")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 16
Impact of TREM1 Variants on the Risk and Prognosis of Glioma in the Chinese Han Population
Authors Hu M, Wei J, Hao J, Jin T, Li B
Received 6 January 2023
Accepted for publication 21 April 2023
Published 3 July 2023 Volume 2023:16 Pages 707—715
DOI https://doi.org/10.2147/PGPM.S403870
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Mingjun Hu,1– 4 Jie Wei,1– 3 Jie Hao,1– 3 Tianbo Jin,1– 3 Bin Li1– 3
1College of Life Sciences, Northwest University, Xi’an, Shaanxi Province, People’s Republic of China; 2Provincial Key Laboratory of Biotechnology of Shaanxi, Northwest University, Xi’an, Shaanxi Province, People’s Republic of China; 3Key Laboratory of Resource Biology and Biotechnology in Western China, Ministry of Education, Northwest University, Xi’an, Shaanxi Province, People’s Republic of China; 4Department of Neurosurgery, Xi’an Chang’an District Hospital, Xi’an, Shaanxi Province, People’s Republic of China
Correspondence: Mingjun Hu, College of Life Sciences, Northwest University, #229, Taibai North Road, Xi’an, Shaanxi Province, 710069, People’s Republic of China, Tel +86-15339228629, Email [email protected]
Background: Glioma is the main pathological subtype of brain tumors with high mortality.
Objective: This study aimed to elucidate the correlation between TREM1 variants and glioma risk in the Chinese Han population.
Methods: Genotyping of six variants of TREM1 was completed by Agena MassARRAY platform in 1061 subjects (503 controls and 558 glioma patients). The relationship between TREM1 polymorphisms and glioma risk was calculated using the logistic regression model, with odds ratio (OR) and 95% confidence intervals (CIs). A multifactor dimensionality reduction (MDR) method was performed to assess SNP–SNP interactions to predict glioma risk.
Results: In this research, overall analysis illustrated an association between TREM1 rs9369269 and an increased risk of glioma. Rs9369269 was also related to the risk of glioma in patients aged ≤ 40 years and females. Subjects with rs9369269 AC genotype were likely to obtain glioma compared to people with CC genotype (patients with astroglioma vs healthy people). Compared to TT genotype carriers, carriers with AT genotype of rs1351835 were significantly associated with overall survival (OS).
Conclusion: Taken together, the study identified the association between TREM1 variants and glioma risk and TREM1 variants were significantly associated with the prognosis of glioma. In the future, larger samples are needed to verify the results.
Keywords: glioma, TREM1, single nucleotide polymorphisms, risk
Introduction
Glioma, originated from glial or precursor cells, is the main pathological subtype of brain tumors, taking up about 80% of primary malignant brain tumors in human.1 Gliomas include astrocytoma, oligodendroglioma and ependymoma.2 According to their clinicopathological features, gliomas can be divided into grades I–IV, thereinto, grade IV glioma is also called glioblastoma multiforme. Despite great advances in glioma diagnosis, the number of gliomas remains increasing. In 2015, it was reported that 1,016,000 cases of brain and central nervous system (CNS) tumor were newly diagnosed in China, and the incidence rate in males was slightly higher than that in females.3 At present, surgery is the main treatment for glioma, and there are various treatments, such as chemotherapy, radiotherapy and immunotherapy. However, malignant brain tumors remain difficult to treat, and the overall survival rate (OS) was low.2 Therefore, it is urgent to study the pathogenesis of glioma. In recent years, some studies have shown that genetic factors were correlated with the risk and prognosis of glioma.4,5 The effect of genetic variants in glioma risk has attracted high attention, revealing that single nucleotide polymorphisms (SNPs) in cancer-related genes, such as TREH, IL4R, CCDC26, RTEL1, TERT, etc., were linked to the risk and prognosis of glioma.6–8
Triggering receptor expressed on myeloid cells 1 (TREM1) was a recently discovered cell surface receptor expressed on neutrophils and monocytes.9 As a member of the immunoglobulin superfamily, it can trigger the release of pro-inflammatory chemokines and cytokines (interleukin-8, tumor necrosis factor α and interleukin-1)10,11 and activate downstream signaling pathways by interacting with DAP12. In an article reported by Wu et al,12 loss of TREM1 attenuated hepatocellular carcinoma induced by diethylnitrosamine (DEN). When deletion is complemented, the development of hepatocellular carcinoma is exacerbated. Thus, TREM1 was a key determinant of hepatocellular carcinoma. Yang et al have also found that TREM1 level was increased under anoxic conditions and were associated with a marker of THP1-induced macrophage M2 polarization in glioblastoma cell line.13 TREM1 downregulation can reduce the migration and vascular morphology in glioblastoma cells. In vivo, it can inhibit tumor growth, probably by reducing the release of CSF1 cytokine.13 Therefore, TREM1 played a critical role in the development of glioma. SNPs have also been reported to be associated with the occurrence of diseases. For example, rs4711668 polymorphism in TREM1 gene was significantly associated with severe coronary atherosclerosis in Russian population.14 TREM1 rs2234237 was associated with malaria susceptibility in Colombian populations.15 However, no studies illustrated the association between TREM1 SNPs and glioma susceptibility.
In this study, based on the Agena MassARRAY platform, the association between polymorphisms of TREM1 and the risk of glioma was assessed in the Chinese population by logistic regression analysis, providing the theoretical basis for elucidating the mechanism of TREM1 in glioma.
Materials and Methods
Study Population
On the basis of G*Power (3.1.9.7) software, 1061 subjects (503 controls and 558 glioma patients) were randomly recruited from Xi’an Chang’an District Hospital. All glioma patients were confirmed by imaging and histopathological examination. The clinical information about glioma patients was collected by professionals, which included age, gender, surgical method, chemotherapy and radiotherapy regimen, the date of the last follow-up and the patient’s survival at the last follow-up. People with a history of cancer or brain and CNS diseases were excluded from the control group. The study was approved by the ethics committee of Xi’an Chang’an District Hospital and Northwest University and followed the Declaration of Helsinki. Each participant was informed of the purpose of this study and signed written informed consent.
SNP Selection and Genotyping
Based on the 1000 Genomes Project data, SNPs in TREM1 with minor allele frequency (MAF) >5%, Hardy-Weinberg equilibrium (HWE) >0.01 and r2 > 0.8 were selected from the global population. Blood samples (5mL) extracted from all participants were collected in EDTA-containing vacutainers, and gDNA was subsequently extracted by the GoldMag whole-blood genomic DNA purification kit (GoldMag Co. Ltd., Xi’an, China) to be the amplification template. MassARRAY iPLEX Gold Assay (Agena Bioscience, San Diego, CA, USA) was used for the genotyping of TREM1 polymorphisms. Also, the primers for amplification and extension were designed using the Agena MassARRAY Assay Design software, version 3.0 and remove the ineffective primers and nonspecific primers, and the sites with call rate greater than 95% were retained. The PCR reaction consisted of 1μL of 10ng/μL gDNA and 4μL of PCR mixture that contained 1.8μL of water, 0.5μL of 10×PCR buffer, 0.4μL of 25mM MgCl2, 0.1μL of 25mM dNTP, 1μL of PCR primer mix and 0.2μL of 5U/μL PCR Taq (Agena Bioscience, Inc., USA). The PCR conditions were as follows: initial denaturing at 95°C for 2 min, followed by 45 cycles of denaturing at 95°C for 30 s, annealing at 56°C for 30 s, and final extension at 72°C for 60 s. Then, the final step was to keep it at 25°C indefinitely. Matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) mass spectrometry was used to identify SNP alleles of different quality extension primers after alkaline phosphatase reaction, single group extension and resin desalination reaction. Finally, six SNPs (rs9369269, rs4714447, rs2170887, rs2234242, rs1351835 and rs2234237) were selected, and the information of PCR primers are shown in Supplementary Table 1. The MassARRAY Typer 4.0 software was used to perform data processing.
Statistical Analysis
Independent sample t-test and Pearson’s Chi-squared test were used to assess differences in the information of study subjects (age, gender, etc.). The genotype frequencies distribution of selected SNPs in the control group was evaluated by Pearson’s Chi-squared test to determine whether they were consistent with HWE. The distribution of allele frequencies of selected SNPs between cases and controls were also compared by Pearson’s Chi-squared test. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to evaluate the association between polymorphisms of TREM1 and glioma risk using logistic regression analysis. Codominant, dominant, recessive, and log-additive models were used for testing the relationship between TREM1 SNPs and glioma risk, as shown by PLINK software. In addition, using a bioinformatics database,16,17 we examined the expression level and prognosis of TREM1 in glioma patients. We also performed multivariate analyses of associations among genotypes, various factors, overall survival (OS) and progression-free survival (PFS), with hazard ratios (HRs) and 95% CIs. Multifactor dimensionality reduction (MDR) was conducted to assess SNP–SNP interactions in glioma risk assessment. All statistical analyses were calculated with SPSS software, version 27.0, and Excel software, version 22.0. p <0.05 was considered statistically significant.
Results
Study Subjects and Selected SNPs
This study included 503 controls and 558 glioma patients. The average ages of the two groups (p = 0.815) were 40.75 ± 13.99 years and 40.52 ± 18.08 years, respectively, and no age-related difference was observed. In addition, there was no gender difference between the two groups (p = 0.832). The clinical information about participants is shown in Table 1. Table 2 listed the information about the selected SNPs (rs9369269, rs4714447, rs2170887, rs2234242, rs1351835 and rs2234237) in TREM1. All SNPs were in accordance with HWE (p > 0.05).
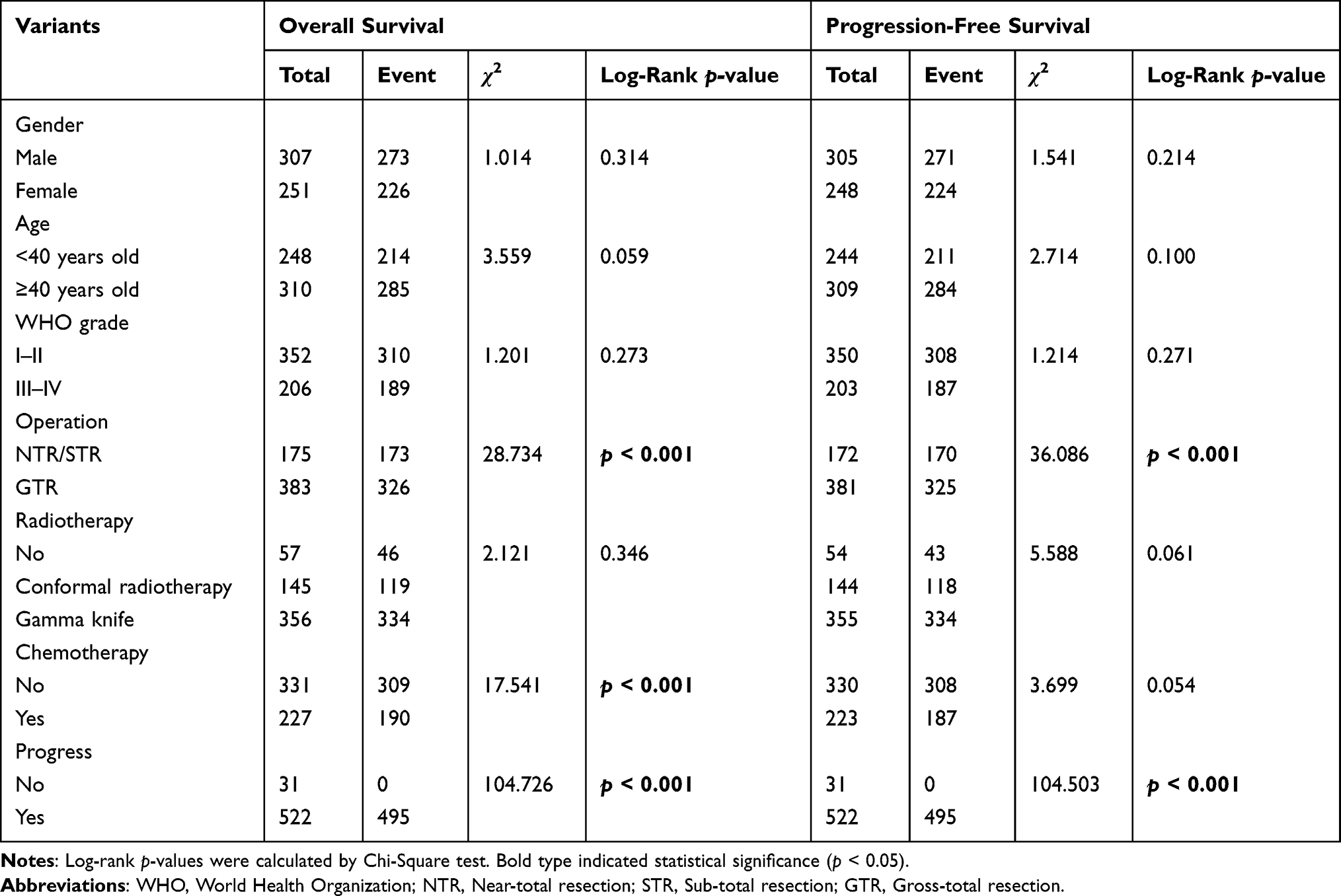 |
Table 1 Demographic and Clinical Information About Participants |
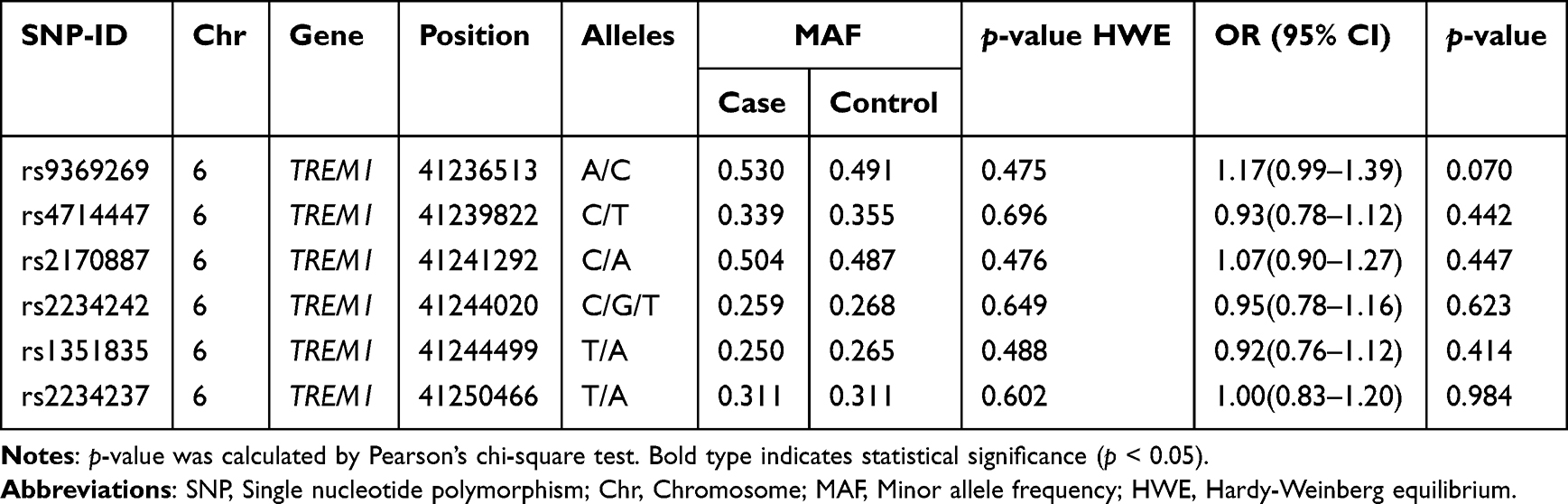 |
Table 2 The Basic Information About Selected SNPs |
The Correlation Between TREM1 Polymorphisms and Glioma Susceptibility
Multiple model analysis for the association between TREM1 polymorphisms and glioma risk is presented in Table 3 and Figure 1. The results showed a relationship between rs9369269 AC genotype and an increased glioma risk in the codominant model (OR = 1.46, 95% CI: 1.08–1.97, p = 0.014), and there was a correlation between C/C-A/C genotype of rs9369269 and an increased glioma risk in the dominant model, compared to the A/A genotype (OR = 1.44, 95% CI: 1.08–1.91, p = 0.013).
 |
Table 3 The Overall Association Analysis of TREM1 Variants with Glioma Susceptibility in Genetic Models |
 |
Figure 1 Overall analyses for the association between TREM1 variants and glioma susceptibility. Abbreviations: CI, Confidence interval; OR, Odds ratio. |
Besides, age- and gender-stratified analyses were completed to explore the influence of TREM1 polymorphisms on glioma risk (Table 4). Compared with the C/T-C/C genotype, the T/T genotype of rs4714447 in TREM1 could remarkably decrease the risk of glioma in patients aged >40 years in the recessive model (adjusted OR = 0.59, 95% CI: 0.35–0.99, p = 0.046), while rs9369269 was associated with a reduced risk of glioma (adjusted OR = 0.62, 95% CI: 0.40–0.95, p = 0.028) in patients aged ≤40 years. Furthermore, rs9369269 was found to be related to glioma risk in females (codominant model: adjusted OR = 1.94, 95% CI: 1.13–3.35, p = 0.017; dominant model: adjusted OR = 1.62, 95% CI: 1.05–2.50, p = 0.029; log-additive model: adjusted OR = 1.40, 95% CI: 1.06–1.83, p = 0.016), but no significance was observed in males.
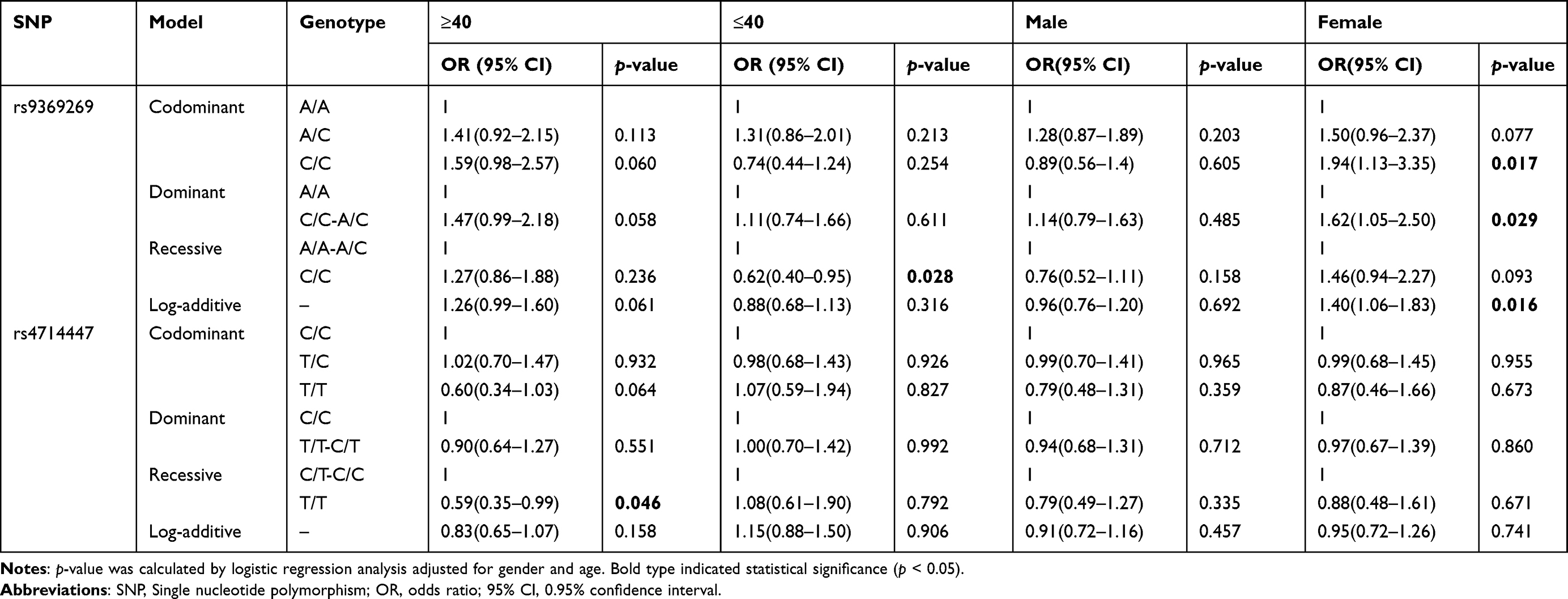 |
Table 4 The Association Between rs9369269 and rs4714447 and Glioma Susceptibility After Age- and Gender-Stratified Analyses |
Further, we assessed the association between TREM1 polymorphisms and clinical features of patients Supplementary Tables 2–4. As shown in Supplementary Table 2, while comparing patients with astroglioma and healthy subjects, subjects with rs9369269 A/C genotype were more likely to suffer from glioma than people with A/A genotype in the codominant model (adjusted OR = 1.39, 95% CI: 1.01–1.91, p = 0.045). While comparing patients with WHO grades I–II and patients with WHO grades III–IV, we observed a significant association between rs1351835 and a reduced risk of glioma, as shown in Supplementary Table 3 (adjusted OR = 0.38, 95% CI: 0.15–0.93, p = 0.035). In the Supplementary Table 4, we performed the multivariate analysis of associations among SNP genotypes, various factors, OS and PFS. As for rs1351835, compared to T/T genotype carriers, carriers with A/T genotype were significantly associated with OS (HR = 0.81, 95% CI: 0.67–0.97, p = 0.025), but not with PFS (HR = 0.86, 95% CI: 0.71–1.04, p = 0.119). Significant associations between rs9369269, rs4714447, rs2170887, rs2234242 and rs2234237 and OS, PFS were not observed.
SNP-SNP Interaction Was Used to Predict the Glioma Risk
In the Supplementary Table 5, MDR analysis showed that the model composed of rs9369269, rs4714447, rs2170887, rs2234242, rs1351835 and rs2234237, with 10/10 cross-validation consistency (CVC), the training accuracy of 61.39% and the testing accuracy of 49.3%, might be the best model to predict glioma risk (p < 0.001). The circle graph (Figure 2) indicates a positive interaction between rs2234242 and rs4714447, with the information gain (Ig) value of 0.2%. Rs430615 was also correlated with rs1351835 and rs2170887, with Ig value of 0.02%, 0.02%, respectively.
 |
Figure 2 Multifactor dimensionality reduction (MDR) was completed to assess the interaction among SNPs in TREM1 to predict glioma risk. |
Discussion
In this study, overall results illustrated that TREM1 rs9369269 was related to an increased glioma risk. Rs9369269 was also related to the risk of glioma in patients aged ≤40 years and females. Subjects with rs9369269 AC genotype were more susceptible to suffer glioma compared with people with CC genotype (patients with astroglioma vs healthy people). As for rs1351835, compared to TT genotype carriers, carriers with AT genotype were significantly associated with OS. Therefore, polymorphisms of TREM1 were important in the development and prognosis of glioma.
TREM1, also called CD354, is located in the chromosome of 6p21.1. TREM1 has been reported to enlarge the inflammatory response and act as a key mediator of inflammation. According to the report, elevated serum/plasma levels of sTREM-1 have been found in infectious and non-infectious inflammatory diseases.9,18 TREM1 downregulation can inhibit sepsis in mice.19 However, Mansur et al have20 reported that there was no association between the SNP-rs2234237- and the clinical course of sepsis in critically ill Caucasus patients. No correlation between rs2234237 and sepsis patients’ survival was detected. However, Su et al have discovered that the TREM1 expression level in the non-survival group was significantly higher than that in the survival group. TREM1 rs2234237 was also related to the prognosis of Chinese patients with sepsis, so it may be a risk factor for sepsis prognosis in Chinese individuals.21 The above results have shown that the association of TREM1 rs2234237 with sepsis is associated with the study population. In our study, TREM1 rs2234237 was first discovered to be related to the risk of glioma. However, we did not find a significant correlation between this locus and OS and PFS through multivariate analysis, and no significant correlation was found between rs2234237 and OS and PFS. In the future, we still need to explore the correlation between the TREM1 polymorphisms and OS and PFS through larger samples and extensive experiments.
The present study has some shortcomings. The collection of samples mainly concentrated in the Han nationality, and people of different races are needed to be collected for verification of the results. And the source of sample was mainly in one hospital, so glioma patients and healthy people from multiple hospitals are needed to be collected to verify the results. Besides, on the basis of the GEPIA database (http://gepia.cancer-pku.cn/), the association between TREM1 expression level and the prognosis of lower grade glioma was observed (Supplementary Figure 1). We need to continue to collect samples to verify the results, laying a theoretical foundation for the mechanism of TREM1 and its sites in the pathogenesis of glioma.
Data Sharing Statement
The data sets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Our research was approved by the ethics committee of the Xi’an Chang’an District Hospital and Northwest University, and all participants signed informed consent.
Acknowledgments
The authors thank the staff of Xi’an Chang’an District Hospital for their help in providing samples. The authors would also like to thank Dr Wenqian Zhou for her contributions in this study.
Funding
The study was supported by the Shaanxi Province Key Research and Development Program [grant number: 2022SF-582], the Scientific Research Project of Xi’an Municipal Health Commission [grant number: 2021ms04], and the Xi’an Science and Technology Plan Project [grant number: 21YXYJ0074].
Disclosure
The authors have declared that they have no conflicts of interest in this work.
References
1. Amirian ES, Armstrong GN, Zhou R, et al. The glioma international case-control study: a report from the genetic epidemiology of glioma international consortium. Am J Epidemiol. 2016;183(2):85–91. doi:10.1093/aje/kwv235
2. Lapointe S, Perry A, Butowski NA. Primary brain tumours in adults. Lancet. 2018;392(10145):432–446. doi:10.1016/s0140-6736(18)30990-5
3. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA. 2016;66(2):115–132. doi:10.3322/caac.21338
4. Chen Y, Wu Y, Huang X, et al. Leukocyte telomere length: a novel biomarker to predict the prognosis of glioma patients. J Cancer Res Clin Oncol. 2015;141(10):1739–1747. doi:10.1007/s00432-015-1938-x
5. Jin T, Wang Y, Li G, et al. Analysis of difference of association between polymorphisms in the XRCC5, RPA3 and RTEL1 genes and glioma, astrocytoma and glioblastoma. Am J Cancer Res. 2015;5(7):2294–2300.
6. Li S, Jin T, Zhang J, et al. Polymorphisms of TREH, IL4R and CCDC26 genes associated with risk of glioma. Cancer Epidemiol. 2012;36(3):283–287. doi:10.1016/j.canep.2011.12.011
7. Li G, Jin T, Liang H, et al. RTEL1 tagging SNPs and haplotypes were associated with glioma development. Diagn Pathol. 2013;8:83. doi:10.1186/1746-1596-8-83
8. Jin TB, Du S, Zhu XK, et al. Polymorphism in the IL4R gene and clinical features are associated with glioma prognosis: analyses of case-cohort studies. Medicine. 2016;95(31):e4231. doi:10.1097/md.0000000000004231
9. Bouchon A, Dietrich J, Colonna M. Cutting edge: inflammatory responses can be triggered by TREM-1, a novel receptor expressed on neutrophils and monocytes. J Immun. 2000;164(10):4991–4995. doi:10.4049/jimmunol.164.10.4991
10. Klesney-Tait J, Turnbull IR, Colonna M. The TREM receptor family and signal integration. Nat Immunol. 2006;7(12):1266–1273. doi:10.1038/ni1411
11. Liu N, Gu Q, Zheng YS. Expression of triggering receptor-1 in myeloid cells of mice with acute lung injury. World J Emerg Med. 2010;1(2):144–148.
12. Wu J, Li J, Salcedo R, et al. The proinflammatory myeloid cell receptor TREM-1 controls Kupffer cell activation and development of hepatocellular carcinoma. Cancer Res. 2012;72(16):3977–3986. doi:10.1158/0008-5472.Can-12-0938
13. Kong Y, Feng ZC, Zhang YL, et al. Identification of immune-related genes contributing to the development of glioblastoma using weighted gene co-expression network analysis. Front Immunol. 2020;11:1281. doi:10.3389/fimmu.2020.01281
14. Kutikhin AG, Ponasenko AV, Khutornaya MV, et al. Association of TLR and TREM-1 gene polymorphisms with atherosclerosis severity in a Russian population. Meta Gene. 2016;9:76–89. doi:10.1016/j.mgene.2016.04.001
15. Mario-Vásquez JE, Naranjo-González CA, Montiel J, et al. Association of variants in IL1B, TLR9, TREM1, IL10RA, and CD3G and Native American ancestry on malaria susceptibility in Colombian populations. Infect Genet Evol. 2021;87:104675. doi:10.1016/j.meegid.2020.104675
16. Dang HH, Ta HDK, Nguyen TTT, et al. Prospective role and immunotherapeutic targets of sideroflexin protein family in lung adenocarcinoma: evidence from bioinformatics validation. Funct Integr Genomics. 2022;22(5):1057–1072. doi:10.1007/s10142-022-00883-3
17. Dang HH, Ta HDK, Nguyen TTT, et al. Identifying GPSM family members as potential biomarkers in breast cancer: a comprehensive bioinformatics analysis. Biomedicines. 2021;9(9):1144. doi:10.3390/biomedicines9091144
18. Determann RM, Weisfelt M, de Gans J, et al. Soluble triggering receptor expressed on myeloid cells 1: a biomarker for bacterial meningitis. Intensive Care Med. 2006;32(8):1243–1247. doi:10.1007/s00134-006-0240-4
19. Chen Q, Zhou H, Wu S, et al. Lack of association between TREM-1 gene polymorphisms and severe sepsis in a Chinese Han population. Hum Immunol. 2008;69(3):220–226. doi:10.1016/j.humimm.2008.01.013
20. Runzheimer J, Mewes C, Büttner B, et al. Lack of an association between the functional polymorphism TREM-1 rs2234237 and the clinical course of sepsis among critically ill caucasian patients-a monocentric prospective genetic association study. J Clin Med. 2019;8(3):301. doi:10.3390/jcm8030301
21. Su L, Liu C, Li C, et al. Dynamic changes in serum soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) and its gene polymorphisms are associated with sepsis prognosis. Inflammation. 2012;35(6):1833–1843. doi:10.1007/s10753-012-9504-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.