")
Back to Journals » Patient Preference and Adherence » Volume 10
Impact of fixed orthodontic appliance and clear-aligner on daily performance in adult patients with moderate need for treatment
Authors Lin F, Yao L, Bhikoo C, Guo J
Received 24 May 2016
Accepted for publication 19 June 2016
Published 26 August 2016 Volume 2016:10 Pages 1639—1645
DOI https://doi.org/10.2147/PPA.S113466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
This paper has been retracted
Feiou Lin,1 Linjie Yao,2 Chandradev Bhikoo,1 Jing Guo3
1Department of Orthodontics, 2Department of Pedodontics, School of Stomatology, Wenzhou Medical University, Wenzhou, 3Department of Orthodontics, School and Hospital of Stomatology, Shandong University, Jinan, People’s Republic of China
Objective: To assess the impact of wearing fixed orthodontic appliance (FOA) or clear-aligner, on daily performance in adult patients.
Methods: The Oral Impacts on Daily Performance (OIDP) index was assessed in 152 adults aged 25–35 years at baseline (T0), 6 months after bonding (T1), and 12 months after bonding (T2). Participants were randomly divided into two groups: CA group (participants treated with clear-aligner) and a control group (FOA group; participants treated with FOA). Baseline malocclusion severity was assessed using the Index of Orthodontic Treatment Need.
Results: There were no significant differences in sociodemographic variables and OIDP scores at baseline between the two groups. Significant changes in OIDP total and subscale scores were observed while wearing FOA: OIDP total score and subscale scores of eating, cleaning teeth, smiling, and social relation at T1 and T2 were significantly higher than at baseline (P<0.05 or P<0.01). However, only OIDP total score was significantly increased at T1 compared to the baseline in the CA group. OIDP total score and subscale scores of eating, cleaning teeth, smiling, and social relation were significantly higher in patients wearing FOA than in patients wearing clear-aligner at T1 and T2 (P<0.05 or P<0.01).
Conclusion: Patients wearing clear-aligner have fewer impacts on daily life than those wearing FOA during treatment, and have no significant changes in OIPD subscale scores at 12 months. FOA therapy significantly impacts daily performance in adult patients during treatment.
Keywords: clear-aligner, fixed orthodontic appliance, OIDP, quality of life, oral health
Introduction
Nowadays, it is widely believed that malocclusion has a negative impact on people’s physical, social, and psychological well-being.1 Patients seek orthodontic treatment to improve their appearance, oral function, psychosocial well-being, and quality of life, and the main motivation of adult patients seeking orthodontic treatment is improving appearance.2,3 However, brackets may cause unesthetic appearance, functional limitations, discomfort, and pain during treatment.4 The demand for esthetic dentistry has increased in recent decades, and more and more adult patients are choosing esthetic brackets. Ceramic bracket, lingual bracket, and clear-aligner have been invented to improve esthetics during treatment.5,6
Over the past few decades, researchers have developed a questionnaire on oral health-related quality of life (OHRQoL) to evaluate orthodontic treatment needs and outcomes.7 Discomfort and concern with a fixed orthodontic appliance (FOA) will affect the attitudes and compliance of patients with therapy.8–10 Understanding the discomfort associated with and consequences of wearing an orthodontic appliance in daily life may help orthodontists have realistic expectations regarding orthodontic treatment and select a more suitable treatment method; this may also help patients have a greater adherence to treatment. However, only few researchers have focused on the oral impacts of clear-aligner on daily performance in adult patients.
The Oral Impacts on Daily Performance (OIDP) is one of the most widely used indicators to measure oral impacts that seriously affect individuals’ daily activities. It consists of eight items that assess the impact of oral conditions on basic activities and behaviors that cover the physical, psychological, and social dimensions of daily life. Previous studies have demonstrated its validity and reliability in various countries and languages, including Chinese.11–15 The aim of the present study is using OIDP to assess the different impacts of wearing FOA and clear-aligner on daily performance in adult patients.
Materials and methods
The study was approved by the Health Research Ethics Board at Wenzhou Medical University. Each patient was given oral as well as written information and signed a written consent form before participating in research. All patients were consecutively recruited from April 2014 to April 2015, based on the following inclusion criteria: 25–35 years of age, moderate or borderline need for treatment, no teeth missing, and willing to answer the questionnaire. Patients with the following conditions were excluded: requiring esthetic appliances, or single-arch or sectional fixed appliance treatment, and presence of class III malocclusion, skeletal discrepancy, cleft lip or palate, extractions, craniofacial syndrome, or systemic disease.
The research was designed as a prospective, randomized controlled two-group parallel trial (Figure 1). The required sample size for a chi-square test with a 0.05 level of significance to have 80% power to detect a 25% difference in the prevalence of impacts was calculated to be 63 subjects in each group. In order to compensate for a 20% nonresponsive rate, a total of 76 patients were selected in each group. Eligible patients were randomized into two groups using blocked randomization by a computer-generated table of random numbers with a block size of ten and an allocation ratio of 1:1. Patients were sequentially allocated to the treatments in the order in which they were recruited.
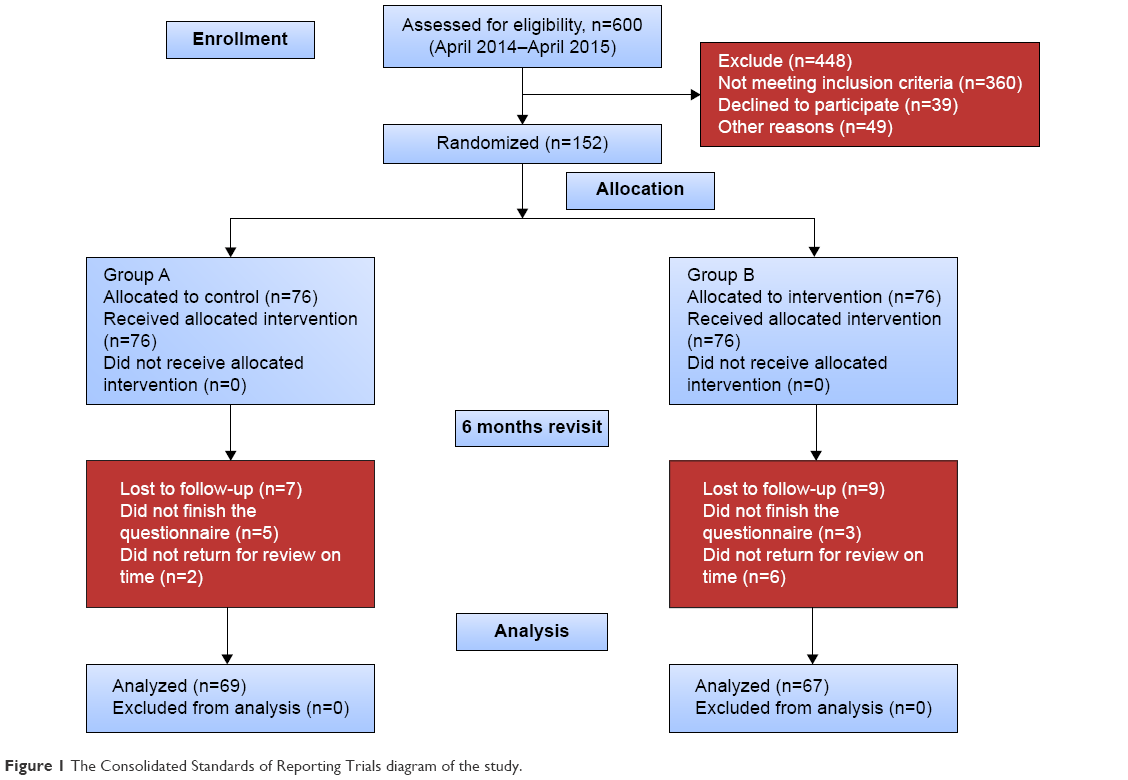 | Figure 1 The Consolidated Standards of Reporting Trials diagram of the study. |
Group A (FOA group) was treated with a traditional FOA, and Group B (CA group) was treated with clear-aligner (Angel Align; EA-angel Co. Ltd, Shanghai, People’s Republic of China). All evaluators and investigators were blinded to group assignment for the duration of the study.
Outcomes and statistical analysis
Before treatment, all patients were assessed using the Index of Orthodontic Treatment Need, which can classify the anatomical and esthetic aspects. The index consists of two components, the Dental Health Component and the Aesthetic Component.16 The Dental Health Component grade was determined from the records according to the highest scoring anomaly in the hierarchical scale. Patients with Dental Health Component grade 3, which represents moderate or borderline need for treatment, were included in this research. A descriptive data questionnaire was used to collect baseline data of patients. OIDP was used to assess impacts of FOA and clear-aligner on daily life. Patients were evaluated at baseline, that is, prior to any treatment (T0), 6 months after bonding (T1), and 12 months after bonding (T2). The OIDP only takes into account the frequency and perceived severity of the ultimate impacts, and can only be assessed by the individuals themselves. The OIDP index was quantified by multiplying the frequency and severity scores to obtain the performance score for each of the eight dimensions (eating, speaking, cleaning teeth, working, social relation, sleeping/relaxing, smiling, and emotional status). The OIDP frequency scores were assessed on a four-point scale as follows: 0: never, 1: less than once a month, 2: once or twice a month up to once or twice a week, and 3: three to four times a week or more often. The severity scores were assessed as follows: 0: not at all, 1: little severe, 2: severe, and 3: very severe. Finally, the total OIDP score was calculated from the sum of eight dimensions.
SPSS software (version 15.0; SPSS Inc., Chicago, IL, USA) was used to calculate frequencies and percentages, and the Kolmogorov–Smirnov test was used to verify the distribution of the data. A Wilcoxon signed-rank test was used to assess intergroup OIDP differences, since the OIDP scores were not normally distributed. Friedman test with Student–Newman–Keuls test was used to compare the relative changes in OIDP scores at T0, T1, and T2. Internal consistency reliability was assessed using Cronbach’s alpha, and test–retest reliability was determined on a randomly selected subsample. The results were evaluated within a 95% confidence interval. The statistical significance level was established at P<0.05.
Results
Participant demographics are shown in Table 1. There were no significant differences in sociodemographic variables between the two groups. Figure 1 shows the Consolidated Standards of Reporting Trials diagram of the study. Figure 2 shows the intraoral photographs of the two types of orthodontic appliances. Sixteen patients (seven in Group A and nine in Group B) were lost to follow-up as they failed to review on time or submitted invalid questionnaire. The final number of patients who completed the study was 136 who were from Wenzhou, People’s Republic of China. The mean age of the CA group was 29.4±4.9 years, and that of the FOA group was 30.1±5.4 years.
 | Table 1 The demographic characteristics of the participants |
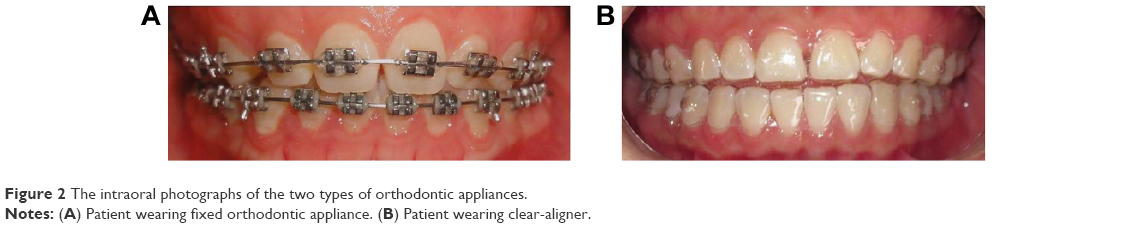 | Figure 2 The intraoral photographs of the two types of orthodontic appliances. |
The internal consistency of the OIDP was found to be satisfactory as indicated by a Cronbach coefficient of 0.82. The corrected item total correlation (ie, the correlation between each item and the total score omitted for that item) ranged from 0.30 to 0.63 for the OIDP, and a Kappa statistic of 0.76 indicated a very good reproducibility. Data recorded at different periods and a comparison of OIDP total and subscale scores in each group are shown in Tables 2 and 3. Significant changes in OIDP scores were observed while wearing FOA: OIDP total score and subscale scores of eating, cleaning teeth, smiling, and social relation at T1 and T2 were significantly higher than at baseline (P<0.05 or P<0.01); working subscale scores at T1 were significantly higher than at baseline; OIDP total scores (P<0.01) and smiling subscale scores (P<0.05) at T2 were significantly lower than those at T1. Only OIDP total score was significantly increased at T1 compared to the baseline in Group B, and no other significant changes in OIDP scores were observed while wearing clear-aligner. A comparison of OIDP total and subscale scores between the two groups at each period is shown in Table 4.
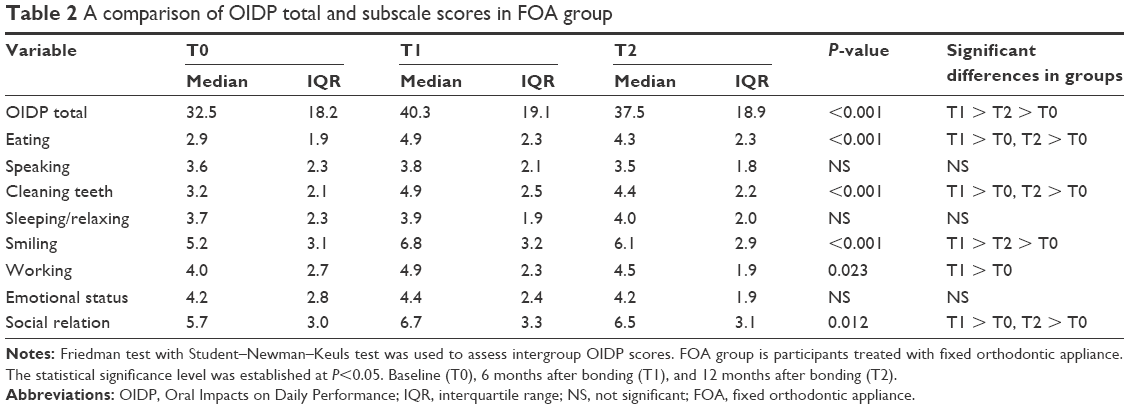 | Table 2 A comparison of OIDP total and subscale scores in FOA group |
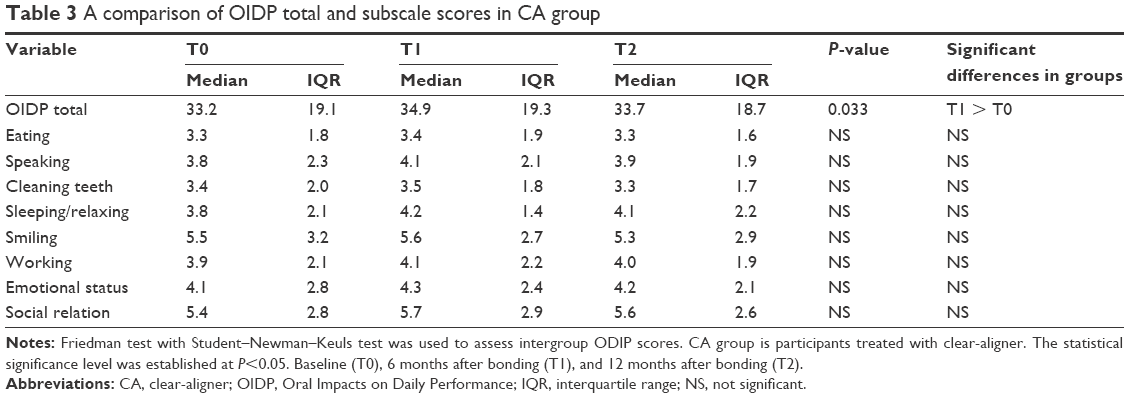 | Table 3 A comparison of OIDP total and subscale scores in CA group |
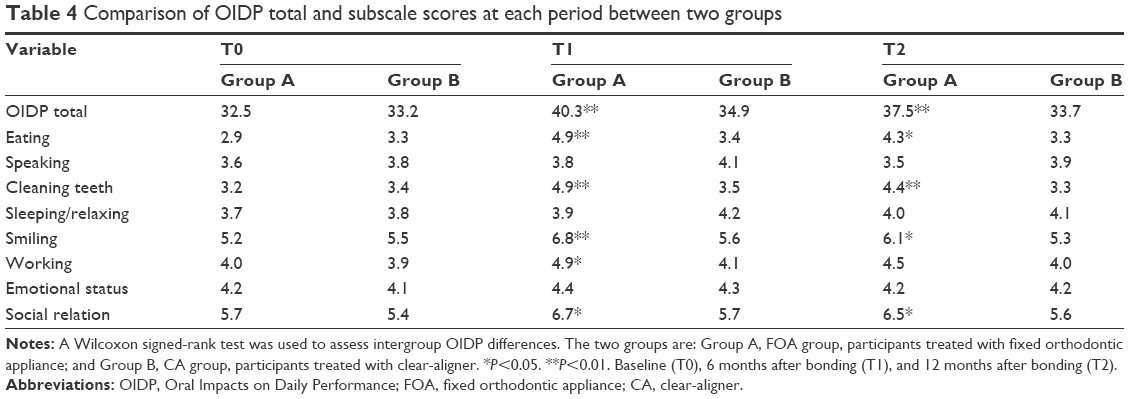 | Table 4 Comparison of OIDP total and subscale scores at each period between two groups |
There were no significant differences in OIDP scores at baseline (P>0.05). OIDP total score and subscale scores of eating, cleaning teeth, smiling, and social relation were significantly higher in patients wearing FOA than patients wearing clear-aligner at T1 and T2 (P<0.05 or P<0.01); working subscale scores at T1 were significantly higher in patients wearing FOA.
Discussion
Clear-aligners are orthodontic devices that use elastic thermoplastic material that applies pressure to the teeth to move into the aligner’s position, which are an alternative to dental braces. They are esthetic, efficient, and comfortable compared to traditional FOAs for mild-to-moderate malocclusion.17 On average, the treatment process takes 13.5 months, and treatment time varies based on the complexity of the planned teeth movements.18 Some patients prefer interproximal reduction, which could reduce the treatment time compared to molar distalization. In addition, patient adherence is also essential for the success of clear-aligner; nonadherence can result in poor outcomes.19 Owing to this concern, we used the clear-aligner for adults in this research. Adolescents should only be considered if they are very carefully screened.
In recent years, more and more adult patients are seeking orthodontic treatment with a greater preference for esthetic and comfortable alternatives compared to conventional fixed appliances. Recent researches have shown that adult patients are motivated to receive orthodontic treatment mainly because of their concern for dental–facial appearance and other psychosocial factors.2,20 In clinics, some adult patients who had given up seeking orthodontic treatment due to their concerns about the negative effects of wearing FOA on daily life8 have accepted to undergo orthodontic treatment again since the invention of clear-aligner. A greater understanding of what patients will experience during orthodontic treatment can provide insight into the true benefits and drawbacks associated with orthodontic appliances. Thus, this research used OIDP to investigate the impacts of FOA and clear-aligner on daily performance in adult patients.
The findings of the present study showed that significant changes in OIPD were observed during FOA treatment, especially in the first 6 months. This supports earlier findings that a patient’s OHRQoL is frequently worse during treatment.10,21–23 Zhang et al23 found that a child’s OHRQoL was frequently worse during treatment (oral symptoms, functional limitations) and the greatest deterioration in OHRQoL occurs during the first month of treatment. Liu et al22 also found that deterioration in OHRQoL occurs during FOA therapy in adult patients, with significant changes being observed in scores of five of the oral health impact profile domains (functional limitation, physical pain, psychological discomfort, psychological disability, social disability). These results were very similar to the results of the present research, which found a deterioration in OIDP total score and subscale scores of eating, cleaning teeth, smiling, working, and social relation. In patients who used clear-aligner, there were no significant changes observed during the treatment, except in the OIDP total score at 6 months; all of the OIDP scores became similar to the pretreatment scores after 12 months of treatment. The less impacts of clear-aligner on daily life might be attributed to its esthetic and removable features; patients could remove the appliance on special occasions.
A previous research in adolescents found that specific impacts on daily living, related to wearing orthodontic appliances, were higher among patients wearing FOA compared to those wearing removable appliances.21 Relying on the similar baseline before treatment in both the groups, our study also found similar results on the impacts of orthodontic appliances on eating, cleaning teeth, smiling, working, and social relation in daily life; the impacts were significantly weaker in patients wearing clear-aligner. Azaripour et al24 found that patients using clear-aligner have better periodontal health and quality of life compared to FOA-treated patients. Furthermore, it has been proved that FOA can reduce oral hygiene and lead to increased plaque accumulation during orthodontic treatment.25 These results were consistent with the outcomes of the present research (cleaning teeth). FOA and clear-aligner had little effect on speaking, sleeping/relaxing, and emotional status of patients during treatment.
In general, clear-aligner had less impact on daily life than FOA during treatment, and this is the reason why more and more adult patients have chosen clear-aligner in clinic in recent years. However, a recent systematic review concluded that there is insufficient evidence to determine the effectiveness of clear-aligner treatment and it is recommended for simple malocclusions.26 Thus, clear-aligner should be used in suitable cases to improve treatment effect and quality of life during treatment.
Limitations
The present research has some potential limitations. First, adult participants having a certain malocclusion were recruited from one particular university hospital, and thus do not reflect the characteristics of other occlusion and population. This limited representativeness might reduce the scope for generalization of these findings to the broader public. Second, the duration of this research was only 12 months, which is not long enough for the investigation of final impact. Third, individual characteristics and other currently unknown factors may influence patients’ self-report. Hence, further investigation is needed.
Conclusion
Significantly negative effects on daily life occurred during the first year of FOA therapy, and participants’ OIDP scores generally were worse during treatment compared with pretreatment. There were also negative effects with aligners but were less pronounced.
Patients wearing clear-aligner have less impact on daily life than those wearing FOA during treatment and have no significant changes at 12 months.
Disclosure
The authors report no conflicts of interest in this work.
References
Feu D, de Oliveira BH, de Oliveira Almeida MA, Kiyak HA, Miguel JA. Oral health-related quality of life and orthodontic treatment seeking. Am J Orthod Dentofacial Orthop. 2010;138(2):152–159. | ||
Tang X, Cai J, Lin B, Yao L, Lin F. Motivation of adult female patients seeking orthodontic treatment: an application of Q-methodology. Patient Prefer Adherence. 2015;9:249–256. | ||
Hassan AH, Amin Hel S. Association of orthodontic treatment needs and oral health-related quality of life in young adults. Am J Orthod Dentofacial Orthop. 2010;137(1):42–47. | ||
Doll GM, Zentner A, Klages U, Sergl HG. Relationship between patient discomfort, appliance acceptance and compliance in orthodontic therapy. J Orofac Orthop. 2000;61(6):398–413. | ||
Wiechmann D. A new bracket system for lingual orthodontic treatment. Part 1: theoretical background and development. J Orofac Orthop. 2002;63(3):234–245. | ||
Ellis CP. Invisalign and changing relationships. Am J Orthod Dentofacial Orthop. 2004;126(1):20A–21A; author reply 21A. | ||
Manjith CM, Karnam SK, Manglam S, Praveen MN, Mathur A. Oral Health-Related Quality of Life (OHQoL) among adolescents seeking orthodontic treatment. J Contemp Dent Pract. 2012;13(3):294–298. | ||
Yao L, Xu X, Ni Z, Zheng M, Lin F. Use of Q methodology to assess the concerns of adult female individuals seeking orthodontic treatment. Patient Prefer Adherence. 2015;9:47–55. | ||
Sergl HG, Klages U, Zentner A. Functional and social discomfort during orthodontic treatment – effects on compliance and prediction of patients’ adaptation by personality variables. Eur J Orthod. 2000;22(3):307–315. | ||
Chen M, Wang DW, Wu LP. Fixed orthodontic appliance therapy and its impact on oral health-related quality of life in Chinese patients. Angle Orthod. 2010;80(1):49–53. | ||
Hongxing L, List T, Nilsson IM, Johansson A, Astrom AN. Validity and reliability of OIDP and OHIP-14: a survey of Chinese high school students. BMC Oral Health. 2014;14:158. | ||
Purohit BM, Singh A, Acharya S, Bhat M, Priya H. Assessment and validation of the oral impact on daily performance (OIDP) instrument among adults in Karnataka, South India. Community Dent Health. 2012;29(3):203–208. | ||
Montero J, Lopez JF, Vicente MP, Galindo MP, Albaladejo A, Bravo M. Comparative validity of the OIDP and OHIP-14 in describing the impact of oral health on quality of life in a cross-sectional study performed in Spanish adults. Med Oral Patol Oral Cir Bucal. 2011;16(6):e816–e821. | ||
Naito M, Suzukamo Y, Ito HO, Nakayama T. Development of a Japanese version of the Oral Impacts on Daily Performance (OIDP) scale: a pilot study. J Oral Sci. 2007;49(4):259–264. | ||
Dorri M, Sheiham A, Tsakos G. Validation of a Persian version of the OIDP index. BMC Oral Health. 2007;7:2. | ||
Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod. 1989;11(3):309–320. | ||
Kim TW, Echarri P. Clear aligner: an efficient, esthetic, and comfortable option for an adult patient. World J Orthod. 2007;8(1):13–18. | ||
Malik OH, McMullin A, Waring DT. Invisible orthodontics part 1: invisalign. Dent Update. 2013;40(3):203–204, 207–210, 213–215. | ||
Chenin DA, Trosien AH, Fong PF, Miller RA, Lee RS. Orthodontic treatment with a series of removable appliances. J Am Dent Assoc. 2003;134(9):1232–1239. | ||
Wedrychowska-Szulc B, Syrynska M. Patient and parent motivation for orthodontic treatment – a questionnaire study. Eur J Orthod. 2010;32(4):447–452. | ||
Bernabe E, Sheiham A, de Oliveira CM. Impacts on daily performances related to wearing orthodontic appliances. Angle Orthod. 2008;78(3):482–486. | ||
Liu Z, McGrath C, Hagg U. Changes in oral health-related quality of life during fixed orthodontic appliance therapy: an 18-month prospective longitudinal study. Am J Orthod Dentofacial Orthop. 2011;139(2):214–219. | ||
Zhang M, McGrath C, Hagg U. Changes in oral health-related quality of life during fixed orthodontic appliance therapy. Am J Orthod Dentofacial Orthop. 2008;133(1):25–29. | ||
Azaripour A, Weusmann J, Mahmoodi B, et al. Braces versus Invisalign®: gingival parameters and patients’ satisfaction during treatment: a cross-sectional study. BMC Oral Health. 2015;15:69. | ||
Heintze SD, Jost-Brinkmann PG, Loundos J. Effectiveness of three different types of electric toothbrushes compared with a manual technique in orthodontic patients. Am J Orthod Dentofacial Orthop. 1996;110(6):630–638. | ||
Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod. 2015;85(5):881–889. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.