Back to Journals » Clinical Epidemiology » Volume 18
Implementation of Day Surgery in Denmark Compared with Benchmarks from the United Kingdom: A Nationwide Register-Based Cohort Study
Authors Hald K ![]() , Hedegaard JN, Petersen JA, Bartholdy J, Johnsen SP
, Hedegaard JN, Petersen JA, Bartholdy J, Johnsen SP
Received 24 November 2025
Accepted for publication 19 February 2026
Published 23 March 2026 Volume 2026:18 584054
DOI https://doi.org/10.2147/CLEP.S584054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Vera Ehrenstein
Kathrine Hald,1 Jakob Nebeling Hedegaard,1 John Asger Petersen,2 Jens Bartholdy,3 Søren Paaske Johnsen1
1Danish Center for Health Services Research, Department of Clinical Medicine, Aalborg University, Aalborg, Denmark; 2Department of Anaesthesiology, Næstved, Slagelse, and Ringsted Hospitals, Slagelse, Denmark; 3Department of Day Case Surgery, Amager-Hvidovre Hospital, Copenhagen, Denmark
Correspondence: Kathrine Hald, Danish Center for Health Services Research, Department of Clinical Medicine, Aalborg University, Selma Lagerløfs Vej 249, Gistrup, Aalborg, 9260, Denmark, Tel +45 41 19 56 70, Email [email protected]
Background: Day surgery is a safe and cost-effective alternative to inpatient surgery, and the British Association of Day Surgery (BADS) has developed national benchmarks which provide recommended day surgery case rates to guide implementation and monitoring. Although Denmark has seen substantial growth in day surgery over recent decades, the absence of national benchmarks limits systematic assessment and international comparison. Thus, the aim of this study was to map and evaluate the implementation of day surgery in Denmark between 2013 and 2022 and to compare it with recommended day-case rates from BADS.
Methods: A nationwide, historical register-based open cohort study was conducted, including all Danish citizens aged ≥ 18 years who underwent one of 16 selected surgical procedures between 2013 and 2022 in public or private hospitals. The primary outcome was the annual distribution of outpatient and inpatient procedures, compared with the BADS 2025 recommended day-surgery case rates. Secondary outcomes were mean inpatient length of stay, 30-day readmission, 30-day reoperation, and 90-day all-cause mortality.
Results: Of 441,413 procedures, 189,584 (42.9%) were performed as outpatient and 251,829 (57.1%) as inpatient procedures. The proportion of outpatient procedures increased steadily and exceeded the proportion of inpatient procedures by 2022. Comparison with BADS 2025 targets showed substantial variation in the implementation of day surgery across types of procedures. The mean inpatient length of stay declined from 2.8 to 1.9 days. Patient safety indicators showed consistently low risks both among inpatient and outpatient procedures.
Conclusion: Day surgery increased markedly in Denmark from 2013 to 2022 and now exceeds inpatient volumes for selected procedures. However, major variability across surgical fields remains. The findings support the hypothesis that a continued focus on implementation of day surgery could improve efficiency, free hospital capacity, and align Danish practice with British benchmarks without compromising patient safety.
Keywords: surgery, day surgery, implementation, health policy, epidemiology
Introduction
In day surgery, also known as ambulatory surgery, procedures are performed on an outpatient basis, and is associated with a high level of patient satisfaction and significant healthcare cost savings, without an increase in complication rates.1–17 These benefits are particularly evident in procedures such as hip, knee and shoulder arthroplasty, where outpatient procedures showed outcomes comparable to inpatient procedures.2,12,13 Additionally, significant cost reductions have been documented.,5,15,16 with inpatient surgery remaining 41.1% more expensive than outpatient alternatives even after adjusting for inpatient-specific charges.17 Comparative analyses of same-day versus next-day discharge following total joint arthroplasty indicate equivalent safety regarding healthcare services and clinical outcomes, including 30-day emergency department visits, 90-day complications, readmissions, and revision surgeries.1
In the 2019 guidelines for day-case surgery, the British Association of Anaesthetists and the British Association of Day Surgery (BADS) stated that most surgical procedures for both adults and children could be performed as day cases.18 Furthermore, in 2020, the British National Health Service recommended that day surgery should be recognized as a key component of the future of surgical services and should serve as the default setting for more than 200 procedures.19 BADS developed in 2005 “the BADS Directory of Procedures” which provides recommended day surgery case rates. The rates are defined by a combination of reported practice, actual hospital statistics and expert opinions and updated annually. The directory allows hospitals across the United Kingdom (UK) to monitor and assess whether their use of day surgery aligns with standardized national recommendations, as the recommended case rates are available online.20,21
Denmark has also seen a substantial shift toward day surgery over the past decades, driven in part by national research on fast-track pathways that emphasize early mobilization and reduced hospital stays.22–26 However, unlike the UK, there is no publicly available benchmarking tool for day-case rates across surgical procedures. While Danish registry infrastructure allows for comprehensive population-level analyses,27 little is known about how the implementation of day surgery in Denmark compares internationally. This knowledge gap limits opportunities for cross-system learning, quality benchmarking, and policy development.
Therefore, this study aimed to map and evaluate the implementation of day surgery, defined as outpatient procedures, in Denmark from 2013 to 2022 and compare it to the latest BADS recommended day-case rates in order to compare the implementation with current state-of-art. Additionally, the study estimated temporal trends in the length of stay for inpatient procedures. Furthermore, it examined the safety of outpatient procedures by comparing selected safety proxy indicators - readmissions, reoperations and all-cause mortality - to inpatient procedures.
Materials and Methods
Design
The study used national, Danish registries that cover the entire population and was performed as a historical, open cohort study. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines28 were used in the reporting of the study. The completed STROBE checklist is available in Additional File 1.
Setting
The Danish population constitutes six million people. The Danish healthcare system is based on the “Scandinavian Welfare Model” which implies that healthcare is universal. The tax funded healthcare services are nearly all free-of-charge, and all citizens have equal access. Denmark is structurally divided into regions and municipalities. The five regions (Capital, Central, North, Zealand, South) are responsible for health services provided by hospitals, general practice, and other medical specialists. The regions organise their own health services and have authority to adjust the provided services.29 The study includes data from both public and private hospitals.
Population
The study population consisted of all Danish citizens >18 years undergoing a surgical procedure in Denmark from 1 January 2013 to 31 December 2022. Baseline was defined as the day of the surgical procedure. A total of 16 procedures were selected for analysis. The procedures were selected because they either represent a large part of the total number of surgeries during the study period or constitute a major expense. The specific surgical procedures and Danish procedure codes which were included are shown in Additional File 2. Procedures were classified as outpatient if the patient was discharged on the same calendar day as the procedure was performed, and as inpatient if the hospital stay extended beyond one calendar day. This corresponds to the BADS definition of day case surgery, either zero-night stay or practice-based procedure.20,21
Data Sources
Data was encoded via individual-level record linkage using The Danish Civil Registration System. Every Danish citizen is assigned a personal and unique identification number; a CPR-number. The CPR-number ensures an individual linkage and is used across all national registries.30 Data from the national registries was retrieved at Statistics Denmark.27,31 The following registries and data were included: The Danish Civil Registration System regarding age, sex, place of residence, cohabitation status and date of death if any.30 The Danish National Patient Registry32 using information regarding procedures, readmissions, reoperations, and comorbidity. The Income Statistics Register33 regarding family income. The Population Education Register34 regarding education level.
Outcomes
The primary outcome was the distribution of outpatient and inpatient procedures which were compared to BADS recommended day surgery case rates from 2025.20,21 We chose not to use the historical BADS targets contemporaneous with the study period as we preferred to evaluate the historical implementation through the lens of current state-of-art recommendations in order to assess the feasibility of the targets. The secondary outcomes included the average length of inpatient hospital stay as well as patient safety proxy indicators, including a) readmission, defined as any unplanned acute hospitalization within 30 days following the baseline procedure, b) reoperation, defined as any unplanned surgical procedure within 30 days following the baseline procedure, c) all-cause mortality, defined as all causes of death within 90 days following the baseline procedure.
Statistical Analysis
A summary of the population was given in terms of descriptive statistics of the covariates, the distribution of procedure types, the yearly numbers of included procedures, and the yearly rates of procedures relative to the Danish background population. For the primary outcome, unadjusted prevalences stratified by calendar time and type of procedure, along with corresponding confidence intervals, were estimated using the Wilson score interval. These estimates were also presented graphically, with reference lines indicating the recommended day-case rates as defined by BADS. For the secondary outcome, lengths of stay were estimated as the area under the Kaplan-Meier survival curves and interpreted as restricted mean lengths of stay. Cumulative incidences were computed separately for inpatients and outpatients, stratified by calendar year, using the Aalen-Johansen estimator (or Kaplan-Meier for mortality). Cumulative incidences were reported at 30 days for readmission and reoperation, and at 90 days for mortality. Missing data was negligible, except for educational level (2.6%) and region of residence (0.09%). A sensitivity analysis excluding all participants aged 65 years or older was conducted to account for potential variation, based on the assumption that older individuals are generally frailer, have a higher prevalence of comorbidities, and are therefore more likely to undergo inpatient procedures. Additionally, a sensitivity analysis was performed to explore potential geographic variation, categorizing each patient’s place of residence according to the five geographical regions in Denmark. All analyses were made using Stata/MP 18 (StataCorp LLC).
Patient and Public Involvement
This study was developed with members and clinicians from the Danish Association of Day Surgery who have an extensive experience with implementing day surgery in the Danish health care sector during the last three decades. However, as the study was conducted using register-based data there was no direct involvement with either patients or the public.
Results
Between 2013 and 2022, a total of 441,413 procedures were performed in Denmark that met the study’s inclusion criteria. Of these, 251,829 (57.1%) were conducted in an inpatient setting and 189,584 (42.9%) as outpatient procedures. Figure 1 shows the flow diagram detailing the selection process. Table 1 presents baseline characteristics for all included procedures, stratified by setting. Procedures performed in an inpatient setting were generally associated with older patients, with a median age of 67.4 years (IQR: 54.6–75.4), compared to 54.9 years (IQR: 39.6–68.0) for outpatient procedures. Among inpatients, 42.2% of procedures were performed on individuals aged 70 years or older, compared to 21.0% among outpatients. The sex distribution differed between settings: 55.5% of inpatient procedures were performed on women, while 56.5% of outpatient procedures were performed on men. Regarding socioeconomic status, a higher proportion of inpatient procedures involved patients with lower educational level (29.7%) and lower median disposable family income (DKK 230,000; IQR: 180,000–310,000) compared to outpatient procedures (24.4% with low education level and median disposable family income DKK 250,000; IQR: 190,000–330,000). A slightly higher share of inpatients lived with a partner (56.6%) compared to outpatients (54.8%). Comorbidity burden also differed notably. Among inpatient procedures, 38.9% were associated with patients who had at least one comorbidity (CCI ≥1), compared to 26.2% among outpatient procedures. Procedures were geographically distributed across all five Danish regions. Among inpatient procedures, the Capital Region accounted for the largest share (30.1%), followed by Central (21.4%), South (21.0%), Zealand (16.2%), and North (11.3%). In contrast, outpatient procedures were most frequently performed in the Central Region (26.0%), followed by the Capital (24.9%), South (24.3%), Zealand (14.2%), and North (10.6%). Over the study period, the total number of procedures increased in both inpatient and outpatient settings. Among inpatient procedures, 30.7% were performed in 2013–2015, 29.1% in 2016–2018, and 40.1% in 2019–2022. For outpatient procedures, the increase was more pronounced: from 22.1% in 2013–2015 to 26.8% in 2016–2018, and 51.1% in 2019–2022. Additional File 3 presents the hourly distribution of the timing of the procedures among in- and outpatient procedures, respectively. For both groups, only few patients had procedures performed during nighttime.
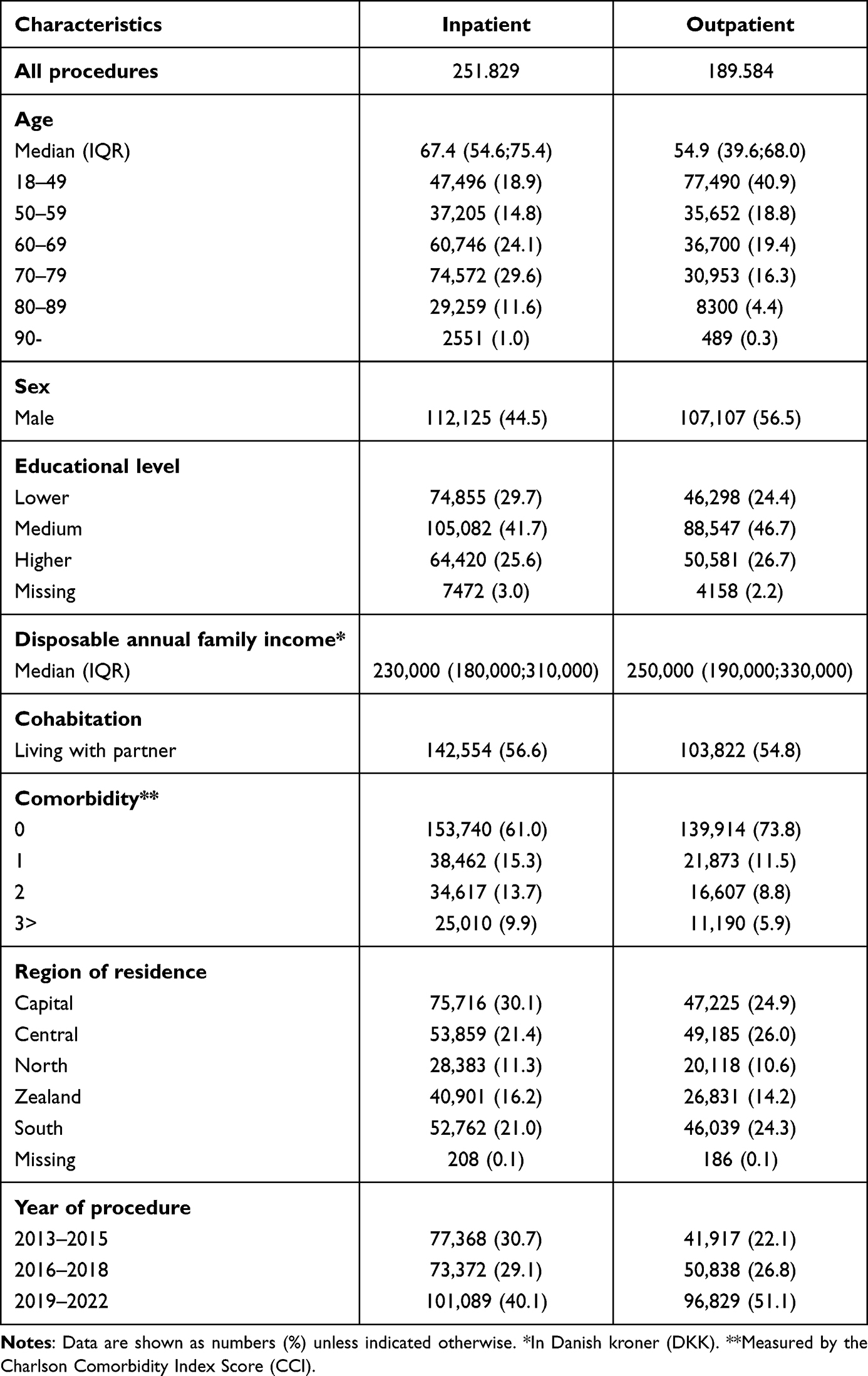 |
Table 1 Baseline Characteristics |
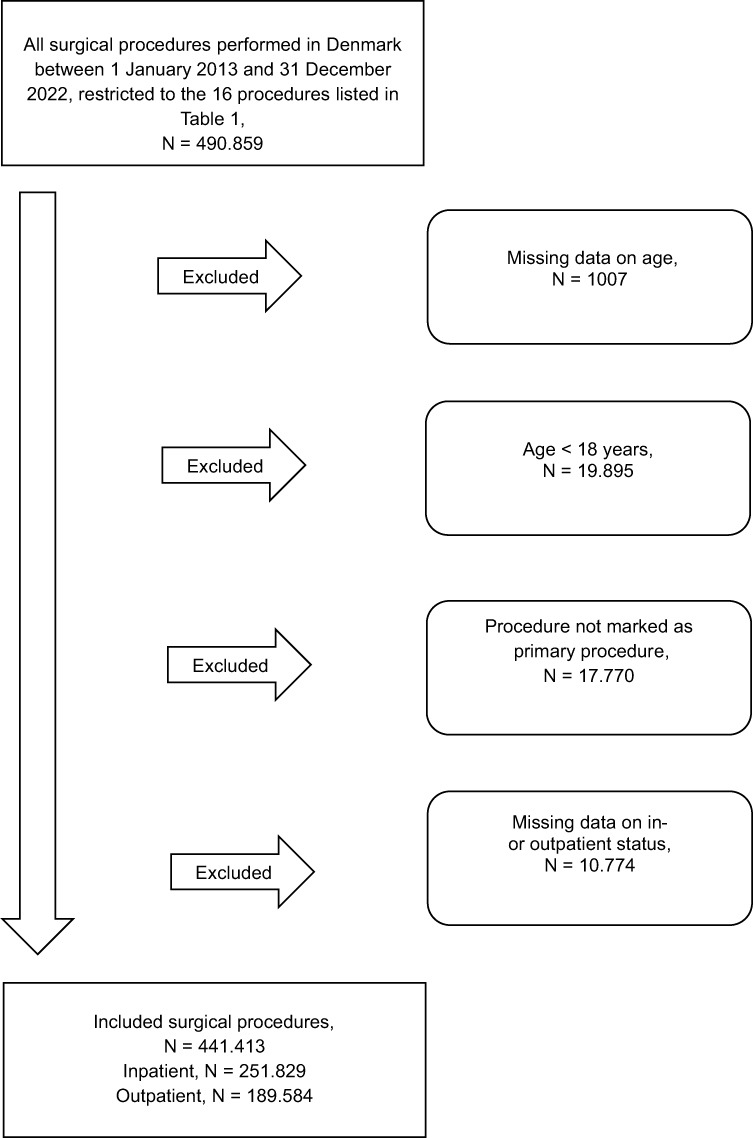 |
Figure 1 Flow diagram of surgical procedures included in the study. |
Baseline characteristics for the sensitivity population, restricted to procedures performed on patients <65 years, are presented in Additional File 4. A total of 242,050 procedures were included, of which 110,785 (45.8%) were inpatient and 131,265 (54.2%) were outpatient. As expected, the median age was lower (52.4 years for inpatient and 46.4 years for outpatient procedures), and the comorbidity burden was reduced. Among inpatient procedures, 74.4% were performed on individuals with no registered comorbidities, compared to 83.9% of outpatient procedures. Women accounted for 61.7% of inpatient procedures, whereas men accounted for 50.7% of outpatient procedures. The educational level was generally higher, with 29.7% of inpatients and 27.7% of outpatients having a high educational level. Median income levels were similar across settings (DKK 260,000), and 53.8% of inpatient procedures were performed on individuals living with a partner, compared to 48.1% among outpatients. Procedures were geographically distributed across all five regions. For inpatient procedures, the Capital Region contributed the highest proportion (29.7%), followed by the Central Region (22.3%), South (20.7%), Zealand (15.4%), and North (12.3%). Among outpatient procedures, the Central Region accounted for the largest share (25.6%), followed by the Capital (25.2%), South (24.9%), Zealand (14.3%), and North (9.8%). Temporal trends mirrored those observed in the total population. The overall number of procedures increased over time in both settings.
Primary Outcomes
Over the study period, the total number of procedures increased, driven primarily by a marked rise in outpatient activity. The number of inpatient procedures remained relatively stable, with minor fluctuations and a comparable volume in 2022 to that observed in 2013. In contrast, outpatient volumes increased steadily throughout the period and ultimately surpassed inpatient volumes in the final year, indicating a substantial shift in surgical care delivery (Figure 2). In the sensitivity analysis restricted to procedures performed on patients <65 years, a similar trend was observed. The number of inpatient procedures showed some year-to-year variation but declined slightly overall between 2013 and 2022. Meanwhile, the number of outpatient procedures rose consistently throughout the study period, becoming the dominant setting from 2016 onwards (Additional File 5). While some variation in procedural prevalence was observed across regions and study periods, all five Danish regions demonstrated a consistent temporal shift toward increased use of outpatient procedures (Additional File 6). This trend was also evident in the sensitivity analysis restricted to procedures performed on patients <65 years (Additional File 7).
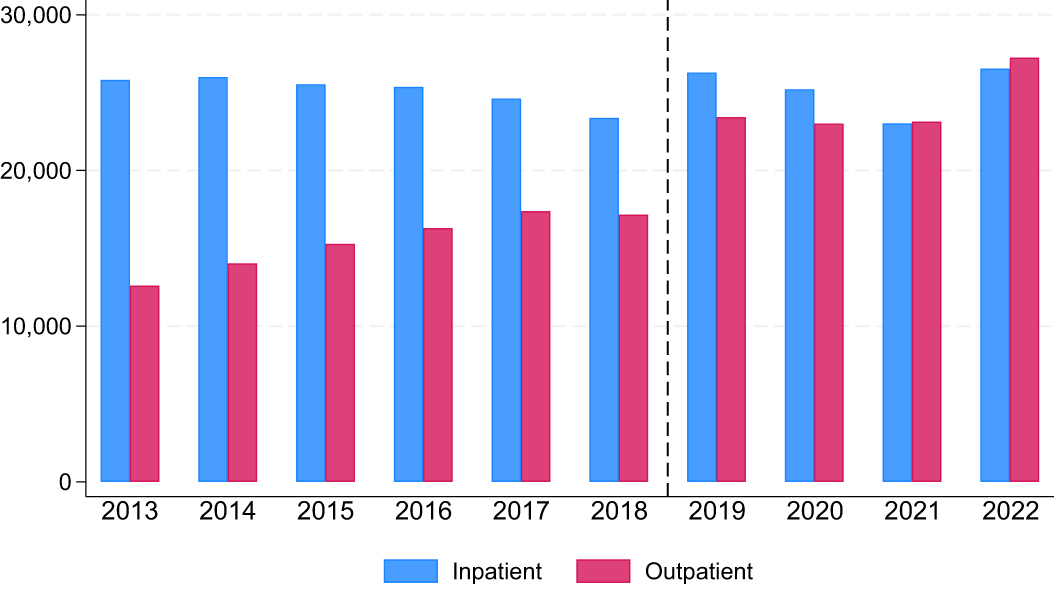 |
Figure 2 The number of procedures stratified by year and setting. The vertical dashed line between 2018 and 2019 indicates the transition from the Danish National Patient Registry version 2 (LPR2) to version 3 (LPR3). |
Figure 3 illustrates the proportion of outpatient procedures over time for each of the 16 included procedures, along with the recommended day surgery case rates 2025 according to BADS.20,21 Across most procedures, a gradual or stable increase in outpatient delivery was observed over the study period, with some variation in overall outpatient proportions and temporal patterns. For several procedures, such as Endoscopic resection/destruction of lesion of bladder (TUR-B), and rotator cuff repair, the outpatient proportion approached or exceeded the BADS target during the study period. In contrast, procedures such as thyroid surgery, tonsillectomy, and abdominal hysterectomy, remained close to or below the BADS target throughout. In the sensitivity analysis restricted to patients <65 years, patterns were largely similar. For most procedures, outpatient proportions were slightly higher compared to the total population, and in some cases aligned more closely with BADS targets (Additional File 8).
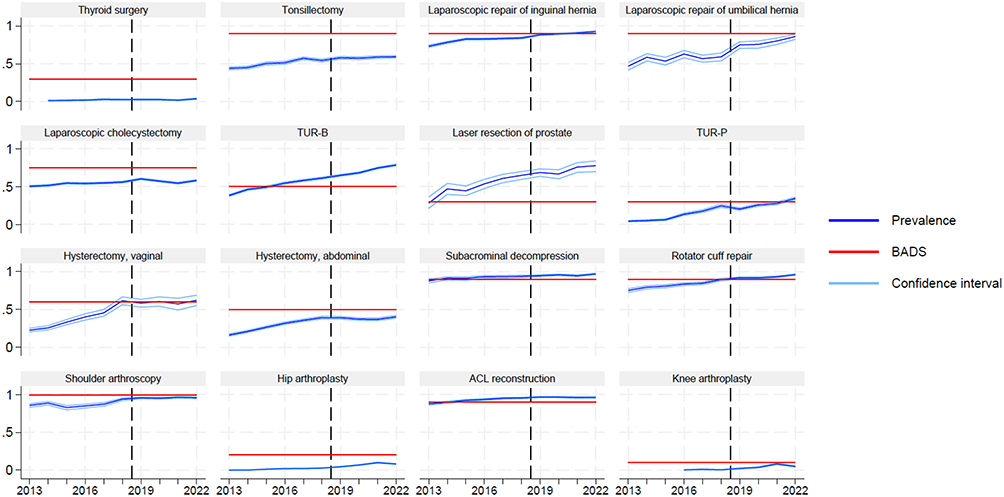 |
Figure 3 The prevalence of outpatient procedures compared to the BADS recommended day surgery case rates stratified by year and type of procedure. The dark blue line represents the annual prevalence of outpatient procedures, the light blue line indicates the 95% confidence interval, and the red horizontal line denotes the BADS recommended target rates in 2025. The vertical dashed line between 2018 and 2019 indicates the transition from the Danish National Patient Registry version 2 (LPR2) to version 3 (LPR3). Abbreviations: TUR-B, Endoscopic resection/destruction of lesion of bladder; TUR-P, Endoscopic resection of prostate; ACL reconstruction, Arthroscopic repair of anterior cruciate ligament. |
Secondary Outcomes
The average length of inpatient hospital stay decreased over the study period. In 2013, the restricted mean length of stay was 2.80 (95%-CI: 2.75;2.85) days, gradually declining to 1.85 (95%-CI: 1.81;1.89) days by 2022. Although some year-to-year variation was observed, the overall trend indicated a reduction in hospitalization duration among inpatients (Additional File 9). In the sensitivity analysis restricted to patients <65 years, the pattern was similar (Additional File 10).
Additional file 11 shows the cumulative incidence of readmission within 30 days following the baseline procedure. Throughout the study period, the readmission incidence was consistently higher following inpatient procedures compared to outpatient procedures. The overall incidence of readmission remained low in both groups, with only modest year-to-year variation and a stable difference between settings. Additional File 12 shows that cumulative incidence of reoperation within 30 days following the baseline procedure was likewise low across the study period. The incidence was generally higher following inpatient procedures; however, in 2022, the incidence following outpatient procedures slightly exceeded that of inpatient procedures. Despite this crossover, the overall frequency of reoperation remained low in both settings. All-cause mortality within 90 days following the baseline procedure is presented in Additional File 13 as a failure proportion. The failure proportion was markedly higher following inpatient procedures but remained low overall, with no substantial temporal variation. Outpatient procedures were consistently associated with very low mortality. In the sensitivity analysis restricted to patients <65 years, a similar pattern was observed (Additional File 14–16).
Discussion
Principal Findings
The total number of procedures increased steadily during the study period from 2013 to 2022. A shift was observed towards a higher proportion of outpatient procedures and a lower proportion of inpatient procedures. When compared with the BADS recommended day surgery case rates from 2025, the proportion of outpatient procedures in Denmark at the end of the study period showed considerable variation. For some procedures, day surgery was implemented in line with the targets, whereas for other procedures a substantial potential for further implementation remained. The mean inpatient length of stay declined over time, reaching an average of just under two days at the end of the study period. Patient safety proxy indicators measured by 30-day readmission, 30-day reoperation and 90-day mortality showed consistently low risks and did not vary substantially. Sensitivity analyses, restricted to patients < 65 years and stratified by region of residence aligned with these overall patterns.
Strengths and Weaknesses of the Study
A major strength of this study is the use of nationwide, comprehensive Danish registers. Due to the personal and unique CPR-number that all Danish citizens receive, individual-level record linkage across the registers is possible, providing almost complete population coverage and follow-up along with a minimum of missing data. Another notable strength of this study is the extended follow-up period, which captures the development of day surgery implementation in Denmark across a decade. The length of follow-up strengthens the validity of the findings by making it possible to observe stable trends and reducing the likelihood that the observed increase in day surgery merely reflects short-term variations. The robustness of the findings is further validated by the sensitivity analyses and patient safety proxy indicators, which demonstrate not only that the implementation of day surgery increased during the study period, but also that it was achieved in a safe and apparently appropriate way. Another strength of the study is that the 16 procedures included in the analysis were selected in collaboration with clinicians, based on the representation of either a substantial proportion of all procedures performed during the study period or the contribution to major healthcare expenditures. Moreover, the selected procedures are directly comparable to specific BADS day case surgery rates, which were likewise identified on the basis of a combination of reported practice, hospital statistics, and expert opinion. By relying on procedures and corresponding targets that have been agreed upon by clinicians, the study ensures that its findings genuinely reflect, and remain relevant to, clinical practice. In addition, the external validity of the study is strengthened by comparing the results with British targets for day case surgery rates.
A limitation of this study is that the Danish definition of day surgery is not completely identical to that used by BADS, where it is defined as a hospital stay of less than 24 hours. A new version of the Danish National Patient Registry was introduced in 2019. In the previous version, the exact times of admission and discharge were not registered, and day surgery was therefore defined in this study as admission and discharge occurring on the same calendar day. This difference could have led to some misclassification. However, the degree of misclassification is likely to be minor as elective surgery is rarely scheduled to take place overnight as also confirmed by our data (Additional File 3). Another limitation is that the registry does not distinguish between procedures that were planned as day surgery and those that were carried out as such. This could have resulted in either an overestimation or an underestimation of the true implementation of day surgery. A further limitation related to the transition between the two versions of the Danish National Patient Registry from 2018 to 2019 is the marked increase in the number of outpatient procedures observed from 2018 to 2019. This suggests that a change in registration practice may have occurred, and that the increase does not solely reflect greater implementation of day surgery. Nevertheless, the upward trend continued throughout the rest of the study period, indicating that the development cannot be explained by changes in registration practice alone, but also reflects a genuine increase in day surgery implementation in the later years of the study. Finally, the results, which extend only through 2022, are compared with BADS 2025 targets. Although the Danish results and the British targets are not directly comparable, they nevertheless provide a useful indication of the Danish day surgery implementation, given that the BADS targets represent the most robust and internationally recognised benchmarks.
Comparison with Other Studies
BADS are the frontrunners of developing benchmarks for day surgery and comparison with these data is therefore relevant when estimating the implementation of day surgery in Denmark. In addition to the BADS 2025 targets, national data from September 2025 provide insight into the actual distribution of day surgery across hospitals in the UK. Data are reported as the 50th and 95th percentiles of hospital performance. The 50th percentile reflects the level at which half of the hospitals perform below, and half perform above, representing the typical practice. The 95th percentile reflects the level achieved by the top hospitals, with 95% of hospitals performing below this threshold. Thus, the percentiles add to the official targets by providing a yearly overview of what is achieved across the UK.21 As shown in Figure 3 and Table 2 a heterogeneous picture emerges when comparing the Danish results from 2022 with the BADS 2025 targets. For some procedures the proportion of Danish day surgery were in line with or exceeded the BADS targets. Other procedures remained well below the recommended day-case rates, indicating a potential for further implementation. Comparison with the 2025 performance percentiles from the UK provide further nuance. For some procedures the Danish outpatient proportions approached or exceeded not only the BADS targets but also the 95th percentile of UK hospitals. Conversely, for some procedures Danish outpatient proportions were below both the 50th and the 95th percentile in the UK, showing that there remain areas with significant implementation gaps relative to practice in the UK. These findings suggest that while Denmark has successfully implemented day surgery in certain surgical areas, there is a marked variability across procedures. The comparison highlights that for certain procedures Denmark performs at a level comparable to the best hospitals in the UK, whereas for others, day surgery remains under-implemented relative to both the BADS targets, and the typical levels of implementation observed in the healthcare system in the UK in 2025.
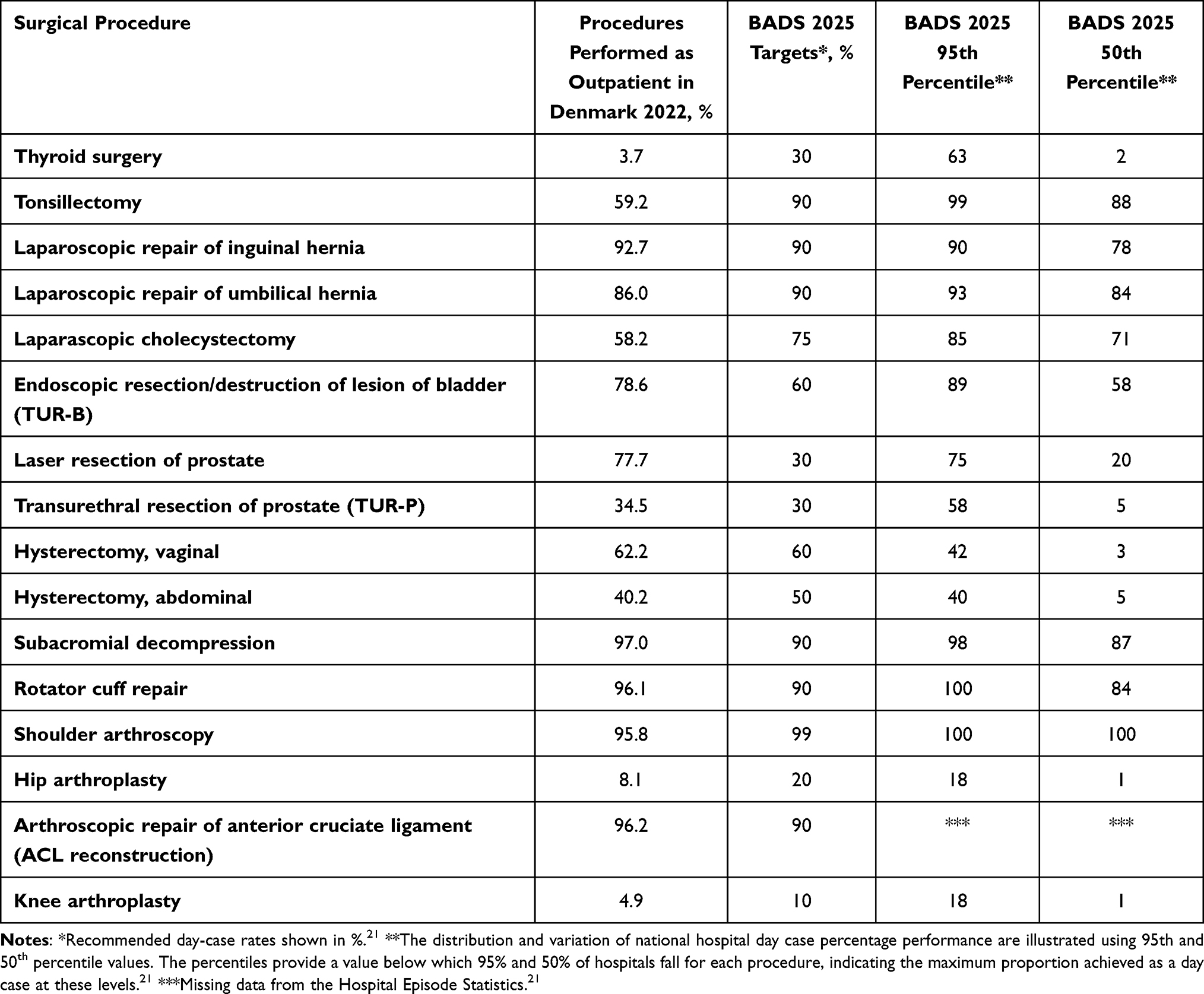 |
Table 2 Procedures Performed as Outpatient Procedures in Denmark in 2022 Compared to BADS 2025 Targets and BADS 2025 Collected 95th and 50th Percentiles |
Other Scandinavian countries have examined the implementation of day surgery. In Norway, a report described the use of day surgery between 2013 and 2017 across 12 selected procedures, with a focus on the degree of implementation and geographical variation. The report demonstrated substantial regional variation in the implementation of day surgery. Overall, the number of procedures performed as day surgery remained relatively stable during the study period, although marked declines were observed for certain procedures, such as meniscus procedures, reflecting changes in clinical practice.35 The Norwegian study period lies within this study’s period, which, however, covers a considerably longer time span and thereby provides a more robust basis for assessing the implementation of day surgery. In contrast to the Norwegian findings, the Danish analyses revealed no notable overall geographical variation at regional level in the degree of implementation.
In Sweden, the development of day surgery has likewise been investigated. A report found that the number of procedures performed as day surgery doubled between 2005 and 2023.36 This trend is consistent with that observed in Denmark, where a similar increase occurred between 2013 and 2022. Importantly, the general shift towards day surgery is not limited to Scandinavia. For example, an Australian study from 2023 evaluated the implementation, feasibility, and safety of day surgery for joint replacement procedures. Echoing the Scandinavian experience, the study concluded that implementation of day surgery is feasible. Moreover, in line with the findings of the present study, it demonstrated that day surgery can be carried out with a high degree of patient safety.37
Implications for Research and Practice
Denmark has, over the past 20 years, succeeded in partial implementation of day surgery. However, substantial potential for further implementation remains when compared with international guidelines and targets for day case rates. A continued focus on aligning with these established targets could enhance efficiency and free up hospital resources without compromising patient safety. Policymakers should recognize the importance of maintaining momentum in implementing day surgery as a strategy to optimize hospital capacity. It could also be considered to develop Danish targets, which would support more consistent national implementation, provide clearer guidance for clinical practice, and enable more standardized monitoring. Further research should examine the potential health economic benefits of expanded day surgery implementation, including both cost savings and the opportunity to redistribute resources within the healthcare sector.
Conclusion
This nationwide register-based study found a marked increase in day surgery in Denmark between 2013 and 2022, with outpatient procedures exceeding inpatient procedures by the end of the study period. While day surgery was implemented for several procedures, others remained well below the recommended rates in the UK, highlighting variability across surgical fields. Compared with benchmarks from BADS, Denmark overall performs at a level comparable to leading British hospitals for some procedures but lags behind for others. The study results suggest that a continued focus on implementation of day surgery could release hospital capacity, improve efficiency, and align Danish practice with standards in the UK without compromising patient safety.
Ethics Approval
The Danish Data Protection Agency approved this study. Register-based studies do not require approval from an ethics committee according to Danish law.
Data Sharing Statement
Data are available on reasonable request.
Acknowledgments
ChatGPT 5.1 was used for language improvement as all authors are non-native English speakers.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kay RD, Taylor AJ, Tye EY, Bryman JA, Runner RP. Outpatient total Hip and knee arthroplasty performed in a safety net hospital system. JAAOS Glob Res Rev. 2021;5:e21. doi:10.5435/JAAOSGlobal-D-21-00117
2. De Wouters S, Petronilia S, Paulet D, De Baere T, Willemart E, Cornu O. Outpatient total Hip arthroplasty: the future? Acta Orthop Belg. 2021;87:313–13. doi:10.52628/87.2.16
3. Rosinsky PJ, Chen SL, Yelton MJ, et al. Outpatient vs. inpatient Hip arthroplasty: a matched case-control study on a 90-day complication rate and 2-year patient-reported outcomes. J Orthop Surg Res. 2020;15:367. doi:10.1186/s13018-020-01871-8
4. Courtney PM, Froimson MI, Meneghini RM, Lee GC, Della Valle CJ. Can total knee arthroplasty be performed safely as an outpatient in the Medicare population? J Arthroplasty. 2018;33:S28–31. doi:10.1016/j.arth.2018.01.003
5. Huang A, Ryu JJ, Dervin G. Cost savings of outpatient versus standard inpatient total knee arthroplasty. Can J Surg. 2017;60:57–62. doi:10.1503/CJS.002516
6. Tedder C, DeBell H, Dix D, et al. Comparative analysis of short-term postoperative complications in outpatient versus inpatient total ankle arthroplasty: a database study. J Foot Ankle Surg. 2019;58:23–26. doi:10.1053/j.jfas.2018.06.003
7. Plantz MA, Sherman AE, Kadakia AR. A propensity score-matched analysis comparing outpatient and short-stay hospitalization to standard inpatient hospitalization following total ankle arthroplasty. J Orthop Surg Res. 2020;15:292. doi:10.1186/s13018-020-01793-5
8. Saadat LV, Mahvi DA, Jolissaint JS, et al. Twenty-three-hour-stay colectomy without increased readmissions: an analysis of 1905 cases from the National Surgical Quality Improvement Program. World J Surg. 2020;44:947–956. doi:10.1007/s00268-019-05257-8
9. Chen SY, Radomski SN, Stem M, et al. Safety and feasibility of ≤24-h short-stay right colectomies for primary colon cancer. World J Surg. 2023;47:2761–2774. doi:10.1007/s00268-023-07041-1
10. Angeramo CA, Dreifuss NH, Olivero AA, Sadava EE, Schlottmann F. Risk factors for readmission after short-hospital-stay laparoscopic appendectomy. World J Surg. 2020;44:4006–4011. doi:10.1007/s00268-020-05730-9
11. Aftab H, Fagerland MW, Gondal G, Ghanima W, Olsen MK, Nordby T. Gastric sleeve resection as day-case surgery: what affects the discharge time? Surg Obes Relat Dis. 2019;15:2018–2024. doi:10.1016/j.soard.2019.09.070
12. Kelly MP, Calkins TE, Culvern C, Kogan M, Della Valle CJ. Inpatient versus outpatient Hip and knee arthroplasty: which has higher patient satisfaction? J Arthroplasty. 2018;33:3402–3406. doi:10.1016/j.arth.2018.07.025
13. Leroux TS, Zuke WA, Saltzman BM, et al. Safety and patient satisfaction of outpatient shoulder arthroplasty. JSES Open Access. 2018;2:13–17. doi:10.1016/j.jses.2017.11.002
14. McDonald CE, Paynter C, Francis JJ, et al. Exploring patient acceptability of a short-stay care pathway in hospital post arthroplasty: a theory-informed qualitative study. Health Expect. 2022;25:2002–2014. doi:10.1111/hex.13561
15. Aynardi M, Post Z, Ong A, Orozco F, Sukin DC. Outpatient surgery as a means of cost reduction in total Hip arthroplasty: a case-control study. HSS J. 2014;10:252–255. doi:10.1007/s11420-014-9401-0
16. McKenna NP, Bews KA, Shariq OA, et al. Is same-day and next-day discharge after laparoscopic colectomy reasonable in select patients? Dis Colon Rectum. 2020;63:1427–1435. doi:10.1097/DCR.0000000000001729
17. Gregory JM, Wetzig AM, Wayne CD, Bailey L, Warth RJ. Quantification of patient-level costs in outpatient total shoulder arthroplasty. J Shoulder Elbow Surg. 2019;28(6):1066–1073. doi:10.1016/j.jse.2018.10.006
18. British Association of Day Surgery; Association of Anaesthetists. Guidelines for day-case surgery 2019. London: BADS; 2019 [cited November 17, 2025]. Available from: https://bads.co.uk/guidelines.
19. NHS England. National day surgery delivery pack. London: NHS England; 2020 [cited November 17, 2025]. Available from: https://www.england.nhs.uk/outpatient-transformation-programme/national-day-surgery-delivery-pack.
20. Jackson IJB, McWhinnie D, Skues M. The British Association of Day Surgery directory of procedures. Ambul Surg. 2010;16:87–89.
21. British Association of Day Surgery. BADS directory of procedures & national dataset. London: BADS; 2025. Available from: https://bads.co.uk/for-members/bads-directory-of-procedures-national-dataset/.
22. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78:606–617. doi:10.1093/bja/78.5.606
23. Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg. 2008;248:189–198. doi:10.1097/SLA.0b013e31817f2c1a
24. Engbæk J, Bartholdy J, Hjortsø NC. Return hospital visits and morbidity within 60 days after day surgery: a retrospective study of 18,736 day surgical procedures. Acta Anaesthesiol Scand. 2006;50:911–919. doi:10.1111/j.1399-6576.2006.01090.x
25. Majholm B, Engbæk J, Bartholdy J, et al. Is day surgery safe? A Danish multicentre study of morbidity after 57,709 day surgery procedures. Acta Anaesthesiol Scand. 2012;56:323–331. doi:10.1111/j.1399-6576.2011.02631.x
26. Petersen PB, Kehlet H, Jørgensen CC. Improvement in fast-track Hip and knee arthroplasty: a prospective multicentre study of 36,935 procedures from 2010 to 2017. Sci Rep. 2020;10:21233. doi:10.1038/s41598-020-77127-6
27. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
28. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344–349. doi:10.1016/j.jclinepi.2007.11.008
29. Ministry of Health. Healthcare in Denmark – an overview. Copenhagen: Ministry of Health; 2017 [cited November 17, 2025]. Available from: https://www.ism.dk/Media/637643691542085966/Healthcare%20in%20Denmark%20-%20An%20overview.pdf.
30. Mainz J, Hess MH, Johnsen SP. The Danish unique personal identifier and the Danish Civil Registration System as a tool for research and quality improvement. Int J Qual Health Care. 2019;31:635–638.
31. Statistics Denmark. History. Copenhagen: Statistics Denmark; 2025. Available from: https://www.dst.dk/da/OmDS/historie.
32. Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
33. Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39:103–105. doi:10.1177/1403494811405098
34. Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39:91–94. doi:10.1177/1403494810394715
35. Uleberg B, Mathisen S, Shu J, et al. Dagkirurgi i Norge 2013–2017: utvalgte inngrep. Tromsø: Senter for klinisk dokumentasjon og evaluering (SKDE); 2018 [cited November 17, 2025]. Available from: https://apps.skde.no/helseatlas/files/dagkirurgi_2013-2017.pdf.
36. Sveriges Kommuner och Regioner (SKR). Hälso- och sjukvårdsrapporten 2024. Stockholm: SKR; 2024 [cited November 17, 2025]. Available from: https://skr.se/download/18.26ad6aaa1924717b3ba3249/1727798901809/SKR_A4_Halso-sjukvardsrapporten_2024_webbpdf.pdf.
37. Tutty A, Martin S, Scholes C, et al. Implementation of a day-stay joint replacement pathway in an Australian regional public hospital: a descriptive study. Aust J Rural Health. 2024;32:703–714. doi:10.1111/ajr.13127
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.