")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Implications of Atopic Dermatitis on the Quality of Life of 6–11 Years Old Children and Caregivers (PEDI-BURDEN)
Authors Neri I, Galli E, Baiardini I , Picozza M, Rossi AB, Matruglio P, Moretti D, Cipriani F
Received 10 January 2023
Accepted for publication 20 March 2023
Published 12 April 2023 Volume 2023:16 Pages 383—396
DOI https://doi.org/10.2147/JAA.S404350
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Iria Neri,1 Elena Galli,2 Ilaria Baiardini,3,4 Mario Picozza,5,6 Ana B Rossi,7 Paolo Matruglio,8 Devis Moretti,8 Filippo Cipriani8
1Dermatology Unit, IRCCS Azienda Ospedaliero Universitaria Bologna, University of Bologna, Bologna, Italy; 2UOS Immuno-Allergologia dell’Età evolutive, Ospedale S.Pietro-Fatebenefratelli, Rome, Italy; 3Respiratory Unit for Continuity of Care, IRCCS, Ospedale Policlinico San Martino, Genova, Italy; 4Personalized Medicine Asthma, & Allergy Clinic, IRCCS Humanitas Research Hospital, Milan, Italy; 5National Association of Atopic Dermatitis (ANDeA), Prato, Italy; 6Neuroimmunology Unit, Santa Lucia Foundation IRCCS, Rome, Italy; 7Sanofi, Cambridge, MA, USA; 8Sanofi, Milan, Italy
Correspondence: Filippo Cipriani, Sanofi, Viale Bodio 37b, Milan, Italy, Email [email protected]
Purpose: Atopic dermatitis (AD) is a chronic, relapsing and remitting inflammatory skin disease characterized by intense itch. The disease burden includes physical limitations, psychosocial discomfort, and a reduced quality of life (HRQoL). This study presents the results of a parent-reported survey on the psychosocial impact of AD on Italian pre-adolescent children (6– 11 years old), with a specific focus on bullying, self-isolation, absenteeism, and presenteeism.
Methods: An online questionnaire was sent to 3067 random recipients and 160 matched the inclusion criteria for age, self-reported AD diagnosis, localizations (according to ISAAC), and disease severity (POEM ≥ 8). 100 children, with comparable ages, not matching the inclusion criteria for AD, were recruited as a control group.
Results: Children with AD and their caregivers had a significantly lower quality of sleep (QoS) compared to the control group. The presence of AD was directly responsible for many restless nights, both in children and caregivers (58.9 and 55.4 respectively). Children with AD and their parents also experienced significantly more daytime drowsiness (43.6 and 54.6 days, respectively). Children with AD were more frequently victims of bullying at school (20.0% vs 9.0%; p≤ 0.05) or in other social environments (16.9% vs 3.0%; p≤ 0.05). AD caused 17.7 days of absenteeism and 20.1 days of presenteeism per student over the previous 12 months, accounting for 37.8 days of study impairment overall. Severe/very severe AD had a significantly greater impact on presenteeism than moderate AD (25.1 vs 17.5 days; p≤ 0.05). Presenteeism, which was more pronounced among bullied students, was positively correlated with absenteeism only in the AD cohort.
Conclusion: AD has a detrimental impact on the HRQoL of pediatric patients, causing stigmatization and social isolation. Functional distress was also reported by caregivers. Our study might inform the public and policymakers about the disease burden of AD at a young age.
Keywords: atopic dermatitis, absenteeism, presenteeism, sleep impairment, daily drowsiness
Introduction
Atopic dermatitis (AD) is a chronic, relapsing, and remitting inflammatory skin disease, affecting up to 20% of children worldwide. In Italy, the overall prevalence of AD in children is 17.6%, 34.2% with moderate, and 5% with severe disease manifestations.1
AD, whose primary manifestations include xerosis, eczematous lesions, and lichenification is more commonly localized on the neck, hands, feet, face, and on the flexural surfaces of the body.2–4 AD lesions have also an age-related distribution: infants often present with widely distributed xerosis and acute skin lesions, typically on the face, cheeks, and trunk. In childhood, the eczematous and exudative lesions are more localized (typically to the flexor surfaces. AD lesions in adolescents and adults can be either diffuse or localized, typically affecting hands, eyelids, and flexures).2,3
Itch, or pruritus, is a defining symptom of AD and the most burdensome clinical manifestation.5–7 The consequences of pruritus extend far beyond physical distress to include great psychosocial discomfort and social stigma. AD is associated with sleep disturbances and prolonged sleep deprivation may result in irritability, lack of concentration, depression, and anxiety.8–12 AD is also associated with psychological comorbidities in children and their caregivers, behavioral issues, and a substantial reduction in health-related quality of life (HRQoL).13,14
Altogether, AD has a profound impact on the social development of affected children, who feel ashamed, miss school days, give up sports activities, spend more time by themselves, and may have fewer friends than their non-AD peers, particularly in presence of severe AD.15 Due to the visible nature of the disease, children with AD are also victims of disease-related stigmatization.16,17 Bullying, with rates varying across studies from ≤10% to 60%,18–21 further undermines children’s self-esteem which, in turn, further increases their risk of being victimized,13 resulting in a vicious circle of psychosocial distress.
AD affects not only children but also their families. However, limited research has been conducted on parents of children with AD. AD has a great impact on the HRQoL of families, is time-consuming, and expensive. Parents may lose workdays or be less productive at work due to poor quality of sleep.22–26
In the year 2000, the point prevalence of AD in Italian schoolchildren was estimated to be 5.8% (with a lifetime prevalence of 15.2%) and was strongly associated with the presence of AD in at least one parent.27 In the last few decades, the Italian scientific community has committed to the diagnosis, management, and understanding of the burden of AD in children, adolescents, and adults. Compared to controls, AD children up to 7 years old, as well as family members, showed a moderate alteration of the HRQoL. Itching, sleep disturbance, cost of disease management, tiredness, and irritability of parents caused by the disease contributed to reduce HRQoL.28 A second study of children aged 1–12 found a strong association between severe AD and poor HRQoL of both children and their mothers.29 A recent Italian study described the high social stigma associated with AD, showing that 2 out of 5 adolescents with AD are victims of bullying and more than 3 out of 10 adults with AD suffer discrimination in the workplace. Notably, bullying and discrimination were positively associated with rates of absenteeism and presenteeism.21
The limited data on bullying, self-isolation, absenteeism, and presenteeism in preadolescent children and the burden of the disease on their caregivers stimulated our interest. Here we present the results of a parent-reported survey on the psychosocial impact of AD on Italian children aged 6–11 years and their caregivers.
Materials and Methods
Study Design
This study was based on data collected through Computer Assisted Web Interviews (CAWI). An online semi-structured and self-administered questionnaire was sent randomly by email to a sample of a nationally representative population database (DOXA, Milan, Italy). Data were gathered between September and December 2021.
Questionnaire Development
The CAWI questionnaire was aimed at understanding the emotional and physical impact of AD on children and their caregivers compared to their non-AD counterparts. The questionnaire, administered in Italian, required approximately 30 minutes to be completed and was divided into two sections. The first section (screening) was aimed at assessing whether responders were eligible for the study, whereas the second section contained the research questions, based on a review of the relevant literature.30–32 The survey included open/closed questions, multiple choice questions, 5-point Likert-scale questions, 11-point rating scale questions, and in-depth open-ended questions.
Absenteeism was measured in terms of school absences, late entries, or early exits; presenteeism was defined as the difficulty in remaining focused and concentrated at school or while doing homework at home. Overall study impairment was defined as the sum of absenteeism and presenteeism. Bullying was investigated both explicitly with direct questions, and indirectly, by presenting some daily situations.
Data Analysis
Statistical analyses were performed using the Diana software version 2.06.019 (NIPO, Amsterdam, The Netherlands). The internal consistency of the questionnaire was measured using Cronbach’s α coefficient. Categorical variables were compared using the χ2 test. For continuous variables, non-parametric Spearman correlation tests were used. Statistical significance was set at p≤0.05 (two tailed).
Study Population
Participants were enrolled according to age (6–11 years), ISAAC criteria (presence of itchy rashes for at least 6 months in the past year, and affecting the inside of the elbows, the region around the knees/ankles, under the buttocks, or around the neck, ears, or eyes),33 self-reporting an AD diagnosis by a healthcare professional and a POEM disease severity score ≥8.26,33,34
Results
Population Characteristics and Clinical Manifestations of AD
The questionnaire was sent to 3067 recipients and was completed by 1231 respondents. The final study population consisted of 160 children with AD and a control group of age-matched 100 children without AD who were randomly selected among respondents who did not match the inclusion criteria (Supplementary Figure 1). Demographic and clinical data are summarized in Table 1.
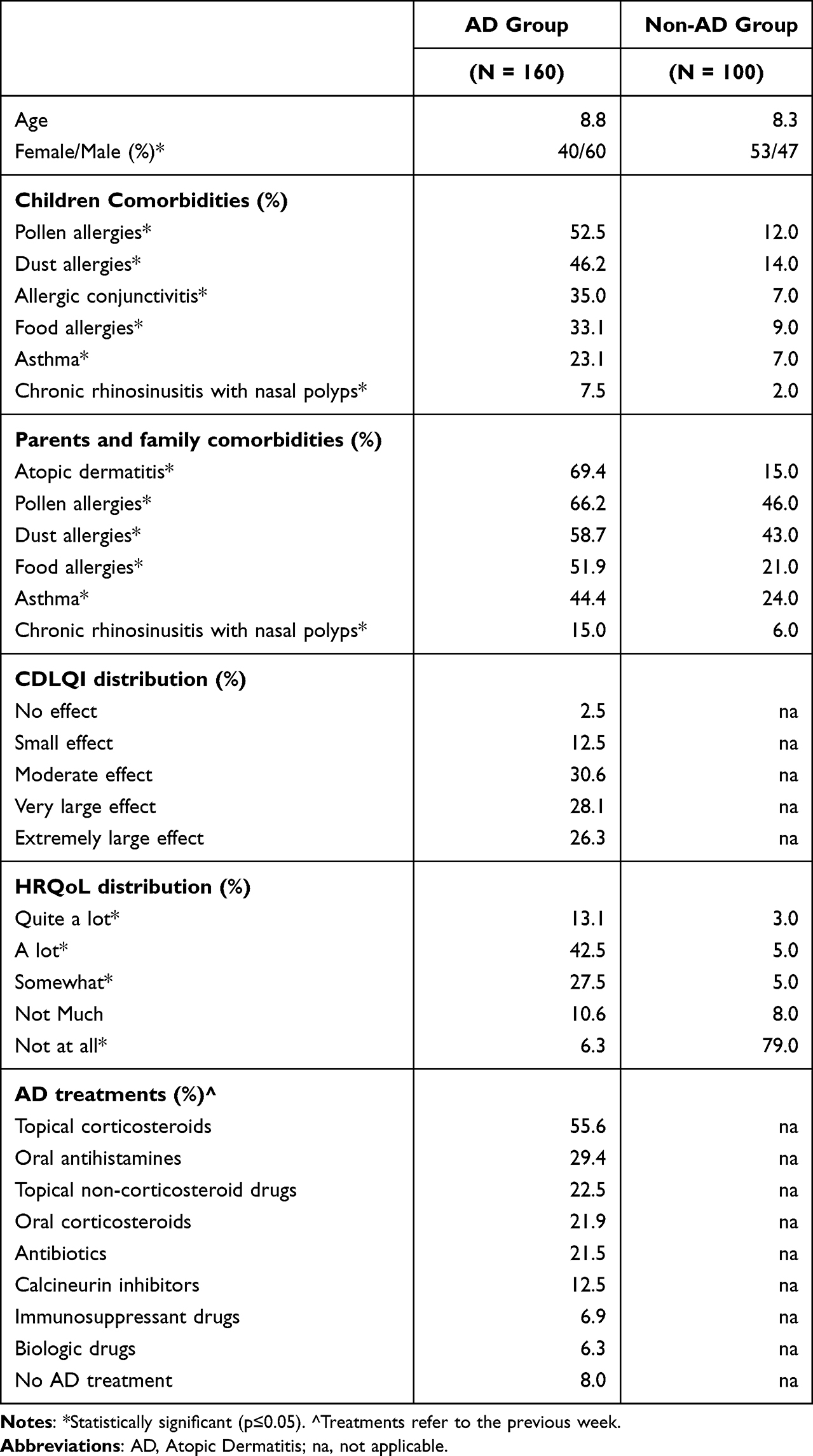 |
Table 1 Demographic and Clinical Data of the Final Study Population |
The AD population presented a significantly higher number of comorbidities than controls (4.1 vs 1.0; p≤0.05); comorbidities were typically allergies (pollen, dust, food), allergic conjunctivitis, allergic rhinitis, and asthma. Parents, siblings, and close relatives (grandparents, uncles, cousins) of AD children showed similar patterns of comorbidity (3.8 vs 1.3; p≤0.05), where AD was the most frequent condition (69.4%), followed by allergies, asthma, and chronic rhinosinusitis with nasal polyps. The first AD manifestations developed on average at 5 years of age (15.6% before 2 years of age). Diagnosis of AD was made by dermatologists (51.2%), pediatricians (29.4%), allergists/immunologists (14.4%), or general practitioners (GP) (5.0%).
According to the POEM score, 66.2% had a moderate disease. Severe and very severe AD accounted for the remaining 28.8% and 5.0%, respectively. Interestingly, when asked directly about the perceived severity of the disease, 13.8% of caregivers underestimated the severity of their children’s AD, classifying as mild/clear skin what was classified as moderate according to the POEM score.
AD affected exposed/visible areas of the body of 93.7% of children. In most cases (59.4%), AD affected 25% to 50% of the body surface area (BSA), with 5.6% of children reporting a >50% BSA involvement. Face (40.0%), hands (12.5%), and arms (11.3%), which were perceived as the body parts most visible to others (85.9%, 75.0%, and 83.3%, respectively), were considered the localizations with the highest social impact.
At the moment of the survey, children were seeing more than one physician (mean 2.2), including a dermatologist (81.9%), a pediatrician (75.6%), an allergist/immunologist (34.4%) or a GP (30.0%). Approximately half of the children reported consulting the dermatologist (47.9%), the pediatrician (50.0%) or the GP (46.4%) once every 2–3 months. In the previous week, only 51.9% used specific detergents and 48.7% moisturizing creams, 92% were on active treatment for AD, whereas 8% were not, primarily for fear of corticosteroids. In the past year, despite the support of multiple physicians and the availability of alternative treatments, 91.9% of parents reported at least one flare of the disease (mean value 7.6 flares); in 30.0% of cases, flares required a visit to the emergency room (mean value 2.9 visits) and in 15.0% of cases, a hospitalization (mean value 2.5 admissions).
HRQoL, Daily Limitations, Relationships and Feelings
AD had a very large effect on children’s lives (mean CDLQI score 13.8), with an “extremely large effect” for 1 out of 4 children (26.3%). The perceived HRQoL varied largely across groups, with 55.6% of responders in the AD group reporting a negative perception vs 8.0% in the control group (p≤0.05) (Table 1).
In daily routine, AD-related limitations overcome any other health-related limitations (63.1% vs 13.1%; p≤0.05) whereas only 6.0% in the non-AD group reported health-related limitations in their daily routine (Figure 1A).
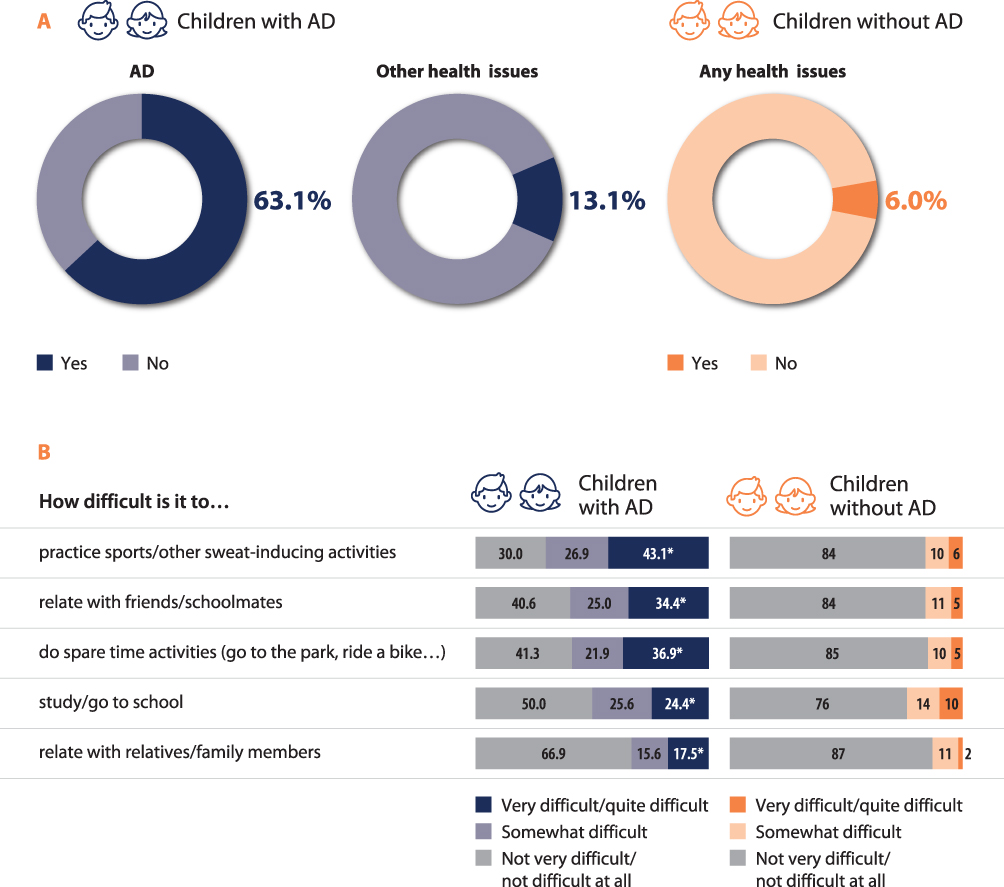 |
Figure 1 Limitations and implications on daily activities. Abbreviation: AD, atopic dermatitis. Notes: AD and non-AD related limitations in the AD group vs any health limitation in the non-AD group (A); specific daily limitations in the AD population (B). *Statistically significant (p≤0.05). |
Referring to the previous week, and compared to their counterparts, children with AD more often experienced difficulties in practicing sport (43.1% vs 6.0%; p≤0.05) or leisure activities (36.9% vs 5.0%; p≤0.05), in studying/going to school (24.4% vs 10.0%; p≤0.05), in interacting with their school friends (34.4% vs 5.0%; p≤0.05) or family members (17.5% vs 2.0%; p≤0.05) (Figure 1B). Children with AD also gave up extracurricular activities more frequently than those in the non-AD group. (45.6% vs 10.0%; p≤0.05).
Data also show the substantial emotional burden of AD. Compared to controls, children with AD reported more frequently negative feelings, such as uneasiness-embarrassment (39.4% vs 1.0%; p≤0.05), judgment by others-shame (31.9% vs 5.0%; p≤0.05) and worry-uncertainty (24.4% vs 9.0%; p≤0.05) and less often positive feelings such as calm-tranquility (16.3% vs 42.0%; p≤0.05), strength-determination (13.1% vs 27.0%; p≤0.05) and peace freedom (11.3% vs 58.0%; p≤0.05) (Figure 2A).
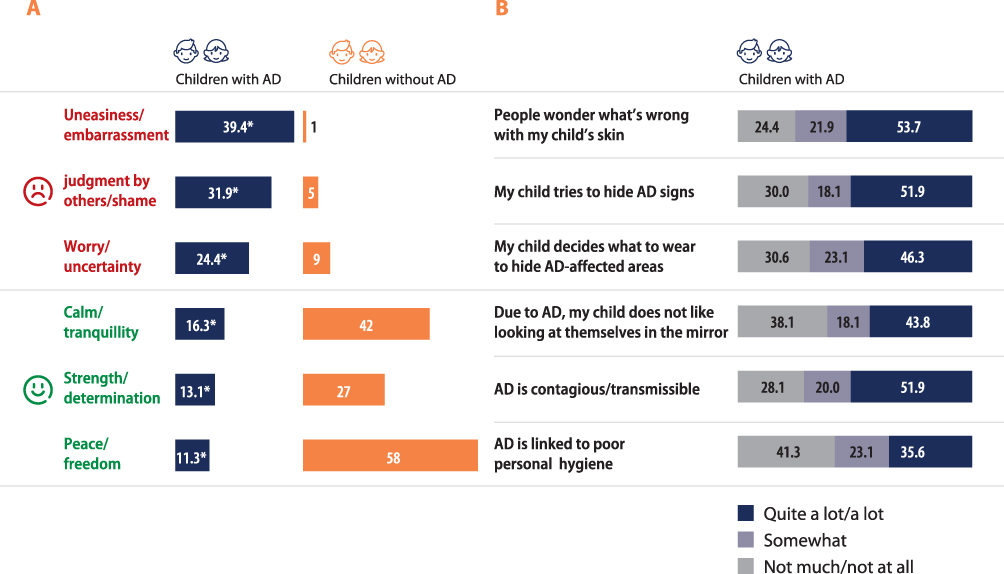 |
Figure 2 Emotional burden. Abbreviation: AD, atopic dermatitis. Notes: Emotional burden of atopic dermatitis expressed as positive and negative feelings (A). (B) shows behaviors and beliefs associated with atopic dermatitis. *Statistically significant (p≤0.05). |
Children with AD did not feel comfortable with their condition from a personal perspective. More than 1 in 2 children believed that other people wondered what was wrong with their skin (53.7%) and covered their skin to prevent others from seeing any sign of AD (51.9%), mostly with an adequate choice of clothes (46.3%), or did not look at themselves in the mirror, as reported by about 2 out of 5 children. The data also captured common beliefs about AD such as, according to our participants, the general population thinking that AD is contagious (51.9%) or associated to poor personal hygiene (35.6%) (Figure 2B).
Quality of Sleep and Daily Drowsiness
AD has a great impact on the quality of sleep (QoS) of children. During the past week, 60% of them had a poor QoS compared to only 1% of their non-AD peers (p≤0.05), with 61.3% reporting sleep problems for 3 or more nights and 23.1% for 5–7 nights. Data also suggested a negative association between disease severity and QoS. On a 0 to 10 scale, over the past year, children without AD had an average QoS score of 8.5 against the 4.5 score of those with severe/very severe AD and the 5.5 score reported by those with moderate AD. Parents of non-AD children had a mean score of 6.9, whereas parents of a child with AD had lower scores of 5.4 and 5.1 for moderate and severe/very severe AD, respectively (Figure 3A). Furthermore, the proportion of children with a very poor QoS (0–5) was greater among those with severe/very severe AD compared to those with moderate disease (66.7% vs 45.3%; p≤0.05) (Figure 3A).
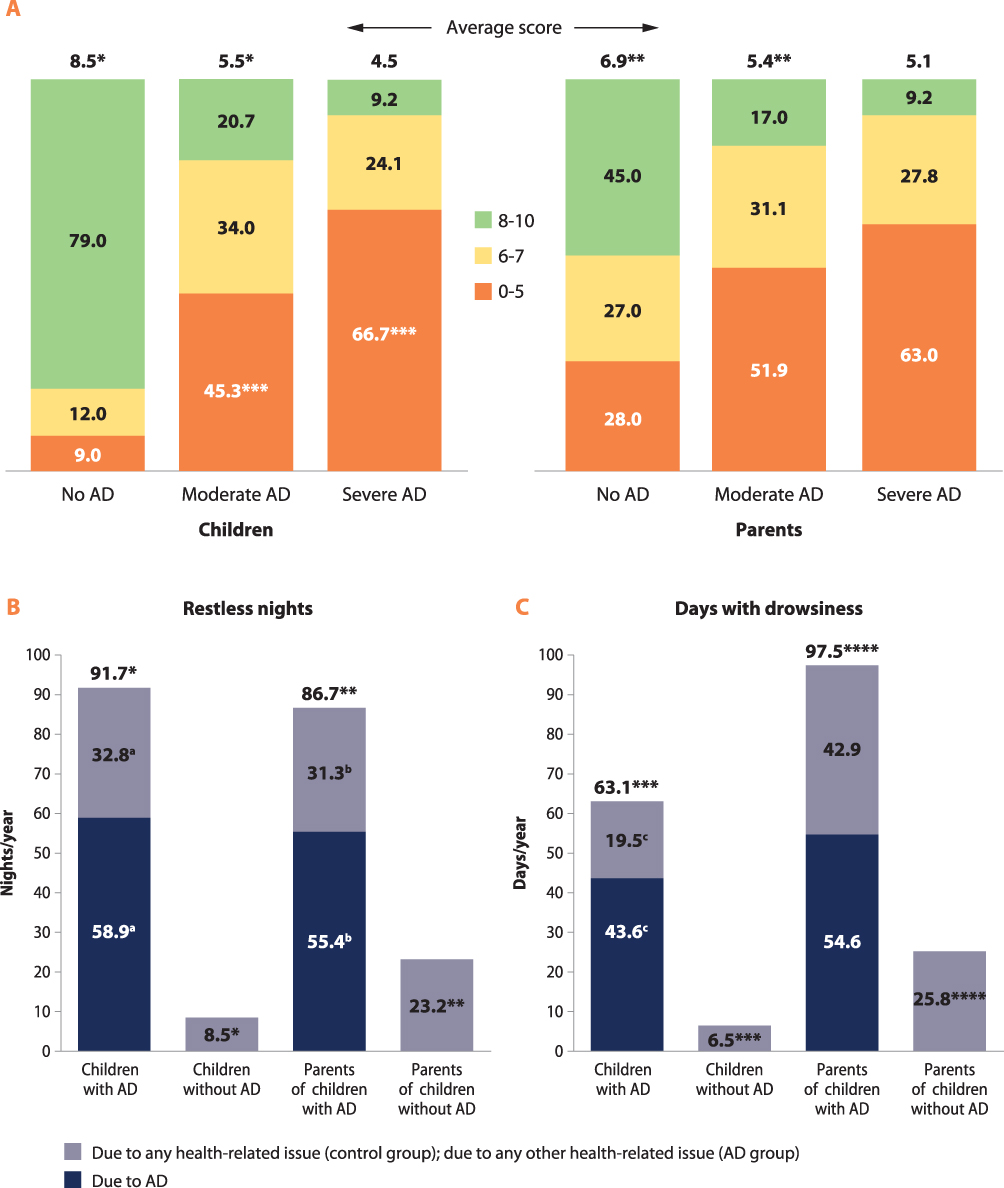 |
Figure 3 Sleep impairment and daily drowsiness. Abbreviation: AD, atopic dermatitis. Notes: Quality of sleep for parents and children with or without atopic dermatitis over the past year (A). The average score is on a 0 to 10 scale. Number of nights with poor sleep (B) and days with drowsiness (C). a,b,c,*,**,***,****Statistically significant (p≤0.05). |
In our study, QoS was defined as having difficulty falling asleep, frequently waking up, and having difficulty falling back to sleep after waking up. We also compared the number of nights with QoS disturbances and of days with drowsiness experienced by participants over the past 12 months and assessed whether those were due to AD or any other health-related issue (Figure 3B and C).
Children with AD were reported on average as having 91.7 restless nights (vs 8.5 nights reported for their peers without AD; p ≤ 0.05). Overall, active AD had a strong impact on rest, causing more nights of broken sleep than any other health-related issue (58.9 vs 32.8; p≤0.05) (Figure 3B). The disease also had a negative impact on caregivers’ sleep. Parents of children with AD reported 86.7 restless nights per year (vs 23.3 nights reported by parents of children without AD; p≤ 0.05). Children’s AD caused significantly more nights with sleep disturbances than any other health-related issue (55.4 vs 31.3; p≤0.05).
The inability to rest during the night translated into heaviness/drowsiness during the day. Children with AD experienced significantly more daytime drowsiness than their non-AD peers (63.1 days vs 6.5; p≤0.05) (Figure 3C), whereas their parents reported 97.5 days with drowsiness per year against the 25.8 days reported by their counterparts in the control group (p≤0.05). Overall, AD caused more sleepiness and tiredness than any other health-related issue in children (43.6 days vs 19.5; p≤0.05) whereas no significant differences were reported by their caregivers (54.6 days vs 42.9).
Bullying and Self-Isolation
Children with AD were more frequently victims of bullying than their non-AD peers, both at school (20.0% vs 9.0%; p≤0.05) and in other social environments (16.9% vs 3.0%; p≤0.05). Over the previous year, nearly half of the AD children (48.7%) had experienced at least one episode of direct bullying at school because of their disease: classmates were excluding/isolating (39.4%) or being bossy (38.1%) with them, targeting them with nicknames (33.7%) and teasing them (40.1%) about their AD. Nearly half (51.9%) of the AD children also experienced indirect bullying, such as being stared at because of their disease. Altogether, most children with AD (66.9%) had experienced at least one episode of direct/indirect bullying or self-isolation related to AD in the previous year.
AD commonly triggered self-isolating behaviors (59.4%). In particular, children with AD found it difficult to interact with classmates of the opposite sex (48.7%), gave up on some extracurricular activities or did not attend parties (40.6% in both cases), or were afraid of going to school, to avoid bullying linked to their disease (35.6%) (Supplementary Table 1).
About 16% of parents of AD children declared that without the disease their child would have more friends. However, AD did not affect children’s social development: no significant difference was found in the number of close friends between the two groups (6.6 vs 6.2).
Distance Learning During COVID Pandemic
During the COVID-19 pandemic, in-class teaching was replaced by emergency distance learning. Overall, without making any reference to the disease, most children experienced distance learning negatively, albeit more frequently in the non-AD group (73.0% vs 51.3% in the AD group; p≤0.05); on the other hand, the frequency of children with AD which considered the opportunity to stay at home as a relief was twice compared to peers without AD (29.4% vs 14.0%; p≤0.05) (Supplementary Figure 2A). The feeling of relief due to not attending school in person was positively correlated with the disease severity (40.9% vs 22.4% for severe/very severe AD and moderate AD, respectively; p≤0.05). Distance learning was experienced favorably because AD was less visible to classmates (34.8%), children were less likely to be teased or bullied (21.7%), they felt more relaxed (19.6%) and had more flexibility about their clothing and skin care (6.5%) (Supplementary Figure 2B).
Absenteeism and Presenteeism
Absenteeism was measured in terms of school absences, late entries or early exits due to AD; presenteeism was defined as the difficulty in remaining focused and concentrated at school or while doing homework at home. Study impairment was defined as the sum of absenteeism and presenteeism.
We compared absenteeism and presenteeism over the past 12 months between groups, making explicit enquiries on the number of days of absenteeism and presenteeism due to AD (AD group) and any/any other health-related reasons (AD and non-AD groups).
When asked about school attendance and performance, 46.3% of parents reported school absences, late entries or early exits due to AD for “a few days per year”, 43.1% reported absenteeism for “a few days every 2 weeks/a few days a month” (from 15 to 30 days per year) and 10.6% reported absences for “one or more days per week”, meaning a minimum of 50 days per year (Figure 4A).
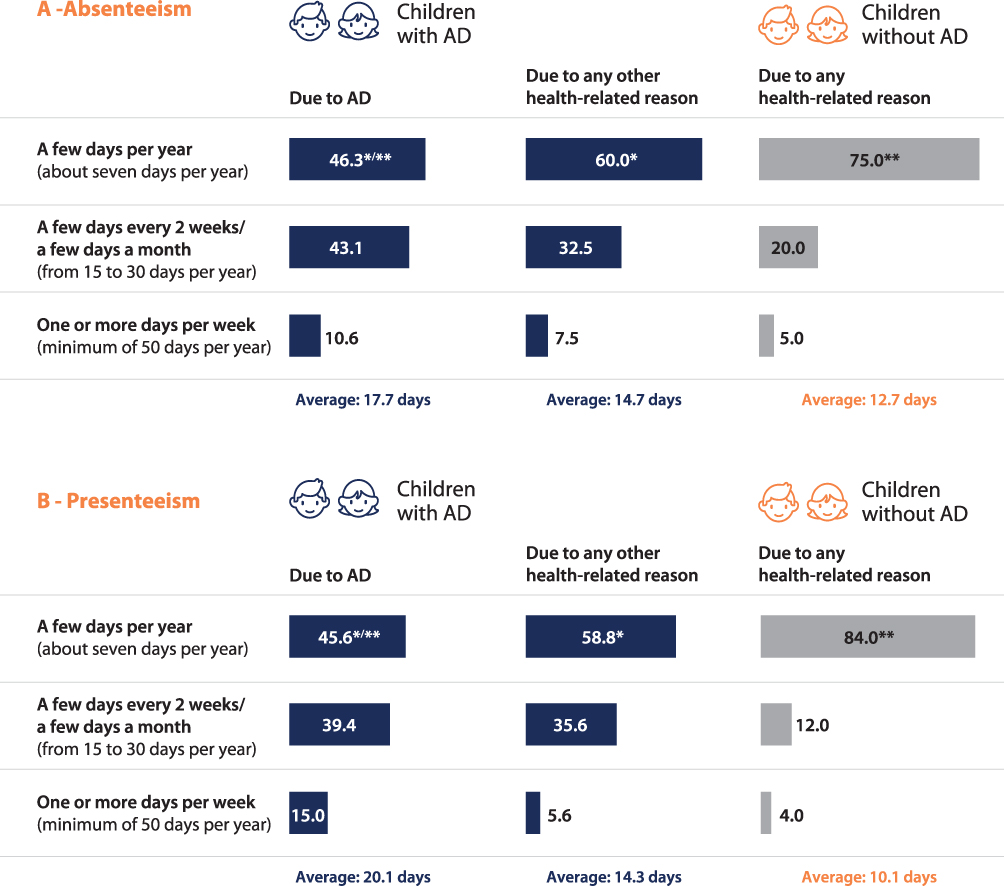 |
Figure 4 Absenteeism and presenteeism. Abbreviation: AD, atopic dermatitis. Notes: Absenteeism as number of days of school missed over the past 12 months (A) and presenteeism as number of days with decreased focus/functionality (B) due to atopic dermatitis or any/any other health-related issue over the past 12 months. Data expressed as percentages and average. *,**Statistically significant (p≤0.05). |
AD accounted for 17.7 days of absenteeism per student on average whereas all other health issues accounted for 14.7 days. In the non-AD group, we calculated 12.7 total days of absenteeism (Figure 4A). Health status accounted for 14.3 and 10.1 days of presenteeism per student/year for children with and without AD respectively, whereas AD alone caused 20.1 days of presenteeism per student/year (Figure 4B). For about one in six (15.0%) children there were difficulties in keeping focus and concentration at school or while doing homework at home for least one or more days per week, 39.4% for a few days every 2 weeks/a few days a month, and 45.6% for a few days per year. One student out of 20 (5.6%) reported presenteeism for 67.1 days per year. Overall, AD-induced absenteeism + presenteeism resulted in a study impairment of 37.8 days per student/year.
Interestingly, presenteeism and absenteeism were positively correlated in the AD cohort (Pearson’s r=0.63; p≤0.05), while no correlation was found for non-AD children (r=0.34).
We also found a positive association between presenteeism/absenteeism and bullying and between presenteeism/absenteeism and disease severity. Presenteeism was more pronounced among bullied students with AD (25.5 vs 11.6; p≤0.05), who also lost on average more days of school compared to not-bullied ones (21.3 vs 12.2; p≤0.05). Severe/very severe AD had a significantly greater impact on presenteeism compared to moderate AD (25.1 days vs 17.5; p≤0.05), although absenteeism (19.6 vs 16.7 days; p ns) did not vary across disease severity. Approximately 1 out of 3 caregiver parents (38.1%) acknowledged the negative impact of AD on school performance and said such perception had been largely confirmed by teachers (60.6%), with AD being perceived as a future obstacle to their children’s academic or professional career by 22.5% of caregivers. This perception was even more prominent in the presence of severe/very severe AD (40.7% p≤0.05).
Personal, Professional, and Economic Impact of AD on Caregiver Parents
Compared to controls, caring for children with AD required more time and energy (57.5% vs 43.0%; p≤0.05), and caregivers felt overwhelmed by the responsibility of being a parent (29.4% vs 16.0%; p≤0.05) up to the point that 1 in 5 of them (18.1% vs 3.0%; p≤0.05) reconsidered having children. Caregivers feared about their children’s future, including the fear of AD becoming chronic (47.5%), its worsening over time (38.1%), scars becoming permanent (29.4%), occurrence of long-term adverse effect of drugs such as cortisone (28.8%), professional/personal renounces (26.3%), or serious skin infections (24.4%).
Caregivers of children with AD experienced more difficulties than their counterparts: nearly 1 in 4 reported difficulties with their job (24.4% vs 1.0%, p≤0.05), 1 in 10 had to change their job/alter their career paths (10.0 vs 1.0%, p≤0.05) and 39.4% had asked for days off/hours of leave in the previous month (50.6% in the last 6 months) to care for their child’s AD.
The impact of AD also extended to the emotional and personal well-being of parents, who, compared to controls, lost friendships more frequently (9.4% vs 0.0%, p≤0.05) and had periods of depression (13.8% vs 2.0%, p≤0.05). Severe/very severe AD had a higher impact on parent depression than moderate AD (22.2% vs 9.4%; p≤0.05).
Finally, on average, the annual out of pocket expenses related to managing the disease was €1393.2, 55.0% of which was spent on skin care products (excluding the cost of drugs and visits), and 45.0% for clothes, house cleaning products, laundry services and similar.
Discussion
This study evaluated the psychosocial burden of moderate to severe AD on 6- to 11-year-old children and their parents. Altogether, children with AD did not seem comfortable with their condition from both a personal and a relational perspective, developing a negative perception of themselves. AD was perceived as a difficult-to-hide skin condition which had a negative impact on everyday activities and on the emotional state of the children who often felt ashamed and judged by others, unlike their peers without AD. Our data are consistent with those from other studies, suggesting that children with AD are at increased risk of developing mental health disorders.35,36
In our study, parents reported children with AD having a totally different set of feelings compared to their peers. AD suppressed the positive feelings typical of childhood (ie, strength and freedom) while triggering negative feelings such as uncertainty, embarrassment, and self-consciousness/shame. These negative feelings are known to correlate with disease severity,37 with up to 70% of children with AD feeling ashamed with peers during their primary school years.15
AD had a great impact on physical, emotional, and social functioning in children. AD negatively affected the quality of life of nearly 1 out of 2 children and was a real limitation to daily life (eg, sport and free-time activities) for about 2/3 of children, impairing well-being. Similar findings were reported by Chernyshov et al in their international study on the HRQoL and family HRQoL of children with AD.38
Our analysis showed that 1 out of 2 children experienced AD-related bullying, 3 out of 5 experienced self-isolation and nearly 7 out of 10 experienced both, which led to giving up social activities (eg, parties, school trips, sports, and extracurricular activities). Our findings are similar to those of Magin, Brenninkmeijer, Xie et al,15,16,39 according to whom children with AD are often bullied and participate in fewer leisure activities than their non-AD controls. Not surprisingly, for nearly 1 out of 3 children, remote schooling forced by the COVID-19 pandemic was an opportunity to relieve the stress associated with the daily management of their disease (eg, allowing to dress more comfortably), as well as to avoid the interpersonal relations that resulted in bullying. It would be interesting to confirm this result with other independent studies performed during the same period.
Overall, we documented a significant burden of AD in terms of night rest and daily functioning. AD generated a ≈10-fold increase in the number of restless nights and days with drowsiness in children and a ≈4-fold increase for their parents. Our data suggest the existence of a substantial “comorbidity load” because AD children experience more Quality of Sleep disturbances due to their overall health than their non-AD peers (91.7 vs 8.5 nights). The same considerations can be made for daily sleepiness and tiredness of AD vs non-AD children (63.1 vs 6.5 days per year). Multimorbidity in subjects with AD is not uncommon: worldwide, 92.0% of 6–11 year-old children, regardless of disease severity, has at least 1 atopic comorbidity, typically asthma, allergic rhinitis, or other allergies.40
In our study population, children with AD and their parents presented with typically 4 other conditions, primarily allergies, allergic rhinitis, and asthma. Almost all family members (92.5%) referred a history of allergies, AD and other Type-2 comorbidities (asthma, nasal polyposis, and eosinophilic esophagitis). The large-scale, population-based study by Gilaberte et al on Spanish children younger than 18 years, showed that 43% of them had both atopic and non-atopic multimorbidity.41 There is a significant association between a parental history of atopic disease and AD in the offspring, with similar effect size for the two parents, and the association gets stronger with the number of parental atopic diseases and the number of affected parents.42
However, we believe we had higher percentages of comorbidities since our question referred to the entire family circle and not only to parents and siblings.
Over the previous year, about 1 in 2 children missed school or presented impaired focus and concentration for at least 15+ days per year. Overall, AD was responsible for a significant increase in absenteeism, as well as presenteeism (≈2.5-fold and ≈3.5-fold compared to non-AD controls, respectively). Our findings are in the same range as those by Stingeni,21 who studied >12 yo adolescents and calculated an average of 17.1 missed days of school and 19.5 days per year of decreased productivity at school due to AD. As in the work by Stingeni et al, we also found a positive association between bullying, presenteeism and absenteeism.
Parenting for a child with AD can be extremely complex and stressful, at the cost of a decreased parental psychosocial functioning and HRQoL.24 Compared to controls, more parents of children with AD feel distressed and experience sleepless nights, absenteeism or reduced productivity at work, and difficulties in their interpersonal relationships.25,43 The responders to our survey struggled at work, due to their poor quality of sleep, had to request changes in their working hours or felt forced to change their job. Overall, they felt overwhelmed by the responsibilities of being a parent of a child with AD.
The out of pocket economic burden of AD for families is substantial, being estimated in €1393.2/year to cover for skincare and house-related expenses. Our estimates do not include frequent consultations with private physicians, which can also be expensive. However, the overall financial burden is much higher, when considering both direct costs (for national healthcare systems, eg, visits to the emergency room, hospitalizations) and indirect costs (eg, productivity loss due to caregivers’ absenteeism, presenteeism or job loss).
Considering that about a third of the population included in the survey had severe/very severe AD, we would expect most children to be on active therapy. On the other hand, the prescribed therapies did not seem effective in controlling AD, as documented by the multiple hospitalizations and emergency room visits (15% and 30%, respectively) required to manage the recurrent disease flares (7.6 on average in the previous 12 months). Parents avoided corticosteroids for fear of potential side effects. Topical corticosteroid phobia is a well-known phenomenon among caregivers of children with AD and is widespread among Italian families, as 81% of Italian caregivers of pediatric patients with AD reported a certain degree of corticophobia.44,45 Strikingly, only half of children used detergents and moisturizing creams (51.9% and 48.8%, respectively), although guidelines state their importance in the management of AD and dermatologists encourage their constant use.
In our study, approximately 15% of parents underestimated the severity of moderate AD. Very recently, Ezzedine et al also reported a difference of severity between POEM and patient (or parent) assessments, with parents tending to underestimate the severity of their children’s AD.46 Twenty-seven percent of caregivers underestimated the severity of their children’s disease whereas in another study, AD was underestimated by parents in 37.1% of cases compared to adolescent patient’s self-assessment.46,47
Drawing a conclusion, our study is consistent with the results from previous scientific literature linking AD to psychosocial functioning: itch-induced sleep deprivation seems to be one of the major triggers of physical and mental exhaustion which result in emotional distress, impaired concentration and poor daily performance.48 Furthermore AD, like other pediatric dermatologic disorders, can undermine self-esteem and the willingness to go to school and spend time with peers.39,49 The functional and psychosocial disfunctions caused by AD limit the ability of children to perform daily activities and cause stigma.50 The burden of the disease is shared between children and their parents. Based on our results, one can conclude that urgent policy interventions are needed to transform the school setting from an unfriendly environment into a supportive and inclusive space. Finally, educating parents may help to overcome the underestimation of disease severity and enhance the effectiveness of shared decision-making, to improve willingness to start/adhere to therapy and the use of appropriate daily care routines able to prevent AD flaring up.51
Study Limitations
This study has some limitations to be considered. The first, typical of any survey, is that all observations were based on self-reporting, which may be intrinsically associated with recall bias. Our questionnaire mostly referred to a timeframe ranging from the past 7 days to the past year. This time-window could mitigate any recall bias. Another limitation is that online surveys imply a certain degree of computer literacy and therefore may inevitably introduce a selection bias. Compared to a very recent study about Italian adolescent and adults with AD,21 this survey relies on a self-reported AD diagnosis based on the ISAAC criteria and supported by a confirmation by a physician. The application of the POEM score ensured the selection and stratification of children with moderate to severe AD. We selected a matched control group of children without AD to provide context to the answers.
Conclusion
This Italian study on the burden of moderate to severe atopic dermatitis showed the detrimental impact of the disease on the quality of life of pre-adolescent patients and their caregivers. Stigmatization and psychosocial distress may negatively impact daily home-, school- and work-related activities and may result in poor academic performance. Children with atopic dermatitis must face frequent prejudices about their skin, are more likely to experience bullying and self-isolation and are more exposed to presenteeism and absenteeism. Given the young age, parents are overwhelmed by the long-term consequences of the disease, experiencing disruption in the personal and professional sphere. Further studies on this topic are necessary to better understand the physical and psychosocial comorbidities of atopic dermatitis and may contribute towards the development of strategies aimed to minimize the burden of disease and ameliorate the wellbeing within the family circle.
Statement of Compliance
All procedures were in accordance with both national and international ethical standards as well as with the 1964 Helsinki Declaration, its later amendments, or comparable ethical standards. The survey-based study did not require ethics approval from IRB or local ethics committee; participation was voluntary, anonymous, and informed written consent was obtained upfront from all participants.
Acknowledgment
The authors would like to thank responders for their time, making this study possible. Questionnaire development and statistical analysis were performed by DOXA, funded by Sanofi. Medical writing and editorial assistance were provided by Maurizio Tarzia, an independent medical writer, on behalf of Springer Healthcare, and was funded by Sanofi.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Sanofi.
Disclosure
I. Neri acts as advisor, speaker, investigator and/or consultant for Sanofi, Janssen, Roche-Posay, Giuliani, Leo Pharma. E. Galli reports scientific consultations and/or lectures for Lofarma, Hal_Allergy and Sanofi. I. Baiardini IB reports scientific consultations and/or lectures from Boehringer Ingelheim, Chiesi Farmaceutici, GlaxoSmithKline, Menarini, Novartis, Sanofi, Biofutura, Mundifarma, AstraZeneca. M. Picozza declares no conflicts of interest in this work. AB. Rossi, P. Matruglio, D. Moretti and F. Cipriani are Sanofi employees, and may hold stock and/or stock options in the company.
References
1. Silverberg JI, Barbarot S, Gadkari A, et al. Atopic dermatitis in the pediatric population. Ann Allergy Asthma Immunol. 2021;126(4):417–428.e2. doi:10.1016/j.anai.2020.12.020
2. Weidinger S, Beck LA, Bieber T, Kabashima K, Irvine AD. Atopic dermatitis. Nat Rev Dis Primers. 2018;4:1. doi:10.1038/s41572-018-0001-z
3. Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet. 2020;396(10247):345–360. doi:10.1016/S0140-6736(20)31286-1
4. Girolomoni G, de Bruin-Weller M, Aoki V, et al. Nomenclature and clinical phenotypes of atopic dermatitis. Ther Adv Chronic Dis. 2021;12:20406223211002979. doi:10.1177/20406223211002979
5. Silverberg JI, Gelfand JM, Margolis DJ, et al. Patient burden and quality of life in atopic dermatitis in US adults. Ann Allergy Asthma Immunol. 2018;121(3):340–347. doi:10.1016/j.anai.2018.07.006
6. Simpson EL, Bieber T, Eckert L, et al. Patient burden of moderate to severe atopic dermatitis (AD): insights from a phase 2b clinical trial of dupilumab in adults. J Am Acad Dermatol. 2016;74(3):491–498. doi:10.1016/j.jaad.2015.10.043
7. Mollanazar NK, Smith PK, Yosipovitch G. Mediators of chronic pruritus in atopic dermatitis: getting the itch out? Clin Rev Allergy Immunol. 2016;51(3):263–292.
8. Bawany F, Northcott CA, Beck LA, Pigeon WR, Disturbances S. Atopic dermatitis: relationships, methods for assessment, and therapies. J Allergy Clin Immunol Pract. 2021;9(4):1488–1500. doi:10.1016/j.jaip.2020.12.007
9. Camfferman D, Kennedy JD, Gold M, Martin AJ, Lushington K. Eczema and sleep and its relationship to daytime functioning in children. Sleep Med Rev. 2010;14(6):359–369. doi:10.1016/j.smrv.2010.01.004
10. Na CH, Chung J, Simpson EL. Quality of life and disease impact of atopic dermatitis and psoriasis on children and their families. Children. 2019;6(12):133. doi:10.3390/children6120133
11. Slattery MJ, Essex MJ, Paletz EM, et al. Depression, anxiety, and dermatologic quality of life in adolescents with atopic dermatitis. J Allergy Clin Immunol. 2011;128(3):668–671. doi:10.1016/j.jaci.2011.05.003
12. Fishbein AB, Cheng BT, Tilley CC, et al. Sleep disturbance in school-aged children with atopic dermatitis: prevalence and severity in a cross-sectional sample. J Allergy Clin Immunol Pract. 2021;9(8):3120–3129.e3. doi:10.1016/j.jaip.2021.04.064
13. Kelly KA, Balogh EA, Kaplan SG, Feldman SR. Skin disease in children: effects on quality of life, stigmatization, bullying, and suicide risk in pediatric acne, atopic dermatitis, and psoriasis patients. Children. 2021;8(11):1057. doi:10.3390/children8111057
14. Kern C, Wan J, LeWinn KZ, et al. Association of atopic dermatitis and mental health outcomes across childhood: a longitudinal cohort study. JAMA Dermatol. 2021;157(10):1200–1208. doi:10.1001/jamadermatol.2021.2657
15. Brenninkmeijer EEA, Legierse CM, Sillevis Smitt JH, Last BF, Grootenhuis MA, Bos JD. The course of life of patients with childhood atopic dermatitis. Pediatr Dermatol. 2009;26(1):14–22. doi:10.1111/j.1525-1470.2008.00745.x
16. Magin P. Appearance-related bullying and skin disorders. Clin Dermatol. 2013;31(1):66–71. doi:10.1016/j.clindermatol.2011.11.009
17. Chernyshov PV. Stigmatization and self-perception in children with atopic dermatitis. Clin Cosmet Investig Dermatol. 2016;9:159–166. doi:10.2147/CCID.S91263
18. Hon KLE, Leung TF, Wong KY, Chow CM, Chuh A, Ng PC. Does age or gender influence quality of life in children with atopic dermatitis? Clin Exp Dermatol. 2008;33(6):705–709. doi:10.1111/j.1365-2230.2008.02853.x
19. Lawson V, Lewis‐Jones MS, Finlay AY, Reid P, Owens RG. The family impact of childhood atopic dermatitis: the dermatitis family impact questionnaire. Br J Dermatol. 1998;138(1):107–113. doi:10.1046/j.1365-2133.1998.02034.x
20. Zuberbier T, Orlow SJ, Paller AS, et al. Patient perspectives on the management of atopic dermatitis. J Allergy Clin Immunol. 2006;118(1):226–232. doi:10.1016/j.jaci.2006.02.031
21. Stingeni L, Belloni Fortina A, Baiardini I, Hansel K, Moretti D, Cipriani F. Atopic dermatitis and patient perspectives: insights of bullying at school and career discrimination at work. J Asthma Allergy. 2021;14:919–928. doi:10.2147/JAA.S317009
22. Balkrishnan R, Housman TS, Grummer S, et al. The family impact of atopic dermatitis in children: the role of the parent caregiver. Pediatr Dermatol. 2003;20(1):5–10. doi:10.1046/j.1525-1470.2003.03002.x
23. Carroll CL, Balkrishnan R, Feldman SR, Fleischer AB
24. Yang EJ, Beck KM, Sekhon S, Bhutani T, Koo J. The impact of pediatric atopic dermatitis on families: a review. Pediatr Dermatol. 2018;36(1):66–71. doi:10.1111/pde.13727
25. Capozza K, Gadd H, Kelley K, Russell S, Shi V, Schwartz A. Insights from caregivers on the impact of pediatric atopic dermatitis on families: “I’m tired, overwhelmed, and feel like i’m failing as a mother”. Dermatitis. 2020;31(3):223–227. doi:10.1097/DER.0000000000000582
26. Barbarot S, Silverberg JI, Gadkari A. Pediatric population: results from an international cross-sectional study. J Pediatr. 2022;246:220–226.e5. doi:10.1016/j.jpeds.2022.04.027
27. Girolomoni G, Abeni D, Masini C, et al. The epidemiology of atopic dermatitis in Italian schoolchildren. Allergy. 2003;58(5):420–425. doi:10.1034/j.1398-9995.2003.00112.x
28. Ricci G, Bendandi B, Bellini F, Patrizi A, Masi M. Atopic dermatitis: quality of life of young Italian children and their families and correlation with severity score. Pediatr Allergy Immunol. 2007;18(3):245–249. doi:10.1111/j.1399-3038.2006.00502.x
29. Monti F, Agostini F, Gobbi F, Neri E, Schianchi S, Arcangeli F. Quality of life measures in Italian children with atopic dermatitis and their families. Ital J Pediatr. 2011;37(1):59. doi:10.1186/1824-7288-37-59
30. Lewis-Jones MS, Finlay AY. The Children’s Dermatology Life Quality Index (CDLQI): initial validation and practical use. Br J Dermatol. 1995;132(6):942–949. doi:10.1111/j.1365-2133.1995.tb16953.x
31. Berry JO, Jones WH. The parental stress scale: initial psychometric evidence. J Soc Pers Relat. 1995;12(3):463–472. doi:10.1177/0265407595123009
32. Thomas KS, Apfelbacher CA, Chalmers JR, et al. Recommended core outcome instruments for health-related quality of life, long-term control and itch intensity in atopic eczema trials: results of the HOME VII consensus meeting. Br J Dermatol. 2020;185:139–146. doi:10.1111/bjd.19751
33. Asher MI, Keil U, Anderson HR, et al. International Study of Asthma and Allergies in Childhood (ISAAC): rationale and methods. Eur Respir J. 1995;8(3):483–491. doi:10.1183/09031936.95.08030483
34. Weidinger S, Simpson EL, Eckert L, et al. 15115 The patient-reported disease burden in pediatric patients with atopic dermatitis: a cross-sectional study in the United States, Canada, Europe, and Japan. J Am Acad Dermatol. 2020;83(6):AB29. doi:10.1016/j.jaad.2020.06.203
35. Yaghmaie P, Koudelka CW, Simpson EL. Mental health comorbidity in patients with atopic dermatitis. J Allergy Clin Immunol. 2013;131(2):428–433. doi:10.1016/j.jaci.2012.10.041
36. Strom MA, Fishbein AB, Paller AS, Silverberg JI. Association between atopic dermatitis and attention deficit hyperactivity disorder in U.S. children and adults. Br J Dermatol. 2016;175(5):920–929. doi:10.1111/bjd.14697
37. Ben-Gashir MA, Seed PT, Hay RJ. Quality of life and disease severity are correlated in children with atopic dermatitis. Br J Dermatol. 2004;150(2):284–290. doi:10.1111/j.1365-2133.2004.05776.x
38. Chernyshov PV, Ho RC, Monti F, et al. An international multi-center study on self-assessed and family quality of life in children with atopic dermatitis. Acta Dermatovenerol Croat. 2015;23(4):247–253.
39. Xie Q-W, Chan CL, Chan CH. The wounded self-lonely in a crowd: a qualitative study of the voices of children living with atopic dermatitis in Hong Kong. Health Soc Care Community. 2020;28(3):862–873. doi:10.1111/hsc.12917
40. Silverberg J, Simpson E, Weidinger S, et al. Children With Atopic Dermatitis (AD) have a high burden of atopic comorbidities: results from a large worldwide survey. J Allergy Clin Immunol. 2021;147(2):AB31. doi:10.1016/j.jaci.2020.12.149
41. Gilaberte Y, Pérez-Gilaberte JB, Poblador-Plou B, Bliek-Bueno K, Gimeno-Miguel A, Prados-Torres A. Prevalence and comorbidity of atopic dermatitis in children: a large-scale population study based on real-world data. J Clin Med. 2020;9:6. doi:10.3390/jcm9061632
42. Ravn NH, Halling A-S, Berkowitz AG, et al. How does parental history of atopic disease predict the risk of atopic dermatitis in a child? A systematic review and meta-analysis. J Allergy Clin Immunol. 2020;145(4):1182–1193. doi:10.1016/j.jaci.2019.12.899
43. Daud LR, Garralda ME, David TJ. Psychosocial adjustment in preschool children with atopic eczema. Arch Dis Child. 1993;69(6):670–676. doi:10.1136/adc.69.6.670
44. El Hachem M, Gesualdo F, Ricci G, et al. Topical corticosteroid phobia in parents of pediatric patients with atopic dermatitis: a multicentre survey. Ital J Pediatr. 2017;43(1):22. doi:10.1186/s13052-017-0330-7
45. Kojima R, Fujiwara T, Matsuda A, et al. Factors associated with steroid phobia in caregivers of children with atopic dermatitis. Pediatr Dermatol. 2013;30(1):29–35. doi:10.1111/j.1525-1470.2012.01808.x
46. Ezzedine K, Shourick J, Merhand S, Sampogna F, Taieb C. Perceived clinical severity of atopic dermatitis in adolescents: comparison between patients’ and parents’ evaluation. J Am Acad Dermatol. 2021;84(1):164–165. doi:10.1016/j.jaad.2020.04.037
47. Xu X, Olsson M, Bajpai R, et al. Concordance between physician-rated and caregiver-perceived disease severity in children with atopic dermatitis: a cross-sectional study. Acta Derm Venereol. 2020;100(18):adv00308. doi:10.2340/00015555-3540
48. Lewis-Jones S. Quality of life and childhood atopic dermatitis: the misery of living with childhood eczema. Int J Clin Pract. 2006;60(8):984–992. doi:10.1111/j.1742-1241.2006.01047.x
49. Vivar KL, Kruse L. The impact of pediatric skin disease on self-esteem. Int J Womens Dermatol. 2017;4(1):27–31. doi:10.1016/j.ijwd.2017.11.002
50. Silverberg JI. Associations between atopic dermatitis and other disorders. F1000Res. 2018;7:303. doi:10.12688/f1000research.12975.1
51. Capozza K, Funk M, Hering M, et al. Patients’ and caregivers’ experiences with atopic dermatitis-related burden, medical care, and treatments in 8 countries. J Allergy Clin Immunol Pract. 2022;11(1):264–273.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.