Back to Journals » Clinical Interventions in Aging » Volume 15
Implementation and Evaluation of a Fall Risk Screening Strategy Among Frail Older Adults for the Primary Care Setting: A Study Protocol
Authors Meekes WMA ![]() , Leemrijse CJ
, Leemrijse CJ ![]() , Korevaar JC
, Korevaar JC ![]() , Henquet JMAE
, Henquet JMAE ![]() , Nieuwenhuis M, van de Goor LAM
, Nieuwenhuis M, van de Goor LAM
Received 21 March 2020
Accepted for publication 19 July 2020
Published 9 September 2020 Volume 2020:15 Pages 1625—1636
DOI https://doi.org/10.2147/CIA.S254864
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Richard Walker
WMA Meekes,1 CJ Leemrijse,2 JC Korevaar,2 JMAE Henquet,3 M Nieuwenhuis,4 LAM van de Goor1
1Tranzo, Tilburg School of Social and Behavioral Sciences, Tilburg University, Tilburg, Noord-Brabant, Netherlands; 2NIVEL, Utrecht, Netherlands; 3Huisartsenpraktijk de Ypelaer, Hilvarenbeek, Noord-Brabant, Netherlands; 4Fysiotherapie Nieuwenhuis, Best, Noord-Brabant, Netherlands
Correspondence: WMA Meekes
Tranzo, Tilburg School of Social and Behavioral Sciences, Tilburg University, 5000 LE Tilburg, Postbus 90153, Netherlands
Tel +31 13 466 4451
Email [email protected]
Background: Falls are an increasing problem among older people. There are several evidence-based interventions available to prevent falls. However, these are not always well implemented in the primary care setting. General practitioners (GPs) are often the first point of contact for health issues, making them the designated professionals for providing falls prevention. Because GPs are often unaware which patients have a high fall risk and patients themselves do not always know they have a high fall risk, this study aims to evaluate the implementation of a targeted fall risk screening strategy among independently living, frail older people in the primary care setting.
Materials and Methods: The targeted fall risk screening strategy used in this study consists of tools for screening high fall risk and for identifying the underlying cause(s) of the high fall risk, an accredited training course in falls prevention for professionals, and service provision by certified physio- and exercise therapists who are able to offer evidence-based falls prevention interventions. This targeted fall risk screening strategy will be implemented in the primary care setting and evaluated at the level of the GP practice and at the level of the patient by using the RE-AIM model of Glasgow et al. In a pre-posttest design, data will be collected of the total number of frail older people who are screened, referred and enrolled for fall-preventive care. Furthermore, barriers and facilitators of the implementation of the fall risk screening strategy will be identified by conducting focus groups and interviews with the care providers and frail older patients. Additionally, the influence of the falls prevention interventions on frail older patients will be evaluated by using a pre-posttest design with a 12-month follow-up period during which data are collected regarding patients’ stability, mobility, strength, balance, self-efficacy, health status, and daily activities.
Study Registration: This study is approved by the Medical Ethics Committee Brabant, the Netherlands (NL61582.028.17/ P1732) and registered at the Netherlands Trial Register, NL7917.
Keywords: preventive medicine, primary care, geriatric medicine, risk management
Introduction
Worldwide, falls are a major public health problem.1 Approximately 30% of the older people aged 65 and over and 50% of the people aged 80 and over fall at least once a year.2–4 The consequences of a fall can vary, for example, from a scratch or bruise to a hip fracture, brain injury, or even death.5 In the Netherlands, every 5 min, an older person is admitted to the emergency department (ED) due to the consequences of a fall, which resulted in 108,000 treatments at EDs in 2018.6 These numbers are expected to rise due to the increase in the number of older people.6 Treatment and rehabilitation after a fall can result in considerable medical costs (€960 million direct medical costs). In the Netherlands, the majority of these costs are caused by falls among independently living, frail older people (€810 million direct medical costs).6
There is a reasonable level of evidence that several interventions prevent falls and fall-related trauma among independently living older people.7–9 Falls prevention interventions differ per target group, intensity, type of treatment (group or individual), and approach (eg exercise therapy or addressing risk factors). Multicomponent group or home-based exercises, environmental modifications, medication reviews and addressing cardiovascular problems are examples of evidence-based interventions.10 For example, Hopewell et al assessed the effects of interventions designed to reduce the incidence of falls among independently living older people and found that multifactorial interventions reduce the rate of falls among older people (Rate Ratio 0.77, 95% CI 0.67 to 0.87; 19 trials; 5853 participants).11 Furthermore, Sherrington et al identified that exercise can reduce the rate of falls by 23% (Rate Ratio 0.77, 95% CI 0.71 to 0.83; 59 trials, 12,981 participants).12
Overall, multifactorial programs that address evidence-based interventions are recommended,10,13 but evidence of the efficacy of the programs that address various causes of fall risk in real-life settings is still limited or not available.14
In the Netherlands, general practitioners (GPs) are the gatekeepers for healthcare and thus often the first point of contact for health issues, making them the designated professionals for providing falls prevention to independently living, frail older people. Nonetheless, systematic screening for fall risk does not take place at GP practices, and GPs only know of 20–30% of the falls that occur among their patients.15 This means that GPs are often unaware which of their patients have an increased risk of falling and are, therefore, unable to offer them adequate fall-preventive care.16–18 These issues occur not only in the Netherlands but in other countries as well.16,17 All this leads to the unfavorable situation in which frail older people, for whom falls prevention interventions are potentially effective, do not receive this care. This can result in severe adverse health consequences and lower quality of life for frail older people, including loss of independence.
Currently, there is no strategy for engaging GPs in falls prevention in the Netherlands. According to Paul, falls are preventable, and a systematic approach for identifying risks and addressing them in a concerted manner is key to prevention.19 Therefore, systematic implementation of falls prevention with a targeted screening strategy at GP practices appears to be essential for making falls prevention more accessible to independently living, frail older people. To improve the implementation and to make long-term engagement in falls prevention possible, it is important to identify and understand the experienced barriers and facilitators of the implementation of the fall risk screening strategy.
Therefore, the aim of this study is to evaluate the implementation of a targeted fall risk screening strategy among independently living, frail older people in the primary care setting. To better understand and improve the implementation of the fall risk screening strategy, experienced barriers and facilitators will be investigated. Evaluation of the implementation of the fall risk screening strategy will primarily be conducted at the level of the GP practice and secondarily at the level of the frail older patient.
In this study, the following research questions will be answered:
- What is the influence of the targeted fall risk screening strategy in the primary care setting on the number of screened, referred, and enrolled frail older people for falls prevention? (GP practice level)
- What are the barriers and facilitators of the implementation of the targeted fall risk screening strategy in the primary care setting? (GP practice level)
- What is the influence of evidence-based falls prevention interventions offered by certified physio- and exercise therapists in a real-life setting on frail older patients’ balance, mobility, frequency of falling, fear of falling, self-efficacy, and quality of life? (Patient level)
Materials and Methods
Design
In this study, a targeted fall risk screening strategy will be implemented at GP practices. The fall risk screening strategy will be evaluated at the level of the GP practice and at the level of the frail older patient by using two pre-posttest designs. The targeted fall risk screening strategy consists of two parts. In the first part, GP practices receive the following tools to screen for fall risk and to offer falls prevention interventions:
- A validated fall risk screening instrument: this screening instrument is selected after an informal focus group consisting of primary care providers, followed by a systematic literature search (see Appendix I). (The systematic literature is not part of this protocol and will be described elsewhere.)
- A checklist to diagnose the underlying cause(s) of the fall risk: the items on the checklist are based on previous literature regarding risk factors for falls.20–22 The checklist is completed after a discussion within the research group that includes a GP specialized in geriatric care (see Appendix I).
- An overview of all physio- and exercise therapists certified to offer evidence-based falls prevention interventions in the surrounding area of the GP practices.
- A 4-hour accredited training session about falls prevention for health care professionals: the training session is offered by a trainer from the organization “VeiligheidNL”23 and is suitable for practice nurses and assistants. The training is not compulsory and is offered free of charge as part of this project.
In the second part, physio- and exercise therapists in the surrounding area are recruited to participate in this study so that each participating GP practice has access to the services of certified physio- or exercise therapists for falls prevention interventions. Physio- and exercise therapists who are not certified to provide an evidence-based falls prevention intervention are offered training.
Theoretical Framework
The targeted fall risk screening strategy will be evaluated by using the RE-AIM model of Glasgow et al.24 This model helps to focus on essential program elements for improving the sustainable adoption and implementation of effective, generalizable, and evidence-based interventions.25 The model uses the concepts Reach, Effectiveness, Adoption, Implementation, and Maintenance to translate research into action. Reach refers to the proportion of people who are willing to participate in an intervention, and in this study, it concerns the proportion of frail older patients with a high fall risk willing to participate in falls prevention interventions. Effectiveness refers to the impact of the intervention and will be assessed by the patient-related outcome measures such as fall incidents, balance, fear of falling, and quality of life (see Outcome measures). Adoption relates to the development of organizational support to deliver the intervention. This concept will be investigated by describing the proportion of GP practices of the GP care group that were willing to participate in this study. Implementation refers to how to ensure the intervention is delivered properly, and Maintenance relates to the long-term incorporation of the intervention. These last two concepts will be explored by identifying the experiences, barriers, and facilitators of the care providers when implementing and providing falls prevention. Table 1 provides an overview of the concepts of the RE-AIM model with the corresponding definitions, data sources, and the data to be collected.
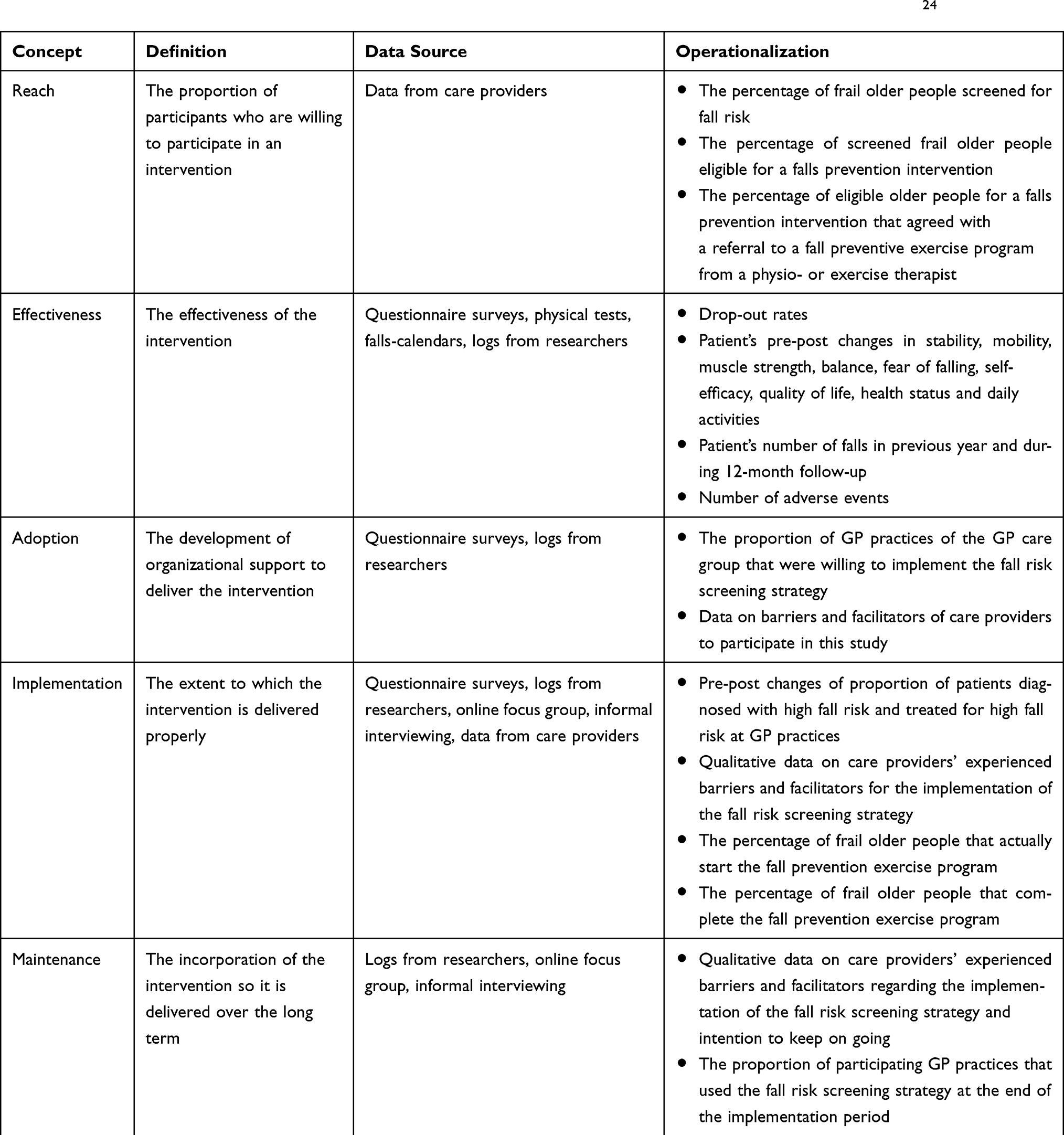 |
Table 1 Definitions, Data Sources and Operationalization of the Concepts of the RE-AIM Model of Glasgow et al24 |
Ethics and Dissemination
This study is approved by the Medical Ethics Committee Brabant, the Netherlands (NL61582.028.17/ P1732). The results from this study will be disseminated through peer-reviewed publications, through conference presentations, and by informing policymakers and consumers to maximize health impact.
Setting
In 2011, a home care organization and a GP care group (owned by 155 GPs) developed a strategy to improve healthcare for frail older people, which led to the Care Program for Frail Older People for the area Midden-Brabant, the Netherlands.26 Since 2014, other primary care providers (pharmacists, dieticians, occupational therapists) and secondary care providers (geriatricians) have also joined in the Care Program for Frail Older People. To date, 74 of the 155 GPs and their practice and district nurses have been participating in the program aimed at the coordination of healthcare for frail older people.27 As part of the program, frailty in older people is systematically diagnosed and registered. For the assessment of frailty, the TRAnsmuraal Zorg Assessment Geriatrie (TRAZAG) instrument or the Tilburg Frailty Indicator is used. TRAZAG makes use of several instruments to assess Activities Daily Living (ADL), instrumental ADLs, nutrition, mobility, fall risk, incontinence, medication, vision and hearing impairment, cognition and depressive symptoms.28,29 The Tilburg Frailty Indicator assesses demographics, physical, psychological, and social components of frailty.30,31 Each frail older person is assigned a care coordinator, and a care plan is drafted, which is evaluated during bimonthly multidisciplinary consultations. Although falls prevention is one of the priorities of the Care Program for Frail Older People, not every GP in the GP care group provides falls prevention in a systematic manner and if falls prevention is provided, the quality varies between practices. According to unpublished data obtained from an informal focus group with GPs, practice nurses and district nurses from the GP care group, some GPs immediately take action when they know a patient has fallen once while other GPs might take action after they know a patient has fallen several times. Therefore, the care group wants to promote the implementation of a targeted fall risk screening strategy among all their GPs. More information about the Dutch primary health care setting, in general, can be found in the report of Schäfer et al.32
Patient and Public Involvement
Although we tried to set up a patient advisory group consisting of frail older people, we did not succeed, mainly due to transportation and health issues. Therefore, before starting the implementation of the targeted fall risk screening strategy, we interviewed five frail older people and an informal focus group was conducted with GPs and practice and district nurses to investigate their needs and wishes regarding falls prevention. In addition, an advisory board consisting of two frail older people and important stakeholders (ie, physiotherapists; representatives of the municipality, a home care organization, and the GP care group; and researchers of other falls prevention studies in the Netherlands) will meet annually to discuss the set-up, execution, and results of the study.
Participants
GP Practices
All GP practices from the GP care group are invited to participate in this study through emails, letters, presentations, and face-to-face visits. Furthermore, the consultant of the GP care group and a GP specialized in geriatric care involved in this study will approach GPs and practice nurses in person or by phone for participation.
Physio- and Exercise Therapists
Physio- and exercise therapists are recruited through emails sent via the Royal Dutch Association for Physiotherapy (Dutch: "Koninklijk Nederlands Genootschap voor Fysiotherapie, KNGF") or by phone by the research team. Therapists are eligible to participate in this study if they are certified to offer an evidence-based falls prevention intervention or if they are willing to participate in an evidence-based falls prevention training program.
Patients
Patients are eligible to participate if they meet all of the following inclusion criteria:
- speak Dutch or English;
- are aged 70 years or older;
- have the cognitive capacity to give informed consent according to their GPs’ professional expertise;
- are classified as frail by their GPs based on the Tilburg Frailty Indicator (TFI),30 the TRAZAG Start Document,28 another frailty screening strategy, or the GPs’ professional expertise;
- have a high fall risk according to the validated fall risk screening instrument (see Appendix I) or according to the professional expertise of their GPs;
- have a Care Intensity Package (CIP; Dutch: "Zorg Zwaarte Pakket") between one and five. The CIP indicates the type and intensity of the required care. For CIP 5 and above, patients do not live independently anymore.
Patients are not eligible to participate in this study if they meet one of the following exclusion criteria:
- are currently participating in a physio- or exercise therapist’s falls prevention intervention;
- have moderate to severe communication restrictions or impairments according to the professional expertise of their GPs;
- are not healthy enough to participate in this study according to the professional expertise of their GPs (for example, life expectancy <2 year).
Interventions from Physio- or Exercise Therapists
When frail older patients with a high fall risk are referred to physio- or exercise therapists, the therapists will offer the patients one of the falls prevention interventions presented in Table 2.33–40 These interventions are described as qualified evidence-based falls prevention exercise programs by the Dutch Center for Healthy Living.41,42 This Center maintains a database containing preventive interventions available in the Netherlands ranked by level of evidence.42 The physio- or exercise therapists offer evidence-based falls prevention interventions tailored to the needs and wishes of the patient. If several exercise programs are available within the region, the patient will be referred to the intervention that best suits the patient’s individual needs.
Because not all physio- and exercise therapists in the area are certified to provide these falls prevention interventions, they are offered the falls prevention intervention training A Matter of Balance-NL (Dutch: “Zicht op Evenwicht”).
Study Procedure
The five steps below describe the evaluation process of the targeted fall risk screening strategy at the level of both the GP practice and the patient. In addition, Appendix II provides flowcharts describing the steps for 1) the set-up of the implementation of the targeted fall risk screening strategy, 2) the data collection at the GP practices, 3) the data collection from physio-and exercise therapists and 4) the data collection among the frail older patients.
STEP 1: Identification of Important Factors for the Fall Risk Screening Strategy
Before starting the implementation of the targeted fall risk screening strategy, an informal focus group with six to eight GPs and practice and district nurses will be organized.43 During this focus group, the primary care providers’ needs and wishes regarding falls prevention and a fall risk screening instrument will be explored. Subsequently, a systematic literature study will be conducted to identify a validated fall risk screening instrument that best meets their needs and wishes.
Furthermore, about five informal interviews will be conducted with frail older people who had a fall. During these interviews, patients’ perspectives, experiences, needs, wishes, barriers, and facilitators regarding falls prevention will be identified. These interviews will provide insight into how to approach and treat frail older patients with an increased risk of falling (See Appendix II, Flow Figure 1)
STEP 2: Assessment of Current Care
To assess current care, the participating GP practices will receive a short questionnaire regarding the number of frail older patients screened for fall risk, referred to falls prevention interventions, and enrolled in a falls prevention exercise program during the previous 12 months. In addition, the care providers will describe the barriers and facilitators they encountered in the provision of falls prevention. This self-reported data act as baseline data for the evaluation of the targeted fall risk screening strategy at GP practice level (See Appendix II, Flow Figure 2)
STEP 3: Provision of Tools to Implement the Fall Risk Screening Strategy
The GP care group’s GPs and practice nurses will be invited for a training program on the targeted fall risk screening strategy. Besides the screening for fall risk instruction, attention will be paid to the psychosocial barriers of older people to participate in falls prevention. For example, as indicated in the literature, patients’ pride and concerns with public appearance are important reasons to decline participation in a falls prevention program.44 Additionally, the GPs and practice nurses will receive both a checklist to diagnose the underlying cause of the fall risk (see Appendix I) and an overview of certified physio- and exercise therapists who are able to offer evidence-based falls prevention interventions in the surrounding area (see Table 2). They will also be offered the possibility to follow a four-hour training session concerning falls prevention for health care professionals (See Appendix II, Flow Figure 1)
 |
Table 2 Evidence-Based Falls Prevention Interventions |
STEP 4: Implementation of the Fall Risk Screening Strategy
The majority of the GP practices already systematically assess patients for frailty based on the Tilburg Frailty Indicator (TFI),30 the TRAZAG Start Document, or their own professional expertise.28,29 The screening for fall risk will be added to this systematic frailty screening. The integration of falls prevention within existing protocols and guidelines of GP care groups is expected to positively influence implementation. Patients who are eligible and interested in participating in this study will receive a flyer, a patient information letter, and an informed consent form. In addition, the practice nurse will contact the patients by phone in case they need any further information about the study.
Based on the patients’ risk profiles, the GPs (or the practice nurses) will offer the patients an intervention to reduce their high fall risk, such as a referral to an exercise program offered by a certified physio- or exercise therapist in the neighborhood, treatment of urine incontinence, and/or adjustment of medication. (See Appendix II, and Flow Figure 4)
STEP 5: Evaluation of the Implementation of the Fall Risk Screening Strategy
To evaluate the implementation of the targeted fall risk screening strategy at the level of the GP practice, data regarding the GP practice’s number of screened, referred, and enrolled frail older patients for falls prevention as a percentage of the total number of frail older patients will be collected. Furthermore, an online focus group and informal interviews will be conducted with participating GPs and practices nurses, and an online focus group will be conducted with participating physio- and exercise therapists. Data from the online focus groups and informal interviews will be used to identify barriers and facilitators regarding the implementation of the fall risk screening strategy and to identify the care providers’ intention to continue using the fall risk screening strategy. Additionally, logs will be kept by the researchers to keep track of the proportion of GPs that wanted to participate in this study and the proportion of GPs that used the fall risk screening strategy at the end of the study (see Table 1) (See Appendix II, Flow Figure 2).
To evaluate the influence of the falls prevention interventions at patient level, frail older patients will be divided into the following four groups after they have been diagnosed with high fall risk:
Group 1: Patients who want to participate in the study are referred to a falls prevention intervention from a physio- or exercise therapist, and may or may not receive treatment from the GP, for example, for urine incontinence, vision problems, or medication adjustment.
Group 2: Patients who want to participate in the study and are not referred to a physio- or exercise therapist but are treated by the GP, for example, for urine incontinence, vision problems, or medication adjustment.
Group 3: Patients who want to participate in the study but do not want to be treated for high fall risk.
Group 4: Patients who do not want to participate in this study and, therefore, cannot be followed up.
Patients from group 1 will receive a more intensive followed-up to investigate the influence of the exercise program offered by certified physio- and exercise therapists. During a 12-month follow-up, all participating frail older patients will be assessed using the outcome measures described below, see paragraph Outcome measures.
In addition, a few randomly selected patients from groups 1 and 2 will be interviewed to explore their experiences with the fall preventive care received (See Appendix II, Flow Figure 3 and Flow Figure 4)
Outcome Measures
The targeted fall risk screening strategy will be evaluated at the level of the GP practice by using the following outcome measures:
- the percentage of frail older patients screened for fall risk;
- the percentage of screened frail older patients eligible for a falls prevention intervention;
- the percentage of older patients eligible for a falls prevention intervention who agreed to participate in a falls prevention exercise program;
- the percentage of frail older patients that start the falls prevention exercise program;
- the percentage of frail older patients that complete the falls prevention exercise program.
The influence of the falls prevention interventions at patient level will be assessed by using the following outcome measures:
- Functional Reach Test to assess stability45–47
- Timed-Get-Up-and-Go Test to assess mobility;48–51
- Timed Chair Stand Test to assess muscle strength;52–54
- Tandem Stance Test to assess balance;55,56
- Short Falls Efficacy Scale-International to assess fear of falling and self-efficacy;57,58
- EQ-5D-5L to measure health status;59,60
- a 5-item questionnaire to assess fall history;
- a 5-item questionnaire to assess patients own perspectives on their health status;
- a 5-item questionnaire on daily activities;
- a 3-item questionnaire to assess which intervention(s) the patient received to prevent falls.
As described above, frail older patients are divided into four groups after they have been diagnosed with high fall risk. Figure 1A and B show which assessments are conducted in each group of patients. Additionally, all participants keep track of their falls during the 12-month follow-up with the help of daily falls calendars. The calendars will be sent to the researchers on a monthly basis. If a fall occurs, the researcher will phone the patient to ask a few questions about the cause of the fall, any related injuries, and hospital admission. If a patient fails to send the calendars, the researcher will call the patient and ask about the occurrence of any falls in the previous month.
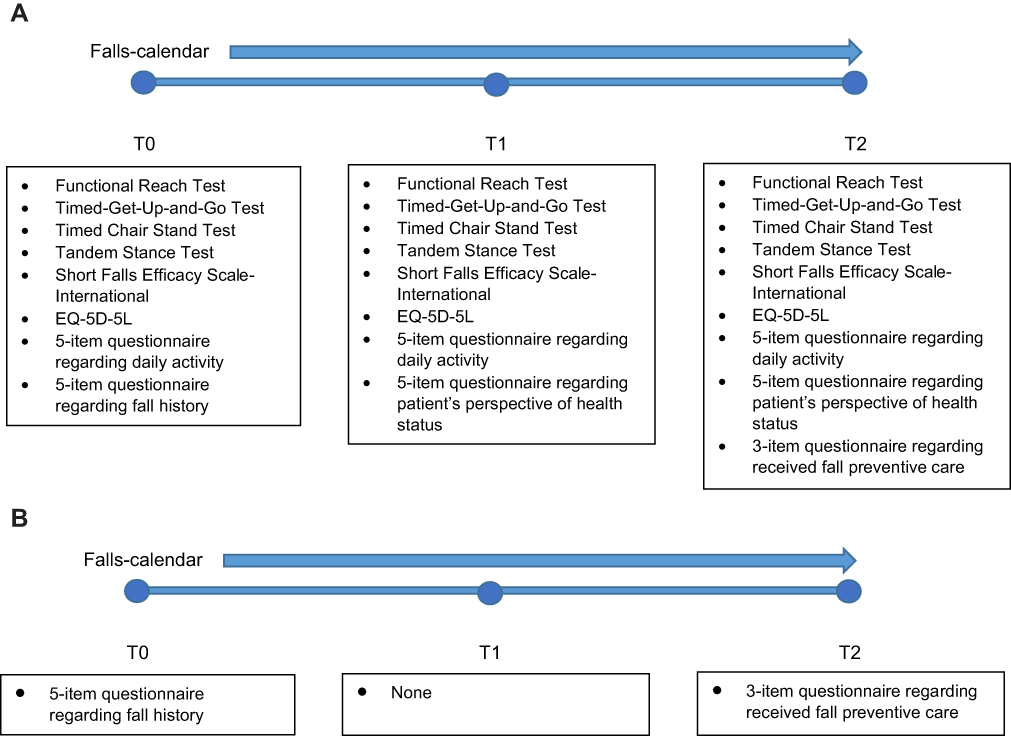 |
Figure 1 (A) Timeline assessments of group 1 patients who receive an intervention from a physio- or exercise therapist before intervention starts (T0), directly after the intervention (T1) and 12 months after starting the intervention (T2). (B) Timeline assessments of group 2 and group 3 patients who do not receive an intervention from a physio- or exercise therapist before intervention starts (T0), directly after the intervention (T1) and 12 months after starting the intervention (T2). |
Analysis
Data regarding the evaluation of the implementation of the fall risk screening strategy at GP practice level will be analyzed by using descriptive analysis in SPSS.61 Data from the standardized performance tests and questionnaires will be used to investigate the influence of the falls prevention interventions at patient level. The data will be analyzed by conducting a multilevel analysis for longitudinal data, adjusted for potential confounders.
Interviews with participating patients will be conducted until data saturation, when no new themes emerge in the analysis, is reached. The interviews will be transcribed. The interviews and online focus groups will be open coded by two researchers. The codes will be discussed and a coding scheme will be developed from the different themes that emerge. The interviews and online focus groups will be selective coded and compared by two researchers. After consensus has been reached, the coding will be thematic analyzed using the ATLAS.ti 8 coding program for qualitative data analysis.62
Sample Size Calculation
A sample size calculation was conducted based on the study of Schoon who stated that GPs in the Netherlands know of 20–30% of the falls among their older patients.15 Furthermore, according to a report by Seymour, 11% of the people with moderate or severe frailty are registered to have experienced a fall.63 Considering that of the overall population of frail older people in the Netherlands about 20% are diagnosed with high fall risk and 30% in the intervention population, 137 frail older people will be required to achieve 80% power (type II error of 0.20) with a type I error of 5%. The complete sample size calculation can be found in Appendix III.
Discussion
The primary objective of this study is to evaluate the implementation of a targeted fall risk screening strategy among independently living, frail older people in the primary care setting. In the Netherlands, as well as in many other countries, GPs are often the first point of contact for health issues.64 They have insight into the patient’s medical history, home setting, and social network. Therefore, they appear to be the designated professional for recognizing and offering falls prevention. An expected result of this study is that the targeted fall risk screening strategy will support GPs and practice nurses in their daily practice routines when it comes to recognizing high fall risk and offering falls prevention. The care providers might also become more aware of the importance of falls prevention. Therefore, compared to the usual care, the targeted fall risk screening strategy is expected to lead to more referrals to falls prevention interventions.
We expect that the targeted fall risk screening strategy will make falls prevention interventions more accessible to frail older people and, consequently, reduce falls. This expectation can be supported by Rubenstein, who concluded in his study that detection and amelioration of fall risk factors can reduce falls.65 Older people are often not aware of having a high fall risk, and they are often unfamiliar with the available fall preventive services. When primary care providers help older patients to gain access to fall preventive services, this could result in better health outcomes for these patients. Falls and patients’ fear of falling can be reduced and patients’ balance, strength, confidence, quality of life, and independence might be maintained or improved. These health outcomes can result in a reduction in hospital admissions, revalidation treatments, and other related treatments, which in turn could lead to a reduction in health care costs.66 Overall, this would be a more efficient provision of health care. Moreover, we expect that the results of this study will add valuable information to the knowledge of the systematic implementation of falls prevention for those who need a tailored treatment geared to their personal situations. Previous research often investigated the effect of falls prevention interventions in a controlled setting. This means that, at the moment, only scarce evidence is available about the effectiveness of multifactorial programs preventing falls among older people in a real-life setting.14,67
Furthermore, this study will provide important insights into the experienced barriers and facilitators when implementing falls prevention at GP practices. Child et al concluded in their literature review that “factors underpinning the successful implementation of fall-prevention programmes are complex” and that “no single factor can be identified as key facilitator”.44 One of the factors pointed out by Child et al is the importance of access to falls prevention interventions. Interventions to prevent falls are offered on a limited scale in the primary care setting, both internationally68 and in the Netherlands.69 This is obviated in the current study by recruiting certified physio- and exercise who are able to offer evidence-based falls prevention interventions.
Protocol Adaptations
Originally, this prospective cohort study consisted of two parts with two different research designs to evaluate the targeted fall risk screening strategy (see The Netherlands National Trial Register: NL7917). First, we wanted to use a quasi-experimental design to evaluate the screening strategy at the level of the GP practice. The intervention group, consisting of GPs participating in the Care Program for Frail Older People of the GP care group, would have been compared to a non-randomized comparison group of GPs who provide care as usual for a period of 12 months. However, during the study, the quasi-experimental design was changed into a pre-posttest design. Recruitment of GPs for the intervention group turned out to be more difficult than expected, and it took 1 year longer than anticipated. Some GP practices started with the implementation in January 2018 and others in January 2019. As a result, the time available for the implementation and evaluation of the targeted fall risk screening strategy differed among GP practices of the intervention group (follow-up between 4 and 16 months). The control group, on the other hand, received follow-up for a period of 12 months. This made an adequate comparison between the two groups impossible. Therefore, we decided to change the quasi-experimental design to a pre- posttest design. In the second part of the study, we intended to use a pre- posttest design to evaluate the influence of falls prevention interventions on patients. This pre-posttest did not change. We did not have a control group in this part of the study because it would be unethical to prevent patients at risk of falling from participating in a falls prevention program. Health care providers should offer all eligible patients adequate care.
Abbreviations
GP, general practitioner; ED, emergency department; TRAZAG, Transmuraal Zorg Assessment Geriatrie; TFI, Tilburg Frailty Indicator.
Ethics Approval and Informed Consent
This study is approved by the Medical Ethics Committee Brabant, the Netherlands (NL61582.028.17/ P1732).
Acknowledgments
We would like to thank Zorggroep RCH; Thebe Wijkverpleging; and all participating GPs, practice nurses, district nurses, physio- and exercise therapists, and patients for their support and participation in this study.
Author Contributions
All authors made substantial contributions to the conception and design of the study and acquisition, analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Disclosure
J.C Korevaar reports grants from Ministry of Health, during the conduct of the study. The authors report no other potential conflicts of interests in this work.
References
1. World Health Organization. Falls, Fact sheet. 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/falls.
2. Desforges JF, Tinetti M, Speechley M. Prevention of falls among the elderly. N Engl J Med. 1989;320(16):1055–1059. doi:10.1056/NEJM198904203201606
3. Tinetti ME. Where is the vision for fall prevention? J Am Geriatr Soc. 2001;49(5):676–677. doi:10.1046/j.1532-5415.2001.49132.x
4. Deandrea S, Lucenteforte E, Bravi F, Foschi R, La Vecchia C, Negri E. Risk factors for falls in community-dwelling older people:” a systematic review and meta-analysis”. Epidemiology. 2010;21(5):658–668. doi:10.1097/EDE.0b013e3181e89905
5. Terroso M, Rosa N, Marques AT, Simoes R. Physical consequences of falls in the elderly: a literature review from 1995 to 2010. Eur Rev Aging Phy Act. 2014;11(1):51–59. doi:10.1007/s11556-013-0134-8
6. Van der Does H, Baan A, Panneman M Privé-ongevallen bij ouderen, Cijfers valongevallen in de privésfeer 2018. VeiligheidNL;2019. Available from: https://www.veiligheid.nl/.ibmmodres/domino/OpenAttachment/Veiligheid/Website.nsf/8A4AF131AEE9AD92C12584950034833B/asset/Cijferrapportage%20Valongevallen%20ouderen%20in%20de%20priv%C3%A9sfeer%202018.pdf.
7. Balzer K, Bremer M, Schramm S, Luhmann D, Raspe H. Falls prevention for the elderly. GMS Health Technol Assess. 2012;8:Doc01.
8. Tricco AC, Thomas SM, Veroniki AA, et al. Comparisons of interventions for preventing falls in older adults: a systematic review and meta-analysis. JAMA. 2017;318(17):1687–1699. doi:10.1001/jama.2017.15006
9. Sherrington C, Michaleff ZA, Fairhall N, et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med. 2017;51(24):1750–1758. doi:10.1136/bjsports-2016-096547
10. Luk JKH, Chan TY, Chan DKY. Falls prevention in the elderly: translating evidence into practice. Hong Kong Med J. 2015;21(2):165–171. doi:10.12809/hkmj144469
11. Hopewell S, Adedire O, Copsey BJ, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2018;7.
12. Sherrington C, Fairhall NJ, Wallbank GK, et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2019;1.
13. Force UPST. Interventions to prevent falls in community-dwelling older adults: US preventive services task force recommendation statement. JAMA. 2018;319(16):1696–1704. doi:10.1001/jama.2018.3097
14. Glasgow RE, Lichtenstein E, Marcus AC. Why don’t we see more translation of health promotion research to practice? Rethinking the efficacy-to-effectiveness transition. Am J Public Health. 2003;93(8):1261–1267. doi:10.2105/AJPH.93.8.1261
15. Schoon Y. Vallen, een systematische benadering bij het zoeken naar de oorzaak. Bijblijven. 2013;29(6):12–18. doi:10.1007/s12414-013-0057-3
16. Mackenzie L, McIntyre A. How do general practitioners (GPs) engage in falls prevention with older people? A pilot survey of GPs in NHS England suggests a gap in routine practice to address falls prevention. Front Public Health. 2019;7.
17. Mueller CA, Klaaßen-Mielke R, Penner E, Junius-Walker U, Hummers-Pradier E, Theile G. Disclosure of new health problems and intervention planning using a geriatric assessment in a primary care setting. Croat Med J. 2010;51(6):493–500. doi:10.3325/cmj.2010.51.493
18. Vetter N, Lewis P. Reasons for poor detection of frequent falls in elderly people by general practitioners. Aging Clin Exp Res. 1995;7(6):430–432. doi:10.1007/BF03324357
19. Paul S. Falls: prevention and management. Geriatric Med. 2018;109–119.
20. VeiligheidNL, VVaN. Valanalyse, screeningtool valrisico voor de eerstelijnszorg. VeiligheidNL;2015. Available from: https://www.veiligheid.nl/valpreventie/interventies/screening/valanalyse.
21. World Health Organization, ALCU. WHO Global Report on Falls Prevention in Older Age. World Health Organization; 2008.
22. Federatie Medisch Specialisten. Richtlijn, Preventie van valincidenten bij ouderen. 2017. Available from: https://mijn.venvn.nl/databanken/richtlijnen/Lists/Databank%20richtlijnen/Attachments/175/Preventie_van_valincidenten_bij_ouderen.pdf.
23. Basiscursus valpreventie voor professionals. [webpage on the Internet]. Netherlands: VeiligheidNL; 2019. Available from: https://www.veiligheid.nl/valpreventie/trainingen/basiscursus-valpreventie-voor-professionals.
24. Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89(9):1322–1327. doi:10.2105/AJPH.89.9.1322
25. RE-AIM. What is RE-AIM [webpage on the Internet].; 2019. Available from: http://www.re-aim.org/about/what-is-re-aim.
26. Zorggroep RCH Midden-Brabant. Zorgprogramma kwetsbare ouderen. 2020. Available from: https://www.rchmbr.nl/fileadmin/RCH/Zorg/Ouderenzorg/RCH20.158-1.0_Zorgprogramma_kwetsbare_ouderen.pdf.
27. Zorggroep RCH Midden-Brabant. Jaarverslag Zorggroep RCH Midden-Brabant 2017. 2017. Available from: https://www.rchmbr.nl/fileadmin/RCH/Over_RCH/RCH18.481-1.0_Jaarverslag_2017_Zorggroep_RCH.pdf.
28. Warnier R. TraZAG: transmuraal zorg assessment Geriatrie Maastricht. Tijdschr Gezondh Ethiek. 2012;22(3):93.
29. Warnier R TRAnsmuraal Zorg Assessment Geriatrie, Complexe zorg voor thuiswonende ouderen. 2011. Available from: http://www.platformouderenzorg.nl/bestanden/trazag_vierde_druk_inleiding.pdf.
30. Gobbens RJJ, van Assen MALM, Luijkx KG, Wijnen-Sponselee MT, Schols JMGA. The Tilburg Frailty Indicator: psychometric properties. J Am Med Dir Assoc. 2010;11(5):344–355. doi:10.1016/j.jamda.2009.11.003
31. Metzelthin SF, Daniëls R, van Rossum E, de Witte L, van den Heuvel WJ, Kempen GI. The psychometric properties of three self-report screening instruments for identifying frail older people in the community. BMC Public Health. 2010;10(1):176. doi:10.1186/1471-2458-10-176
32. Schäfer W, Kroneman M, Boerma W, et al. The Netherlands: health system review. 2010.
33. Zijlstra GAR, van Haastregt JCM, Du Moulin MFMT, de Jonge MC, van der Poel A, Kempen GIJM. Effects of the implementation of an evidence-based program to manage concerns about falls in older adults. Gerontologist. 2012;53(5):839–849. doi:10.1093/geront/gns142
34. Zijlstra GAR, van Haastregt JCM, Kempen GIJM. ‘Zicht op Evenwicht’: een effectieve interventie om bezorgdheid om te vallen en gerelateerd vermijdingsgedrag bij ouderen te verminderen. Tijdschr Gerontol Geriatr. 2012;43(4):164–174. doi:10.1007/s12439-012-0026-9
35. Faber MJ, Bosscher RJ, Chin A, Paw MJ, van Wieringen PC. Effects of exercise programs on falls and mobility in frail and pre-frail older adults: a multicenter randomized controlled trial. Arch Phys Med Rehabil. 2006;87(7):885–896. doi:10.1016/j.apmr.2006.04.005
36. Weerdesteyn V, Rijken H, Geurts ACH, Smits-Engelsman BCM, Mulder T, Duysens J. A five-week exercise program can reduce falls and improve obstacle avoidance in the elderly. Gerontology. 2006;52(3):131–141. doi:10.1159/000091822
37. Campbell AJ, Robertson MC, Gardner MM, Norton RN, Buchner DM. Falls prevention over 2 years: a randomized controlled trial in women 80 years and older. Age Ageing. 1999;28(6):513–518. doi:10.1093/ageing/28.6.513
38. Campbell AJ, Robertson MC, Gardner MM, Norton RN, Tilyard MW, Buchner DM. Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women. BMJ. 1997;315(7115):1065–1069. doi:10.1136/bmj.315.7115.1065
39. Robertson MC, Devlin N, Gardner MM, Campbell AJ. Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls. 1: randomised controlled trial. BMJ. 2001;322(7288):697–701. doi:10.1136/bmj.322.7288.697
40. Robertson MC, Gardner MM, Devlin N, McGee R, Campbell AJ. Effectiveness and economic evaluation of a nurse delivered home exercise programme to prevent falls. 2: controlled trial in multiple centres. BMJ. 2001;322(7288):701–704. doi:10.1136/bmj.322.7288.701
41. Interventies zoeken [webpage on the Internet]. Netherlands: Loketgezondleven, Rijksinstituut voor Volksgezondheid en Milieu; 2019. Available from: https://interventies.loketgezondleven.nl/leefstijlinterventies/interventies-zoeken?trefwoord=&title=0&approved=&theme=A09i_VALPREV&setting=&target=&organisation=&review=&methodology=.
42. Movisie N, Nisb N, Ji RIVM. Dutch Recognition System for Interventions. Criteria for Joint Quality Assessment 2013-2018; 2013.
43. Creswell JW, Creswell JD. Research Design: Qualitative. Sage publications; 2017.
44. Child S, Goodwin V, Garside R, Jones-Hughes T, Boddy K, Stein K. Factors influencing the implementation of fall-prevention programmes: a systematic review and synthesis of qualitative studies. Implement Sci. 2012;7.
45. Duncan PW, Weiner DK, Chandler J, Studenski S. Functional Reach: a new clinical measure of balance. J Gerontol. 1990;45(6):M192–M197. doi:10.1093/geronj/45.6.M192
46. Jonsson E, Henriksson M, Hirschfeld H. Does the functional reach test reflect stability limits in elderly people? J Rehabil Med. 2003;35(1):26–30. doi:10.1080/16501970306099
47. Weiner DK, Duncan PW, Chandler J, Studenski SA. Functional Reach: a marker of physical frailty. J Am Geriatr Soc. 1992;40(3):203–207. doi:10.1111/j.1532-5415.1992.tb02068.x
48. Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the” get-up and go” test. Arch Phys Med Rehabil. 1986;67(6):387–389.
49. Schmitz T, Wagner J Uitgebreide toelichting van het meetinstrument Timed Up & Go test (TUG). 2014. Available from: https://meetinstrumentenzorg.nl/wp-content/uploads/instrumenten/TUG-form.pdf.
50. Podsiadlo D, Richardson S. The Timed up and Go - a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
51. Van Wegen EEH, LIIK L-DV, Nieuwboer A, et al. Klinimetrie bij de ziekte van Parkinson, een praktische handleiding. In: Klinimetrie Bij De Ziekte Van Parkinson, Een Praktische Handleiding NPI. Amersfoort; 2005.
52. Csuka M, McCarty DJ. Simple method for measurement of lower extremity muscle strength. Am J Med. 1985;78(1):77–81. doi:10.1016/0002-9343(85)90465-6
53. Hayes KW, Johnson ME. Measures of adult general performance tests: the Berg Balance Scale, Dynamic Gait Index (DGI), Gait Velocity, Physical Performance Test (PPT), Timed Chair Stand Test, Timed Up and Go, and Tinetti Performance‐Oriented Mobility Assessment (POMA). Arthritis Care Res. 2003;49(S5):S28–S42. doi:10.1002/art.11411
54. Mijnarends DM, Meijers JM, Halfens RJ, et al. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: a systematic review. J Am Med Dir Assoc. 2013;14(3):170–178. doi:10.1016/j.jamda.2012.10.009
55. van Abbema R, de Vries NM, Weening-Dijksterhuis E, de Greef MHG, Hobbelen JSM. KNGF standaard Beweeginterventie kwetsbare ouderen. 2015. Available from: https://research.hanze.nl/ws/portalfiles/portal/5899891/standaard_bi_kwetsbare_ouderen_2015.pdf.
56. Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85–94. doi:10.1093/geronj/49.2.M85
57. Kempen GIJM, Todd CJ, Van Haastregt JCM, et al. Cross-cultural validation of the Falls Efficacy Scale International (FES-I) in older people: results from Germany, the Netherlands and the UK were satisfactory. Disabil Rehabil. 2007;29(2):155–162. doi:10.1080/09638280600747637
58. Kempen GI, Yardley L, van Haastregt JC, et al. The Short FES-I: a shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing. 2008;37(1):45–50. doi:10.1093/ageing/afm157
59. The EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy (New York). 1990;16(3):199–208. doi:10.1016/0168-8510(90)90421-9
60. Van Reesen M, Janssen B. EQ-5D-5L User Guide, Basic Information on How to Use the EQ-5D-5L Instrument. Rotterdam: EuroQol Research Foundation;2015.
61. IBM. SPSS Statistics for Windows, Version 25.0 [Computer Program]. Armonk, NY: IBM Corp; 2017.
62. ATLAS.ti 8 Windows [computer program]. 2002-2019.
63. Seymour D. One small step for older people with frailty, one giant leap for frailty care? An analysis of GP Contract Services data for routine frailty identification and frailty care through the GP Contract 2017/2018. Fusion. 2018;48.
64. Boerma WGW Profiles of general practice in Europe: An international study of variation in the tasks of general practitioners. 2003.
65. Rubenstein LZ. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing. 2006;35(Suppl 2):ii37–ii41. doi:10.1093/ageing/afl084
66. Olij BF, Ophuis RH, Polinder S, et al. Economic evaluations of falls prevention programs for older adults: a systematic review. J Am Geriatr Soc. 2018;66(11):2197–2204. doi:10.1111/jgs.15578
67. Saturni S, Bellini F, Braido F, et al. Randomized controlled trials and real life studies. Approaches and methodologies: a clinical point of view. Pulm Pharmacol Ther. 2014;27(2):129–138. doi:10.1016/j.pupt.2014.01.005
68. Phelan EA, Mahoney JE, Voit JC, Stevens JA. Assessment and management of fall risk in primary care settings. Med Clin North Am. 2015;99(2):281–293. doi:10.1016/j.mcna.2014.11.004
69. Koopmans B, Korevaar J, Nielen M, et al. NIVEL Overzichtstudies: preventie kan effectiever! Deelnamebereidheid en deelnametrouw aan preventieprogramma’s in de zorg. NIVEL. 2012.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.