Back to Journals » Clinical Ophthalmology » Volume 18
Improved Glaucoma Medication Access Through Pharmacy Partnership: A Single Institution Experience
Authors Choi JG ![]() , Amin P
, Amin P ![]() , Tarantino A, Qiu M
, Tarantino A, Qiu M ![]()
Received 19 November 2023
Accepted for publication 15 February 2024
Published 2 April 2024 Volume 2024:18 Pages 981—987
DOI https://doi.org/10.2147/OPTH.S450629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jin G Choi,1,2 Pathik Amin,3 Alaina Tarantino,4 Mary Qiu3
1Pritzker School of Medicine, University of Chicago, Chicago, IL, USA; 2Department of Ophthalmology, California Pacific Medical Center, San Francisco, CA, USA; 3Department of Ophthalmology and Visual Science, University of Chicago, Chicago, IL, USA; 4Ambulatory Pharmacy Services, University of Chicago, Chicago, IL, USA
Correspondence: Mary Qiu, Department of Ophthalmology and Visual Science, University of Chicago, Chicago, IL, USA, Tel +1 (773) 702-3937, Email [email protected]
Purpose: A major barrier to glaucoma medication adherence is the patient’s out-of-pocket costs. At the University of Chicago Medical Center (UCMC), the institutional pharmacy piloted a program to query out-of-pocket costs for each patient’s medication list based on their insurance coverage. This study aims to describe the impact of this collaboration between the glaucoma service and the outpatient pharmacy service.
Methods: This study is a single institution, retrospective chart review of glaucoma patients with a formulary inquiry placed by a single glaucoma specialist between 4/1/2020 and 2/28/2022. Main outcome measures included medications before and after formulary inquiries, additional steps required to access the medications (ie, formulary exceptions, prior authorizations, tier exceptions), and out-of-pocket costs.
Results: A total of 343 formulary inquiries, representing 568 individual medication inquiries, were conducted. Out of the 568 medication inquiries, only 78 could be filled for an affordable price without any additional steps. For 45 inquiries, additional steps were required for the medication to become covered at an affordable price. The remaining 445 inquires required additional steps with subsequent denial or prohibitive out-of-pocket costs.
Conclusion: The UCMC workflow provided transparent out-of-pocket costs for patients to access glaucoma medications. This workflow may be cost-effective as it minimizes the burden on the overall system by reducing the number of patients who are unable to fill a prescription at the pharmacy due to issues with coverage or affordability. This model of physician-pharmacy collaboration can guide other institutions to implement similar workflows which directly mitigate costs and improve quality of care.
Keywords: medication, access, cost
Introduction
Glaucoma is the second leading cause of irreversible blindness worldwide,1 estimated to affect over 7 million US adults by 20502–4 and costing approximately $2.86 billion annually.5 Intraocular pressure (IOP) is the only modifiable risk factor, and the primary treatment is a life-long prescription of IOP-lowering eyedrops. The considerable expense can impact patient adherence.6 Poor medication adherence can precipitate uncontrolled IOP, disease progression, and permanent vision impairment, which may require surgical intervention to control.7–13
A major barrier to medication adherence is the out-of-pocket costs faced by patients.14–18 In the United States, this issue is compounded by the complexity and heterogeneity of insurance and pharmacy pricing including formulary drug exclusions, which can be major deterrents to prompt initiation of therapy.19,20 Furthermore, simplifying treatment regimens with fewer medications can also improve patient adherence to therapy.21 Maximizing the likelihood of medication compliance in the first year is particularly important, as adherence patterns over the first year may be predictive of long-term medication adherence and therefore outcomes.22
Patient-physician communication is important,23 but after the face-to-face clinical encounter with the physician, the patient may feel relatively unequipped to effectively navigate the complex pharmacy and insurance system to minimize medication costs according to their personal insurance status and treatment plan. At the University of Chicago Medical Center (UCMC), the institutional pharmacy has piloted a new program during the COVID-19 era whereby a “Pharmacy Medication Access Referral order” can be placed in the electronic medical record (EMR) system to ascertain out-of-pocket costs for any generic or brand-name medications for each individual patient based on their specific insurance coverage. As part of the workflow, patients were always initiated on generic medication options. If medical escalation became required to delay surgical management, potentially more expensive brand-name and combination agents could be considered. Keeping in mind the out-of-pocket cost to the patient, the physician can make an informed determination about which medication to prescribe next or initiate an application for prior authorization, formulary exception, or tier exception, if necessary, which is also facilitated by the pharmacy. Once it has been determined that a specific medication is available to and affordable for the individual patient, the physician can discuss this option with the patient, and only then will the medication be prescribed. Medication prescriptions may then be fulfilled by the institutional outpatient pharmacy and mailed directly to the patient’s home, reducing unnecessary risk of COVID-19 exposure from in-person visits to pharmacy only to discover prohibitively high out-of-pocket medication costs.
This new workflow facilitates a more informed, cost-conscious, and practical real-world conversation between the patient and physician during the in-person visit, where both parties are equipped with the actual out-of-pocket cost patients will face when considering various therapeutic options. The purpose of this study is to quantitatively describe the impact of this multidisciplinary collaboration between the glaucoma service and the ambulatory pharmacy program in facilitating patient access to glaucoma medications at affordable out-of-pocket costs.
Methods
This study is a single institution, retrospective chart review of glaucoma patients at the UCMC who had an “Pharmacy Medication Access Referral order” placed by a single glaucoma specialist (MQ) between 4/1/2020 and 2/28/2022. The study was approved by the UCMC Institutional Review Board (IRB20-2001).
During a patient visit in outpatient glaucoma clinic, the physician could submit a formulary inquiry for various medications through the hospital electronic medical record system (Epic Systems, Verona, WI). Patients were always initiated on generic, presumably more affordable, medications such as generic dorzolamide-timolol, brimonidine, and latanoprost until intraocular pressures were uncontrolled and required an escalation of medical therapy to delay surgical management. Five medications were the focus of most formulary inquiries because they were either brand-name only (eg, Rhopressa, Vyzulta) or combination agents without generic alternatives (eg, Rocklatan, Simbrinza, Combigan; after the study period, in February 2022, Combigan became available as a generic). Additionally, Simbrinza and Combigan were considered as alternatives to generic dorzolamide-timolol for patients with contraindications (eg, asthma/COPD or systemic beta-blocker use as a contraindication to timolol or corneal endothelial issues as a contraindication to dorzolamide).
The institutional pharmacist liaison responded through Epic inbasket messages with out-of-pocket medication costs based on each patient’s current insurance coverages and specified whether the medications were 1) on formulary and covered at a certain out-of-pocket co-pay, 2) on formulary but required prior authorization, or 3) not on formulary. If the medication of interest was on formulary but the out-of-pocket cost was relatively high, a tier exception could be submitted in attempt to lower the out-of-pocket cost. If a prior authorization was required, this application could be submitted, and if approved, an updated out-of-pocket cost could be obtained. If the medication of interest was not on formulary, a formulary exception could be submitted, and if approved, an updated out-of-pocket cost could be obtained. If any of these additional steps were required, the physician authorized application for these additional steps through return Epic in-basket messages to the pharmacy, and the applications would be submitted by the clinical pharmacist to the patient’s insurance company. Subsequent decisions and lowest out-of-pocket costs were relayed from the pharmacy to the physician via Epic message, and ultimately from the physician’s team to the patient via telephone call.
Patients were included in this study if there was at least one formulary inquiry order through the institutional pharmacy during the observed period. For patients with multiple formulary inquiry orders during this period, all instances were included in the study. Demographic information extracted from the electronic medical record included age, sex, race, and insurance status. Additional information collected included starting and final medications after each formulary inquiry and subsequent steps taken, the number of formulary inquiries, formulary exceptions, prior authorizations, and tier exceptions, and the final out-of-pocket costs for each medication per patient.
Results
A total of 343 formulary inquiries for 326 patients met inclusion criteria and were analyzed. The mean age was 71.3 ± 14.0 years, 57% of patients were female, 79% of patients were Black; the primary insurance was 75% Medicare, 18% commercial insurance, 7% Medicaid, and 0.3% uninsured (Table 1). An average of 3.42 Epic in-basket message correspondences between physician and pharmacy were required for each formulary inquiry plus additional steps with initial responses available within 24–48 hours.
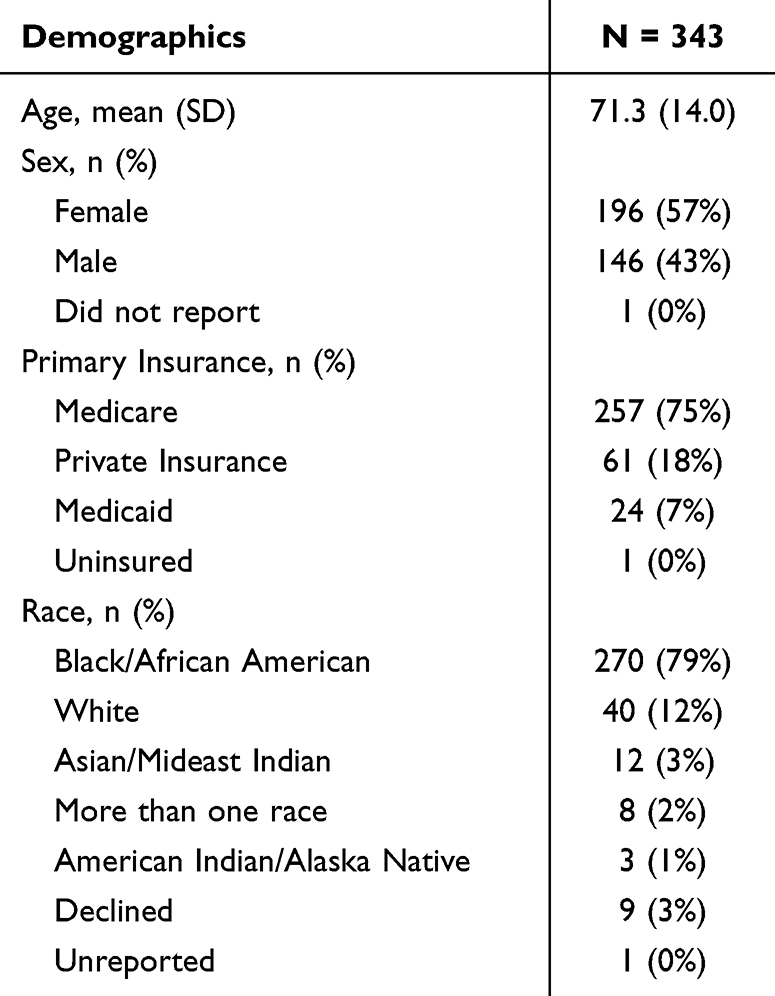 |
Table 1 Demographics |
Table 2 summarizes the formulary inquiry results for the 5 most common medications of interest (ie, Rocklatan, Rhopressa, Simbrinza, Vyzulta, and Combigan), including the percentage of formulary inquiries resulting in medication changes for the patient, the out-of-pocket costs, and the proportion of patients with additional steps required (ie, prior authorizations, formulary exceptions, and tier exceptions). In the absence of published metrics for affordability of out-of-pocket medication costs, the quoted out-of-pocket costs were categorized into 30-day costs of $0 to $10, $11 to $50, $51 to $100, and over $100 to estimate affordability. For approximately 40–46% of formulary inquiries plus additional steps, the final out-of-pocket cost was within the lowest cost category of $0 to $10 per 30-day supply. Of note, 13–20% of formulary inquiries plus additional steps still yielded out-of-pocket costs of greater than $100 per 30-day supply resulting in the medication being cost prohibitive. These medications were not added to the patient’s existing regimen either because medication escalation could be deferred for now, or the quoted out-of-pocket cost was too high for the patient. For each medication, the majority (57–100%) of additional steps required after the initial formulary inquiry was submitting an application for formulary exception.
 |
Table 2 Summary of All Formulary Inquiries |
The initial response to each formulary inquiry from the pharmacy is described for the 5 medications of interest in patients not already on the medication. A total of 211 formulary inquiries were made about Rocklatan for patients not already on Rocklatan; the results were 59% covered, 38% not on formulary, and 4% requiring prior authorizations (Table 3). A total of 152 formulary inquiries were made about Rhopressa for patients not already on Rhopressa; the results were 87% covered, 11% not on formulary, and 3% requiring prior authorizations. A total of 112 inquiries were made about Simbrinza for patients not already on Simbrinza; the results were 89% covered, 8% not on formulary, and 4% requiring prior authorizations. A total of 90 inquiries were made about Vyzulta for patients not already on Vyzulta; the results were 77% covered, 18% not on formulary, and 6% requiring prior authorizations. A total of 3 inquiries were made about Combigan for patients not already on Combigan; the results were 33% covered, 67% not on formulary, and 0% requiring prior authorizations.
 |
Table 3 Formulary Inquiries for New Pharmacologic Agents |
A subset of patients were able to have their medication of interest covered (40–80% depending on medication) by their insurance at an affordable out-of-pocket cost of $0-$10 per 30-day supply (Table 3). Unfortunately, there was still a substantial number of patients (11–53% depending on medication) whose insurance did not cover the medications of interest despite additional steps performed (eg, formulary exception, tier exception, prior authorization). For these patients, the workflow spared them the physical and emotional demands of visiting a pharmacy in person only to find out that the medication was not affordable.
Discussion
Many factors affecting glaucoma medication adherence have been described in literature including doctor-patient communication, patient’s health-related beliefs, and financial barriers. While various patient education programs have been implemented to address medication nonadherence, affordability of glaucoma medications has been identified as a major barrier for up to 25% of patients.24–26 Institutionally addressing the financial barriers to medication access is particularly difficult given the complexity of the United States payment structure and individual patient circumstances and concerns. Furthermore, we hope that in the future insurance companies will place newer brand-name medications on their formularies to minimize the logistical steps required for patients to gain access to appropriate medical therapies. To our knowledge, no other studies have been published proposing an institutional program to confront patient-level financial barriers to glaucoma medication access.
In our study, 343 discrete formulary inquiries, representing 568 instances of individual medication inquiries (since each formulary inquiry may include multiple medications for one patient), were conducted. For the purpose of simplifying the discussion, we can imagine each individual medication inquiry as a single individual patient at the pharmacy fulfilling a single medication prescription, although in reality, some individual patients had multiple medication inquiries for multiple different medications simultaneously. If we had sent in the prescribed medication for these 568 patients (211 Rocklatan, 152 Rhopressa, 112 Simbrinza, 90 Vyzulta, 3 Combigan) to their pharmacy, only 78 patients (31 Rocklatan, 6 Rhopressa, 24 Simbrinza, 17 Vyzulta, 0 Combigan) would have been able to pick up the prescribed medication on that day without any additional steps (Table 3). For another 45 patients (35 Rocklatan, 4 Rhopressa, 3 Simbrinza, 3 Vyzulta, 0 Combigan), the medications were not accessible without additional steps (ie, prior authorization, formulary exception, tier exception). The majority of these 123 patients (78 plus 45) who were able to successfully start a new medication would have predominantly paid in the most affordable category of $0-$10 per 30-day supply for the medication of interest (ie, 80% for Rocklatan, 75% for Vyzulta, and 70% for Simbrinza – the percentage represents the percentage of patients who were able to start that medication at a cost of $0-$10 per 30-day supply). Through this workflow, we were able to appropriately identify the 123 patients out of 568 total who would successfully access their new medications at an affordable price without requiring them to physically visit a pharmacy. The remaining 445 patients (145 Rocklatan, 142 Rhopressa, 85 Simbrinza, 70 Vyzulta, 3 Combigan) would have been spared the need to physically visit a pharmacy to fill a prescription to be quoted prohibitive out-of-pocket costs or require additional insurance authorization steps with subsequent denial. Many of these 445 patients who did not start a new medication would have been quoted an out-of-pocket 30-day supply price in the most expensive category of greater than $100 (ie, 22% for Rocklatan, 20% for Rhopressa, 19% for Vyzulta, and 16% for Simbrinza), supporting the prior literature that high cost can be a significant barrier to medication access.
A large proportion of patients did not have medications added to their regimen following the formulary inquiry and additional step process. Ultimately, affordability is a personal metric for each patient and using the out-of-pocket cost category of greater than $100 per 30-day supply may be an oversimplification of this issue. Additionally, many formulary inquiries were issued preemptively for potential escalation therapy options in patients stable enough to be managed on their current regimens. While not all formulary inquiries resulted in medications being added to patient regimens, this workflow provided valuable information to both patient and physician to help guide future management decisions.
There are several limitations to our study. First, as a single institution experience at a tertiary academic medical center, the generalizability of our findings are limited especially considering the heterogeneity of out-of-pocket costs based on insurance coverage across insurance companies, geographic regions, and individual patient deductibles.27 The formulary restrictions may not be transferable to other states or institutions. However, we anticipate that the outlined model of physician-pharmacy collaboration can serve to guide other institutions to consider implementing similar workflows to directly mitigate the out-of-pocket medication costs for patients to improve quality of care. There is a nontrivial cost to implementing this workflow given the additional demand on pharmacy personnel to file and process the paperwork required for formulary inquiries and subsequent additional steps. This may be offset by the amount of time saved by reducing the number of patients who arrive at the pharmacy counter to fill a prescription but are ultimately unable to purchase the medication of interest due to additional steps required or high out-of-pocket costs. The proposed workflow could ideally filter all patient-pharmacy interactions to only medication prescriptions that are known by all three parties (patient, physician, and pharmacy) to be a guaranteed available and affordable option, ultimately improving pharmacy workflow efficiency. Furthermore, prior economic analyses have suggested improving glaucoma medication adherence is cost-effective from a societal perspective as well.28 In this study, we were unable to reliably capture the out-of-pocket medication costs prior to the formulary inquiry step which would have allowed for a more robust, quantitative cost analysis. Additional prospective analyses would be particularly helpful in quantifying the invasive IOP-lowering surgical interventions avoided or delayed by improving access to affordable glaucoma medications which may be a particularly important outcome measure. Our statistical method was limited by the comparator data available. Unfortunately, we were unable to reliably collect cost data on patients’ out-of-pocket costs prior to the initiation of our study. The out-of-pocket medication costs were directly obtained from pharmacy running each medication under the patient’s individual insurance at a specific point in time. We were unable to retroactively collect out-of-pocket costs for a patient in a similar methodology or through patient responses as the reliability of the responses were poor. Similarly, we found randomization of patients between lowering out-of-pocket costs versus no intervention to be unethical during a pandemic where patients were already under significant financial strain and vulnerable to poor medical management. In hopes of improving access to affordable medical care during a time of poor access globally, we made the decision to forgo a more rigorous statistical analysis. Ultimately, the results of our initiatives led to a considerable increase in medication coverage and lowering out-of-pocket costs for the entire subject population.
The UCMC workflow was effective in providing absolute transparency of out-of-pocket glaucoma medication costs for patients in a timely manner and facilitating pragmatic goal-oriented conversations between the patient and physician, resulting in enhanced access to appropriate glaucoma medications. Up to 77% of physicians have demonstrated difficulty advising patients on out-of-pocket costs for medications due to the complexity of payment structures in the United States across medical specialties.29 This transparent workflow directly mitigates any potential misinformation, therefore, improving the patient–physician relationship beyond the ophthalmologic setting as well, since the UCMC pharmacy order set is made available to any department inquiring about any medication. The efficient workflow and time saved by determining out-of-pocket costs and relaying this information to patients may positively impact patient access as well. The improved access has the potential to improve medication adherence18,21,24,26 and glaucoma management since a significant barrier to medication access is directly addressed, as transparently as possible.
Ethics and Consent Statements
Informed consent for retrospective chart review not required given no more than minimal risk to subjects, and data confidentiality was maintained and storage in compliance with Declaration of Helsinki.
Acknowledgment
This paper was presented at a conference as a poster presentation at ARVO 2023 and AGS 2023 (https://iovs.arvojournals.org/article.aspx?articleid=2785985).
Funding
No funding was received for conducting this study.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Kingman S. Glaucoma is second leading cause of blindness globally. Bull World Health Organ. 2004;82(11):887–888.
2. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–267. doi:10.1136/bjo.2005.081224
3. Friedman DS, Wolfs RC, O’Colmain BJ, et al. Prevalence of open-angle glaucoma among adults in the United States. Arch Ophthalmol. 2004;122(4):532–538.
4. Vajaranant TS, Wu S, Torres M, Varma R. The changing face of primary open-angle glaucoma in the United States: demographic and geographic changes from 2011 to 2050. Am J Ophthalmol. 2012;154(2):303–314 e303. doi:10.1016/j.ajo.2012.02.024
5. Malvankar-Mehta MS, Feng L, Hutnik CM. North American cost analysis of brand name versus generic drugs for the treatment of glaucoma. Clinicoecon Outcomes Res. 2019;11:789–798. doi:10.2147/CEOR.S156558
6. Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120(10):1268–1279. doi:10.1001/archopht.120.10.1268
7. The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130(4):429–440. doi:10.1016/S0002-9394(00)00538-9
8. Burr J, Azuara-Blanco A, Avenell A, Tuulonen A. Medical versus surgical interventions for open angle glaucoma. Cochrane Database Syst Rev. 2012;9:CD004399. doi:10.1002/14651858.CD004399.pub3
9. Richter GM, Coleman AL. Minimally invasive glaucoma surgery: current status and future prospects. Clin Ophthalmol. 2016;10:189–206. doi:10.2147/OPTH.S80490
10. Kim CY, Park KH, Ahn J, et al. Treatment patterns and medication adherence of patients with glaucoma in South Korea. Br J Ophthalmol. 2017;101(6):801–807. doi:10.1136/bjophthalmol-2016-308505
11. Chen PP. Blindness in patients with treated open-angle glaucoma. Ophthalmology. 2003;110(4):726–733. doi:10.1016/S0161-6420(02)01974-7
12. Kooner KS, AlBdoor M, Cho BJ, Adams-Huet B. Risk factors for progression to blindness in high tension primary open angle glaucoma: comparison of blind and nonblind subjects. Clin Ophthalmol. 2008;2(4):757–762. doi:10.2147/OPTH.S3139
13. Paula JS, Furtado JM, Santos AS, Coelho Rde M, Rocha EM, Rodrigues Mde L. Risk factors for blindness in patients with open-angle glaucoma followed-up for at least 15 years. Arq Bras Oftalmol. 2012;75(4):243–246. doi:10.1590/S0004-27492012000400004
14. Sleath B, Robin AL, Covert D, Byrd JE, Tudor G, Svarstad B. Patient-reported behavior and problems in using glaucoma medications. Ophthalmology. 2006;113(3):431–436. doi:10.1016/j.ophtha.2005.10.034
15. Schmier JK, Halpern MT, Jones ML. The economic implications of glaucoma: a literature review. Pharmacoeconomics. 2007;25(4):287–308. doi:10.2165/00019053-200725040-00003
16. Patel SC, Spaeth GL. Compliance in patients prescribed eyedrops for glaucoma. Ophthalmic Surg. 1995;26(3):233–236.
17. Alexander GC, Casalino LP, Meltzer DO. Patient-physician communication about out-of-pocket costs. JAMA. 2003;290(7):953–958. doi:10.1001/jama.290.7.953
18. Dreer LE, Girkin C, Mansberger SL. Determinants of medication adherence to topical glaucoma therapy. J Glaucoma. 2012;21(4):234–240. doi:10.1097/IJG.0b013e31821dac86
19. Rodin HA, Heaton AH, Wilson AR, Garrett NA, Plocher DW. Plan designs that encourage the use of generic drugs over brand-name drugs: an analysis of a free generic benefit. Am J Manag Care. 2009;15(12):881–888.
20. Egilman AC, Wallach JD, Ross JS, Dhruva SS. Medicare spending and potential savings on brand-name drugs with available generic substitutes excluded by 2 large pharmacy benefit managers, 2012 through 2015. JAMA Intern Med. 2018;178(4):567–569. doi:10.1001/jamainternmed.2017.8016
21. Sleath B, Blalock SJ, Covert D, Skinner AC, Muir KW, Robin AL. Patient race, reported problems in using glaucoma medications, and adherence. ISRN Ophthalmol. 2012;2012:902819. doi:10.5402/2012/902819
22. Newman-Casey PA, Blachley T, Lee PP, Heisler M, Farris KB, Stein JD. Patterns of glaucoma medication adherence over four years of follow-up. Ophthalmology. 2015;122(10):2010–2021. doi:10.1016/j.ophtha.2015.06.039
23. Slota C, Davis SA, Blalock SJ, et al. Patient-physician communication on medication cost during glaucoma visits. Optom Vis Sci. 2017;94(12):1095–1101. doi:10.1097/OPX.0000000000001139
24. Friedman DS, Hahn SR, Gelb L, et al. Doctor-patient communication, health-related beliefs, and adherence in glaucoma results from the Glaucoma Adherence and Persistency Study. Ophthalmology. 2008;115(8):1320–1327, 1327 e1321–1323. doi:10.1016/j.ophtha.2007.11.023
25. Newman-Casey PA, Niziol LM, Lee PP, Musch DC, Resnicow K, Heisler M. The impact of the support, educate, empower personalized glaucoma coaching pilot study on glaucoma medication adherence. Ophthalmol Glaucoma. 2020;3(4):228–237. doi:10.1016/j.ogla.2020.04.013
26. Gupta D, Ehrlich JR, Newman-Casey PA, Stagg B. Cost-related medication nonadherence in a nationally representative US population with self-reported glaucoma. Ophthalmol Glaucoma. 2021;4(2):126–130. doi:10.1016/j.ogla.2020.08.010
27. Arora V, Moriates C, Shah N. The challenge of understanding health care costs and charges. AMA J Ethics. 2015;17(11):1046–1052.
28. Newman-Casey PA, Salman M, Lee PP, Gatwood JD. Cost-utility analysis of glaucoma medication adherence. Ophthalmology. 2020;127(5):589–598. doi:10.1016/j.ophtha.2019.09.041
29. Sloan CE, Millo L, Gutterman S, Ubel PA. Accuracy of physician estimates of out-of-pocket costs for medication filling. JAMA Network Open. 2021;4(11):e2133188. doi:10.1001/jamanetworkopen.2021.33188
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Early Real-World Safety and Short-Term Outcomes of Combined iStent Infinite and Intracameral Travoprost Implant (iDose TR) with or without Cataract Surgery
Yadgarov A
Clinical Ophthalmology 2026, 20:597257
Published Date: 20 May 2026