Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Impact of Sex on Circulating Leukocytes Composition in COPD Patients
Authors Troianova N, Mariotti B, Micheletti V, Calzetti F, Donini M, Salvagno G, Ferrari M, Crisafulli E, Bazzoni F
Received 1 October 2021
Accepted for publication 6 December 2021
Published 25 December 2021 Volume 2021:16 Pages 3539—3550
DOI https://doi.org/10.2147/COPD.S341623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Natalia Troianova,1,* Barbara Mariotti,1,* Valentina Micheletti,2,3 Federica Calzetti,1 Marta Donini,1 Gianluca Salvagno,4,5 Marcello Ferrari,2,3 Ernesto Crisafulli,2,3 Flavia Bazzoni1
1Department of Medicine, Division of General Pathology, University of Verona, Verona, Italy; 2Department of Medicine, Respiratory Medicine Unit, University of Verona and Verona University Hospital, Verona, Italy; 3Department of Medicine, Section of Internal Medicine, University of Verona and Verona University Hospital, Verona, Italy; 4Section of Clinical Biochemistry, University Hospital of Verona, Verona, Italy; 5Service of Laboratory Medicine, Pederzoli Hospital, Peschiera del Garda, Italy
*These authors contributed equally to this work
Correspondence: Flavia Bazzoni
Department of Medicine, Division of General Pathology University of Verona, Strada le Grazie 8, Verona, 37134, Italy
Tel +39 045 8027128
Email [email protected]
Purpose: Chronic obstructive pulmonary disease is characterized by chronic inflammatory response both at the lung site and at the systemic level. Abnormalities in circulating leukocytes have been reported to occur in COPD patients and have been often shown to correlate with the decline in lung function. COPD affects men and women at a virtually comparable rate, even though distinct sex specific symptoms, progression and therapeutic implications have been described. Nonetheless, these sex-associated differences have not been analyzed in terms of circulating leukocytes. To assess the impact of sex on the changes of circulating immune cells in COPD patients.
Patients and Methods: Blood samples were collected from 50 COPD patients (31 males, 19 females) and 63 age and sex-matched controls (35 males, 28 females) enrolled in this pilot study. Complete blood cell count and multi-parametric flow cytometry analysis were performed to characterize the leukocyte populations and subsets.
Results: Male COPD patients are distinguished from controls by a significant increase in white blood cell counts, neutrophil total and differential counts, and neutrophil-to-lymphocyte ratio. Conversely, a generalized leukocyte decrease discriminated female COPD patients from the related controls. The impact of sex is further remarked by a decrease in adaptive immune cell subpopulations in males as opposed to a consistent increase of innate immune cell types in females correlating with disease severity.
Conclusion: These data indicate that the definition of specific changes of circulating leukocytes to be used as reliable biomarkers of the disease severity cannot be accomplished irrespectively of sex.
Keywords: sex, COPD, blood leukocytes, neutrophil-to-lymphocyte ratio, neutrophilia
Introduction
Chronic obstructive pulmonary disease (COPD) is an inflammatory disease of the lung characterized by airway obstruction and destruction of the parenchyma, leading to a progressive and irreversible decline in lung function.1 COPD is currently the third cause of death globally, after stroke and heart diseases,2 and it is expected to increase in the coming decades.3
Although the primary site of disease is the lung, COPD is recognized as a chronic inflammatory disorder. Initially considered a neutrophilic disease, based on the increased neutrophil count in bronchoalveolar lavage and peripheral blood, COPD is currently acknowledged as a disease in which innate and adaptive immunity play important roles in the development and progression.4 Furthermore, the components of this systemic inflammation may account for the systemic manifestations of COPD and may worsen comorbid diseases that affect outcomes in COPD patients, who mainly die of non-respiratory disorders such as cardiovascular diseases or cancer.5 Indeed, markers of systemic inflammation, including inflammatory cytokines, chemokines, acute phase proteins, and abnormalities in circulating leukocytes, have been correlated with different clinical aspects of the disease, such as incidence of exacerbations, disease severity, increased mortality or increased risk to develop one or more COPD-associated comorbidities.6
Among the different markers of disease severity, changes in the total and differential counts of circulating leukocyte populations have been reported to occur in COPD patients and have been often shown to correlate with the decline in lung function. In addition, the neutrophil-to-lymphocyte ratio (NLR), a reliable marker of systemic inflammation in several pathologies,7 is significantly elevated in acute as well as in stable COPD patients, suggesting that this simple, rapid, and cost-effective blood count index could be adopted as a valid parameter in the clinical evaluation of the disease.7 However, data on alterations of specific circulating leukocyte populations or of NLR values in COPD patients are highly discordant. The lack of consensus on the suitability of these parameters as disease biomarkers has been mainly ascribed to the considerable heterogeneity of the cohorts studied and the impact of factors such as comorbidities and smoking habits. Still, one factor likely impacting the inconsistency of circulating leukocyte data is represented by the patient sex, frequently neglected in the most of the analysis performed. However, COPD cannot be longer considered a disease that predominantly affects men, since in the last decade the prevalence of COPD among women has equaled that of men.8 Furthermore, several sex-based differences concerning susceptibility to tobacco exposure, phenotypic differences, symptoms, clinical parameters, quality of life, and therapeutic implication have been recently reviewed.9 Nevertheless, only few studies addressed the difference in circulating leukocyte in male and female COPD.
In order to fill up this gap of information, a preliminary study aimed at thoroughly characterizing changes in the absolute number and frequency of circulating leukocytes in stable male and female COPD patients and identifying potential correlations between defined leukocyte traits and clinical/diagnostic features was undertaken.
Patients and Methods
Patients
COPD patients (n = 50) and age- and sex-matched controls (n = 63) were obtained from the Respiratory Medicine Unit, Verona University Hospital, Verona, Italy. The local ethics committee approved the research protocol (protocol n. 42052/2015) in agreement with the principles of the Declaration of Helsinki. All patients and control subjects enrolled signed an informed consent form before participating in the study. Patients fulfilling the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria were diagnosed as COPD and graded for disease severity.10 All subjects met the following criteria: (i) older than 55 years old; (ii) not affected by infectious, inflammatory, autoimmune, lung (other than COPD), and neoplastic diseases or cancer history in the last three years; (iii) not under treatment with oral or systemic steroids.
Lung function was tested according to international recommendations.11 Forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), and FEV1/FVC ratio were measured with a flow-sensing spirometer connected to a computer for data analysis (Jaeger MasterScreen PFT System). FEV1 and FVC were expressed as absolute values and as percentage of the predicted values.12,13
Whole Blood Leukocyte Composition Analysis
Blood samples were collected in K2EDTA and analyzed using XN-9000 (Sysmex Co., Kobe, Japan), within 2 hours from sample collection. Blood leukocyte composition was reported both as count (cells × 106/mL) and as percentage of white blood cells (WBC). Neutrophil and lymphocyte counts obtained from automated Complete Blood Count (CBC) were used to calculate the Neutrophil-to-Lymphocyte Ratio (NLR).
Flow Cytometric Analysis of Circulating Leukocyte Populations
Leukocyte populations were characterized by multiparametric FACS analysis. Briefly, 50 µL of whole blood were incubated with specific fluorochrome-conjugated antibodies (Supplementary Table 1) for 15 min at room temperature in the dark. Erythrocytes were lysed by incubation with BD Pharm Lyse™ lysing Solution (BD Bioscience, San Diego, CA, USA) for 5 minutes followed by washing and resuspension in PBS + 2% FBS (≤10 EU/mL endotoxin, Millipore Sigma, St. Louis, Missouri, United States) + 2mM EDTA (Millipore Sigma, St. Louis, Missouri, United States) and immediately analyzed on the 8-colour MACSQuant Analyzer 10 flow cytometer (Miltenyi Biotec, Auburn, CA, USA). Data were analyzed using the FlowJo software (FlowJo 10.6.2, Ashland) following published guidelines.14 Cell count (cells ×106/mL) for each leukocyte population identified by FACS analysis was calculated based on the WBC count obtained from CBC.
Statistics
Dataset distribution was evaluated using the Shapiro–Wilk normality test. According to normality test results, analysis of differences was performed with Mann Whitney test or Student’s t-test. Impact of comorbidities and smoking on leukocyte counts was tested with the analysis of variance (ANOVA); non-normally distributed data were previously log-transformed. The correlation coefficient was determined using the Spearman rank correlation or the Pearson correlation test as appropriate. Statistical significance was defined as a P-value below 0.05. Statistical analysis was performed using GraphPad Prism version 8.0 (GraphPad Software Inc.) and R.
Results
Peripheral Blood Leukocyte Composition in COPD Patients
A case–control study of peripheral blood leukocytes composition was conducted in 50 COPD patients (31 males and 19 females) and 63 age and sex-matched controls (35 males and 28 females). The main features of COPD patients and age-matched controls enrolled in this study are summarized in Table 1. In order to characterize in details differences in the composition of circulating white blood cell (WBC), we first examined the absolute concentration and differential count of peripheral blood leukocytes from COPD patients. Total WBC counts, assessed by automated coulter Complete Blood Count (CBC), were not significantly different between the cohorts of COPD patients (6.5 [5.5–7.4] × 106/mL) and control subjects (6.1 [5.3–6.9] × 106/mL) (Figure 1A). No significant difference in total (Figure 1A) and differential counts (Figure 1B) of any leukocytes type was detected. Consequently, the neutrophil-to-lymphocyte ratio (NLR) value in COPD vs control cohorts was comparable (Figure 1A). However, when the same analysis was performed stratifying subjects by sex, male COPD patients were characterized by a significant leukocytosis (COPD 6.9 [5.8–7.6] × 106/mL vs Control 5.9 [5.3–6.6] × 106/mL, p = 0.0017) (Figure 1C), whereas female COPD showed a significant reduction of circulating leukocytes (COPD 5.6 [4.2–6.8] × 106/mL vs control 6.3 [5.3–7.9] × 106/mL, p = 0.038) (Figure 1E), as compared to the respective age and sex-matched controls (Supplementary Table 2).
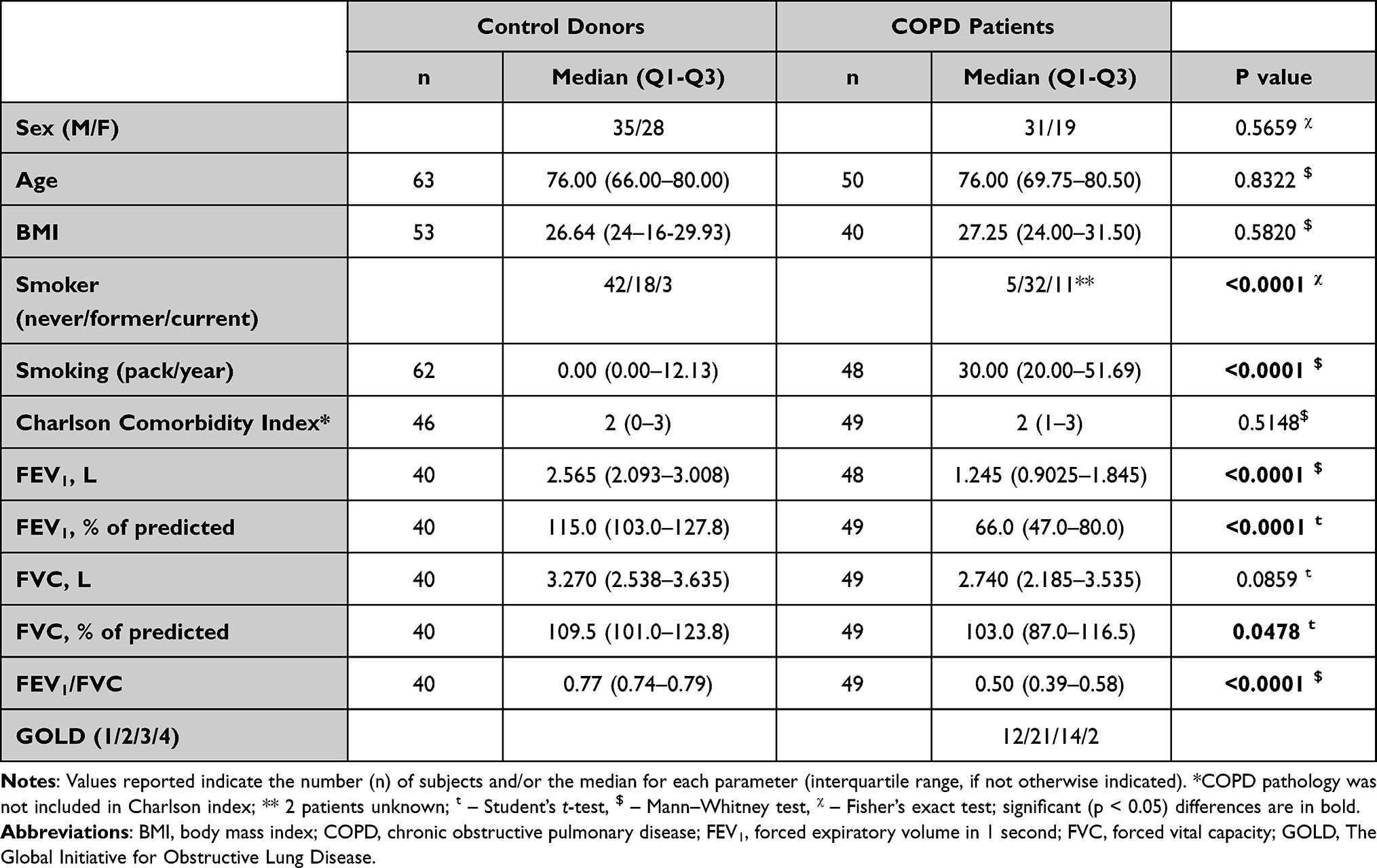 |
Table 1 Demographic Data for Recruited COPD and Control Subjects |
 |
Figure 1 Sex-specific alteration of circulating leukocytes in COPD patients and controls. White blood cells (WBC), neutrophils (N), lymphocytes (L), monocytes (M), eosinophils (E), basophils (B) total counts in controls (ctrl, empty dots) and COPD patients (black dots) complete cohorts (A), male cohort (C) and female cohort (E). Differential counts of neutrophils (N), lymphocytes (L), monocytes (M), eosinophils (E), basophils (B) in controls (empty dots) and COPD patients (black dots) complete cohorts (B), male cohort (D) and female cohort (F). The red line represents the median. *P < 0.05, **P < 0.01 according to Mann Whitney or Student’s t-test. |
A significant increase in NLR value was observed in the male COPD cohort compared to controls (Figure 1C). In contrast, the NLR value in female COPD patients and controls was comparable (Figure 1E), indicating that the increased NLR value detected in the total COPD versus the control cohort (2.4 [1.7–3.6] vs 2.1 [1.7–2.7], p = 0.073), even though not statistically significant, reflects an increase confined in the male population (Supplementary Table 2).
Analysis of the absolute and differential counts of leukocyte populations showed that the increased WBC and NLR in the male COPD cohort directly results from the increase in absolute (Figure 1C) as well as differential (Figure 1D) counts of neutrophils (Supplementary Table 2). Consequently, the lymphocyte frequency in WBCs decreased (Figure 1D), whereas the absolute number of lymphocytes was comparable to that of controls (Figure 1C). Conversely, absolute count and frequency of lymphocytes, monocytes, eosinophils and basophils were equally represented in male COPD and control group (Figure 1C and D and Supplementary Table 2). On the opposite, the reduction of total WBC in female COPD patients versus the respective controls (Figure 1E) resulted from a reduction of each leukocyte population analyzed that reached statistically significant values for lymphocytes (p = 0.029) and monocytes (p = 0.0286) (Figure 1E). As expected, the frequency of every leukocyte population in female COPD patients was comparable to that of controls (Figure 1F and Supplementary Table 2). Collectively, data show that in COPD patients sex is a relevant factor conditioning circulating leukocyte homeostasis. Data also uncover that while neutrophilia is a potential hallmark of COPD in males, a generalized leukopenia characterizes COPD in the female population.
Characterization of Circulating Leukocyte Subtypes in COPD Patients
We then characterized leukocyte subsets of COPD patients by flow-cytometry. Myeloid cell subtypes were identified according to the gating strategy shown in Supplementary Figure 1. Flow-cytometry analysis showed that the frequencies of different monocyte subsets, (classical, monocyte-myeloid-derived suppressor cells (M-MDSC), intermediate, and non-classical), were similarly represented in COPD and controls both for males (Figure 2A) and females (Figure 2B and Supplementary Table 3). Likewise, no difference in total dendritic cells (DC) and DC subtypes (pDC, cDC1, cDC2) was detected (Figure 2C-F and Supplementary Table 3).
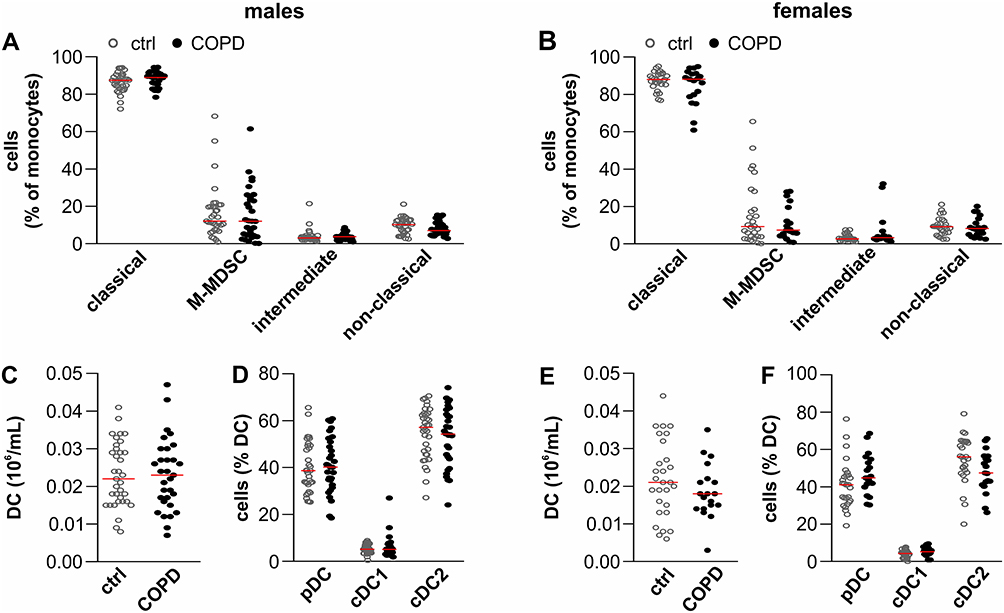 |
Figure 2 Characterization of monocyte and dendritic cell subtypes populations in COPD patients and controls. Frequency of classical monocytes, monocytic-myeloid derived suppressor cells (M-MDSC), intermediate monocytes and non-classical monocytes in total monocytes are shown for male (A) and female (B) COPD patients and controls (ctrl). In addition, total DCs (C and E), as well as the frequency of plasmacytoid (pDC), conventional DC1 (cDC1) and DC2 (cDC2) in DCs (D and F) are shown for male (C and D) and female (E and F) COPD and control donors. Controls: empty dots, COPD: black dots. The red line represents the median. |
Lymphoid populations and CD4+ T lymphocyte subtypes were identified according to the gating strategy shown in Supplementary Figure 2. No significant difference in the absolute numbers of T (CD3+), B (CD3−CD19+), NK (CD3−CD19+CD56+) and NKT (CD3+CD56+) cells in male COPD patients versus controls was observed (Figure 3A). Conversely, a reduction of each of these lymphocyte populations was detected in female COPD compared to controls (Figure 3B). However, such a reduction reached statistically significant value only for B cells (Supplementary Table 4). Notably, these data further strengthened the observation that every single leukocyte subtype contributes to the significant reduction of WBC detected in the female COPD cohort.
 |
Figure 3 Characterization of lymphoid populations in COPD patients and controls. (A and B) T lymphocytes, B lymphocytes, NK cells and NKT cells counts in male (A) and female (B) COPD and control (ctrl) donors. (C and D) Differential counts of T helper cells (CD3+CD4+, Th) and cytotoxic T-lymphocytes (CD3+CD8+, CTLs) in total T cells in male (C) and female (D) COPD and control donors. (E and F) Differential counts of Th1, Th2, Th17, Th1/Th17 and regulatory T cells (Treg) in total T helper cells in male (E) and female (F) COPD and control donors. Controls: empty dots, COPD: black dots. The red line represents the median. *P < 0.05 according to Mann Whitney test, **P < 0.01 according to Student’s t-test. |
No significant variation in the frequencies of CD4+ T helper (Th) and CD8+ cytotoxic T-lymphocyte (CTL) subsets was observed (Figure 3C male, and 3D female). However, in the context of CD4+ Th lymphocytes, the frequency of regulatory T-cells (Treg, CD127−CD25+) was significantly increased both in male (Figure 3E) and female (Figure 3F) COPD patients as compared to their related controls. Otherwise, the frequency of Th1 (CXCR3+CCR6−), Th2 (CD3+CRTH2+), Th17 (CXCR3−CCR6+) Th1/17 (CXCR3+CCR6+) lymphocytes (Figure 3E male and 3F female) in COPD patients and controls was comparable.
These data collectively emphasize that changes in circulating leukocyte composition in COPD patients are influenced by sex. While general leukopenia can be demonstrated in female COPD patients, male COPD patients are characterized by a significant increase in the absolute number of circulating leukocytes resulting from increased neutrophils. Remarkably, both male and female COPD patients show a significant increase in Treg frequency within CD4+ T cells.
Impact of COPD Severity, Comorbidities and Smoking on Circulating Leukocyte Composition
COPD is usually associated with concomitant chronic diseases, such as hypertension, diabetes, dyslipidemia, cardiovascular diseases (CVD), and coronary artery disease (CAD); these comorbidities increase COPD morbidity and mortality.5 Moreover, these pathological conditions have been shown to cause by themselves systemic changes, including alteration in peripheral blood leukocyte composition. Smoking is also known to have a profound impact per se on circulating leukocyte composition.15 Concerning comorbidities, while the female cohort (COPD and controls) was perfectly balanced, the male cohort was not balanced for the incidence of CAD, hypertension and arthrosis (Supplementary Table 5). Regarding the smoking habit, both smoking frequency and index (pack/year) were significantly different in the male and female COPD as compared to their respective controls (Supplementary Table 5).
On these bases, the influence of CAD, hypertension and arthrosis in the male cohort, together with the influence of smoking history in male and female cohorts on peripheral blood cell homeostasis was evaluated by Analysis of Variance (ANOVA) (Figure 4). CAD, hypertension, and arthrosis were not sufficient per se to determine the significant changes in WBC, NLR, neutrophil counts and frequency of Treg in CD4+ T cells observed in the male cohort (Figure 4A). Similarly, smoking was not responsible of the changes observed in COPD vs controls, both in the male and female cohorts (Figure 4). Collectively, this analysis indicates that the COPD pathology is an independent factor responsible for the majority of the statistically significant variations of the leukocyte parameters identified in male and female cohorts also after adjustment to smoking and comorbidities.
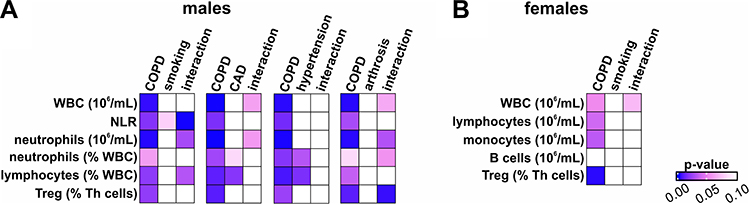 |
Figure 4 Impact of smoking and comorbidities on leukocyte parameters in male and female COPD patients. Heat map representation of the ANOVA analysis in male (A) and female (B) COPD patients and sex matched controls. P-value obtained from the ANOVA analysis for COPD, smoking, CAD, hypertension or arthrosis alone or interacting with COPD (interaction) are plotted according to the scale shown on the right. The smoking impact was evaluated by grouping donors according to smoking index (pack/year) in: “very light” (pack/year < 15); “light” (pack/year 15–30), and “heavy” (pack/year ≥ 30). |
Imbalanced distribution of the degree of disease severity, smoking habit and/or comorbidities between male and female COPD patients, independently from their respective controls, may also introduce a bias in the analysis of the role of sex in circulating leukocyte composition of COPD patients compared to sex-matched controls. Therefore, the distribution of clinical parameter of COPD severity (GOLD stage, FEV1% of predicted, FEV1/FVC), smoking habits, and comorbidities (Carlson Comorbidity Index – CCI, CVD, CAD, allergy, hypertension, dyslipidemia, arthrosis, thyroid disease and BMI) in male and female COPD enrolled in the study was examined. Statistical analysis showed that male and female COPD groups were perfectly balanced for all these parameters, except than for CCI and allergy (Supplementary Table 6). To determine the potential impact of CCI and allergy on circulating leukocytes, we first identified WBC population significantly different between the male and female COPD groups (Supplementary Figure 3A). WBC, neutrophil and monocyte counts were significantly higher in male as compared to female COPD, while the opposite was observed for lymphocytes (Supplementary Figure 3A). ANOVA analysis of the impact of sex, CCI and allergy alone or in combination allowed us to exclude that an uneven distribution of factors, such as CCI and/or allergy, affect the outcome of this analysis (Supplementary Figure 3B).
Correlation of Leukocyte Counts to Clinical Parameters
To understand whether circulating leukocyte composition varied according to COPD disease severity, we searched for potential correlations between defined leukocyte traits and clinical features. There is consensus that FEV1 does not adequately describe the complexity of the disease and that FEV1 alone cannot be used for an optimal diagnosis. However, a clear alternative has not yet been defined. To overcome this limitation, FEV1% of predicted, FEV1/FVC, and GOLD stage were chosen as representative of COPD severity. A direct correlation between the cell counts and FEV1%, FEV1/FVC, and an inverse correlation between cell counts and GOLD stage indicates a progressive decrease of the given cell type with the disease severity. On the contrary, an inverse correlation between the number and/or the frequency of a given cell type with FEV1% of predicted, FEV1/FVC, and a direct correlation with GOLD stage marks a progressive increase of the indicated cell type with disease severity. Among all circulating leukocytes, some populations were found to correlate with one or more parameters of COPD severity (Figure 5 and Supplementary Table 7). Remarkably, heat map representation of the type and number of correlations indicated that circulating leukocytes and disease severity changes are once again influenced by sex (Figure 5). Specifically, a decrease in WBC, total lymphocytes, B, and NKT cell counts and the increase in COPD severity were observed in the male cohort (Figure 5 and Figure 6). Conversely, an increase in the frequency of Th1 and Treg in CD4+ Th lymphocytes correlated with reduced lung function in the female cohort. Remarkably, an increase only of the myeloid cell types was observed in more severe female COPD patients (Figures 5 and 7). Specifically, both eosinophils (Figure 7E and F) and basophils (Figure 7G) correlated with disease severity in female COPD patients. Moreover, a progressive imbalance in DC populations, with an increase in cDC1 frequency in females (Figure 7H-J) and cDC2 frequency in males (Figure 6I), associated with the disease progression was observed. Surprisingly, a significant decrease in M-MDSC number (not shown) and frequency in monocytes (Figures 5 and 7K-M) was detected in more severe female COPD patients.
 |
Figure 5 Correlation of leukocyte populations with parameters of COPD severity. Correlation analysis between all leukocyte populations and FEV1% of predicted, FEV1/FVC or GOLD was performed separately for male and female COPD patients. Heatmap shows all leukocyte populations correlating in a statistically significant manner (P < 0.05) with at least one clinical parameter in male (left) or female (right) COPD patients. The color scale indicates the degree of the correlation: blue = leukocyte amount decreases with COPD severity; red = leukocyte amount increases with diseases severity. Raw Spearman or Pearson correlation coefficient is reported inside the heatmap. |
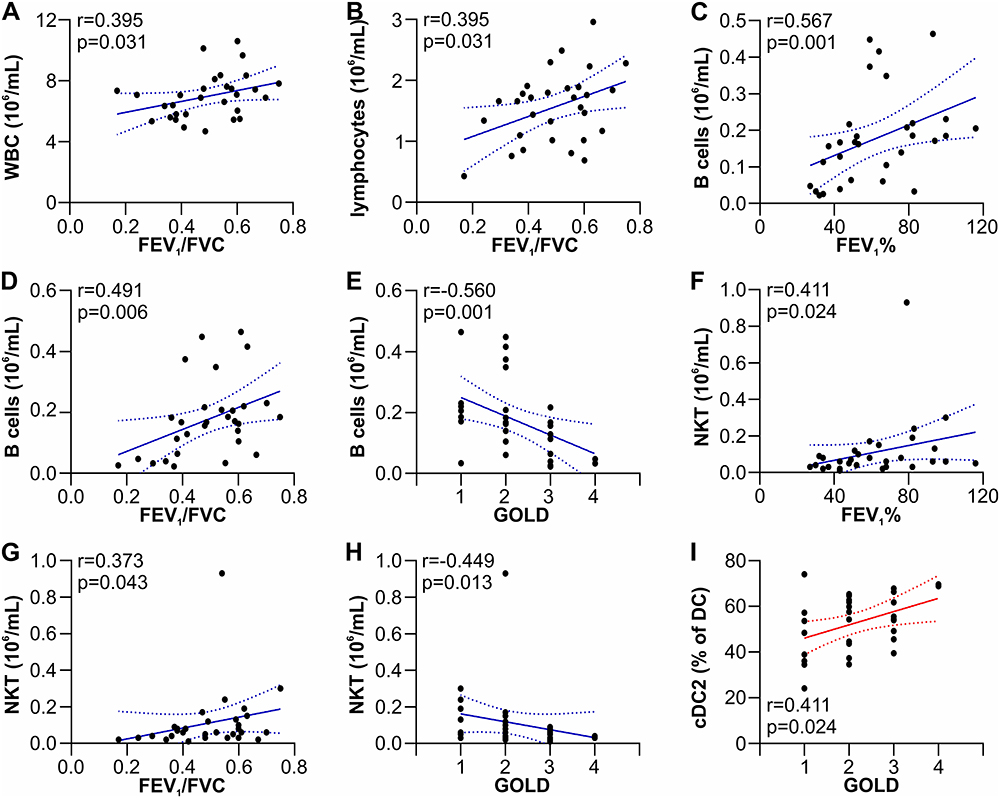 |
Figure 6 Correlation of leukocyte populations with COPD severity parameters in male COPD patients. Correlation between: WBC (A) or lymphocyte count (B) with FEV1/FVC; B cell count with FEV1% (C), FEV1/FVC (D) and GOLD (E); NKT cell count with FEV1% (F), FEV1/FVC (G) and GOLD (H); cDC2 frequency with GOLD (I). Linear regression and 95% confidence interval are drawn. Spearman of Pearson correlation coefficient (r) and p-value (P) are shown. |
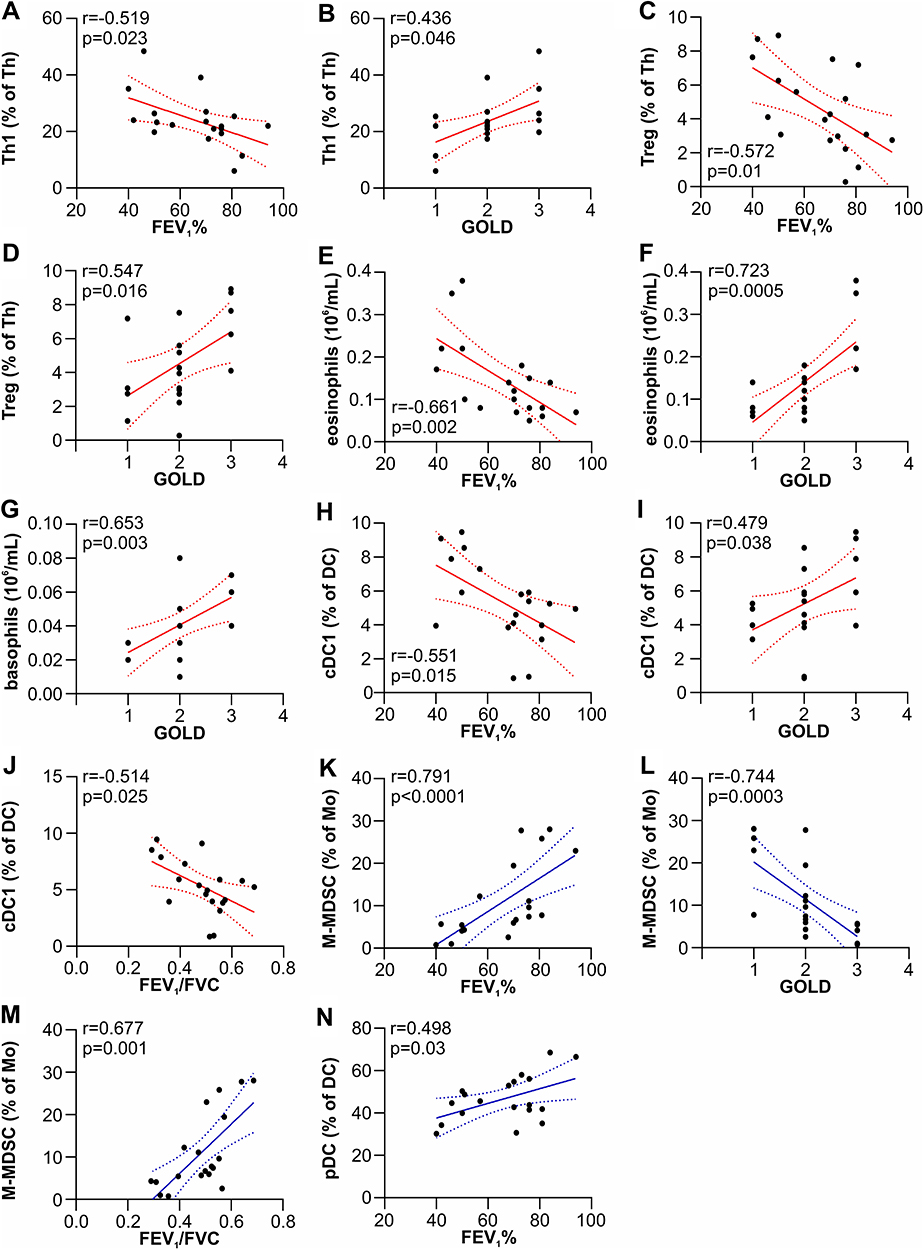 |
Figure 7 Correlation of leukocyte populations with COPD severity parameters in female COPD patients. Correlation between: Th1 cell frequency with FEV1% (A) and GOLD (B); Treg cell frequency with FEV1% (C) and GOLD (D); eosinophil count with FEV1% of predicted (E) and GOLD (F); basophil count with GOLD (G); cDC1 frequency with FEV1% (H), GOLD (I) and FEV1/FVC (J); M-MDSC frequency with FEV1% (K), GOLD (L), and FEV1/FVC (M); pDC count with FEV1% (N). Linear regression and its 95% confidence interval are drawn. Spearman or Pearson correlation coefficient (r) and p-value (P) are shown. |
Discussion
Analysis of circulating blood leukocyte composition conducted on a pilot study of stable COPD patients and age-matched controls uncovered that sex plays a role in driving changes in the absolute number and differential counts of discrete circulating leukocyte types. Briefly, male COPD patients are characterized by a significantly higher neutrophil-to-lymphocyte ratio (NLR), consequent to a significant increase in neutrophils’ total number and frequency. Differently, female COPD patients are characterized by a generalized leukopenia, involving the majority of leukocyte populations. The only feature shared by both male and female COPD cohorts is the increased frequency of Treg within CD4+ T cells. Even though limited to a small cohort of subjects, such sex-specific profiles identified could not be attributed to coexisting conditions, such as comorbidities or smoking habit, or differences in the clinical parameters of the male and female COPD patients enrolled, as assessed by ANOVA analysis.
These findings are particularly relevant in the context of recent works suggesting NLR as diagnostic and prognostic marker in COPD7 and help re-evaluate discrepancies in the literature data. For example, studies that identified differences in NLR values yielded contrasting results, ranging from significantly higher to equivalent NLR values in stable COPD than age-matched controls. Similarly, inconsistencies also exist concerning either the association between NLR and clinical parameters in stable COPD or the potential use of NLR as a predictor of COPD severity. Such differences have been attributed mainly to methodological issues and the variability of the different cohorts investigated. Such variables include ethnic differences, age range, comorbidities, but no attention to sex distribution has been given. While gender differences in plasma biomarker levels have been investigated,16 very few studies focused on the role of sex on white blood cell composition changes in COPD patients has been performed. Of note, this is somehow surprising, since the impact of sex on several features of COPD, such as susceptibility, clinical presentation, symptoms, prognosis, severity, and comorbidities, is widely acknowledged.17 Indeed, retrospectively, studies reporting a significant increase in WBC and neutrophil count have been performed on cohorts composed predominantly of male subjects, while no difference in circulating leukocyte parameters have been reported in studies performed on sex-balanced cohorts. This issue is emphasized in a recent comprehensive meta-analysis, claiming that the most significant limitation of the study was that men were the sole focus of almost one-third of the screened articles.18 This lack of information represents a hurdle in the identification of reliable biomarkers, particularly of those related to persistent elevation of inflammatory markers, which are related to the progression of the disease, clinical and functional parameters, and the development of comorbidities.
Remarkably, we found that sex, other than being relevant in driving changes in peripheral blood cell homeostasis, also impacted on changes of circulating leukocyte composition during different stages of the disease. Specifically, while a decrease of the absolute number of lymphocytes (B cells, T cells, and NKT) correlated with COPD disease severity in males, an increase in the absolute number of granulocytes (eosinophils and basophils) and the frequency of cDC1 dendritic cell populations marked severe COPD patients in females.
Over the last years, several other circulating leukocytes have been investigated, and imbalances in the number and/or activation status of different circulating immune cell subsets have been associated with various diagnostic and prognostic parameters. However, once again, because of the variability of the different cohorts investigated together with the variation in the way leukocyte subtypes were sampled and analyzed, it is not surprising that contrasting results occur in this field. For these reasons, we believe that discussing the results obtained in this work for each leukocyte subtype in the context of the literature would not add a significant contribution to the current knowledge. We are aware that the sample size of the cohort investigated represents a limitation and results need to be validated on larger cohorts. Nevertheless, the added value of this preliminary study consists in providing evidence for the role of sex as a significant driver of the dynamic changes occurring in COPD patients. Most importantly, seen as a whole, our data show that sex may affect the dynamic of these modifications at different stages: a pro-inflammatory profile characterized by an increase in innate immune cells (i.e. neutrophils) is an early hallmark of COPD in males, clearly detectable from GOLD stage 1 to 4. Otherwise, a decrease in lymphocyte number can be observed only in more severe male patients. In contrast, a decrease in adaptive immune cells types marks female COPD from the initial stages of the disease. In addition, a pro-inflammatory profile, characterized by increased eosinophils and basophils count and Th1 cell frequency, is detectable at more severe stages of the disease in females (Figure 8).
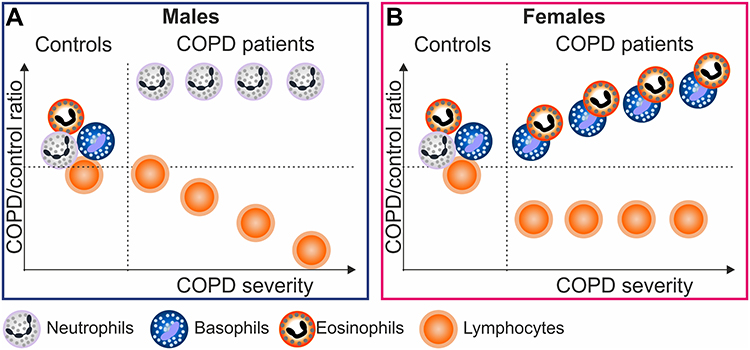 |
Figure 8 Dynamic changes in circulating leukocytes in different stages of COPD in males and females. Graphs represent the ratio COPD/controls for granulocytes and lymphocytes. In male COPD (A), a significant increase in neutrophils compared to controls, is detectable at early stages and it is maintained elevated throughout all the disease stages, while a decrease in lymphocyte number can be observed only in more severe male patients. In females (B), hallmark of COPD is represented by a significant reduction in lymphocyte number compared to controls, and an increase in eosinophils and basophils can be observed only as the disease progresses. |
Accumulating evidence show that sex affects innate and adaptive immune responses to self and foreign antigens, consequentially yielding to differences in several pathologic conditions, as well as in responses to infections and vaccines19,20 This preliminary study provides experimental evidence supporting the awareness that sex-disaggregated data should be considered when searching for reliable biomarkers21 and that sex should be integrated as biological variable in all stages, from basic research to clinical analysis and evaluation.22
Conclusion
This study provides experimental evidence supporting the awareness that sex-disaggregated data should be considered as an essential rule when moving toward precision pulmonary medicine. In fact, the results of our study uncovered that sex plays a role not only in driving changes in the absolute number and frequency of discrete circulating leukocyte types in COPD patients as compared to age- and sex-matched controls but also that it affects the dynamic of these modifications at different stages: a pro-inflammatory profile is an early hallmark of COPD in males, followed by a reduction of lymphocytes as the disease progresses. In contrast, a decrease in adaptive immune cells types marks female COPD from the initial stages of the disease, while a proinflammatory profile is detectable at more severe stages of the disease in females.
Abbreviations
CAD, coronary artery disease; CBC, complete blood count; cDC1, type 1 conventional dendritic cells; cDC2, type 2 conventional dendritic cells; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; DC, dendritic cells; FACS, fluorescence activated cell sorter; FBS, fetal bovine serum; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GOLD, The Global Initiative for Obstructive Lung Disease; M-MDSC, monocyte-myeloid-derived suppressor cells; NK, natural killer cells; NKT, natural killer T cells; NLR, neutrophil-to-lymphocyte ratio; pDC, plasmacytoid dendritic cell; Th, T helper cells; Th1, type 1 T helper cells; Th2, type 2 T helper cells; Th17, T helper 17 cells, Th1/17, Th1-like T helper 17 cells; Treg, regulatory T cells; WBC, white blood cells.
Ethics Approval and Informed Consent
All samples were obtained after donors provided written informed consent and after approval of the study by the Ethics Committee for Clinical Research of Verona and Rovigo Province (research protocol n. 42052/2015).
Acknowledgments
We are grateful to all the donors who participated this study.
Author Contributions
N.T., B.M. collected and analyzed the data, V.M., F.C., M.D. recruited patients and controls and performed FACS analysis, G.S. provided automated cell counts for all the subjects enrolled, M.F., E.C., conceived and designed the study. F.B. conceived and designed the study and drafted the manuscript. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by Progetti di Ricerca di Interesse Nazionale (PRIN2017, Prot. 20174T7NXL), and by Joint Project 2017 (JPVR2017), Ateneo di Verona.
Disclosure
Valentina Micheletti present affiliation: U.O.C. Palliative Cares, ULSS8 Berica, Vicenza, Italy. The authors declare no conflicts of interest.
References
1. Barnes PJ. Chronic obstructive pulmonary disease. N Engl J Med. 2000;343(4):269–280. doi:10.1056/NEJM200007273430407
2. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
3. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
4. Halper-Stromberg E, Yun JH, Parker MM, et al. Systemic markers of adaptive and innate immunity are associated with chronic obstructive pulmonary disease severity and spirometric disease progression. Am J Respir Cell Mol Biol. 2018;58(4):500–509. doi:10.1165/rcmb.20170373OC
5. McGarvey LP, Magder S, Burkhart D, et al. Cause-specific mortality adjudication in the UPLIFT(R) COPD trial: findings and recommendations. Respir Med. 2012;106(4):515–521. doi:10.1016/j.rmed.2011.10.009
6. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
7. Pascual-Gonzalez Y, Lopez-Sanchez M, Dorca J, Santos S. Defining the role of neutrophilto-lymphocyte ratio in COPD: a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2018;13:3651–3662. doi:10.2147/COPD.S178068
8. Buttery SC, Zysman M, Vikjord SAA, Hopkinson NS, Jenkins C, Vanfleteren L. Contemporary perspectives in COPD: patient burden, the role of gender and trajectories of multimorbidity. Respirology. 2021;26(5):419–441. doi:10.1111/resp.14032
9. Perez TA, Castillo EG, Ancochea J, et al. Sex differences between women and men with COPD: a new analysis of the 3CIA study. Respir Med. 2020;171:106105. doi:10.1016/j.rmed.2020.106105
10. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
11. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
12. Cotes JE, Chinn DJ, Quanjer PH, Roca J, Yernault JC. Standardization of the measurement of transfer factor (diffusing capacity). Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J Suppl. 1993;16:41–52.
13. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC. Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J Suppl. 1993;16:5–40.
14. Cossarizza A, Chang HD, Radbruch A, et al. Guidelines for the use of flow cytometry and cell sorting in immunological studies (second edition). Eur J Immunol. 2019;49(10):1457–1973. doi:10.1002/eji.201970107
15. Pedersen KM, Colak Y, Ellervik C, Hasselbalch HC, Bojesen SE, Nordestgaard BG. Smoking and increased white and red blood cells. Arterioscler Thromb Vasc Biol. 2019;39(5):965–977. doi:10.1161/ATVBAHA.118.312338
16. de Torres JP, Casanova C, Pinto-Plata V, et al. Gender differences in plasma biomarker levels in a cohort of COPD patients: a pilot study. PLoS One. 2011;6(1):e16021. doi:10.1371/journal.pone.0016021
17. Grabicki M, Kuznar-Kaminska B, Rubinsztajn R, et al. COPD course and comorbidities: are there gender differences? Adv Exp Med Biol. 2019;1113:43–51. doi:10.1007/5584_2018_160
18. Han MK. Chronic obstructive pulmonary disease in women: a biologically focused review with a systematic search strategy. Int J Chron Obstruct Pulmon Dis. 2020;15:711–721. doi:10.2147/COPD.S237228
19. Klein SL, Flanagan KL. Sex differences in immune responses. Nat Rev Immunol. 2016;16(10):626–638. doi:10.1038/nri.2016.90
20. Markle JG, Fish EN. SeXX matters in immunity. Trends Immunol. 2014;35(3):97–104. doi:10.1016/j.it.2013.10.006
21. DeMeo DL. Sex and gender omic biomarkers in men and women with COPD: considerations for precision medicine. Chest. 2021;160(1):104–113. doi:10.1016/j.chest.2021.03.024
22. Klein SL, Schiebinger L, Stefanick ML, et al. Opinion: sex inclusion in basic research drives discovery. Proc Natl Acad Sci USA. 2015;112(17):5257–5258. doi:10.1073/pnas.1502843112
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.