Back to Journals » Patient Preference and Adherence » Volume 16
Improving Patient Adherence to Lifestyle Changes for the Management of Gastroesophageal Reflux
Authors Guadagnoli L, Simons M ![]() , McGarva J, Taft TH
, McGarva J, Taft TH ![]() , van Tilburg MAL
, van Tilburg MAL
Received 31 December 2021
Accepted for publication 19 March 2022
Published 5 April 2022 Volume 2022:16 Pages 897—909
DOI https://doi.org/10.2147/PPA.S356466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Livia Guadagnoli,1 Madison Simons,2 Josie McGarva,2 Tiffany H Taft,2 Miranda AL van Tilburg3– 5
1Department of Chronic Diseases, Metabolism, and Ageing, Laboratory for Brain-Gut Axis Studies (LABGAS), Translational Research Center for Gastrointestinal Disorders (TARGID), KU Leuven, Leuven, Belgium; 2Department of Medicine, Division of Gastroenterology and Hepatology, Northwestern University Feinberg School of Medicine, Chicago, IL, USA; 3Joan C Edwards School of Medicine, Department of Internal Medicine, Marshall University, Huntington, WV, USA; 4Department of Medicine, Division of Gastroenterology and Hepatology, University of North Carolina, Chapel Hill, NC, USA; 5School of Social Work, University of Washington, Seattle, WA, USA
Correspondence: Miranda AL van Tilburg, Email [email protected]
Abstract: Gastroesophageal reflux disease (GERD) is a common gastrointestinal illness with symptoms of heartburn, chest pain, and regurgitation. Management of GERD can involve medication use, lifestyle modification (eg, dietary modification), and surgical intervention depending on the individual patient and disease severity. Poor adherence to medication and recommended lifestyle changes may result in increased symptom severity and decreased quality of life. This paper aimed to systematically review the literature on lifestyle modification for the management of GERD. Fourteen articles were included based on search criteria. Following review and analysis, three types of lifestyle modifications were present in the literature and include medication use, dietary recommendations, and sleep recommendations. Despite being a pharmacological treatment, medication adherence was included in the review, as health behavior change can be used to improve adherence. Overall, the factors associated with adherence to modifications varied in terms of impact and directionality, depending on the type of lifestyle modification. Symptom severity emerged as important across all lifestyle modifications, and is associated with increased adherence to medication use, but decreased adherence to dietary guidelines. While patient–provider communication appeared to improve patient knowledge, it is unclear if increased knowledge translates to improved adherence. The review also demonstrated a lack of clear and standardized guidelines across lifestyle modifications, which may have an influence on adherence and adherence reporting. Future research in GERD treatment adherence would benefit from the use of validated measures to assess adherence. Specific recommendations to improving patient adherence are discussed.
Keywords: GERD, nutrition, sleep, medication, compliance
Introduction
Gastroesophageal reflux disease (GERD) is a chronic esophageal disease marked by stomach acid and other contents moving upward into the esophagus, causing symptoms including heartburn, chest pain, regurgitation, and difficulty swallowing. GERD and symptoms of gastroesophageal reflux are commonly reported in the general population. A recent study of over 70,000 people in the United States found that 44% of participants report experiencing GERD symptoms in the past, with just over 30% reporting them in the previous week.1
GERD pathophysiology is multifactorial and includes both peripheral and central mechanisms. At the level of the esophagus, dysfunction of the esophagogastric junction (eg, decreased lower esophageal sphincter pressure) and impaired esophageal clearance contribute to the presence of acid and other stomach contents refluxing into the esophagus and remaining there for longer than normal, causing GERD symptoms.2 In addition, central processes such as visceral hypersensitivity (ie, increased sensitivity to pain) can influence symptom perception, such as experiencing a benign stimulus as painful.2,3 The multifactorial pathology of GERD renders a comprehensive and individualized treatment approach that consists of medication, lifestyle modifications and, in severe cases, surgery.2,4 Proton-pump inhibitors (PPIs), which reduce gastric acid secretion, remain the first-line medical treatment for GERD.4 For lifestyle modification, American College of Gastroenterology’s 2021 Clinical Guideline for the Diagnosis and Management of GERD suggests dietary modification, smoking cessation, weight loss, avoiding excessive exercise, and changes to sleeping position.2
Despite comprehensive treatment guidelines and approaches, refractory reflux is a common enduring problem in the GERD population.5 Clinical and population-based studies have demonstrated that up to 50% of individuals continue to report GERD symptoms despite PPI use.1,6 In addition, PPI efficacy differs based on the presenting symptoms and presence or absence of esophagitis and/or abnormal endoscopic or pH-metry findings.4,7 PPI treatment for typical GERD symptoms (eg, esophagitis healing) demonstrates the highest efficacy, followed by atypical symptoms (eg, chest pain, cough), and then extra-esophageal symptoms (eg, reflux laryngitis, asthma).7
Similarly, there is a significant body of literature on the role of diet in gastroesophageal reflux, though the data does not always support the proposed dietary guidelines. For example, many providers and patients perceive certain foods to be associated with gastroesophageal reflux, including caffeine, chocolate, spicy foods, and alcohol.8 However, the data is mixed on whether consumption of these foods is truly associated with reflux symptoms.9 While some of the mechanisms for these associations are known,10 in other cases it is unclear how particular foods or drinks induce reflux. For example, some studies suggest alcohol use influences GERD through decreased lower esophageal sphincter pressure or altered gastric motility,10,11 however data is indeed mixed on if lab studies translate to clinical findings.4,10
The exact reason for refractory symptoms remains unclear and GERD symptom perception is influenced by non-reflux-based processes (eg, visceral hypersensitivity, esophageal hypervigilance),3,12 which contributes to the complexity. However, behavioral processes, such as adherence to medication and lifestyle modifications are suggested as potential mechanisms. A recent systematic review suggests a majority of patients are relatively adherent to PPI.13 However, adherence was mostly determined by the medication possession ratio (an indirect measure of adherence) and patient self-report, which has limitations.13 In addition, adherence to PPI considers more than just consistent use, it also takes into account factors such as correct dosage and timing. Indeed, PPIs are most effective when taken 30–45 minutes before a meal,4 which requires the patient to understand and take their medication accordingly. Likewise, the recommended lifestyle modifications require behavior change, which can be difficult to implement and adhere to, especially when guidelines may be unclear.
Poor adherence to medication and lifestyle modifications may result in worsening symptoms, which can negatively influence quality of life.14 The benefits of medication adherence extend beyond symptom severity to diminished healthcare utilization. Gosselin et al evaluated the relationship between PPI adherence and healthcare utilization and costs in patients with GERD and found that increased adherence resulted in decreased healthcare utilization, including fewer emergency room visits, inpatient visits, and the number of hospitalization days, as well as decreased total annual healthcare costs.
Thus, it is important to evaluate factors associated with treatment adherence to more effectively intervene and improve overall disease experience. The current study sought to systematically review the literature on adherence to lifestyle modification for the management of GERD. Specific recommendations for improvement to treatment adherence are provided.
Methods
The following electronic databases were searched: EMBASE and PubMed in August 2021. Detailed information about the keyword searches used are described in Supplementary Item 1. We retrieved articles based on available subject headings and keywords in both databases and duplicates were removed. The reference lists of articles selected for full-text review were manually screened for additional articles.
The search was limited to peer-reviewed original studies published in English. Conference proceedings and review articles were excluded. In this search, the population of interest was adults diagnosed with GERD; studies were excluded if GERD symptoms were a secondary outcome or not the target population (eg GERD symptoms among people with obesity). We did not restrict by date of publication to ensure that all available sources were included in the results. Studies including patients with laryngopharyngeal reflux were also included, as it was determined lifestyle modifications and recommendations would likely be similar to those of GERD.
Our initial searches retrieved 154 results, of which we excluded 112 based on title and abstract review. We reviewed 42 full-text articles and, based on the exclusion criteria described above, were left with 14 articles that were appropriate for inclusion. Included articles were reviewed and analyzed based on modification type (Figure 1). Three types of lifestyle modifications were present and included adherence related to medication use, dietary recommendations, and sleep recommendations. Despite being a pharmacological treatment, medication use was included as a lifestyle modification, as health behavior change can improve medication use as well as other non-pharmacological treatments such as diet and sleep. Table 1 provides a list of the articles included in this review.
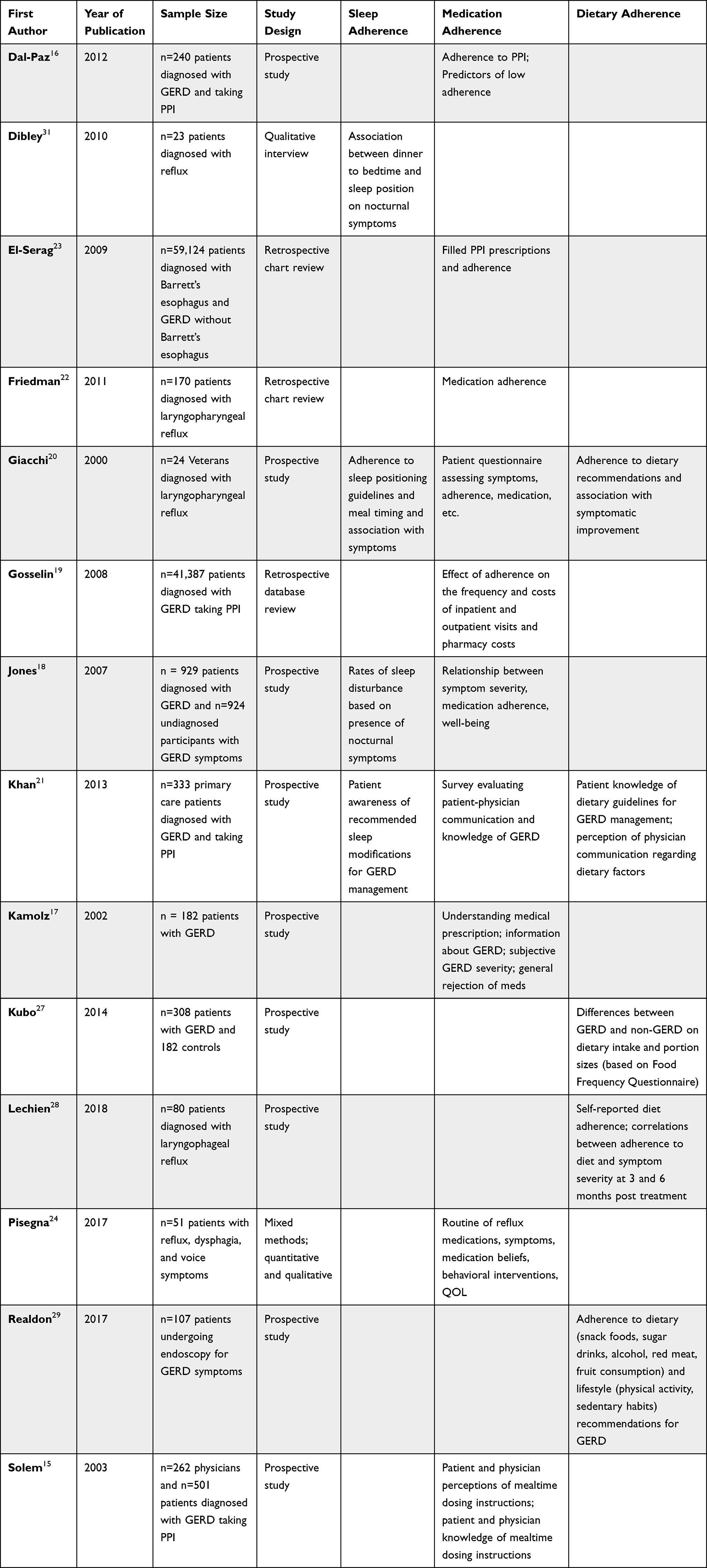 |
Table 1 Characteristics of Included Studies |
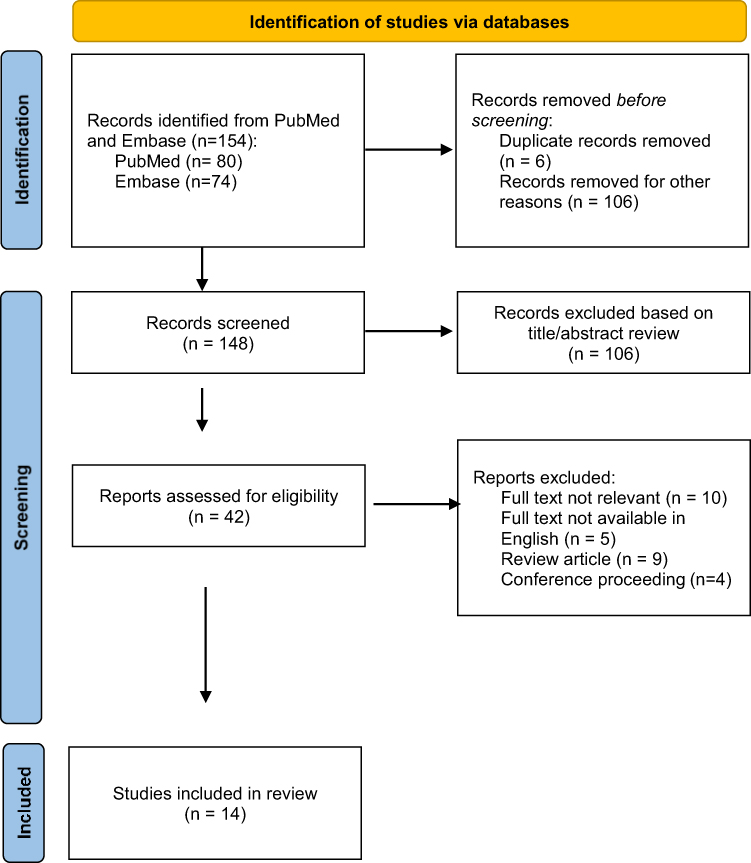 |
Figure 1 PRISMA.37 Diagram reflecting article review process. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.37 |
Risk of Bias
The included studies were examined for risk of bias. The main factors assessed were the representativeness of the source population, response rate for the study, presence of missing data, the clinical sensibility of the survey (s), and psychometric validity of surveys used. Unfortunately, 13 of the 14 included studies are at high risk of bias based on the psychometric validity of the survey instruments used, as all but one study relied on unvalidated study specific questionnaires to assess adherence to lifestyle recommendations for GERD management. These questionnaires were specifically designed to assess adherence to behaviors that have been traditionally associated with management of GERD symptoms, so participants may have been more likely to over-estimate adherence to lifestyle modification. No study included daily dairies or other methods that control for recall overestimation. We proceeded with the review, despite the included studies being at high risk of bias, to highlight the need for more rigorous research on lifestyle modification adherence for GERD management.
Results
Medication Adherence
Overview of Medication Adherence Studies
Ten studies evaluated medication adherence.15–20 Eight out of ten studies specifically focused on adherence to PPI,15,16,18,19,21–24 while the others either included medications in addition to PPI20 or evaluated adherence to medications more broadly.17 In terms of study population, two studies were specifically interested in the laryngopharyngeal reflux population,20,22 two studies included GERD with comorbid disorders (eg, laryngopharyngeal reflux, Barrett’s esophagus),23,24 and the remainder specifically evaluated GERD patients.
Methods of Assessment
Half of the studies included used questionnaire or survey-based approaches to assess medication adherence. However, the type and purpose of the questionnaire varied significantly between studies. Morisky et al was the only study to use a validated questionnaire, the Morisky Medication Adherence Scale,25 to evaluate medication adherence. All others used self-made questionnaires or surveys with self-reported adherence.15,18,20,21 In addition, El-Serag et al assessed adherence based on patient interviews, and Gosselin et al determined adherence by patient-report at follow up visit. Two studies measured adherence through behavioral data, such as PPI prescriptions filled23 and the medication possession ratio.19
Medication Adherence Rates
Six articles summarized rates of adherence to medication in patients with GERD and found rates of partial to total adherence to be moderate-high, ranging from 50–93% depending on the study.15–18,20 However, it is important these numbers are interpreted with caution, as each study imposed different methodology to define and assess medication adherence. In two studies, patients were stratified into groups based on self-reported adherence. Dal-Paz et al grouped 240 patients diagnosed with GERD prescribed a PPI (omeprazole) into “low adherence” and “high adherence” groups based off of the Morisky Medication Adherence Scale25 and found that 52.2% of patients with GERD were considered highly adherent, while 47.5% had low adherence to medication. Similarly, Kamolz (2002) grouped 182 patients diagnosed with GERD into total (39% of the sample), partial (36%), and non-compliant (25%) groups based on their subjective response to a standardized phrase. Other studies applied questionnaires to assess if and the frequency with which patients take medication as directed/prescribed. Responses ranged from 50% reporting taking medication as prescribed,20 71% indicating “usually” or “always” taking medication per the product label,18 and 93% taking PPI as directed “most of the time” or “always” over a period of one month.15
Effects of Medication Adherence on Symptoms
In relation to GERD symptoms, multiple studies suggest increased medication adherence is associated with decreased disease severity16,24 and symptom improvement or reduction.17,18,20 Specifically, Kamolz found that 11% of responders in the “totally compliant” group reported experiencing persistent GERD symptoms, compared to 57% and 80% in the “partial compliance” and “non-compliance” groups, respectively. In another study, over half of respondents treated with medication continued to experience breakthrough symptoms “some of the time,” but self-reported decreased symptom severity when on their PPI.24 However, when the authors evaluated the Reflux Symptom Index26 to assess symptom severity, it did not significantly differ by adherence group (adherence vs non-adherent). Disease duration is also an important factor to consider, as longer disease duration and length of time GERD medications have been prescribed was associated with improved medication adherence in two studies.17,23
Demographic and Clinical Characteristics of Improved Medication Adherence
Four articles assessed the relationship between age and adherence and all found that older age was associated with higher adherence rates.16,17,19,23 Being unmarried16 and identifying as female17 was also associated with improved adherence. Additional clinical considerations associated with improved medication adherence include the presence of Barrett’s Esophagus,23 concomitant H2RA use,23 undergoing 24-hour pH monitoring,22 as well as higher reports of sleeplessness, chronic pain, and other comorbidities.19
Perceptions of Medication
Patient and physician perceptions about GERD and pharmacological treatment can also be a factor impacting medication adherence. One study found that patients do not perceive taking a PPI as inconvenient, which is contrary to physicians’ perceptions of PPIs as being inconvenient for patients.15 However, both felt taking a PPI as directed is “important.” Additionally, two studies found that patients believe adherence to medications results in decreased symptoms.15,24 Interestingly, despite the perceptions of medications as both important and beneficial, one study found that only 35% of patients report feeling “very satisfied” with their treatment.18
Kamolz evaluated factors associated with GERD medication adherence. In the total compliance group, perceiving high levels of symptom and disease severity were major factors contributing to adherence, while perceiving low-levels of symptom and disease-severity was a major factor in the partial compliance and non-compliance groups. In addition, a general rejection of drugs (ie, “In general, I do not like to take any medication at all”) was reported by 21% of patients in the partial compliance group and 80% of patients in the non-compliance group.
Education and Patient Knowledge of Medication
Several studies evaluated patient’s knowledge of GERD medication and usage, such as the name of the medication, instructions on how to take the medication, and medication routine. In one study, 60.8% of GERD patients were unaware of the name of the disease, and approximately 35% of patients did not take their PPI correctly.16 This is similar to a mixed-methods study, which found that 17.6% of participants reported being unable to identify the pill that is their reflux medication, and when describing their medication routine, over two-thirds of participants reported a medication routine that is incorrect compared to the product label instructions.24 The three behaviors most associated with incorrect routines in this study include taking the medication in the morning with no attention to the mealtime dosing (ie, 30 minutes before a meal), taking it alongside other medication, and taking it after meals after symptom onset.
Solem et al evaluated the prescribing physician’s knowledge of GERD medication and found that up to 65% of physicians report incorrect mealtime-related dosing directions for PPI use. It should be noted, the number of physicians reporting incorrect/unsure directions varies (29–65%) depending on the type of PPI, and includes both primary care physicians and gastroenterologists. When broken down by physician-type, gastroenterologists report more correct directions and feeling less “unsure” of the directions compared to primary care physicians. This translated to the findings that over a third of patients with mealtime-related directions and 82% of patients on PPI’s without mealtime-related directions received instructions from their prescribing physicians that were incorrect or inconsistent with the product instructions.
Dietary Adherence
Overview of Dietary Adherence
Five of the included studies measured adherence to dietary recommendations for GERD management.20,21,27–29 Although the dietary and eating behavior recommendations were similar across the studies, they were not homogeneous and in some cases there was room for patient interpretation, particularly around the type of foods that would fall into a particular food group.
The guidelines assessed in these studies typically included avoidance of dietary triggers associated with GERD symptoms and avoiding eating or drinking for some time interval prior to bed. Four of the five studies provided clear information about what was being assessed with respect to avoidance of foods traditionally associated with GERD symptoms. The most commonly assessed triggers included caffeine,20,21,27 alcohol,20,21,27,29 and fatty foods,20,27,29 though citrus21,27 and dairy20,21 were also included in two studies. In one study,28 the authors indicated participants were given individualized dietary recommendations based on Koufman’s low acid-diet for laryngopharyngeal reflux but these guidelines were not specified and did not appear to be consistent across participants.30
Two studies specifically assessed adherence to eating behaviors including avoiding eating or drinking before bed.20,21 However, the time between eating and bed differed between the two studies with one inquiring about eating two hours before bed20 and the other inquiring about eating four hours before bed.21
Methods of Assessment
Four of the five studies were cross-sectional in design,20,21,27,29 and just one included follow up assessments at three and six months.28 Researchers measured adherence to dietary recommendations using self-report, study-specific questionnaires that differed in content and depth, so it is difficult to draw conclusions across studies. In each study, participants recorded how often or to what degree they engaged in various behaviors, such as avoiding dietary triggers or modifying their eating behaviors. In four of the five studies, participants rated adherence to specific dietary recommendations for GERD management (where only GERD related behaviors were assessed); in the other, authors used a Food Frequency Questionnaire to assess dietary patterns over the last year and compared these with healthy controls.27
Dietary Adherence Rates
Across the studies, adherence to dietary recommendations was not typically reported as a percentage or value, except in one case, where participants self-reported their adherence to dietary recommendations to be 6.42/10, with 10 being fully adherent to the recommendations.28 In their study involving Veterans diagnosed with laryngopharyngeal reflux (n=24), Giacchi et al found that adherence with dietary recommendations (including avoidance of dairy, fatty food, caffeine, and alcohol) was higher than for sleeping position or medication, though this was not necessarily correlated with significant improvement in symptoms (r=0.2674).20 This finding was corroborated by Realdon et al,29 who found adherence to lifestyle modifications for GERD symptoms was highest around recommendations for snack foods, sugar drinks, and limiting alcohol across varying degrees of disease severity in patients undergoing endoscopy for GERD symptoms (n=107). In this study, disease progression was associated with less adherence to guidelines on physical activity, sedentary habits, consumption of fruit, and consumption of processed meat.29
Effects of Dietary Adherence on Symptoms
The data on effects of adherence on symptom improvement is mixed. With respect to laryngopharyngeal symptoms of reflux, there was not a significant association between avoidance of fatty food (r=0.11), caffeine (r=0.21), alcoholic beverages (r=0.12), or dairy (r=0.21) on symptomatic improvement, though this was in a small entirely male sample.20 Compared to healthy controls, patients with moderate to severe GERD symptoms were more likely to consume soft drinks, one or more cups of tea per day, fried foods, and foods high in fat, and they were less likely to consume citrus fruits and alcoholic beverages based on their responses to a Food Frequency Questionnaire.27 In this same study, severity and frequency of GERD symptoms were not associated with portion sizes, coffee consumption, or tomato consumption.27 Lechien et al were the only study to report longitudinally that self-reported adherence to dietary recommendations, which again were unspecified, contributed to improvements in symptom severity and pyrosis score at three months.28 Within a small male Veteran sample, not eating or drinking in the 2–3 hours leading up to bedtime was moderately correlated with symptomatic improvement (r=0.48; p<0.05).20
An in-depth conversation with a primary care physician was associated with increased knowledge of GERD symptoms and management.21 Patients who had an in-depth conversation were more likely to report knowledge that GERD could be managed via lifestyle modification (53% compared to 23%; p<0.001), but overall knowledge around dietary recommendations remained low across the entire sample (18%).21 However, this study did not assess whether improvements in knowledge of the condition or its management was associated with improved adherence to lifestyle recommendations.
Sleep
Overview of Sleep Modification Adherence
Disruption to sleep due to nocturnal symptoms and the impact on QoL are frequent complaints from patients with GERD.18,19 Modifications surrounding sleeping position20,21,24 and time between meals and bed20,31 are common recommendations given by providers. For the purpose of this review, no studies specifically measured adherence to sleep modifications. However, sleep and sleep-related behaviors were discussed in four of the included articles18,20,21,31 with mixed findings, as each study assessed and viewed sleep using different methodology.
Recommended lifestyle modifications related to sleep are specific and require patient education to implement. Increasing the time between last meal and bed, known as the dinner to bed time (DTBT) window, is a common modification and was discussed by two of the included articles20,31 Both of the studies discussing DTBT found that waiting less than 2–3 hours between eating and sleep led to increased nocturnal symptoms, increased tiredness throughout the day and decreased QoL.20,31 Sleep position (head of the bed, including torso, raised 9 inches) is another recommended modification that demonstrates a decrease in nocturnal symptoms,20,21,24 however, only 33% of surveyed patients were aware of this modification and its benefits.21
Methods of Assessment
All four of the studies were cross-sectional designs.18,20,21,31 Questionnaires were used in two studies, one evaluating the impact of lifestyle modifications (including sleep) on laryngopharyngeal reflux symptoms,20 while the other assessed the relationship between GERD symptoms and sleep disturbances.18 In both cases, the questionnaire used was not validated. One study included a structured interview to examine their perceptions of lifestyle modifications on GERD symptoms.31 The fourth study surveyed patients education and understanding of lifestyle modifications and recommendations by providing a multiple-choice quiz with a question asking the best position to sleep in.21
Effect of Sleep and Sleep Modification on Symptoms
In a structured interview with 23 GERD patients, Dibley et al suggested a common theme of time between the last meal and its impact on nocturnal symptoms. Fourteen participants noticed a difference in symptoms when engaging in a DTBT window. Three of these patients ignored DTBT recommendations but adhered to a change in sleep position and therefore did not experience nocturnal symptoms. Three patients ignored DTBT recommendations and sleep position modifications, experiencing nighttime symptoms. The additional eight patients adhered to elongated DTBT windows to avoid previously experienced symptoms while sleeping. Similarly, another study found that avoiding eating close to bedtime (2 hours or less) and elevating the head of the bed had the most significant influence on laryngopharyngeal reflux symptoms, even more than medication adherence or changes in diet, especially when combined.20
In Jones et al sleep disturbances related to GERD symptoms were indicated in 48–55% of participants, resulting in patients awakening on average 3 times per week for over an hour at each occurrence. This varied by PPI medication response. Of patients taking PPI’s, complete responders to the medication had no sleep disturbances caused by symptoms, while more than 50% of those who were non-responders reported sleep disturbances due to nocturnal symptoms. The study participants reported decreased work and leisure time which the authors attributed to symptom-induced sleep disturbances.
Education and Patient Knowledge of Sleep Modifications
In a prospective study surveying patient education and understanding of lifestyle modifications and recommendations, patients were given a multiple-choice quiz with a question asking the best position to sleep in.21 An average of 33% of participants gave the correct answer - with the head of the bed, including the torso, raised 9 inches. This study demonstrated the lack of knowledge patients have surrounding their diagnosis but did not study the number of patients making these modifications or the effect of them on symptoms.
Discussion
The current study reviewed the literature in adherence to lifestyle modifications in patients with GERD and reflux-related symptoms.
A common theme discussed throughout the studies was the impact of medication adherence on GERD symptoms. Medication adherence was associated with decreased disease severity16,24 and symptom improvement or reduction17,18,20 in several studies. However, the directional relationship between PPI/medication use and symptom severity is unclear and results in these questions – does low medication adherence lead to more severe GERD symptoms, or does increased symptom severity drive non-adherence, as patients may perceive the treatment as not effective? Studies included in this review suggest that GERD patients perceive adherence to GERD medication, including taking the medication as directed, as important and effective in decreasing symptoms.15,24 In addition, disease severity might encourage adherence behavior, as the patients who were more adherent to medication were those who perceived higher disease severity, and less disease severity was a major factor contributing to partial or non-adherence.17
Adherence to dietary recommendations may be higher than other lifestyle modifications but it remains undetermined whether this actually translates to change in physical symptoms. Dietary modification often represents one of the first strategies people use when experiencing chronic gastrointestinal symptoms, though based on these studies it is unclear this is an effective strategy. Certain behaviors are associated with more frequent or severe symptoms, such as consumption of fried/fatty foods, soft drinks, and tea; however, this was not demonstrated with other dietary patterns that have typically been associated with GERD symptoms such as citrus consumption.
In terms of the sleep literature, adhering to sleep modifications is a predictor of decreased symptoms24 and increased QoL31 due to better rest, independent of weight loss24 and adherence to medication.18 Thus, adapting to sleep modifications may be an important predictor of increased QoL. It has been observed that, in general, adherence to medications in chronic illness populations is alarmingly low, with those with sleep disorders ranking lower than the general chronic illness population.22 This could be an important consideration when prescribing sleep modifications to GERD patients, who have a chronic illness that impacts sleep. Medication and lifestyle modifications could be less likely to be adhered to without the proper education from healthcare professionals.
In terms of patient knowledge and education, patients had a moderate level of awareness that GERD symptoms could be managed via dietary or lifestyle modification, but a very low percentage of patients had knowledge around specific dietary or sleep guidelines for GERD management. This may represent an overall low health literacy within this population or the convoluted nature of nutrition education and language. Notably, the language used to define foods high in fat differed across studies, which may lead to differences in how participants interpret the guideline. Terms used to describe this group of foods ranged from “fried foods” to “energy dense foods” and “fatty foods.” Without a basic understanding of the macronutrient properties of foods, patients could understandably have significant confusion around how to organize their diets in a way that adheres to nutritional guidelines.
For medication adherence, several studies suggested gaps in knowledge regarding GERD medication and usage that may impact adherence.16,24 In addition, studies evaluating the prescribing physician’s knowledge of GERD medication revealed that providers, especially in primary care, provide incorrect instructions.15 This is significant, as GERD is commonly diagnosed and treated in the context of primary care settings.6 Improving adherence can start with identifying behaviors associated with incorrect routines and developing targets for behavior change. For example, if a patient reports taking their PPI after symptom onset (as opposed to 30 minutes before a meal), a provider can work with them to 1) provide accurate education, and 2) identify barriers to proper adherence (eg, they forget to take the PPI until they notice symptoms), and 3) implement a behavioral strategy to improve adherence (eg, setting alarm on phone to remind before meal time).
This review highlighted that in-depth conversations with a physician led to increased knowledge around GERD management. Engaging in in-depth physician-patient conversations is associated with increased patient education, including knowing the best time to take anti-reflux medications as well as knowledge about the beneficial effects of lifestyle modifications on symptom and disease severity.21 However, it was not assessed whether increased knowledge translated to improved adherence and subsequent symptom management.
One aspect unique to medication adherence is a patient’s attitude toward medication use. One study demonstrated that a general rejection of medication was evident in the majority of patients non-adherent to their GERD medication.17 If symptoms can be managed without medication, providers should work with patients to develop a treatment plan that is most consistent with their preferences. However, if medication is clinically indicated, providers should engage in a patient-focused conversation to discuss the patients’ concerns about medication use.
Strategies for Improving Adherence
Prior research on behavior change has consistently demonstrated that behavior change is not driven by increased education around a topic but is more often predicted by patient motivation for change.32 In other disease groups, behavioral interventions, such as self-monitoring or cognitive restructuring, are effective at improving adherence to lifestyle modification.33 For example, providers may ask patients to begin tracking their food and beverage intake, sleep habits, or medication use to help build awareness of how these factors uniquely impact their symptoms. It may also be appropriate to refer patients to providers trained in health behavior change, such as health psychologists or those specifically trained in gastroenterology, to help facilitate lifestyle modification for GERD management. These providers may address behaviors and cognitions that may interfere with behavior change.
Patients will also likely benefit from increased conversation around their condition and its management with their healthcare providers. During these conversations, the use of Motivational Interviewing techniques to identify patient values/motivation for change, establish specific goals around reflux management, and explore potential barriers for change would likely produce the greatest likelihood of behavior change compared to information giving.32,34 Discussion of barriers to change should take into account social, cognitive, financial, and treatment-related factors that may impact a patient’s ability to implement behavior change, and include support for problem solving around these barriers.35 For example, finding ways to simplify the patient’s medication regimen is likely to improve adherence (eg, reducing number of doses per day when possible, using medications that require the least restrictions around dose timing, etc.).34,36 Table 2 provides suggestions on language providers may use to help engage patients in conversations regarding their GERD management. Behavior change is likely to be most successful when the plan for care is individualized based on the patient’s time, values, and resources; thus, spending the time to identify these factors early on in treatment will facilitate improved behavioral modification.
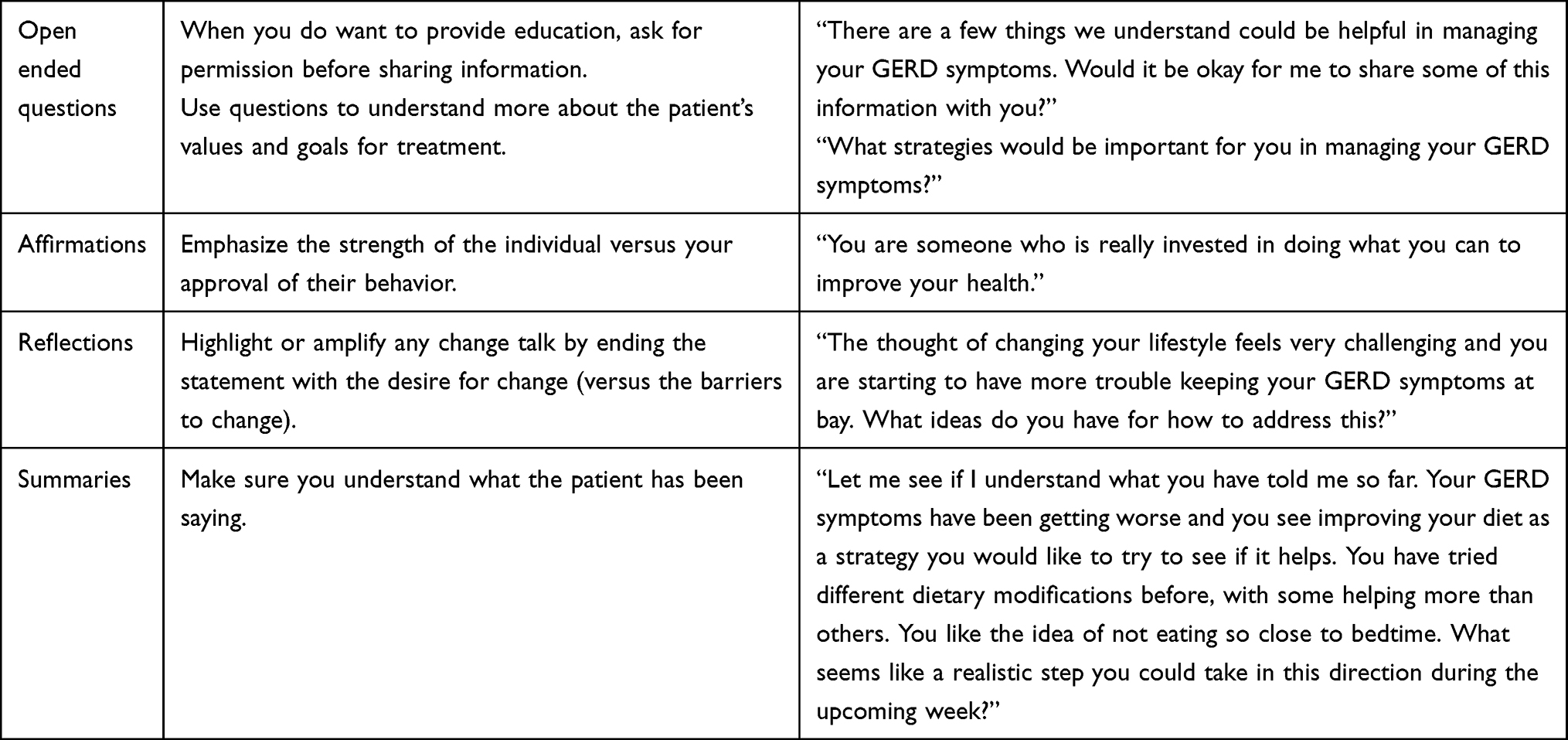 |
Table 2 Examples of Language Providers May Use to Facilitate Behavior Change |
Conclusion
Factors associated with increased adherence to lifestyle modification for GERD were variable. Symptom severity was positively correlated with adherence to PPI use but negatively correlated with adherence to dietary guidelines. In-depth conversations with providers seemed to improve patient knowledge around lifestyle modifications for GERD management; however, it remains to be tested whether this knowledge contributes to greater adherence to modifications. This review highlights one of the primary barriers to adherence to lifestyle modification for GERD management, whether that is medication use, dietary advice, or altered sleep habits, may be lack of clear and standardized guidelines. However, even with the correct information, it is unclear whether adherence to the guidelines translates to improved symptom management. Future research on adherence to lifestyle modifications would benefit from the use of validated measures of adherence and evaluation of the association between knowledge, adherence, and symptom severity, particularly for dietary and sleep recommendations. We recommend providers engage patients in conversations around their values associated with lifestyle management of GERD symptoms to facilitate the greatest likelihood of behavior change. Other cognitive and behavioral strategies demonstrated to be effective in behavior modification are also likely to be helpful for GERD management including self-monitoring, cognitive restructuring, and goal setting and problem solving.
Author Contributions
Miranda van Tilburg, PhD is guarantor of the article. MS, LG, and JG contributed to the design and preparation of the manuscript. TT and MVT contributed to the interpretation and substantial revision of the manuscript.
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Tiffany Taft is supported by an NIDDK Grant (No. P01DK117824/DK/NIDDK). Livia Guadagnoli is a postdoctoral Research Fellow of the Research Foundation Flanders (FWO, 12A7822N).
Disclosure
Tiffany Taft has 100% ownership in Oak Park Behavioral Medicine LLC. Miranda van Tilburg is a consultant for Mahana Therapeutics Inc and received personal fees from IQVIA. The authors report no other conflicts of interest in this work.
References
1. Delshad SD, Almario CV, Chey WD, Spiegel BMR. Prevalence of gastroesophageal reflux disease and proton pump inhibitor-refractory symptoms. Gastroenterology. 2020;158(5):1250–1261.e2. doi:10.1053/j.gastro.2019.12.014
2. Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2021. doi:10.14309/ajg.0000000000001538
3. Weijenborg PW, Smout AJ, Verseijden C, et al. Hypersensitivity to acid is associated with impaired esophageal mucosal integrity in patients with gastroesophageal reflux disease with and without esophagitis. Am J Physiol Gastrointest Liver Physiol. 2014;307(3):G323–9. doi:10.1152/ajpgi.00345.2013
4. Gyawali CP, Fass R. Management of gastroesophageal reflux disease. Gastroenterology. 2018;154(2):302–318. doi:10.1053/j.gastro.2017.07.049
5. Kahrilas PJ, Keefer L, Pandolfino JE. Patients with refractory reflux symptoms: what do they have and how should they be managed? Neurogastroenterol Motil. 2015;27(9):1195–1201. doi:10.1111/nmo.12644
6. El-Serag H, Becher A, Jones R. Systematic review: persistent reflux symptoms on proton pump inhibitor therapy in primary care and community studies. Aliment Pharmacol Ther. 2010;32(6):720–737. doi:10.1111/j.1365-2036.2010.04406.x
7. Katzka DA, Pandolfino JE, Kahrilas PJ. Phenotypes of gastroesophageal reflux disease: where Rome, Lyon, and Montreal meet. Clin Gastroenterol Hepatol. 2020;18(4):767–776. doi:10.1016/j.cgh.2019.07.015
8. Surdea-Blaga T, Negrutiu DE, Palage M, Dumitrascu DL. Food and gastroesophageal reflux disease. Curr Med Chem. 2019;26(19):3497–3511. doi:10.2174/0929867324666170515123807
9. Wang SE, Hodge AM, Dashti SG, et al. Diet and risk of gastro-oesophageal reflux disease in the Melbourne Collaborative Cohort Study. Public Health Nutr. 2021;24(15):5034–5046. doi:10.1017/s1368980021000197
10. Newberry C, Lynch K. The role of diet in the development and management of gastroesophageal reflux disease: why we feel the burn. J Thorac Dis. 2019;11(Suppl 12):S1594–s1601. doi:10.21037/jtd.2019.06.42
11. Castell DO, Murray JA, Tutuian R, Orlando RC, Arnold R. Review article: the pathophysiology of gastro-oesophageal reflux disease - oesophageal manifestations. Aliment Pharmacol Ther. 2004;20(Suppl 9):14–25. doi:10.1111/j.1365-2036.2004.02238.x
12. Guadagnoli L, Yadlapati R, Taft T, Pandolfino JE, Tye M, Keefer L. Esophageal hypervigilance is prevalent across gastroesophageal reflux disease presentations. Neurogastroenterol Motil. 2021;33(8):e14081. doi:10.1111/nmo.14081
13. Hungin APS, Hill C, Molloy–Bland M, Raghunath A. Systematic review: patterns of proton pump inhibitor use and adherence in gastroesophageal reflux disease. Clin Gastroenterol Hepatol. 2012;10(2):109–116. doi:10.1016/j.cgh.2011.07.008
14. Liker HR, Ducrotté P, Malfertheiner P. Unmet medical needs among patients with gastroesophageal reflux disease: a foundation for improving management in primary care. Dig Dis. 2009;27(1):62–67. doi:10.1159/000210106
15. Solem C, Mody R, Stephens J, Macahilig C, Gao X. Mealtime-related dosing directions for proton-pump inhibitors in gastroesophageal reflux disease: physician knowledge, patient adherence. J Am Pharm Assoc. 2014;54(2):144–153. doi:10.1331/JAPhA.2014.13117
16. Dal-Paz K, Moraes-Filho JP, Navarro-Rodriguez T, Eisig JN, Barbuti R, Quigley EM. Low levels of adherence with proton pump inhibitor therapy contribute to therapeutic failure in gastroesophageal reflux disease. Dis Esophagus. 2012;25(2):107–113. doi:10.1111/j.1442-2050.2011.01227.x
17. Kamolz T. Analysis of medical compliance in gastro-oesophageal reflux disease patients referred to pre-surgical examination. Dig Liver Dis. 2002;34(3):183–189. doi:10.1016/s1590-8658(02)80191-8
18. Jones R, Liker HR, Ducrotté P. Relationship between symptoms, subjective well-being and medication use in gastro-oesophageal reflux disease. Int J Clin Pract. 2007;61(8):1301–1307. doi:10.1111/j.1742-1241.2007.01475.x
19. Gosselin A, Luo R, Lohoues H, et al. The impact of proton pump inhibitor compliance on health-care resource utilization and costs in patients with gastroesophageal reflux disease. Value Health. 2009;12(1):34–39. doi:10.1111/j.1524-4733.2008.00399.x
20. Giacchi RJ, Sullivan D, Rothstein SG. Compliance with anti-reflux therapy in patients with otolaryngologic manifestations of gastroesophageal reflux disease. Laryngoscope. 2000;110(1):19–22. doi:10.1097/00005537-200001000-00004
21. Khan N, Bukhari S, Lakha A, et al. Gastroesophageal reflux disease: the case for improving patient education in primary care. J Fam Pract. 2013;62(12):719–725.
22. Friedman M, Maley A, Kelley K, et al. Impact of pH monitoring on laryngopharyngeal reflux treatment: improved compliance and symptom resolution. Otolaryngol Head Neck Surg. 2011;144(4):558–562. doi:10.1177/0194599811399240
23. El-Serag HB, Fitzgerald S, Richardson P. The extent and determinants of prescribing and adherence with acid-reducing medications: a national claims database study. Am J Gastroenterol. 2009;104(9):2161–2167. doi:10.1038/ajg.2009.312
24. Pisegna JM, Yang S, Purcell A, Rubio A. A mixed-methods study of patient views on reflux symptoms and medication routines. J Voice. 2017;31(3):
25. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. doi:10.1097/00005650-198601000-00007
26. Belafsky PC, Postma GN, Koufman JA. Validity and reliability of the reflux symptom index (RSI). J Voice. 2002;16(2):274–277. doi:10.1016/s0892-1997(02)00097-8
27. Kubo A, Block G, Quesenberry CP
28. Lechien JR, Finck C, Huet K, et al. Impact of laryngopharyngeal reflux on subjective, aerodynamic, and acoustic voice assessments of responder and nonresponder patients. J Voice. 2019;33(6):929–939. doi:10.1016/j.jvoice.2018.05.014
29. Realdon S, Antonello A, Arcidiacono D, et al. Adherence to WCRF/AICR lifestyle recommendations for cancer prevention and the risk of Barrett’s esophagus onset and evolution to esophageal adenocarcinoma: results from a pilot study in a high-risk population. Eur J Nutr. 2016;55(4):1563–1571. doi:10.1007/s00394-015-0975-1
30. Koufman JA. Low-acid diet for recalcitrant laryngopharyngeal reflux: therapeutic benefits and their implications. Ann Otol Rhinol Laryngol. 2011;120(5):281–287. doi:10.1177/000348941112000501
31. Dibley LB, Norton C, Jones R. Don’t eat tomatoes: patient’s self-reported experiences of causes of symptoms in gastro-oesophageal reflux disease. Fam Pract. 2010;27(4):410–417. doi:10.1093/fampra/cmq020
32. Rosengren DB. Building Motivational Interviewing Skills: A Practitioner Workbook. Applications of Motivational Interviewing. Guilford Publications; 2009.
33. Burgess E, Hassmén P, Welvaert M, Pumpa KL. Behavioural treatment strategies improve adherence to lifestyle intervention programmes in adults with obesity: a systematic review and meta-analysis. Clin Obes. 2017;7(2):105–114. doi:10.1111/cob.12180
34. Izeogu C, Kalinowski J, Schoenthaler A. Strategies to improve adherence to anti-hypertensive medications: a narrative review. Curr Hypertens Rep. 2020;22(12):105. doi:10.1007/s11906-020-01115-4
35. Laba TL, Bleasel J, Brien JA, et al. Strategies to improve adherence to medications for cardiovascular diseases in socioeconomically disadvantaged populations: a systematic review. Int J Cardiol. 2013;167(6):2430–2440. doi:10.1016/j.ijcard.2013.01.049
36. Kane SV. Strategies to improve adherence and outcomes in patients with ulcerative colitis. Drugs. 2008;68(18):2601–2609. doi:10.2165/0003495-200868180-00006
37. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71–n71. doi:10.1136/bmj.n71
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.