Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Improving Influenza Vaccination Coverage Among Patients With COPD: A Pilot Project
Authors Li A, Chan YH, Liew MF, Pandey R ![]() , Phua J
, Phua J
Received 9 July 2019
Accepted for publication 31 October 2019
Published 15 November 2019 Volume 2019:14 Pages 2527—2533
DOI https://doi.org/10.2147/COPD.S222524
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Andrew Li,1 Yiong-Huak Chan,2 Mei Fong Liew,1,3 Rakshya Pandey,4 Jason Phua1,3
1Division of Respiratory and Critical Care Medicine, University Medicine Cluster, National University Hospital, National University Health System, Singapore; 2Biostatistics Unit, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 3Fast and Chronic Programmes, Alexandra Hospital, National University Health System, Singapore; 4Department of Respiratory Medicine, Ng Teng Fong General Hospital, National University Health System, Singapore
Correspondence: Andrew Li
Yong Loo Lin School of Medicine, National University of Singapore Division of Respiratory and Critical Care Medicine, National University Hospital, NUHS Tower Block, Level 10 5 Lower Kent Ridge Road, 119228 Singapore
Email [email protected]
Background and objective: Guidelines for chronic obstructive pulmonary disease (COPD) advocate regular influenza vaccination, which has been shown to reduce exacerbations. However, influenza vaccination rates remain low. This quality improvement project was initiated to help improve influenza vaccination rates in a tertiary hospital.
Methods: All patients with COPD in the airway program (TAP) in the National University Hospital at the end of 2013 were recruited. The interventions were implemented in 2014; thus, population was stratified into the pre-intervention group and post-intervention group. Those who died in 2014 were excluded. They were (1) patient education posters in the clinics on the need for regular influenza vaccination, (2) direct interventions by physicians, and (3) intervention by the nurses when vaccinations were neglected. Physicians were made aware of previous vaccination rates, vaccination card reminders were placed in the clinics, and a new electronic healthcare record system (EHR) was implemented. The patients were followed up till the end of 2015 or until death. When an influenza vaccination was administered, the patients were asked which of the interventions led to the vaccination. A questionnaire was delivered to the physicians to determine the interventions that led to any change in vaccination prescription practices.
Results: The pre-intervention influenza vaccination rate was low at 47.7%. The post-intervention influenza vaccination rate improved to 80.7% with the multi-pronged approach. Physicians initiated the majority of vaccinations (87.9%), while nurses helped intervene in a further 12.1%. Physicians’ vaccination prescription practices changed as a result of self-awareness of low vaccination rates, vaccination card reminders, and the new EHR. Patient education made minimal impact.
Conclusion: This project demonstrates that with regular audits to track progress and several easy-to-implement interventions, improving influenza vaccination rates is an achievable goal.
Keywords: influenza vaccination, quality improvement project, COPD
Introduction
Chronic obstructive pulmonary disease (COPD) remains a significant public health problem,1 with exacerbations being one of the leading causes of hospitalisations in many countries. The impact of COPD exacerbations is far-reaching and includes accelerated lung function decline,2,3 impaired quality of life,4 and mortality rates of up to 20%.5 Every COPD exacerbation also portends an increased risk of future exacerbations.6 The majority of infective COPD exacerbations have been attributed to viral infections,7,8 of which the most common are influenza virus, rhinovirus and respiratory syncytial virus.8 Patients with viral-induced exacerbations tend to be more symptomatic and require a longer recovery time.9
Prevention is better than cure. This has led to the recommendation of regular annual influenza vaccinations for patients with COPD.10 Influenza vaccinations can reduce influenza-related exacerbations, total number of exacerbations and death.11–13 National-based initiatives such as the Healthy People 2020 initiative in the USA had targeted a 70% influenza vaccination coverage among the general population.14 However, the actual take-up rate has consistently been dismally low at 20–60%.15–18 In Singapore, more than 88% of the patients with COPD did not receive their influenza vaccination within the last year.18 There are many barriers to improving these rates, including undervaluation of vaccination, lack of awareness, costs, lack of adequate health resources, infrastructure and reduced accessibility to vaccines.19–22 Programmes to improve vaccination rates in adults in various settings, ranging from community-based practices, family physician practices to public hospital settings, have seen mixed success. Incentivising patients with monetary rewards, provision of home visits, implementing patient reminder and recall systems, formulating clinical protocols and creating immunisation information systems are some of the measures studied.23–31 This not withstanding, most influenza vaccination studies are mainly among the elderly patients, some of whom have COPD.30–34 There have been limited studies dedicated to patients with COPD alone.11,12
As part of a comprehensive effort to improve care and follow-up, all patients with COPD who are seen in the inpatient or outpatient setting in National University Hospital, one of Singapore’s tertiary referral hospitals with a full complement of specialties, are offered the opportunity to participate in the “integrated nurse-led, specialist-supported” airway program (TAP). An internal audit of the national TAP registry found that Singapore’s average influenza vaccination rate among patients with COPD was approximately 40%. Through TAP, the authors embarked on a quality improvement project to improve the influenza vaccination rates among patients with COPD. We hypothesize that a multi-pronged approach influencing physicians’ vaccination behaviour, an additional reminder from nurses and public education would help to improve the influenza vaccination rates among patients with COPD.
Methods
Subjects
This before–after study of a quality improvement project was conducted in the National University Hospital. The population studied was all existing COPD TAP patients at the end of 2013. The interventions were implemented in 2014; thus, the population was stratified into the pre-intervention group and post-intervention group. The pre-intervention group comprised existing COPD TAP patients who received their influenza vaccinations prior to the end of 2013. Thereafter, the post-intervention group comprised of all COPD TAP patients who received their influenza vaccinations within 2014. COPD TAP patients who died in 2014 were excluded.
Study Protocol And Intervention
TAP is a nurse-led, specialist-supported program designed to provide holistic care to all patients with COPD. TAP nurses are tasked to support follow-up care post-discharge, provide coordination between different care providers (pulmonary rehabilitation referrals, advanced care planning, referrals to medical social workers) and assist physicians to optimise treatment. Specialist care is provided by the Division of Respiratory and Critical Care Medicine.
Demographic data (age, gender and ethnicity), comorbid diseases (sleep disorders, ischemic heart disease, hypertension, hyperlipidemia and diabetes mellitus), premorbid functional status, family support and smoking history were collected for all patients studied. Family support is defined by the presence of a family member who accompanied the patient for his/her outpatient clinic visit. Baseline lung function test, number of hospital admissions in the preceding year of the study and the modified medical research council (mMRC) dyspnea scale scores were also recorded. Baseline evaluation of COPD severity (GOLD staging) was determined based on the existing 2018 GOLD guidelines, so as to ensure relevance to current guidelines.10 In addition, the presence of pulmonary hypertension (defined as pulmonary artery systolic pressure ≥ 38 mmHg on echocardiography) and cor pulmonale (defined as dilation of the right ventricle on echocardiography) were also determined. Prior intubation episodes, prior non-invasive ventilation use and long-term oxygen therapy were also noted.
The baseline vaccination rate of all pre-intervention patients with COPD in TAP was determined through paper and electronic vaccination records. Influenza vaccinations that were administered in the year 2013 were recorded. Prior pneumococcal vaccination was also recorded. Three groups of interventions were then implemented and reinforced from 1st January to 31st December 2014 to improve the vaccination rates. Three groups of interventions were performed to improve vaccination rates. These were broadly targeted at (1) patients, (2) physicians, and (3) nurses.
The first intervention involved patient education. In order to raise awareness, education posters reminding patients of the need for and efficacy of influenza vaccination were created. They were prominently placed in the clinics and at the registration counters, for the public to view. Refer to Figure 1 with regards to the poster. It was hoped that such reminders would prompt the patients with COPD to remind their physicians about their influenza vaccination status.
 |
Figure 1 Vaccination poster. |
The second intervention targeted physicians. This intervention relied on three measures targeted at improving physician vaccination prescription practices. Cognitive aids in the form of vaccination card reminders were attached to the clinic computer screens. This was instituted as the clinics were usually busy, with a physician being able to spend only a limited amount of time with each patient. As such, the physicians would usually focus on the acute medical issues and may often neglect to consider influenza vaccinations for patients with COPD. Such provider reminders have been shown to be effective.24 Coincidentally, a new electronic healthcare record system (EHR) was also implemented in January 2014 as part of a hospital systems overhaul. We utilised the EHR to improve the record-keeping of physician’s clinic notes and vaccination dates as it had been shown to be an effective method of improving vaccination rates, with the vaccination data being much more easily retrievable.25 In addition, health professionals have generally been one of the most trusted source of information regarding vaccinations for most patients.35,36 However, physician prescription practices may vary. This could be due to pre-conceived notions about vaccinations,36,37 forgetting about vaccinations due to a busy clinic or even just assuming that the physicians have been performing their due diligence when this may not be the actual reality. As such, a department briefing to the physicians was then conducted in December 2013, prior to the start of the quality improvement project, highlighting the baseline influenza vaccination rates and the various interventions in place to help improve these rates.
All patients with COPD will have to visit the TAP nurse after every clinic consultation with the physician. The TAP nurse plays many roles to complement the clinic visit, including ensuring inhaler technique adequacy, smoking cessation advice and playing a dual-role of a medical social worker. As part of their job scope, they would also have to look and ensure that their influenza vaccination dates are up-to-date. If the patients are due for their influenza vaccinations, they would check if the physicians have already taken steps to order for it. For the third intervention, she would highlight to the primary physician if the influenza vaccination was due but omitted. The physician would then facilitate the vaccination accordingly.
The patients with COPD were followed up till the end of 2015. Influenza vaccination rates were recorded by TAP nurses. Once an influenza vaccination was ordered and administered, the TAP nurses would then interview the patient and record down whether the patients themselves, physicians, or nurses initiated the vaccination process. Adverse outcomes to vaccination, if any, were also recorded.
A questionnaire was also created to poll the physicians on which of the various physician-centric interventions influenced a change in vaccination prescription practices. Each physician was allowed multiple options. This questionnaire was sent to all 24 physicians in the Division of Respiratory and Critical Care Medicine.
Outcome Measures
The primary outcome was the rate of influenza vaccination coverage among all patients with COPD in TAP. The secondary outcome was the proportion of vaccinations that was attributed to each intervention.
Ethical Considerations
This study was originally a clinical cum administrative quality-improvement-project (QIP) with the data being collected prospectively to document outcomes for the purpose of reporting to hospital clinicians and management. Informed consent was not required then. The National Healthcare Group Domain-Specific Review Board subsequently approved the study with a waiver of informed consent (2016/01311).
Statistical Analysis
Descriptive statistics for categorical variables were presented as frequency (percentage) and mean (SD) for numerical variables with a normal distribution. P-values were calculated with the use of the chi-square statistic, with statistical significance set at p < 0.05. The statistical software STATA version 15.0 was used.
Results
There were 370 patients with COPD in the pre-intervention group. Of these, 22 patients died over the course of 2014 and were excluded. Hence, only the remaining 348 patients with COPD were included in this quality improvement project. The patient characteristics are shown in Table 1. The majority of patients were male and Chinese. Close to 80% were community ambulant and 66.7% of the patients had family support. Most belonged to GOLD A and B. Approximately 5% had developed cor pulmonale, while 33.1% had pulmonary hypertension. Approximately 25% had previously received non-invasive ventilation and 18.7% of patients had had prior episodes of intubation.
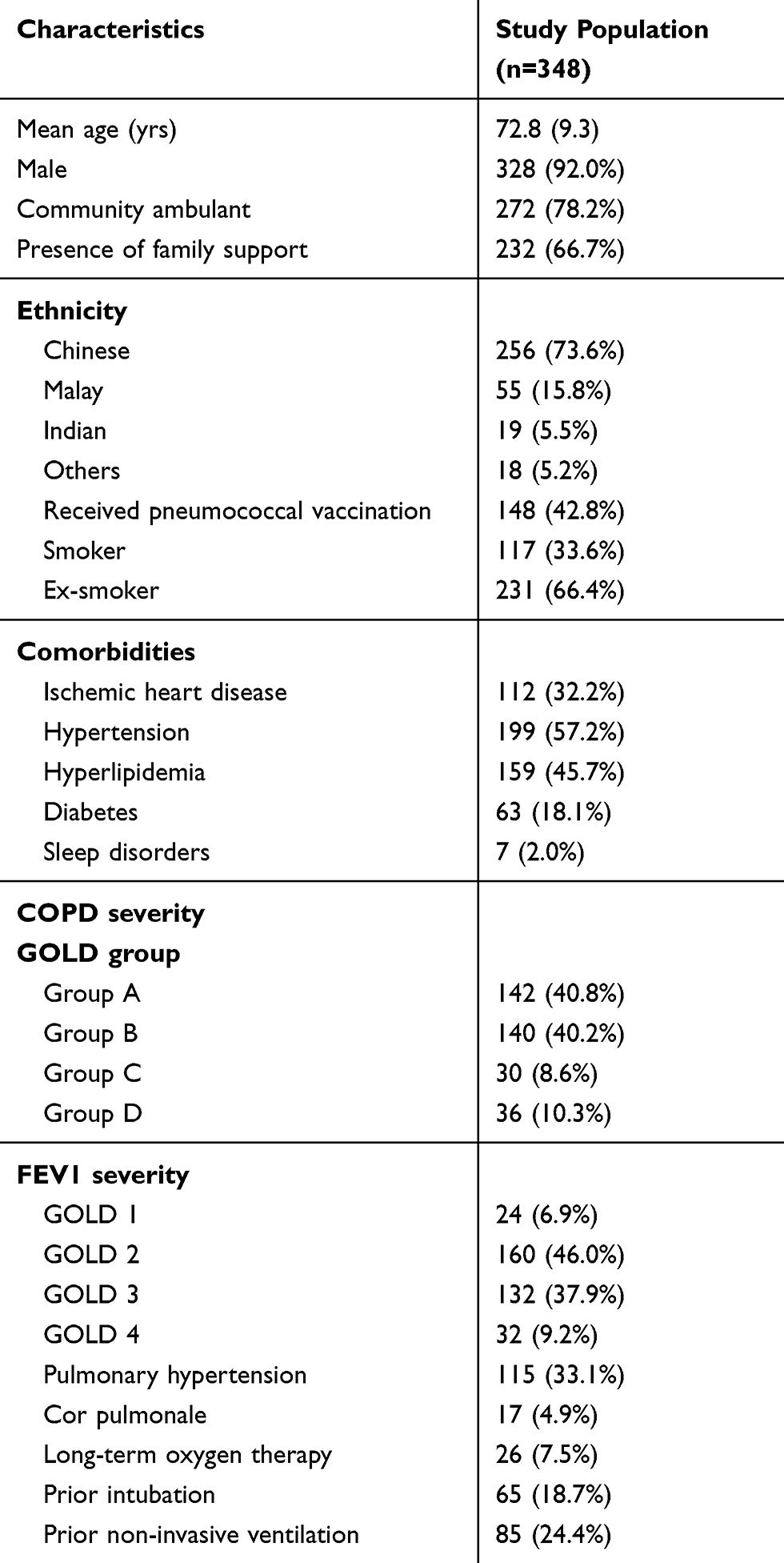 |
Table 1 Baseline Characteristics Of The Study Population |
Baseline influenza vaccination rate among the pre-intervention group was 47.7% (166 out of 348 patients) (Table 2). In the post-intervention group, the influenza vaccination rate improved significantly to 80.7% (281 out of 348 patients) (p<0.001). Sixty-three patients refused vaccination pre-intervention, but this number reduced to 22 patients post-intervention. Chinese patients (p=0.036) and patients with COPD of lower FEV1 severity (p=0.017) were more likely to receive their vaccinations after the interventions were implemented. GOLD staging did not have an impact on vaccination rates (p=0.18), and neither did good family support (p=0.81).
 |
Table 2 Influenza Vaccination Status |
In the post-intervention group, physicians were the predominant reason for initiating influenza vaccination in 247 patients (87.9%). An additional 34 patients (12.1%) received their vaccinations as a result of nurses’ reminders. None of the patients attributed their updated vaccination status to the patient education posters. There was a significant drop in the number of patients declining vaccination (18.1% vs 6.3%) in the post-intervention group (p<0.01).
The physician response rate for the questionnaire on interventions which influenced vaccination practices was 67% (16/24). While the vaccination card reminders on the computers and the newly minted electronic system influenced practices, the main impetus for change was the realisation that current vaccination rates were low (Table 3).
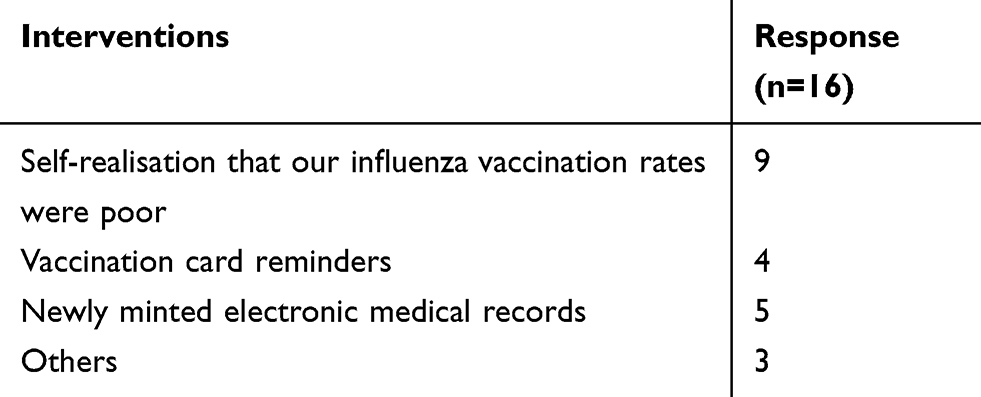 |
Table 3 What Improved Doctor’s Vaccination Prescription Behaviour? |
Discussion
A multi-pronged approach consisting of education posters for patients, interventions to improve physicians’ vaccination prescription practices through self-awareness, cognitive aids, and implementation of a new EHR, and empowering nurses proved pivotal in improving the influenza vaccination rates among patients with COPD from 47.7% to 80.7%. In particular, the realisation that influenza vaccination rates were suboptimal was one of the main impetuses for change.
Successful implementation of the various interventions is dependent on an intricate inter-play of prevailing local barriers to vaccination and the amount of health resources available. Several studies have described successful interventions, including telephone and letter reminders,24 community outreach,27 incentivisation,28 adequate staffing and better clinic organisation,30 and pharmacist and nurse actions.29,31 However, interventions must be contextualised to local settings. Awareness of influenza vaccination remains poor in Singapore: in a study of diabetic patients by Tan EK and colleagues, the majority felt they did not require vaccinations and were not advised on the need for vaccinations.32 This lack of awareness is likely to be equally if not more prevalent among patients with COPD who are generally elderly and who often have poor health literacy.33,34
It is interesting to note that the patient education material had minimal impact on patients with COPD. It is possible that patients with poor health literacy rely more on physicians to provide the necessary advice.34 This may also be a reflection of the older Asian’s socio-cultural outlook on chronic disease management in general and vaccinations specifically.35 In Asian culture, communication tends to be more paternalistic38 rather than an open two-way communication. Patients’ beliefs and preferences with regard to medications are very much dependent on the patient–doctor relationship and professional expertise provided.39 The patients are more inclined to be compliant with medications and by inference, vaccinations, when the physicians actively promote and recommend vaccination.35 As demonstrated in this study, when the physicians became more active in promoting vaccination, the number of patients who rejected vaccinations decreased. A better understanding of the impact of patient education, and the type of material used, is required to facilitate a change in vaccination perceptions and acceptance, starting first within healthcare facilities before scaling to the larger population.40
Changing physician practice is always difficult, especially if there is a perception that all is well with the quality of care provided.37 Self-awareness is required before change can be contemplated. In this study, realisation by physicians that vaccination rates were not up to par provided motivation for improvement. While the EHR25 and card reminders24 are interventions that have helped improve vaccination rates, they require tailoring to local settings. In the study hospital, where the majority of patients with COPD are reviewed in the busy outpatient clinic setting without home visits, home-based interventions are unlikely to succeed, and clinic-based interventions should be intuitive and not impose additional cognitive workload. Various EHR templates for vaccination exist. Some have pre-loaded vaccination records and alerts for missing or delayed vaccinations.41 Others have made influenza vaccination a standing order.42 As such functions are not available in the study hospital’s EHR, physicians manually recorded the vaccination dates down on the electronic clinic notes. These notes can be reviewed easily at the click of a button and were a vast improvement from the paper clinical records of the past.
Nurses play an important role in the holistic care of patients with COPD. In line with studies showing the effectiveness of both pharmacist and nurse interventions,29,31 empowerment of the TAP nurses in our study proved invaluable. The close rapport between them and the patients with COPD helped in convincing patients who were initially resistant to vaccinations to proceed with vaccinations.
To the best of the authors’ knowledge, this is the largest prospective study dedicated to influenza vaccination for patients with COPD. Strengths include the minimal loss of patient follow-up, the detailed assessment of reasons for change in prescription practices, and the real-world nature with easy-to-implement interventions. The study, however, has limitations. As it was non-blinded before-and-after study, a Hawthorne effect resulting in physicians increasing vaccination rates simply because of awareness of the ongoing investigation cannot be excluded. In addition, the current study analysed results after 1 year of interventions and did not evaluate sustainability over a longer period. Sustained reminders, constant audits, and regular feedback are required to ensure long-term practice change.
Conclusion
A multi-pronged approach can help improve influenza vaccination rates among patients with COPD. With greater self-awareness of current practices by physicians, coupled with reminders through cards, the EHR, and nurses, vaccination rates improved to 80.7%. Further reinforcement and regular audits are important to ensure the sustainability of this vaccination program.
Statement Of Data Availability
The authors confirm that the data supporting the findings of this study are available within the article and tables. They are also available on request from the corresponding author, Andrew Li. The data is not publicly available due to the information that could compromise the privacy of the research participants.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Lopez-Campos JK, Tan W, Soriano JB. Global burden of COPD. Respirology. 2016;21:14–23. doi:10.1111/resp.12660
2. Makris D, Moschandreas J, Damianaki A, et al. Exacerbations and lung function decline in COPD: new insights in current and ex-smokers. Respir Med. 2007;101:1305–1312. doi:10.1016/j.rmed.2006.10.012
3. Kanner RE, Anthonisen NR, Connet JE. Lower respiratory illnesses promote FEV1 decline in current smokers but not ex-smokers with mild chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164:358–364. doi:10.1164/ajrccm.164.3.2010017
4. Miravitlles M, Ferrer M, Pont A, et al. Effect of exacerbations on quality of life in patients with chronic obstructive pulmonary disease: a 2 year follow up study. Thorax. 2004;59:387–395. doi:10.1136/thx.2003.008730
5. Singanayagam A, Schembri S, Clamers JD. Predictors of mortality in hospitalized adults with acute exacerbation of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2013;
6. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128–1138. doi:10.1056/NEJMoa0909883
7. Wedzicha JA. Role of viruses in exacerbations of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2004;1:115–120. doi:10.1513/pats.2306030
8. Kurai D, Saraya T, Ishii H, Takizawa H. Virus-induced exacerbations in asthma and COPD. Front Microbiol. 2013;4:293. doi:10.3389/fmicb.2013.00293
9. Seemungal TAR, Donaldson GC, Bhowmik A, Jeffries DJ, Wedzicha JA. Time course and recovery of exacerbations in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161:1608–1613.
10. 2018 Global strategy for prevention, diagnosis and management of COPD.
11. Poole P, Chacko EE, Wood-Baker R, Cates CJ. Influenza vaccine for patients with chronic obstructive pulmonary disease. Cochrane Database of Syst Rev. 2006;1:CD002733.
12. Bekkat-Berkani R, Wilkinson T, Buchy P, et al. Seasonal influenza vaccination in patients with COPD: a systematic review. BMC Pulm Med. 2017;17:79. doi:10.1186/s12890-017-0420-8
13. Grohskopf LA, Sokolow LZ, Broder KR, et al. Prevention and control of seasonal influenza with vaccines recommendations of the advisory committee on immunization practices - United States, 2016–2017 influenza season. MMRW Recommend Rep. 2016;65:1–52. doi:10.15585/mmwr.rr6505a1
14. National Vaccine Advisory Committee. Strategies to achieve the Healthy People 2020 annual influenza vaccine coverage goal for health-care personnel: recommendations from the national vaccine advisory committee. Public Health Rep. 2013;128:7–25. doi:10.1177/003335491312800103
15. Ciblak MA, Platformu G. Influenza vaccination in Turkey: prevalence of risk groups, current vaccination status, factors influencing vaccine uptake and steps taken to increase vaccination rate. Vaccine. 2013;31:518–523. doi:10.1016/j.vaccine.2012.11.022
16. European Centre for disease prevention and control (ECDC). Seasonal influenza vaccination in Europe - overview of vaccination recommendations and coverage rates in the EU member states for the 2012–2013 influenza season, technical report. Eur Centre Dis Prev Control. 2015.
17. Centers for disease control and prevention (CDC). Flu vaccination coverage, United States, 2014–15 influenza season; 2016. Available from: http://www.cdc.gov/flu/fluvaxview/coverage-1415estimates.htm].
18. Chronic obstructive pulmonary disease. MOH Singapore clinical practice guidelines 2/2017.
19. Kimmel SR, Burns IT, Wolfe RM, Zimmerman RK. Addressing immunization barriers, benefits, and risks. J Fam Pract. 2007;56(2 Suppl Vaccines):S61–69.
20. Prins W, Butcher E, Hall LL, Puckrein G, Rosof B. Improving adult immunization equity: where do the published research literature and existing resources lead? Vaccine. 2017;35:3020–3025. doi:10.1016/j.vaccine.2017.02.016
21. Tan LLJ. A review of the key factors to improve adult immunization coverage rates: what can the clinician do? Vaccine. 2018;36:5373–5378. doi:10.1016/j.vaccine.2017.07.050
22. Garcia DA, Velandia-Gonzalez M, Trumbo SP, et al. Understanding the main barriers to immunization in Colombia to better tailor communication strategies. BMC Public Health. 2014;14:669. doi:10.1186/1471-2458-14-669
23. United States community preventive services task force. Increasing appropriate vaccination. Guide to community preventive services. 2017.
24. Jacobson Vann JC, Szilagy PG. Patient reminder and recall systems to improve immunization rates. Cochrane Database of Syst Rev. 2005;3:CD003941.
25. Ruffin MT, Plegue MA, Rockwell PG, et al. Impact of an electronic health record (EHR) reminder on human papillomavirus (HPV) vaccine initiation and timely completion. J Am Board Fam Med. 2015;28:324–333. doi:10.3122/jabfm.2015.03.140082
26. Groom H, Hopkins DP, Pabst LJ, et al. Immunization information systems to increase vaccination rates: a community guide systematic review. J Public Health Manag Pract. 2015;21:227–248. doi:10.1097/PHH.0000000000000069
27. Tran CH, Sugimoto JD, Pulliam JR, et al. School-located influenza vaccination reduces community risk for influenza and influenza-like illness emergency care visits. PLoS ONE. 2014;9:e114479. doi:10.1371/journal.pone.0114479
28. Marteau TM, Ashcroft RE, Liver A. Using financial incentives to achieve healthy behaviour. BMJ. 2009;9:b1415. doi:10.1136/bmj.b1415
29. Cotugno S, Morrow G, Cooper C, Cable M, Cohn S. Impact of pharmacist intervention on influenza vaccine assessment and documentation in hospitalized psychiatric patients. Am J Health-Syst Pharm. 2017;74(suppl 4):90–94. doi:10.2146/ajhp160755
30. Dexter LJ, Teare MD, Dexter M, Siriwardena AN, Read RC. Strategies to increase influenza vaccination rates: outcomes of a nation-wide cross-sectional survey of UK general practice. BMJ Open. 2012;2:e000851. doi:10.1136/bmjopen-2011-000851
31. Thomas RE, Russel M, Lorenzetti D. Interventions to increase influenza vaccination rates of those 60 years and older in the community. Cochrane Database Syst Rev. 2010;9:CD005188.
32. Tan EK, Lim LH, Teoh YL, Ong G, Bock HL. Influenza and seasonal influenza vaccination among diabetics in Singapore: knowledge, attitude and practices. Singapore Med J. 2010;51:623–630.
33. Bozkurt H, Demirci H. Health literacy among older persons in Turkey. Aging Male. 2018;10:1–6.
34. Nguyen MH, Chen LL, Lim KW, Chang WT, Mamun K. Vaccination in older adults in Singapore: a summary of recent literature. Proc Singapore Healthcare. 2015;24:94–102. doi:10.1177/201010581502400205
35. Blendon RJ, Benson JM, Hero OJ. Public trust in physicians – U.S. medicine in international perspective. N Engl J Med. 2014;371:1570–1572. doi:10.1056/NEJMp1407373
36. Eve D, Laberge C, Guay M, Bramadat P, Roy R, Bettinger J. Vaccine hesitancy, an overview. Hum Vaccin Immunother. 2013;9:1763–1773. doi:10.4161/hv.24657
37. Kelly MP, Barker M. Why is changing health-related behaviour so difficult? Public Health. 2016;136:109–116. doi:10.1016/j.puhe.2016.03.030
38. Claramita M, Nugraheni MDF, van Dalen J. van der Vleuten C. Doctor-patient communication in Southeast Asia: a different culture? Adv Health Sci Educ Theory Pract. 2013;18:15–31. doi:10.1007/s10459-012-9352-5
39. Goff SL, Mazor KM, Meterko V, Dodd K, Sabin J. Patients’ beliefs and preferences regarding doctors’ medication recommendations. J Gen Intern Med. 2008;23:236–241. doi:10.1007/s11606-007-0470-3
40. Ory MG, Smith ML, Mier N, Wenicke MM. The science of sustaining health behavior change: the Health maintenance consortium. Am J Health Behav. 2010;34:647–659. doi:10.5993/AJHB.34.6.2
41. Au L, Oster A, Yeh GH, Magno J, Paek HM. Utilizing an electronic health record system to improve vaccination coverage in children. Appl Clin Inform. 2010;1:221–231. doi:10.4338/ACI-2009-12-CR-0028
42. Zimmerman RK, Albert SM, Nowalk MP, Yonas MA, Ahmed F. Use of standing orders for adult influenza vaccination a national survey of primary care physicians. Am J Prev Med. 2011;40:144–148. doi:10.1016/j.amepre.2010.10.027
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.