Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Improving Efficiency and Safety with Prefilled Syringes: A Model-Based Economic Evaluation for US Healthcare Settings
Authors Borms M ![]() , Taneja A
, Taneja A ![]() , Weiss M, Girgis H, Frolet C, Lucaci JD
, Weiss M, Girgis H, Frolet C, Lucaci JD ![]()
Received 2 June 2025
Accepted for publication 26 September 2025
Published 4 October 2025 Volume 2025:17 Pages 673—685
DOI https://doi.org/10.2147/CEOR.S544296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Matthias Borms,1 Ashley Taneja,2 Mia Weiss,2 Haymen Girgis,1 Cecile Frolet,1 Julia D Lucaci2
1Becton, Dickinson and Company, Le Pont de Claix, 38800, France; 2Becton, Dickinson and Company, Franklin Lakes, NJ, 07417, USA
Correspondence: Julia D Lucaci, Becton, Dickinson and Company, 1 Becton Drive, Franklin Lakes, NJ, 07417, USA, Email [email protected]
Background: Prefilled syringes provide an opportunity to improve clinical safety and operational efficiency in hospital settings, especially amid mounting and ongoing challenges such as staff shortages, escalating drug costs, and increasing importance of safe medication administration. Despite these potential benefits, adoption remains limited. This study develops an economic model to assess the clinical and financial impacts of switching from conventional vial-and-syringe methods to prefilled syringes in United States (US) hospitals’ intensive care units (ICU).
Methods: To address the gap between the potential benefits of prefilled syringes and their limited adoption, an economic model was developed to help decision-makers make informed choices based on the clinical and financial impact of switching to prefilled syringes in US ICUs. The model used peer-reviewed literature and hospital practices around the most utilized dosages in a US hospital. To illustrate model utility, three hypothetical ICU cases were developed: administering 30 daily doses of atropine 1mg/10mL, epinephrine 1mg/10mL, and ephedrine 25mg/10mL. Sensitivity analyses were performed to test model robustness.
Results: Switching to prefilled syringes resulted in annual cost savings of $729,912 for atropine, $786,502 for epinephrine, and $709,772 for ephedrine. The model estimated annual savings to be $696,551 due to fewer pADEs, along with savings of $53,411, $89,744 and $50,244 annually, due to unused drug wastage reduction for each drug, respectively. Hospital staff preparation time decreased by 255 hours for atropine, 285 for epinephrine and 227 hours for ephedrine per year. Sensitivity analyses confirmed the robustness of the model by varying drug wastage rates, with potential savings of up to $740,443, $795,894 and $724,757 for each drug, respectively, showing the model’s adaptability across different ICU scenarios.
Conclusion: This model suggests prefilled syringes may help hospitals address pharmacy operational challenges by reducing preparation time, drug wastage, and pADEs. They offer a practical approach to support safer and more efficient medication delivery in clinical settings.
Keywords: prefilled syringes, ready-to-administer, preventable adverse events, drug wastage, economic evaluation, resource utilization
Introduction
In current hospital settings in the United States (U.S.), the need for enhanced operational efficiency and safety in medication administration has never been more critical, particularly with the growing complexity of care and the pressure to optimize resources. A possible solution to these challenges could be provided by ready-to-administer (RTA) medication delivery devices, such as prefilled syringes, which are pre-prepared injectable medications that require no further preparation before administration compared to conventional medication delivery methods. Despite this potential, prefilled syringes remain significantly underused in hospitals.1
Conventional vial-and-syringe methods are associated with several humanistic and economic burdens that span across both patient safety and healthcare efficiency. Errors in medication preparation and administration are a persistent concern, contributing to preventable adverse drug events (pADEs) that increase healthcare costs and prolong hospital stays.2 It was estimated that, in the US, adverse events related to the administration of injectable medicines contribute to an increase from $2.7 to $5.1 billion in annual costs.2 The cumulative impact of such errors, coupled with the time-intensive preparation processes, places considerable strain on healthcare resources.3–6
Pharmacy and nursing workforce shortages in the US have intensified following the COVID-19 pandemic, placing significant strain on hospital operations.7,8 Labor costs rose by nearly 40% between 2019 and early 2022, and more than 200,000 additional nurses are projected to be needed annually through 2031 to fill staffing gaps.9,10 Additionally, nearly 1 in 10 hospitals have lost over 40% of their pharmacy technicians, and 89% of pharmacy leaders report that pharmacists are increasingly performing technician-level tasks like medication preparation, adding burden to already stretched pharmacy workflows.11 Moreover, 41% of pharmacy administrators report outsourcing medication preparation and products because of staffing constraints, reflecting the urgency to streamline medication delivery workflows.11 In this context, prefilled syringes may help relieve operational burdens by reducing preparation time and supporting pharmacy efficiency. Time-and-motion studies have also shown that the use of prefilled syringes reduces healthcare professionals’ time spent on medication preparation, translating into more efficient workflows and potentially reducing staff fatigue, which is a known contributor to medical errors.12,13
Currently, many US hospitals use decentralized medication distribution, where drugs are stored and prepared directly on care units, especially for emergency medications like atropine and epinephrine or in oncology where rapid access and tailored dosing are common.14,15 This approach can strain pharmacy teams, especially as chief pharmacy officers look to centralize certain services to improve consistency and reduce inefficiencies.14 Given these challenges, prefilled syringes represent a practical solution by offering a standardized ready-to-administer format that can help reduce preparation time, ease staffing demands, and support more efficient medication administration at the point of care.
To support improvements in patient safety, U.S.-specific incentive programs such as the Hospital-Acquired Condition (HAC) Reduction Program encourage hospitals to implement best practices that reduce preventable harm and associated penalties.16 By reducing errors in medication preparation and administration, prefilled syringes may provide a practical way to align with these safety goals and help maintain Medicare reimbursement. Studies have demonstrated that prefilled syringes use can reduce pADEs by nearly half, leading to substantial clinical and economic benefits.17,18 Moreover, prefilled syringes can limit drug wastage by eliminating the need to prepare doses that may not be administered, leading to cost savings and resource optimization in both high- and low-acuity settings.19
Beyond patient safety concerns, drug wastage presents another considerable financial strain. It is estimated that 20–50% of doses prepared in emergency departments and operating rooms are discarded due to narrow administration windows or expiration times.19,20 This wastage translates into direct financial losses for hospitals and missed opportunities for resource optimization, especially when high-cost medications are involved.
This analysis builds on earlier economic modeling work done in European hospital settings,21,22 which showed the benefits of prefilled syringes in reducing drug wastage, preparation time, and preventable adverse drug events. However, US hospitals face their own set of challenges, including centralized medication preparation and decentralized distribution, rising labor costs, and greater financial and legal consequences tied to medication errors. This underlines the need for a U.S.-specific model that reflects the pressures of this environment and can help guide more informed decision-making. Compared to conventional vial-and-syringe methods, prefilled syringes have been associated with improved operational efficiency in hospital settings, particularly by addressing common challenges for healthcare institutions facing growing financial and patient safety pressures.23,24 To address the gap between the potential benefits of prefilled syringes and their limited adoption, an economic model was developed to enable decision-makers to make informed choices based on the clinical and financial impact of switching from conventional vial-and-syringe methods to prefilled syringes in US hospital ICUs.
Methods
Model Development
An excel-based, customizable economic model was developed to assess the impact of switching from conventional vial-and-syringes methods to prefilled syringes in hospital settings. The model was structured following the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) guidelines for budget impact analyses, and the initial framework was informed by targeted literature reviews (Supplementary Information Figure 1). The model was adapted from a previously published framework developed through expert consultation with pharmacists, physicians, and hospital administrators.22 The model focused on four key outcome domains: pADEs, unused drug wastage, dose preparation time, and cost of supplies.
Model Structure
The model provides insight into the annual impact of transitioning from conventional methods (vials and syringes) to prefilled syringes in a US hospital setting. This was achieved by calculating the outcomes across four domains and integrating them into five user-facing worksheets, covering cost inputs, institutional parameters, and results (Figure 1). Model costs were inflation-adjusted to 2025 US dollars and included the following: cost of drugs; equipment for vials, syringes, and prefilled syringes; pADEs; and other associated expenses.
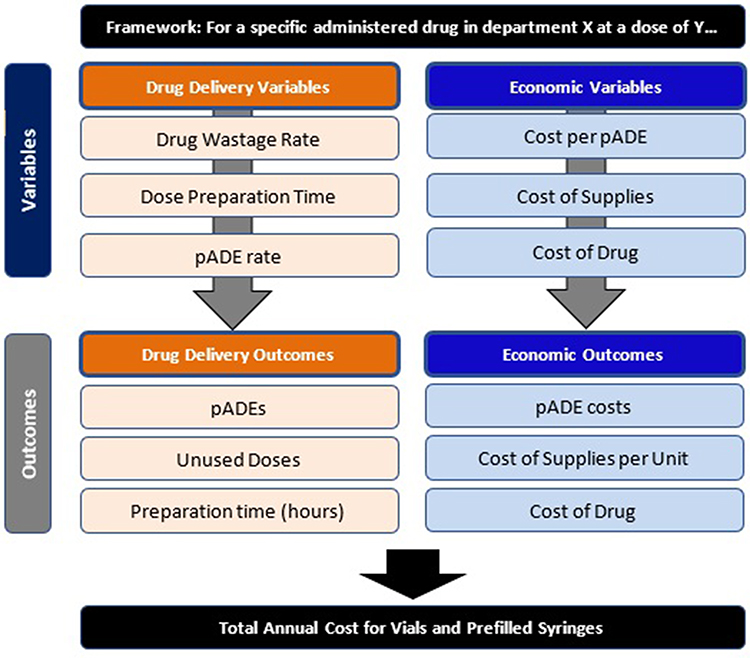 |
Figure 1 Economic Model Structure and Flow. |
Case Studies
To demonstrate the practical application and utility of the model, the case studies were conducted in a hypothetical US cardiac intensive care unit (CICU) administering 30 doses daily. Three different drugs were included as three case studies for atropine 1 mg/10 mL, epinephrine 1 mg/10 mL and ephedrine 25 mg/10 mL. To ensure examples broadly reflect hospital practices, the model development involved a thorough literature review of wastage and preventable adverse events with vials and prefilled syringes, and consultation with ICU specialists. The complete list of inputs is presented in Tables 1 and 2.
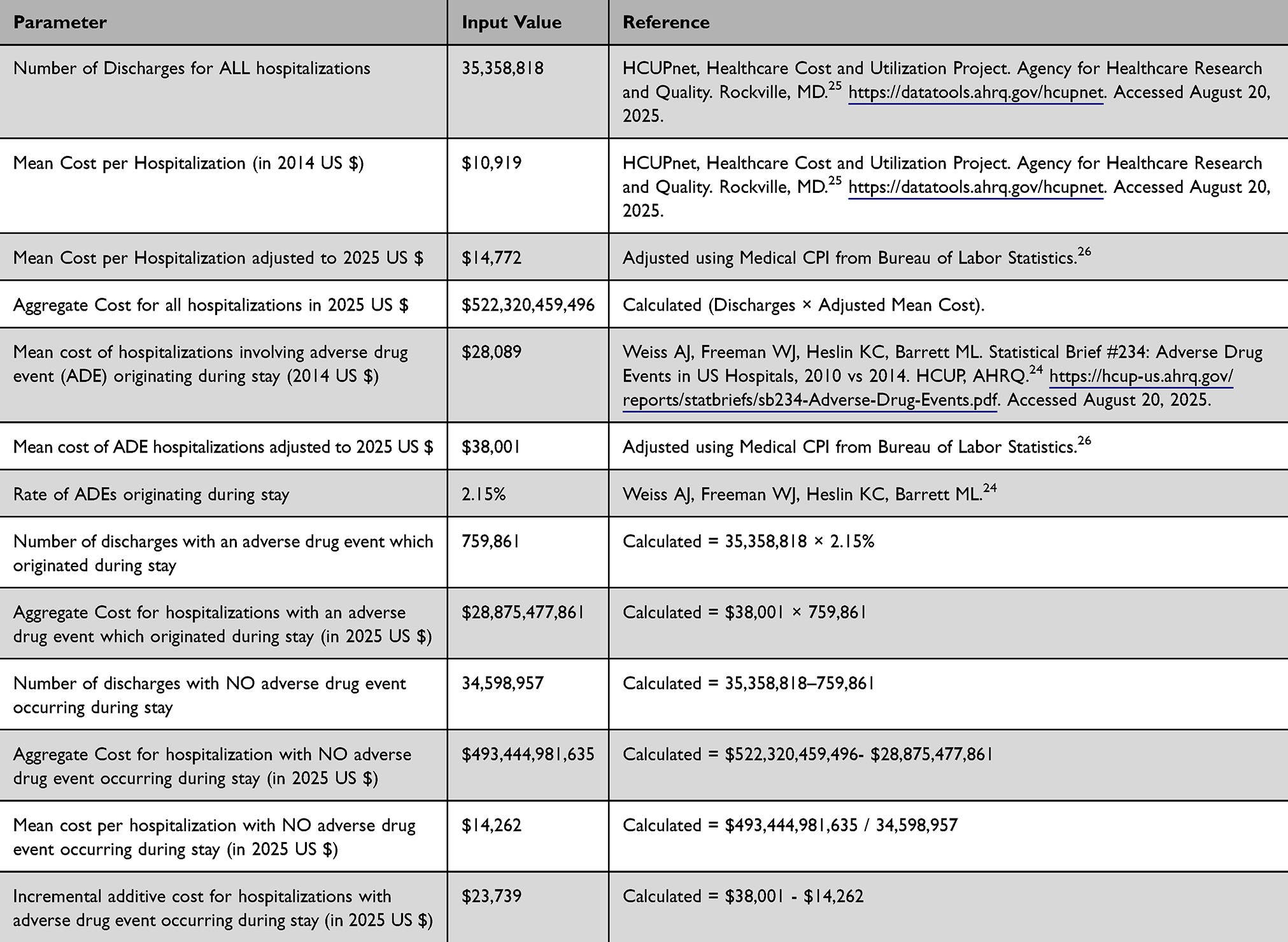 |
Table 1 Calculation Details of the Incremental Additive Cost for Hospitalizations with Adverse Drug Event Occurring During Stay |
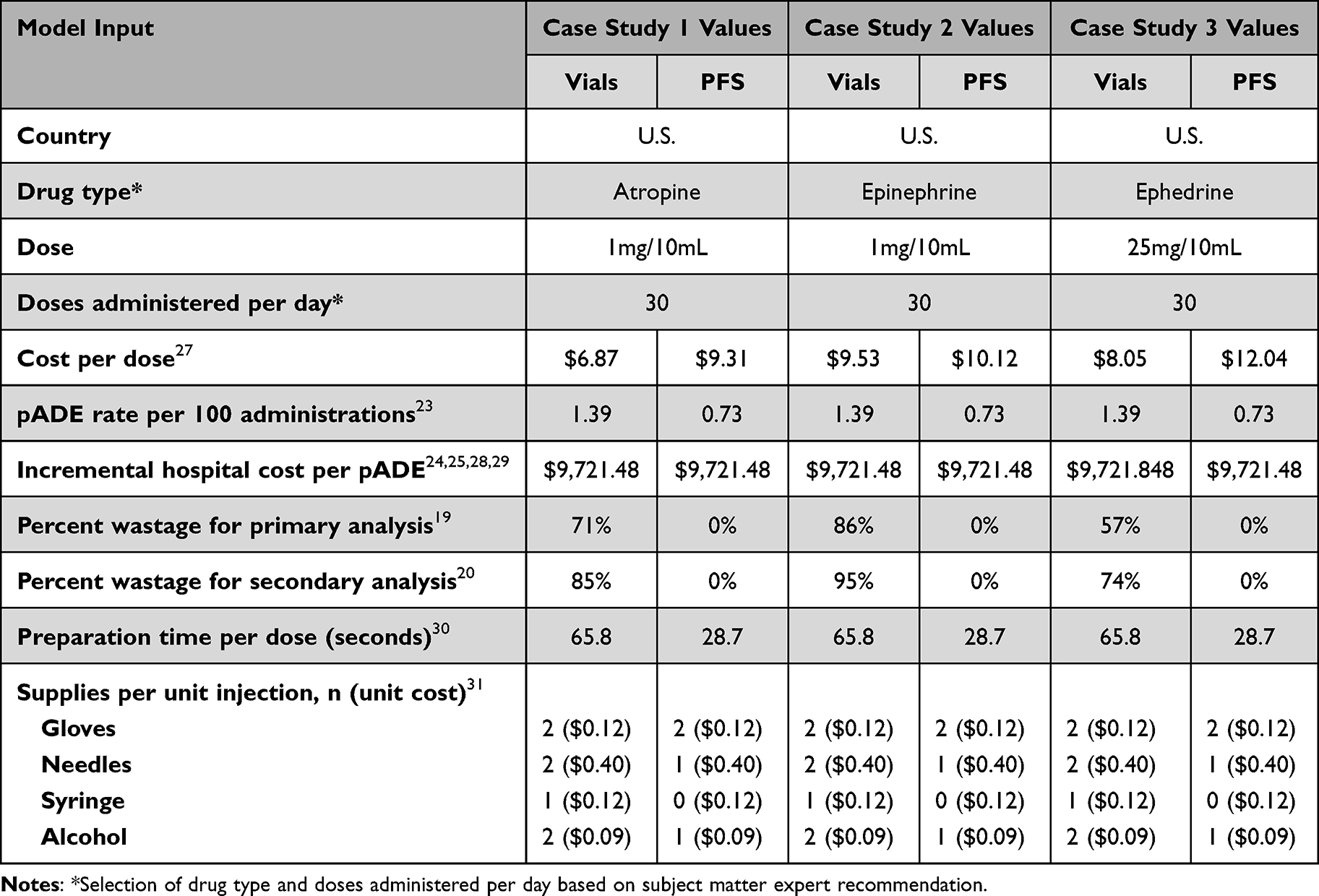 |
Table 2 Atropine, Epinephrine and Ephedrine Case Study Input Values and References for Primary Analysis and Sensitivity Analyses |
Parameters and Assumptions
To inform the selection of model parameters and assumptions, we relied on the findings of a recently published systematic literature review.1 We prioritized the selection of studies conducted in the US to ensure relevance. In cases where U.S.-specific data were limited or unavailable, we selected international studies deemed most appropriate based on clinical comparability and methodological rigor. Alternative sources and assumptions were evaluated through sensitivity analyses to assess the robustness of the model outcomes.
To complement the findings from the systematic literature review, expert input was gathered to inform drug selection and doses administered per day. Experts were selected based on their clinical and operational experience, particularly in hospital and acute care settings. The recruitment process involved identifying professionals with relevant expertise through professional networks and prior collaborations. Data was collected through structured interviews.
Preventable Adverse Drug Events
pADEs are a subset of adverse drug events that result from medication errors and can cause patient harm. The pADE rate was modeled at 1.39 per 100 administrations for vials and 0.73 per 100 administrations for prefilled syringes, reflecting the error reduction potential of prefilled syringes due to reduced manual handling and labeling errors.23 While the referenced study did not report pADE rate for each drug included in this analysis, the authors reported an overall pADE rate based on 3,671 medication administrations of different drugs commonly used in ICUs. We assumed that the overall pADE rate reported reflects common error rates associated with manual preparation and labeling, which are applicable across all ICUs medications. The weighted average cost of treating a pADE at $9,721.48 was calculated based on 12% of pADEs being severe events, with an estimated cost of $23,739 (detailed calculation is presented Table 1),24,25,28 and 88% being minor events, with a cost of $7,810.29 All costs were adjusted for inflation to 2025 USD.
Unused Drug Wastage
Conventional vial-based methods were modeled to have a drug wastage of 71%, 86%, and 57% for atropine, epinephrine and ephedrine, respectively, based on a study looking at drug preparation efficiencies in operating rooms and emergency departments.19,20 Although these estimates are drawn from international sources due to limited U.S.-specific data, they align with reported clinical practice challenges and were tested through sensitivity analyses. Prefilled syringes wastage was set at 0%.18 Other drugs with high wastage potential were also included in the model, although not explicitly shown in the case studies. These included: epinephrine 5 mg/5 mL, cisatracurium 20 mg/10 mL, midazolam 5 mg/15, midazolam 5 mg/5 mL, propofol 200 mg/20 mL, rocoronium 100 mg/10 mL, normal saline 10 mL, normal saline 20 mL, and urapidil 50 mg/10 mL.19
Preparation Time
Preparation time was defined as the total time it took for hospital staff to prepare a single dose of medication.12 The specific time assumptions were based on a US time and motion study that found 65.8 seconds per vial and 28.7 seconds per prefilled syringe.30 The model user could choose to select from additional options.12,13,32,33 Preparation time did not factor in monetarily to the cost calculations of the model.
Drug and Supply Costs
The unit costs of drugs were based on country-level IQVIA data for list prices from 2024.27 The costs per dose were $6.87, $9.53, and $8.05 for vials of atropine, epinephrine and ephedrine, respectively, and $9.31, $10.12, and $12.04 for prefilled syringes of atropine, epinephrine and ephedrine, respectively. The unit costs for supplies included gloves ($0.12/pair), needles ($0.40 each), syringes ($0.12 each), and alcohol swabs ($0.09 each), which were applied equally for both prefilled syringes and conventional methods.31 The supplies cost per injection was calculated based on the number of doses administered.
Sensitivity Analyses
The sensitivity analyses follow ISPOR guidelines,34 which recommend conducting alternative scenarios to quantify uncertainty for key parameters. Therefore, scenario analyses were conducted using alternative references for drug wastage. For other parameters, such as preparation time, error rates, and cost inputs, while multiple sources were available, the reported values were relatively consistent across studies and did not exhibit sufficient variability to warrant inclusion in the sensitivity analysis. A scenario analysis was performed to increase conventional method wastage to 85%, 95% and 74% for atropine, epinephrine and ephedrine, respectively, while keeping prefilled syringes wastage at 0%.20 The results of these analyses were used to assess the robustness of the model across different healthcare scenarios (See Tables 3–5).
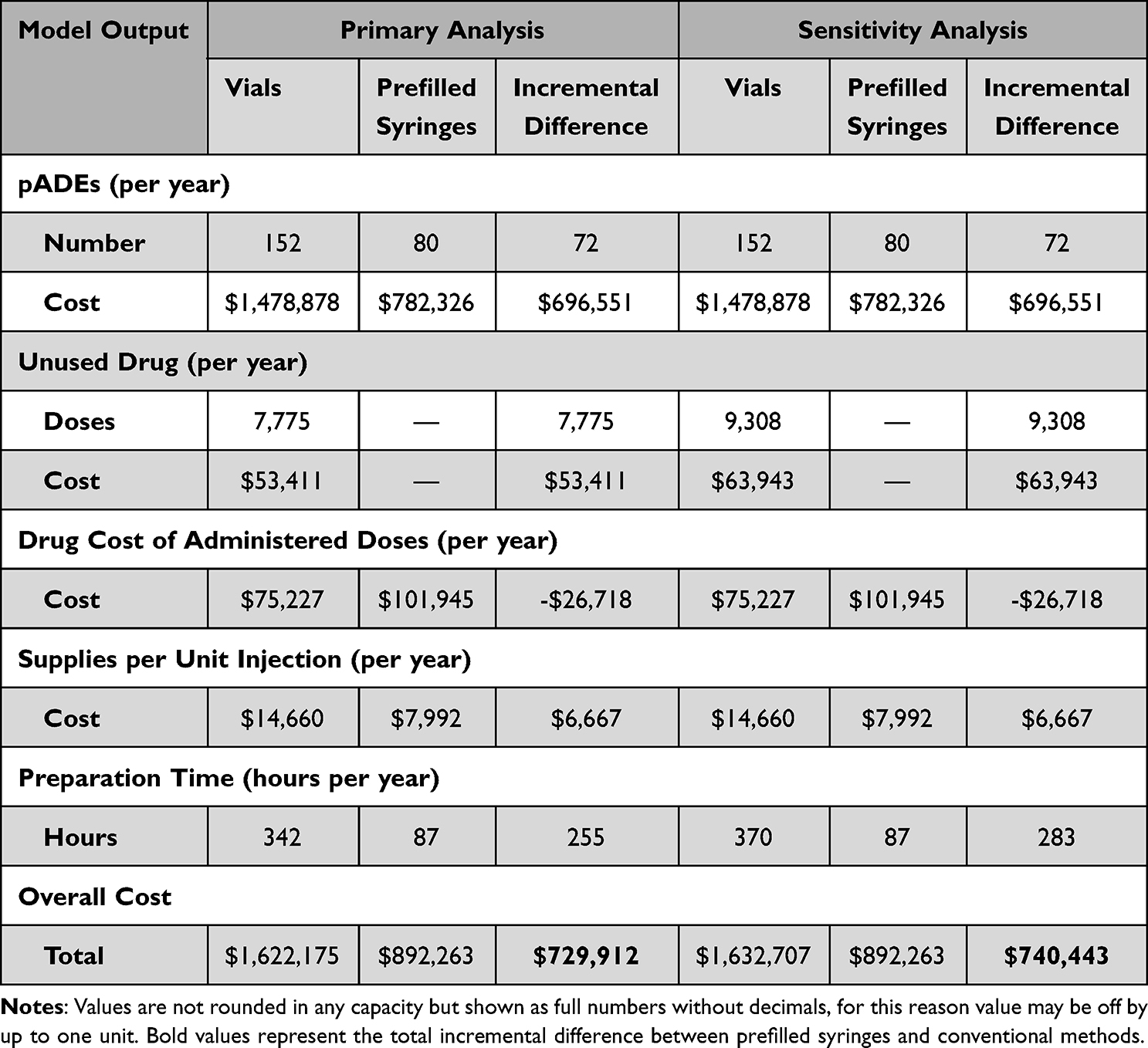 |
Table 3 Atropine Case Study 1 Primary Analysis and Sensitivity Analysis Results |
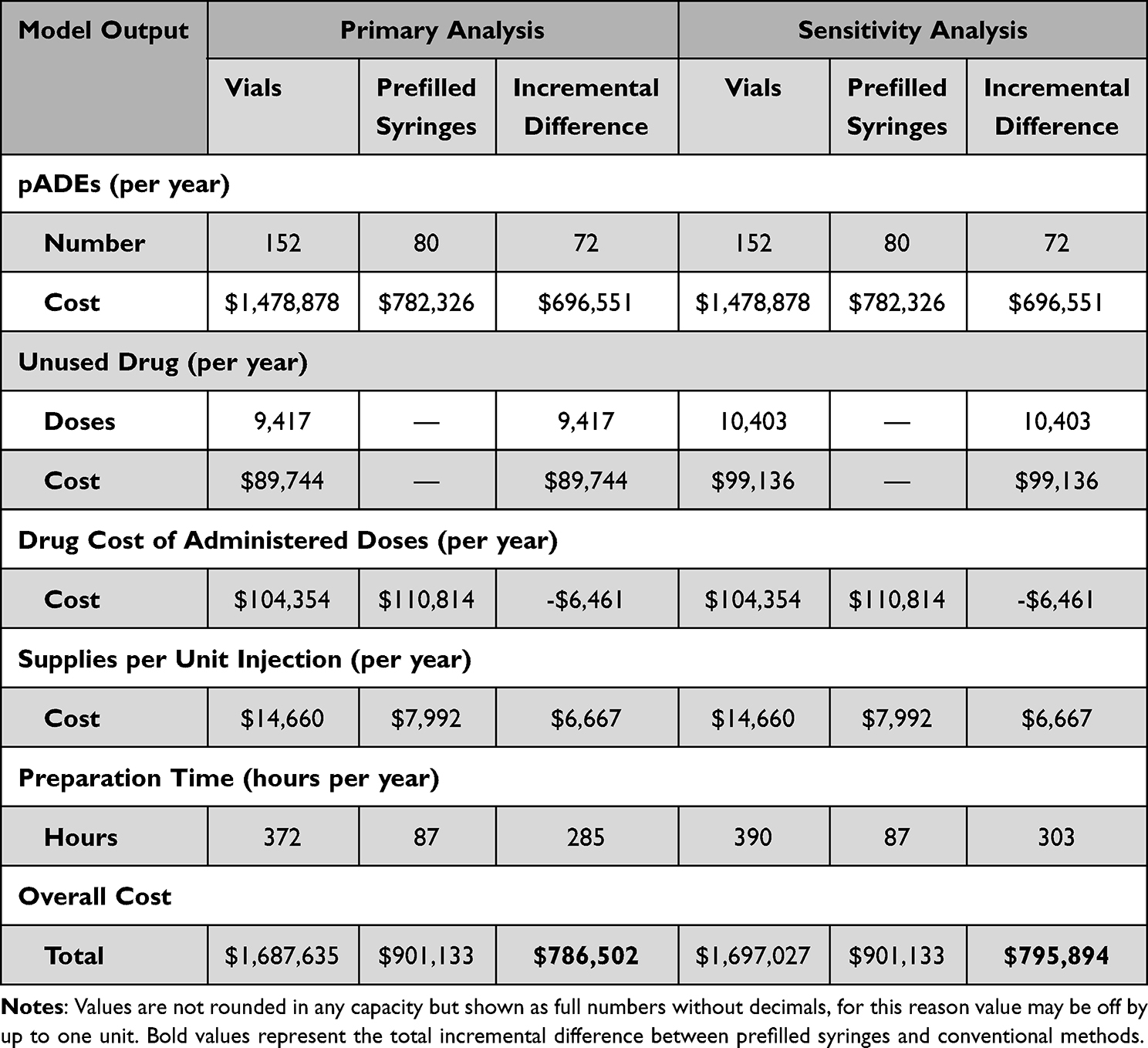 |
Table 4 Epinephrine Case Study 2 Primary Analysis and Sensitivity Analysis Results |
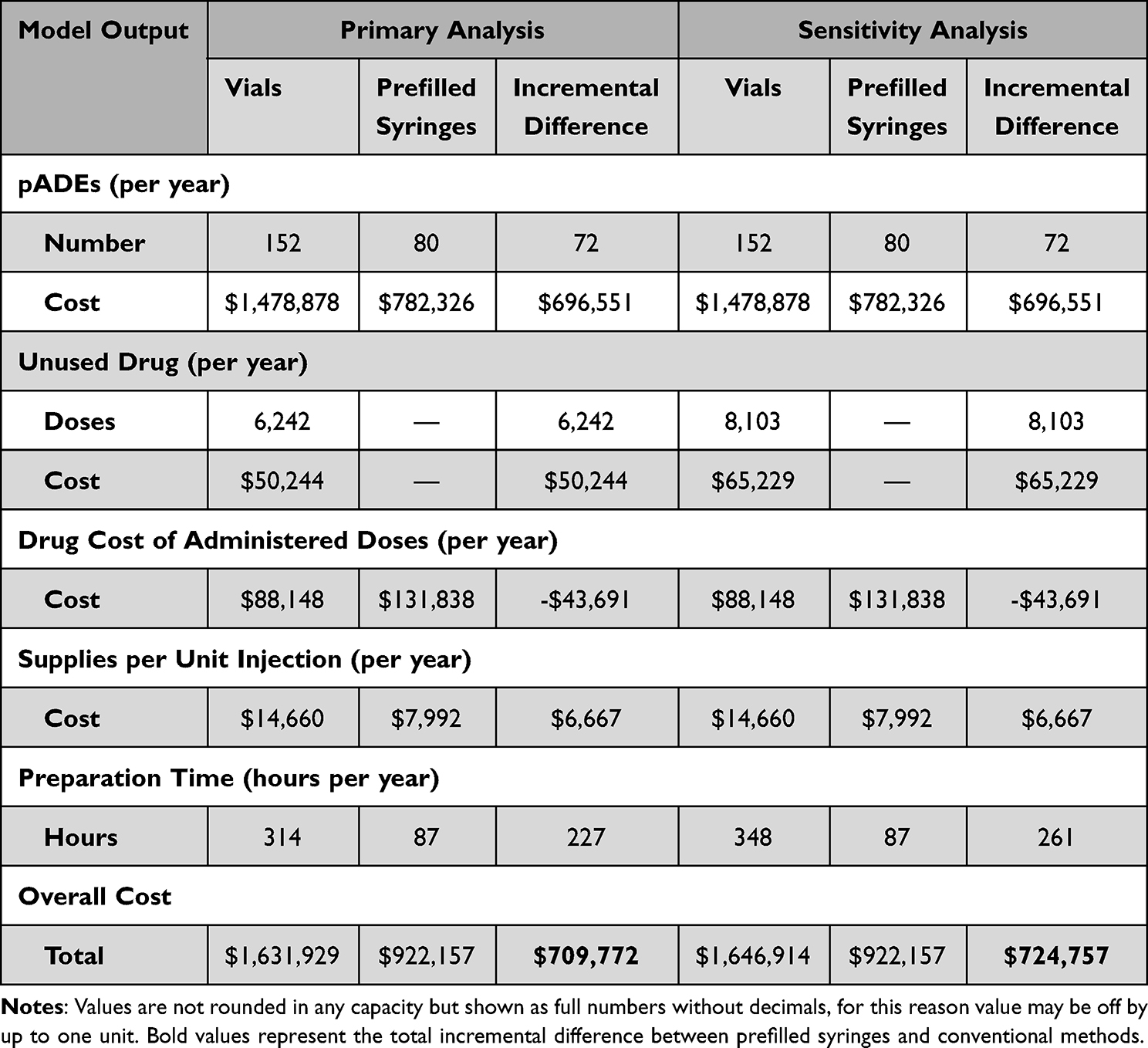 |
Table 5 Ephedrine Case Study 3 Primary Analysis and Sensitivity Analysis Results |
Results
The economic model results indicated that the additional cost for acquiring prefilled syringes could be offset by the cost savings from avoiding medication errors, wastage, and supplies usage. Across all three scenarios, pADE and supply costs remained constant, while preparation time, drug waste, and associated drug costs varied. Key results from the atropine, epinephrine, and ephedrine primary analysis and sensitivity analyses are outlined below, with graphical representations in Figures 2–4. Complete results are presented in Tables 3–5.
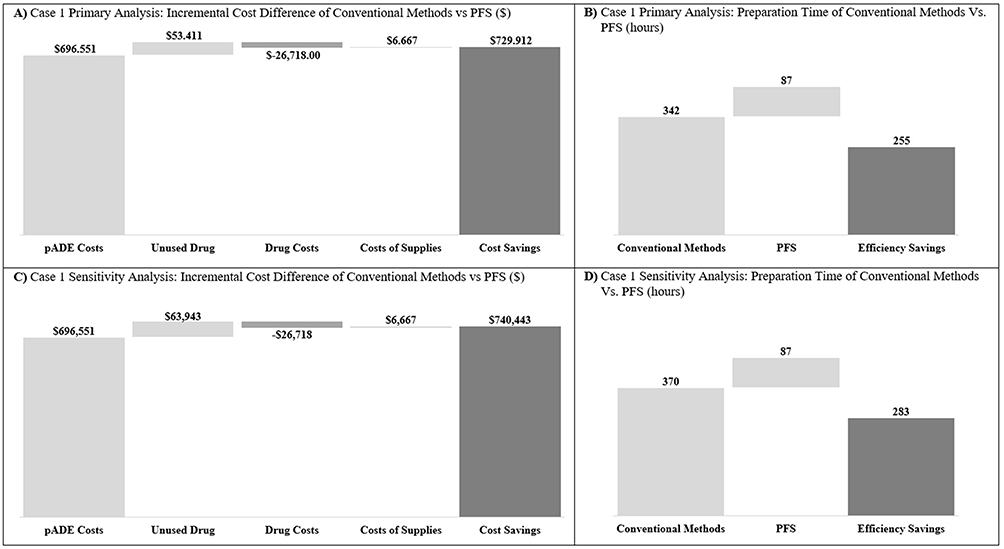 |
Figure 2 Graphical Depiction of Atropine Case Primary Analysis and Sensitivity Analysis Results. (A) Case 1 Primary Analysis: Incremental Cost Difference of Conventional Methods vs PFS ($). (B) Case 1 Primary Analysis: Preparation Time of Conventional Methods Vs PFS (hours). (C) Case 1 Sensitivity Analysis: Incremental Cost Difference of Conventional Methods vs PFS ($). (D) Case 1 Sensitivity Analysis: Preparation Time of Conventional Methods Vs PFS (hours). |
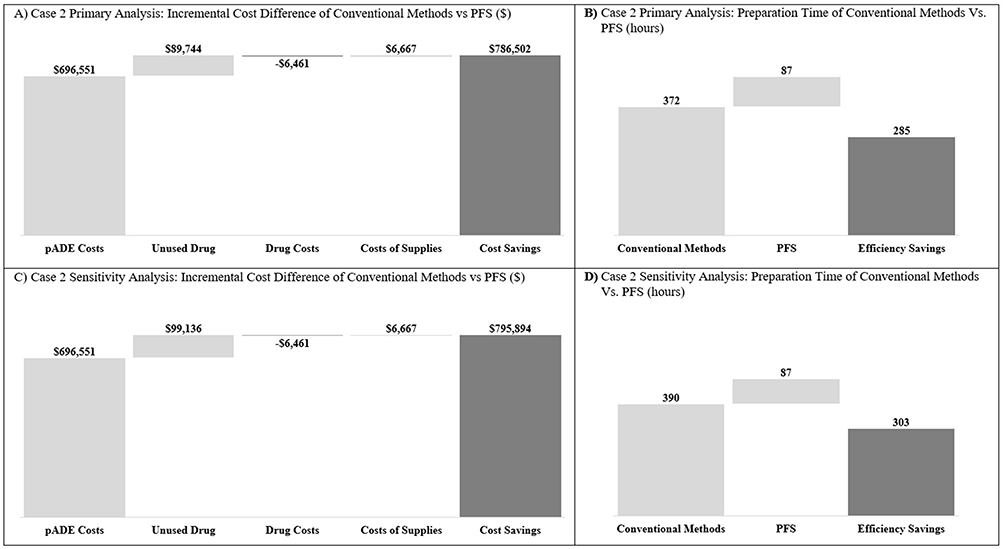 |
Figure 3 Graphical Depiction of Epinephrine Case Primary Analysis and Sensitivity Analysis Results. (A) Case 2 Primary Analysis: Incremental Cost Difference of Conventional Methods vs PFS ($). (B) Case 2 Primary Analysis: Preparation Time of Conventional Methods Vs PFS (hours). (C) Case 2 Sensitivity Analysis: Incremental Cost Difference of Conventional Methods vs PFS ($). (D) Case 2 Sensitivity Analysis: Preparation Time of Conventional Methods Vs PFS (hours). |
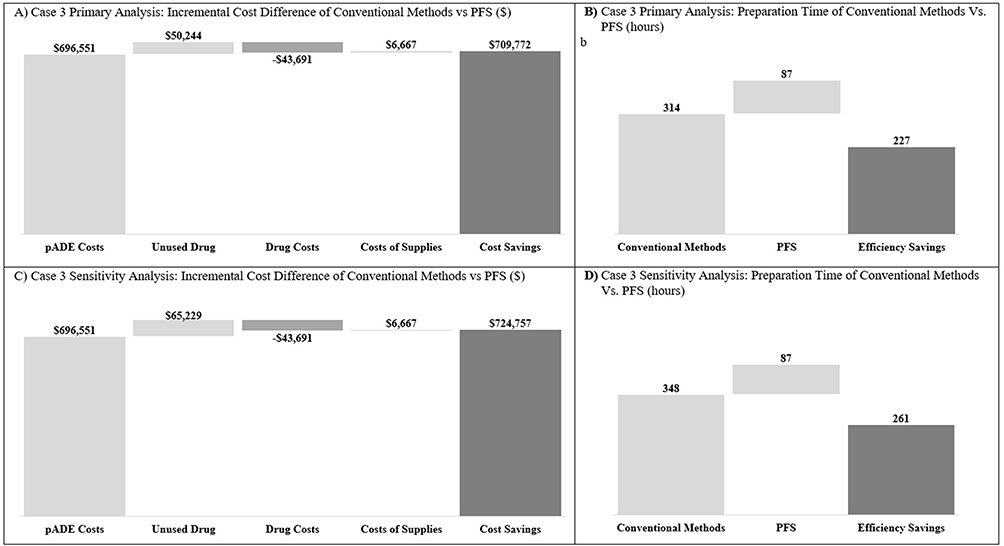 |
Figure 4 Graphical Depiction of Ephedrine Case Primary Analysis and Sensitivity Analysis Results. (A) Case 3 Primary Analysis: Incremental Cost Difference of Conventional Methods vs PFS ($). (B) Case 3 Primary Analysis: Preparation Time of Conventional Methods vs PFS (hours). (C) Case 3 Sensitivity Analysis: Incremental Cost Difference of Conventional Methods vs PFS ($). (D) Case 3 Sensitivity Analysis: Preparation Time of Conventional Methods vs PFS (hours). |
Preventable Adverse Drug Events
The number of pADEs per year decreased from 152 with conventional methods to 80 with prefilled syringes, a reduction of 72 pADEs annually. Given the estimated cost per pADE of $9,721.48, this reduction translated into annual savings of $696,551 due to fewer pADEs (see Tables 3–5).
Cost of Supplies
The total annual savings on ancillary supplies amounted to $6,667. This cost reduction was primarily attributed to the decreased need for additional materials, such as syringes, needles, gloves, and alcohol swabs, since prefilled syringes are preloaded and ready for administration (see Tables 3–5).
Case Study 1
In total, the model estimated annual savings of $729,912 for a hypothetical ICU in the US administering 30 doses/day of atropine when switching from conventional methods to prefilled syringes. The model estimated that 71% of doses prepared using conventional methods were wasted, corresponding to 7,775 doses for atropine in unused doses per year. In contrast, prefilled syringes had no wastage. With the cost per vial dose calculated at $6.87 for atropine, this reduction resulted in annual savings of $53,411. The average preparation time reduction of 37.1 seconds per dose allowed by prefilled syringes of atropine resulted in total hospital staff preparation time savings of 255 hours per year. These cost savings were primarily driven by reductions in pADEs, drug wastage, and preparation time (see Table 3).
Case Study 2
The overall cost savings for administering 30 doses/day of epinephrine is $786,502 per year when switching from conventional methods to prefilled syringes. The model showed that 86% of doses prepared using conventional methods were wasted, or 9,417 epinephrine unused doses per year. Prefilled syringes had no wastage, resulting in the elimination of all wasted doses. Considering the cost per vial dose calculated at $9.53 for epinephrine, this reduction resulted in annual savings of $89,744 annually. Similarly to atropine, prefilled syringes of epinephrine led to total hospital staff preparation time savings of 285 hours per year. Reductions in pADEs, drug wastage, and preparation time were the main contributors of the savings (See Table 4).
Case Study 3
The analysis for case study 3 showed an overall cost savings of $709,772 for a hypothetical ICU in the US administering 30 doses/day of ephedrine when switching from conventional methods to prefilled syringes. The model estimated that 57% of doses prepared using conventional methods were wasted, corresponding to 6,242 for ephedrine in unused doses per year. In comparison, prefilled syringes had no wastage. With the cost per vial dose calculated at $9.31 for ephedrine, this reduction resulted in annual savings of $50,244 annually. Prefilled syringes of ephedrine resulted into total hospital staff preparation time savings of 227 hours per year. These savings were largely attributed to reductions in pADEs and drug wastage (See Table 5).
Sensitivity Analyses
Sensitivity analyses were conducted to test the robustness of the model:
Case Study 1
When increasing the drug wastage of atropine prepared with conventional methods to 85%, the total savings increased from $729,912 to $740,443. In this scenario, the cost of unused drugs rose from $53,411 to $63,943, while preparation time savings increased from 255 hours to 283 hours annually (see Table 3).
Case Study 2
In this scenario, the drug wastage of epinephrine using conventional methods was increased from 86% to 95%. As a result, the total savings rose from $786,502 to $795,894. Under these assumptions, the cost of unused drugs rose from $89,744 to $99,136 and preparation time savings also increased – from 285 hours to 303 hours annually (see Table 4).
Case Study 3
A sensitivity analysis for ephedrine was conducted by increasing conventional method drug wastage to 74% from 57%, leading to the total savings increase from $709,772 of $724,757. The annual cost of unused drugs rose from $50,244 to $65,229, and preparation time savings grew from 227 hours to 261 hours annually (see Table 5). These findings further reinforce the model’s reliability with varying drug wastage assumptions.
Discussion
The economic model results indicated the higher acquisition cost of prefilled syringes may be offset by the cost savings from reduced medication errors, wastage, and supplies use. Findings from the case studies suggest that prefilled syringes can help prevent pADEs, decrease drug wastage, and improve operational efficiency, particularly in high-acuity settings like ICUs.
Medication errors, which often arise from manual dose preparation, remain a major source of preventable harm in healthcare delivery.17,23 By simplifying the administration process, prefilled syringes reduced the number of pADEs from 152 per year to 80 per year. At an estimated cost of $9721.48 per pADE,24,25,28,29 this reduction led to annual savings of $696,551. These case studies underscored the influence of drug pricing on cost savings, particularly through reductions in pADEs and unused doses when compared to conventional methods.
In recent years, many regulatory, accreditation, and professional organizations have turned their focus toward improving medication safety through better standards for clinical practices, labeling, and packaging. The safety benefits of prefilled syringes align well with these efforts, supporting broader goals outlined by the ASHP Guidelines on Preventing Medication Errors in Hospitals and the ISMP Medication Errors Reporting Program.35,36 Moreover, elevated hospitalization costs in the US amplify the economic impact of each pADE, reinforcing the case for adoption. While comparative studies from the UK and France reported lower incremental costs per ADE (£791.61 and €914.25, respectively), these differences largely reflect the varying healthcare cost structures across countries.22 As a result, the US hospital setting presents a unique potential for greater cost reductions through the adoption of prefilled syringes, given the high financial burden of hospitalizations and pADEs in the current system.
In addition to reducing pADEs, prefilled syringes eliminated drug wastage. Conventional methods resulted in 71%, 86%, and 57% wastage for atropine, epinephrine, and ephedrine,19 respectively – amounting to 7775, 9417, and 6242 wasted doses annually. Given the per-dose cost of $6.87, $9.53, and $9.31,33 eliminating this wastage saved $53,411, $89,744, and $50,244 per year for each drug. This reduction in wastage is particularly significant for high-cost drugs or drugs with short shelf lives, where minimizing waste can result in substantial financial benefits.18 Given the variability in drug wastage rates, the sensitivity analysis was conducted to explore how different assumptions could impact overall outcomes, underscoring the value of a customizable model.
Another key benefit of prefilled syringes is the time saved during dose preparation. Prefilled syringes reduced the dose preparation time from 65.8 seconds per vial to 28.7 seconds per syringe, resulting in annual time savings of 255, 285, and 227 hours per year for atropine, epinephrine, and ephedrine, respectively. Although this time savings did not directly impact the cost analysis, it represents a meaningful efficiency gain for hospital staff, freeing up time for more patient-centered tasks. This is especially valuable in high-pressure environments where time management is critical.
Limitations
The model has several limitations. The results are based on data from a specific CICU administering atropine, epinephrine and ephedrine, and while the outcomes are promising, they may not be directly generalizable to other hospital settings or drugs. Future studies should use hospital-specific data to enhance the accuracy and relevance of the model. Additionally, the wastage data was sourced from international studies, as noted above, due to limited U.S.-specific data. However, the model is designed to be customizable and can be updated as new data on drug wastage becomes available, helping to improve its applicability over time. Furthermore, the model did not account for some practical considerations, such as microbial contamination risks, sharps disposal costs, and the storage requirements of prefilled syringes, which may affect the overall cost-effectiveness.12,13 These factors should be considered in real-world implementation.
Implications for Practice
The broader implications of adopting prefilled syringes are worth considering in today’s US healthcare environment. As hospitals face increasing challenges such as staff shortages, rising costs, and the need to improve patient outcomes, the potential safety and efficiency from prefilled syringes may offer some practical benefits. By helping reduce pADEs and drug wastage, and by shortening preparation time, prefilled syringes could support ongoing efforts to improve care delivery and resource use. While not a standalone solution, they may represent a useful option for healthcare decision makers evaluating ways to enhance operational efficiency.
Conclusion
The findings from this study suggest that prefilled syringes may provide both economic and clinical benefits in US hospital settings, including potential cost savings and improved patient safety. These benefits appear especially relevant in high-acuity environments, such as ICUs, where medication errors and wastage can have significant consequences. As healthcare systems continue to face staffing shortages and increasing patient volumes, prefilled syringes may contribute to more streamlined and efficient care delivery.
Data Sharing Statement
Data analyzed during the current study is available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Becton Dickinson and Company.
Disclosure
All authors are employees of Becton, Dickinson and Company. The authors report no other conflicts of interest in this work.
References
1. Benhamou D, Weiss M, Borms M, et al. Assessing the clinical, economic, and health resource utilization impacts of prefilled syringes versus conventional medication administration methods: results from a systematic literature review. Ann Pharmacother. 2024;58(9):921–934. doi:10.1177/10600280231212890
2. Lahue BJ, Pyenson B, Iwasaki K, Blumen HE, Forray S, Rothschild JM. National burden of preventable adverse drug events associated with inpatient injectable medications: healthcare and medical professional liability costs. Am Health Drug Benefits. 2012;5(7):1–10.
3. Keers RN, Williams SD, Cooke J, Ashcroft DM. Prevalence and nature of medication administration errors in health care settings: a systematic review of direct observational evidence. Ann Pharmacother. 2013;47(2):237–256. doi:10.1345/aph.1R147
4. Berdot S, Gillaizeau F, Caruba T, Prognon P, Durieux P, Sabatier B. Drug administration errors in hospital inpatients: a systematic review. PLoS One. 2013;8(6):e68856. doi:10.1371/journal.pone.0068856
5. Leape LL. Errors in Medicine. Complications in Pediatric Surgery. CRC Press; 2008:21–30.
6. Quality AfHRa. Medication Errors and Adverse Drug Events. Patient Safety Network, U.S. Department of Health and Human Services. Available from: https://psnet.ahrq.gov/primer/medication-errors-and-adverse-drug-events,2019.
7. Beauvais B, Kruse CS, Beauvais R, et al. An exploratory analysis of the association between hospital labor costs and the quality of care. Risk Manag Healthc Policy. 2023;16:1075–1091. doi:10.2147/RMHP.S410296
8. Hall K. The financial effects of hospital workforce dislocation. National Health Foundation; 2022. Available from: https://www.kaufmanhall.com/sites/default/files/2022-05/KH-NHFR-Special-Report-2.pdf.
9. U.S. Bureau of Labor Statistics. Occupational outlook handbook: registered nurses. U.S. Department of Labor. Available from: https://www.bls.gov/ooh/healthcare/registered-nurses.htm.
10. Zhang X, Tai D, Pforsich H, Lin VW. United States registered nurse workforce report card and shortage forecast: a revisit. Am J Med Qual. 2018;33(3):229–236. doi:10.1177/1062860617738328
11. American Society of Health-System Pharmacists. Pharmacy Technician Shortage Survey: executive Summary. American Society of Health-System Pharmacists; 2022. Available from: https://www.ashp.org/-/media/assets/pharmacy-technician/docs/Technician-Shortage-Survey-Exec-Summary.pdf.
12. Subhi Y, Kjer B, Munch IC. Prefilled syringes for intravitreal injection reduce preparation time. Dan Med J. 2016;63(4):A5214.
13. Souied E, Nghiem-Buffet S, Leteneux C, et al. Ranibizumab prefilled syringes: benefits of reduced syringe preparation times and less complex preparation procedures. Eur J Ophthalmol. 2015;25(6):529–534. doi:10.5301/ejo.5000629
14. Woller TW, Knoer S, Daniels R. Strategic considerations for centralization of services across the pharmacy enterprise. Am J Health Syst Pharm. 2015;72(1):74–77. doi:10.2146/ajhp140401
15. Pedersen CA, Schneider PJ, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: dispensing and administration—2011. Am J Health Syst Pharm. 2012;69(9):768–785. doi:10.2146/ajhp110735
16. Centers for Medicare & Medicaid Services. Hospital-Acquired Condition (HAC) Reduction Program. CMS.gov. Updated September 10, 2024. Available from: https://www.cms.gov/medicare/quality/value-based-programs/hospital-acquired-conditions.
17. Wazny LD, Raymond CB, Do MK, Skwarchuk DE. Reduced drug costs from switching hemodialysis patients from epoetin alfa in multidose vials to pre-filled syringes. CANNT J. 2009;19(3):39–41.
18. Atcheson CL, Spivack J, Williams R, Bryson EO. Preventable drug waste among anesthesia providers: opportunities for efficiency. J Clin Anesth. 2016;30:24–32. doi:10.1016/j.jclinane.2015.12.005
19. Barbariol F, Deana C, Lucchese F, et al. Evaluation of drug wastage in the operating rooms and intensive care units of a regional health service. Anesth Analg. 2021;132(5):1450–1456. doi:10.1213/ANE.0000000000005457
20. Benhamou D, Piriou V, De Vaumas C, et al. Ready-to-use pre-filled syringes of atropine for anaesthesia care in French hospitals - a budget impact analysis. Anaesth Crit Care Pain Med. 2017;36(2):115–121. doi:10.1016/j.accpm.2016.03.009
21. Larmené-Beld KHM, Spronk JT, Luttjeboer J, Taxis K, Postma MJ. A cost minimization analysis of ready-to-administer prefilled sterilized syringes in a dutch hospital. Clin Ther. 2019;41(6):1139–1150. doi:10.1016/j.clinthera.2019.04.024
22. Eijsink JFH, Weiss M, Taneja A, et al. Creating an evidence-based economic model for prefilled parenteral medication delivery in the hospital setting. Eur J Hosp Pharm. 2024;31(6):564–570. doi:10.1136/ejhpharm-2022-003620
23. Nanji KC, Patel A, Shaikh S, Seger DL, Bates DW. Evaluation of perioperative medication errors and adverse drug events. Anesthesiology. 2016;124(1):25–34. doi:10.1097/ALN.0000000000000904
24. Weiss AJ, Freeman WJ, Heslin KC, Barret ML. Adverse drug events in U.S. Hospitals, 2010 Versus 2014. 2018;234:1.
25. HCUPnet. Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality. Rockville, MD. Available from: https://datatools.ahrq.gov/hcupnet.
26. U.S. Bureau of Labor Statistics. Medical Consumer Price Index. Department of Labor. Available from: https://www.bls.gov/cpi/data.htm.
27. IQVIA. Injectable Drug Universe Data in IQVIA Smart MIDAS; 2023.
28. Panagioti M, Khan K, Keers RN, et al. Prevalence, severity, and nature of preventable patient harm across medical care settings: systematic review and meta-analysis. BMJ. 2019;366:14185. doi:10.1136/bmj.l4185
29. Bysshe T, Gao Y, Heaney-Huls K, et al. Estimating the additional hospital inpatient cost and mortality associated with selected hospital-acquired conditions. Agency Healthcare Res Qual. 2017;2017:1–75.
30. Burger M, Degnan D. Comparative safety, efficiency, and nursing preference among 3 methods for intravenous push medication preparation: a randomized crossover simulation study. J Patient Saf. 2019;15(3):238–245. doi:10.1097/PTS.0000000000000269
31. Diamedical. Shop Products. Available from: https://www.diamedicalusa.com.
32. Adapa RM, Mani V, Murray LJ, et al. Errors during the preparation of drug infusions: a randomized controlled trial. Br J Anaesth. 2012;109(5):729–734. doi:10.1093/bja/aes257
33. Moreira ME, Hernandez C, Stevens AD, et al. Color-coded prefilled medication syringes decrease time to delivery and dosing error in simulated emergency department pediatric resuscitations. Ann Emerg Med. 2015;66(2):97–106.e3. doi:10.1016/j.annemergmed.2014.12.035
34. Cohen MR, Smetzer JL, Vaida AJ, Vaida A. ASHP guidelines on preventing medication errors in hospitals: advancing medication safety to the next level. Am J Health Syst Pharm. 2018;75(19):1444–1445. doi:10.2146/ajhp180283
35. Mauskopf JA, Sullivan SD, Annemans L, et al. Principles of good practice for budget impact analysis: report of the ISPOR task force on good research practices—budget impact analysis. Value Health. 2007;10(5):336–347. doi:10.1111/j.1524-4733.2007.00187.x
36. Institute for Safe Medication Practices. ISMP Medication Errors Reporting Program. PSNet. Published December 14, 2010. Available from: https://psnet.ahrq.gov/issue/ismp-medication-errors-reporting-program.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.