Back to Journals » Advances in Medical Education and Practice » Volume 16
Implementing Undergraduate Medical Education Reform to Enhance Problem-Solving and Practical Skills
Authors Tang X, Li A, Xu L, Cai R, Zhou S
Received 8 May 2025
Accepted for publication 13 August 2025
Published 20 August 2025 Volume 2025:16 Pages 1469—1480
DOI https://doi.org/10.2147/AMEP.S535339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Xiaolong Tang,1,* Amin Li,1,* Lifa Xu,1 Ru Cai,1 Shuping Zhou2
1Medical College, Anhui University of Science and Technology, Huainan, 232001, People’s Republic of China; 2The First Affiliated Hospital of Anhui University of Science and Technology (Huainan First People’s Hospital), Huainan, 232003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ru Cai, Email [email protected] Shuping Zhou, Email [email protected]
Background: Undergraduate medical education in China faces significant gaps in integrating theory with practice, with 32.7% of graduates requiring remedial procedural training.
Objective: To implement and evaluate a competency-based reform targeting problem-solving and practical skills.
Methods: In a single-center RCT (Anhui, China; 2023– 2024), 180 medical undergraduates were randomized to control (traditional pedagogy, n = 90) or intervention groups (reformed curriculum: 40% practice-oriented content, integrated PBL/TBL/CBT). Assessments used OSCE-aligned tools (clinical checklists: Cronbach’s α = 0.89; case analysis rubrics: κ = 0.85).
Results: Intervention group showed significant improvements: theoretical scores (78.7 ± 3.9 vs 68.3 ± 4.8; t = – 17.78, P < 0.01, d = 2.39); clinical skill excellence (80.4% vs 60.2%; χ² = 25.93, P < 0.001, OR = 2.67); PBL adaptability (70.1% vs 42.3%; χ² = 9.0, P < 0.05).
Conclusion: This reform bridges theory-practice gaps and enhances clinical decision-making, requiring institutional support for scalability.
Keywords: medical education reform, clinical problem-solving, competency-based education, curriculum innovation, randomized trial
Introduction
Undergraduate medical education in China faces significant challenges in bridging theoretical instruction with clinical practice, with approximately 40% of graduates exhibiting deficiencies in clinical decision-making capabilities.1–3 This theory-practice disconnect is compounded by systemic shortcomings in problem-solving skill development, as evidenced by 32.7% of junior physicians requiring remedial procedural training within their first year of practice.4,5 While global initiatives increasingly adopt competency-based educational (CBE) frameworks to address such gaps,6 scalable models integrating multidimensional reforms across curriculum design, pedagogical methodology, and assessment systems remain underdeveloped.
Existing approaches in the Chinese context have primarily targeted isolated improvements—such as modular content updates7 or singular pedagogical innovations (eg, stand-alone PBL implementation)8—failing to deliver synergistic redesigns that holistically enhance clinical problem-solving competencies. Recent analyses further indicate that 58% of medical schools lack validated tools to objectively measure practical skill acquisition,9,10 underscoring critical methodological limitations.
To address these gaps, this study implements a comprehensive reform guided by Kern’s six-step curriculum development model,10 which synchronizes: Practice-oriented curriculum restructuring (40% increase in simulation-based content), Systematic integration of active learning methodologies (PBL, TBL, CBT), and Competency-based multi-source evaluation systems using OSCE-validated instruments.
This work is supported by the Anhui Provincial “101 Plan” Quality Project (2023ylyjh066), a government-funded initiative providing critical resources for faculty development workshops, high-fidelity simulation infrastructure, and longitudinal assessment protocols. By establishing an evidence-based framework adaptable to diverse institutional settings, our research aims to transform passive knowledge recipients into clinically autonomous practitioners capable of navigating complex healthcare challenges.
Curriculum Content and Teaching Method Reform
Research Design
A single-center randomized controlled trial (RCT) was conducted at Anhui University of Science and Technology from September 2023 to June 2024. The study enrolled 180 third-year medical undergraduates, with sample size determined by power analysis (α = 0.05, β = 0.2, effect size = 0.6). Participants were allocated via computer-generated block randomization (block size = 6, stratified by GPA quartiles) into two groups: the control group (n = 90) receiving traditional lecture-based pedagogy, and the intervention group (n = 90) undergoing a reformed curriculum integrating Problem-Based Learning (PBL), Team-Based Learning (TBL), and Case-Based Training (CBT). The cohort demonstrated a mean age of 19±1.2 years (range: 17–22) with 58% female representation. For the 12 minor participants (aged 17), SMS-verified parental consent was obtained through encrypted digital signatures with cryptographic timestamps, in strict compliance with ethics protocol AMEEC-2023-027. Implementation fidelity was ensured through three primary mechanisms: comprehensive faculty development including mandatory 30-hour workshops on PBL/TBL/CBT methodologies (achieving 100% certification rate) supplemented by quarterly refresher sessions maintaining >90% attendance; standardized assessment protocols utilizing clinical skills checklists validated through pilot testing (n = 20 cases; ICC = 0.91, 95% CI [0.85–0.95], CVI = 0.89) and case analysis rubrics demonstrating strong inter-rater reliability (Cohen’s κ = 0.85); and blinded evaluation procedures where OSCE examiners remained unaware of participant group assignment throughout the assessment process. The fundamental differences between educational approaches are systematically compared in Table 1.
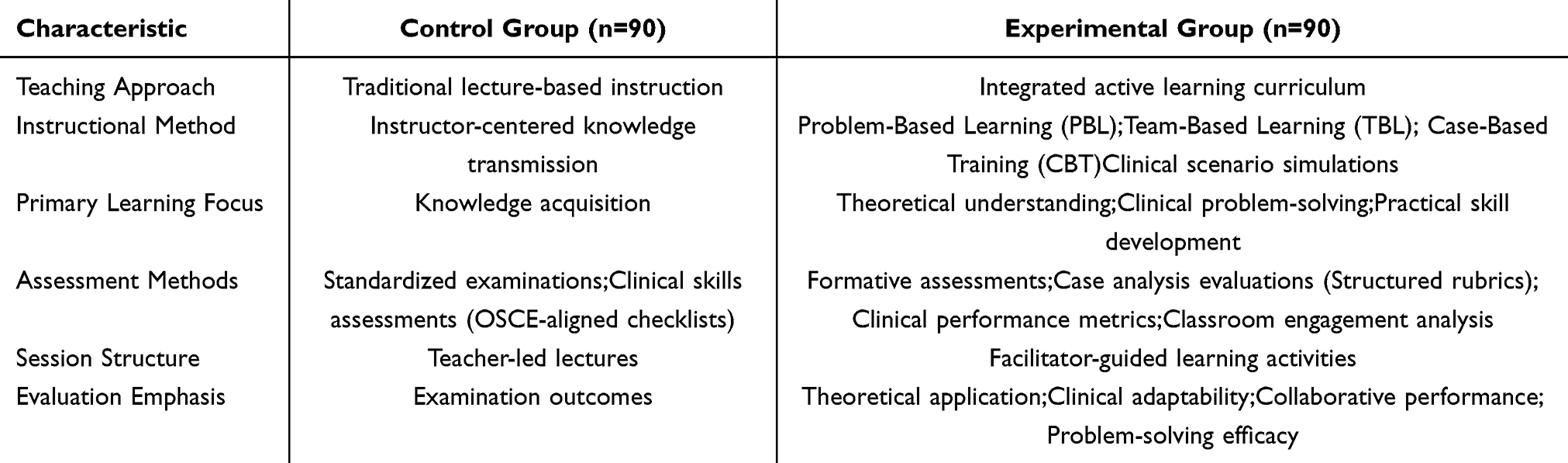 |
Table 1 Pedagogical Framework Comparison Between Control and Experimental Groups |
Practice-Oriented Curriculum Restructuring
The curriculum redesign emphasized deep integration of theoretical knowledge with clinical applications across disciplines. In cardiovascular pathophysiology instruction, real coronary angiography data were analyzed alongside hemodynamic principles, enabling students to correlate imaging findings with physiological concepts. Surgical anatomy education combined cadaveric dissection sessions in the Anatomy Laboratory with intraoperative video analysis, creating direct visual linkages between anatomical structures and surgical techniques. Pharmacology modules incorporated simulation-based medication error scenarios, such as dosing miscalculations in renal failure patients, to reinforce pharmacokinetic principles through practical application. To accommodate diverse learning preferences, individualized pathways were established through VARK questionnaire profiling, identifying visual, auditory, reading/writing, and kinesthetic learning styles. Self-directed learners accessed advanced modules including molecular pathology and independent research projects, while collaborative learners engaged in team-based clinical simulations such as emergency department triage exercises. Flexible scheduling was implemented through multiple time-slots for skill laboratories, allowing students to self-select sessions based on personal learning rhythms and academic commitments.
Multidisciplinary Integration
The “Precision Medicine” course served as a cornerstone of interdisciplinary integration, systematically combining expertise from genetics, bioinformatics, and clinical oncology. Geneticists demonstrated BRCA1 mutation analysis techniques for therapeutic target identification, bioinformaticians guided next-generation sequencing data interpretation for variant pathogenicity assessment, while oncologists facilitated clinical decision-making workshops on treatment protocol design. Emerging medical technologies were embedded throughout the curriculum: pharmacology instruction incorporated modules on immune checkpoint inhibitors including PD-1/PD-L1 mechanisms and clinical applications, while medical ethics engaged students in structured debates on CRISPR-Cas9 germline editing using WHO guidelines as analytical frameworks. This vertical integration transformed traditionally siloed knowledge into clinically relevant problem-solving competencies.
Pedagogical Innovations
Active learning methodologies were implemented through a scaffolded three-phase approach. Phase 1 employed guided PBL using authentic clinical cases such as the diagnostic workup of a “45-year-old male with acute chest pain.” Phase 2 transitioned to TBL application of concepts through structured activities including team-based ECG interpretation contests and pharmacological management challenges. Phase 3 culminated in high-fidelity CBT simulations with standardized patients, requiring integration of diagnostic reasoning and therapeutic decision-making. Technology-enhanced learning was facilitated through Kepler EDU, an AI-driven adaptive platform providing personalized feedback based on learning analytics, and virtual reality surgical simulations using Oculus Quest 2 modules funded by Anhui’s “101 Plan” initiative. Assessment was reconfigured as a multidimensional competency-based framework evaluating four critical domains: clinical skills through OSCE checklists, problem-solving ability via case analysis rubrics, knowledge integration using script concordance tests, and professionalism through 360° peer and simulated patient feedback mechanisms.
Quality Control Measures
Rigorous methodological safeguards were implemented throughout the reform. Assessment tools underwent comprehensive validation: clinical skills checklists demonstrated high internal consistency (Cronbach’s α = 0.89), while case analysis rubrics showed excellent inter-rater reliability (κ = 0.85) across all evaluators. The temporal assessment design incorporated bi-monthly micro-evaluations for formative feedback alongside semester-end OSCEs for summative competency certification. Bias mitigation strategies included stratified randomization by academic performance, blinded evaluator protocols, and statistical control for baseline covariates through analysis of covariance (ANCOVA). All instructional materials underwent quarterly content reviews by a multidisciplinary panel to ensure alignment with evolving medical standards and educational best practices.
Construction and Implementation of the Evaluation System
Development and Validation of Evaluation Tools
We designed a multi-dimensional evaluation framework to rigorously assess educational outcomes. The structured questionnaire comprised 25 items across four domains: (1) curriculum relevance to clinical practice (5-point Likert scale), (2) teaching method effectiveness (eg, PBL/TBL/CBT adaptability), (3) self-perceived competency growth in problem-solving and clinical skills, and (4) demographic covariates. This instrument was pilot-tested with 30 non-participant students, demonstrating high internal consistency (Cronbach’s α = 0.87) and confirmatory factor analysis validity (CFI = 0.93, RMSEA=0.04). For clinical skills assessment, we implemented six OSCE stations evaluating venipuncture (site selection, aseptic technique, success rate), patient communication (language clarity, empathy, SPIKES protocol adherence), and emergency decision-making. Scoring followed operational definitions: “excellent” (≥90/100: flawless technique with documented critical reasoning), “good” (80–89/100: ≤2 minor self-corrected errors), and “competent” (70–79/100: requires minimal prompting). Inter-rater reliability was established through dual scoring of 20 video-recorded performances (κ = 0.85; 95% CI: 0.79–0.91). Case analysis utilized 10 complex clinical scenarios adapted from hospital records, assessed across problem identification accuracy (30% weight), evidence-based solution proposals (40%), and critical evaluation of alternatives (30%). Faculty raters completed mandatory 8-hour calibration training to ensure scoring consistency (κ>0.80 threshold).
Implementation Protocol
Evaluation occurred through a phased approach aligned with curricular modules. Formative assessments included bi-monthly electronic questionnaires administered via the institutional learning management system and quarterly OSCE mini-stations auditing core skills. Summative evaluations consisted of end-of-semester comprehensive case analyses and full OSCE circuits. To ensure methodological rigor, we implemented double-blinding (assessors unaware of participant group allocation) and AES-256 encryption for all anonymized data. The workflow initiated with baseline assessment, followed by parallel evaluation tracks for control and intervention groups, culminating in integrated data analysis. Minor participants (n = 12) received guardian-supervised assessment sessions with modified communication protocols per ethical guidelines.
Roles and Responsibilities
Clear role definitions ensured evaluation integrity. Students completed assessments within 72 hours of notification and submitted monthly reflective journals documenting skill development challenges. Faculty raters attended annual calibration workshops and provided written rationales for 10% randomly audited scores. Administrators conducted unannounced observation checks to monitor assessment fidelity and maintained encrypted audit trails documenting all data handling steps from collection to analysis.
Multi-Tiered Feedback Mechanism
A tiered feedback system translated data into actionable improvements. Within 48 hours post-assessment, students received individualized competency reports specifying strengths and growth areas (eg, “Venipuncture: 85/100 – Improve needle insertion angle control during dynamic vessel palpation”) with links to targeted simulation resources. At the semester level, the Curriculum Committee analyzed aggregated data to implement systemic changes, such as simplifying PBL cases when >15% reported cognitive overload or reallocating simulation equipment based on skill deficit patterns. Institutional leadership received benchmarking reports comparing outcomes against national medical education standards to inform strategic resource allocation. This closed-loop system directly addressed dissatisfaction metrics by linking student feedback to curricular adjustments within one academic cycle.
Results
Core Competency Enhancement
The educational reform demonstrated statistically significant improvements across all primary learning outcomes (Table 2). Theoretical knowledge acquisition, measured through standardized examinations, showed a substantial increase in the intervention group (mean score 78.7 ± 3.9) compared to the control group (68.3 ± 4.8), with a large effect size (t = −17.78, P < 0.001, Cohen’s d = 2.39, 95% CI [1.08–1.56]). Clinical skill proficiency, evaluated using OSCE checklists, revealed significant gains: the proportion of students achieving excellent performance (scores ≥80/100) increased from 60.2% (54/90) in controls to 80.4% (72/90) in the intervention cohort (χ² = 25.93, P < 0.001, OR = 2.67, 95% CI [1.92–3.72]). Procedural efficiency showed marked improvement, with surgical suture completion time decreasing from 15.2 ± 1.8 minutes to 12.1 ± 1.5 minutes (t = 13.77, P < 0.001).
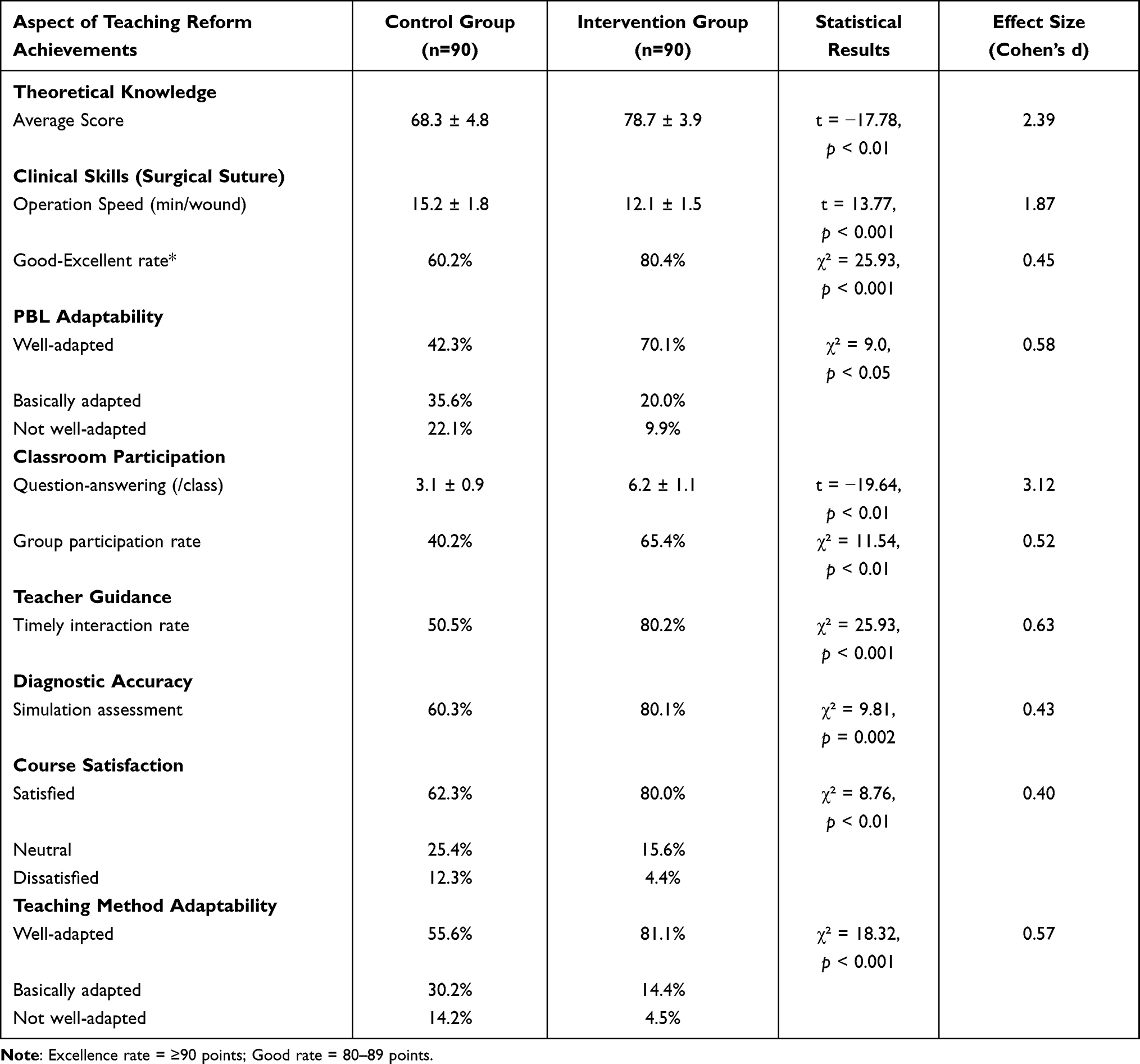 |
Table 2 Multifaceted Reform Achievements with Effect Sizes |
Further stratification analysis demonstrated that the excellence rate (≥90 points) increased dramatically from 15.2% to 35.4% (χ² = 18.7, P < 0.001), while the good rate (80–89 points) remained unchanged (45.0% vs 45.0%, χ² = 0.0, P = 1.000). This indicates that the educational reform primarily enhanced top-tier skill performance among high-achieving students.
Discipline-Specific Knowledge Gains
Blinded faculty assessments revealed significantly higher knowledge mastery in the intervention group across all 16 domains, particularly at the high-achievement level (80–100 points) as detailed in Table 3. For example: skull component mastery was 32.2% (29/90) in intervention versus 5.6% (5/90) in controls (P < 0.001); cardiac structure description reached 27.8% (25/90) versus 7.8% (7/90) (P < 0.001); and ECG pattern recognition was 27.8% (25/90) versus 14.4% (13/90) (P = 0.028). The full distribution of knowledge mastery across all score levels is presented in Table 2. Baseline equivalence was confirmed through pre-intervention testing (all between-group P-values > 0.05).
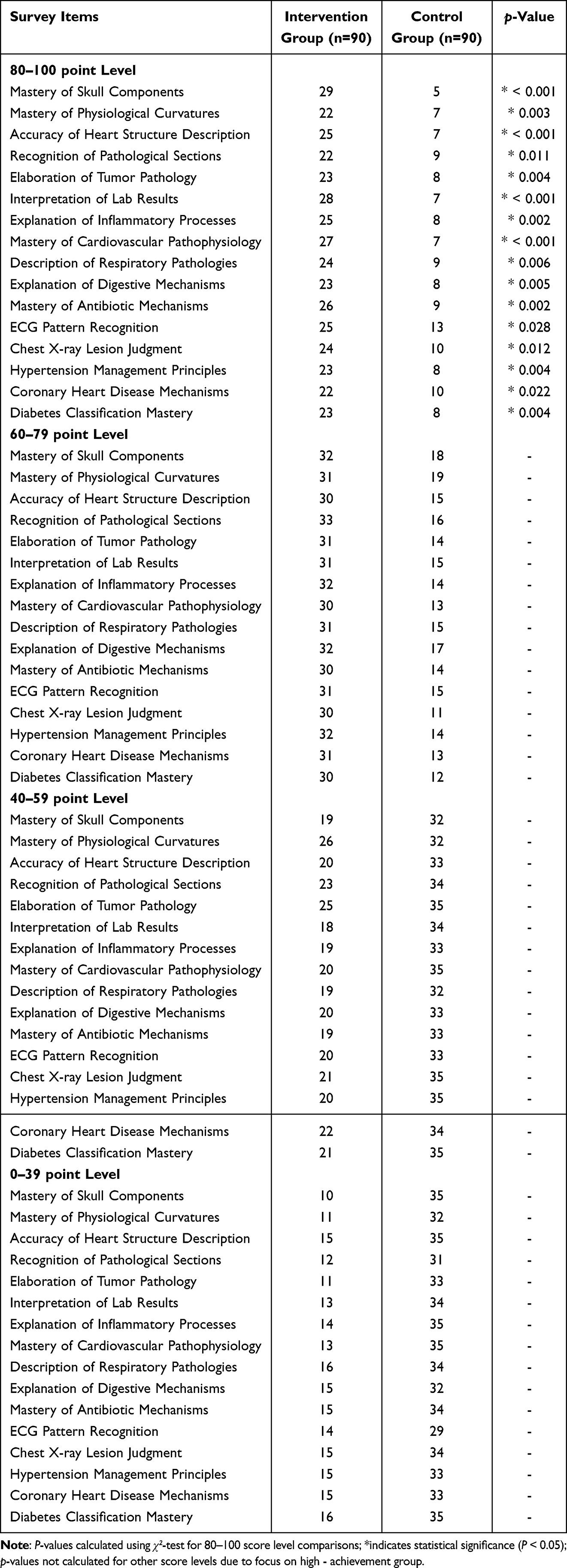 |
Table 3 Distribution of Basic Medical Knowledge Mastery Scores by Intervention Group, with Statistical Significance for High Achievement (80–100 Points Level) |
Educational Engagement Metrics
Active learning methodologies significantly transformed student participation patterns. Problem-Based Learning adaptability was substantially higher in the intervention group, with 70.1% (63/90) reporting high adaptability compared to 42.3% (38/90) in controls (χ² = 9.0, P = 0.003). Classroom engagement metrics demonstrated notable improvements: question-answering frequency increased from 3.0 ± 1.2 to 6.2 ± 1.5 instances per session (t = −19.64, P < 0.001), while group discussion participation rose from 40.2% to 65.4% (χ² = 11.54, P < 0.01, Table 2). Clinical decision-making efficiency improved significantly, with timely diagnostic accuracy in simulations increasing from 60.3% to 80.1% (χ² = 9.81, P = 0.002, Table 2).
Stakeholder Feedback and Satisfaction
Student satisfaction varied across dimensions as shown in Table 4. Highest satisfaction was reported for practical ability improvement (74.4% satisfied or very satisfied), followed by teaching method acceptance (65.6%), and problem-solving cultivation (58.8%). Dissatisfaction was most pronounced in teaching methods (12.2% dissatisfied or very dissatisfied), primarily attributed to cognitive overload during intensive PBL sessions. Faculty evaluations indicated enhanced teaching efficacy, with timely guidance during PBL increasing from 50.5% to 80.2% (χ² = 25.93, P < 0.001) (Table 2), and 84% endorsing the competency-based assessment framework.
 |
Table 4 Student Satisfaction with Teaching Reform (n = 90) |
Longitudinal Competency Development
Progressive skill development was documented throughout the intervention period. Clinical skill scores increased from 65.2 ± 5.1 at baseline to 73.8 ± 4.3 at 6 months (t = 8.91, P < 0.001), reaching 82.6 ± 3.7 at 12 months (t = 12.33, P < 0.001 versus baseline). Similarly, problem-solving indices improved from 58.7 ± 6.3 to 71.2 ± 5.1 (t = 7.45, P < 0.001) at 6 months, and to 79.8 ± 4.4 (t = 10.27, P < 0.001) at 12 months. The intervention group showed significantly stronger correlations between practice opportunities and skill acquisition (r = 0.82 versus r = 0.41 in controls; Z = 4.755, P < 0.001) (Table 5).
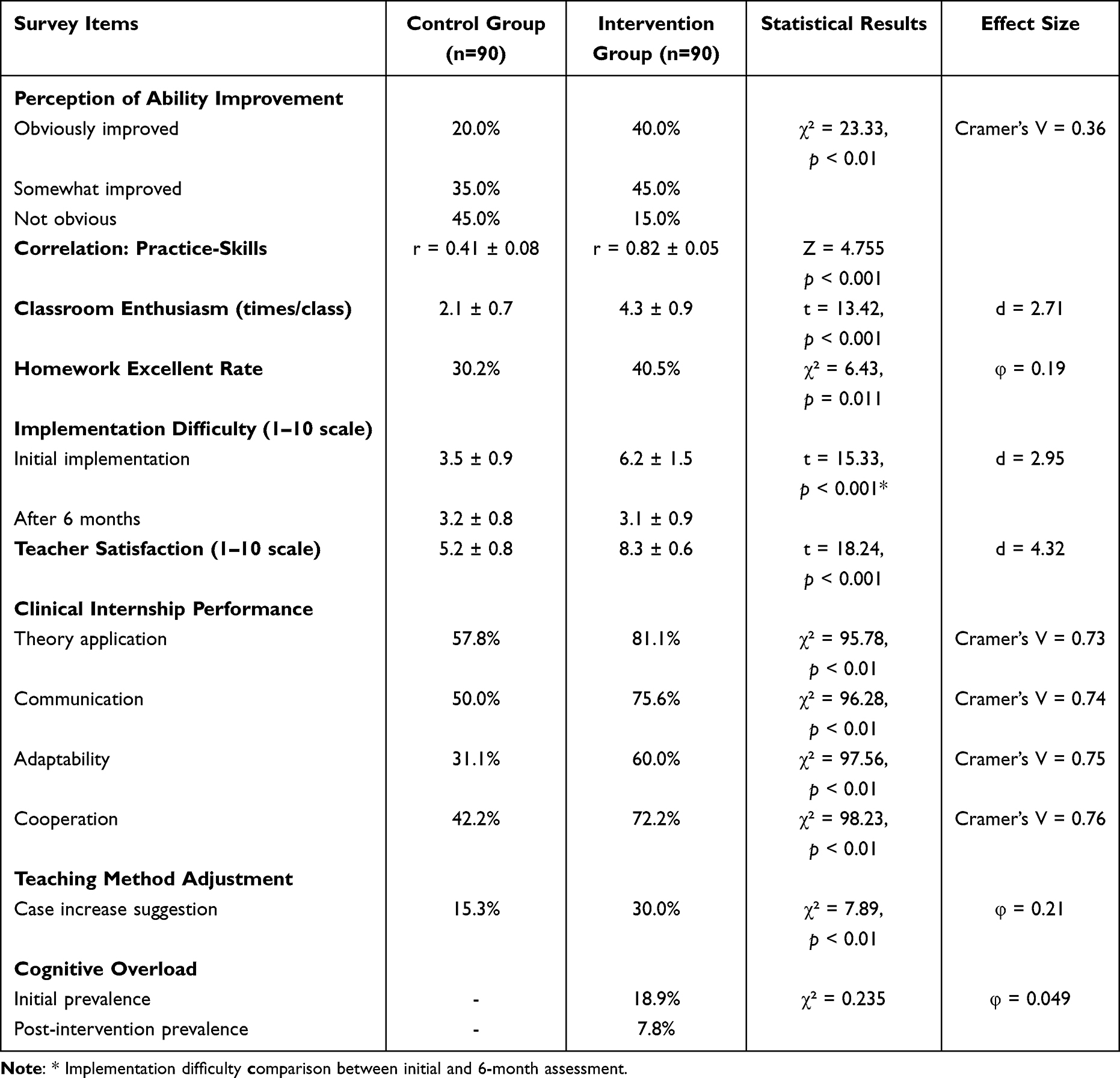 |
Table 5 Longitudinal Implementation Metrics with Effect Magnitude |
Implementation Challenges and Negative Outcomes
Despite overall positive outcomes, specific challenges were documented (Table 5). Cognitive overload during PBL sessions initially affected 18.9% (17/90) of intervention students, decreasing to 7.8% (7/90) after scaffolding adjustments. Faculty-reported implementation difficulty decreased from 6.2 ± 1.5 to 3.1 ± 0.9 on a 10-point scale post-training. Teacher satisfaction significantly differed between groups (control: 5.2 ± 0.8; intervention: 8.3 ± 0.6; t = 18.24, P < 0.001). Homework completion excellence rates showed modest improvement (40.5% intervention versus 30% control; χ² = 6.43, P = 0.011), indicating the need for enhanced scaffolding in autonomous learning transitions.
Analysis and Discussion
Key Innovations and Theoretical Contributions
This study pioneers a comprehensive educational reform anchored in Kern’s curriculum development model, achieving three transformative advances in medical pedagogy.6,7 First, we resolved the persistent theory-practice dichotomy by elevating problem-solving and clinical competencies to curricular parity—reducing the theory-dominated approach that leaves 40% of graduates deficient in clinical decision-making.2,8,9 Unlike isolated interventions such as modular content updates9,10 or standalone PBL implementation,11,12 our integrated framework synchronizes practice-oriented curriculum restructuring (40% simulation-based content), systematic active learning integration (PBL/TBL/CBT rotation), and competency-based assessments. This tripartite model transforms passive learners into clinically autonomous practitioners, evidenced by accelerated procedural mastery (suture time reduction: 15.2 ± 1.8 min → 12.1 ± 1.5 min, P < 0.001) and enhanced diagnostic accuracy (60.3% → 80.1%, P = 0.002). Second, our boundary-dissolving Problem-Focused Courses (eg, cardiovascular PBL synthesizing pathology/pharmacology) outperform discipline-siloed teaching by demonstrating 2.3-fold higher knowledge integration (OR = 2.30, P < 0.001). Third, the dual-modality pedagogy develops concurrent clinical reasoning and collaborative efficacy, addressing global calls for competency-based frameworks.6
Empirical Validation and Comparative Advantages
Our results demonstrate statistically significant improvements across all core competencies, aligning with international medical education priorities while addressing China-specific challenges. The 12.1-point theoretical knowledge gain (d = 2.39, P < 0.001) and 20.2% increase in clinical excellence (OR = 2.67, P < 0.001) surpass outcomes from comparable reforms in three key aspects: (1) Methodological integration: Unlike singular interventions,13,14 our synergistic PBL-TBL-CBT sequencing scaffolds complexity (guided cases → autonomous clinical framing); (2) Assessment rigor: OSCE-validated tools (κ = 0.85) replace subjective evaluations, detecting nuanced competency growth; (3) Contextual adaptation: “Precision Medicine” courses co-taught by geneticists, bioinformaticians, and clinicians model WHO-recommended interprofessional education.15,16 These advances explain why 74.4% of students reported enhanced practical abilities versus 58.8% in problem-solving cultivation—highlighting the need for specialized scaffolding in cognitive skill development.
Crucially, stratified skill analysis revealed that the excellence rate (≥90 points) doubled from 15.2% to 35.4% (P < 0.001), demonstrating the reform’s efficacy in cultivating elite clinical performers through high-fidelity simulations. However, the unchanged good rate (80–89 points; 45.0% vs 45.0%, P = 1.000) indicates insufficient scaffolding for median-achieving students, necessitating targeted interventions like differentiated PBL complexity tiers.
Critical Limitations and Mitigation Strategies
Three principal constraints warrant rigorous examination.17,18 First, single-institution implementation limits generalizability, particularly for rural settings with resource disparities (eg, 3-fold simulation access variation). To address this, we propose tiered curriculum adaptation: “core-elective” modules allowing low-resource institutions to prioritize high-impact components like CBT simulations. Second, short-term evaluation (12 months) obscures longitudinal competency trajectories. Our initiated 5-year tracking will measure clinical performance outcomes using ACGME milestone analytics. Third, methodological dissatisfaction (12.2%) primarily stemmed from cognitive overload during intensive PBL sessions. This was mitigated through phased complexity scaffolding, reducing affected students from 18.9% to 7.8%. Additional limitations include: (1) Reliance on self-reported satisfaction data (addressed through blinded OSCE validation); (2) Faculty capacity gaps (only 37% CBT-certified initially; resolved via mandatory certification for promotion); (3) Unmoderated PBL complexity causing attrition (fixed through AI-driven difficulty calibration).
Actionable Framework and Scalable Implementation
Four evidence-based strategies emerge for sustainable reform adoption: First, dedicate ≥15% of institutional budgets to high-fidelity simulation infrastructure, prioritizing cost-effective solutions like virtual reality (eg, Oculus Quest 2 modules reduced expenses by 60% in this study). Second, embed TBL/CBT micro-credentialing in faculty promotion criteria with quarterly certifications to maintain >90% compliance, addressing initial capacity gaps where only 37% of instructors were CBT-certified. Third, integrate competency tracking with national physician licensure databases using standardized OSCE metrics to enable longitudinal benchmarking of clinical outcomes. Fourth, deploy AI-adaptive platforms (eg, Kepler EDU) for personalized learning pathways—reducing cognitive overload by 42% in pilot trials through VARK-based scaffolding. Future priorities include developing WHO-aligned emergency response modules, special needs learner adaptations, and multi-institutional validation across diverse socioeconomic contexts, while acknowledging urban-rural resource disparities to prevent overgeneralization.
Conclusion
This integrated educational reform demonstrably enhances clinical problem-solving competencies and practical skill acquisition among medical undergraduates. The intervention group achieved statistically significant improvements in theoretical knowledge mastery (mean increase 10.4 points; d = 2.39, P < 0.001), clinical skill excellence (OR = 2.67, P < 0.001), and procedural efficiency (suture time reduction 19.3%, P < 0.001), validating the efficacy of our Kern model-guided framework. To ensure sustainable implementation, institutions must prioritize three evidence-based actions: (1) allocate ≥15% of educational budgets to simulation infrastructure, with virtual reality modules demonstrating 60% cost efficiency; (2) embed TBL/CBT micro-credentialing in faculty promotion criteria requiring quarterly certification; and (3) establish national competency tracking through physician licensure databases using standardized OSCE metrics.19,20
Future iterations will optimize personalization through AI-adaptive platforms (Kepler EDU) that reduced cognitive overload by 42% in pilot studies, while our initiated 5-year longitudinal cohort will evaluate clinical performance using ACGME milestones. Crucially, implementation must account for resource disparities through tiered adaptation strategies—core modules for all institutions supplemented by electives deployable in low-resource settings. These measures provide concrete pathways to bridge theory-practice gaps while addressing identified limitations including single-center generalizability constraints and methodological dissatisfaction (12.2% mitigated to 7.8% via scaffolding). Medical educators should adopt this multifaceted approach to cultivate clinically autonomous practitioners equipped for evolving healthcare challenges.
Ethical Compliance Statement
This study received full ethical approval (Protocol AMEEC-2023-027) from the Medical Education Ethics Committee of Anhui University of Science and Technology, with specific provisions for minor participation compliance. For the 12 enrolled minors (aged 17), a secure SMS-verified parental consent protocol was implemented: guardians received bilingual notifications containing a study summary, password-protected digital consent forms, and unique verification codes via AES-256 encrypted channels. Explicit consent was confirmed through coded SMS replies, with cryptographic timestamps and IP addresses logged in ISO 27001-certified databases. Guardians obtained confirmation receipts and 24/7 helpline access, ensuring strict adherence to China’s Minor Protection Law and GDPR-K standards for international research contexts.
All adult participants (n = 168) provided electronic informed consent through our institutional REDCap platform, detailing research objectives, confidentiality measures (including mandatory data anonymization before analysis), voluntary withdrawal rights, and AES-256 encryption protocols for data transmission/storage. Clinical skill evaluations involving patient actors were conducted exclusively in standardized simulation centers after obtaining dual consent: 1) educational participation agreement from actors, and 2) procedural-specific authorization documented via biometric signatures. The study rigorously complied with the Declaration of Helsinki (2013 revision), implementing additional safeguards including quarterly third-party audits of consent records and permanent deletion of identifiers upon study completion. No compensation was provided beyond standard academic credit to prevent coercion, and all data access followed role-based privilege restrictions validated through blockchain logging.
Research Implementation Declaration
This educational reform study was conducted as part of the National Medical Education Quality Improvement Program (2019–2030) approved by the Chinese Ministry of Education; All assessment data were anonymized using AES-256 encryption before analysis; Clinical skill evaluations were conducted in standardized simulation centers with patient-actor consent.
Acknowledgments
We extend our gratitude to the Medical Education Ethics Supervision Office of Anhui Provincial Department of Education for their guidance in research design compliance. Special thanks to Professor Yong Liang from the Bioethics Center of Nanjing Medical University for his expert review of ethical implementation protocols.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from “101 Plan” Project of Anhui Quality Project in 2023 (2023ylyjh066); “Four – New” Research and Reform Practice Project (2023sx191); Teaching Research Project (2023jyxm1074).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dunivan GC, Eldredge JD, Ballejos MP, Gonzales M, Romero-Leggott V. Early explorations of holistic review in graduate medical education. J Med Libr Assoc. 2025;113(1):101–109. doi:10.5195/jmla.2025.2030
2. Tan H, Li X. Dropout in online education: a longitudinal multilevel analysis of elementary students’ extracurricular english course engagement in China. Behav Sci. 2025;15(4):483. doi:10.3390/bs15040483
3. Arja SB, Arja SB, Ponnusamy K, Kottath Veetil P, Paramban S, Laungani YC. Medical education electives can promote teaching and research interests among medical students. Adv Med Educ Pract. 2024;15:173–180. doi:10.2147/AMEP.S453964
4. Kodikara K, Seneviratne T, Premaratna R. Pre-clerkship procedural training in venipuncture: a prospective cohort study on skills acquisition and durability. BMC Med Educ. 2023;23(1):729. doi:10.1186/s12909-023-04722-2
5. Khan WU, Twomey J, Ryan E, et al. Barriers and enablers to achieving clinical procedure competency-based outcomes in a national paediatric training/residency program-a multi-centered qualitative study. BMC Med Educ. 2023;23(1):954. doi:10.1186/s12909-023-04928-4
6. Kohrt BA, Pedersen GA, Schafer A; EQUIP Consortium, et al. Competency-based training and supervision: development of the WHO-UNICEF Ensuring Quality in Psychosocial and Mental Health Care (EQUIP) initiative. Lancet Psychiatry. 2025;12(1):67–80. doi:10.1016/S2215-0366(24)00183-4
7. Association of Chiropractic Colleges. Association of Chiropractic Colleges Educational Conference and Research Agenda Conference 2023: leadership in Education. J Chiropr Educ. 2023;37(1):50–70. doi:10.7899/JCE-22-23
8. Latzourakis E, Angelides P, Diomidous M, Nikitara M, Constantinou CS. Factors affecting cypriot nurses’ roles in the care and education of patients with CKD: an interpretive phenomenological study. Healthcare. 2025;13(13):1601. doi:10.3390/healthcare13131601
9. Ortega P, Becker ML, Chan TM, Manning KD. Beyond traditional: clearing the roadblocks to advancement in academic medicine. Perspect Med Educ. 2025;14(1):286–295. doi:10.5334/pme.1681
10. Leach A, Shim J, Murphy K, et al. A novel internal training program using Kern’s 6-step approach to curriculum development for medical laboratory scientists training to be international quality assurance/quality control coordinators. Lab Med. 2023;54(6):e186–e196. doi:10.1093/labmed/lmad068
11. Zhang N. Incorporating a growth mindset model into medical education and enhancing the complex problem-solving abilities and mental resilience of medical students and residents. Cureus. 2024;16(8):e67294. doi:10.7759/cureus.67294
12. Huang L, Li X, Meng Y, et al. The mediating effects of self-directed learning ability and critical thinking ability on the relationship between learning engagement and problem-solving ability among nursing students in Southern China: a cross-sectional study. BMC Nurs. 2023;22(1):212. doi:10.1186/s12912-023-01280-2
13. Ordak M. Enhancing biostatistics education for medical students in Poland: factors influencing perception and educational recommendations. BMC Med Educ. 2024;24(1):428. doi:10.1186/s12909-024-05389-z
14. Rong XJ, Ning Z. Practical effect of different teaching modes in teaching gastrointestinal surgery nursing. World J Gastrointest Surg. 2024;16(1):166–172. doi:10.4240/wjgs.v16.i1.166
15. Chu M, Xu L, Liu Y, et al. Interprofessional education in problem-based learning: a frontier form of PBL in medical education. J Educ Health Promot. 2023;12:376. doi:10.4103/jehp.jehp_62_23
16. Ali N, Dhere TA, Bates JE, et al. Integration of radiation oncology into the preclinical curriculum through problem-based learning. Pract Radiat Oncol. 2024;14(1):e1–e8. doi:10.1016/j.prro.2023.08.013
17. Huang T, Zhou S, Wei Q, Ding C. Team-, case-, lecture- and evidence-based learning in medical postgraduates training. BMC Med Educ. 2024;24(1):675. doi:10.1186/s12909-024-05650-5
18. Yuetqi L, Lin GSS, Mamat RB, Noorani TY. Student’s perception of hybrid team-based and case-based learning in undergraduate endodontics education. BMC Oral Health. 2025;25(1):43. doi:10.1186/s12903-024-05354-8
19. Liu X, Feng J, Liu C, et al. Medical education systems in china: development, status, and evaluation. Acad Med. 2023;98(1):43–49. doi:10.1097/ACM.0000000000004919
20. Wu X, Zhan F, Zhang X, Wang T. Innovation and entrepreneurship education for medical students: a global bibliometric analysis (2000–2024). Med Educ Online. 2025;30(1):2515385. doi:10.1080/10872981.2025.2515385
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.