Back to Journals » Advances in Medical Education and Practice » Volume 16
Implementing a Near-Peer Mentorship Program to Enhance Surgical Research Among Medical Students: A Protocol for a Mixed-Methods Evaluation
Authors Pitua I ![]() , Nandera KV, Atukunda RA, Raizudheen R, Lwembawo KD
, Nandera KV, Atukunda RA, Raizudheen R, Lwembawo KD ![]() , Muyanja MF, Nampiinga MG
, Muyanja MF, Nampiinga MG ![]() , Abidha M, Otto KA
, Abidha M, Otto KA ![]() , Kamugisha D, Noori M, Kasagga B
, Kamugisha D, Noori M, Kasagga B ![]() , Bongomin F
, Bongomin F ![]() , Akello VV
, Akello VV
Received 9 May 2025
Accepted for publication 10 September 2025
Published 12 September 2025 Volume 2025:16 Pages 1665—1673
DOI https://doi.org/10.2147/AMEP.S539338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Ivaan Pitua,1 Ketra Venesa Nandera,1 Ronaldine Anne Atukunda,1 Raafidha Raizudheen,1 Kiragga Denis Lwembawo,1 Mark Fedrick Muyanja,1 Maria Gabriella Nampiinga,1 Musfira Abidha,1 Kim Andrew Otto,1 Dickens Kamugisha,1 Misba Noori,1 Brian Kasagga,2,3 Felix Bongomin,4 Vivian Valin Akello2,3
1School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda; 2Department of Surgery, School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda; 3Department of Surgery, Mulago National Referral Hospital, Kampala, Uganda; 4Faculty of Medicine, Gulu University, Gulu, Uganda
Correspondence: Ivaan Pitua, School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda, Email [email protected]
Background: Research is vital in medical education, fostering evidence-based practice and professional growth. However, medical students in low- and middle-income countries, such as Uganda, face significant barriers to research participation, including limited mentorship and resources. At Makerere University, these challenges impede surgical research output among students. Near-peer mentorship programs (NPMPs) offer a promising solution by leveraging senior students and residents to guide peers, enhancing research skills and productivity. This study implements and evaluates an NPMP within the Makerere University Surgery Society (MUSS) to boost student-led surgical research.
Methods: A mixed-methods implementation research design, guided by the RE-AIM Framework, will assess the NPMP over 12 months at Makerere University College of Health Sciences. The program involves 120 participants: 15 surgical residents mentoring 30 senior students (Years 3– 5), who mentor 75 junior students (Years 1– 5). Convenience and purposive sampling will recruit participants. Quantitative data (surveys, logs) will measure reach, effectiveness (research output, competency), adoption, implementation, and maintenance. Qualitative interviews with 25 participants will explore feasibility, acceptability, and sustainability. Data analysis includes descriptive/inferential statistics and thematic analysis. This protocol has been approved by the Mulago Hospital Research and Ethics Committee (Protocol Approval Number MHREC 2931).
Discussion: The NPMP aims to increase surgical research output, improve skills, and establish a sustainable mentorship culture within MUSS. By addressing mentorship gaps, it could enhance student engagement and offer a scalable model for resource-limited settings. Limitations include the lack of a control group and potential selection bias. This implementation research aims to establish a scalable model rather than prove direct causality in this initial phase.
Plain Language Summary: This study will introduce a near-peer mentorship program at Makerere University to address the lack of research opportunities for medical students in Uganda. Residents will mentor senior students who will in turn mentor junior students in surgical research, with the goal of improving research skills and increasing research output mainly through the writing of case reports. Over 12 months, investigators will evaluate the program’s output, feasibility, how well it is liked by participants, and its potential for long-term use, using surveys and interviews to gather information. Ultimately, this project seeks to create a sustainable mentorship model that can be used in similar settings to boost student research and contribute to better healthcare.
Keywords: near-peer mentorship, surgical research, medical students, Makerere University, RE-AIM framework
Introduction
Research is integral to medical education, equipping students with skills for evidence-based practice, academic advancement, and professional growth.1 Early research engagement enhances strong grounding in research methodology, critical appraisal, and statistical analysis as well as competitiveness for various programs.1,2 Globally, medical students face barriers to research participation, including limited mentorship and inadequate resources, but these challenges are amplified in low- and middle-income countries (LMICs).3,4 At Makerere University, a premier medical training institution in East Africa, students doing surgical research encounter systemic obstacles that hinder their ability to contribute to scientific knowledge. Most of them citing that lack of protected research time, difficulty in finding research topics, and inadequate mentorship are the main challenges to conducting research projects.5
Surgical research, particularly through case reports, provides an accessible entry point for medical students. Case reports require fewer resources than large-scale studies, allowing students to analyze clinical scenarios and develop scholarly skills.6 However, producing publishable work demands guidance, which is often lacking. At Makerere University, a survey revealed that mentors required training in mentorship skills, along with logistical and financial support, to effectively carry out their roles. Junior scientists and students reported that mentorship was not yet institutionalized and was instead occurring informally. Additionally, there was limited awareness of the specific responsibilities of mentors and mentees.7
Near-peer mentoring has emerged as an effective alternative to traditional faculty-student mentorship, particularly in medical education. This model, where senior students or residents guide their peers, capitalizes on relatable role models to enhance learning.8 Solomon and colleagues found that Years with Near Peer Mentorship Program (NPMP) led to a 122% (55 in 2019 vs 122 in 2020) and 232% (50 in 2021 vs 166 in 2022) increase in medical student conference posters compared to the previous year without NPMP.8 A similar model also reported that the number of peer-reviewed PubMed publications increased after their intervention (47.8%, in year-1; 167.4% in year-2).9 Grounded in Social Learning Theory, near-peer mentoring facilitates skill acquisition through observation and modeling, making it accessible and engaging.10 More so, Dhairya and colleagues concluded that a “Resident managed peer-mentoring program” was a productive method that proved especially beneficial for students, residents, and early career physicians in our clinically focused training program.9 Our NPMP’s tiered structure-integrating senior students and residents-builds on this evidence to create a practical, student-led framework at Makerere University. Near-peer mentoring’s feasibility lies in its low resource demands, leveraging existing student and resident capacity rather than relying on overburdened faculty. Its acceptability is enhanced by peers’ relatability, which increases student satisfaction and engagement.8–10
Uganda’s medical education context highlights the urgency of this intervention. With a strained healthcare system and limited research funding, students are underrepresented in research. A study across 12 universities in Uganda reported that despite a high proportion of HPS showing interest in getting involved in research, less than one-third reported previous involvement.11 The NPMP aims to shift this narrative by establishing a mentorship program that is feasible within existing constraints and acceptable to students, potentially increasing surgical research output. Its impact could extend beyond publications, enhancing skills critical for evidence-based practice and professional development.
By implementing this program, Makerere University can contribute to local healthcare solutions while offering a model for other institutions. The study’s focus on sustainability ensures long-term benefits, embedding a research culture within MUSS that could endure beyond the initial intervention. This implementation research thus holds promise for transforming student engagement in surgical research, with implications for medical education in resource-limited settings worldwide.
Conceptual Framework
This conceptual framework posits that the NPMP’s implementation within MUSS harnesses a tiered mentorship system, residents mentoring senior students (Years 3–5), who mentor junior students (Years 1–5) using MakCHS’s resources and MUSS’s structure. Inputs include residents as expert mentors, senior students as intermediaries, and junior students as learners, supported by training and constrained by logistics. The mentorship process integrates Social Learning Theory (SLT) and the Cognitive Apprenticeship Model (CAM): residents model advanced skills to seniors, who guide juniors through practice, reinforced by feedback and faded as independence grows. This tiered cascade, operationalized via workshops and meetings, aims to enhance surgical research skills across all levels. The RE-AIM Framework evaluates outcomes: Reach tracks participation across tiers; Effectiveness measures research output and competency gains; Adoption assesses tier-specific acceptability; Implementation tests feasibility of the tiered delivery; and Maintenance explores its sustainability within MUSS. Activities will be coordinated by MUSS, with fidelity tracked via biweekly checklists (eg, attendance, tasks completed) that will also log mentor-mentee contact frequency and topics discussed to assess engagement and adherence to the structured approach. Quality of interactions will be gauged through participant feedback during regular feedback sessions facilitated by MUSS coordinators, ensuring adaptability to participant needs and addressing any logistical challenges promptly. Feedback loops refine the system, hypothesizing that a well-implemented tiered NPMP will boost student-led surgical research, prove feasible and acceptable, and establish a lasting mentorship culture Figure 1.
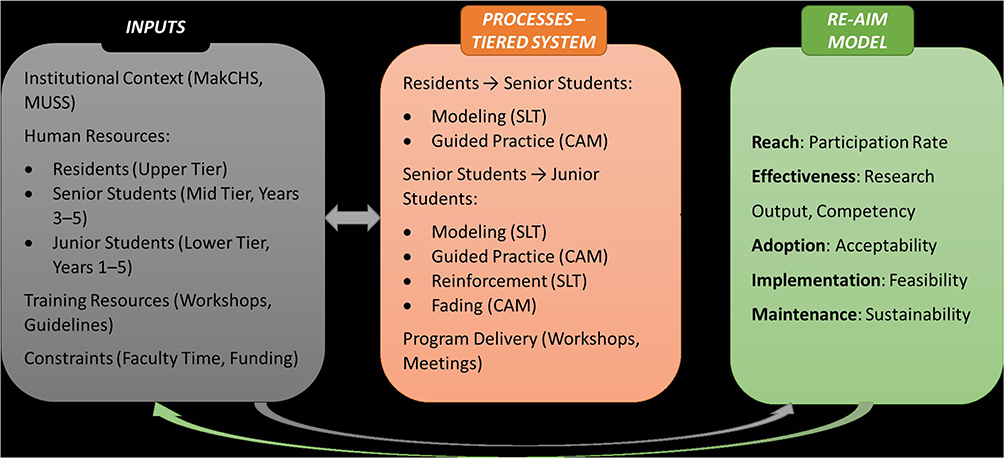 |
Figure 1 Conceptual Framework of the Near-Peer Mentorship Program. |
Methods and Materials
Objectives
The main objective of our study is to implement an NPMP through the MUSS to enhance student-led surgical research. Specific objectives are:
- To evaluate the feasibility and acceptability of the NPMP among medical students at Makerere University.
- To assess the impact of the NPMP on students’ surgical research output and skills.
- To explore the sustainability of the NPMP within the MUSS.
Study Design
This study will employ a mixed-methods implementation research design, guided by the RE-AIM Framework, to assess the NPMP’s rollout and impact within MUSS. A prospective cohort approach will track implementation over 12 months. This protocol adheres to the Template for Intervention Description and Replication (TIDieR) guidance.12 Filled copies of the checklist is attached as a Supplementary File.
Study Location
The NPMP will be implemented at MakCHS, located in Kampala, Uganda. MakCHS, a leading medical training institution in East Africa affiliated with Mulago National Referral Hospital, providing a rich clinical environment for surgical research. The study will leverage MUSS, an established student organization within MakCHS, as the implementation platform.
Study Population
The study population comprises medical students enrolled at MakCHS in Years 1–5, with a focus on those interested in surgical research. MakCHS has approximately 1500 medical students across all years including residency years, making the target sample size of 120 participants feasible within this larger population. This includes preclinical (Years 1–2) and clinical (Years 3–5) students, reflecting the NPMP’s tiered structure: junior mentees (Years 1–5) and senior mentors (Years 3–5 who have completed surgery rotation or with prior research experience). Surgical residents from Mulago Hospital, affiliated with MakCHS, will serve as upper-tier mentors to guide senior students.
Selection Criteria
The study will include medical students in Years 1–5 at Makerere University College of Health Sciences (MakCHS) who are willing to participate in the Near-Peer Mentorship Program (NPMP) for 12 months, regardless of prior research experience, and surgical residents from Mulago Hospital interested in mentoring and available for monthly sessions, all committed to attending at least 80% of scheduled activities like seminars and meetings. Excluded will be students unable to participate for the full duration due to academic or personal conflicts (eg, final exams and relocation), and residents unavailable due to clinical rotations or other obligations. Those with prior experience in similar structured research mentorship programs at MakCHS or elsewhere will be excluded to better assess the specific impact of the proposed NPMP without confounding from previous structured mentorship experiences.
Sample Size and Sampling Technique
A total of 120 participants will be recruited for the study, structured according to the mentorship model at the Makerere University Surgery Society (MUSS), comprising 15 residents as upper-tier mentors, 30 senior medical students (Years 3–5) with each resident mentoring 2 seniors, and 75 junior medical students (Years 1–5) with each resident’s senior pair mentoring 5 juniors on the same clinical case. This sample size, calculated using G*Power 3.1 to detect a 25% increase in research output (from 10% to 35%) with 80% power and α = 0.05, will start at 98 participants but increase to 120 to account for a 20% dropout buffer due to academic workload and fatigue, a standard in educational research. The 10% baseline rate for research output is an estimated current output among medical students at Makerere University, reflecting the existing challenges in research participation due to limited mentorship and resources. Research output will be the gains in case report production and research skills, measured by the number of case reports produced, submitted, and published and a survey. For the qualitative component, 25 participants-5 residents, 10 senior students, and 10 junior students-will be purposively selected to capture diverse mentorship experiences. Convenience sampling will recruit MUSS and non-MUSS members through announcements (emails, flyers, and WhatsApp) with a shared link for form submission, prioritizing accessibility and interest, while senior mentors will be purposively chosen from this pool based on prior research experience (eg, publications) or completion of a surgery rotation, and junior mentees will be enrolled on a first-come, first-served basis with balanced year-level representation, with non-qualifying senior applicants filling junior mentor roles after consent. Residents will be recruited via the Department of Surgery, targeting those interested in teaching, using snowball sampling to meet the target number.
Study Procedure
The study will follow a structured timeline over 12 months, divided into pre-intervention, implementation, and post-intervention phases to evaluate the impact of the NPMP.
Pre-Intervention Survey
At baseline (Month 0), all 120 recruited participants – 15 residents, 30 senior medical students (Years 3–5), and 75 junior medical students (Years 1–5) – will complete a pre-intervention survey. This survey, administered via paper or Google Forms, will use the validated Research Self-Efficacy Scale to assess baseline research competency (eg, methodology, critical appraisal) and include Likert-scale items to gauge initial perceptions of mentorship and surgical research interest. While this scale has not been specifically validated in the Ugandan context, it is a widely recognized and utilized instrument for assessing research competency. Demographic data (eg, year and gender) and prior research experience will also be collected. The survey will take approximately 20–30 minutes, with responses stored securely in an Excel spreadsheet for analysis.
Implementation Strategy
From Months 1 to 12, the NPMP will be rolled out in a tiered structure. Residents will attend an initial 2-day training seminar on mentorship and case report writing, led by experienced facilitators, followed by monthly 2-hour meetings to guide 2 senior students each. Senior students, trained concurrently in research skills (eg, literature review, data analysis), will mentor 5 junior students per pair through biweekly 1-hour workshops and case report projects based on clinical cases from Mulago Hospital. Activities will be coordinated by MUSS, with fidelity tracked via biweekly checklists (eg, attendance and tasks completed) that will also log mentor-mentee contact frequency and topics discussed to assess engagement and adherence to the structured approach. Quality of interactions will be gauged through participant feedback during regular feedback sessions facilitated by MUSS coordinators, ensuring adaptability to participant needs and addressing any logistical challenges promptly. Feedback sessions will refine the process, ensuring adaptability to participant needs.
Post-Intervention Survey
At Month 12, all participants will complete a post-intervention survey mirroring the pre-intervention tool, assessing changes in research competency, mentorship satisfaction (Likert items), and perceived NPMP impact. Additional open-ended questions will explore experiences and challenges. Case report outputs (completed, submitted, published) will be logged by coordinators. The survey, taking 20–30 minutes, will be followed by semi-structured interviews with 25 purposively selected participants (5 residents, 10 seniors, 10 juniors) to probe feasibility, acceptability, and sustainability. These interviews are anticipated to last approximately 30–45 minutes each and will be recorded and transcribed for qualitative analysis recorded and transcribed for qualitative analysis.
Study Outcomes
The primary outcomes (feasibility and acceptability) and secondary outcomes (effectiveness, adoption, and sustainability) will stem from the RE-AIM Framework, with measurement specifics detailed in Table 1.
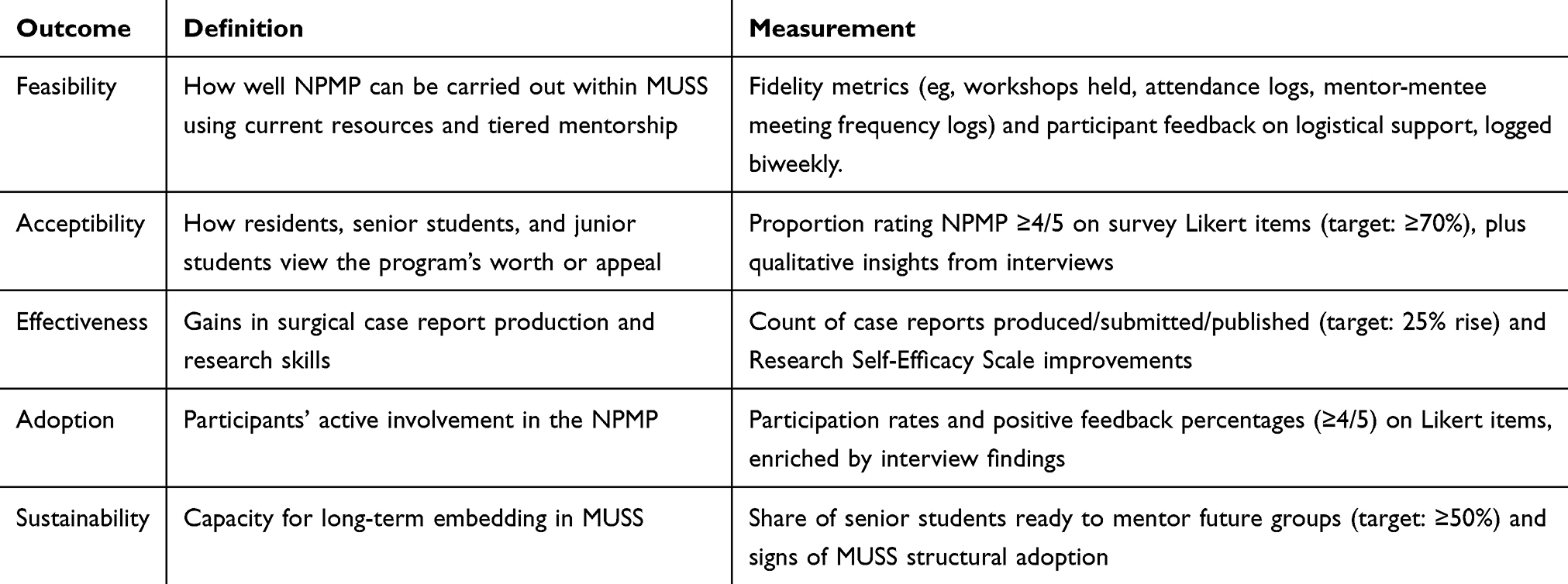 |
Table 1 Study Outcomes and Measurements |
Data Management and Analysis
Quantitative data will be collected from recruitment logs (Reach), pre- and post-intervention surveys (Effectiveness, Adoption), and implementation checklists/logs (Implementation) to assess the NPMP’s impact on research output, competency, and feasibility. Data will be entered into a secure Excel spreadsheet, cleaned for missing values and inconsistencies, and exported to R for analysis. Missing data (<10%) will be addressed with multiple imputation if random, or list-wise deletion if not. Descriptive statistics will include Reach as the proportion of enrolled participants relative to eligible students, stratified by year and gender with 95% CIs; Effectiveness as case report outputs and competency scores summarized with means, SDs, medians, and IQRs; Adoption as the percentage rating NPMP ≥4/5 on Likert scales with subgroup analysis by role; and Implementation as fidelity metrics (eg, workshops held) with means, SDs, and dropout rates. Inferential statistics will involve paired t-tests (or Wilcoxon signed-rank tests for non-normal data) to compare pre/post competency scores with Cohen’s d effect sizes, chi-square tests to evaluate a 25% increase in publication rates, one-sample proportion tests to benchmark acceptability (≥70%) with logistic regression for predictors, and one-way ANOVA (or Kruskal–Wallis) to compare fidelity across mentor groups.
Qualitative data will stem from semi-structured interviews with 25 participants (5 residents, 10 seniors, 10 juniors), focusing on Adoption (acceptability), Implementation (feasibility), and Maintenance (sustainability), with English transcriptions analyzed in NVivo v.12. Using Braun & Clarke’s six-phase thematic analysis, we will conduct a reflexive thematic analysis, where two researchers will independently familiarize themselves with the data, generate initial codes, search for themes, review themes, define and name themes. Discrepancies during the coding process will be resolved via consensus meetings, aiming to enhance the rigor of interpretation and achieve inter-rater discussion leading to conceptual agreement. While an inter-rater reliability statistic (target Cohen’s κ ≥ 0.8) will be calculated for initial coding consistency, the primary focus will be on the iterative and interpretive process of theme development, ensuring a nuanced understanding of feasibility, acceptability, and sustainability. Themes will highlight acceptability factors (eg, “value of NPMP”, “motivation”), feasibility issues (eg, “resource adequacy”, “logistical challenges”), and sustainability aspects (eg, “institutional support”, “mentor succession”), providing depth to quantitative findings.
Statistical assumptions will presume normality for parametric tests, verified with Q-Q plots, while qualitative results will rely on participant honesty, safeguarded by anonymity and rapport-building. Potential biases, such as self-selection due to convenience sampling and the exclusion of students with prior structured mentorship, will be noted and acknowledged as limitations in the final report, with sensitivity analyses (eg, excluding dropouts) conducted to test finding robustness. This mixed-methods approach will ensure a comprehensive evaluation of the NPMP’s outcomes, balancing statistical rigor with contextual insights.
Discussion
Medical students in low- and middle-income countries like Uganda face significant barriers to engaging in surgical research, including limited mentorship, inadequate resources, and a lack of structured opportunities, particularly at institutions like Makerere University. Our proposed NPMP innovatively integrates a tiered mentorship model-residents guiding senior students, who mentor juniors-harnessing the relatability of near-peers and the expertise of residents to address these contextual challenges. This approach builds on evidence of near-peer mentoring’s success in boosting research output, as seen in prior studies reporting over 100% increases in conference posters and publications.8,9 By leveraging existing student and resident capacity within the Makerere University Surgery Society (MUSS), we aim to create a supportive framework that fosters research skills, overcomes mentorship gaps, and enhances students’ contributions to surgical knowledge, potentially improving local healthcare solutions.
Beyond immediate skill development, our model promotes a sustainable research culture by empowering students as active participants in their education. Engaging senior students as mentors not only builds their leadership but also ensures a pipeline of future mentors, enhancing scalability and penetration within MUSS. This study could indirectly elevate the competitiveness of Makerere graduates for residency programs, where research experience is increasingly valued while fostering a collaborative academic environment. Successful implementation of the NPMP will provide a feasible, student-led framework replicable in other resource-limited settings, laying the groundwork for larger trials to assess its long-term impact on research productivity and professional growth. By increasing surgical research output, we aim to strengthen evidence-based practice in Uganda, contributing to global medical education goals and addressing disparities in research participation.
The NPMP’s tiered structure also tackles practical barriers, such as overburdened faculty, by redistributing mentorship responsibilities across existing human resources. Its low-resource design-relying on workshops and case reports rather than extensive funding-enhances its adaptability to similar contexts worldwide. If effective, this intervention could shift the narrative of student research involvement in East Africa, aligning with broader efforts to institutionalize mentorship, as highlighted in prior Makerere surveys.7 Our findings will offer a blueprint for embedding research training within medical curricula, potentially influencing policy at MakCHS and beyond, while providing data to refine mentorship strategies in resource-constrained settings. Beyond immediate skill development, our model promotes a sustainable research culture by empowering students as active participants in their education. The evaluation of sustainability within this protocol focuses on assessing the program’s capacity for long-term embedding within MUSS, laying the groundwork for future longitudinal studies to track its continued impact.
We anticipate challenges, such as scheduling conflicts due to academic and clinical demands, which will be mitigated by offering flexible workshop timings (eg, evenings, weekends) and virtual options where feasible. Resistance to mentorship roles among senior students or residents, possibly due to time constraints, will be addressed through incentives like co-authorship on case reports, formal recognition by MUSS, certificates of participation, and skill development workshops that enhance their CVs and future career prospects. Attrition risks from workload fatigue will be minimized by maintaining a 20% dropout buffer in our sample size and providing ongoing support via feedback sessions. This threshold is consistent with the widely cited “20% rule”, which notes that loss-to-follow-up of up to 20% rarely introduces serious bias, while >20% can downgrade the strength of evidence in research.13 The allowance therefore provides a conservative yet methodologically sound margin to safeguard study validity over a 12-month follow-up period. Ethical concerns, such as pressure to participate, will be managed through voluntary consent and clear communication of benefits, ensuring participant autonomy and well-being throughout the study. The NPMP aims to increase surgical research output, improve skills, and establish a sustainable mentorship culture within MUSS. While a 12-month implementation period may be limited for observing a significant increase in published case reports, our primary focus is on boosting the production and submission of quality case reports and developing core research competencies within this timeframe, fostering a foundation for future publications. Limitations of the study will include the lack of a control group and potential selection bias; however, this implementation research will aim to establish a scalable model rather than prove direct causality.
Conclusion
A tiered near-peer mentorship model leveraging residents and senior students, specifically designed for the resource-limited context of Makerere University, could significantly enhance surgical research output, skills, and engagement among medical students. By addressing key barriers such as limited mentorship, inadequate resources, and lack of structured opportunities, this approach within the Makerere University Surgery Society (MUSS) may prove more sustainable and feasible, fostering a lasting research culture. These findings could pave the way for improved evidence-based practice in Uganda, warranting further investigation into its scalability and long-term impact across similar settings.
Abbreviations
MakCHS, Makerere University College of Health Sciences; MUSS, Makerere University Surgery Society; NPMP, Near-Peer Mentorship Program; RE-AIM, Reach, Effectiveness, Adoption, Implementation, Maintenance; SLT, Social Learning Theory; CAM, Cognitive Apprenticeship Model.
Data Sharing Statement
Data and materials will be accessible upon reasonable request from the corresponding author (Ivaan Pitua) with institutional approval. Findings will be disseminated to students, faculty, and stakeholders via MUSS meetings, briefs, and media, as well as to the scientific community through peer-reviewed publication and conferences.
Ethical Approval and Consent to Participate
This protocol has been approved by the Mulago Hospital Research and Ethics Committee (Protocol Approval Number MHREC 2931). Written informed consent will be obtained from all participants prior to recruitment emphasizing their voluntary participation and right to withdraw at any time without penalty. To ensure confidentiality, all collected data will be de-identified using unique participant codes, and sensitive information will be stored in password-protected files accessible only to the research team. Discussions related to mentorship relationships will be conducted in a confidential and respectful manner, with a clear emphasis on fostering a supportive environment and managing any perceived power imbalances through clear communication channels and an explicit opt-out mechanism for any participant feeling undue pressure.
Acknowledgments
We acknowledge the Makerere University Surgery Society (MUSS) and the Department of Surgery at Mulago National Referral Hospital for supporting efforts critical to shaping this research protocol.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Study will be funded by first author with contribution from co-authors. There is no external funding.
Disclosure
The authors declare no competing interests.
References
1. Ofei-Dodoo S. The importance of basic research knowledge in undergraduate medical education. Kans J Med. 2025;18(1):28–30. doi:10.17161/kjm.vol18.22599
2. Conover GM, Monk MB, Nigli S, Awalt A. Early exposure of medical students to a formal research program promotes successful scholarship in a multi-campus medical school. Med Sci Educator. 2024;34(5):1091–1103. doi:10.1007/s40670-024-02098-6
3. Ng’oda M, Gatheru PM, Oyeyemi O, et al. Mentorship in health research institutions in Africa: a systematic review of approaches, benefits, successes, gaps and challenges. PLOS Global Public Health. 2024;4(9):e0003314. doi:10.1371/journal.pgph.0003314
4. Dakhil ZA, Cader FA, Banerjee A. Challenges in clinical research in low and middle income countries: early career cardiologists. Perspect Global Heart. 2024;19(1). doi:10.5334/gh.1293
5. Elobu A, Kintu A, Galukande M, et al. Research in surgery and anesthesia: challenges for post-graduate trainees in Uganda. Education for Health. 2015;28(1):11–15. doi:10.4103/1357-6283.161826
6. Nissen T, Wynn R. The clinical case report: a review of its merits and limitations. BMC Res Notes. 2014;7(1):264. doi:10.1186/1756-0500-7-264
7. Nakanjako D, Byakika-Kibwika P, Kintu K, et al. Mentorship needs at academic institutions in resource-limited settings: a survey at Makerere university college of health sciences. BMC Medical Education. 2011;11(1):53. doi:10.1186/1472-6920-11-53
8. Oak S, Glickman C, McMackin K. Near-peer mentorship: promoting medical student research with resident pairing. J Med Educ Curricular Develop. 2025;12:23821205251329659. doi:10.1177/23821205251329659
9. Lakhani D, Swaney K, Hogg J. “Resident managed peer-mentoring program”: a novel way to engage medical students and radiology residents in collaborative research. Acad Radiol. 2021;29(9):1425–1431. doi:10.1016/j.acra.2021.11.004
10. Murrell AJ, Blake-Beard S, Porter DM Jr. The Importance of peer mentoring, identity work and holding environments: a study of African American leadership development. Int J Environ Res Public Health. 2021;18(9):4920. doi:10.3390/ijerph18094920
11. Kiyimba B, Atulinda L, Nalunkuma R, et al. Research involvement among undergraduate health profession students in a resource-limited setting: awareness, attitude, motivators and barriers. BMC Med Educ. 2022;22(1):249. doi:10.1186/s12909-022-03320-y
12. Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687.
13. Fewtrell MS, Kennedy K, Singhal A, et al. How much loss to follow-up is acceptable in long-term randomised trials and prospective studies? Arch Dischildhood. 2008;93(6):458. doi:10.1136/adc.2007.127316
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.