")
Back to Journals » Clinical Interventions in Aging » Volume 16
Impaired Oral Health in Older Orthopaedic In-Care Patients: The Influence of Medication and Morbidity
Authors Andersson P, Kragh Ekstam A
Received 23 June 2021
Accepted for publication 24 August 2021
Published 18 September 2021 Volume 2021:16 Pages 1691—1702
DOI https://doi.org/10.2147/CIA.S326095
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Pia Andersson,1 Annika Kragh Ekstam2
1Department of Health Sciences, Kristianstad University, Kristianstad, SE-291 88, Sweden; 2Department of Orthopaedics, Region Skåne Office for Hospitals in North-Eastern Skåne, Kristianstad, SE-291 85, Sweden
Correspondence: Annika Kragh Ekstam Email [email protected]
Introduction: Fall-related injuries are prevalent in older patients and often lead to increased morbidity, medication, and impaired functions. We studied older trauma patients with the aim to describe their oral health in comparison to morbidity and medication.
Material and Methods: The study included 198 patients, ≥ 65 years, admitted with an orthopedic trauma. Oral examinations included number of natural teeth, dental implants, missing, decayed and restored teeth, root remnants, and pocket depth. Data on comorbidities and medication were assembled. Statistical analyses were carried out with logistic regression models, adjusted for age, gender, comorbidity, and polypharmacy.
Results: Overall, 198 patients participated, 71% women, mean age 81 years (± 7.9), 85% resided in their own homes, 86% had hip fractures. Chronic diseases and drug use were present in 98.9%, a mean of 6.67 in Charlson comorbidity index (CCI), 40% heart diseases, 17% diabetes, and 14% dementia. Ninety-one percent were dentate (181), mean number of teeth 19.2 (± 6.5), 24% had decayed teeth, 97% filled teeth, 44% < 20 teeth, and 26% oral dryness. DFT (decayed, filled teeth) over mean were identified in patients with diabetes (p=0.037), COPD (p=0.048), polypharmacy (p=0.011), diuretics (p=0.007), and inhalation drugs (p=0.032). Use of ≥ 2 strong anticholinergic drugs were observed in patients with < 20 teeth and DFT over mean (p=0.004, 0.003). Adjusted for age, gender, CCI, and polypharmacy.
Conclusion: The study showed that impaired oral health was prevalent in older trauma patients and that negative effects on oral health were significantly associated with chronic diseases and drug use. The results emphasize the importance of identifying orthogeriatric patients with oral health problems and to stress the necessity to uphold good oral care during a period when functional decline can be expected.
Keywords: oral health, orthogeriatric patients, risk factors, DFT, medication, comorbidity
Introduction
Fall injuries are a global public health problem and affects mainly older people (WHO, 2018. Falls). In Sweden approximately 50,000 individuals, 65 years and older, are hospitalized due to fall injuries every year and a majority of the affected are women, over 85 years (Public Health Agency of Sweden, 2020). Hip fractures and other fractures in the lower extremities are common injuries among older people and leads to hospitalization and in most cases surgery.1 Socio-economic factors, dementia and living conditions have been reported to be the main causes of falls that require hospitalization.2–5 Further major risk factors are Parkinson’s disease, dizziness, impaired walking, disturbed balance and use of medications.3,6,7 Many who are treated for fractures in the lower extremities will become more care-dependent in the daily life due to disabilities.8 Help with the daily activities and personal care, including oral hygiene, is important to avoid deteriorated oral health in fragile older individuals.9
Improvement in oral health status has been recorded in recent decades in Sweden and teeth retention is common in old age10 as well as in other countries.11 Impaired ability to perform oral hygiene and reduced salivary flow due to ageing, medications and chronic diseases may however increase the risk of oral conditions such as caries and periodontitis in older individuals.12–15 Associations have also been reported between oral diseases and other chronic diseases, such as heart disease, stroke, diabetes and dementia and the relations become more apparent with increased age.16 Furthermore, associations between number of teeth, periodontitis, masticatory function, number of oral health problems and frailty have been shown.17 Impaired oral health, especially reduced masticatory ability due to a low number of teeth, may interfere with eating and thereby negatively affect nutritional status, general health status and quality of life.18–20 It has also been reported that poor oral health is a risk factor for care associated pneumonia in elderly in both hospitals and nursing homes.21 Poor oral health status has been reported among older residents in nursing homes,22 hospitalized rehabilitation patients,18 and community-dwelling dependent older people.23 Barbe et al15 have reported that oral health is impaired in older orthopaedic patients with fall injuries. The knowledge about the oral health status in patients urgently admitted with different fractures in need of surgery is however limited and need to be further studied. These patients represent an old and often frail population that frequently will be care-dependent after a fall injury, and in need of help with daily activities including oral care.24,25
The aims of the present study were to examine the oral health status in hospitalized older orthopaedic patients and to compare the oral health results with the presence of other co-existing health variables such as chronic diseases and medication.
Methodology
Data Sources
This cross-sectional study took place at an emergency orthopaedic department in a hospital (255 beds) in the south of Sweden. The sample population was included consecutively during November 2016 to March 2019 among patients 65 years and older, urgently admitted to the department mainly due to fractures in the lower extremities and in need of emergency surgery. During the study period 504 eligible patients were admitted to the orthopaedic department. Consent to participate in the study was given by 240 patients (48%). Of these, 42 patients were excluded; five patients later withdrew their consent, four were moved to another ward or hospital, two died, two patients were below 65 years of age and in 29 patients the oral health examination was missing. In total 198 patients participated in the study. A drop-out analysis showed no statistical differences between gender and age in the included participants compared to patients who declined to participate.
Study Design
The study included assembly of data from medical records and an oral health examination. The patients were given written and verbal information about the study procedures from the care staff in the department before they decided to sign an informed consent. The medical data was compiled, by a physician (AKE), from the medical records kept for the patients. The oral health examination was conducted by two experienced dental hygienists and took place in relation to admission and performed in the patients’ room at the ward. The patients were either lying in their bed (the majority) or sitting in a comfortable chair during the examination that was conducted with light sources and standard dental instruments according to methods applicable in general dental care (WHO, Oral health survey. Basic methods. 2013). Calibration of the clinical procedures between the two dental hygienists was performed before the study and good inter-rater reliability was shown.
Demographic and Medical Data
The retrieved medical data included cause of admission, type of fracture or other urgent orthopaedic condition, comorbidities, medications, weight, and blood tests (creatinine). Included demographic data were age, gender, and whether the patients were community-dwellers or care home residents. The participants use of medications prior to admission was compiled from their medical records and divided into subgroups (see below) according to the drug’s potential influence on oral health. Only medications that were noted as taken on a regular basis were included. Drugs that are previously shown to have a detrimental effect on oral health, caused either by oral dryness or through other adverse side-effects, were included.9,26–28
Medications
The regular use of five or more drugs (polypharmacy) and ten or more drugs (severe polypharmacy) in the patients was analyzed. Drugs included in the analyses were categorized into groups according to the ATC system (Anatomical Therapeutic Chemical classification system) as to enable to compare the data with other studies. Drugs with potentially adverse effects on oral health, including oral dryness, comprised of all the here mentioned groups of medications. Among those analysed were diuretics (C03), drugs with effects on the renin-angiotensin system (C09), proton pump inhibitors (A02BC), antidepressants (N06A), antipsychotics (N05A), opioids (N02A), sedatives (N05C, N05B), and drugs with strong anticholinergic effects with high risk of causing oral dryness (A03AA, A03BA, A03AB, A03BB, A03C, A04AD, C01BA, G04BD, N02AG, N04A, N05AA, N05AB04, N05AC02, N05AF03, N05BB01, N06AA, R05CA10, R06AA02, R06AB, R06AD, and R06AX02).9,27–29 Furthermore, drugs with anticoagulative effects and potential risk of causing increased bleeding tendency (B01A), were also analysed.
Co-Morbidity
Several medical conditions and chronic diseases have been shown to correlate with negative influence on oral health, causing increased risk of developing periodontitis, gingivitis, dental plaque formations and oral dryness with reduced saliva quality or production.16,27 We included earlier identified related diagnosis such as diabetes, heart disease, dementia, Parkinson, rheumatic disease, and chronic obstructive pulmonary disease (COPD) in this study. Since kidney diseases and kidney dysfunction are common conditions in the older population and also known to have potentially negative effects on oral health30,31 an evaluation of renal function was carried out based on the estimated glomerular filtration rate (eGFR) which was calculated based on gender, age, weight, and plasma creatinine at admission.
The Charlson Comorbidity Index (CCI), age-adjusted, was used to describe the general morbidity of the patients and the mean value was used for comparison between groups.32,33
Oral Health Examination
In the clinical oral examination edentulousness, number of natural teeth, dental implants, missing teeth, decayed teeth, root remnants, teeth with restorations, pairs of teeth in contact, pocket depth, tooth mobility, gingival bleeding, dental plaque, saliva and breath odour were registered. Number of teeth was dichotomized into <20 teeth versus ≥20 teeth.34 Decayed (D) and filled (F) teeth (T) and DFT was used to describe the previous and present caries situation (WHO, 2013). When a carious cavity (tooth or root remnant) was apparent by visual inspection (manifest caries) the tooth was recorded as decayed. When there was doubt whether the tooth was decayed it was registered as free of caries. Periodontal pocket depth was assessed using the Ramfjord teeth, tooth number 16, 14, 21, 46, 41 and 34.35 When one of these teeth were missing an adjacent tooth was assessed in respective region of molars, premolars, or incisors. If this was not possible the tooth was recorded as missing. Pocket depth of ≥4 mm on the mesial, buccal, distal, and lingual surfaces was recorded from the free gingival margin to the base of the pocket using a millimetre-graded colour-coded periodontal probe.36 Oral dryness was measured by the nurses at the department by sliding a mouth mirror along the buccal mucosa37 and by grading according to the Revised Oral Assessment Guide (ROAG).18 The third molars were excluded from the clinical examination.
Ethics
The study was performed in accordance with the Declaration of Helsinki (Declaration of Helsinki, 2013) and permission was given by the Ethics Committee in Lund, Sweden (2016–199). Approval was also received by the head of the orthopaedic clinic, the head of the trauma unit and the doctor in charge of the trauma department. Written informed consent was given by the participating subjects and when needed, due to cognitive impairment, from next of kin representing the patient. Patients who were unable to cooperate for the oral status examination and those who could not understand the study procedure information in Swedish were excluded.
Statistical Analysis
Descriptive statistics for each variable were calculated using IBM SPSS Statistics version 26. Descriptive data were compared with relation to gender and age groups (65–79 years and ≥80 years). Data for continuous variables were presented as mean and standard deviation (SD), and categorical data as proportions (%). Continuous data was compared between groups with an unpaired Student’s t-test while a χ2-test or Fishers’ exact test was used for comparison of categorical data. Stepwise logistic regression analysis was applied to explore any associations between the independent clinical variables (diseases and drugs) in relation to oral health variables in patients with natural teeth: less than 20 teeth, pocket depth of 4 mm or more and DFT over mean 15 (dependent variables). Adjustments were made separately for possibly confounding factors such as age, comorbidity (CCI), and gender. One variable was also adjusted for polypharmacy: the use of two or more drugs with strong anticholinergic effects. These possible confounders were all included in the final multivariate regression model. Odds ratios (OR) with 95% confidence intervals (CI) were estimated to identify if any significant differences were present between the analysed oral health variables and the exposure to diseases or medications. P-values <0.05 and when the 95% confidence interval excluded 1.0 were regarded as statistically significant.
Results
The sample consisted of 198 patients (71% women) urgently admitted to an orthopaedic ward, Table 1. Mean age was 81 years (SD 7.9, range 65−100 years) and was the same for women and men. The patients were dichotomized into two age groups, based on the mean age and the mean survival age in Sweden (81 years in 2018), with age group 80 years and older represented in 59% of the sample (Table 1). Most of the patients were living in their own apartments or houses before admission while 15% lived in nursing homes (14% of the women and 17% of the men). After adjustments for age, gender and CCI there was no significant differences in oral health status found between community-dwelling participants and residents in nursing homes.
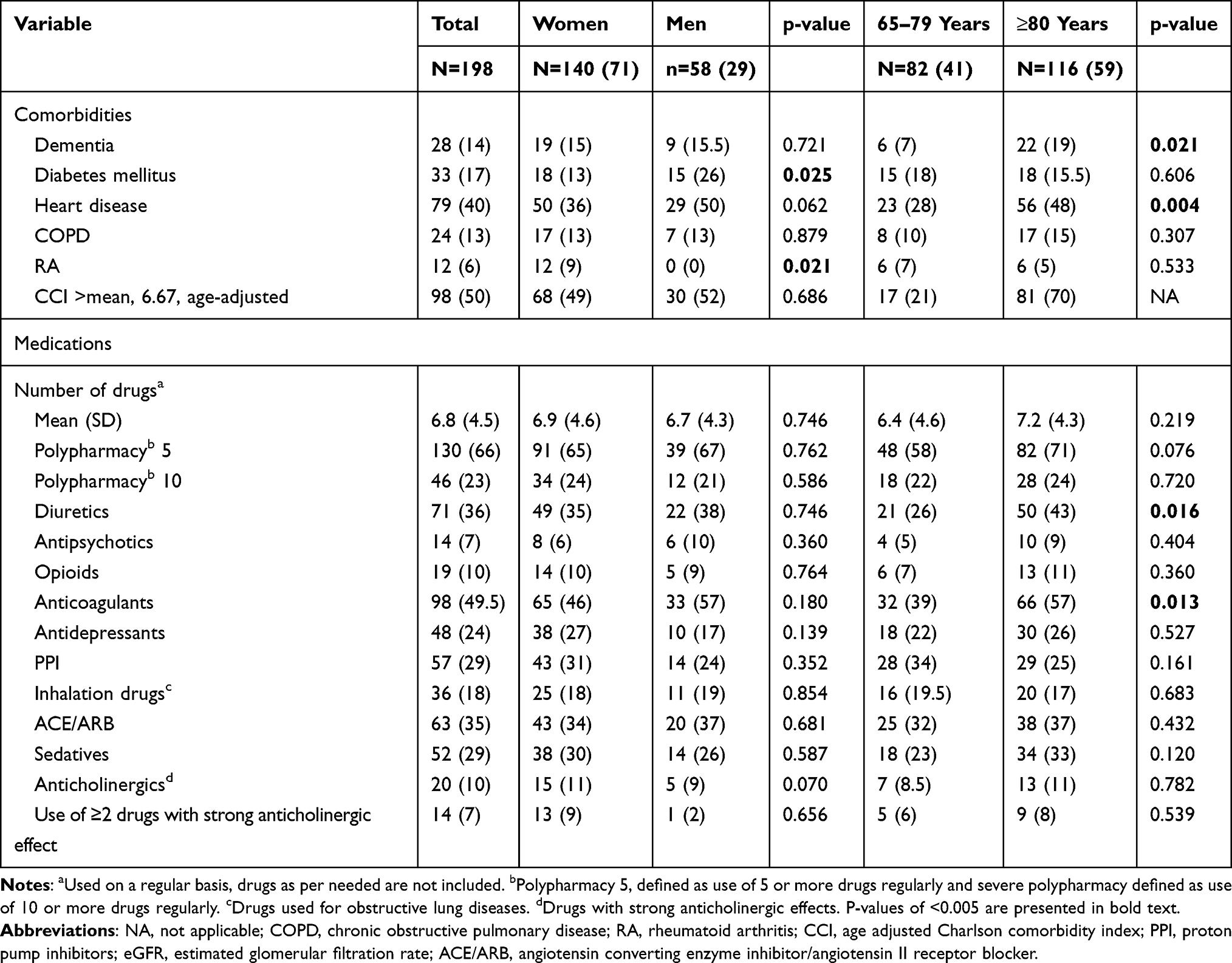 |
Table 1 Baseline Characteristics, Total and in Relation to Gender and Age Groups, 198 Patients, Number of Patients (%) |
The majority of the patients were urgently admitted to the hospital with fractures of the lower extremities and needed surgery. Fractures of the hip or femur were present in 171 patients (86%), with fractures of tibia occurring in 24 of the patients, while three patients needed amputation of the lower limb due to acute severe vascular insufficiency. After adjustments for age, gender and CCI there was no significant differences in oral health status found between patients with hip fractures compared to those with other fractures or vascular insufficiency.
Comorbidity
The evaluation of the patients’ comorbidity, using the age adjusted Charlson comorbidity index (CCI), resulted in a mean value for all participants of 6.67 (SD 2.8, range 1–15), with no difference seen between sexes. More than 40% of the patients suffered from heart diseases, 50% had moderate to low renal function and all but two patients (99%) had one or more chronic diseases. In the older participants dementia, heart disease, and Parkinson’s disease (not in table) were significantly more often present than in the younger patients, p=0.021, 0.004 and 0.023 respectively. Diabetes mellitus was more frequent in male participants (p=0.025) whereas rheumatoid arthritis was more often observed in women (p=0.021). Moderate to low kidney function, defined as eGFR (estimated glomerular filtration rate) lower than 60 mL/min, was present in 99 patients (50%) and the mean eGFR value of all patients was 50.9 mL/min (SD 21.0). An eGFR lower than 30 mL/min (severe renal dysfunction) was present in 13 patients (7%).
Medication
The mean number of drugs used regularly at admission was 6.8 (SD 4.5, range 0–25) with no significant differences between gender or age groups concerning the use of multiple drugs and only two patients did not use any drugs regularly. The number of patients treated on a regular basis with five or more drugs (polypharmacy) was 130 (66%) and severe polypharmacy, treatment with ten or more drugs, was present in 23% of the patients (Table 1).
There was no significant difference in the use of strong anticholinergic drugs between sexes or age groups and neither was there a difference in the use of multiple anticholinergic drugs. Treatment with inhalation drugs for COPD and other obstructive lung diseases was seen in 36 patients (18%) whereas the number of patients diagnosed with obstructive lung diseases was 24 (13%).
In the older group of patients, ≥80 years, the use of diuretics and anticoagulants were more frequent than in the younger participants, p=0.016 and 0.013 respectively (Table 1). A large part of the population, 50.5% (98 patients), was treated with drugs used for reducing blood clotting and therefore with a potential risk of increased oral bleeding. In the whole population 28% were treated with antiplatelet drugs and 21% with anticoagulants (not in table).
Oral Health Status
In the study population (n=198) 17 patients (9%) were edentulous and this was more frequent, 12%, in the older than in the younger patients, 4% (p= 0.037), but no significant difference was found between sexes. Natural teeth were present in 181 (91%) of the patients and they had a mean age of 81 years, 127 were women (70%) and 22 (12%) were nursing home residents. The mean number of natural teeth per patient was 19.2 (SD 6.5, range 2–28). The patients in the younger age group had in mean 20.5 (SD 6.5) natural teeth compared to 18.2 (SD 6.4) in the older patients (p=0.020) (not in table).
Almost all (97%) of the dentate patients had one or more (range 1–26) missing teeth. In 21 patients (12%) missing teeth were replaced with dental implants (range 1–12). Decayed teeth (range 1–17) were found in 24% of the patients, of which one single decayed tooth was present in 52% of them. Also, the majority of the patients (97%) had one or more filled teeth (range 1–28). In Table 2 is shown that fewer than 20 teeth were present in 44% of the dentate patients and that DFT was in mean 14.8 (SD 5.8). Furthermore, a CCI score over mean was associated with a DFT score over mean, p=0.002. Periodontal pocket depth of ≥4 mm was measured in 81% of the patients (Table 3) and the mean pocket depth was 5.3 (SD 5.1). Oral dryness was present in 26.5% of the patients (missing data n=11) and was more common in the older patients (p=0.003), no difference was seen between sexes. It was also significantly more frequently seen in patients with a CCI score higher than the mean, p=0.037.
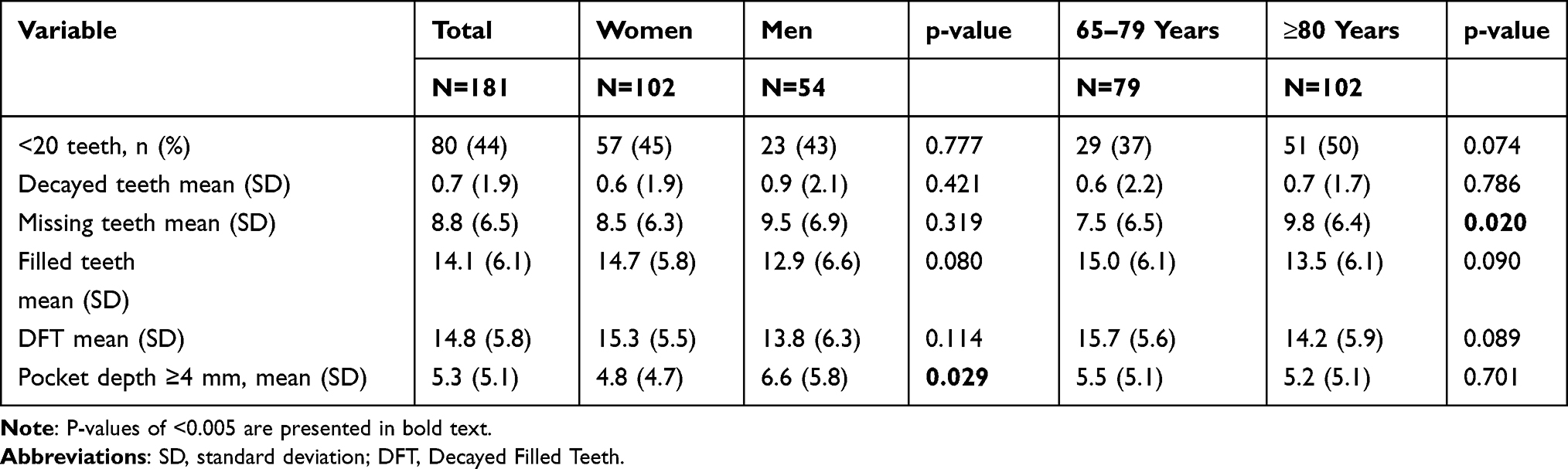 |
Table 2 Oral Health Status in Dentate Patients, Total and in Relation to Gender and Age Groups (n=181). |
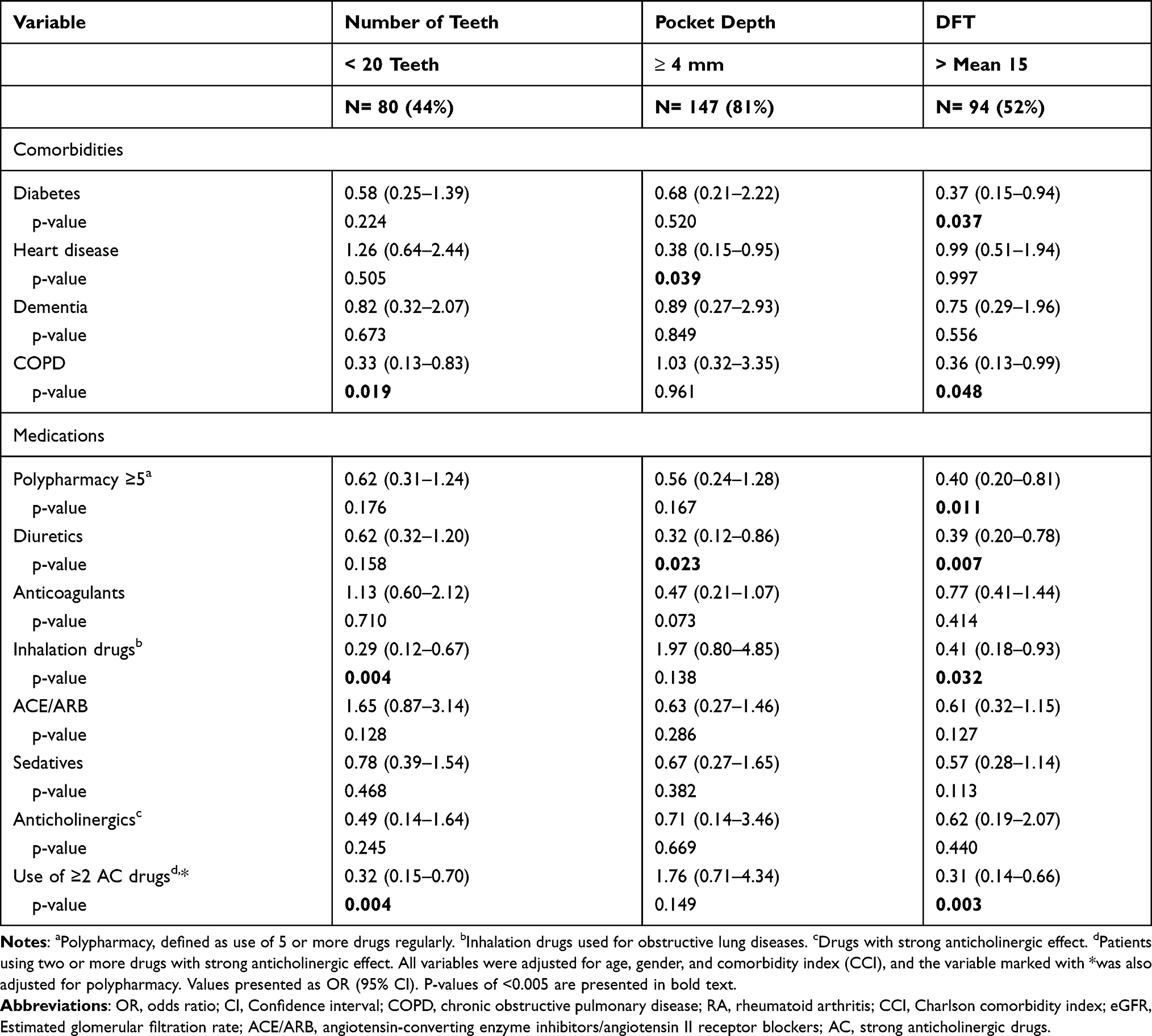 |
Table 3 Oral Health Status in Dentate Patients, in Relation to Comorbidities and Medications (n=181) |
Regression Analysis
As shown in Table 3, when data was adjusted for the possible confounders age, gender, CCI and, where appropriate, polypharmacy, probable associations were seen between the occurrence of a DFT over mean and both diabetes and COPD (p-values 0.037 and 0.048). Also, in patients treated with inhalation drugs for COPD fewer teeth, less than 20, was significantly more often observed, p-value 0.004.
The drug regimens that had probable significant associations with various aspects of impaired oral health, were mainly polypharmacy, diuretics, inhalation drugs used for COPD, and use of two or more drugs with strong anticholinergic effects. Both number of teeth fewer than 20 and a DFT over mean value were significantly more often prevalent in patients treated with two or more strong anticholinergic drugs (p-value 0.004 and 0.003 respectively). A significantly higher presence of pocket depth of 4 mm and over were seen in both patients with heart diseases and in those using diuretics, p-values 0.039 and 0.023 respectively.
Discussion
Among the results of this descriptive cross-sectional study in older hospitalized orthopaedic patients were that most of the patients had impaired oral health and nearly a quarter of them needed dental care due to manifest visible caries. Furthermore, probable associations were found between impaired oral health and heart diseases, diabetes, and COPD as well as treatment with diuretics, inhalations, polypharmacy, and two or more strong anticholinergic drugs.
This study covers, to our present knowledge, a seldom described population consisting of older people mainly living in their own homes, who were urgently admitted after a traumatic incidence leading to major fractures and in need of surgery. The study population encompassed a vulnerable category of patients due to the risk of complications associated with oral health problems, such as post-operative wound infections and delayed wound healing. The study also contributes to an enhanced knowledge of a mixed older population´s oral health and was carried out in collaboration between medical and dental care professionals.
Oral Health
A considerable amount of dental care had been performed in 97% of the patients during the previous years as evidenced by both extracted missing teeth and the quantity of existing teeth with restorations. A large proportion of the patients had deep periodontal pockets (81%) and in a quarter of the patients manifest visible caries was present, indicating a current need for dental care. However, due to the clinical settings no radiographic examination necessary for caries diagnostics in hidden tooth surfaces could be performed. It is therefore likely to assume that the occurrence of manifest caries was underestimated in this population. DFT was in this study in mean 15.7 in the age group 65–79 years and somewhat lower, 14.2, among those 80 years and older. This reduction is probably an effect of the fact that the older participants had fewer teeth. Compared to the findings in a Norwegian study38 where DFT was 14.6 in the ages 65–79 years and 12.2 in 80–94 years this corresponds rather well with our study.
During the last decades preventive efforts in dentistry has been performed and dental diseases have decreased among adults in many countries.39 This important work has resulted in more remaining natural teeth in the older Swedish population.10 Even though both older people living in their own homes as well as nursing home residents were included in this study, as many as 91% had remaining natural teeth. The presence of natural teeth in old age has been shown to have a positive effect on both eating and quality of life,40,41 and it is therefore important to keep natural teeth in good condition for as long as possible. In this study 44% of the patients had less than 20 teeth, which is likely the limit for maintaining good chewing ability.34 However, when comorbidities become more frequent and functional abilities decline the need for oral care assistance increases.42 In a study on frail older residents in nursing homes (mean age 85 years) as many as 79% had fewer than 20 teeth and in mean they had 14.8 teeth,22 which can be compared to 19.2 natural teeth in the patients in this study. This indicates an expected deterioration in the chewing ability when older persons become frailer and in need of nursing home care. Furthermore, this shows that efforts from both nursing care and dental care personnel to identify patients with poor oral health in hospital settings may be of future benefit in this group of patients, especially as the functional capacity to perform oral hygiene may be reduced, temporarily or permanently.
Oral Dryness
Oral dryness is a frequently occurring problem in older patients and can have a negative impact on both nutrition and quality of life. We found that 26.5% of the patients had oral dryness, measured by the nurses by sliding a mouth mirror along the buccal mucosa. This is a somewhat blunt method, but the otherwise commonly used clinical method of five minutes stimulated saliva sampling,43 was not considered applicable in these patients due to pain, nausea, and other difficulties to cooperate because of the trauma. It is therefore not improbable to assume that oral dryness was underestimated and that more of the study patients had problems with a dry mouth. Hyposalivation measured by stimulated saliva was reported in 33.5% in a systematic review including mixed populations (community dwellings and nursing homes) of 60 years and older (range 60–100 years),44 which is somewhat higher than we found. It is well known that oral dryness may be a side-effect from drug treatment and that drugs can have a negative impact on oral health have been shown in several studies.45–47 The selection of drugs analysed in this study was based on their probable tendency to negatively affect the production of saliva and we also found a probably significant association between impaired oral health and polypharmacy as well as with treatment with anticholinergic drugs when given in a combination of two or more.
Comorbidity
In older populations multi-morbidity as well as polypharmacy is frequent48 which is consistent with the results of this study. The older patients admitted to the orthopaedic department had a high prevalence of comorbidity and used multiple medications. When analysing comorbidity in the participants, we applied the frequently used age adjusted Charlson comorbidity index, a validated instrument for measuring and grading comorbidity.32,33,49 The index score ranges from 0 to 37 points and evaluates the prevalence and degree of chronic diseases. Findings in this study can be compared to those of a study by Jiang in 201850 where over 1000 hip fracture patients were analysed regarding their CCI and they found that a mean value of over 6 was both severe and associated with an increased 5-year mortality risk. The mean value of 6.67 in our study indicates that the participants were indeed multi-morbid and had a considerably heavy disease burden.
Among the complications that can accompany orthopedic surgery are delayed wound healing51,52 and wound infections,53,54 both superficial and deep infections. These nosocomial infections can be deleterious to older orthogeriatric patients and even cause premature death. Since malnutrition in connection with impaired oral health is especially frequent in older multi-diseased patients the risk of complications and care-related infections in our group of patients were high.
The occurrence of chronic diseases among the study patients which is known to negatively affect oral health was frequent, with 40% suffering from heart diseases and 17% from diabetes. Also, other chronic diseases that can have detrimental effects on oral health were present such as dementia (14%), obstructive lung diseases (13%) and rheumatoid arthritis (6%) whereas 50% presented with moderate to low renal function. Previous studies55,56 have reported an association between missing teeth and COPD, which was also found in this study. We found a significant association between COPD in the dentate patients and the presence of fewer than 20 teeth or a DFT of over the mean, (p = value 0.019 and 0.048 respectively). However, as the occurrence of COPD is closely related to smoking it is a limitation to the study that data on smoking habits were not collected, which would have been an important confounding factor to include in the analysis. However, the demographic profile of the patients showed no differences in occurrence of COPD between sexes or age groups suggesting that smoking did not have a major role among the participants. Drugs that are used to treat obstructive lung symptoms, accompanying COPD, work through different pathways: anticholinergic effects, beta-adrenergic receptor stimulating effects, or with anti-inflammatory effects, and are often used in combinations. Both expected effects and side-effects of these drugs can cause impaired oral health. For example, inhaled corticosteroids can give rise to oral fungal infections57 and anticholinergic drugs and beta-adrenergic drugs can cause oral dryness and reduced saliva production.28,58
The study population consisted of older patients, mean age 81 years, with a high number of chronic diseases, demonstrated by a high mean score on the Charlson comorbidity index. Older patients are more susceptible to adverse effects from drugs including dry mouth and hyposalivation, changes in taste, oral candidiasis and other infections affecting the oral mucosa.59 Among the study participants 66% were using five drugs or more, which is the definition of polypharmacy. Only two patients did not use any drugs regularly and described themselves as healthy.
Limitations and Strengths
However, this study did meet with some limitations which has been mentioned in part earlier in the text. A number of patients were not included in the study due to mainly cognitive dysfunction, even so 14% of the included participants were diagnosed with dementia. Another fact that can have impact on the results are that only drugs that were used at admission were included in the analysis and that we did not have access to information on for how long the drugs had been used before hospitalization. Important to note is also that only medications used on a regular basis were included in the analyses since feasible information on usage of drugs prescribed only as per needed are difficult to collect in traumatized patients. Even so, the rationale for only including drugs taken on a regular basis was to ascertain that the drugs most probably were used and thereby increase the consistency of the results. However, as shown in studies on medication in older patients it is likely that more patients were for example using hypnotics and sedatives on a daily basis rather than infrequently (per needed) as prescribed.60,61 This may result in us underestimating the negative effects on oral health caused by these groups of drugs, rather than overestimating it.
On the other hand, this study presents several results that can provide valuable information on how to identify oral health problems in older hospitalized patients as well as to indicate possible pathways to improve oral care after discharge. Therefore, oral health should be considered to be included in the assessment of health risk factors in frail older patients in hospital settings.62
Among the strengths of this study is that it represents a mixed orthogeriatric population with different backgrounds and with varied experience of dental care, they also come from different living conditions and have varied care needs. This may increase the possibility to generalize from the extracted data and to apply the results found in the study to a wider range of older patients. Although data for this study did not include causes or risk factors of the falls leading up to the fractures we did analyse if there were any associations between the type of fracture and the oral health variables and found no significant links.
In Sweden, dental hygienists are licensed and work independently with oral examinations in all age groups.63 Two experienced dental hygienists performed all the oral examinations and they calibrated their examination techniques and data collection before the study started. The examinations were carried out using established methods in dentistry, this we consider an important strength of the study leading to reliable data that are possible to replicate.
The age adjusted Charlson´s comorbidity index was used to present the overall chronic morbidity in the study population and since this method of describing the burden of comorbidity has been used within several research areas it may facilitate the comparison of our results with other studies. The CCI score aided to describe their need for intensified actions in evaluating and assisting them with their oral care during hospitalisation as well as after discharge. It was also used as a confounding factor to adjust for the presence of comorbidities in the participants.
The use of medications was methodically examined by a physician experienced in medication reconciliation procedures and the drugs were divided into different medication classes according to the ATC-classification codes established by the WHO and thereby reproducible and comparable to other studies. Data of included drugs were drawn from the medical records and a drug reconciliation process had preceded the data collection.
The study was conducted in hospital settings and was carried out in collaboration between medical care personnel and dental care professionals. This teamwork we found to be favourable from an educational aspect and helped to increase the general awareness of oral care in these settings.
Further studies are wanted in older hospitalised trauma patients in need of surgery to establish how to identify their need for oral health care during their in-hospital stay and how to establish and communicate their future need for dental and oral care. Of great interest is also to study whether improved oral care both during the hospitalisation and after the discharge, can reduce the risk of post-surgery complications such as wound infections and delayed wound healing.
Conclusions
The study showed that impaired oral health was prevalent in older trauma patients and that negative effects on oral health were significantly associated with chronic diseases and drug use. The results emphasize the importance of identifying orthogeriatric patients with oral health problems and to highlight the necessity to uphold good oral care in a period when functional decline can be expected.
Abbreviations
AC, anticholinergic acting drugs; ACE, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; COPD, chronic obstructive pulmonary disease; DFT, decayed, filled teeth; PPI, proton pump inhibiting drug.
Data Sharing Statement
Data compiled for the study and published in this manuscript are available from the corresponding author at request.
Acknowledgments
We are grateful for the skilled collection of oral health data performed by dental hygienists Elisabeth Fagerström, Folktandvården Skåne and Sladjana Critén, Kristianstad University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Odontological Research Funds in Region Skåne (OFRS), the Research Platform for Collaboration for Health Kristianstad University and Swedish Dental Hygienists Association. The grants had no role in the design or other parts of the research or preparation and submission of the article.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Chen IJ, Chiang CY, Li YH, et al. Nationwide cohort study of hip fractures: time trends in the incidence rates and projections up to 2035. Osteoporos Int. 2015;26(2):681–688. doi:10.1007/s00198-014-2930-z
2. Sharma S, Mueller C, Stewart R, et al. Predictors of falls and fractures leading to hospitalization in people with dementia: a Representative Cohort Study. J Am Med Dir Assoc. 2018;19(7):607–612. doi:10.1016/j.jamda.2018.03.009
3. Early NK, Fairman KA, Hagarty JM, Sclar DA. Joint effects of advancing age and number of potentially inappropriate medication classes on risk of falls in medicare enrollees. BMC Geriatr. 2019;19(1):194. doi:10.1186/s12877-019-1202-3
4. Woolcott JC, Richardson KJ, Wiens MO, et al. Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch Intern Med. 2009;169(21):1952–1960. doi:10.1001/archinternmed.2009.357
5. Tinetti ME, Han L, Lee DS, et al. Antihypertensive medications and serious fall injuries in a nationally representative sample of older adults. JAMA Intern Med. 2014;174(4):588–595. doi:10.1001/jamainternmed.2013.14764
6. Kragh Ekstam A, Elmstahl S. Do fall-risk-increasing drugs have an impact on mortality in older hip fracture patients? A Population-Based Cohort Study. Clin Interv Aging. 2016;11:489–496. doi:10.2147/CIA.S101832
7. Andersen CU, Lassen PO, Usman HQ, Albertsen N, Nielsen LP, Andersen S. Prevalence of medication-related falls in 200 consecutive elderly patients with hip fractures: a Cross-Sectional Study. BMC Geriatr. 2020;20(1):121. doi:10.1186/s12877-020-01532-9
8. da Costa JA, Ribeiro A, Bogas M, et al. Mortality and functional impairment after hip fracture - a Prospective Study in a Portuguese population. Acta Reumatol Port. 2009;34(4):618–626.
9. Lewis A, Wallace J, Deutsch A, King P. Improving the oral health of frail and functionally dependent elderly. Aust Dent J. 2015;60(Suppl 1):95–105. doi:10.1111/adj.12288
10. Norderyd O, Koch G, Papias A, et al. Oral health of individuals aged 3–80 years in Jonkoping, Sweden during 40 years (1973–2013). II. Review of clinical and radiographic findings. Swed Dent J. 2015;39(2):69–86.
11. Stock C, Jurges H, Shen J, Bozorgmehr K, Listl S. A comparison of tooth retention and replacement across 15 countries in the over-50s. Community Dent Oral Epidemiol. 2016;44(3):223–231.
12. van der Putten G-J, de Baat C, De Visschere L, Schols J. Poor oral health, a potential new geriatric syndrome. Gerodontology. 2014;31(Suppl 1):17–24. doi:10.1111/ger.12086
13. Gronbeck Linden I, Hagglin C, Gahnberg L, Andersson P. Factors affecting older persons’ ability to manage oral hygiene: a Qualitative Study. JDR Clin Trans Res. 2017;2(3):223–232.
14. Barbe AG. Medication-induced xerostomia and hyposalivation in the elderly: culprits, complications, and management. Drugs Aging. 2018;35(10):877–885. doi:10.1007/s40266-018-0588-5
15. Barbe AG, Schmidt P, Bussmann M, Kunter H, Noack MJ, Rohrig G. Xerostomia and hyposalivation in orthogeriatric patients with fall history and impact on oral health-related quality of life. Clin Interv Aging. 2018;13:1971–1979. doi:10.2147/CIA.S178370
16. Gil-Montoya JA, de Mello AL, Barrios R, Gonzalez-Moles MA, Bravo M. Oral health in the elderly patient and its impact on general well-being: a nonsystematic review. Clin Interv Aging. 2015;10:461–467. doi:10.2147/CIA.S54630
17. Hakeem FF, Bernabe E, Sabbah W. Association between oral health and frailty: a systematic review of longitudinal studies. Gerodontology. 2019;36(3):205–215. doi:10.1111/ger.12406
18. Andersson P, Hallberg IR, Renvert S. Inter-rater reliability of an oral assessment guide for elderly patients residing in a rehabilitation ward. Spec Care Dentist. 2002;22(5):181–186. doi:10.1111/j.1754-4505.2002.tb00268.x
19. Kandelman D, Petersen PE, Ueda H. Oral health, general health, and quality of life in older people. Spec Care Dentist. 2008;28(6):224–236. doi:10.1111/j.1754-4505.2008.00045.x
20. Okamoto N, Amano N, Nakamura T, Yanagi M. Relationship between tooth loss, low masticatory ability, and nutritional indices in the elderly: a Cross-Sectional Study. BMC Oral Health. 2019;19(1):1. doi:10.1186/s12903-019-0778-5
21. Sjogren P, Wardh I, Zimmerman M, Almstahl A, Wikstrom M. Oral care and mortality in older adults with pneumonia in hospitals or nursing homes: systematic review and meta-analysis. J Am Geriatr Soc. 2016;64(10):2109–2115. doi:10.1111/jgs.14260
22. Andersson P, Renvert S, Sjogren P, Zimmerman M. Dental status in nursing home residents with domiciliary dental care in Sweden. Community Dent Health. 2017;34(4):203–207.
23. Holmen A, Stromberg E, Hagman-Gustafsson ML, Wardh I, Gabre P. Oral status in home-dwelling elderly dependent on moderate or substantial supportive care for daily living: prevalence of edentulous subjects, caries and periodontal disease. Gerodontology. 2012;29(2):e503–11. doi:10.1111/j.1741-2358.2011.00507.x
24. Schulz C, Buchele G, Peter RS, et al. Regional variation of care dependency after hip fracture in Germany: a Retrospective Cohort Study using health insurance claims data. PLoS One. 2020;15(3):e0230648. doi:10.1371/journal.pone.0230648
25. Cary MP
26. Gill TM, Allore HG, Gahbauer EA, Murphy TE. Change in disability after hospitalization or restricted activity in older persons. JAMA. 2010;304(17):1919–1928. doi:10.1001/jama.2010.1568
27. Desoutter A, Soudain-Pineau M, Munsch F, Mauprivez C, Dufour T, Coeuriot JL. Xerostomia and medication: a Cross-Sectional Study in long-term geriatric wards. J Nutr Health Aging. 2012;16(6):575–579. doi:10.1007/s12603-012-0007-2
28. Tan ECK, Lexomboon D, Sandborgh-Englund G, Haasum Y, Johnell K. Medications that cause dry mouth as an adverse effect in older people: a systematic review and metaanalysis. J Am Geriatr Soc. 2018;66(1):76–84. doi:10.1111/jgs.15151
29. Johansson AK, Johansson A, Unell L, Ekback G, Ordell S, Carlsson GE. Self-reported dry mouth in Swedish population samples aged 50, 65 and 75 years. Gerodontology. 2012;29(2):e107–15. doi:10.1111/j.1741-2358.2010.00420.x
30. Carrero JJ, Qureshi AR, Axelsson J, et al. Comparison of nutritional and inflammatory markers in dialysis patients with reduced appetite. Am J Clin Nutr. 2007;85(3):695–701. doi:10.1093/ajcn/85.3.695
31. Thorman R, Neovius M, Hylander B. Clinical findings in oral health during progression of chronic kidney disease to end-stage renal disease in a Swedish population. Scand J Urol Nephrol. 2009;43(2):154–159. doi:10.1080/00365590802464817
32. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
33. Frenkel WJ, Jongerius EJ, Mandjes-van Uitert MJ, van Munster BC, de Rooij SE. Validation of the Charlson Comorbidity Index in acutely hospitalized elderly adults: a Prospective Cohort Study. J Am Geriatr Soc. 2014;62(2):342–346. doi:10.1111/jgs.12635
34. Ueno M, Yanagisawa T, Shinada K, Ohara S, Kawaguchi Y. Masticatory ability and functional tooth units in Japanese adults. J Oral Rehabil. 2008;35(5):337–344. doi:10.1111/j.1365-2842.2008.01847.x
35. Rams TE, Oler J, Listgarten MA, Slots J. Utility of Ramfjord index teeth to assess periodontal disease progression in longitudinal studies. J Clin Periodontol. 1993;20(2):147–150. doi:10.1111/j.1600-051X.1993.tb00330.x
36. Ainamo J, Barmes D, Beagrie G, Cutress T, Martin J, Sardo-Infirri J. Development of the World Health Organization (WHO) community periodontal index of treatment needs (CPITN). Int Dent J. 1982;32(3):281–291.
37. Henricsson V, Svensson A, Axell T. Evaluation of some electrical methods for objective assessment of oral mucosal dryness. Scand J Dent Res. 1990;98(6):520–528.
38. Mulic A, Tveit AB, Stenhagen KR, Oscarson N, Staxrud F, Jonsson B. The frequency of enamel and dentin caries lesions among elderly Norwegians. Acta Odontol Scand. 2020;78(1):6–12. doi:10.1080/00016357.2019.1634283
39. Tonetti MS, Bottenberg P, Conrads G, et al. Dental caries and periodontal diseases in the ageing population: call to action to protect and enhance oral health and well-being as an essential component of healthy ageing - Consensus report of group 4 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J Clin Periodontol. 2017;44(Suppl 18):S135–S44.
40. Hoeksema AR, Spoorenberg S, Peters LL, et al. Elderly with remaining teeth report less frailty and better quality of life than edentulous elderly: a Cross-Sectional Study. Oral Dis. 2017;23(4):526–536. doi:10.1111/odi.12644
41. Singh KA, Brennan DS. Chewing disability in older adults attributable to tooth loss and other oral conditions. Gerodontology. 2012;29(2):106–110. doi:10.1111/j.1741-2358.2010.00412.x
42. Komulainen K, Ylostalo P, Syrjala AM, et al. Determinants for preventive oral health care need among community-dwelling older people: a Population-Based Study. Spec Care Dentist. 2014;34(1):19–26. doi:10.1111/scd.12021
43. Navazesh M, Kumar SK. University of Southern California School of D. Measuring salivary flow: challenges and opportunities. J Am Dent Assoc. 2008;139(Suppl):35S–40S. doi:10.14219/jada.archive.2008.0353
44. Pina GDS, Carvalho RM, Silva BSD, Almeida FT. Prevalence of hyposalivation in older people: a systematic review and meta-analysis. Gerodontology. 2020;37(4):317–331. doi:10.1111/ger.12497
45. Dawes C, Wong DTW. Role of saliva and salivary diagnostics in the advancement of oral health. J Dent Res. 2019;98(2):133–141. doi:10.1177/0022034518816961
46. Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008;168(5):508–513. doi:10.1001/archinternmed.2007.106
47. Janssens B, Vanobbergen J, Petrovic M, Jacquet W, Schols JMGA, De Visschere L. The oral health condition and treatment needs of nursing home residents in Flanders (Belgium). Community Dent Health. 2017;34(3):143–151.
48. Schottker B, Saum KU, Muhlack DC, Hoppe LK, Holleczek B, Brenner H. Polypharmacy and mortality: new insights from a large cohort of older adults by detection of effect modification by multi-morbidity and comprehensive correction of confounding by indication. Eur J Clin Pharmacol. 2017;73(8):1041–1048. doi:10.1007/s00228-017-2266-7
49. Austin SR, Wong YN, Uzzo RG, Beck JR, Egleston BL. Why summary comorbidity measures such as the Charlson comorbidity index and elixhauser score work. Med Care. 2015;53(9):e65–72. doi:10.1097/MLR.0b013e318297429c
50. Jiang L, Chou ACC, Nadkarni N, et al. Charlson comorbidity index predicts 5-year survivorship of surgically treated hip fracture patients. Geriatr Orthop Surg Rehabil. 2018;9:2151459318806442. doi:10.1177/2151459318806442
51. Ottesen TD, Hsiang WR, Malpani R, et al. Underweight patients are the greatest risk body mass index group for 30-day perioperative adverse events after total shoulder arthroplasty. J Am Acad Orthop Surg. 2021;29(3):e132–e42. doi:10.5435/JAAOS-D-20-00049
52. Stechmiller JK. Understanding the role of nutrition and wound healing. Nutr Clin Pract. 2010;25(1):61–68. doi:10.1177/0884533609358997
53. Beiner JM, Grauer J, Kwon BK, Vaccaro AR. Postoperative wound infections of the spine. Neurosurg Focus. 2003;15(3):E14. doi:10.3171/foc.2003.15.3.14
54. Klein JD, Garfin SR. Nutritional status in the patient with spinal infection. Orthop Clin North Am. 1996;27(1):33–36. doi:10.1016/S0030-5898(20)32047-2
55. Wang Z, Zhou X, Zhang J, et al. Periodontal health, oral health behaviours, and chronic obstructive pulmonary disease. J Clin Periodontol. 2009;36(9):750–755. doi:10.1111/j.1600-051X.2009.01448.x
56. Jung ES, Lee KH, Choi YY. Association between oral health status and chronic obstructive pulmonary disease in Korean adults. Int Dent J. 2020;70(3):208–213. doi:10.1111/idj.12535
57. Buhl R. Local oropharyngeal side effects of inhaled corticosteroids in patients with asthma. Allergy. 2006;61(5):518–526. doi:10.1111/j.1398-9995.2006.01090.x
58. Corsonello A, Pedone C, Incalzi RA. Age-related pharmacokinetic and pharmacodynamic changes and related risk of adverse drug reactions. Curr Med Chem. 2010;17(6):571–584. doi:10.2174/092986710790416326
59. Gil-Montoya JA, Silvestre FJ, Barrios R, Silvestre-Rangil J. Treatment of xerostomia and hyposalivation in the elderly: a systematic review. Med Oral Patol Oral Cir Bucal. 2016;21(3):e355–66. doi:10.4317/medoral.20969
60. Miller SL, Miller S, Balon J, Helling TS. Medication reconciliation in a rural trauma population. Ann Emerg Med. 2008;52(5):483–491. doi:10.1016/j.annemergmed.2008.03.021
61. Meyer C, Stern M, Woolley W, Jeanmonod R, Jeanmonod D. How reliable are patient-completed medication reconciliation forms compared with pharmacy lists? Am J Emerg Med. 2012;30(7):1048–1054. doi:10.1016/j.ajem.2011.06.038
62. Pilotto A, Custodero C, Maggi S, Polidori MC, Veronese N, Ferrucci L. A multidimensional approach to frailty in older people. Ageing Res Rev. 2020;60:101047. doi:10.1016/j.arr.2020.101047
63. Erdenborg J, Malmqvist S, Bjurshammar N, Johannsen G, Hultin M, Johannsen A. Stakeholder perception of the professional role and competence of Swedish dental hygienists: a Questionnaire and Interview Study. J Int Soc Prev Community Dent. 2020;10(1):54–61.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.