Back to Journals » Clinical Interventions in Aging » Volume 21
Implementation of Small Group Physiotherapy for People at Risk of Falls with Compromised Bone Mineral Density
Received 14 August 2025
Accepted for publication 13 December 2025
Published 29 January 2026 Volume 2026:21 560594
DOI https://doi.org/10.2147/CIA.S560594
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Christina Ziebart,1 Allison Francis2
1School of Physical Therapy, Western University, London, ON, Canada; 2ReActive Physiotherapy, London, ON, N6H 5S, Canada
Correspondence: Christina Ziebart, School of Physical Therapy, Western University, London, ON, Canada, Email [email protected]
Design: Interventional Implementation Study.
Setting: Outpatient private practice physiotherapy clinic.
Participants: Adults with osteoporosis or at risk of developing osteoporosis.
Intervention: Using the knowledge-to-action framework to implement a group physiotherapy program, participants were enrolled in a 6 week, twice weekly, 60-minute exercise intervention that targeted whole body strength and balance. Participants provided written feedback on the program.
Results: The mean age of the participants was 72 (SD: 6.03, min 60 years, max 84 years). There were 2 males, and 41 females that participated in the study. The program was successfully integrated into an outpatient physiotherapy clinic. All participants enjoyed the exercises, the social aspect, and having a booklet to support their exercise. Participants suggested that the program could be improved by having a class capacity of 9 participants per class due to space, having pictures in the booklet. Preliminary physical outcome measures showed promise, the 30-second sit-to-stand improved by a mean of 3.1 repetitions (p< 0.001).
Conclusion: There was positive patient and clinician feedback on the implementation of the program within the clinic. Future iterations of the program will need to consider sustainability and accessibility of the program within the osteoporosis population.
Plain Language Summary: Osteoporosis weakens bones and increases the risk of falls and fractures, so exercise programs that improve strength, balance, and posture are especially important. However, many people with osteoporosis face barriers to exercising, including cost, lack of knowledge, and fear of injury. They prefer small, supervised group programs that are easy to follow and tailored to their needs.
This study tested whether a physiotherapist-led group exercise program for people with low bone density or at risk of falls could be successfully implemented in a private outpatient clinic. The six-week program ran twice a week for one hour and focused on whole-body strength, balance, and safe movement strategies. Participants also received a take-home booklet to support continued exercise.
A total of 43 participants (average age 72, mostly women) participated in the study. Feedback was very positive: participants enjoyed the social aspect, the exercises, and the instructor, but suggested adding pictures to the booklet and reducing class size.
Physical assessments showed improvements in several areas, including lower body strength (sit-to-stand test), grip strength, posture, and balance. The most meaningful gain was in lower body strength, which is important for everyday activities like getting up from a chair.
The program proved to be safe, enjoyable, and feasible to run in a clinic setting. It improved strength, balance, and posture in just six weeks. Future work should focus on making similar programs more accessible and sustainable, testing them in different settings, and exploring whether participants keep exercising after the program ends.
Keywords: implementation, osteoporosis, exercise, resistance training
Background
Strength training is the primary mode of exercise recommended for people with osteoporosis due to the musculogenic, osteogenic benefits and reduction in fall risk.1,2 The 2014 osteoporosis exercise recommendations emphasized that people with osteoporosis should prioritize strength and balance training.3,4 The 2023 updated guidelines continue to emphasize strength and balance training, however, also recommend engaging in functional training exercises that support daily activities and hobbies.5 Although these guidelines emphasizing strength and balance training also align with the Canadian 24-hour movement guidelines for older adults,6 there is less of an emphasis on aerobic exercise, in the osteoporosis exercise guidelines.5 However, engaging older adults in exercise, in general, continues to be a challenge.
Lack of time, not enjoying exercise, and not knowing how to exercise continue to be commonly cited barriers for people with osteoporosis to engage in exercise and physical activity.6,7 To better understand their exercise preferences, a survey of nearly 300 participants was conducted and found that people with osteoporosis prefer to exercise in small groups, doing activities that are easy to perform and easy to remember.6
Exercise guidelines suggest that people with osteoporosis should engage in a multicomponent exercise program that includes resistance and balance training.4 People with osteoporosis, especially those who have had a vertebral fracture, should seek assistance from a physical therapist to ensure safe and appropriate exercise.4 Although evidence has shown benefit to a multicomponent exercise in people with an osteoporotic vertebral fracture,8–10 it’s not clear whether a group exercise could be implemented in people with osteoporosis, within a private, outpatient physiotherapy clinic. Within Canada, there is an unmet need of providing specialized physiotherapy and exercise training to people with osteoporosis, despite a post graduate training program for healthcare professionals to learn how to teach safe exercise to people with osteoporosis. BoneFitTM is the training program for healthcare professionals, training a wide variety of healthcare professionals including physical therapists, kinesiologists, yoga instructors, and group fitness instructors, among others. BoneFitTM provides knowledge and resources to healthcare professionals but does not provide a specific exercise program. It is dependent on the trained professionals to develop the program to fit the needs of their community. Another challenge in having people with osteoporosis engage in physiotherapy treatment is the financial burden associated with physiotherapy treatment. A group physiotherapy session can be offered at a reduced rate for the patient thereby increasing financial accessibility to specialized services.
Despite strong evidence supporting exercise for osteoporosis management, translation into private outpatient clinics has been limited. Implementation challenges include variable reimbursement structures, competing clinical priorities, and the need for staff with specialized training in osteoporosis management. Many private practices operate under fee-for-service models that prioritize billable one-on-one care, making it difficult to integrate group or education-based programs. In addition, sustaining such programs requires consistent referral pathways, administrative support, and ongoing patient demand—all of which may fluctuate over time.11 Applying an implementation science framework enables identification of these multi-level barriers and supports strategies for program adaptation, clinician engagement, and long-term sustainability.12
Within the community, there is a need to deliver exercises to people with osteoporosis, that is safe and increases access to a physiotherapy-based program. A small group exercise class would address many barriers expressed by people with osteoporosis and address the exercise preferences described in previous studies. The purpose of this project was to design and develop a group physiotherapy class for people with compromised bone mineral density and at risk of falling. Secondarily, determine whether the class could be implemented into a private outpatient physiotherapy clinic. Thirdly, to determine if the program could change strength, balance and posture in the participants, compared to baseline. It is hypothesized that a small group exercise program for people with compromised bone mineral density is suitable and appropriate for implementation in an outpatient physiotherapy clinic.
Methods
Study Design
This was single-arm feasibility/implementation study without a control group of people with self-reported compromised bone mineral density and at fall risk, engaging in a group physiotherapy exercise class. Participants were recruited from the community through physicians at a geriatric specialty clinic, an endocrinology specialty clinic and through advertisements in community centers.
Participants completed the outcome measures at their initial assessment visit, at baseline and at their discharge assessment visit at 6 weeks. At the 6-week time point participants were also asked to complete a feedback form to provide written feedback on the program.
Implementation Framework
This study uses the knowledge-to-action framework and was carried out in three phases to meet the objectives of the study and respect the steps of the knowledge-to-action framework.13–15 See Figure 1 for a summary of the process.
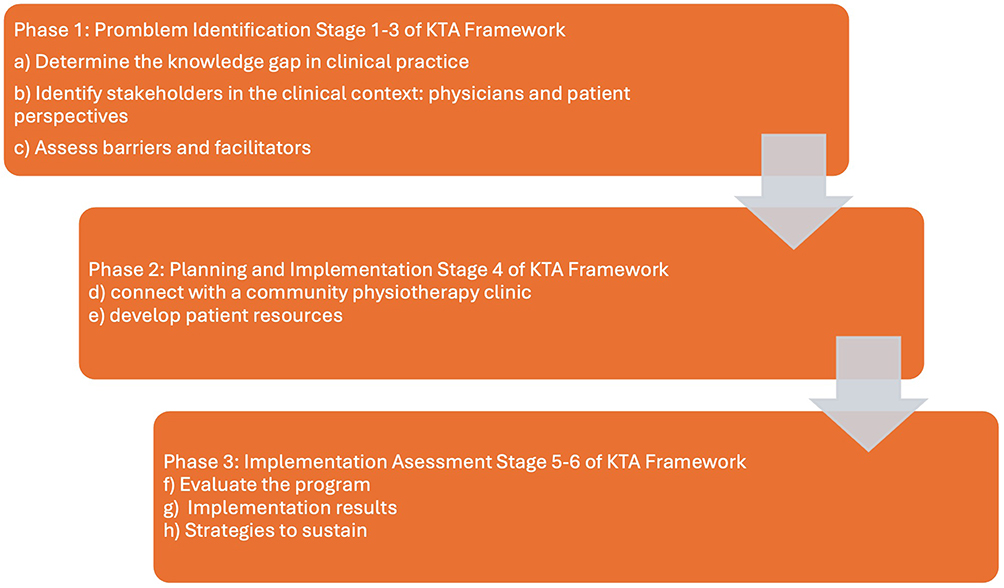 |
Figure 1 Flow chart of phases of program development and implementation into a private practice physiotherapy clinic. |
Phase 1: Problem Identification
Previous work has been conducted by the lead author to understand the barriers and facilitators to engaging in exercise for people with osteoporosis and healthcare providers.6,7,16–18 In a survey of nearly 300 people with osteoporosis, the participants identified that they preferred exercise supervised by a health care professional and support from their peers. Participants ultimately preferred to exercise at home, and on their own time, but wanted to learn how to do the exercises safely first.6
In further consultation with patients and physicians in the community, it was clear there was a need for a group exercise class for people with osteoporosis. Patients wanted somewhere they could learn how to exercise safely for someone with osteoporosis, and physicians wanted a location to refer their patients.
Phase 2: Planning and Implementation
A partnership and collaboration with a local physiotherapy clinic led to the design of a group exercise class for people with osteoporosis, led by a BoneFitTM trained physiotherapist. The program was designed with the movement principles recommended for people with osteoporosis, which included careful consideration of alignment during all exercises, postural re-training, training of the back extensor muscles, and an emphasis on strength, balance, and functional training, which aligned with the current osteoporosis guidelines.
Acknowledging that participants wanted a resource to be able to exercise at home and on their own time, an exercise booklet was created to remind the participants of key educational principles of osteoporosis, and a picture and word description, in English, of the exercises taught in the exercise class. The booklet was designed to support the patient in their management of osteoporosis.
The criteria for success were:
- Enrolment—8 participants enrolled in each cohort offering, 4 cohorts offered throughout the year.
- Feedback—receive feedback from the participants on whether they enjoyed the program and what could be improved.
Phase 3: Implementation Assessment
A small group of participants were invited to participate in a first iteration of the exercise program. Six community dwelling older adults, age ranging from 61 to 83 participated in the twice weekly, 6-week, in person group exercise class. At the end of the six-week program, we sought written feedback from the participants. Participants were asked to complete a program feedback form to offer their feedback on the program. All feedback was analyzed using qualitative thematic analyses with an interpretive descriptive approach.19 Overall, the feedback was positive. The participants enjoyed the instructor, the exercises, the different levels of exercises to account for personalization within the program and learning about osteoporosis. The participants provided feedback that the balance exercises should be integrated within the program, instead of at the end of class. The participants felt that having the balance exercises at the end of the class de-emphasized the importance of balance for people with osteoporosis. The participants also wanted more tactile feedback on their form. The instructor had provided significant verbal feedback, but the participants felt that they learned better from tactile cueing. Finally, the participants overall liked the booklet that was provided to them, but the first version of the booklet did not have pictures for all the exercises, and the participants commented that they would like to have pictures to facilitate their at-home implementation of the exercise program. The feedback was applied to future exercise classes. Written and verbal feedback was sought at the end of each 6-week session.
Study Sample
Participants were recruited from the community through poster advertisement and through referrals from a local endocrinologist and geriatrician to participate in a six-week, in-person, small group physiotherapy class. Participants were included if they had compromised bone mineral density and/or were at an increased risk of falling and/or over the age of 50, as determined by the referring physician. Due to the pragmatic nature of the program, the inclusion criteria remained broad. Participants were excluded if they were not independently ambulatory, could not understand English or if they had any contraindications to exercise.
Participants were asked to sign a written consent form to participate in this research study. This study was approved by the Western University Health Sciences Research Ethics Board in October 2023. This study complies with the Declaration of Helsinki.
Study Setting
This study took place in an outpatient private practice physiotherapy clinic.
Intervention
Participants were enrolled in a 6 week, twice weekly, 60-minute exercise intervention that targeting whole body strength and balance. The group exercise class had a capacity of 8–10 participants, led by a BoneFitTM trained physiotherapist and supported by a kinesiology-graduate volunteer. Eight exercises were included: two exercises targeting core, one for the back extensors, three lower extremity, two upper extremity exercises, and balance exercises. There are three levels to each of the exercises, with increasing levels of difficulty. For example, one is an upper extremity horizonal pushing exercise, to support many functional tasks such as pushing a grocery cart. The easiest version is to have the participant supine on the ground using a resistance band to perform a chest press, the second version of the exercise is to increase the weight by using dumbbells, and the third version of the exercise is to do a push-up, which could be modified to ease into the progression by having the hands elevated or knees on the ground. Progressing through the exercises is dictated by the lead physiotherapist’s assessment of form, quality of the movement, and the participant’s rating of perceived exertion. Participants are encouraged to challenge themselves but while working within their physical limits. All exercises were prescribed at a rep range of 8–15 repetitions for 2–4 sets. Exercises were progressed and intensity was increased when participants and the instructor felt that they could comfortably complete 15 repetitions with good from. All exercises are monitored to encourage best spinal alignment for the patient and to avoid movements that are known to increase the risk of fracturing such as repetitive weighted spinal flexion.
Outcome Measures
Participants received an initial assessment and discharge assessment at the start and end of the 6-week program, respectively. The assessment included a subjective history, and objective assessment of lower body functional strength, as assessed by the 30-second sit to stand, upper body strength as assessed by grip strength, static balance as assessed by single leg stance, dynamic balance as assessed by the four-square balance test, and posture as assessed by the occiput to wall distance (OWD). The outcome measures were selected to align with previous studies,20,21 and to ensure evaluation of lower extremity muscular endurance, upper extremity strength, posture, and balance, all of which are important functional outcomes for people with osteoporosis.
Sample Size Estimation
A total of 45 participants was appropriate for this study design. The sample size was based on a two-tailed paired t-test with a significance of 0.05 and a medium effect size, and a power of 0.8, aligning with grip strength as a primary outcome measure.22 The sample size calculation suggested that 34 participants would be sufficient to achieve a power of 0.8. A sample of 45 participants will achieve a power of 0.9.
Statistical Analysis
The quantitative variables are presented as means and standard deviation and the qualitative variables as numbers and percentages. A students paired t-test will be used to determine the pre and post intervention. A p value of 0.05 will be considered statistically significant. An effect size was used to show the within group effects from baseline to 6-weeks in: 30 second sit to stand, grip strength, OWD, single leg stance, and the 4-square balance test. Using t-shirt effect size a small effect is anything <0.2; a moderate effect is between 0.2 and 0.7 and a large effect is >0.7. All statistical analyses were conducted using SPSS version 24 (SPSS Inc., Chicago, IL, USA). Clinical significance is also be considered. For grip strength, a 5.0 kg change is considered clinically significant.23 For single leg stance, a minimally clinically important change is considered 24 seconds.24 A change of 2 repetitions is considered clinically important in the 30-second sit to stand test.25 An improvement of an OWD to less than 5 cm is considered clinically important.26 The requisite assumptions were evaluated and judged to be acceptable.
Results
Evaluation of Implementation
The program was evaluated through written and verbal feedback. Several participants mentioned that the space constraints of the clinic made a 10-person class feel too crowded. Therefore, in future iterations of the program, the class capacity will be 8 people. All the participants said that they enjoyed the class, the instructor, and the exercises. They liked having a booklet to support their continued exercise once the class was over, however they wanted pictures to support their understanding of each of the exercises. Pictures were added to each exercise in future iterations. All the participants highlighted the benefits of the social aspect of the class and really enjoyed engaging in exercise with their peers. Several participants mentioned that they enjoyed the class format but would like a community program to attend after the physiotherapist led class. One participant had to withdraw from the program because the class times no longer worked for her schedule.
Participant Characteristics
A total of 43 participants signed a letter of information and consent form to access their data for research purposes. A total of 45 individuals were approached for in the study but two did not consent. The mean age of the participants was 72 (SD: 6.03, min 60 years, max 84 years). There were 2 males that enrolled in the program and 42 females enrolled, but 41 females that signed the consent form to provide access to their assessment and discharge data. One participant reported a fall but reported it was unrelated to the intervention (she fell off her chair at home). No participants reported any fractures.
Outcome Assessment
See Table 1 for a summary of the outcomes assessed. Grip strength, posture, single leg stance bilaterally, the four-square balance test, and the 30 second sit to stand improved significantly from baseline to the follow up (Table 1). There were statistically significant improvements in 30 second sit to stand, grip strength bilaterally, OWD, single leg stance on the left, and four-square balance test. There was not a statistically significant improvement in single leg stance on the right. Clinically, only the 30 second sit to stand improved meaningfully, according to the a priori criterion. There was a mean increase of 3 repetitions from baseline to the 6-week follow-up assessment. Grip strength improved on both sides by an average of approximately 1.5 kg. Posture improved by an average of 0.7 cm from baseline to the 6 week follow up. Single leg stance improved by an average of 5 seconds on the leg and by approximately 1 second on the right. The four-square balance test marks an improvement if the time decreases and there was an average decrease of 1 second for that test.
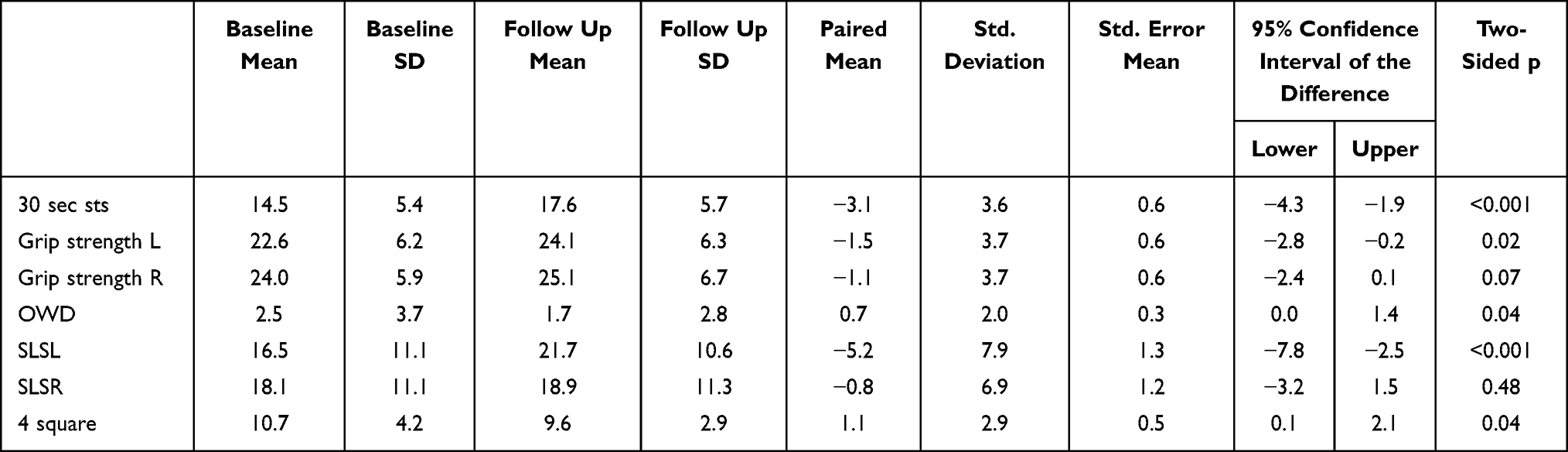 |
Table 1 Mean Difference Between Baseline and Follow Up of the Outcome Assessments |
Table 2 presents the effect size for the outcome measures. There was a large effect size for the 30 second sit to stand and the single leg stance on the left. There was a moderate effect for the grip strength on both sides, OWD and the 4-square balance test. There was a small effect for single leg stance on the right.
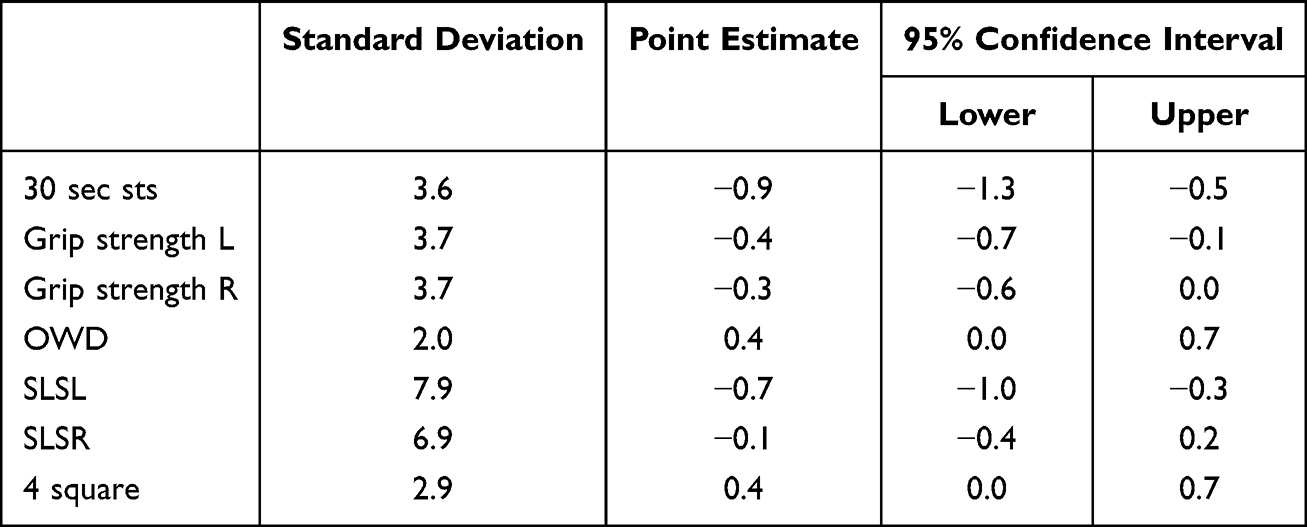 |
Table 2 Effect Size of the Mean Difference Between the Baseline and Follow Up of the Outcome Assessments |
Discussion
This study aimed to implement a physiotherapy led group exercise class for people with compromised bone mineral density and at fall risk. The first phase of the study was to develop the program, which included surveying participants on their preference for exercise,6 then consulting with physicians and patient partners to develop the program. Partnership with a community outpatient physiotherapy clinic and receiving ongoing feedback from patients was essential. Overall, the program was well received and showed functional and statistically significant improvements in strength, balance, and posture after the 6-week program. However, 30 second sit to stand was the only test to show a clinical improvement. It is unclear why the 30-second sit to stand was the only outcome measure that showed clinical improvement; however, one suggestion is that it mostly closely aligned with an exercise in the program, which is the sit-to-stand/squat. It is possible that a longer intervention or longer follow up would have showed clinical improvement in the results which needs to be explored in future iterations of the program. Ultimately, the program aligned with the aims of the study and should be implemented in other outpatient clinics.
Aligning with the guidance on how to develop interventions to improve healthcare, this study followed the development suggestions.27 After the implementation of the program, it is important to continue to monitor short-term and long-term effects of the key outcomes. Ongoing monitoring of adherence to exercise post-intervention and whether the physical benefits are retained would be a necessary next step. The short-term effects include whether the intervention remains relevant, acceptable, feasible, engaging, and if it transfers to other settings.27 Similarly, ongoing monitoring of enrolment to confirm that the program remains engaging, acceptable and continues to be responsive to feedback from participants, while ensuring the program is relevant and acceptable. Long term effects described by the guidance on how to develop interventions to improve healthcare include effectiveness to participants and referral sources, economical for clinic implementation and participants, improving health outcomes, sustainability and reduces research waste.27 The long-term effects for the current program will continue to monitor patient outcome. Future studies will need to evaluate the referral sources and also evaluate who is enrolling in the program to ensure the program is accessible to all individuals that would benefit from the program.28,29
The physical outcome measures in the current study align well with previous literature demonstrating an improvement in strength after an exercise program in people with osteoporosis. In a randomized controlled trial looking at a home-resistance training program, in people with osteoporosis aged 60–80, there were statically significant improvements in the five times sit-to-stand (MD: −1.13 s, 95% CI −1.18 to −1.08 s), and hand grip (MD: 1.29 kg, 95% CI 1.18 to 1.39 kg) outcomes,30 which align with the outcome assessed in the current study. Another study looked at a 12-week exercise program found functional and statistically significant improvements at 12 weeks in timed up and go test, the sit to stand test and the one leg stance test. Once again, these findings align with the current study suggesting that the six-week group physiotherapy program has similar outcomes to a 12-week supervised exercise program. Previous literature was looking at the same population of people with osteoporosis between the age of 60–80 indicating that this population is responsive to a group physiotherapy program and can demonstrate strength improvements in 6 weeks.
The current study looked at OWD as a proxy measure for posture. There was a moderate effect and a statistically significant improvement in OWD from baseline to 6 week follow up, which was a surprising finding given the short length of the intervention. Improving posture is an important outcome for people with osteoporosis as posture can contribute to fall risk,31 vertebral fracture risk32 and poor physical function.33,34 However, these results do align with the literature. A systematic review was conducted in 2014 which found an improvement in at least one measure of posture after an exercise intervention.35 Only one of the studies in the review used OWD as an outcome measure and also found a statistically significant improvement in OWD after a twice weekly, 12-week resistance training program.36 One of the primary studies within the systematic review found a statistically significant improvement in the tragus to wall distance after a yoga-intervention.37 The current program did not include yoga-type exercises, but a post-strength training stretch may further improve the participant’s posture.
Overall, this study presented positive results in strength, balance and posture after a 6-week group exercise program for people with compromised bone mineral density and at an increased risk of falling. These outcomes are promising for people with osteoporosis. The literature is clear that a multifaceted exercise program is beneficial for people with osteoporosis.10,38 One study looked at a community exercise program for people with osteoporosis and found benefits to improving strength, balance and reducing fall risk.39 Future studies will need to evaluate patient preferences and patient confidence in performing further exercise. Ongoing work needs to evaluate adherence to exercise long term, and whether a group exercise class facilitates participant engagement. Further, it is necessary to evaluate whether a 6-week program is sufficient to engage people in an exercise program and encourage their continued participation in exercise post-intervention.
The implementation and sustainability of the program seem promising. The program was integrated into the daily operations of the private practice physiotherapy clinic. The patients were charged a small fee to participate in the program, which covered operational costs, again supporting the sustainability of the program. However, future work will have to consider expanding the program to other sites, a larger sample side and a waitlist control group to determine the effectiveness of the program on clinical, physical, and patient important outcomes.
Strengths and Limitations
This study demonstrated positive outcomes after a small group exercise class for people with compromised bone mineral density and at fall risk, led by a physiotherapist. A strength of this study is the systematic process to design and implement the program. This study received feedback from patient partners and clinicians. A major limitation of this study is that it did not contain a control group, therefore results need to be interpreted with caution. The program is currently only being offered at one clinic, and the implementation may not be suitable in other facilitates. Accessibility, mainly a fee associated with attending the program, and diversity of the participants in the program is a potential limitation and may not translate to other communities or lower-income individuals. Further this study was in community dwelling adults and may not be translatable to the variable severity and functional abilities of people with osteoporosis.
Conclusion
In conclusion, a structured, patient-informed group program is a feasible and promising model for delivering essential exercise intervention to this population in a real-world clinical setting. The knowledge-to-action framework was successfully applied to support the design, development and implementation of a small group physiotherapy program. Clinician and patient partner feedback ensured successful uptake of the program in the outpatient physiotherapy clinic setting. Preliminary analyses were conducted to evaluate the outcomes of the exercise program, which showed promise. Future studies should evaluate the accessibility and diversity of a group physiotherapy program for people with compromised bone mineral density, to ensure improved access to essential care for people with osteoporosis.
Significance/Implications
- A physiotherapy led exercise program for people with osteoporosis or at risk of developing osteoporosis is well-implemented into a physiotherapy clinic.
- Patients demonstrated an increase in strength and balance.
- Future studies should evaluate diversity and accessibility of physiotherapy led group exercise programs.
Funding
No funding was received.
Disclosure
No potential competing interest was reported by the author(s).
References
1. Howe TE, Shea B, Dawson LJ, et al. Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane Database Syst Rev. 2011;2011(7):CD000333. doi:10.1002/14651858.CD000333.pub2
2. Vieira ER, Palmer RC, Chaves PH. Prevention of falls in older people living in the community. BMJ. 2016;353:i1419. doi:10.1136/bmj.i1419
3. Giangregorio L, McGill S, Wark J, et al. Too Fit To Fracture: outcomes of a Delphi consensus process on physical activity and exercise recommendations for adults with osteoporosis with or without vertebral fractures. Osteoporos Int. 2015;26(3):891–10. doi:10.1007/s00198-014-2881-4
4. Giangregorio L, Papaioannou A, Macintyre N, et al. Too fit to fracture: exercise recommendations for individuals with osteoporosis or osteoporotic vertebral fracture. Osteoporos Int. 2014;25(3):821–835. doi:10.1007/s00198-013-2523-2
5. Morin SN, Feldman S, Funnell L, et al. Clinical practice guideline for management of osteoporosis and fracture prevention in Canada: 2023 update. CMAJ. 2023;195(39):E1333–E48. doi:10.1503/cmaj.221647
6. Ziebart C, Bryant D, Szekeres M. Exercise preferences for people with osteoporosis, identifying barriers, facilitators, needs and goals of exercise. J Osteopor Phys Act. 2020;8:1–7.
7. Ziebart C, McArthur C, Lee L, et al. “Left to my own devices, I don’t know”: using theory and patient-reported barriers to move from physical activity recommendations to practice. Osteoporos Int. 2018;29(5):1081–1091. doi:10.1007/s00198-018-4390-3
8. Bergland A, Thorsen H, Kåresen R. Effect of exercise on mobility, balance, and health-related quality of life in osteoporotic women with a history of vertebral fracture: a randomized, controlled trial. Osteoporos Int. 2011;22:1863–1871. doi:10.1007/s00198-010-1435-7
9. Olsen C, Bergland A. The effect of exercise and education on fear of falling in elderly women with osteoporosis and a history of vertebral fracture: results of a randomized controlled trial. Osteoporos Int. 2014;25:2017–2025. doi:10.1007/s00198-014-2724-3
10. Stanghelle B, Bentzen H, Giangregorio L, Pripp A, Skelton DA, Bergland A. Effects of a resistance and balance exercise programme on physical fitness, health-related quality of life and fear of falling in older women with osteoporosis and vertebral fracture: a randomized controlled trial. Osteoporos Int. 2020;31:1069–1078. doi:10.1007/s00198-019-05256-4
11. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50. doi:10.1186/1748-5908-4-50
12. Proctor EK, Powell BJ, McMillen JC. Implementation strategies: recommendations for specifying and reporting. Implement Sci. 2013;8(1):139. doi:10.1186/1748-5908-8-139
13. Torres CP, Mendes FJ, Barbieri-Figueiredo M. Use of “The Knowledge-to-Action Framework” for the implementation of evidence-based nursing in child and family care: study protocol. PLoS One. 2023;18(3):e0283656. doi:10.1371/journal.pone.0283656
14. Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: time for a map? J Contin Educ Health Prof. 2006;26(1):13–24. doi:10.1002/chp.47
15. Graham ID, Tetroe JM. The knowledge to action framework. In: Models and Frameworks for Implementing Evidence-Based Practice. Vol. 207. 2010:222.
16. McArthur C, Ziebart C, Papaioannou A, et al. “We get them up, moving, and out the door. How do we get them to do what is recommended?” Using behaviour change theory to put exercise evidence into action for rehabilitation professionals. Arch Osteoporos. 2018;13(1):1–10. doi:10.1007/s11657-018-0419-7
17. Ziebart C, MacDermid J, Furtado R, et al. An interpretive descriptive approach of patients with osteoporosis and integrating osteoporosis management advice into their lifestyle. Int J Qual Stud Health Well-Being. 2022;17(1):2070976. doi:10.1080/17482631.2022.2070976
18. Ziebart C, MacDermid J, Furtado R, Szekeres M, Suh N, Khan A. An interpretive descriptive approach to understanding osteoporosis management from the perspective of people at risk of fracturing. Patient Prefer Adherence. 2022;16:1673–1686. doi:10.2147/PPA.S366781
19. Thorne S, Kirkham SR, MacDonald‐Emes J. Interpretive description: a noncategorical qualitative alternative for developing nursing knowledge. Res Nurs Health. 1997;20(2):169–177. doi:10.1002/(SICI)1098-240X(199704)20:2<169::AID-NUR9>3.0.CO;2-I
20. Ziebart C, MacDermid J, Bryant D, Szekeres M, Suh N. Hands-Up program: protocol for a feasibility randomised controlled trial of a combined 6-week exercise and education intervention in adults aged 50–65 with a distal radius fracture. BMJ open. 2021;11(7):e046122. doi:10.1136/bmjopen-2020-046122
21. Giangregorio LM, Gibbs JC, Templeton JA, et al. Build better bones with exercise (B3E pilot trial): results of a feasibility study of a multicenter randomized controlled trial of 12 months of home exercise in older women with vertebral fracture. Osteoporos Int. 2018;29(11):2545–2556. doi:10.1007/s00198-018-4652-0
22. Kim JK, Park MG, Shin SJ. What is the minimum clinically important difference in grip strength? Clin Orthop Relat Res. 2014;472(8):2536–2541. doi:10.1007/s11999-014-3666-y
23. Bohannon RW. Minimal clinically important difference for grip strength: a systematic review. J Phys Ther Sci. 2019;31(1):75–78. doi:10.1589/jpts.31.75
24. Goldberg A, Casby A, Wasielewski M. Minimum detectable change for single-leg-stance-time in older adults. Gait Posture. 2011;33(4):737–739. doi:10.1016/j.gaitpost.2011.02.020
25. Wright AA, Cook CE, Baxter GD, Dockerty JD, Abbott JH. A comparison of 3 methodological approaches to defining major clinically important improvement of 4 performance measures in patients with Hip osteoarthritis. J Orthop Sports Phys Ther. 2011;41(5):319–327. doi:10.2519/jospt.2011.3515
26. Wiyanad A, Thaweewannakij T, Wattanapan P, Sooknuan T, Mato AP, Amatachaya P, editors. Appropriate Occiput-wall Distance to screen for a risk of kyphosis. In:
27. O’Cathain A, Croot L, Duncan E, et al. Guidance on how to develop complex interventions to improve health and healthcare. BMJ open. 2019;9(8):e029954. doi:10.1136/bmjopen-2019-029954
28. Greenhalgh T, Hinton L, Finlay T, et al. Frameworks for supporting patient and public involvement in research: systematic review and co‐design pilot. Health Expect. 2019;22(4):785–801. doi:10.1111/hex.12888
29. Lunny C, Zarin W, Chaudhry S, et al. An inclusive and diverse governance structure of the strategy for patient-oriented research (SPOR) Evidence Alliance. FACETS. 2022;7(1):435–447. doi:10.1139/facets-2021-0129
30. Zhang F, Wang Z, Su H, et al. Effect of a home-based resistance exercise program in elderly participants with osteoporosis: a randomized controlled trial. Osteoporos Int. 2022;33(9):1937–1947. doi:10.1007/s00198-022-06456-1
31. Kado DM, Huang M-H, Nguyen CB, Barrett-Connor E, Greendale GA. Hyperkyphotic posture and risk of injurious falls in older persons: the Rancho Bernardo Study. J Gerontol a Biol Sci Med Sci. 2007;62(6):652–657. doi:10.1093/gerona/62.6.652
32. Shipe NK, Billek-Sawhney B, Canter TA, Meals DJ, Nestler JM, Stumpff JL. The intra-and inter-rater reliability of the tragus wall distance (TWD) measurement in non-pathological participants ages 18–34. Physiother Theory Pract. 2013;29(4):328–334. doi:10.3109/09593985.2012.727528
33. Liu-Ambrose T, Eng JJ, Khan KM, Carter ND, McKay HA. Older women with osteoporosis have increased postural sway and weaker quadriceps strength than counterparts with normal bone mass: overlooked determinants of fracture risk? J Gerontol a Biol Sci Med Sci. 2003;58(9):M862–M6. doi:10.1093/gerona/58.9.M862
34. Ziebart C, Adachi JD, Ashe MC, et al. Exploring the association between number, severity, location of fracture, and occiput-to-wall distance. Arch Osteoporos. 2019;14(1):1–8.
35. Bansal S, Katzman WB, Giangregorio LM. Exercise for improving age-related hyperkyphotic posture: a systematic review. Arch Phys Med Rehabil. 2014;95(1):129–140. doi:10.1016/j.apmr.2013.06.022
36. Benedetti MG, Berti L, Presti C, Frizziero A, Giannini S. Effects of an adapted physical activity program in a group of elderly subjects with flexed posture: clinical and instrumental assessment. J Neuroeng Rehabil. 2008;5:1–11. doi:10.1186/1743-0003-5-32
37. Greendale GA, McDivit A, Carpenter A, Seeger L, Huang M-H. Yoga for women with hyperkyphosis: results of a pilot study. Am J Public Health. 2002;92(10):1611–1614. doi:10.2105/AJPH.92.10.1611
38. Jensen AL, Wind G, Langdahl BL, Lomborg K. The impact of multifaceted osteoporosis group education on patients’ decision-making regarding treatment options and lifestyle changes. J Osteoporos. 2018;2018:1–10. doi:10.1155/2018/9703602
39. Carter ND, Khan KM, McKay HA, et al. Community-based exercise program reduces risk factors for falls in 65-to 75-year-old women with osteoporosis: randomized controlled trial. CMAJ. 2002;167(9):997–1004.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Obstacles to the Early Diagnosis and Management of Sarcopenia: Current Perspectives
Ooi H, Welch C
Clinical Interventions in Aging 2024, 19:323-332
Published Date: 20 February 2024
An Effectiveness Trial of an Exercise Physiologist Service to Improve Quality of Life in Adults with Severe Mental Illness: Protocol for the MOVEMENT Study
Chapman JJ, Siskind D, Yung AR, Lee YY, Arnautovska U, Scott JG, Burke K, Malacova E, Korman N, Wyder M, Doohan MA, Keating SE, Parker S, Walker ME, Hu D, O’Brien J, Lau G, Pratt GF, Rosenbaum S, Curtis J, Chatterton ML, Simmons L, Wheeler AJ
Neuropsychiatric Disease and Treatment 2025, 21:1399-1408
Published Date: 11 July 2025