Back to Journals » Drug Design, Development and Therapy » Volume 14
Impacts of CYP2C19 Polymorphism and Clopidogrel Dosing on in-Stent Restenosis: A Retrospective Cohort Study in Chinese Patients
Authors Zhang M, Wang J, Zhang Y, Zhang P, Jia Z, Ren M, Jia X, Ma L, Gao M, Hou Y
Received 12 December 2019
Accepted for publication 29 January 2020
Published 19 February 2020 Volume 2020:14 Pages 669—676
DOI https://doi.org/10.2147/DDDT.S242167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Min Zhang, 1, 2 Jiangrong Wang, 1 Yong Zhang, 1 Pei Zhang, 1 Zhisheng Jia, 2 Manyi Ren, 1 Xiaomeng Jia, 1 Liping Ma, 1 Mei Gao, 1 Yinglong Hou 1
1Department of Cardiology, Shandong Provincial Qianfoshan Hospital, Shandong University, Jinan 250014, Shandong, People’s Republic of China; 2Department of Cardiology, The Fifth People’s Hospital of Jinan, Jinan 250022, Shandong, People’s Republic of China
Correspondence: Mei Gao
Department of Cardiology, Shandong Provincial Qianfoshan Hospital, Shandong University, No. 16766, Jingshi Road, Jinan 250014, Shandong, People’s Republic of China
Tel +86-13791126569
Fax +86-531 8296 3647
Email [email protected]
Yinglong Hou
Department of Cardiology, Shandong Provincial Qianfoshan Hospital, Shandong University, No. 16766, Jingshi Road, Jinan 250014, Shandong, People’s Republic of China
Tel +86-13791120810
Fax +86-531 8296 3647
Email [email protected]
Objective: This retrospective cohort study is to analyze the impacts of CYP2C19 polymorphism and clopidogrel dosing on in-stent restenosis (ISR) after coronary stenting.
Methods: Totally, 111 patients were included, who underwent percutaneous coronary intervention (PCI) with drug-eluting stent. Patients received clopidogrel treatment after the intervention on the background treatment with aspirin, based on the genotypes: 75 mg clopidogrel once each day for subjects without CYP2C19 loss-of-function (LOF) alleles (n=51; EM), 75 mg clopidogrel once each day (n=27; IM75) or twice each day (n=33; IM150) for subjects with one CYP2C19 LOF allele. ISR at 3– 18 months after coronary stenting was assessed.
Results: ISR rate was significantly higher in the IM75 group (40.7%) than the EM group (11.8%). ISR rate in the IM150 group was lower than the IM75 group (6.1% vs 40.7%), and comparable to that in the EM group. Multivariate logistic regression showed that both CYP2C19 genotype and clopidogrel dosing were associated with the risk of ISR after adjusting the relevant confounding factors. ISR risk was higher in the IM patients than the EM patients. Patients with clopidogrel dose of 75 mg once each day had significantly higher risk of ISR than those with the dose of 75 mg twice each day.
Conclusion: Increased dose of clopidogrel may reduce the risk of ISR after PCI in CYP2C19 LOF allele(s) carriers. The presence of CYP2C19 LOF allele(s) increases the risk of ISR after stenting, which could be counteracted by the increased dose of clopidogrel.
Keywords: CYP2C19 polymorphism, in-stent restenosis, ISR, clopidogrel, percutaneous coronary intervention, PCI
Introduction
In patients undergoing percutaneous coronary intervention (PCI), ischemic events often occur, as a result of in-stent restenosis (ISR), with the incidence of 5%-15%, despite the dual antiplatelet therapy (DAPT).1–5 ISR limits the long-term success rate of stents through the recurrence of symptoms and the necessity of repeated vascular reconstruction at the treatment site. We have learned important lessons about the underlying pathophysiology of ISR from autopsy and animal studies. Coronary angioplasty inevitably leads to endothelial denudation, which leads to the disorder of structural integrity in the wall of the diseased artery and the important change of mechanical environment. Within a few minutes, the injured area of the balloon was covered by platelets and leukocytes. After 24–48 hrs, the release of chemokines and mitogen leads to the activation and proliferation of vascular smooth muscle cells. VSMC migrated from medium to intima and changed from contraction to synthesis phenotype 4–14 days after injury. 14 days to 3 months after PCI, VSMC proliferation and extracellular matrix protein deposition resulted in intimal thickening, intimal hyperplasia and ultimately ISR. Macrophages and lymphocytes continued to exist in the stent vessels for more than 3 months. In general, it takes about 6 months for the stent to heal completely.6 The CYP2C19 gene encodes the hepatic enzyme cytochrome P450 (CYP), which transforms the inactive prodrug clopidogrel into the active forms.7,8
Clopidogrel is an inactive prodrug that requires liver activation by the cytochrome P450 enzyme complex, with CYP2C19 being one of the main enzymes involved in this process.9 At least 34 allelic variants of human CYP2C19 have been defined by the Human CYP Allele Nomenclature Committee. Genetic polymorphisms in the CYP2C19 gene have been shown to contribute to alterations in enzyme activity. The variation of cytochrome P450 and paraoxonase can lead to the change of enzyme activity, especially the mutation of CYP2C19*2, CYP2C19*3. Patients carrying CYP2C19*2 (c.681G>A; rs4244285) and CYP2C19*3 (c.636G>A; rs4986893), which are called CYP2C19 loss-of-function (LOF) allele (s), are less sensitive to clopidogrel, while prone to suffer from ischemic events when receiving DAPT after PCI. Mutations in CYP2C19*2, CYP2C19*3, may cause different clopidogrel responses and increased incidence of thrombotic events.8,10–12
A variety of factors contribute to the occurrence of ISR after vascular intervention, including de novo in-stent atherosclerosis and neointimal hyperplasia due to extracellular matrix deposition.4 Early experimental studies indicate a strong association between the platelet and the neointimal proliferation, involving the platelet receptor P2Y12, which can be inhibited by clopidogrel.13–15 Recent clinical studies show an association between the CYP2C19 polymorphism and the high post-treatment platelet reactivity (HPPR).16,17 HPPR has been also correlated with the ISR risk,18,19 suggesting an interaction between the CYP2C19 polymorphism and the ISR development. Specifically, several studies have linked the CYP2C19 LOF alleles to the increased risk of post-stenting ISR.20,21 It has been shown that the impacts of CYP2C19 LOF alleles could be partially compensated by increased clopidogrel dose.22,23 Whether this approach could reduce the risk of ISR remains unclear. However, several studies have failed to verify the relationship between the CYP2C19 polymorphism, HPPR, and ISR,24,25 or the increased clopidogrel dose could reduce the risk of ISR in the CYP2C19 LOF allele carriers.26,27 In this cohort study, the potential effects of the CYP2C19 polymorphism and clopidogrel dosing on ISR were investigated.
Materials and Methods
Study Patients
Patients were included in this study for data analysis if they (a) underwent PCI involving implantation of at least one drug-eluting stent between January 2013 and April 2017; (b) received post-stenting DAPT involving aspirin (100 mg daily) and clopidogrel (75 mg once or twice per day); (c) underwent repeat coronary angiography at 3–18 months after the coronary intervention; and (d) were genotyped for CYP2C19*2 (c.681G>A; rs4244285) and CYP2C19*3 (c.636G>A; rs4986893) LOF alleles. This study was approved by the Ethics Committee of Qianfoshan Hospital of Shandong University.
Coronary interventions were performed in alignment with the international guidelines.28–30 Drug-eluting stent implanted in patients was sirolimus-eluting stent or everolimus-eluting stent. Stent type and usage were carefully determined by experienced interventionist. Decision on the daily clopidogrel doses (75 or 150 mg) was made by physicians, while other medications were prescribed according to the international guidelines.
Data Collection
The primary outcome was ISR within 3–18 months from the last stenting. Angiographic restenosis was defined as ≥50% re-narrowing of the vessel diameter, as determined by the coronary angiography. In patients with multiple restenosis, only the restenosis with the most serious degree was recorded.
Genetic Analysis
Genomic DNA was extracted from the whole blood of patients before they took the first PCI operation during hospitalization. PCR was used to amplify the gene regions encompassing the LOF alleles CYP2C19*2 (681G>A) and CYP2C19*3 (636G>A). Amplicons were hybridized and genotyping was performed using a kit from Saileqi BIOTECH (Zhuhai, Guangdong, China).31 Patients with no LOF allele were defined as extensive metabolizers (EM); those with one LOF allele, as intermediate metabolizers (IM); and those with both LOF alleles, as poor metabolizers (PMs).
Statistical Analysis
Continuous data were expressed as mean ± SD, or median with interquartile range. SPSS 19.0 software (IBM, Chicago, IL, USA) was used for statistical analysis. Group comparison was performed with the Student’s t-test, one-way analysis of variance (ANOVA), or the Kruskal–Wallis or Mann–Whitney U-test, as appropriate. Ranking variables were compared using the non-parametric test. Categorical data were analyzed using the Fisher’s exact test. Multivariate logistic regression was used to test whether CYP2C19 genotype predicted ISR. For the regression, continuous variables such as age, level of low-density lipoprotein cholesterol (LDL-C), fibrinogen concentration (FIB), international normalized ratio (INR), and interval between last PCI and re-angiography were converted to ranking variables, which were set as dummy variables in the regression analysis. These variables, together with the following variables, were then subjected to the univariate analysis (with ISR as dependent variable): sex; cigarette smoking; drinking; hypertension; diabetes mellitus; coronary artery lesions; number of stents at last PCI; history of myocardial infarction, stroke, atrial fibrillation, and coronary artery bypass grafting (CABG); clinical symptoms including acute coronary syndrome and stable angina; CYP2C19 genotype; clopidogrel dose; and interaction item of CYP2C19 genotype and clopidogrel dose. Variables associated with ISR at the P< 0.1 level were subjected to the multivariate logistic regression model. The impacts of CYP2C19 genotype and clopidogrel dose were further analyzed with the multivariate logistic regression. Odds ratios (OR) and corresponding 95% confidence intervals (CI) were calculated for each variable.
Results
Baseline Characteristics of Patients
Initial screen was conducted in a total of 1214 patients who underwent repeat coronary angiography. Out of these, 111 patients (51 EM and 60 IM patients) received DAPT of aspirin (100 mg) and clopidogrel (75 mg once or twice per day) after stenting and were genotyped for CYP2C19*2 and CYP2C19*3 alleles. PM patients were not included since they received ticagrelor instead of clopidogrel as standard clinical practice in our hospital. EM patients took clopidogrel at the dose of 75 mg once each day. Among the 60 IM patients in the final analysis, 27 cases took clopidogrel at the dose of 75 mg once each day (designated as IM75), while the remaining 33 cases took clopidogrel at the dose of 75 mg twice each day (designated as IM150). The three cohorts were generally balanced in the baseline characteristics (Table 1), except for the significantly higher FIB in the IM75 cohort (compared with the EM and IM150 cohorts) and the lower INR in the EM cohort (compared with the IM75 and IM150 cohorts).
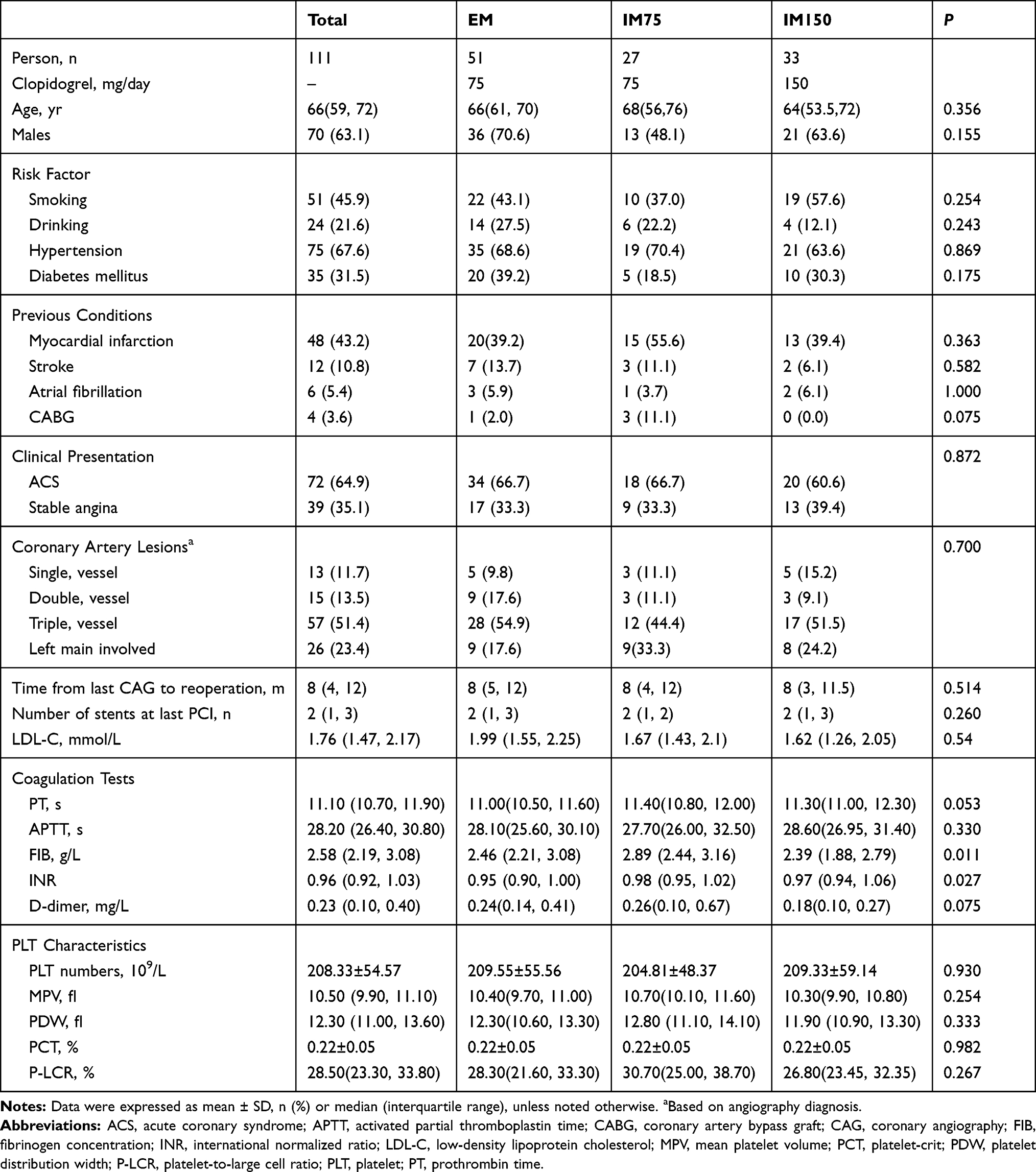 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients Stratified by CYP2C19 Genotype and Clopidogrel Dose |
Analysis of ISR Rates
The ISR rates for these groups were next investigated. Our results showed that, ISR occurred in 6 EM patients (11.8%), 11 IM75 patients (40.7%), and 2 IM150 patients (6.1%) (Table 2). According to Fisher’s exact test, the ISR rate was significantly higher in the IM75 cohort than the EM (OR 5.156, 95% CI 1.638–16.231, P = 0.008) and IM150 (OR 10.656, 95% CI 2.103–54.006, P = 0.002) cohorts, while similar ISR rates were observed for the EM and IM150 cohorts (OR 0.484, 95% CI 0.092–2.556, P = 0.471) (Figure 1). These results suggest that more patients in IM75 cohort experienced ISR than the EM and IM150 cohorts, while there was no significant difference in the proportion of patients experienced ISR between the EM and IM150 cohorts.
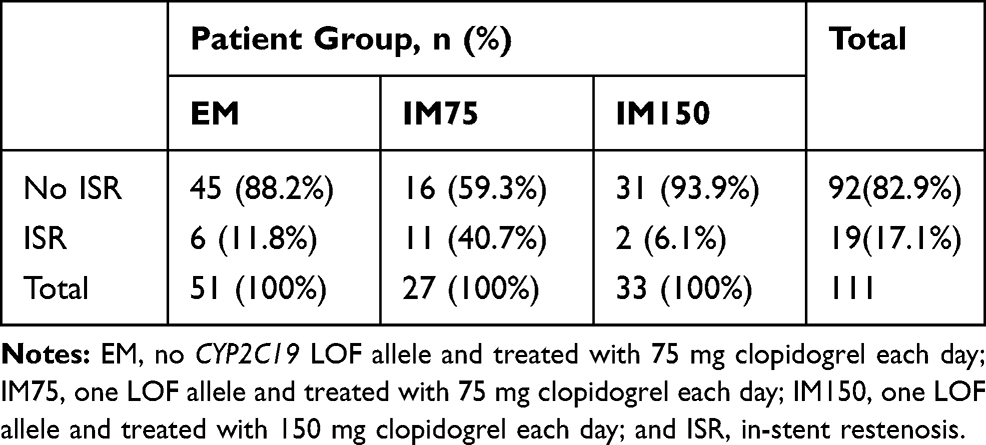 |
Table 2 Occurrence of ISR Within 3–18 Months from Last Stenting in Patients Stratified by CYP2C19 Genotype and Clopidogrel Dose |
 |
Figure 1 Analysis of ISR rates. Risks of ISR at 3–18 months after stenting were analyzed and compared among the patients without CYP2C19 LOF alleles treated with 75 mg clopidogrel daily (EM), and the patients with one LOF allele treated with 75 mg (IM75) or 150 mg (IM150) clopidogrel each day. |
Risk Factors for ISR
The univariate regression showed that only the interaction between CYP2C19 genotype and clopidogrel dose had the P value less than 0.1. Therefore, the multivariate regression was conducted, with the CYP2C19 genotype and clopidogrel dose as the variables. Our results showed that the CYP2C19 genotype was associated with the ISR risk, after adjusting for the clopidogrel dose, i.e., the IM patients had significantly higher risk of ISR than the EM patients (OR 5.063, 95% CI 1.610–15.921, P = 0.006). Moreover, the IM75 patients had higher risk of ISR than the IM150 patients (OR 10.656, 95% CI 2.103–54.006, P = 0.004). Furthermore, the risks for ISR were similar for the EM and IM150 patients (OR 2.067, 95% CI 0.391–10.917, P = 0.393). After adjusting for the genotype, patients with clopidogrel dose at 75mg once each day had significantly higher risk of ISR than those at 75mg twice each day (OR 10.748, 95% CI 2.128–54.297, P = 0.004) (Table 3). Taken together, these results suggest that the CYP2C19 genotype is the risk factor for ISR, after adjusting for the clopidogrel dose.
 |
Table 3 Uni- and Multivariate Regression Analysis to Identify Predictors for ISR Within 3–18 Months Post-Stenting |
Discussion
PCI is not only important in acute coronary syndrome (ACS), but also in stable coronary artery disease (CAD). Although PCI has greatly improved the prognosis of ACS patients, prolonged their life span and improved their quality of life, some patients still suffer from ISR, which may lead to recurrence and poor prognosis. Therefore, ISR has become a common problem in PCI.32 This cohort study provided evidence that the presence of CYP2C19 LOF allele (s) significantly increased the risk of ISR after PCI or patients taking clopidogrel. Moreover, the IM patients daily taking clopidogrel at 75 mg had higher risk of ISR than those at 75mg twice each day. Our results showed that the risk of ISR could be reversed by increasing the clopidogrel dose.
Clopidogrel is a thienopyridine prodrug, which requires metabolism by cytochrome P450 (CYP) enzymes in the liver to exert antiplatelet effect. And clopidogrel is an inhibitor of platelet aggregation that is used to decrease the risk of myocardial infarction and stroke in patients known to have atherosclerosis. Widely used to reduce the risk of myocardial infarction and stroke in patients with coronary heart disease or cerebrovascular disease or previous heart attack or stroke. Current indications include reduction of atherosclerotic events (myocardial infarction, stroke, vascular death) in patients with atherosclerosis and in patients with acute myocardial infarction or unstable angina.33 Different CYP450 isoenzymes, including CYP2C19, CYP2B6, CYP3A4/CYP3A5, CYP1A2, and CYP2C9, are involved in the process of biotransformation of clopidogrel to its active metabolite. Among the enzymes mediating this conversion, CYP2C19 is dominant for clopidogrel bioactivation and the activity of the CYP2C19 enzyme is genetically influenced by the gene polymorphisms. The distribution of CYP2C19 alleles shows wide interethnic differences. The frequencies of CYP2C19 LOF allele *2 and *3 are higher in Asians (with allele frequencies of 29%-35% and 2%-9%, respectively) than Caucasians and Africans (~15% and <1%, respectively). Therefore, it is important to study the impact of the variances in CYP2C19 gene on the antiplatelet effect of clopidogrel in Asians.
A variety of factors contribute to the occurrence of ISR after vascular intervention, including the prolapse of disrupted plaque, elastic recoil of vessel wall, constrictive remodeling, de novo in-stent atherosclerosis and neointimal hyperplasia due to extracellular matrix deposition, and smooth muscle cell hyperplasia.4 Early experimental studies indicate a strong association between the platelet and the neointimal proliferation, involving the platelet receptor P2Y12, which can be inhibited by clopidogrel.13–15 Recent clinical studies show an association between the CYP2C19 polymorphism and the HPPR.16,17 HPPR has been also correlated with the ISR risk,18,19 suggesting an interaction between the CYP2C19 polymorphism and the ISR development. Specifically, several studies have linked the CYP2C19 LOF alleles to the increased risk of post-stenting ISR.20,21 In the current study, our results were generally consistent with these previous findings.
Our results also suggest that the increased clopidogrel dose can counteract the elevated risk of ISR, in the presence of a CYP2C19 LOF allele. These results are consistent with a previous study showing that the increases clopidogrel dose can reduce HPPR22,23 and improve the clinical outcomes.34 On the other hand, several studies have failed to verify the relationship between the CYP2C19 polymorphism, HPPR, and ISR,24,25 and have failed to show that the increased clopidogrel dose could reduce the risk of ISR in the CYP2C19 LOF allele carriers.26,27 These discrepancies might be attributed to the differences in ethnics, since the distribution of CYP2C19 alleles might differ between Caucasians and Asians.8,35 Moreover, other factors (such as clinical or demographic characteristics, platelet activity measurement method, and definition of HPPR) may also contribute to the discrepancies.
Platelet P2Y12 plays a role in the vessel wall response to arterial injury and thrombosis.15,36–38 Inhibition of the P2Y12 receptor is generally believed to be the underlying mechanism for the pharmacological actions of clopidogrel. Insufficient platelet inhibition increases the thrombus formation, inflammatory reaction, neointimal hyperplasia, and atherosclerosis, and therefore aggravates the restenosis.19 There are also several limitations of this study, including the limited sample size and the observational retrospective study design. In addition, the measurement of platelet in response to clopidogrel was not included, and the PM patients were not involved herein, either. Therefore, further in-depth studies are still required to confirm whether the platelet reactivity mediates the observed relationship between the CYP2C19 polymorphism and the risk of ISR.
Conclusion
Our results showed that CYP2C19 polymorphism was associated with the ISR after PCI. Moreover, the increased dose of clopidogrel could reduce the risk of ISR after PCI in the CYP2C19 LOF allele (s) carriers. According to our data, double-dosed clopidogrel is recommended to patients carrying CYP2C19 LOF allele (s) to reduce the risk of ISR after PCI. These findings might contribute to the understanding of the pathogenesis and the clinical treatment of ISR after PCI.
Ethics
This study was approved by the Ethics Committee of Qianfoshan Hospital of Shandong University. Patient consent to review their medical records was required by the Ethics Committee of Qianfoshan Hospital of Shandong University. Patient data confidentiality was kept and the study was in compliance with the Declaration of Helsinki. All the personal information of enrolled participants were concealed and replaced as random ID.
Acknowledgments
This work was supported by the Medical and Health Science and Technology Development Projects of Shandong, China (2015WS0218), the Science and Technology Innovation Program for Clinical Medicine of Jinan (Shandong, China) (201602176), and the Medical and Health Science and Technology Development Projects of Shandong, China(2017WS448).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Kim YH, Park DW, Ahn JM, et al. Everolimus-eluting stent implantation for unprotected left main coronary artery stenosis. The PRECOMBAT-2 (premier of randomized comparison of bypass surgery versus angioplasty using sirolimus-eluting stent in patients with left main coronary artery disease) study. JACC Cardiovasc Interv. 2012;5(7):708–717. doi:10.1016/j.jcin.2012.05.002
2. Sato T, Ono T, Morimoto Y, et al. Differences in clinical and angiographic outcomes with different drug-eluting stents in Japanese patients with and without diabetes mellitus. J Cardiol. 2012;60(5):361–366. doi:10.1016/j.jjcc.2012.07.002
3. Kandzari DE, Leon MB, Meredith I, Fajadet J, Wijns W, Mauri L. Final 5-year outcomes from the Endeavor zotarolimus-eluting stent clinical trial program: comparison of safety and efficacy with first-generation drug-eluting and bare-metal stents. JACC Cardiovasc Interv. 2013;6(5):504–512. doi:10.1016/j.jcin.2012.12.125
4. Byrne RA, Joner M, Kastrati A. Stent thrombosis and restenosis: what have we learned and where are we going? The Andreas Gruntzig lecture ESC 2014. Eur Heart J. 2015;36(47):3320–3331. doi:10.1093/eurheartj/ehv511
5. Ogita M, Miyauchi K, Kurata T, et al. Clinical impact of angiographic restenosis after bare-metal stent implantation on long-term outcomes in patients with coronary artery disease. Circ J. 2011;75(11):2566–2572. doi:10.1253/circj.CJ-11-0469
6. Cornelissen A, Simsekyilmaz S, Liehn E, et al. Apolipoprotein E deficient rats generated via zinc-finger nucleases exhibit pronounced in-stent restenosis. Sci Rep. 2019;9(1):18153. doi:10.1038/s41598-019-54541-z
7. Johnson JA, Cavallari LH. Pharmacogenetics and cardiovascular disease–implications for personalized medicine. Pharmacol Rev. 2013;65(3):987–1009. doi:10.1124/pr.112.007252
8. Desta Z, Zhao X, Shin JG, Flockhart DA. Clinical significance of the cytochrome P450 2C19 genetic polymorphism. Clin Pharmacokinet. 2002;41(12):913–958. doi:10.2165/00003088-200241120-00002
9. Ruedlinger J, Prado Y, Zambrano T, et al. CYP2C19()2 polymorphism in chilean patients with in-stent restenosis development and controls. Biomed Res Int. 2017;2017:5783719. doi:10.1155/2017/5783719
10. Trenk D, Hochholzer W, Fromm MF, et al. Cytochrome P450 2C19 681G>A polymorphism and high on-clopidogrel platelet reactivity associated with adverse 1-year clinical outcome of elective percutaneous coronary intervention with drug-eluting or bare-metal stents. J Am Coll Cardiol. 2008;51(20):1925–1934. doi:10.1016/j.jacc.2007.12.056
11. Simon T, Verstuyft C, Mary-Krause M, et al. Genetic determinants of response to clopidogrel and cardiovascular events. N Engl J Med. 2009;360(4):363–375. doi:10.1056/NEJMoa0808227
12. Zhang Z, Chen M, Zhang L, Zhao Q. The impact of cytochrome 450 and Paraoxonase polymorphisms on clopidogrel resistance and major adverse cardiac events in coronary heart disease patients after percutaneous coronary intervention. BMC Pharmacol Toxicol. 2020;21(1):1. doi:10.1186/s40360-019-0378-7
13. Herbert JM, Tissinier A, Defreyn G, Maffrand JP. Inhibitory effect of clopidogrel on platelet adhesion and intimal proliferation after arterial injury in rabbits. Arterioscler Thromb. 1993;13(8):1171–1179. doi:10.1161/01.ATV.13.8.1171
14. Hermann A, Weber AA, Schror K. Clopidogrel inhibits platelet adhesion and platelet-dependent mitogenesis in vascular smooth muscle cells. Thromb Res. 2002;105(2):173–175. doi:10.1016/S0049-3848(01)00403-0
15. Evans DJ, Jackman LE, Chamberlain J, et al. Platelet P2Y(12) receptor influences the vessel wall response to arterial injury and thrombosis. Circulation. 2009;119(1):116–122. doi:10.1161/CIRCULATIONAHA.107.762690
16. Shuldiner AR, O’Connell JR, Bliden KP, et al. Association of cytochrome P450 2C19 genotype with the antiplatelet effect and clinical efficacy of clopidogrel therapy. JAMA. 2009;302(8):849–857. doi:10.1001/jama.2009.1232
17. Jeong YH, Kim IS, Park Y, et al. Carriage of cytochrome 2C19 polymorphism is associated with risk of high post-treatment platelet reactivity on high maintenance-dose clopidogrel of 150 mg/day: results of the ACCEL-DOUBLE (accelerated platelet inhibition by a double dose of clopidogrel according to gene polymorphism) study. JACC Cardiovasc Interv. 2010;3(7):731–741. doi:10.1016/j.jcin.2010.05.007
18. Mazighi M, Saint MJ, Bresson D, Szatmary Z, Houdart E. Platelet aggregation in intracranial stents may mimic in-stent restenosis. AJNR Am J Neuroradiol. 2010;31(3):496–497. doi:10.3174/ajnr.A1778
19. Fu Z, Dong W, Shen M, et al. Relationship between hyporesponsiveness to clopidogrel measured by thrombelastography and in stent restenosis in patients undergoing percutaneous coronary intervention. Clin Biochem. 2014;47(16–17):197–202. doi:10.1016/j.clinbiochem.2014.08.009
20. Guo B, Tan Q, Guo D, Shi Z, Zhang C, Guo W. Patients carrying CYP2C19 loss of function alleles have a reduced response to clopidogrel therapy and a greater risk of in-stent restenosis after endovascular treatment of lower extremity peripheral arterial disease. J Vasc Surg. 2014;60(4):993–1001. doi:10.1016/j.jvs.2014.03.293
21. Diaz-Villamarin X, Davila-Fajardo CL, Martinez-Gonzalez LJ, et al. Genetic polymorphisms influence on the response to clopidogrel in peripheral artery disease patients following percutaneous transluminal angioplasty. Pharmacogenomics. 2016;17(12):1327–1338. doi:10.2217/pgs-2016-0056
22. Mega JL, Hochholzer W, Frelinger AR, et al. Dosing clopidogrel based on CYP2C19 genotype and the effect on platelet reactivity in patients with stable cardiovascular disease. JAMA. 2011;306(20):2221–2228. doi:10.1001/jama.2011.1703
23. Collet JP, Hulot JS, Anzaha G, et al. High doses of clopidogrel to overcome genetic resistance: the randomized crossover CLOVIS-2 (clopidogrel and response variability investigation study 2). JACC Cardiovasc Interv. 2011;4(4):392–402. doi:10.1016/j.jcin.2011.03.002
24. Ma W, Liang Y, Zhu J, et al. Relationship of paraoxonase-1 Q192R genotypes and in-stent restenosis and re-stenting in Chinese patients after coronary stenting. Atherosclerosis. 2016;251:305–310. doi:10.1016/j.atherosclerosis.2016.07.901
25. Schulz S, Sibbing D, Braun S, et al. Platelet response to clopidogrel and restenosis in patients treated predominantly with drug-eluting stents. Am Heart J. 2010;160(2):355–361. doi:10.1016/j.ahj.2010.05.003
26. Collet JP, Hulot JS, Cuisset T, et al. Genetic and platelet function testing of antiplatelet therapy for percutaneous coronary intervention: the ARCTIC-GENE study. Eur J Clin Pharmacol. 2015;71(11):1315–1324. doi:10.1007/s00228-015-1917-9
27. Price MJ, Berger PB, Teirstein PS, et al. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011;305(11):1097–1105. doi:10.1001/jama.2011.290
28. Section of Interventional Cardiology CS, Cardiology of Chinese Medical Association, Editorial Board of Chinese Journal of Cardiology. [Chinese guideline for percutaneous coronary intervention (pocket guideline)]. Zhonghua Xin Xue Guan Bing Za Zhi. 2012;40(4):271–277.
29. Dehmer GJ, Blankenship JC, Cilingiroglu M, et al. SCAI/ACC/AHA expert consensus document: 2014 update on percutaneous coronary intervention without on-site surgical backup. J Am Coll Cardiol. 2014;63(23):2624–2641. doi:10.1016/j.jacc.2014.03.002
30. Section of Interventional Cardiology of Chinese Society of Cardiology of Chinese Medical Association, Specialty Committee on Prevention and Treatment of Thrombosis of Chinese College of Cardiovascular Physicians, Editorial Board of Chinese Journal of Cardiology. [Chinese guideline for percutaneous coronary intervention (2016)]. Zhonghua Xin Xue Guan Bing Za Zhi. 2016;44(5):382–400. doi:10.3760/cma.j.issn.0253-3758.2016.05.006
31. Dodgen TM, Hochfeld WE, Fickl H, et al. Introduction of the AmpliChip CYP450 test to a South African cohort: a platform comparative prospective cohort study. BMC Med Genet. 2013;14:20. doi:10.1186/1471-2350-14-20
32. Lv L, Ye W, Song P, et al. Relationship between ALDH2 genotype and in-stent restenosis in Chinese Han patients after percutaneous coronary intervention. BMC Cardiovasc Disord. 2019;19(1):176. doi:10.1186/s12872-019-1161-9
33. Clopidogrel. 2012
34. Xie X, Ma YT, Yang YN, et al. Personalized antiplatelet therapy according to CYP2C19 genotype after percutaneous coronary intervention: a randomized control trial. Int J Cardiol. 2013;168(4):3736–3740. doi:10.1016/j.ijcard.2013.06.014
35. Scott SA, Sangkuhl K, Stein CM, et al. Clinical pharmacogenetics implementation consortium guidelines for CYP2C19 genotype and clopidogrel therapy: 2013 update. Clin Pharmacol Ther. 2013;94(3):317–323. doi:10.1038/clpt.2013.105
36. Konishi H, Katoh Y, Takaya N, et al. Platelets activated by collagen through immunoreceptor tyrosine-based activation motif play pivotal role in initiation and generation of neointimal hyperplasia after vascular injury. Circulation. 2002;105(8):912–916. doi:10.1161/hc0802.105256
37. Friedman RJ, Stemerman MB, Wenz B, et al. The effect of thrombocytopenia on experimental arteriosclerotic lesion formation in rabbits. Smooth muscle cell proliferation and re-endothelialization. J Clin Invest. 1977;60(5):1191–1201. doi:10.1172/JCI108872
38. Unterberg C, Sandrock D, Nebendahl K, Buchwald AB. Reduced acute thrombus formation results in decreased neointimal proliferation after coronary angioplasty. J Am Coll Cardiol. 1995;26(7):1747–1754. doi:10.1016/0735-1097(95)00373-8
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.