Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Impacts of Comorbid Chronic Obstructive Pulmonary Disease and Congestive Heart Failure on Prognosis of Critically Ill Patients
Authors Dai Y, Qin S, Pan H, Chen T, Bian D
Received 5 August 2020
Accepted for publication 23 September 2020
Published 28 October 2020 Volume 2020:15 Pages 2707—2714
DOI https://doi.org/10.2147/COPD.S275573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Ying Dai, Shaoyun Qin, Huaqin Pan, Tianyu Chen, Dachen Bian
Department of Respiratory and Critical Care Medicine, Taizhou People’s Hospital, Taizhou, People’s Republic of China
Correspondence: Ying Dai
Department of Respiratory and Critical Care Medicine, Taizhou People’s Hospital, No. 366, Taihu Road, Taizhou 225300, Jiangsu, People’s Republic of China
Email [email protected]
Background: Comorbid congestive heart failure (CHF) was associated with worse prognosis in patients with chronic obstructive pulmonary disease (COPD), while few studies specially investigated critically ill patients. This study investigated the associations between comorbid COPD with or without CHF and prognosis of patients admitted to intensive care units (ICU).
Methods: We conducted a retrospective cohort study in the Medical Information Mart for Intensive Care III database. Adult ICU patients were included and categorized as patients without COPD and CHF, patients with COPD but without CHF, patients with CHF but without COPD, and patients with both COPD and CHF. The study outcomes were 28-day mortality and 90-day mortality after ICU admission. Kaplan–Meier curves were plotted to estimate the survival distributions between groups and multivariable Cox regression analyses were employed to evaluate the associations between comorbid COPD and/or CHF and the study outcomes.
Results: A total of 29,589 patients were included with 20,507 patients without COPD and CHF, 1575 patients with COPD, 6190 patients with CHF, and 1317 patients with both COPD and CHF. The highest 28-day mortality rate and 90-day mortality rate were found in patients with both COPD and CHF (15.95% and 25.74%, respectively), while patients with COPD and patients with CHF had similar mortality rates, also observed in Kaplan–Meier curves. Compared with patients without COPD or CHF, comorbid COPD or CHF both significantly increased the risk of 28-day mortality and 90-day mortality, but comorbid COPD and CHF together was associated with the highest risk of mortality (hazard ratio 1.55 (95% confidence interval (CI) 1.33– 1.80) and 1.25 (95% CI 1.16– 1.35) for 28-day mortality and 90-day mortality, respectively), while no significant interaction between COPD and CHF was found.
Conclusion: ICU patients with comorbid COPD or CHF both experienced greater mortalities, while these two risk factors seemed to play an independent role.
Keywords: chronic obstructive pulmonary disease, comorbidity, heart failure, mortality, critical care
Background
Chronic obstructive pulmonary disease (COPD) and heart failure (HF) are both common in hospitalized patients, especially for elderly patients.1,2 A population-based study from Denmark3 found the gross cost of treating hospitalized COPD patients accounted for 10% of the total cost of treating patients aged 40 years or more. In the United States in 2004, over one million patients were discharged with a first listed diagnosis of HF.4 These two diseases are both also associated with poor prognosis. An European study reported a 10.8% mortality rate of patients admitted with exacerbated COPD, of which 45.7% died in hospital and 54.3% died during the 90-day post-discharge follow-up.5 In the REPORT-HF cohort study which included patients admitted for acute heart failure, 20% died within 1 year after discharge.6
Since the two diseases share similar risk factors, they frequently coexist in clinical practice.7,8 A study including 9748 hospitalized patients with acute decompensated heart failure reported approximately 35% of patients had COPD,9 while 20% of COPD patients were diagnosed with left heart failure after extensive cardiovascular examination, in a study that included patients aged over 65 years.10 Moreover, the coexistence of these diseases is found to be associated with worse prognosis. A recent meta-analysis included 28 studies that compared prognosis of COPD patients with HF with those without HF, and the main finding was that comorbid HF increased risk of all-cause mortality in COPD patients with a pooled hazard ratio of 1.61.11 Another meta-analysis that included 68 studies reported that COPD was associated with increased mortality in non-selected HF patients with a pooled hazard ratio of 1.39.12
However, most of the above studies mainly investigated general hospitalized patients only. Considering patients admitted to intensive care unit (ICU) usually had much more serious conditions and had high prevalence of COPD and HF,12,13 it remains unclear whether these two comorbidities also have the same impact on prognosis of critically ill patients. Thus, to provide relevant evidence in an ICU setting, the study investigated the associations between comorbid COPD with or without congestive heart failure (CHF) and clinical outcomes of patients admitted to ICU.
Methods
Study Design and Participants
The study used a retrospective cohort study design. Data were retrieved from the Medical Information Mart for Intensive Care (MIMIC) III, which is a large, freely-available database comprising deidentified health-related data associated with patients admitted to critical care units of the Beth Israel Deaconess Medical Center between 2001 and 2012.14 This study was exempt from institutional review board approval due to the retrospective design, lack of direct patient intervention, and the security schema for which the reidentification risk was certified as meeting safe harbor standards by Privacert (Cambridge, MA).
All adult (age ≥18 years) patients in the database were included, but for patients who had more than one ICU admission in the database, only the first ICU admission was included. We also excluded patients who stayed in ICU less than 24 hours. Detailed inclusion of the participants is showed in Figure 1.
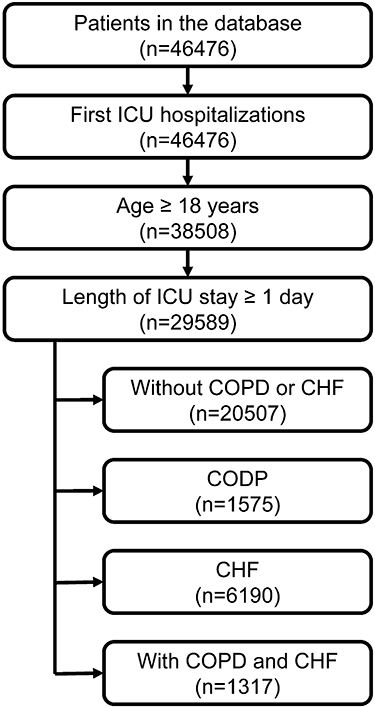 |
Figure 1 Inclusion of the study subjects. |
Variables Extraction
Data on variables needed for analysis were extracted using Structured Query Language (SQL) with the help from the MIMIC Code Repository.15 We defined the date of ICU admission as baseline and extracted baseline characteristics including age, sex, ethnicity, type of admission (elective or urgent), Sequential Organ Failure Assessment (SOFA) score, Simplified Acute Physiology Score (SAPS) II, mechanical ventilation on first day, renal replacement therapy on first day, sepsis, cardiac arrhythmias, valvular disease, pulmonary circulation disorder, hypertension, uncomplicated diabetes, complicated diabetes, renal failure, liver disease, metastatic cancer, and obesity.
COPD and CHF were identified based on International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) (491.20, 491.21, 491.22, and 496 for COPD; 398.91, 428.0, 428.1, 428.20, 428.21, 428.22, 428.23, 428.30, 428.31, 428.32, 428.33, 428.40, 428.41, 428.42, 428.43, and 428.9 for CHF).
Outcomes and Follow-Up
We used 28-day mortality and 90-day mortality after ICU admission as the main study outcomes. ICU mortality, hospital mortality, length of ICU stay, and length of hospital stay were also described. All included participants were categorized as patients without COPD and CHF, patients with COPD but without CHF, patients with CHF but without COPD, and patients with both COPD and CHF, and followed from the date of ICU admission for at least 90 days unless the interested outcome occurred.
Statistical Analysis
Data were presented as median (25–75% percentile) or number (percentage) based on type of variables. Comparisons between groups were examined by Kruskal–Wallis test or Chi-squared test. Kaplan–Meier curves were plotted to estimate the survival distributions of each group and multivariable Cox regression analyses were employed to evaluate the associations between comorbid COPD and/or CHF and the study outcomes. Two models were predefined for adjustment for potential confounding. Model I was adjusted for age and sex; model II was adjusted for age, sex, type of admission; ethnicity, SOFA, SAPS II, sepsis, mechanical ventilation on first day, renal replacement therapy on first day, and comorbidities including cardiac arrhythmias, valvular disease, pulmonary circulation disorder, hypertension, uncomplicated diabetes, complicated diabetes, renal failure, liver disease, metastatic cancer, and obesity. A P-value less than 0.05 is considered as statistically significant. All the analyses were performed using Empower(R) (www.empowerstats.com X&Y solutions, Inc., Boston, MA) program.
Results
Characteristics of the Participants
A total of 29,589 patients were included in the study. Among them, 20,507 patients were without COPD and CHF, 1575 patients were with COPD (without CHF), 6190 patients were with CHF (without COPD), and 1317 patients were with both COPD and CHF. The median age of all the participants was 65.75 (52.78–77.66) years, 56.90% of them were male, and 71.46% of them were white people. Compared with patients without COPD or CHF, the other groups had a greater median age, and patients with COPD and CHF had the largest median age (75.78 (67.56–82.31) years). Proportions of sex and ethnicity were similar between groups, but a higher proportion of white people could be observed in patients with COPD and patients with COPD and CHF.
Most (82.17%) patients in the study were admitted urgently, and compared with patients without COPD or CHF, the other groups had a larger SOFA and SAPS II on admission. Patients with COPD had the highest proportion (52.95%) of mechanical ventilation on first day, while patients with CHF had the highest proportion (4.30%) of renal replacement therapy on first day. Great difference could be found in some comorbidities between groups, such as a much larger prevalence of valvular disease and hypertension in patients with CHF. Detailed characteristics of the participants are shown in Table 1.
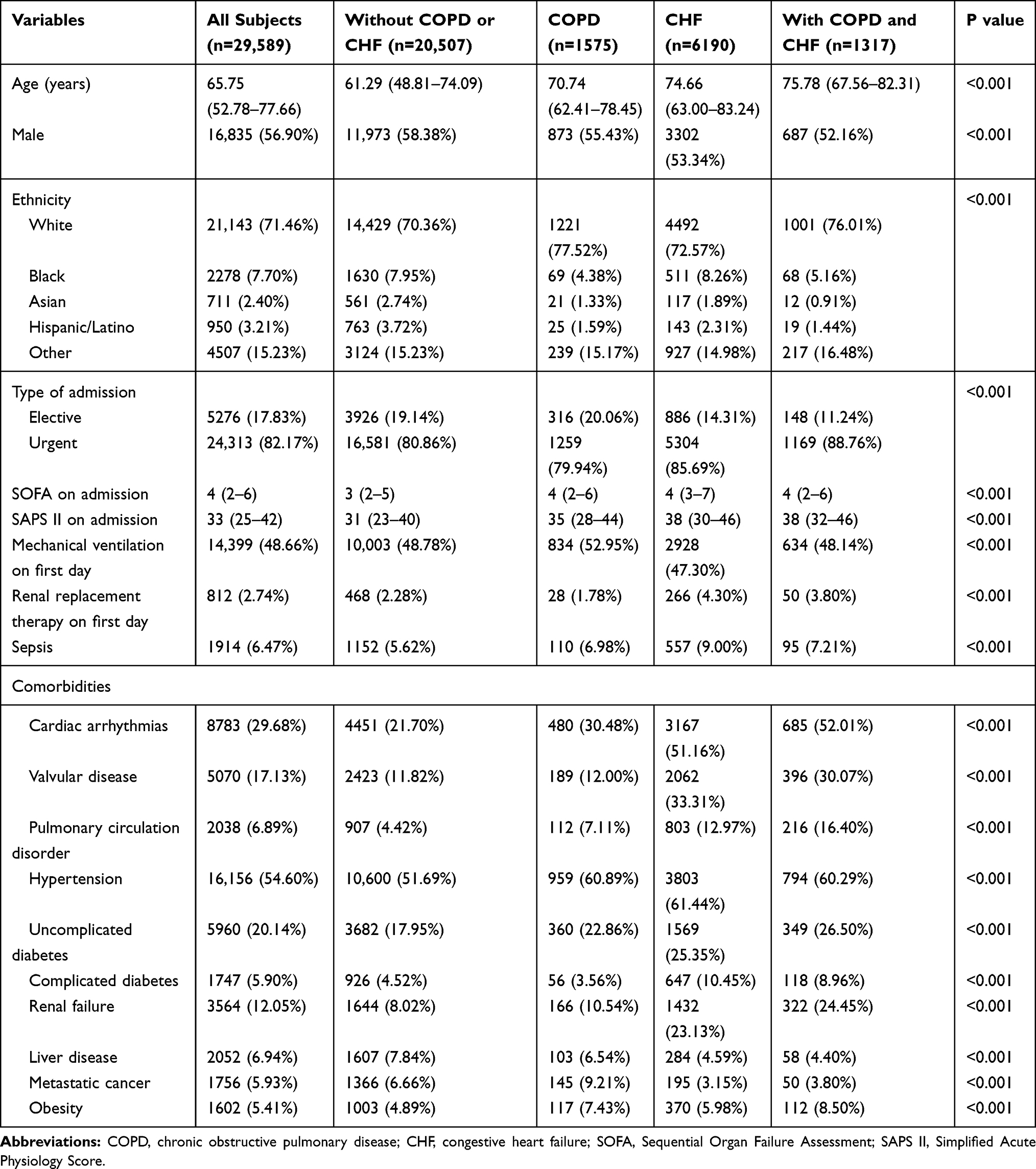 |
Table 1 Characteristics of the Study Subjects |
Prognosis of the Participants
The overall 28-day mortality and 90-day mortality were 8.61% and 13.73% respectively, with a length of ICU stay of 2.42 (1.58–4.46) days and a length of hospital stay 7.82 (4.98–13.00) days. The highest 28-day mortality rate and 90-day mortality rate were found in patients with both COPD and CHF (15.95% and 25.74%), while patients with COPD and patients with CHF had similar mortality rates, which were consistent with results of Kaplan–Meier curves (Figure 2). Similar results could be found for ICU mortality and hospital mortality. Detailed results are shown in Table 2.
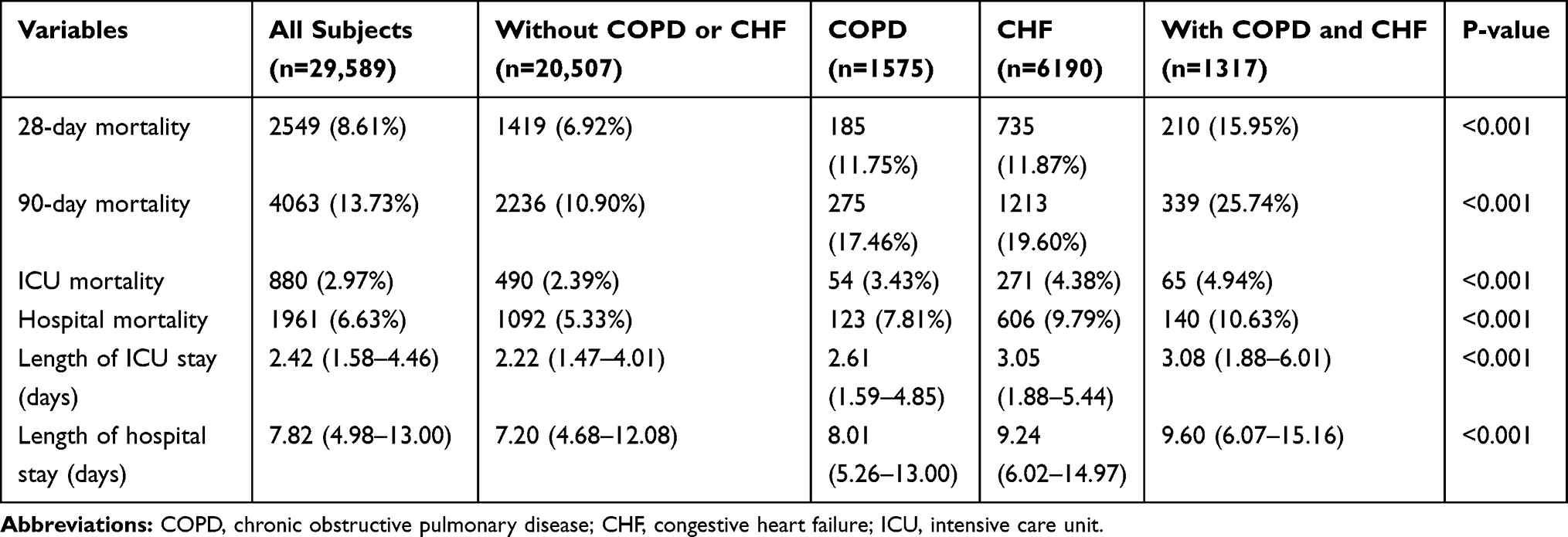 |
Table 2 Clinical Outcomes of the Study Subjects |
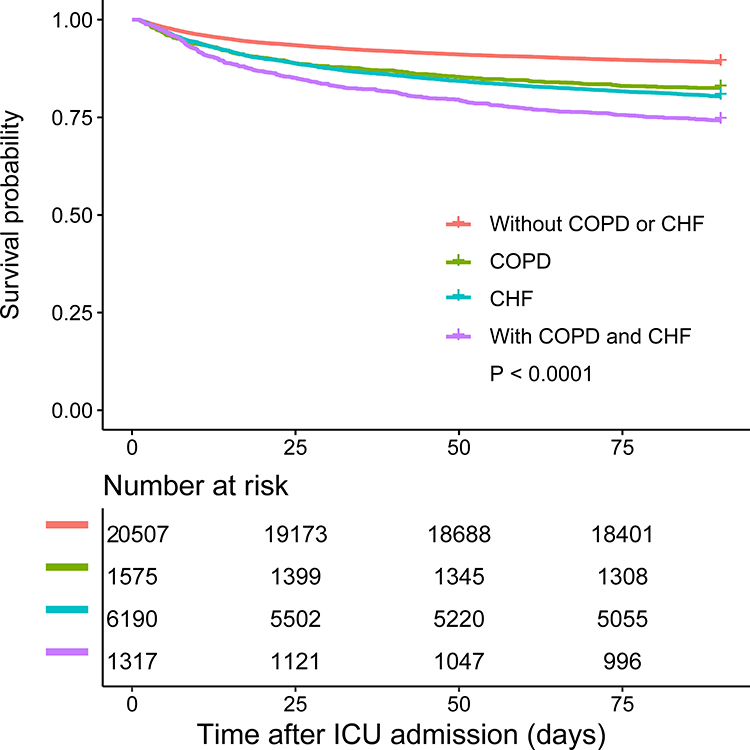 |
Figure 2 Kaplan–Meier curves for survival after ICU admission. |
Associations Between Comorbid COPD and/or CHF and Prognosis
Compared with patients without COPD or CHF, after multivariable adjustment, comorbid COPD or CHF both significantly increased the risk of 28-day mortality and 90-day mortality, but comorbid COPD and CHF together was associated with the highest risk of mortality (hazard ratio 1.55 (95% confidence interval (CI) 1.33–1.80) and 1.25 (95% CI 1.16–1.35) for 28-day mortality and 90-day mortality respectively). The interaction between COPD and CHF was statistically significant in the crude model (P=0.0295 for 28-day mortality and P=0.0220 for 90-day mortality), but after multivariable adjustment it became non-significant either for 28-day mortality or 90-day mortality (P=0.7167 for 28-day mortality and P=0.9533 for 90-day mortality in adjusted model I; P=0.6269 for 28-day mortality and P=0.3671 for 90-day mortality in adjusted model II). Detailed results are shown in Table 3.
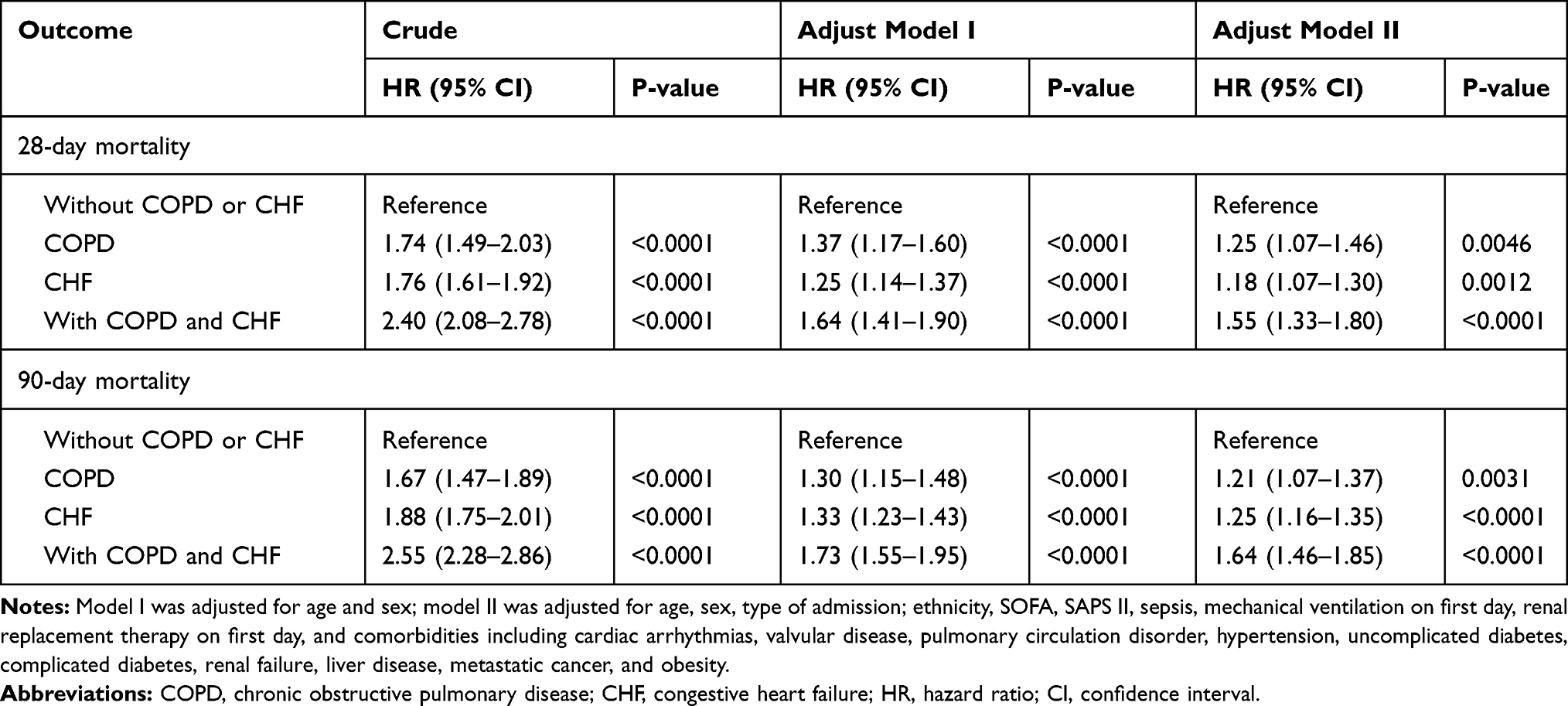 |
Table 3 Associations Between Comorbid COPD and/or CHF and Clinical Outcomes |
Discussion
This study included a large sample size of critically ill patients and investigated differences in the prognosis of patients without COPD and CHF, patients with COPD, patients with CHF, and patients with both COPD and CHF. After taking various confounding factors (including disease severity scores) into account, comorbid COPD and CHF together was found to be associated with worse prognosis compared with patients with one of the comorbidities, but no interaction between COPD and CHF was observed. The results provided prevalence of COPD and CHF in general ICU patients, and evidence about how COPD and CHF impact prognosis of ICU patients, which might help to raise clinicians’ awareness of the importance of these two common comorbidities and take appropriate measures when necessary to further improve prognosis of patients staying in ICU.
Among the 29,589 ICU patients we included, 9.77% (2892/29,589) had COPD, and 25.37% (7507/29,589) had CHF. The prevalence of these two comorbidities was similar to that reported in studies which involved critically ill patients. Funk et al reported the prevalence of COPD was 8.6% in a study that included about 200 thousand adult ICU patients in Austria between 1998 and 2008.13 This figure is slightly lower than our results, which might be because we included a slightly older population. It was estimated that at least 20% of hospital admissions among persons older than 65 were due to HF,16 but prevalence of CHF reported in numerous studies varied due to difference in study population and definition of CHF.17 In our study, 45.54% (1317/2892) COPD patients suffered from CHF, and 17.54% (1317/7507) CHF patients had COPD. The prevalence was different from that reported in hospitalized patients mentioned above (20% and 35%),9,10 which might be related to a difference in disease severity of the study population, definitions of CHF, or different awareness of CHF recognition. Nevertheless, all these results suggest that COPD and CHF are common to see in the same patient.
The associations between the two comorbidities and prognosis we observed in the study were consistent with most of other studies including those pooled estimations from meta-analyses.11,12 Apart from the difference in study population, that our study only included patients admitted to ICU, we included patients without COPD or CHF and took this group as the reference, while most other studies only excluded these patients.18–20 This study design increased our understanding of the impact of COPD and CHF on prognosis of ICU patients. According to our results, after adjusted for potential confounding factors, comorbid COPD or CHF only would increase the risk of 28-day mortality by 25% (95% CI 7–46%) and 18% (95% CI 7–30%) when compared to patients without COPD or CHF, while when a patient had COPD and CHF together, it would increase the risk of 28-day mortality by 55% (95% CI 33–80%), which suggested a combination of these two common diseases would further worsen the prognosis. Although these findings might not be novel to the clinicians, as far as we know it for the first time investigated critically ill patients specially on the impact of these two diseases on prognosis. In addition, we also examined whether there was an interaction effect between COPD and CHF, but the results showed non-significant interaction after multivariable adjustment. This suggested COPD and CHF might play an independent role on deteriorating prognosis of the patients, but it should be noticed that the interaction mentioned here only referred to statistical interaction, which could not be simply equal to biological interaction.21
Although the main findings of our study are known on an anecdotal level, it provided information on the magnitude of the increased risk of mortality in ICU patients when they were comorbid with COPD and CHF (either alone or together). Considering ICU patients were usually with a high baseline risk of mortality, a relative increase of mortality risk by about 20–50% should not be ignored and thus in clinical practice patients comorbid with COPD and CHF should get more attention to improve prognosis. In addition, the increased risk was also observed in a relatively long-term outcome (i.e., 90-day mortality), an outcome which might be usually neglected by clinicians since most ICU patients might stay in ICU less than 90 days, our study suggested efforts should also be put to improve prognosis of discharged ICU patients who were comorbid with COPD and CHF.
Although the large sample size strengthened the power of the study, it had some limitations which should be noted. In the study all the variables were extracted retrospectively, and COPD and CHF were both identified only based on ICD-9-CM instead of using strict definitions. This could be a source of bias of our findings, but the direction of the bias was difficult to evaluate without further data. In addition, since we only included patients from a single center, and the study period was between 2001 and 2012, the generality of our findings might be limited. Similar investigations on updated data using strict definitions are needed to provide evidence on the prevalence of comorbid COPD and CHF.
Conclusion
ICU patients with comorbid COPD or CHF both experienced greater mortality, while these two risk factors seemed to play an independent role.
Abbreviations
COPD, Chronic obstructive pulmonary disease; HF, heart failure; ICU, intensive care unit; CHF, congestive heart failure; MIMIC, Medical Information Mart for Intensive Care; SQL, Structured Query Language; SOFA, Sequential Organ Failure Assessment; SAPS, Simplified Acute Physiology Score; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; HR, hazard ratio; CI, confidence interval.
Data Sharing Statement
The data used in this study was retrieved from a restricted-access database. Steps to get access to the data was provided at https://mimic.physionet.org/gettingstarted/access/.
Ethics Approval and Consent to Participate
This study was exempt from institutional review board approval due to the retrospective design, lack of direct patient intervention, and the security schema for which the reidentification risk was certified as meeting safe harbor standards by Privacert (Cambridge, MA).
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Kumbhare SD, Beiko T, Wilcox SR, Strange C. Characteristics of COPD patients using United States emergency care or hospitalization. Chronic Obstr Pulm Dis. 2016;3(2):539–548.
2. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596.
3. Bilde L, Rud Svenning A, Dollerup J, Baekke Borgeskov H, Lange P. The cost of treating patients with COPD in Denmark–a population study of COPD patients compared with non-COPD controls. Respir Med. 2007;101(3):539–546. doi:10.1016/j.rmed.2006.06.020
4. Writing Group M, Lloyd-Jones D, Adams RJ, et al. Heart disease and stroke statistics–2010 update: a report from the American Heart Association. Circulation. 2010;121(7):e46–e215.
5. Hartl S, Lopez-Campos JL, Pozo-Rodriguez F, et al. Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD Audit. Eur Respir J. 2016;47(1):113. doi:10.1183/13993003.01391-2014
6. Tromp J, Bamadhaj S, Cleland JGF, et al. Post-discharge prognosis of patients admitted to hospital for heart failure by world region, and national level of income and income disparity (REPORT-HF): a cohort study. Lancet Glob Health. 2020;8(3):e411–e422. doi:10.1016/S2214-109X(20)30004-8
7. de Miguel Diez J, Chancafe Morgan J, Jimenez Garcia R. The association between COPD and heart failure risk: a review. Int J Chron Obstruct Pulmon Dis. 2013;8:305–312. doi:10.2147/COPD.S31236
8. Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ. Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology. Eur J Heart Fail. 2009;11(2):130–139. doi:10.1093/eurjhf/hfn013
9. Fisher KA, Stefan MS, Darling C, Lessard D, Goldberg RJ. Impact of COPD on the mortality and treatment of patients hospitalized with acute decompensated heart failure: the Worcester Heart Failure Study. Chest. 2015;147(3):637–645. doi:10.1378/chest.14-0607
10. Rutten FH, Cramer MJ, Grobbee DE, et al. Unrecognized heart failure in elderly patients with stable chronic obstructive pulmonary disease. Eur Heart J. 2005;26(18):1887–1894. doi:10.1093/eurheartj/ehi291
11. Axson EL, Ragutheeswaran K, Sundaram V, et al. Hospitalisation and mortality in patients with comorbid COPD and heart failure: a systematic review and meta-analysis. Respir Res. 2020;21(1):54. doi:10.1186/s12931-020-1312-7
12. Rushton CA, Satchithananda DK, Jones PW, Kadam UT. Non-cardiovascular comorbidity, severity and prognosis in non-selected heart failure populations: a systematic review and meta-analysis. Int J Cardiol. 2015;196:98–106. doi:10.1016/j.ijcard.2015.05.180
13. Funk GC, Bauer P, Burghuber OC, et al. Prevalence and prognosis of COPD in critically ill patients between 1998 and 2008. Eur Respir J. 2013;41(4):792. doi:10.1183/09031936.00226411
14. Johnson AE, Pollard TJ, Shen L, et al. MIMIC-III, a freely accessible critical care database. Sci Data. 2016;3:160035. doi:10.1038/sdata.2016.35
15. Johnson AE, Stone DJ, Celi LA, Pollard TJ. The MIMIC code repository: enabling reproducibility in critical care research. J Am Med Inform Assoc. 2018;25(1):32–39. doi:10.1093/jamia/ocx084
16. Jessup M, Brozena S. Heart failure. N Engl J Med. 2003;348(20):2007–2018. doi:10.1056/NEJMra021498
17. Dar O, Cowie MR. Acute heart failure in the intensive care unit: epidemiology. Crit Care Med. 2008;36(1 Suppl):S3–S8. doi:10.1097/01.CCM.0000296264.41365.80
18. Genao L, Durheim MT, Mi X, Todd JL, Whitson HE, Curtis LH. Early and long-term outcomes of older adults after acute care encounters for chronic obstructive pulmonary disease exacerbation. Ann Am Thorac Soc. 2015;12(12):1805–1812. doi:10.1513/AnnalsATS.201504-250OC
19. Santibanez M, Garrastazu R, Ruiz-Nunez M, et al. Predictors of hospitalized exacerbations and mortality in chronic obstructive pulmonary disease. PLoS One. 2016;11(6):e0158727. doi:10.1371/journal.pone.0158727
20. Betihavas V, Davidson PM, Newton PJ, Frost SA, Macdonald PS, Stewart S. What are the factors in risk prediction models for rehospitalisation for adults with chronic heart failure? Aust Crit Care. 2012;25(1):31–40. doi:10.1016/j.aucc.2011.07.004
21. Siemiatycki J, Thomas DC. Biological models and statistical interactions: an example from multistage carcinogenesis. Int J Epidemiol. 1981;10(4):383–387. doi:10.1093/ije/10.4.383
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.