Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Implementation of Electronic Medical Record Template Improves Screening for Complications in Children with Type 1 Diabetes Mellitus
Authors Choudhary D, Brown B, Khawar N, Narula P, Agdere L
Received 9 October 2019
Accepted for publication 17 June 2020
Published 9 July 2020 Volume 2020:11 Pages 219—223
DOI https://doi.org/10.2147/PHMT.S233998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Deepak Choudhary,1 Brande Brown,2 Nayaab Khawar,2 Pramod Narula,2 Levon Agdere2
1Department of Pediatrics Emergency Medicine, University of Arkansas for Medical Sciences, Arkansas Children’s Hospital, Little Rock, AR 72202, USA; 2New York-Presbyterian Brooklyn Methodist Hospital, Brooklyn, NY 11215, USA
Correspondence: Brande Brown
New York-Presbyterian Brooklyn Methodist Hospital, 506 6th Street, Brooklyn, NY 11215, USA
Tel +1 718-780-5260
Email [email protected]
Objective: Health professionals and patients should follow comprehensive screening guidelines to recognize early signs of long-term complications for insulin-dependent type 1 diabetes mellitus (T1DM). The aim of this study is to demonstrate that utilization of electronic medical record (EMR) templates for diabetes management improves adherence to International Society for Pediatric and Adolescent Diabetes (ISPAD) screening guidelines.
Methods: All patients with T1DM who were seen in the outpatient pediatric endocrine clinic (age 0– 22 years old) at an urban community-based community hospital during the 2014 calendar year were enrolled in the study (n=49). A retrospective chart review was performed and audited against ISPAD guidelines. An EMR template and order set was then created based on ISPAD screening guidelines with the aim of improving compliance. The templates were implemented in 2015 (initial phase) and 2016 (maintenance phase) and these data were compared to baseline data. A chi-squared test was performed to analyze the differences between the data using SAS version 9.4 (SAS Institute, Inc). A p-value less than 0.05 was considered significant.
Results: Significant improvements (p< 0.05) in screening guideline adherence from baseline to maintenance phase data were found for annual retinopathy (0% to 45%) and neuropathic foot (0% to 64%) exams, screening for microalbuminuria (49% to 79%), celiac disease (6% to 81%), lipids (63% to 86%), and basic metabolic panel (69% to 88%). Of note, thyroid function testing was also increased, but was not statistically significant between the years.
Conclusion: The utilization of EMR templates and order sets for T1DM are valuable tools to aid medical providers in adhering to ISPAD screening guideline.
Keywords: type 1 diabetes, electronic medical record, screening tool, disease management, chronic disease, benchmarking, quality improvement, pediatrics, standardized documentation
Introduction
The prevalence of T1DM among children and adolescence has increased 21.1% from 2001 (1.48 per 1000) to 2009 (1.93 per 1000), with the highest prevalence occurring in Caucasians and the lowest in American Indians.1 According to the Diabetes Control and Complication trial, the reduction in HbA1C from 9.8% to 8.1% could reduce the risk of complications including non-proliferative retinopathy by 63%, clinical neuropathy by 60%, and microalbuminuria by 54%.2 Microvascular and macrovascular complications are also more likely to start sooner when HbA1C levels are higher than target values.3–5 Even with the potential reduction in complications, studies have shown that the majority of children and adolescents with T1DM are not meeting target HbA1C recommendations as per the American Diabetes Association guidelines. Among SEARCH for Diabetes in Youth study participants, 95% reported having their blood pressure checked at all or most visits, 88% had lipid levels checked, 83% had kidney function tested, 68% received HbA1C testing, and 66% received an eye examination.6,7 In a children’s hospital in the New York only 35% of the participants diagnosed with diabetes were referred for eye exams.8 In a study by Wood at al, adolescents and children with type 1 diabetes were found to be mostly noncompliant with the ADA guidelines.9
Follow-up appointment adherence is also an important factor in achieving a target HbA1C and compliance with screening.10 A study of over 1,000 children (0–17 years old) with T1DM found that patients who missed two or more appointments were three times more likely to have had diabetic ketoacidosis (DKA) and HbA1C levels greater than or equal to 8.5% as compared to those who missed no appointments.10 A study by Stumetz et al revealed that participants from rural environments were less adherent to appointments and provider communication than participants from urban environments.11 Ethnicity and socioeconomic indicators also demonstrate a role in compliance with screening, as one study showed the odds of screening for diabetic retinopathy being lower in black children and in those with poorer diabetes control.12
Medical provider compliance in adhering to screening guidelines is essential to reduce the acute and chronic complications associated with T1DM. Before the implementation of this study, practitioners in our pediatric endocrine clinic did not follow a standardized protocol, with screening per ISPAD guidelines reliant on clinician preference. The purpose of this study was to create and implement an EMR template and order set for pediatric patients with T1DM in order to increase compliance with ISPAD complication screening guidelines.13
Methods
All patients with T1DM who were seen in an urban community-based outpatient pediatric endocrine clinic during the 2014 calendar year were enrolled in the study (n=49) (Table 1). The baseline population consisted of 27 female and 22 male participants. Patients of age from birth to 22 years of age were included in this study (Median age = 15 years, Average age = 14.06 years). The overall age distribution consisted of 43% of children birth to 12, 45% 13 to 17 year old, and 12% of those 18 to 21 years old.
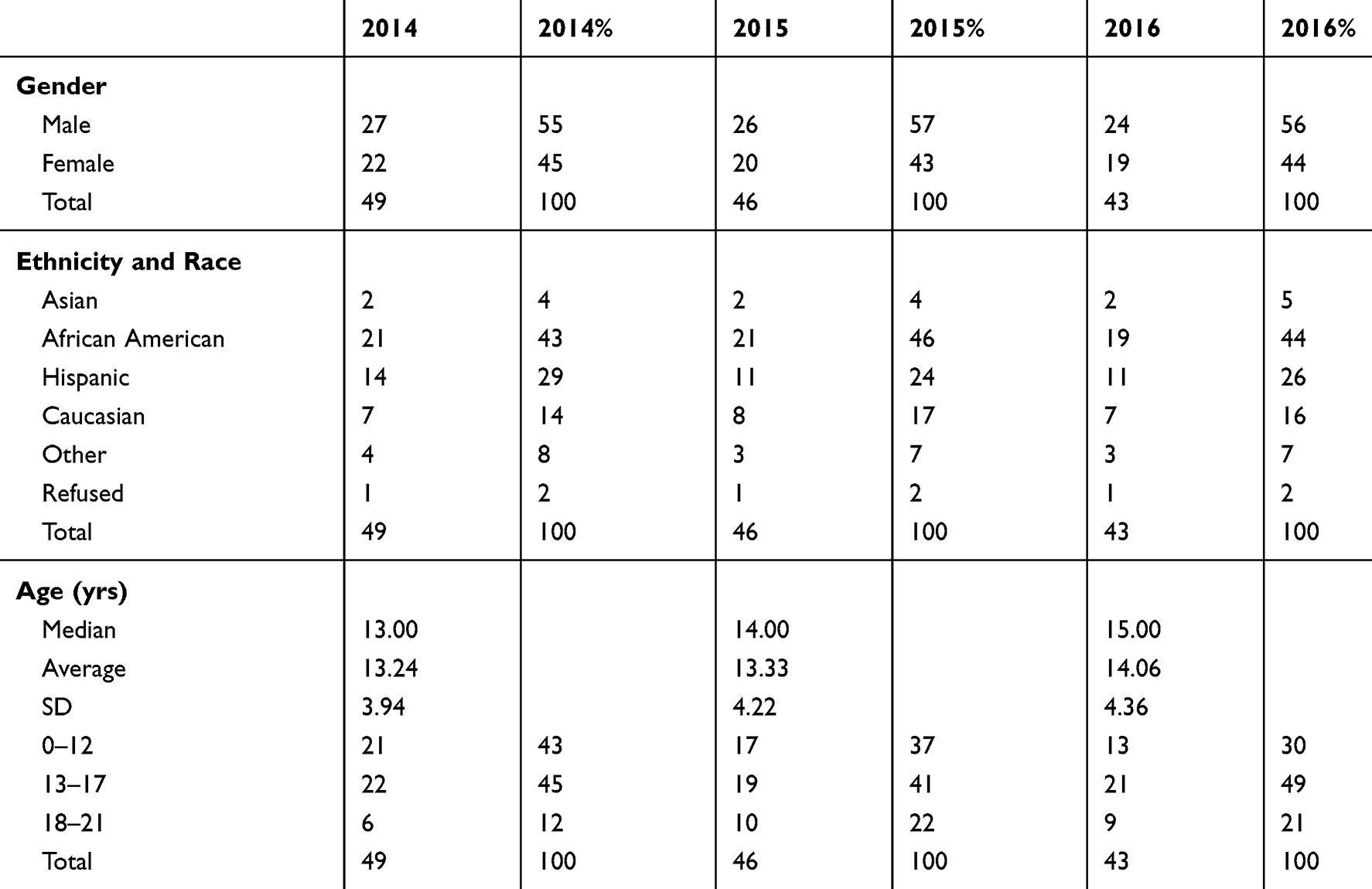 |
Table 1 Study Population |
To provide baseline data, diabetes screening compliance during the clinic visits was audited against ISPAD screening guidelines for these patients. An EMR template was then created and implemented for the pediatric diabetic clinic which included the date of diagnosis, insulin regimen, HbA1C, blood glucose readings, recent illnesses, hypoglycemic episodes, social history, physical exam including blood pressure, lipodystrophy, foot examination, dietary, psychological assessment, and management plan. An order set was also created to include thyroid function tests, celiac panel, hemoglobin A1C, BMP (sodium, potassium, chloride, bicarbonate, blood urea nitrogen, creatinine, glucose), lipid profile and urine microalbumin. After implementation of the EMR template and order set, 2015 data were collected for the initial phase of the study (n = 46) and compared to baseline data (n=49). Maintenance data were collected for the 2016 calendar year (n=43) and also compared to baseline data (Figure 1). A chi-squared test was performed to analyze the differences between the data using SAS version 9.4 (SAS Institute, Inc). A p-value less than 0.05 was considered significant. Of note, 6 patients were dropped from the study due to either aging out of the pediatric clinic (>22 years old), transferring care to a different endocrinology clinic location, or were lost to follow up. This study was approved by the New York Presbyterian Brooklyn Methodist Hospital Institutional Review Board. A waiver of informed consent was obtained, all patient data were maintained with confidentiality and compliance with the Declaration of Helsinki.
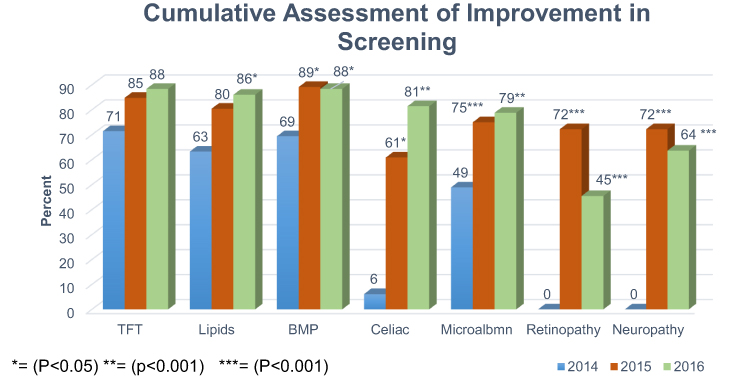 |
Figure 1 Cumulative assessment of improvement in screening. |
Results
Results demonstrate that the use of an electronic medical record template improved compliance with diabetes complication screening guidelines for multiple clinical measures (Figure 1). Basic metabolic panel screening increased from baseline to 2015 (89%, p= 0.024) and maintained significance in 2016 (88%, p=0.042). Compliance for celiac screenings increased from baseline to 2015 (61%, p=0.001) and 2016 (81%, p=0.001). Microalbuminuria screening compliance also increased from baseline to 2015 (59%, p=0.023) as well as 2016 (79%, p=0.009). Although annual retinopathy examinations showed significant improvements from baseline to 2015 and 2016, there was a slight decrease in screening compliance within those years (2015: 72%, p=0.001, 2016: 45%, p=0.001). This trend was also seen in neuropathic foot examination screening (2015: 72%, p=0.001, 2016: 64%, p=0.001). Relative to 2014 baseline data (63%), improvements in compliance with annual lipid screening increased in 2015 (80%), but was not significant. The increase in lipid screening compliance was, however, significant in 2016 (86%, p=0.017). Screenings for thyroid function testing showed minor improvements in compliance; however, the results were not statistically significant.
Discussion
This study demonstrates the use of a diabetes EMR template and order set significantly improved compliance with ISPAD complication screening guidelines in an urban outpatient pediatric endocrinology clinic. Studies have also shown that screening and follow up in children diagnosed with T1DM leads to an improved clinical course.14
Screening for microalbuminuria in diabetic patients (indicative of an early and reversible stage of nephropathy) allows for early detection and the early use of ACE inhibition therapy which can promote ideal glycemic levels during the reversible period.15 Lipid screening may help diagnose dyslipidemia, common in children with type 1 diabetes and often associated with cardiac risks such as atherosclerosis.16 Early screening for retinopathy, after the onset of puberty, may provide optimal preventative and management care for pediatric T1DM patients.17 Furthermore, screening for thyroid autoantibodies and TSH levels allows for detection of thyroid abnormalities.18 According to Mahmud et al many patients with T1D and celiac disease (CD) do not experience CD-related symptoms. Therefore, it is of great benefit to perform routine celiac screenings as a means of early detection for CD.19,20 The importance of standardized screening early and frequently in this population cannot be dismissed.
Recent studies demonstrate an increase in patient and physician adherence to recommended T1DM screening guidelines; however, increased efforts are required to ensure thoroughness in their approach.6,21 A limitation of these previous approaches was the reliance on patients with limited knowledge regarding medical terminology and testing to self-report data on diabetes screening tests.6 Electronic medical records, however, may eliminate this uncertainty and allow for more accurate reports.
This study has some limitations, such as, providing data from a single institution and representation from a low sample size. It is important to note, however, that the small cohort size does not diminish the significance of the findings and translation within a larger cohort is expected. As such, future studies should consider a larger sample size and a longitudinal study design. Another limitation included a wide age range (0–22 years old) in the patients studied, which may cause an effect as age has an important role in glycemic control and management of diabetes. Studies have shown decreased glycemic control and care coordination when transitioning from pediatric to adult care.18,21,22 Further studies should also target the older pediatric populations who are transitioning from pediatric to adult care to ensure full compliance in diabetes screening.
Building upon this, future studies could expand the use of EMR templates in patients with type 2 diabetes as well as those with other chronic disease processes. These studies would look at the effects in adherence to medical guidelines, as well as the long-term implications of disease complication detection and prevention.
Conclusion
The use of an EMR template and order set showed consistent improvement in compliance with ISPAD diabetes complication screening guidelines including annual eye exams, annual foot exams, basic metabolic panel screening, albumin/creatinine ratio screening, and celiac screening in both the initial and maintenance phases of the study. Also, in the maintenance phase, improvements were seen in lipid screening. This increasing result in maintenance phase data may be attributed to longer provider exposure to routine screening protocols through the template and order set, allowing for stricter adherence. This is promising in that stricter adherence to screening guidelines may lead to better detection of disease complications. Stricter adherence to guidelines at each visit also provides clinicians indirect educational opportunities, potentially making patients more aware of potential complications should screening not occur.
Designing and creating specific templates for other chronic conditions may aid physicians in improving the process of care through improved screening and appropriate intervention. Future aims could include the hybridization of smart technology and applications with current screening guidelines. This approach could provide the patient with the opportunity to increase engagement in and understanding of their health care management. Further research is needed to evaluate technology’s influence on patient compliance with medical guidelines for other chronic conditions in the pediatric population to ensure optimal medical care.
Acknowledgments
We would like to thank Oksana Tatarina-Nulman for her contribution and help with manuscript revisions. The abstract of this paper was presented at the 2018 Pediatrics Academic Society Meeting, “The Use of a Diabetes Electronic Medical Record Template Leads to Improvement of Screening for Complications of Type 1 Diabetes Mellitus in the Pediatric Population” as a poster presentation with interim findings. The poster’s abstract was published in “Meeting Abstracts” in Pediatrics Academic Society, May 2018, 142 (1 meeting abstract) 616; DOI:10.1542/peds.142.1MeetingAbstract.616.
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Dabelea D, Mayer-Davis EJ, Saydah S, et al. Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. JAMA. 2014;311:1778–1786. doi:10.1001/jama.2014.3201
2. Genuth S. Insights from the diabetes control and complications trial/epidemiology of diabetes interventions and complications study on the use of intensive glycemic treatment to reduce the risk of complications of type 1 diabetes. Endocr Pract. 2006;12:34–41. doi:10.4158/EP.12.S1.34
3. Cho YH, Hing S, Craig ME, et al. Microvascular complications assessment in adolescents with 2- to 5-yr duration of type 1 diabetes. Pediatr Diabetes. 2011;12:682–689. doi:10.1111/j.1399-5448.2011.00762.x
4. Holl RW, Lang GE, Grabert M, et al. Diabetic retinopathy in pediatric patients with type-1 diabetes: effect of diabetes duration, prepubertal and pubertal onset of diabetes, and metabolic control. J Pediatr. 1998;132(5):790. doi:10.1016/S0022-3476(98)70305-1
5. Wang SY, Andrews CA, Herman WH, Gardner TW, Stein JD. Incidence and risk factors for developing diabetic retinopathy among youths with type 1 or type 2 diabetes throughout the United States. Ophthalmology. 2017;124(4):424–430. doi:10.1016/j.ophtha.2016.10.031.
6. Waitzfelder B, Pihoker C, Klingensmith G, et al. Adherence to guidelines for youths with diabetes mellitus. Pediatrics. 2011;128:531–538. doi:10.1542/peds.2010-3641
7. Corathers SD, Schoettker PJ, Clements MA, et al. Health-system-based interventions to improve care in pediatric and adolescent type 1 diabetes. Curr Diab Rep. 2015;15(11):91. doi:10.1007/s11892-015-0664-8
8. Rosenberg JB, Friedman IB, Gurland JE. Compliance with screening guidelines for diabetic retinopathy in a large academic children’s hospital in the Bronx. J Diabetes Complications. 2011;25:222–226. doi:10.1016/j.jdiacomp.2010.11.001
9. Wood JR, Miller KM, Maahs DM, et al. Most youth with type 1 diabetes in the t1d exchange clinic registry do not meet American Diabetes Association or International Society for Pediatric and Adolescent Diabetes clinical guidelines. Diabetes Care. 2013;36(7):2035–2037. doi:10.2337/dc12-1959
10. Fortin K, Pries E, Kwon S. Missed medical appointments and disease control in children with type 1 diabetes. J Pediatr Health Care. 2016;30(4):381–389. doi:10.1016/j.pedhc.2015.09.012
11. Stumetz KS, YiFrazier JP, Mitrovich C, et al. Quality of care in rural youth with type 1 diabetes: a cross-sectional pilot assessment. BMJ Open Diabetes Res Care. 2016;4(1):e000300. doi:10.1136/bmjdrc-2016-000300
12. Dumser SM, Ratcliffe SJ, Langdon DR, et al. Racial disparities in screening for diabetic retinopathy in youth with type 1 diabetes. Diabetes Res Clin Pract. 2013;101(1):e3–e5. doi:10.1016/j.diabres.2013.03.009
13. Pihoker C, Forsander G, Fantahun B, et al. ISPAD Clinical Practice Consensus Guidelines 2018: the delivery of ambulatory diabetes care to children and adolescents with diabetes. Pediatr Diabetes. 2018;19(Suppl. 27):84–104. doi:10.1111/pedi.12757
14. Barker JM, Goehrig SH, Barriga K, et al. Clinical characteristics of children diagnosed with type 1 diabetes through intensive screening and follow-up. Diabetes Care. 2004;27:1399–1404. doi:10.2337/diacare.27.6.1399
15. Silverstein JH, Klingensmith G, Copeland K, et al. Care of children and adolescents with type-I diabetes. Diabetes Care. 2005;28:184–212. doi:10.2337/diacare.28.1.186
16. McGill HC. Relationship of atherosclerosis in young men to serum lipoprotein cholesterol concentrations and smoking. A preliminary report from the pathobiological determinants of atherosclerosis in youth (pday) research group. JAMA. 1990;264(23):3018–3024.
17. American Academy of Pediatrics. Screening for retinopathy in the pediatric patient with type 1 diabetes mellitus. Pediatrics. 1998;101:313–314. doi:10.1542/peds.101.2.313
18. Kordonouri O, Deiss D, Danne T, et al. Predictivity of thyroid autoantibodies for the development of thyroid disorders in children and adolescents with type 1 diabetes. Diabet Med J Br Diabet Assoc. 2002;19:518–521. doi:10.1046/j.1464-5491.2002.00699.x
19. Mahmud FH, Murray JA, Kudva YC, et al. Celiac disease in type 1 diabetes mellitus in a North American community: prevalence, serologic screening, and clinical features. Mayo Clin Proc. 2005;80(11):1429–1434. doi:10.4065/80.11.1429
20. Gesualdo PD, Bautista KA, Waugh KC, et al. Feasibility of screening for T1D and celiac disease in a pediatric clinic setting. Pediatr Diabetes. 2016;17(6):441–448. doi:10.1111/pedi.12301.
21. Tapley JL, McGwin G, Ashraf AP, et al. Feasibility and efficacy of diabetic retinopathy screening among youth with diabetes in a pediatric endocrinology clinic: a cross-sectional study. Diabetol Metab Syndr. 2015;7:56. doi:10.1186/s13098-015-0054-z
22. Lotstein DS, Seid M, Klingensmith G, et al. Transition from pediatric to adult care for youth diagnosed with type 1 diabetes in adolescence. Pediatrics. 2013;131(4):1062–1070. doi:10.1542/peds.2012-1450
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.