They hate seeing things that are like, pink and like things that say, you know, that they’re only for women. (Participant 2, Focus Group 1)
Conversely, other participants stated they felt comfortable with the pink colors, arguing that the colors made it less medical and reduced feelings of fear associated with medical procedures. One participant shared:
People grasping when they open up the pamphlet and read it, like the color is, I think the color is like inviting because it’s pink, it’s bright, it pulls people in. (Participant 11, Focus Group 3)
Similarly, during all the sessions, participants noticed a QR code that linked to video instructions in different languages, which was very small and did not have a description of its purpose. Additionally, some participants recommended enhancing the accessibility of the QR code by increasing its size, especially since individuals who viewed the video found it to be straightforward and easy to follow and expressed a preference for watching the video over reviewing the printed instructions. Additionally, participants recommended that the link to the video be provided in written form as well, as not everyone may be familiar with how to scan the QR code. One participant shared:
So maybe it’s something next to it that says for more, even if it just has more information, right? More information for videos, frequently asked questions, for resources… Go to this and then maybe have the link typed out [for] those people. (Participant 13, Focus Group 3)
Discussion
Although HPV self-collection is a preferred screening method for cervical cancer screening, a common barrier remains: a lack of self-efficacy and confidence in adequately collecting a self-sample.24,27 We conducted focus groups with women with risk factors for cervical cancer, guided by the Information-Motivation-Behavioral Skills (IMB) Model43 and the Patient Education Materials Assessment Tool for Printable Materials (PEMAT-P).45 This study explored how existing patient education materials for an available HPV self-collection device can be improved to enhance users’ self-efficacy. Participants in our focus groups identified several key areas for enhancement, 1) including the addition of information about HPV and cervical cancer, 2) simplifying language, 3) ensuring inclusive design, 4) translating materials into multiple languages, 4) further delineating the self-collection steps, and 5) enhancing visual aids.
Participants emphasized the importance of including HPV and cervical cancer information in the self-collection instruction guide. Research indicates that knowledge about HPV and its connection to cervical cancer is low in high-risk populations, such as women with low levels of education and/or income.46 Women with knowledge about HPV are more likely to receive HPV testing;47,48 therefore, providing foundational information about HPV and cervical cancer may improve HPV self-collection rates for screening. Additionally, participants expressed the need to simplify the language in the patient education materials. When instructions are clear and concise, patients are more likely to follow them correctly, improving health outcomes. If instructions are overly wordy or complex, they can cause confusion, overwhelm the reader, or lead to misinterpretation. Limited health literacy is associated with limited understanding of HPV and its association with cervical cancer.49 Accordingly, simplification of language to a universal understanding about the connection between HPV and cervical cancer may enhance self-collection. Having accessible language may also enhance overall user experience and reduce anxiety related to the self-collection process.
To improve motivation for self-collection in diverse groups of women, participants emphasized the importance of providing inclusive instructional materials. Specifically, participants recommended offering the instruction guides in multiple languages, using balanced color schemes that avoid overly feminine tones, and ensuring cultural sensitivity in design.50 Cervical cancer disproportionally affects underserved women, including women who may not primarily speak English, racial minorities, and gender-diverse individuals such as transgender men. The importance of incorporating inclusive elements in the HPV self-collection instruction guides has been emphasized in previous research and may increase participation rates among such individuals.50–52
In addition, participants suggested including more detailed and/or zoomed-in images, showing different angles of collection to clarify the self-collection process. Similar to another previous study, participants also shared concerns about individuals with limited mobility or dexterity to perform the self-collection adequately with the existing instructions,53 underscoring the value of patient education materials targeted to groups with different physical abilities. They also suggested that the addition of visuals, such as an image of a physician, may enhance the perception of seriousness associated with the self-collection process.54
The in-depth exploration of participant perspectives was a strength of this study. Focus groups encouraged interactive conversations that allowed participants to connect and relate to each other. Despite this, participants may have been susceptible to groupthink. Facilitators attempted to mitigate this by offering each individual an opportunity to share thoughts and encouraging diverse viewpoints. In addition, the sample size was small, although we reached saturation after the third focus group, as demonstrated by similarities in responses across the focus groups,55 and the study was conducted in a single geographical region, which may limit generalizability. Furthermore, participants were recruited based on specific criteria, which may have resulted in selection bias due to time or access constraints, notwithstanding efforts to provide a convenient meeting time and place for all.
Despite these limitations, this study contributes to the limited literature focused on strategies to improve HPV self-collection uptake. We identified opportunities to improve HPV self-collection in high-risk populations using a theory-informed study design. Our results demonstrate the importance of identifying ways to enhance the accessibility, inclusivity, and effectiveness of HPV self-collection. More research is needed in this field to better understand barriers to HPV self-collection.
While this study contributes to the limited literature highlighting strategies to improve HPV self-collection uptake, it is not without limitations. Firstly, our sample size was small, restricting generalizability. Participants were recruited based on specific criteria, including having chronic conditions or residing in neighborhoods with high poverty rates. Although those criteria add to enhancing the relevance of our findings for high-risk populations, this narrows the broader applicability of our findings.
Although focus groups are valuable in soliciting feedback from individuals while providing the opportunity for the group to enrich feedback by building off each other, they may be susceptible to groupthink.39,56 To mitigate this, focus group facilitators provided each individual the opportunity to share their thoughts and encouraged sharing diverse viewpoints amongst the groups.56 Another limitation of focus groups is that they may be more susceptible to selection bias, since the participation time may not be convenient to all. We planned focus groups to occur at a central location during the work week and also provided incentives and a meal to reduce participation barriers. This study has strengths, including its identification of opportunities to improve HPV self-collection in high-risk populations, as well as its theory-informed design.
Conclusion
Our findings suggest that self-efficacy for HPV self-collection can be improved by enhancing instructional materials. Key modifications include incorporating clear information about HPV and cervical cancer, simplifying the language, and balancing design elements to make sure the materials are relatable and inclusive. Additionally, refining visual aids and using culturally sensitive, inclusive language may further support users in confidently completing the self-collection process.
Acknowledgments
We would like to thank Jacquelyn Orozco, Adrianna Grant, and Keneisha Etienne for their contributions to coding the transcripts in Atlas.ti. We are thankful to the participants whose involvement made this research possible.
Funding
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Number K01CA292583. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. CDC. Cervical cancer statistics. Cervical Cancer; 2024. Available from: https://www.cdc.gov/cervical-cancer/statistics/index.html.
2. Cervical cancer. Available from: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer.
3. Cervical cancer prognosis and survival rates – NCI; 2022. Available from: https://www.cancer.gov/types/cervical/survival.
4. Curry SJ, Krist AH; US Preventive Services Task Force, et al. Screening for cervical cancer: US Preventive Services Task Force recommendation statement. JAMA. 2018;320(7):674–686. doi:10.1001/jama.2018.10897
5. Fontham ETH, Wolf AMD, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J Clin. 2020;70(5):321–346. doi:10.3322/caac.21628
6. Boscoe FP, Johnson CJ, Sherman RL, Stinchcomb DG, Lin G, Henry KA. The relationship between area poverty rate and site-specific cancer incidence in the United States. Cancer. 2014;120(14):2191–2198. doi:10.1002/cncr.28632
7. Cohen CM, Wentzensen N, Castle PE, et al. Racial and ethnic disparities in cervical cancer incidence, survival, and mortality by histologic subtype. J Clin Oncol off J Am Soc Clin Oncol. 2023;41(5):1059–1068. doi:10.1200/JCO.22.01424
8. Maruthur NM, Bolen SD, Brancati FL, Clark JM. The association of obesity and cervical cancer screening: a systematic review and meta-analysis. Obesity. 2009;17(2):375–381. doi:10.1038/oby.2008.480
9. Chen S, Tao M, Zhao L, Zhang X. The association between diabetes/hyperglycemia and the prognosis of cervical cancer patients: a systematic review and meta-analysis. Medicine. 2017;96(40):e7981. doi:10.1097/MD.0000000000007981
10. Miller EA, Pinsky PF. Cervical cancer screening and predictors of screening by diabetes status. Cancer Causes Control. 2022;33(10):1305–1312. doi:10.1007/s10552-022-01615-5
11. Fuzzell LN, Perkins RB, Christy SM, Lake PW, Vadaparampil ST. Cervical cancer screening in the United States: challenges and potential solutions for underscreened groups. Prev Med. 2021;144:106400. doi:10.1016/j.ypmed.2020.106400
12. Chan DNS, Law BMH, So WKW, Fan N. Factors associated with cervical cancer screening utilisation by people with physical disabilities: a systematic review. Health Policy. 2022;126(10):1039–1050. doi:10.1016/j.healthpol.2022.08.003
13. Biddell CB, Spees LP, Smith JS, et al. Perceived financial barriers to cervical cancer screening and associated cost burden among low-income, under-screened women. J Womens Health. 2021;30(9):1243–1252. doi:10.1089/jwh.2020.8807
14. Akinlotan M, Bolin JN, Helduser J, Ojinnaka C, Lichorad A, McClellan D. Cervical cancer screening barriers and risk factor knowledge among uninsured women. J Commun Health. 2017;42(4):770–778. doi:10.1007/s10900-017-0316-9
15. Mensah KB, Boamah Mensah AB, Yamoah P, et al. Socio-demographic factors and other predictors of Pap test uptake among women: a retrospective study in Ghana. Cancer Manag Res. 2023;15:489–499. doi:10.2147/cmar.s398500
16. Mkuu R, Salloum RG, Shenkman E, et al. Screening for cervical cancer among women with behavioral health conditions-A systematic review. Prev Med Rep. 2023;34:102238. doi:10.1016/j.pmedr.2023.102238
17. Boitano TKL, Powell MA, Leath CA, Michael Straughn J, Scarinci IC. Barriers and facilitators affecting presentation in women with early versus advanced stage cervical cancer. Gynecol Oncol Rep. 2022;40:100950. doi:10.1016/j.gore.2022.100950
18. Hall JM, Mkuu RS, Cho HD, et al. Disparities contributing to late-stage diagnosis of lung, colorectal, breast, and cervical cancers: rural and urban poverty in Florida. Cancers. 2023;15(21):5226. doi:10.3390/cancers15215226
19. Mkuu R, Hungu C, Makokha F, et al. “It was not normal, and I had to find a doctor and tell him.” Kenyan Women’s response to cervical cancer symptoms. J Patient Exp. 2024;11:23743735241283200. doi:10.1177/23743735241283200
20. Tekalign T, Teshome M. Prevalence and determinants of late-stage presentation among cervical cancer patients, a systematic review and meta-analysis. PLoS One. 2022;17(4):e0267571. doi:10.1371/journal.pone.0267571
21. Herweijer E, Wang J, Hu K, et al. Overall and cervical cancer survival in patients with and without mental disorders. JAMA Netw Open. 2023;6(9):e2336213. doi:10.1001/jamanetworkopen.2023.36213
22. Amboree TL, Damgacioglu H, Sonawane K, Adsul P, Montealegre JR, Deshmukh AA. Recent trends in cervical cancer incidence, stage at diagnosis, and mortality according to county‐level income in the United States, 2000–2019. Int J Cancer. 2024;154(9):1549–1555. doi:10.1002/ijc.34860
23. Anderson C, Breithaupt L, Marais AD, et al. Acceptability and ease of use of mailed HPV self-collection among infrequently screened women in North Carolina. Sex Transm Infect. 2018;94(2):131–137. doi:10.1136/sextrans-2017-053235
24. Camara H, Zhang Y, Lafferty L, Vallely AJ, Guy R, Kelly-Hanku A. Self-collection for HPV-based cervical screening: a qualitative evidence meta-synthesis. BMC Public Health. 2021;21(1):1503. doi:10.1186/s12889-021-11554-6
25. Vega-Crespo B, Neira VA, Maldonado - Rengel R, et al. Barriers and advantages of self-sampling tests, for HPV diagnosis: a qualitative field experience before implementation in a rural community in Ecuador. Int J Womens Health. 2024;16:947–960. doi:10.2147/IJWH.S455118
26. Mkuu RS, Staras SA, Szurek SM, et al. Clinicians’ perceptions of barriers to cervical cancer screening for women living with behavioral health conditions: a focus group study. BMC Cancer. 2022;22(1):252. doi:10.1186/s12885-022-09350-5
27. Mkuu RS, Staras SA, Chakrabarti C, et al. Acceptability of HPV self-collection: a qualitative study of Black women living with type II diabetes and social vulnerability. J Clin Transl Endocrinol. 2024;35:100331. doi:10.1016/j.jcte.2024.100331
28. Lofters A, Vahabi M, Fardad M, Raza A. Exploring the acceptability of human papillomavirus self-sampling among Muslim immigrant women. Cancer Manag Res. 2017;9:323–329. doi:10.2147/cmar.s139945
29. Baccolini V, Isonne C, Salerno C, et al. The association between adherence to cancer screening programs and health literacy: a systematic review and meta-analysis. Prev Med. 2022;155:106927. doi:10.1016/j.ypmed.2021.106927
30. Bhatia S, Landier W, Paskett ED, et al. Rural–urban disparities in cancer outcomes: opportunities for future research. JNCI J Natl Cancer Inst. 2022;114(7):940–952. doi:10.1093/jnci/djac030
31. Health literacy in healthy people 2030 - healthy people 2030 | odphp.health.gov. Available from: https://odphp.health.gov/healthypeople/priority-areas/health-literacy-healthy-people-2030.
32. Office of Disease Prevention and Health Promotion. Healthy people 2030. Available from: https://odphp.health.gov/our-work/national-health-initiatives/healthy-people/healthy-people-2030.
33. Pham R, Cross S, Fernandez B, et al. “Finding the right FIT”: rural patient preferences for Fecal Immunochemical Test (FIT) characteristics. J Am Board Fam Med. 2017;30(5):632–644. doi:10.3122/jabfm.2017.05.170151
34. Fisher JD, Fisher WA. Changing AIDS-risk behavior. Psychol Bull. 1992;111(3):455–474. doi:10.1037/0033-2909.111.3.455
35. Ghasemi M, Savabi-Esfahani M, Noroozi M, Satari M. Prediction of cervical cancer screening: application of the information-motivation-behavioral skills model. BMC Cancer. 2024;24(1):351. doi:10.1186/s12885-024-12098-9
36. Shoemaker SJ, Wolf MS, Brach C. The Patient Education Materials Assessment Tool (PEMAT) and user’s guide; 2013. Available from: https://www.ahrq.gov/sites/default/files/publications/files/pemat_guide.pdf.
37. McDonald IR, Blocker ES, Weyman EA, Smith N, Dwyer AA. What are the best practices for co-creating patient-facing educational materials? A scoping review of the literature. Healthcare. 2023;11(19):2615. doi:10.3390/healthcare11192615
38. Bashir NY, Moore JE, Buckland D, et al. Are patient education materials about cancer screening more effective when co-created with patients? A qualitative interview study and randomized controlled trial. Curr Oncol. 2019;26(2):124–136. doi:10.3747/co.26.4621
39. Morgan DL. Focus Groups. Annu Rev Sociol. 1996;22(1):129–152. doi:10.1146/annurev.soc.22.1.129
40. World Medical Association. Declaration of Helsinki – ethical principles for medical research involving human participants. World Medical Association; 1964. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki/.
41. ATLAS.ti | the #1 Software for Qualitative Data Analysis - ATLAS.ti. Available from: https://atlasti.com/?x-source=pmax&x-campaign=pmax-en&x-id=21759486841&x-term=pmax-01&utm_source=google&utm_medium=pmax&utm_campaign=21759486841&utm_term=&utm_content=&utm_adgroup=&device=c&placement=&matchtype=&network=x&gad_source=1&gad_campaignid=21759491233&gclid=Cj0KCQjwxdXBBhDEARIsAAUkP6hpe_kkfleZ-S0ARZozWN9OlMwYLboxW9A1TodvEsLhXNnHHm1g_7saAjOaEALw_wcB.
42. Saldaña JM. The Coding Manual for Qualitative Researchers.
43. Fisher JD, Fisher WA, Amico KR, Harman JJ. An information-motivation-behavioral skills model of adherence to antiretroviral therapy. Health Psychol off J Div Health Psychol Am Psychol Assoc. 2006;25(4):462–473. doi:10.1037/0278-6133.25.4.462
44. Waller J, Ostini R, Marlow LAV, McCaffery K, Zimet G. Validation of a measure of knowledge about human papillomavirus (HPV) using item response theory and classical test theory. Prev Med. 2013;56(1):35–40. doi:10.1016/j.ypmed.2012.10.028
45. Shoemaker SJ, Wolf MS, Brach C. Development of the Patient Education Materials Assessment Tool (PEMAT): a new measure of understandability and actionability for print and audiovisual patient information. Patient Educ Couns. 2014;96(3):395–403. doi:10.1016/j.pec.2014.05.027
46. Kim J, Dove MS, Dang JHT. Sociodemographic factors associated with HPV awareness/knowledge and cervical cancer screening behaviors among caregivers in the U.S. BMC Womens Health. 2022;22(1):335. doi:10.1186/s12905-022-01918-4
47. Johnson NL, Head KJ, Scott SF, Zimet GD. Persistent disparities in cervical cancer screening uptake: knowledge and sociodemographic determinants of Papanicolaou and human papillomavirus testing among women in the United States. Public Health Rep. 2020;135(4):483–491. doi:10.1177/0033354920925094
48. Thompson EL, Wheldon CW, Vamos CA, Griner SB, Daley EM. How is health literacy related to pap testing among US women? J Cancer Educ. 2019;34(4):789–795. doi:10.1007/s13187-018-1375-z
49. Best AL, Logan RG, Vázquez-Otero C, et al. Application of a health literacy framework to explore patients’ knowledge of the link between HPV and cancer. J Health Commun. 2018;23(8):695–702. doi:10.1080/10810730.2018.1508257
50. Petrik AF, Rivelli JS, Firemark AJ, et al. A qualitative assessment of the acceptability of human papillomavirus self-sampling and informational materials among diverse populations. Cancer Med. 2024;13(14):e70033. doi:10.1002/cam4.70033
51. Gautom P, Escaron AL, Garcia J, et al. Developing patient-refined colorectal cancer screening materials: application of a virtual community engagement approach. BMC Gastroenterol. 2023;23(1):179. doi:10.1186/s12876-023-02774-8
52. Thompson JH, Rivelli JS, Escaron AL, et al. Developing patient-refined messaging for follow-up colonoscopy after abnormal fecal testing in Hispanic communities: key learnings from virtual boot camp translation. Hisp Health Care Int. 2024;22(4):216–224. doi:10.1177/15404153231212659
53. Gillibrand S, Gibson H, Howells K, et al. Exploring the barriers to cervical screening and perspectives on new self-sampling methods amongst under-served groups. BMC Health Serv Res. 2025;25(1):79. doi:10.1186/s12913-024-12098-2
54. Schubbe D, Scalia P, Yen RW, et al. Using pictures to convey health information: a systematic review and meta-analysis of the effects on patient and consumer health behaviors and outcomes. Patient Educ Couns. 2020;103(10):1935–1960. doi:10.1016/j.pec.2020.04.010
55. Hennink MM, Kaiser BN, Weber MB. What influences saturation? Estimating sample sizes in focus group research. Qual Health Res. 2019;29(10):1483–1496. doi:10.1177/1049732318821692
56. Seal DW, Bogart LM, Ehrhardt AA. Small group dynamics: the utility of focus group discussions as a research method. Group Dyn Theory Res Pract. 1998;2(4):253–266. doi:10.1037/1089-2699.2.4.253
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.