Back to Journals » Clinical Interventions in Aging » Volume 17
Implementing Falls Prevention in Primary Care: Barriers and Facilitators
Authors Meekes WMA ![]() , Leemrijse CJ
, Leemrijse CJ ![]() , Korevaar JC
, Korevaar JC ![]() , Stanmore EK, van de Goor LAM
, Stanmore EK, van de Goor LAM
Received 24 January 2022
Accepted for publication 11 April 2022
Published 2 June 2022 Volume 2022:17 Pages 885—902
DOI https://doi.org/10.2147/CIA.S354911
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Wytske MA Meekes,1,2 Chantal J Leemrijse,2 Joke C Korevaar,2 Emma K Stanmore,3 Lamberdina (Ien) AM van de Goor1
1Tranzo, Tilburg School of Social and Behavioral Sciences, Tilburg University, Tilburg, Netherlands; 2Nivel, Utrecht, Netherlands; 3School of Health Sciences, University of Manchester, Manchester, UK and Manchester Academic Health Science Centre (MAHSC), Manchester, UK
Correspondence: Wytske MA Meekes, Tranzo, Tilburg School of Social and Behavioral Sciences, Tilburg University, Postbus 90153, Tilburg, 5000 LE, Netherlands, Tel +31 13 466 4451, Email [email protected]
Purpose: Limited information is available concerning primary care providers’ encountered barriers and facilitators when implementing falls prevention and providing interventions in a real-life setting. This study aimed to identify barriers and facilitators when i) implementing a falls risk assessment strategy at GP practices and among community nurses and ii) providing evidence-based falls prevention interventions in a real-life setting to independently living, frail older people.
Methods: A researcher’s journal was maintained during the implementation of a falls risk assessment strategy, which entailed notes from informal conversations with GPs, practice nurses and community nurses. After implementation, two online focus groups with GPs, practice and community nurses, physio- and exercise therapists were conducted. Data were thematically analyzed.
Results: Data were collected from 32 GPs, 13 practice nurses, eight community nurses, nine physiotherapists, and two exercise therapists. The GPs and nurses acknowledged that falls prevention is part of their job, meaningful, and that they have sufficient knowledge and skills to offer falls prevention. Collaboration, a previously implemented care program for older people, resources, reimbursement for interventions, and patients’ motivation, awareness and health issues were considered to be important factors for the implementation of falls prevention. Physio- and exercise therapists described collaboration with different disciplines, receiving sufficient referrals, reimbursements, intensity and set-up of the interventions, and patients’ motivation, expectations, goals, self-confidence, awareness, and health issues as important factors when providing falls prevention interventions.
Conclusion: This study identified care provider-, context-, patient-, and innovation (strategy)-related barriers and facilitators when implementing falls prevention and providing interventions in primary care. Development of a more successful implementation strategy should focus on intensifying collaboration, reimbursement for interventions, availability of resources, and patients’ lack of motivation and health issues. Hence, falls prevention may become more structurally applied, reducing a major threat for the quality of life of independently living older people.
Keywords: falls prevention, implementation, barriers and facilitators, frail older people, primary care
Introduction
Falls among older people are a major public health problem.1 Approximately, 30% of people aged ≥65 years and 42% of people aged ≥75 years fall at least once a year.2–5 Worldwide, over 37 million falls occur annually that require medical attention, resulting in approximately 646,000 deaths each year.6,7 These numbers are expected to increase further as society is aging.8
An important risk factor for falls appears to be frailty.9 Frailty can be defined as a state of increased vulnerability to poor resolution of homoeostasis after a stressor event, which increases the risk of adverse outcomes, including delirium, disability, and falls.10–13 Many falls risk factors can be associated with frailty, such as impaired balance and strength, use of sleep medication, dizziness and fear of falling.14–16 Therefore, frail older people are an important group to focus on in regards to the provision of falls prevention.
Falls can result in a reduction in quality of life and independence and may cause, for example, bruising, hip fractures, brain injuries, and even death.17 Previous research shows that several interventions are available to prevent falls and fall-related trauma among independently living older people.18–21 Falls prevention interventions differ per target group in intensity, type of treatment, and approach. Overall, multifactorial programs with evidence-based interventions are recommended.22,23 Most evidence-based interventions are provided by physio- and exercise therapists. Nonetheless, older people often do not realize they have a high falls risk and/or are unfamiliar with available falls prevention interventions. Therefore, it is important that qualified health care providers guide older people to participate in these interventions offered by certified physio- and exercise therapists.24,25
In the Netherlands, as well as in many other countries, general practitioners (GPs), their practice nurses, and community nurses can be considered the designated health care providers to identify high falls risk and to provide falls prevention because they have insight in their patients’ medical history, home setting and social network, and are often the first point of contact for health issues. Nonetheless, systematic assessment for falls risk does not take place at Dutch GP practices nor among community nurses.26 GPs, for example, are only aware of 20–30% of the falls of their patients because older patients often do not inform their GPs.27,28 Consequently, primary care providers are frequently unaware which of their patients have an increased risk of falling and are, therefore, less capable to offer them timely and adequate falls prevention care.29–31 These issues occur internationally.29,30 For example in England, there is a lack of awareness among GPs regarding the falls prevention clinical guidelines, and only 30% of the GPs asked older patients if they had fallen during consultations.29 This lack of systematic falls risk assessments leads to the unfavorable situation in which frail older people, for whom falls prevention interventions are potentially effective, do not receive this care.
According to Paul et al, a systematic approach for identifying risks and addressing them in a concerted manner is key to falls prevention.32 Therefore, the implementation of falls prevention with a systematic and targeted assessment strategy at GP practices and community nurses may be a solution to make falls prevention more accessible for independently living, frail older people. To improve the implementation and make long-term engagement in falls prevention possible, it is important to identify and understand the experienced barriers and facilitators of the implementation of such a falls risk assessment strategy.
Previous studies have identified barriers and facilitators for the implementation of falls prevention in different care settings. Child et al identified, that practical considerations, adapting to community, and psychosocial factors can influence implementation of falls prevention interventions.33 Furthermore, McConville and Hooven conducted a review about factors influencing the implementation of falls prevention in the primary care setting.34 They identified that care providers’ beliefs and practice, lack of knowledge, time constraints, patient engagement and financial issues can negatively influence implementation. Nonetheless, the study of McConville and Hooven mainly focused on barriers, whereas facilitators may be more important for successful implementation.34–36
These two reviews provide important insights in the barriers and facilitators for implementation and provision of falls prevention and interventions. However, knowledge is limited regarding specific barriers and facilitators when implementing a systematic falls risk assessment strategy at GP practices and community nursing teams. In addition, most knowledge regarding barriers and facilitators of physio- and exercise therapists encountered when providing evidence-based falls prevention interventions is retrieved from studies conducted in controlled settings. Consequently, also specific knowledge is lacking concerning the barriers and facilitators physio- and exercise therapists encounter when providing evidence-based interventions among older people in a real-life setting. Therefore, this study aims to;
- identify barriers and facilitators encountered by GPs, practice nurses and community nurses when implementing a falls risk assessment strategy, and
- identify barriers and facilitators encountered by physio- and exercise therapists when providing evidence-based falls prevention interventions among independently living, frail older people in a real-life setting.
Materials and Methods
Design
This study is a sub-study of a larger implementation study. The methods of the implementation study are described in our study protocol article.37 In short, a systematic and targeted falls risk assessment strategy was implemented at GP practices and among community nurses in the area Midden-Brabant, in the Netherlands. The falls risk assessment strategy used in the implementation study consisted of tools for assessing high falls risk and identifying the underlying cause(s), an accredited training course regarding falls prevention for professionals, and service provision by certified physio- and exercise therapists who are able to offer evidence-based falls prevention interventions.38–41 The participating GPs and nurses systematically assessed high falls risk, identified underlying causes and provided adequate care (eg referral to occupational therapist or physiotherapist, medical review) to their independently living, frail older patients. If relevant, patients received evidence-based falls prevention interventions from certified physio- or exercise therapists in the area.
This sub-study aimed to identify barriers and facilitators of the implementation process (from assessing falls risk to providing falls prevention interventions) in a real-life setting. Data collection included a researcher’s journal and two online focus groups with the care providers involved.
A researcher’s journal was kept during the implementation of the falls risk assessment strategy, a period of 16 months. The researcher’s journal entails notes from unstructured interviews, also known as informal conversational interviews, with participating GPs and nurses.42,43 The researcher had one contact person at each GP practice, who conducted most falls risk assessment tasks. The unstructured interviews were conducted every 4–6 weeks via phone calls, secure messenger apps, or face-to-face meetings. The purpose of the unstructured interviews was to identify barriers and facilitators the health care providers encountered while implementing the falls risk assessment strategy during daily practice.
In addition, two online focus groups were conducted to identify the more general encountered barriers and facilitators while implementing and providing falls prevention in a real-life setting. The online focus groups were conducted after the implementation period and participation was voluntary. In the first online focus group, barriers and facilitators among GPs, practice nurses and community nurses were identified when implementing the systematic and targeted falls risk assessment strategy. In the second online focus group, barriers and facilitators were investigated among physio- and exercise therapists when providing evidence-based falls prevention interventions. For the online focus groups, an online platform was used. Participants could login anonymously after receiving login-details. During a period of two weeks, each day a question was published on the platform and participants received a notifying email. Participants could respond to these questions and to responses of other participants. Participants were able to login during these two weeks when it suited them best. They could also respond to earlier posted questions, not only on the question of the day.
Setting
In 2011, a home care organization and a GP care group (owned by 155 GPs) in the area Midden-Brabant, the Netherlands, developed a strategy to improve healthcare for frail older people, which led to the Care Program for Frail Older People.44 As part of this Care Program for Frail Older People, frailty in older people is systematically assessed and registered by using the Transmural Care Assessment Geriatrics instrument (Dutch: “TRAnsmuraal Zorg Assessment Geriatrie (TRAZAG) instrument”), the Tilburg Frailty Indicator or the care provider’s clinical judgement.45,46 The implementation study, of which this study is a sub-study, was carried out in collaboration with the GP care group and home care organization. The implementation study aimed to implement the systematic falls risk assessment strategy which was complementary to the Care Program for Frail Older People.
Provision of Evidence-Based Falls Prevention Interventions by Physio- or Exercise Therapists
The participating physio- and exercise therapists offered one of the following evidence-based falls prevention interventions: A Matter of Balance-NL (Dutch: “Zicht op Evenwicht”), In Balance (Dutch: “In Balans”), Nijmegen Falls Prevention Program (Dutch: “Vallen Verleden Tijd”), or OTAGO (see Appendix I).47–54 These interventions are described by the Dutch Center for Healthy Living as qualified evidence-based falls prevention exercise programs.55,56 This Center has a database containing prevention interventions available in the Netherlands ranked by level of evidence.56 The physio- or exercise therapists offered the evidence-based falls prevention interventions customized to the needs and wishes of the patient.
Recruitment
Recruitment for this study took place within the implementation study. A flowchart of the recruitment within the implementation study can be found in Appendix II.
GP Practices and Community Nurses
A contact person of each GP practice and all community nurses participating in the implementation study, participated in the unstructured interviews for the researcher’s journal. All GPs and nurses participating in the implementation study were invited to also participate in the online focus group through e-mails, phone calls, and/or secure messenger apps.
Physio- and Exercise Therapists
All physio- and exercise therapists participating in the implementation study and who received at least one or more referrals from a GP practice or community nurse were invited to participate in the online focus group. The therapists were invited through e-mails and phone calls.
Ethical Approval
This study is approved by the Medical Ethical Committee Brabant, Netherlands (NL61582.028.17/ P1732) and registered at the Netherlands Trial Register, NL7917. Participating health care providers signed a research agreement in which they gave consent to collect data during this study and publish anonymized responses. Participation of the health care providers was voluntary in every phase of data collection.
Theoretical Framework
The Theoretical Domains Framework (TDF) described by Atkins et al and Huijg et al informed the analysis of the experienced barriers and facilitators when implementing the falls risk assessment strategy.57,58 The TDF helps to explain and understand what may influence the care provider’s behavior change. According to Atkins et al, the TDF does not propose testable relationships between the domains, but it provides a theoretical lens through which to view factors that may influence the care providers’ behavior.57
The domains of the TDF (see Table 1) were both used to create a topic list for the focus groups and to guide the analysis of the results.
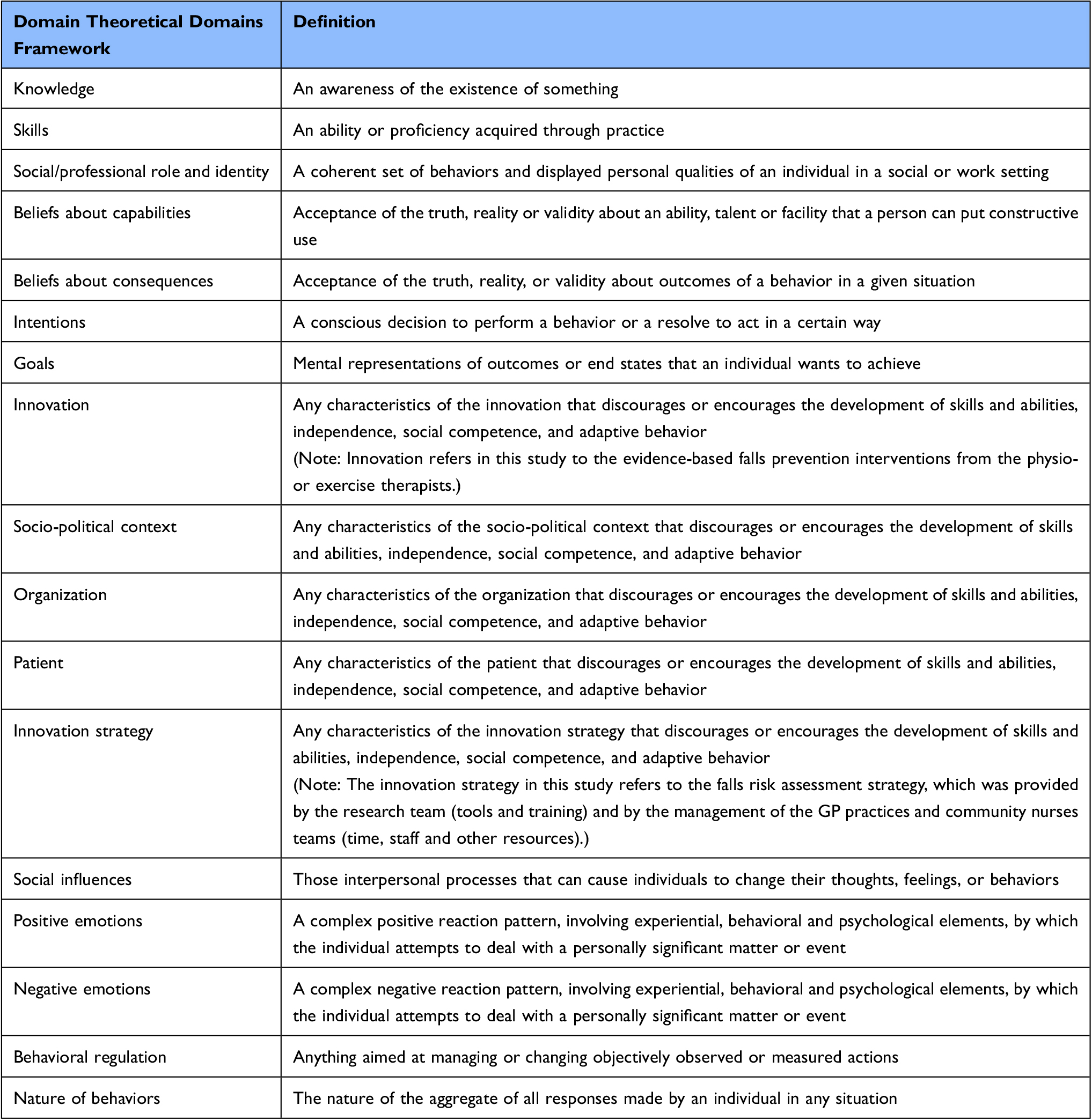 |
Table 1 Theoretical Domains Framework Domains Used in This Study as Presented and Described by Huijg et al58 |
Analysis
The experienced barriers and facilitators, drawn from the notes of the unstructured interviews in the researcher’s journal, were listed and reported.
The written responses from the online focus groups were downloaded from the online platform and imported into ATLAS.ti 8 coding program for qualitative data analysis.59 The results from the online focus groups were independently coded by two researchers (WM and IG). The codes were discussed and a coding scheme was developed based on the different themes that emerged, see Appendix III. After consensus was reached, the coding was thematically analyzed by two researchers (WM and IG).
A directed content analysis approach was used when collecting, analyzing, and describing the data.60,61 The TDF helped to understand, analyze, and interpret the barriers and facilitators encountered by the participants.
Results
Participation of GPs and Nurses
GPs, practice nurses and community nurses were invited to participate in this study to identify barriers and facilitators encountered when implementing the falls risk assessment strategy. The researcher’s journal, with notes from unstructured interviews conducted during implementation, concerned 32 GPs, 13 practice nurses (from twelve GP practices) and eight community nurses. In the online focus group participated two GPs, four practice nurses, and four community nurses.
GPs’ and Nurses’ Barriers and Facilitators When Implementing a Falls Risk Assessment Strategy
The identified barriers and facilitators experienced by the GPs, practice nurses and community nurses when implementing the falls risk assessment strategy are summarized in Figure 1A and B. In these figures, the identified barriers and facilitators are categorized into four broader categories identified during data analysis: care provider-, context-, patient-, and innovation strategy-related characteristics. The results are further described according to the domains of the TDF (as mentioned in Table 1). Figure 1 Continued. Figure 1 (A) GPs and nurses encountered barriers when implementing and providing falls prevention. (B) GPs and nurses encountered facilitators when implementing and providing falls prevention. aData from researcher’s journal. bData from focus groups.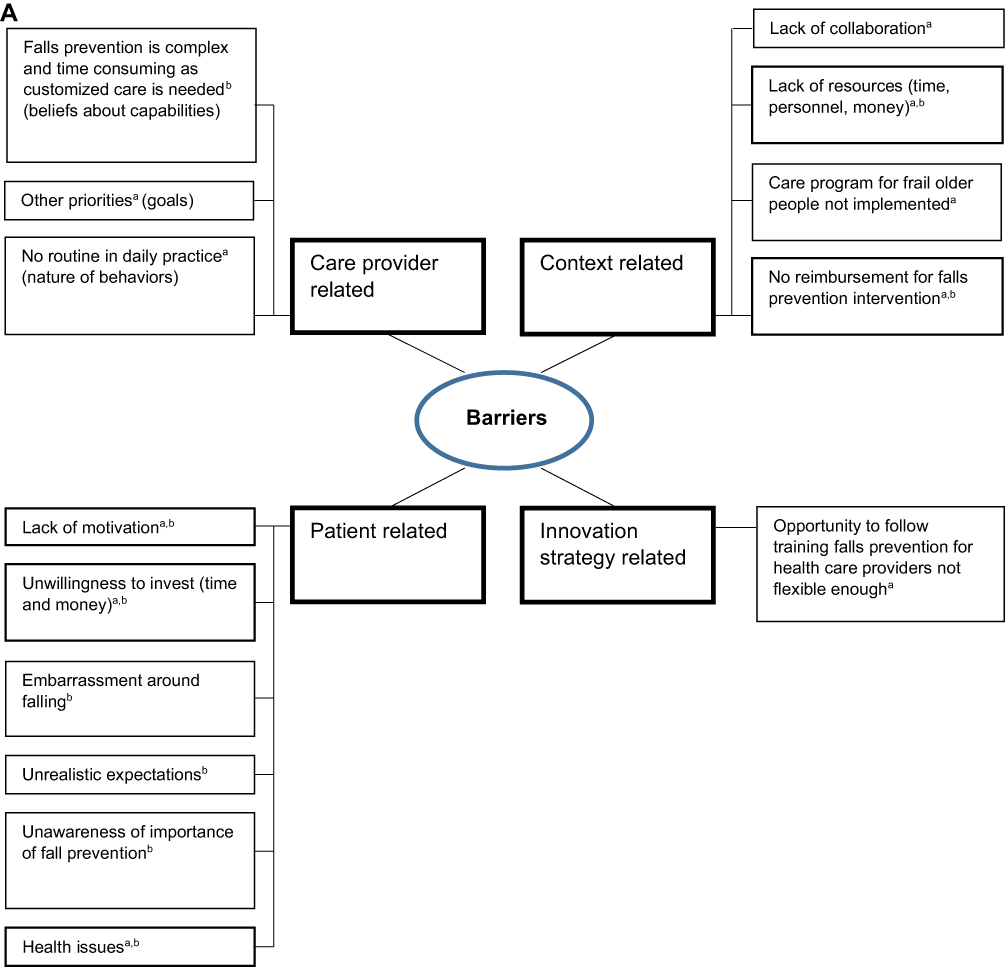

Care Provider-Related Characteristics
The GPs and nurses described several care provider characteristics that influenced implementation and provision of falls prevention that can be related to the following domains of the TDF: social and professional role and identity, beliefs about consequences, knowledge and skills, beliefs about capabilities, intentions and goals, and the nature of behaviors and behavioral regulation.
Social and professional role and identity: All GPs and nurses in the FG believed that the provision of falls prevention is part of their work. Participants described that the role of the GP is to signal high falls risk and of the practice nurses to identify high falls risk and underlying causes and to refer patients to interventions. Some participants described that the role of the community nurses was to assess high falls risk, start the conversation with the patient and subsequently refer the patient to the GP and practice nurse. Most participants mentioned that the practice nurse played a key role in the provision of falls prevention care at GP practices, which was also confirmed in the researcher’s journal.
Beliefs about consequences: All GPs and nurses in the FG believed the provision of falls prevention care is important and useful. Reasons why they believed it is useful were: prevention of fractures to maintain quality of life, reduction of fear of falling, maintaining patients’ peace, improvement of patient’s movement radius, and maintenance of independently living, physical and mental health. A few participants mentioned in specific the importance of systematic falls risk assessment:
I find this [assessment of high falls risk] useful. Even though you regularly visit older people, they do not always tell that they fell or almost fell or have a fear of falling. With these questions, you start the conversation and you let people reflect about what they think. But you also have an entrance to look together at possible ways to prevent falls (Care provider 10, Community nurse, FG 1)
Knowledge and skills: In the FG, almost all participants reported that they have the knowledge and skills to provide falls prevention care. Some participants also described the importance of additional probing questions when assessing high falls risk, especially when patients hesitate while answering.
Furthermore, some participants described that insight in other care providers’ expertise was important when implementing falls prevention.
Beliefs about capabilities: The GPs and nurses said that the provision of falls prevention care entails many different tasks and differs for each patient, so customized care is needed. This can make the provision of falls prevention care complex and time consuming. Many participants underlined to experience a lack of time when implementing the falls risk assessment strategy.
Intentions and goals: Most participants mentioned that they intend to provide falls prevention care in the future. However, their intentions sometimes seemed to strongly depend on whether or not experienced barriers such as lack of time could be overcome.
Priority to provide falls prevention varied among participants. High priority was related to the relevance of reducing falls and maintaining patients’ independence. According to data from the researcher’s journal, the priorities of some GP practices and community nurses changed during the implementation of the assessment strategy, which negatively influenced implementation of falls prevention. Priorities changed due to urgent matters such as practice takeover, practice split, reorganization of teams, and/ or sickness in family of the health care provider even though the health care providers were initially motivated to implement falls prevention.
Nature of behaviors and Behavioral regulation: Successful implementation of falls prevention in daily routine seemed to vary. Some care providers described that they identified all (eligible) frail older patients with high falls risk after a period of time. After this period, assessment of high falls risk and identification of underlying causes becomes incidental and not automatic and part of daily routine.
Data from the researcher’s journal noted that highly motivated practice nurses encouraged their colleagues to provide falls prevention care by informing and reminding them about the importance of falls prevention. They also most often conducted all the falls prevention related tasks in the GP practice.
Participants also mentioned that by actively involving informal caregivers when providing falls prevention, patients’ retention to interventions could be improved.
Context-Related Characteristics
Aspects with respect to care providers’ social support, the organization of the GP practices and nursing teams, as well as certain socio-political factors were mentioned as context-related characteristics that influenced implementation of the falls risk assessment strategy.
Social influences: Support from other care providers when implementing the assessment strategy was experienced differently. Participants who experienced insufficient support, tried to compensate this by involving other care providers such as the GP (for community nurses) or physiotherapist.
Organization: Participants described that good collaboration between different disciplines is essential to provide falls prevention care. The researcher’s journal also described that, in specific, communication between care providers was important when implementing the falls risk assessment strategy. When, for example, the GP did not adequately communicate with the practice nurse about falls prevention, due to other priorities, implementation of the assessment strategy did not start or was less successful.
All participants experienced a lack of time when providing falls prevention care. Data from the research journal also confirmed that lack of time was a serious obstacle. Participants described that they have to conduct many different tasks when providing falls prevention care, which also differs for each patient:
The execution of it, assessing, looking at causes at home, looking at the medication list, judging what should be stopped, starting treatment, and discussing this all, is not feasible in the available time. Often, all this must be included to the existing tasks, for example during a visit which was requested for another reason. Luckily, we have now expansion within our team of a practice nurse-somatic, with a focus on older people. The average time [needed for each patient] is difficult to estimate. It varies a lot and it often requires more time than initially anticipated. (Care provider 8, GP, FG 1)
All this makes provision of falls prevention care complex and time consuming. More time, money or personnel, factors related to one another, are desired to be able to conduct all tasks adequately.
According to data from the researcher’s journal, implementation of the assessment strategy appeared to be more successful among GP practices that have a “Care Program for Older People” already in place compared to GP practices that do not have this program in place. Within this program, patients are screened for frailty and seen by the GP or practice nurse at least twice a year.
Socio-political context: According to the GPs and nurses, costs are a barrier for patients to participate in falls prevention interventions. Patients are often unwilling to start or continue an intervention if it is not reimbursed by their health insurance. Furthermore, according to data from the researcher’s journal, participants also experienced it as demotivating to assess high falls risk, identify underlying causes and refer to falls prevention interventions when, in the end, the patient cannot afford the intervention anyway.
Patient-Related Characteristics
As described above, patients’ willingness to pay (additional) costs for an intervention appeared to influence their decision to start and complete an intervention.
In the FG, the GPs and nurses described two other patient characteristics that seem to influence the provision of falls prevention care: patients’ motivation and their health issues.
The participants described that motivation to start and complete falls prevention interventions varies strongly among patients. Most participants experienced patients’ lack of motivation:
“It is difficult to motivate elderly patients to participate in falls prevention treatment.” (Care provider 5, Practice nurse, FG 1)
According to the GPs and nurses, patients’ motivation can be influenced by their willingness to invest time and money, embarrassment, expectations and (un)awareness. They described that patients sometimes have the unrealistic expectation that their GP can solve their problems during one consultation, which can negatively influence their motivation. Some participants reported that patients are often unaware of the importance of falls prevention or have counteracting beliefs (eg “I already fell so it is useless now”, “I will not fall because I am careful”). According to the participants, a reason for this could be the lack of falls prevention education for patients. The GPs and nurses believe that improving patient’s awareness and understanding about the importance of falls prevention care can enhance their motivation.
Furthermore, the participants highlighted that patients’ poor health, comorbidities or frailty could negatively influence the provision of falls prevention care.
Innovation Strategy-Related Characteristics
The assessment instrument used in this study was described by some care providers as short, clear, and easy to integrate into other assessments or consultations.
According to data from the researcher’s journal, the implementation of falls prevention seemed to be less successful (none or fewer patients identified with high falls risk and referred to falls prevention care) when the practice nurse did not follow the “Falls prevention training for health care providers”, which was offered for free at three different days within the implementation strategy.
Participation of Physio- and Exercise Therapists
Physio- and exercise therapists were recruited to identify barriers and facilitators encountered when providing evidence-based falls prevention interventions in a real-life setting. Out of the 38 therapists participating in the implementation study, 15 therapists received one or more referrals from a GP practice or community nurse. Nine physiotherapists and two exercise therapists agreed to participate in the FG to identify experienced barriers and facilitators when providing evidence-based falls prevention interventions.
Therapists’ Barriers and Facilitators When Providing Falls Prevention Interventions
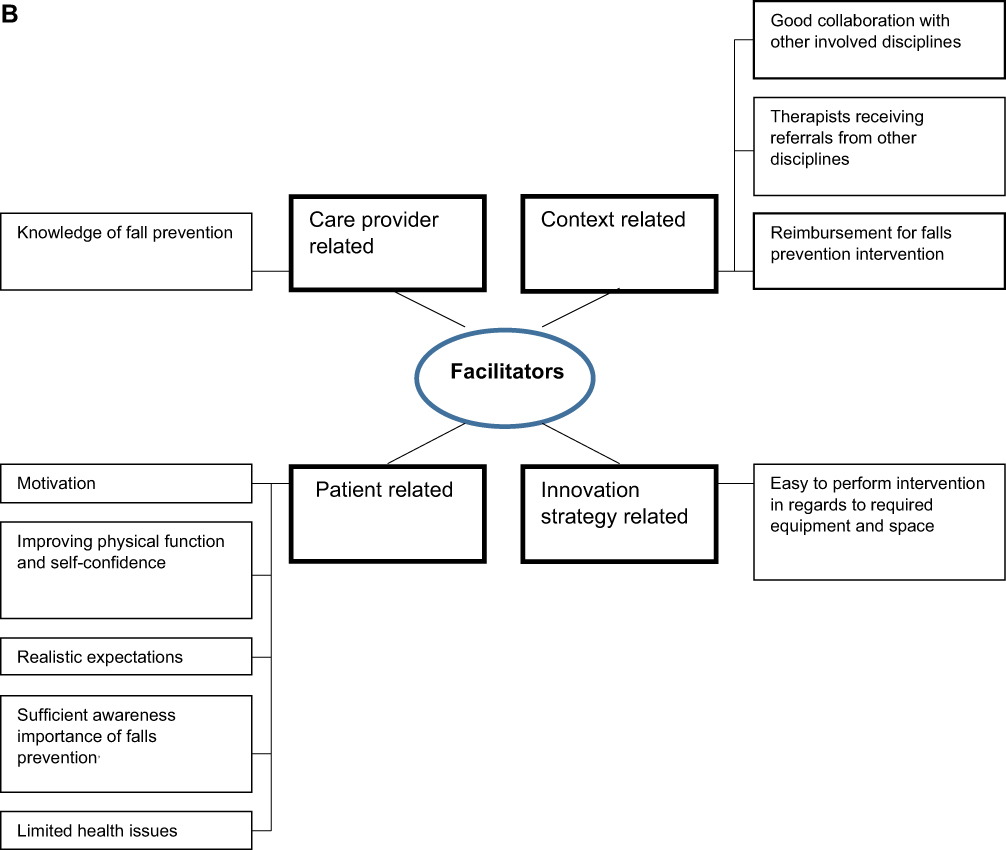
The identified barriers and facilitators experienced by the physio- and exercise therapists, retrieved from the second online FG, are summarized in Figure 2A and B. The identified barriers and facilitators are described according to domains of the TDF as above (see Table 1). Figure 2 Continued. Figure 2 (A) Physio- and exercise therapists encountered barriers when providing falls prevention interventions. (B) Physio- and exercise therapists encountered facilitators when providing falls prevention interventions.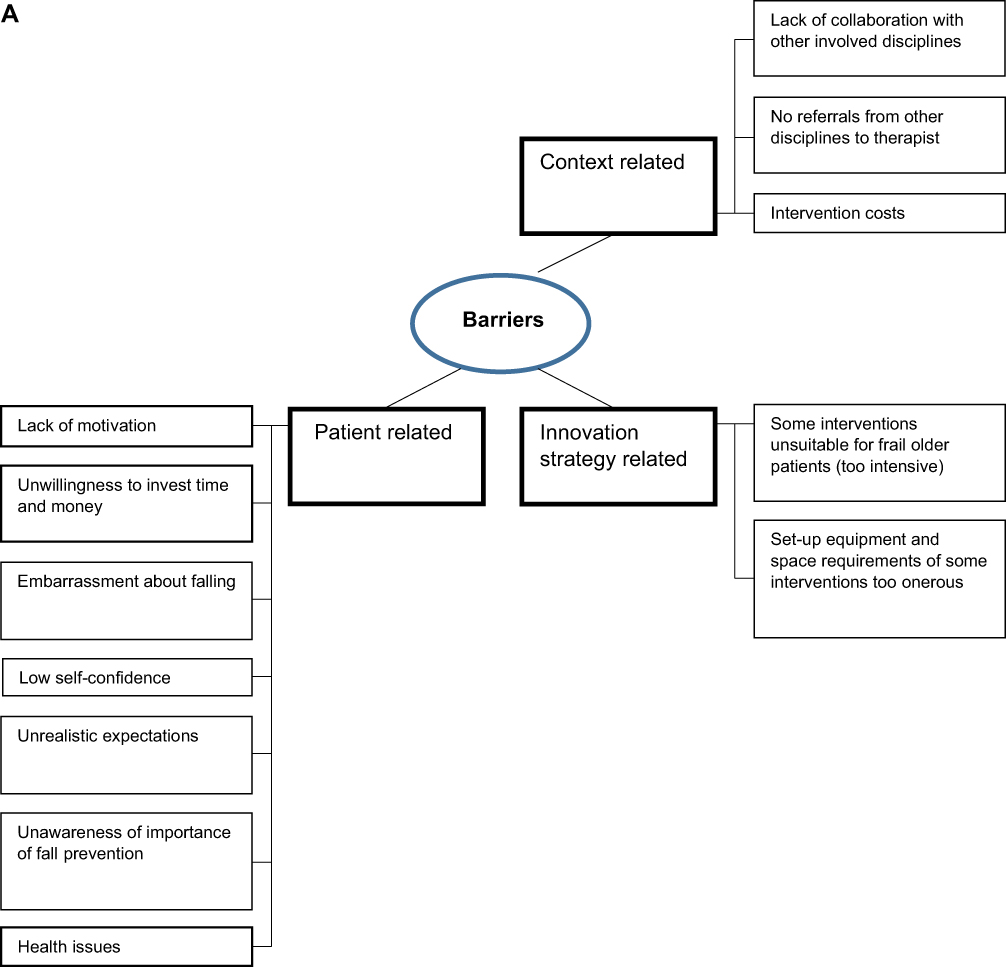
Care Provider-Related Characteristics
Knowledge and skills: The therapists explained they followed different training to be able to provide falls prevention interventions. Almost all therapists experienced it as useful.
No other care provider-related characteristics were described.
Context-Related Characteristics
The therapists described the organization and social-political context as context-related characteristics that influence their behavior when providing evidence-based falls prevention interventions.
Organization: The therapists described that good collaboration between physio- or exercise therapist, community nurse, GP practice, and other disciplines is important to provide falls prevention interventions.
The therapists highlighted that they did not receive enough referrals to provide the interventions in a group setting, as it was intended. Some therapists mentioned that the number of referrals might increase with closer communication with other care providers, sending feedback forms after receiving patients from other disciplines and with “brand awareness” of the therapist among other care providers.
Socio-political context: According to the therapists, costs are a barrier for patients to participate in falls prevention interventions. If falls prevention interventions are not reimbursed in the patient’s health insurance, patients are often unwilling to start or continue the intervention.
One therapist elaborated the need for change in behavior among patients, in relation to appreciation of prevention care and one’s health in general:
For clients, costs often play a role to drop-out prematurely. A behavioral change concerning clients/costs is needed. Clients should take responsibility to invest [financially] in and maintain their health. Clients more often have to pay themselves for health care [instead of health insurance], which, in my opinion, has a negative influence. Financial investment in maintenance of a car is generally not an issue, but for your own health it is. (Therapist 10, Physiotherapist, FG 2)
Patient-Related Characteristics
The therapists described that the patient-related characteristics, patients’ motivation and their health issues, influence the provision of falls prevention interventions.
They mentioned that motivation to start and complete falls prevention interventions varies strongly among patients. They experienced a lack of patients’ motivation as a barrier when offering falls prevention interventions. According to the therapists, patients’ motivation can be influenced by or is related to their (un)willingness to invest time and money, embarrassment about falling, experiences and self-confidence, (unrealistic) expectations, and (un)awareness.
If they see that they achieved results in 6 to 8 weeks, it is motivating for both parties [both physiotherapist as well as patient]. With good results, patients are often also more motivated to continue exercising at for example a “KBO” [senior citizens’ association]. (Therapist 4, Physiotherapist, FG 2)
It was also reported that patients’ confidence and retention rate could be improved by involving informal caregivers or family. Some therapists described that patients are often unaware of the importance of falls prevention. They believe that improving patients’ awareness and understanding about the importance of falls prevention can improve their motivation.
The therapists emphasized that patients’ poor health, comorbidities or frailty could negatively influence the provision of falls prevention interventions. They reported that most of the frail older patients did not meet the inclusion criteria (eg being able to walk without walking aid) for the evidence-based falls prevention interventions. The therapists highlighted that customized care is required for these patients.
Due to the many health issues of the patients, the therapists experienced the falls prevention interventions they provided not as prevention care but rather as treatment. They emphasized that they prefer to see patients earlier in life when they have less health issues.
A few therapists mentioned that they believe some interventions are sometimes too intensive or maybe unsuitable for frail older patients. A few therapists reported that, because of health issues and immobility, patients often prefer treatment at home, and that transport to the physio- or exercise therapy location was experienced as a barrier by patients.
Innovation-Related Characteristics
Some of the evidence-based interventions were experienced by the therapists as easy to perform in practice (eg OTAGO), while other interventions took a lot of effort to carry out (eg Nijmegen Falls Prevention Program) as they require a lot of equipment and space.
Even though the therapists tried to remain as close as possible to the original format of the intervention, they described that in many cases they had to adapt the evidence-based interventions in order to meet the patients’ needs and wishes, so customized care was provided.
Discussion
This study aimed to identify i) barriers and facilitators encountered by GPs, practice nurses and community nurses when implementing a falls risk assessment strategy, and ii) barriers and facilitators encountered by physio- and exercise therapists when providing evidence-based falls prevention interventions to independently living, frail older people.
Barriers and Facilitators Encountered by GPs and Nurses When Implementing Falls Prevention
The main barriers which GP practices and community nurses encountered when implementing the falls risk assessment strategy were care provider-related (having other priorities within the team, experiences and beliefs that falls prevention is complex and time consuming, the lack of routines of providing falls prevention in daily practice), context-related (lack of resources, lack of collaboration), and patient-related (patients’ lack of motivation and health issues). Most of the encountered barriers are also described in previous studies.33,34,62 However, we could not find any literature mentioning having no routine in providing falls prevention as a barrier.
The main facilitators were all context-related characteristics: good collaboration, support within a team, sufficient resources, and patients receiving adequate reimbursement for exercise sessions. These facilitators are in line with previous studies.62–64 Another context-related facilitator, which was not previously clearly identified, was having an adequately implemented care program for older people. Within the “Care Program for Older People” that was offered by the GP care group in this study, frailty is systematically assessed among older people aged ≥75 years. The falls risk assessment can be added to the frailty screening and/or it can be conducted during the annual visits that are part of the care program. Thereby, the threshold for the care providers, concerning which patients should be systematically approached for falls risk assessment, is lower which makes the first steps of implementing falls prevention easier and more practical because a work structure is already in place.
Furthermore, certain innovation strategy-related characteristics (the provision of tools and falls prevention training for health care providers), and care provider-related characteristics (having beliefs that falls prevention is part of their job and useful, and that they have the knowledge and skills to offer falls prevention), seemed to facilitate the implementation.
Role of the Practice Nurse in Falls Prevention
Our study also emphasizes the important role of the practice nurse in Dutch GP practices in regards to the implementation of the falls risk assessment strategy. The practice nurses conducted assessment of high falls risk, identification of underlying causes and provision of treatment (in consultation with the GP). Some highly motivated practice nurses also encouraged their colleagues to perform falls prevention tasks such as assessing patients’ high falls risk. In addition, practice nurses seem to have more time than GPs to identify underlying causes of falls risk and to provide falls prevention care. The important role of the practice nurse when providing prevention care was also seen in previous studies.65,66 Therefore, motivated practice nurses seem to be an important facilitator for the implementation of a falls risk assessment strategy in primary care practice.
Barriers and Facilitators Encountered by Therapists When Providing Falls Prevention Interventions
The physio- and exercise therapists mainly encountered innovation-related (the set-up of certain interventions) and context-related barriers and facilitators ((lack of) collaboration, (limited) reimbursement for exercise sessions) when providing falls prevention interventions. In addition, the majority of the therapists in the implementation study received no or limited referrals from GP practices or community nurses, which also relates to the importance of collaboration with other disciplines. This is an essential context-related barrier for therapists. Older people often do not realize they have a high falls risk and/or are unfamiliar with available falls prevention interventions, and therefore they need to be guided or referred by other care professionals to these interventions.24,25 The therapists were therefore unable to provide falls prevention interventions or could not provide them in the original format (group session).
Furthermore, the therapists experienced patients’ lack of motivation and health issues as important patient-related barriers when providing falls prevention interventions. The therapists would prefer to see patients earlier, when they were still less frail or had less health issues. They had to adjust the formats of the evidence-based interventions to offer customized care to compensate for patients’ health issues. The therapists experienced the provision of falls prevention interventions therefore more as falls treatment than as prevention due to the severity of patients’ health issues. It was also mentioned that certain evidence-based falls prevention interventions might be too intensive and thus unsuitable for some frail older patients suffering from serious health issues. This implies that it is important for therapists to explore which falls prevention intervention is most suitable to provide to their patient population and most practical in regards to their resources (space, equipment).
Comparison of Barriers and Facilitators Encountered by Different Disciplines
In this study, GPs and nurses described several care provider-related characteristics that positively and negatively influenced the implementation of the falls risk assessment strategy, whereas the physio- and exercise therapists only mentioned one specific care provider related characteristic. The therapists mentioned the training they followed to provide evidence-based falls prevention interventions as the only care provider-related facilitator. This is interesting as it shows that the encountered barriers and facilitators experienced by therapists are external, outside their own scope, emphasizing that therapists depend almost exclusively on other care providers’ collaboration and patients’ motivation to be able to offer falls prevention interventions.
When comparing the experienced barriers and facilitators from GPs, practice nurses, and community nurses with physio- and exercise therapists, also some similarities can be found. All care providers mentioned the importance of good collaboration, adequate reimbursements for interventions, and patients’ motivation and severity of health issues to enhance implementation and provision of falls prevention. These factors have also been previously described in other care settings.33,34,62,64 As these barriers and facilitators occur among different disciplines and in different care settings, they appear to be quite essential to focus on in future research and when implementing falls prevention.
Strengths and Limitations
This study is, to the authors’ knowledge, the first study to explore barriers and facilitators in the entire process from assessment of high falls risk by GPs and nurses to providing falls prevention interventions by therapists. As provision of falls prevention involves different disciplines, therefore gaining insights from different perspectives at different stages of the care process adds valuable knowledge.
A limitation of our study is that we may not have reached data saturation. Not all care providers who participated in the implementation study also participated in the focus groups. All care providers were invited to participate in the online FGs. Care providers who experience certain barriers and who had less time for the implementation of falls prevention might also have been less able or willing to participate in the online FGs. Therefore, we might have missed important barriers and facilitators experienced by these care providers. However, by enriching the online FGs with data from the researcher’s diary, containing notes from unstructured interviews conducted with all participating GP practices and community nurses, we hope to approximate data saturation as closely as possible, within the boundaries of this study.
Another limitation is that we did not include the patient’s perspective. Our results show that the patient, more specifically the patient’s motivation and health issues, are important factors for successful provision of falls prevention according to the health care providers. Not also taking the patient’s perspective into account, limits the conclusions and recommendations of this study. Even so, the perspective of the health care providers remains most important in this study as the purpose of this study was to identify barriers and facilitators encountered by the care providers when implementing and providing falls prevention.
The strength of our study is that the gathered data represent barriers and facilitators from a real-life setting. In a controlled setting, certain barriers and facilitators will not occur and/or be identified.
Recommendations for Daily Practice
From our study, important recommendations for daily practice in primary care can be derived. Before starting implementation, care providers and management should anticipate certain barriers (for example, changing priorities due to practice take-over, practice split, and reorganization) and discuss an adequate work structure within the team. As described above, some care practices already had a special care program for frail older people in place in which patients are seen systematically at least twice a year. These systematic visits appeared to help to take the first steps in assessing patients. Although every GP practice and community nursing team works slightly different, a structured protocol or existing work-routine, in which older people are systematically seen twice a year, could enhance implementation of falls prevention.
Previous studies described a lack of knowledge and skills among care professionals regarding the provision of falls prevention.34,62 From our findings it appears that the tools (a suitable assessment instrument, a checklist to diagnose underlying causes, an overview of physio and exercise therapists who offer evidence-based falls prevention interventions in the area) as well as a free of charge accredited training provided for nurses, may have contributed to the participants acknowledging they have the skills and knowledge to provide falls prevention care. Therefore, these tools and training (see Meekes et al37) can be helpful once GPs, practice nurses and community nurses have decided to implement falls prevention in their daily care practice.
Furthermore, the therapists in our study emphasized to prefer to see patients when they are less or not yet frail. This indicates that an adapted systematic and targeted falls risk assessment strategy should preferably focus also on younger and healthier older people and not only on frail older people. These younger and healthier patients need to be made aware of the importance of falls prevention and offered the possibility to take part in falls prevention interventions.
Further Research
One of the main barriers to the successful implementation of falls risk prevention identified by care professionals in our study is the complexity of assessing, diagnosing and treating high falls risk adequately, as it differs for each patient, in combination with lack of time as experienced by GPs and nurses. Even though the practice nurses in our study seem to have more time available than GPs to provide falls prevention care, they still experienced a lack of time to adequately provide falls prevention care. Dierick-van Daele et al emphasized in their study the increasing involvement of specially trained practice nurses in primary care.65 Further research could in this respect investigate the role of practice nurses, for instance by studying the impact of practice nurses with a specialized task in prevention care at GP practices on the provision of falls prevention.
It is also clear from the care providers’ perspective that patients play an important role for successfully providing falls prevention care. Motivating patients to participate in falls prevention interventions has been previously investigated.67 Still, being able to motivate patients as a care provider is experienced as difficult. For example, motivational interviewing has been previously developed to help care providers to enhance patients’ motivation.68,69 However, the effect of motivational interviewing is not conclusive.70 Therefore, further research might be conducted to investigate how care providers can motivate their patients better to participate in and complete falls prevention interventions.
Conclusion
In conclusion, this study identified care provider-, context-, patient-, and innovation (strategy)-related barriers and facilitators when implementing falls prevention at GP practices and community nursing teams, and when providing evidence-based falls prevention interventions by physio- or exercise therapists. These insights offer the opportunity to develop a more successful implementation strategy for primary care daily practice in a real-life setting. Such an implementation strategy, for instance, should focus on intensifying collaboration between care providers, reimbursement for interventions, availability of resources (eg time, personnel), and patients’ lack of motivation, and health issues. By taking these barriers and facilitators into account when developing an implementation strategy, falls prevention may become more widely and structurally applied, thereby contributing to the reduction of a major threat for the quality of life of independently living older people.
Acknowledgment
We would like to thank Zorggroep PrimaCura; Thebe Wijkverpleging; and all participating GPs, practice nurses, district nurses, physio- and exercise therapists, and patients for their support and participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by ZonMw, the Netherlands Organization for Health Research and Development, grant number [531001210] (see https://www.zonmw.nl/nl/over-zonmw/ehealth-en-ict-in-de-zorg/programmas/project-detail/preventie-5-deelprogramma-4-preventie-in-de-zorg/valpreventie-in-de-zorg-geimplementeerd). The funder had no role in the creation of the research question, design of the study, data collection, analysis, interpretation, or the writing of this manuscript.
Disclosure
The authors report no conflicts of interests in this work.
References
1. World Health Organization. Falls, Fact sheet; 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/falls.
2. Deandrea S, Lucenteforte E, Bravi F, et al. Risk factors for falls in community-dwelling older people: “a systematic review and meta-analysis”. Epidemiology. 2010;21(5):658–668. doi:10.1097/EDE.0b013e3181e89905
3. Gosney M, Harper A, Conroy S. Oxford Desk Reference: Geriatric Medicine. Oxford university press; 2012.
4. Tinetti ME. Where is the vision for fall prevention? J Am Geriatr Soc. 2001;49(5):676–677. doi:10.1046/j.1532-5415.2001.49132.x
5. Tinetti ME, Speechley M. Prevention of falls among the elderly. N Engl J Med. 1989;320(16):1055–1059. doi:10.1056/NEJM198904203201606
6. World Health Organization. Falls: fact sheet; 2018: 25.
7. World Health Organization. Fact sheet, Falls; 2021 Available from: https://www.who.int/news-room/fact-sheets/detail/falls#:~:text=Each%20year%20an%20estimated%20646,medical%20attention%20occur%20each%20year.
8. Van der Does H, Baan A, Panneman M Privé-ongevallen bij ouderen, Cijfers valongevallen in de privésfeer 2018 [Private accidents among older people, Figures on private falls in 2018: veiligheidNL; 2019.
9. Cheng MH, Chang SF. Frailty as a risk factor for falls among community dwelling people: evidence from a meta‐analysis. J Nurs Scholarsh. 2017;49(5):529–536. doi:10.1111/jnu.12322
10. Clegg A, Young J, Iliffe S, et al. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
11. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–M57. doi:10.1093/gerona/56.3.M146
12. Walston J, Hadley EC, Ferrucci L, et al. Research agenda for frailty in older adults: toward a better understanding of physiology and etiology: summary from the American Geriatrics Society/National Institute on aging research conference on frailty in older adults. J Am Geriatr Soc. 2006;54(6):991–1001. doi:10.1111/j.1532-5415.2006.00745.x
13. Eeles EM, White SV, O’Mahony SM, et al. The impact of frailty and delirium on mortality in older inpatients. Age Ageing. 2012;41(3):412–416. doi:10.1093/ageing/afs021
14. Boelens C, Hekman EE, Verkerke GJ. Risk factors for falls of older citizens. Technol Health Care. 2013;21(5):521–533. doi:10.3233/THC-130748
15. Pfortmueller C, Lindner G, Exadaktylos A. Reducing fall risk in the elderly: risk factors and fall prevention, a systematic review. Minerva Med. 2014;105(4):275–281.
16. Bandeen-Roche K, Seplaki CL, Huang J, et al. Frailty in older adults: a nationally representative profile in the United States. J Gerontol A. 2015;70(11):1427–1434. doi:10.1093/gerona/glv133
17. Terroso M, Rosa N, Marques AT, et al. Physical consequences of falls in the elderly: a literature review from 1995 to 2010. Eur Rev Aging Phys Act. 2014;11(1):51–59. doi:10.1007/s11556-013-0134-8
18. Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2012;(9). doi:10.1002/14651858.CD007146.pub3
19. Balzer K, Bremer M, Schramm S, et al. Falls prevention for the elderly. GMS Health Technol Assess. 2012;8:Doc01. doi:10.3205/hta000099
20. Tricco AC, Thomas SM, Veroniki AA, et al. Comparisons of interventions for preventing falls in older adults: a systematic review and meta-analysis. JAMA. 2017;318(17):1687–1699. doi:10.1001/jama.2017.15006
21. Sherrington C, Michaleff ZA, Fairhall N, et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med. 2017;51(24):1750–1758. doi:10.1136/bjsports-2016-096547
22. Luk JKH, Chan TY, Chan DKY. Falls prevention in the elderly: translating evidence into practice. Hong Kong Med J. 2015;21(2):165–171. doi:10.12809/hkmj144469
23. Grossman DC, Curry SJ, Owens DK; Force UPST. Interventions to prevent falls in community-dwelling older adults: US preventive services task force recommendation statement. JAMA. 2018;319(16):1696–1704. doi:10.1001/jama.2018.3097
24. Shankar KN, Taylor D, Rizzo CT, et al. Exploring older adult ED fall patients’ understanding of their fall: a qualitative study. Geriatr Orthop Surg Rehabil. 2017;8(4):231–237. doi:10.1177/2151458517738440
25. Yardley L, Donovan-Hall M, Francis K, et al. Older people’s views of advice about falls prevention: a qualitative study. Health Educ Res. 2006;21(4):508–517. doi:10.1093/her/cyh077
26. Olij BF, Erasmus V, Kuiper JI, et al. Falls prevention activities among community-dwelling elderly in the Netherlands: a Delphi study. Injury. 2017;48(9):2017–2021. doi:10.1016/j.injury.2017.06.022
27. Schoon Y. Vallen, een systematische benadering bij het zoeken naar de oorzaak. Bijblijven. 2013;29(6):12–18. doi:10.1007/s12414-013-0057-3
28. Stel VS, Smit JH, Pluijm SM, et al. Consequences of falling in older men and women and risk factors for health service use and functional decline. Age Ageing. 2004;33(1):58–65. doi:10.1093/ageing/afh028
29. Mackenzie L, McIntyre A. How do general practitioners (GPs) engage in falls prevention with older people? A pilot survey of GPs in NHS England suggests a gap in routine practice to address falls prevention. Front Public Health. 2019;7. doi:10.3389/fpubh.2019.00032
30. Mueller CA, Klaaßen-Mielke R, Penner E, et al. Disclosure of new health problems and intervention planning using a geriatric assessment in a primary care setting. Croat Med J. 2010;51(6):493–500. doi:10.3325/cmj.2010.51.493
31. Vetter N, Lewis P. Reasons for poor detection of frequent falls in elderly people by general practitioners. Aging Clin Exp Res. 1995;7(6):430–432. doi:10.1007/BF03324357
32. Paul S. Falls: prevention and Management. In: Geriatric Medicine. 2018:109–119.
33. Child S, Goodwin V, Garside R, et al. Factors influencing the implementation of fall-prevention programmes: a systematic review and synthesis of qualitative studies. Implement Sci. 2012;7:7. doi:10.1186/1748-5908-7-91
34. McConville A, Hooven K. Factors influencing the implementation of falls prevention practice in primary care. J Am Assoc Nurse Pract. 2021;33(2):108–116. doi:10.1097/JXX.0000000000000360
35. Walsh K, Ford K, Morley C, et al. The development and implementation of a participatory and solution-focused framework for clinical research: a case example. Collegian. 2017;24(4):331–338. doi:10.1016/j.colegn.2016.06.003
36. Bloor R, Pearson D. Brief solution-focused organizational redesign: a model for international mental health consultancy. Int J Ment Health. 2004;33(2):44–53. doi:10.1080/00207411.2004.11043368
37. Meekes W, Leemrijse C, Korevaar J, et al. Implementation and evaluation of a fall risk screening strategy among frail older adults for the primary care setting: a study protocol. Clin Interv Aging. 2020;15:1625. doi:10.2147/CIA.S254864
38. VeiligheidNL V. Valanalyse, screeningtool valrisico voor de eerstelijnszorg: VeiligheidNL; 2015 [Fall analysis, fall risk screening tool for primary care: VeiligheidNL, 2015].
39. World Health Organization ALCU. WHO global report on falls prevention in older age: World Health Organization; 2008.
40. Federatie Medisch Specialisten. Richtlijn, Preventie van valincidenten bij ouderen; 2017 [Guideline, prevention of falls among older people, 2017.].
41. VeiligheidNL. Basiscursus valpreventie voor professionals; 2019 [Basic fall prevention course for professionals 2019]. Available from: https://www.veiligheid.nl/valpreventie/trainingen/basiscursus-valpreventie-voor-professionals.
42. The role of informal conversations in generating data, and the ethical and methodological issues. Forum Qualitative Sozialforschung/Forum: Qualitative Social Research; 2020.
43. Sanchez C. Unstructured Interviews. In: Michalos AC, editor. Encyclopedia of Quality of Life and Well-Being Research. Dordrecht: Springer Netherlands; 2014:6824–6825.
44. Zorggroep RCH T Zorgprogramma kwetsbare ouderen, Mogelijk gemaakt door de samenwerking tussen Zorggroep RCH Midden-Brabant en Thebe; 2015 [Care program for frail older people, made possible by the collaboration between Zorggroep RCH Midden-Brabant and Thebe].
45. Warnier R. TraZAG: Transmuraal zorg assessment Geriatrie Maastricht [Transmural care assessment Geriatrics Maastricht]. Tijdschr Gezondh Ethiek. 2012;22(3):93.
46. Gobbens RJ, Van assen MA, Luijkx KG, et al. The Tilburg frailty indicator: psychometric properties. J Am Med Dir Assoc. 2010;11(5):344–355. doi:10.1016/j.jamda.2009.11.003
47. Zijlstra GAR, van Haastregt JCM, Du Moulin MF, et al. Effects of the implementation of an evidence-based program to manage concerns about falls in older adults. Gerontologist. 2013;53(5):839–849. doi:10.1093/geront/gns142
48. Zijlstra GAR, van Haastregt JCM, Kempen GIJM. ‘Zicht op Evenwicht’: een effectieve interventie om bezorgdheid om te vallen en gerelateerd vermijdingsgedrag bij ouderen te verminderen. Tijdschr Gerontol Geriatr. 2012;43(4):164–174. doi:10.1007/s12439-012-0026-9
49. Faber MJ, Bosscher RJ, Chin A, et al. Effects of exercise programs on falls and mobility in frail and pre-frail older adults: a multicenter randomized controlled trial. Arch Phys Med Rehabil. 2006;87(7):885–896. doi:10.1016/j.apmr.2006.04.005
50. Weerdesteyn V, Rijken H, Geurts ACH, et al. A five-week exercise program can reduce falls and improve obstacle avoidance in the elderly. Gerontology. 2006;52(3):131–141. doi:10.1159/000091822
51. Campbell AJ, Robertson MC, Gardner MM, et al. Falls prevention over 2 years: a randomized controlled trial in women 80 years and older. Age Ageing. 1999;28(6):513–518. doi:10.1093/ageing/28.6.513
52. Campbell AJ, Robertson MC, Gardner MM, et al. Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women. BMJ. 1997;315(7115):1065–1069. doi:10.1136/bmj.315.7115.1065
53. Robertson MC, Devlin N, Gardner MM, et al. Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls. 1: randomised controlled trial. BMJ. 2001;322(7288):697–701. doi:10.1136/bmj.322.7288.697
54. Robertson MC, Gardner MM, Devlin N, et al. Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls. 2: controlled trial in multiple centres. BMJ. 2001;322(7288):701–704. doi:10.1136/bmj.322.7288.701
55. Loketgezondleven. Interventieszoeken[Search interventions]; 2019.
56. MOVISIE N, NISB, NJi, RIVM Dutch recognition system for interventions. Criteria for joint quality assessment 2013–2018; 2013.
57. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
58. Huijg JM, Gebhardt WA, Dusseldorp E, et al. Measuring determinants of implementation behavior: psychometric properties of a questionnaire based on the theoretical domains framework. Implement Sci. 2014;9(1):33. doi:10.1186/1748-5908-9-33
59. ATLAS.ti Scientific Software Development GmbH [ATLAS.ti version 8 Windows]. (2019). Retrieved from https://atlasti.com.
60. Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
61. van Staa A, de Vries K. Directed content analysis: een meer deductieve dan inductieve aanpak bij kwalitatieve analyse. Kwalon. 2014;19(3). doi:10.5117/2014.019.003.046
62. Vlaeyen E, Stas J, Leysens G, et al. Implementation of fall prevention in residential care facilities: a systematic review of barriers and facilitators. Int J Nurs Stud. 2017;70:110–121. doi:10.1016/j.ijnurstu.2017.02.002
63. Casey CM, Parker EM, Winkler G, et al. Lessons learned from implementing CDC’s STEADI falls prevention algorithm in primary care. Gerontologist. 2017;57(4):787–796. doi:10.1093/geront/gnw074
64. Abrahamson KA, Fox RL, Doebbeling BN. Facilitators and barriers to clinical practice guideline use among nurses. Am J Nurs. 2012;112(7):26–35. doi:10.1097/01.NAJ.0000415957.46932.bf
65. Dierick‐van Daele AT, Metsemakers JF, Derckx EW, et al. Nurse practitioners substituting for general practitioners: randomized controlled trial. J Adv Nurs. 2009;65(2):391–401. doi:10.1111/j.1365-2648.2008.04888.x
66. Helmink JH, Meis JJ, de Weerdt I, et al. Development and implementation of a lifestyle intervention to promote physical activity and healthy diet in the Dutch general practice setting: the BeweegKuur programme. Int J Behav Nutr Phys Act. 2010;7(1):1–10. doi:10.1186/1479-5868-7-49
67. Finnegan S, Bruce J, Seers K. What enables older people to continue with their falls prevention exercises? A qualitative systematic review. BMJ open. 2019;9(4):e026074.
68. Arkkukangas M, Söderlund A, Eriksson S, et al. One-year adherence to the Otago exercise program with or without motivational interviewing in community-dwelling older adults. J Aging Phys Act. 2018;26(3):390–395. doi:10.1123/japa.2017-0009
69 Kiyoshi-Teo H, Northup-Snyder K, Cohen DJ, et al. Feasibility of motivational interviewing to engage older inpatients in fall prevention: a pilot randomized controlled trial. J Gerontol Nurs. 2019;45(9):19–29. doi:10.3928/00989134-20190813-03
70. Frost H, Campbell P, Maxwell M, et al. Effectiveness of motivational interviewing on adult behaviour change in health and social care settings: a systematic review of reviews. PLoS One. 2018;13(10):e0204890.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.