Back to Journals » Risk Management and Healthcare Policy » Volume 16
Implementation of Telemonitoring in Health Care: Facilitators and Barriers for Using eHealth for Older Adults with Chronic Conditions
Authors Liljeroos M, Arkkukangas M ![]()
Received 7 November 2022
Accepted for publication 5 January 2023
Published 10 January 2023 Volume 2023:16 Pages 43—53
DOI https://doi.org/10.2147/RMHP.S396495
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Maria Liljeroos,1,2,* Marina Arkkukangas2– 4,*
1Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden; 2Centre for Clinical Research Sörmland, Uppsala University, Eskilstuna, Sweden; 3Department of Medicine and Sport Sciences, School of Health and Welfare, Dalarna University, Falun, Sweden; 4Department of Physiotherapy, School of Health, Care and Social Welfare, Mälardalen University, Västerås, Sweden
*These authors contributed equally to this work
Correspondence: Marina Arkkukangas, Research and Development in Sörmland, Eskilstuna, Sweden, Tel +46 706468868, Email [email protected]
Purpose: The retrospective study used a hybrid design aimed to a) describe the implementation process of telemonitoring from stakeholders’ perspectives and b) identify facilitators and barriers perceived by the care team.
Patients and Methods: Qualitative interview data were analyzed using manifest inductive qualitative content analysis to describe what was perceived as barriers and what facilitated the implementation. Participating healthcare professionals recruited from a multi-professional care team in Sweden. Overall, 14 healthcare professionals comprising 8 assistant nurses, 3 nurses, 1 physiotherapist, 1 occupational therapist, and one general practitioner participated in five interviews.
Results: Four categories were derived from the interview analysis: previous experience with digital technology, the need for preparation before implementation, perceptions of using telemonitoring in daily practice from the patient’s perspective, and perceptions of the relevance and reasons for applying telemonitoring from the care team’s perspective. The identification of stakeholders and the need to plan carefully when proposing the introduction of telemonitoring systems into work practices are both crucial.
Conclusion: The attitudes of healthcare professionals can be a significant factor in the acceptance and efficiency of the use of telemonitoring in practice. Therefore, implementing new technology in healthcare should involve healthcare professionals at an early stage to gain common understanding.
Keywords: implementation, technology, multimorbidity, homecare
Introduction
A key challenge in health care is to provide the best care to all persons with health issues. Older adults with complex long-term needs require coordinated and seamless care from several providers. Globally, the older age group is rapidly growing and as the older population consumes relatively more healthcare services,1,2 fulfilling the growing demand for such services is expected to be a challenge in the future. Thus, new ways of providing care are urgently needed.3 Moreover, aging is well known to be associated with disabilities, frailty, and a reduction in independence in daily life.4,5 Therefore, new ways to support and promote health and well-being in old age are important.
There is growing interest in providing care using technology. According to the World Health Organization (WHO), eHealth involves “using information and communication technologies (ICT) for health”. In, 2021 the Global strategy on digital health 2020–2025 was presented by the WHO, wherein they urged the creation of a long-term strategic plan for developing and implementing eHealth services.6 This warrants more research on eHealth.
Telemonitoring is commonly defined as
the remote monitoring of patients, including the use of audio, video, and other telecommunications and electronic information processing technologies, to monitor patient status at a distance.7
Telemonitoring, a suggested future alternative in health care, could increase patient care and the effectiveness of treatment.8 Furthermore, telemonitoring has been shown to enhance clinicians’ ability to manage patients in non-traditional healthcare settings.9 The different types of sensors and measures commonly tested in recent decades include accelerometer, electrocardiogram (ECG), blood pressure, blood glucose, body temperature, weight, and oxygen saturation.10 However, the optimal use of telemonitoring remains a challenge, though smaller pilot studies have presented promising results.11,12 Nonetheless, these results are difficult to replicate when implemented on a large scale. Thus, the evidence for large-scale interventions and the cost-effectiveness of telemonitoring remains scant.13,14 Moreover, some patients miss the face-to-face interaction and office-based visits to healthcare clinics when using telemonitoring.15 Some hospitals do not plan ahead before implementing telemonitoring and, therefore, have no routines for documenting transmissions and lack action plans for managing alerts.15 Furthermore, successful implementation of eHealth is challenging, as reported in several studies.16,17 Additionally, managers and policymakers must consider applying this new way of work to existing practices within and across organizations. This aspect is crucial to address in a complex inter-organizational setting such as health care.
For healthcare providers, factors such as capacity and knowledge, state of mind, way of thinking, and attitudes are important aspects that have been sparsely investigated.18 Considering the lack of evidence supporting the effects and implementation of telemonitoring in healthcare organizations, there is a need to further investigate them, both qualitatively and quantitatively.
In 2020, a unique collaboration between two public health care providers in middle Sweden, the region and municipality, was initiated. These public health care providers have different documentation and patient journal systems. The collaboration was a cohesive multi-professional care team for older adults with multimorbidity and complex needs. The team aimed to increase patients’ sense of independence and security and their ability to handle their own health and reduce the need for hospitalizations and emergency visits. One of the team’s assignments given by the project leaders was to test the use of e-health and telemonitoring. The technology consisted of a customized care platform with different sensors depending on each patient’s diagnoses and individual needs. The available sensors included a weighing scale and blood pressure and heart rate, ECG, oxygen saturation, and physical activity level monitors. Each patient’s daily measurements were sent to the nurses in the care team through a web interface. The nurses were informed of the telemonitoring test and received information regarding the technology early in the process.
As there is a lack of research concerning e-health solutions and telemonitoring used in clinical practice, the overall study aims to investigate 1) the implementation process and 2) clinical outcomes of telemonitoring among older adults with chronic conditions receiving home care from two different caregivers working in the same care team, the region and municipality. This study reports the first phase describing the implementation process of care using telemonitoring.
The aim was to a) describe the implementation process from stakeholders’ perspectives and b) identify facilitators and barriers perceived by the care team.
Materials and Methods
Design
A hybrid design19 was used in the overall project, which refers to the project testing effects of a clinical intervention on relevant outcomes while observing and gathering information on the implementation process when introducing technology in the home of older adults with multimorbidity according to the Quality Implementation Framework.20 The framework comprises five parts: (1) Adaptation and preparation capacity and competence to perform the implementation are mapped out, (2) Competence development, practical, and theoretical training based on the findings in part 1; (3) Consensus regarding objectives is created; (4) Continuous support and skills development, (5) Evaluation and continuous feedback.20
A hybrid design facilitates both determining the utility of an implementation intervention and assessing clinical outcomes associated with implementation. This study only reports the adaptation and preparation (Phases 1 and 2) of the first phase of the main project from stakeholders’ perspectives, that is, the implementation process until intervention is started.
Data were analyzed using a qualitative design, and The COREQ checklist was used in this study.21
Data Collection and Participants
In Phase 1, a mapping of the stakeholders assumed to be involved in or affected by the implementation of telemonitoring in the context of the care team was undertaken. Field notes, commonly used in qualitative research, were used to document contextual information.22 This map was based on our experience and understanding of the empirical arena. The project group, comprising two project leaders, collaborated with the researchers during the entire implementation process. The project leaders were responsible for arranging regular stakeholder meetings to keep everyone updated and document the entire process. They were also responsible for driving the process toward the goal.
Identification of frail older outpatients and family members in need of help in their own homes was included in the map but is not part of Phases 1 and 2 in this study. Scheduled meetings were conducted among the mapped stakeholders to discuss the implementation of telemonitoring in health care.
In Phase 2, all members of the care team were invited to participate in interviews with a letter describing the purpose of the study. This care team consisted of a special composition in which two healthcare providers were involved: the municipality and region. The care team consisted of three nurses, one employed by the region and two by the municipality; 14 municipally employed assistant nurses; and one physician which all cared for all patients admitted in the care team. Other professions associated with the team include a psychologist, dietician, pharmacist, counselor, physiotherapist, and occupational therapist. The interviews were conducted by a moderator (first author) who was responsible for directing the discussion and facilitating the conversation flow. The second author also attended the interviews as an observer and was responsible for taking field notes and tape recording the interview sessions.
Five interviews were performed and a total of 14 care team members were interviewed; they comprised assistant nurses (8), nurses (3), a physiotherapist (PT; 1), an occupational therapist (OT; 1), and a general practitioner (GP; 1). As the purpose was to perform the interviews with each occupational group separately, the number of participants was not the same in every interview (see Table 1). None of the team members declined participation. During the interviews, participants were asked about their previous experiences with any kind of technology previously used in a healthcare setting; expected problems associated with the implementation; potential modifications that could be made to maximize implementation; potential implementation strategies, skills, or training necessary for healthcare professionals to work with the technology; and their thoughts regarding patients’ perspectives. Trustworthiness was addressed, and the authors were aware of their pre-understandings and existing knowledge about the context. The first author, a registered nurse (RN), performed the interviews and transcriptions, and was also aware of the RN lens that she possessed. The second author was a registered physiotherapist (RPT).
 |
Table 1 Description of Participants per Each Interview |
Data Analysis
Descriptive observational field notes were used for Phase 1 of the study. For Phase 2, transcribed text from interviews was analyzed using manifest inductive qualitative content analysis23 to describe what was perceived as a barrier and what facilitated the implementation.19,24 By using the chosen approach, the description of what the informants actually said is the focus, remains close to the text, and describes what is visible and obvious in the text. The analysis began with open coding of all transcribed data and observational field notes, creating preliminary sub-categories that described the phenomenon by deciding which codes could be combined based on how they were related and linked.23 Based on the relationships among subcategories, we combined them into categories. The software NVivo 12 Plus was used to support the analysis. NVivo software is commonly used to support qualitative and mixed-methods research and facilitate the sorting and labling of data. NVivo gives a good overview during the entire analysis.
Ethics
This study was approved by the Swedish Ethical Review Authority (board of Linköping, 2020-06420), and was performed in accordance with the 1964 Declaration of Helsinki. Participants received no compensation for their participation. Written informed consent, including publication of anonymized responses was obtained before the onset of the study. Clinical trial registration: NCT04955600.
Results
Phase 1 Description of the Implementation Process from Stakeholders’ Perspectives
The following stakeholders were identified by the project leaders and the researchers: employees in the care team, innovators of the technology, local politicians in the municipality and in the region, project managers, and the IT department in the region. When the research project was being developed, it was outlined as a cooperative effort among municipalities, the region, vendors, and researchers. The researchers were present at all meetings with the stakeholders; they took field notes of the discussions and decisions made during the meetings. These discussions identified barriers to implementation, which could be from a legal, logistical, or economical perspective or any combination of these. As this was a regional project with an aim to upscale in the future, the meetings included acceptance and support of the project from politicians and head managers in the region and from all the nine municipalities in the region. Issues such as municipality and region regulations and legislation involving data sharing and cloud service were identified and resolved in collaboration. Cloud services outside the European Union (EU) were not accepted according to Swedish laws, and the intended telemonitoring´s cloud service was in the EU. One of the most challenging parts of the project was the procurement of the intended technology; as the project included services from both the region and the municipality, such agreements were previously unknown for both organizations. This issue was resolved after receiving support from the IT departments and representatives from both the region and the municipalities in collaboration.
To ensure the architecture for data management and workflow, the IT department held meetings with healthcare staff to map their daily routines to develop the architectural landscape for telemonitoring, including investigation of the security and privacy of essential data and cloud service management. This process led to an identified workflow developed in collaboration across organizational boundaries. The need for this workflow was expressed by the healthcare staff as a prerequisite for understanding the technology and for the impact the technology would have on their daily work.
Phase 2 Interviews with Healthcare Staff
Interviews with healthcare staff were conducted to gain an understanding of the empirical arena for telemonitoring. Before the interviews, the participants were informed that the purpose of the interview was to explore their previous experiences with technology and perceptions of implementing telemonitoring in clinical practice. The team members were given a short introduction to the technology by the researchers prior to the interview. They also browsed the company’s web (OPTILOGG®) page to view the platform and sensors. A total of 14 healthcare professionals participated in five interviews (see Table 1).
Four categories described healthcare professionals` perspectives and expectations of telemonitoring (see Table 2). Identified facilitators and barriers and clinical implications based on the team members are presented in Table 3.
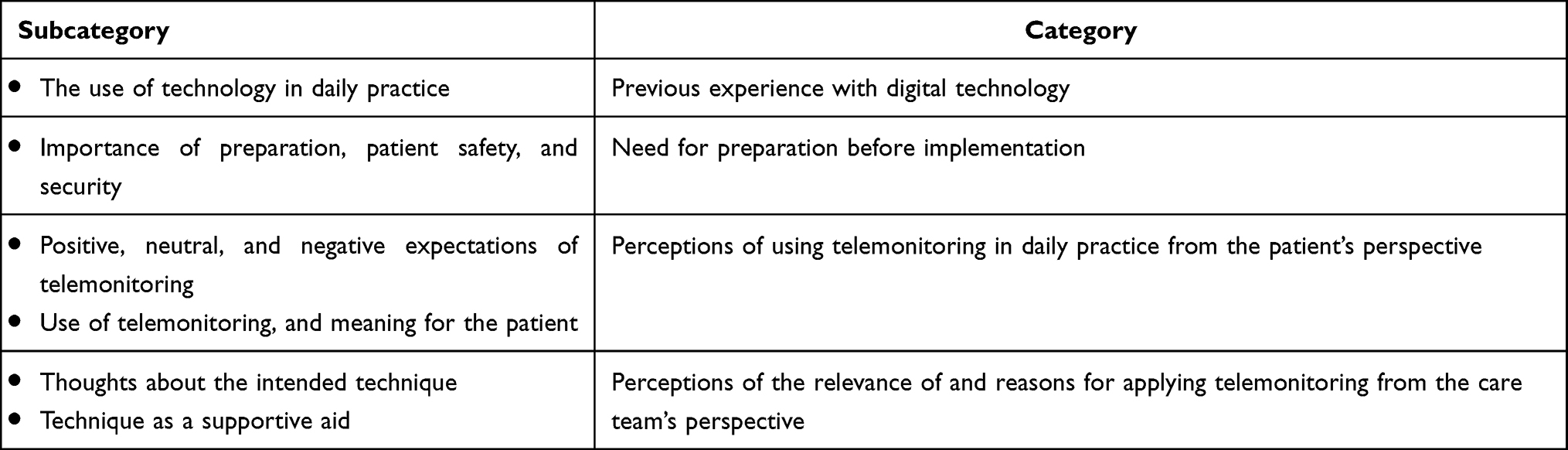 |
Table 2 Overview of Subcategories and Categories |
 |
Table 3 Identified Facilitators and Barriers, Weighted Results, and Clinical Implications |
Team Members’ Previous Experience with Digital Technology
The Use of Technology in Daily Practice
Previous experience with digital technology varied among professions in the care team. Nurses and assistant nurses reported using smartphones in their daily work when visiting patients at home. They used their mobile phones to assess the care plan and patients’ medical treatment, which was reported to be accessible and easy to read on the phone. The assistant nurses were also able to digitally connect with nurses when they were in the patient’s home and the nurse was at the clinic. However, this technology was newly implemented and had not been used by all members of the care team. Nonetheless, nurses perceived this type of digital meeting as helpful when evaluating symptoms and signs of deterioration and being able to see and speak to the patient from a distance. However, most patients were unable to use digital consultations by themselves without help from assistant nurses as a secure personal identification system, which was unfamiliar to most patients, was required to be able to access the system. One assistant nurse expressed the following:
Because it’s required to be able to have a secure personal identification system to be able to log in, and then it gets difficult. But now it must go through us, so you have to be in place. (Assistant nurse)
The physiotherapist and occupational therapist expressed that the use of digital technology in their daily work was sparse; they were more dependent on physical contact with the patient when performing assessment and treatment, adjusting environmental aspects, and delivering different aids.
We still need to go personally to the user and make an assessment in real life. We would like to see, feel, and live it as well, directly. Therefore, we do not want everything to be digital.
Different experiences using digital technology in daily practice were expressed among different professions. The overall experience of digital technology was that it is useful when it worked as planned, but malfunctions were commonly attributed to either loss of contact with the network or patients’ lack of experience using digital services in their daily lives.
Need for Preparation Before Implementation
Importance of Preparation, Patient Safety, and Security
The participants expressed the importance of their involvement in the implementation process and of having the opportunity to ask questions to prepare themselves and the patients before the implementation. An assistant nurse expressed the following:
Well, I do not really know what vital factors you can monitor with that, so it’s not only weight, I think. (Assistant nurse)
Most participants stressed the importance of planning ahead, changing routines, and involving all team members prior to implementation. The need for safety routines if the technology did not function was also highlighted. Some assistant nurses expressed the following:
We all know that technology does not run like clockwork all of the time, and it is clear that… I think that in the preparations, finding routines for the day is also included when the technology does not work, when the Internet is down or not. (Assistant nurse)
After a routine is created, who should do the observations; is it the nurses or the assistant nurses? I think that if you start a project like this, it should not only be for someone who only sits to observe because we all want to learn it, but it is a routine that we have to create where everyone can take part. (Assistant nurse)
The nurses and assistant nurses recognized the need to be able to conduct emergency visits if patients send worsening vital factors, and when that happens, they need easy access to the general practitioner for advice.
Perceptions of Using Telemonitoring in Daily Practice from the Patients’ Perspective
Positive, Neutral, and Negative Expectations of Telemonitoring
The care team expressed positive, neutral, and negative expectations when asked what they thought implementing telemonitoring would mean for the patients. They thought that some patients would feel less bound to adapting their daily life around the time of home visits by the care team. Telemonitoring might also empower patients and make them more active when they are able to perform self-care activities by themselves or with support from the care team from a distance when they feel the need.
And it creates opportunities…for a little more freedom. The patients themselves can follow, like this: “Okay, now I see that the weight has gone up, and then I will do this.” (General practitioner)
Changes in activity could be one way to detect signs of deterioration in time-adapted exercises, which, in turn, would result in a more preventive way of working. Therefore, participants expressed that this type of monitoring would likely lead to more home visits. A physiotherapist expressed the following:
Maybe even more visits, if you saw that exercise, for example, or something we had prescribed to the person, reduced the number of performances maybe, something like that. Or vice versa, such that when we see that this person is not moving, then perhaps we need to go there and see what is happening, and why. We may include the prescription of exercise in this case.
The team highlighted the importance of individually choosing measures needed for each patient and not thinking that “one size fits all.” Determining which vital factors would be useful and what equipment each patient would be likely to manage could be a challenge. For some patients, distance monitoring could mean that the team makes more home visits because more health data is available. One nurse expressed the following:
It could also be that they received more visits. If you notice that they feel bad and they do not say anything, then maybe we will see it anyway with this type of monitoring.
Use of Telemonitoring and Meaning for the Patient
For some patients, telemonitoring can increase loneliness as those managed by the team are the oldest and most frail. Of these, many patients live alone, and their only regular visitors are members of the care team. They were also hesitant regarding how many of the patients would be able to handle the technology as they do not use smartphones or computers in their daily lives.
Maybe they will feel lonelier; it will not be that visit to the patient. (Nurse)
The personal contact may be lost. (Nurse)
Yes exactly. Therefore, it may mean fewer visits if you can communicate like this. However, if the patient is ill, you go there. So, when you see them… about the patient… they are bad values, and the patient is short of breath, then you go there. (Nurse)
Perceptions of the Relevance of and Reasons for Applying Telemonitoring from the Care Team’s Perspective
Thoughts About the Intended Technique
From the care team’s perspective, some felt they had not been involved in the process of deciding to implement telemonitoring and asked what the reason for implementation was. During the interviews, they questioned whether there were economic reasons and whether it indicated less caring and more administration for them. One assistant nurse asked the following:
What spins in my head is what you gain from it, that is, in the long run, financially, or health-wise. If you say that the free life means that they will become more independent, will it give positive results for the person?
Hence, they realized that telemonitoring is the future, and it is important to be on the frontline, testing the new technique. However, the need for the technology to be adapted to suit the care rather than care being adapted to technology, was emphasized. A general practitioner and a nurse stated the following:
What’s going on here now… for my professional role? If I can just sit and assess lung X-rays, what should happen to my job? On the other hand, it creates completely new opportunities and develops jobs. (General practitioner)
Yes, you should probably look at it, so to speak, as an aid and nothing that fully replaces us. (Nurse)
Technique as a Supportive Aid
On the positive side, when telemonitoring is set up in the patient’s home, the assistant nurses do not have to carry the equipment when visiting the patients. Moreover, being able to access patients’ measurements every day at the office makes it easier to prioritize which patients to visit each day.
Some of the reflections also regarded technology providing safe, secure, and accurate health data documentation, compared to taking notes of various health data during home visits by several different professionals on a daily basis.
Perhaps monitoring will provide more accurate information or something like that. (occupational therapist)
Maybe monitoring will lead to security for certain things. However, it cannot be wrong if the values are where they are. With the values today, they can disappear because of human factors. (Assistant nurse)
Discussion
This study aimed to describe the implementation process from the perspectives of both stakeholders and healthcare professionals. When integrating two public health care providers, aiming to provide health care in a non-traditional way, two aspects should be highlighted. First, using telemonitoring needs careful planning for both the organizations and the health care professionals involved. Second, in the planning, several important aspects were identified; responsibilities, safety, workflows, and knowledge and education, were judged by the research team to be important to address for further successful implementation of telemonitoring in this study.
This study identified important stakeholders for the successful implementation of telemonitoring, which was viewed as a prerequisite when two healthcare providers were involved. The identified stakeholders largely agreed to support the implementation of the suggested technology, providing resources for the intervention. Implementing telemonitoring includes individual and organizational efforts in managing changing organizational boundaries that are often context-bounded, along with key factors such as organizational culture, motivation of front-line professionals, and funding.25–27 Moreover, this change includes the ability to cross-disciplinary, professional, and cultural boundaries and collaborate in interdisciplinary and inter-professional teams.28 In the implementation process, the need to study the workflow(s) and the clinical processes involved was crucial, which has been identified in previous studies.29 However, the process of employing telemonitoring, especially in terms of focusing on ensuring the right to privacy and protection of personal data, was complex, and the need to involve experts handling these issues was the core in the implementation process. The need for support from stakeholders has been suggested for successful interventions in previous studies when implementing and delivering technology services on a large scale.30,31 Therefore, it is applied by using the study design. In a previous study, the authors highlighted the importance that technology companies, healthcare providers, and public health officials operate with the highest ethical standards, especially when existing privacy regulations do not apply.32 As this is the first study in Sweden to integrate two healthcare providers, the municipality and the region, telemonitoring represents a new and potentially problematic incursion into the privacy of people when applied in the users’ homes, and this must be addressed.
The interviews with the care team highlighted several important aspects related to the usefulness and relevance and reasons for using telemonitoring in their daily work. Clinical usefulness has previously been reported; the intended telemonitoring must be evaluated regarding clinical usefulness, patient safety, and effects on staff workload,33 aspects confirmed by our study results. They all agreed that technology will certainly change the future way of work with respect to caring for older adults regarding the importance of planning ahead, changing routines, and involving all team members. The need for safety routines for technology backup, network issues, and other disturbances related to the function of the technology was highlighted as important to secure prior to implementation. Expressed barriers included a perceived lack of technical literacy among older adults, as many of whom have issues using technology and secure personal identification systems. This barrier was also confirmed in a systematic review, in which older adults expressed barriers such as technical literacy, lack of desire, cost, lack of technical support, privacy and security concerns, and medical literacy.34 Increased loneliness among older adults when fewer physical home visits were performed was a concern, which correlates with a recent study in which nurses expressed fear of weakening their relationship with older adults when implementing in-home sensors.35 Conversely, the care team expressed that telemonitoring could support older adults to become empowered and more active when they are able to perform self-care activities in their daily life. This was confirmed by older adults in a study at the post-implementation stage, in which the benefits that technology can have on their lives were highlighted.29
This study presents results from two perspectives, that of stakeholders and that of healthcare professionals. Notably, stakeholders should consider factors other than organizational factors that may affect implementation, including involving, engaging, and supporting healthcare professionals, prior to implementation. These aspects were not addressed from the stakeholder’s perspective in this study.36 This gap was confirmed by the care team as they expressed a lack of education and involvement in the process prior to implementation. These identified gaps between stakeholders and the care team provided valuable insight for further implementation of telemonitoring. Moreover, some reflections regarding differences in attitudes and views of patients’ abilities among the different professionals on the care team should be highlighted. These views relate to challenges in providing person-centered care (PCC).37,38
This study focussed on describing the implementation process from the perspectives of the stakeholders and healthcare providers. However, in the next phase, telemonitoring must be personalized for the needs, capabilities, and preferences of older patients, with adaptation over time as care needs evolve. This will be investigated in the second phase of this project.
Although telemonitoring has been the subject of much research and development for several years, this study contributes to the knowledge of using telemonitoring when two healthcare providers are involved. Recruiting participants from all involved healthcare professionals enrichened the results as they had different experiences from the caring perspective. The interaction in the group interviews gave rich narratives where participants were inspired by each other. However, being interviewed in a group may be a barrier to expressing opinions for some; therefore, some interviews are in smaller groups or individually performed. At the end of each interview, the participants were encouraged to discuss topics they considered important that were not addressed during the interviews. Further, the combination of telemonitoring, including wearable sensors and in-home monitoring systems in a real-life setting, has only been minimally investigated,39 leading to the relevance of this study. Some successful telemonitoring interventions in primary care have been presented; recent evidence indicates that home telemonitoring of chronic patients reduces the use of healthcare resources. However, further studies exploring this issue are needed in primary care, particularly regarding experiences during the COVID-19 pandemic and the importance of digital solutions in health care.40,41
Conclusion
The identification of stakeholders and the need to plan carefully when proposing the introduction of telemonitoring systems into work practices are both crucial. However, opinions from a broader range of stakeholders are needed before a coherent strategic plan can be formulated. This study also highlights the importance of including involving, engaging, and supporting healthcare professionals, prior to implementation of telemonitoring in health care. The attitudes of healthcare professionals can be a significant factor in the acceptance and efficiency of the use of telemonitoring in practice. Therefore, implementing new technology in healthcare should involve healthcare professionals at an early stage to gain common understanding. Furthermore, one of the main reasons for implementing telemonitoring in in-home settings was to promote older adults’ independence and self-care, a promising insight from the study.
Data Sharing Statement
Data are available from corresponding author, Marina Arkkukangas upon request.
Acknowledgments
We would like to thank all of the care team members and project leaders for their valuable contributions during this portion of the implementation process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Swedish Association of Local Authorities and Regions (SALAR). The sponsors had no involvement in any of the stages from study design to publication.
Disclosure
The authors report that there are no competing interests to declare for this work.
References
1. Hajek A, Brettschneider C, Scherer M, et al. Needs and health care costs in old age: a longitudinal perspective: results from the AgeMooDe study. Aging Ment Health. 2020;24(10):1763–1768. doi:10.1080/13607863.2019.1673310
2. Lehnert T, Heider D, Leicht H, et al. Review: health care utilization and costs of elderly persons with multiple chronic conditions. Med Care Res Rev. 2011;68(4):387–420. doi:10.1177/1077558711399580
3. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi:10.1016/S0140-6736(12)60240-2
4. Saedi AA, Feehan J, Phu S, Duque G. Current and emerging biomarkers of frailty in the elderly. Clin Interv Aging. 2019;14:389–398. doi:10.2147/CIA.S168687
5. LeBrasseur NK, de Cabo R, Fielding R, et al. Identifying biomarkers for biological age: geroscience and the ICFSR task force. J Frailty Aging. 2021;10(3):196–201. doi:10.14283/jfa.2021.5
6. World Health Organization. Global Strategy on Digital Health 2020–2025. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
7. Institute of Medicine. (US) Committee on Evaluating Clinical Applications of Telemedicine. Telemedicine: A Guide to Assessing Telecommunications for Health Care. Field MJ, editor. Washington (DC): National Academies Press; 1996. doi:10.17226/5296
8. Farias FAC, Dagostini CM, Bicca YA, Falavigna VF, Falavigna A. Remote patient monitoring: a systematic review. Telemed J E Health. 2020;26(5):576–583. doi:10.1089/tmj.2019.0066
9. Aamodt IT, Lycholip E, Celutkiene J, et al. Health care professionals’ perceptions of home telemonitoring in heart failure care: cross-sectional survey. J Med Internet Res. 2019;21(2):e10362. doi:10.2196/10362
10. Do Nascimento LMSD, Bonfati LV, Freitas MB, Mendes JJA, Siqueira HV, Stevan SL. Sensors and systems for physical rehabilitation and health monitoring—a review. Sensors. 2020;20(15):4063. doi:10.3390/s20154063
11. Hägglund E, Lyngå P, Frie F, et al. Patient-centred home-based management of heart failure. Findings from a randomised clinical trial evaluating a tablet computer for self-care, quality of life and effects on knowledge. Scand Cardiovasc J. 2015;49(4):193–199. doi:10.3109/14017431.2015.1035319
12. Hovland-Tånneryd A, Melin M, Hägglund E, Hagerman I, Persson HE. From randomised controlled trial to real world implementation of a novel home-based heart failure tool: pooled and comparative analyses of two clinical controlled trials. Open Heart. 2019;6(1):e000954. doi:10.1136/openhrt-2018-000954
13. Witt Udsen F, Lilholt PH, Hejlesen O, Ehlers L. Cost-effectiveness of telehealth care to patients with chronic obstructive pulmonary disease: results from the Danish “TeleCare North” cluster-randomised trial. BMJ. 2017;7(5):e014616. doi:10.1136/bmjopen-2016-014616
14. Wootton R. Twenty years of telemedicine in chronic disease management – an evidence synthesis. J Telemed Telecare. 2012;18(4):211–220. doi:10.1258/jtt.2012.120219
15. Liljeroos M, Thylén I, Strömberg A. Patients’ and nurses’ experiences and perceptions of remote monitoring of implantable cardiac defibrillators in heart failure: cross-sectional, descriptive, mixed methods study. J Med Internet Res. 2020;22(9):e19550. doi:10.2196/19550
16. Christensen MC, Remler D. Information and communications technology in U.S. health care: why is adoption so slow and is slower better? J Health Polit Policy Law. 2009;34(6):1011–1034. doi:10.1215/03616878-2009-034
17. Murray E, Burns J, May C, et al. Why is it difficult to implement e-health initiatives? A qualitative study. Implement Sci. 2011;6:6. doi:10.1186/1748-5908-6-6
18. Koivunen M, Saranto K. Nursing professionals’ experiences of the facilitators and barriers to the use of telehealth applications: a systematic review of qualitative studies. Scand J Caring Sci. 2018;32(1):24–44. doi:10.1111/scs.12445
19. Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217–226. doi:10.1097/MLR.0b013e3182408812
20. Meyers DC, Durlak JA, Wandersman A. The quality implementation framework: a synthesis of critical steps in the implementation process. Am J Commun Psychol. 2012;50(3–4):462–480. doi:10.1007/s10464-012-9522-x
21. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
22. Phillippi J, Lauderdale J. A guide to field notes for qualitative research: context and conversation. Qual Health Res. 2018;28(3):381–388. doi:10.1177/1049732317697102
23. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
24. Landes SJ, McBain SA, Curran GM. Reprint of: an introduction to effectiveness-implementation hybrid designs. Psychiatry Res. 2020;283:112630. doi:10.1016/j.psychres.2019.112630
25. Ashton T. Implementing integrated models of care: the importance of the macro-level context. Int J Integr Care. 2015;15:e019. doi:10.5334/ijic.2247
26. Auschra C. Barriers to the integration of care in inter-organisational settings: a literature review. Int J Integr Care. 2018;18(1):5. doi:10.5334/ijic.3068
27. Nolte E, Pitchforth E. What is the evidence on the economic impacts of integrated care? [Technical report]. Denmark: World Health Organization; 2014. Available from: https://researchonline.lshtm.ac.uk/id/eprint/2530944.
28. Coughlan C, Manek N, Razak Y, Klaber RE. How to improve care across boundaries. BMJ. 2020;369:m1045. doi:10.1136/bmj.m1045
29. Granja C, Janssen W, Johansen MA. Factors determining the success and failure of ehealth interventions: systematic review of the literature. J Med Internet Res. 2018;20(5):e10235. doi:10.2196/10235
30. Bujnowska-Fedak MM, Grata-Borkowska U. Use of telemedicine-based care for the aging and elderly: promises and pitfalls. Smart Homecare Technol TeleHealth. 2015;3:91–105. doi:10.2147/SHTT.S59498
31. Peek STM, Wouters EJ, Luijkx KG, Vrijhoef HJ. What it takes to successfully implement technology for aging in place: focus groups with stakeholders. J Med Internet Res. 2016;18(5):e98. doi:10.2196/jmir.5253
32. Gerke S, Shachar C, Chai PR, Cohen IG. Regulatory, safety, and privacy concerns of home monitoring technologies during COVID-19. Nat Med. 2020;26(8):1176–1182. doi:10.1038/s41591-020-0994-1
33. Glock H, Nymberg VM, Borgström BB, et al. Attitudes, Barriers, and Concerns Regarding Telemedicine Among Swedish Primary Care Physicians: a Qualitative Study. Int J Gen Med. 2021;14:9237–9246. doi:10.2147/IJGM.S334782
34. Kruse C, Fohn J, Wilson N, Nunez Patlan E, Zipp S, Mileski M. Utilization barriers and medical outcomes commensurate with the use of telehealth among older adults: systematic review. JMIR Med Inform. 2020;8(8):e20359. doi:10.2196/20359
35. Pais B, Buluschek P, DuPasquier G, et al. Evaluation of 1-year in-home monitoring technology by home-dwelling older adults, family caregivers, and nurses. Front Public Health. 2020;8:518957. doi:10.3389/fpubh.2020.518957
36. Xyrichis A, Iliopoulou K, Mackintosh NJ, et al. Healthcare stakeholders’ perceptions and experiences of factors affecting the implementation of critical care telemedicine (CCT): qualitative evidence synthesis. Cochrane Database Syst Rev. 2021;2:CD012876. doi:10.1002/14651858.CD012876.pub2
37. Malterud K, Kamps H. General practice – a fertile lagoon in the ocean of medical knowledge. Scand J Prim Health Care. 2021;39(4):515–518. doi:10.1080/02813432.2021.2004831
38. Mikkola I, Morgan S, Winell K, et al. Association of personalised care plans with monitoring and control of clinical outcomes, prescription of medication and utilisation of primary care services in patients with type 2 diabetes: an observational real-world study. Scand J Prim Health Care. 2022;40(1):39–47. doi:10.1080/02813432.2022.2036458
39. Peetoom KKB, Lexis MAS, Joore M, Dirksen CD, De Witte LP. Literature review on monitoring technologies and their outcomes in independently living elderly people. Disabil Rehabil Assist Technol. 2015;10(4):271–294. doi:10.3109/17483107.2014.961179
40. Martín-Lesende I, Orruño E, Mateos M, et al. Telemonitoring in-home complex chronic patients from primary care in routine clinical practice: impact on healthcare resources use. Eur J Gen Pract. 2017;23(1):135–142. doi:10.1080/13814788.2017.1306516
41. Thulesius H. Increased importance of digital medicine and ehealth during the Covid-19 pandemic. Scand J Prim Health Care. 2020;38(2):105–106. doi:10.1080/02813432.2020.1770466
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.