Back to Journals » International Journal of Women's Health » Volume 12
Impact of Recurrent Miscarriage on Maternal Outcomes in Subsequent Pregnancy: The Mutaba’ah Study
Authors Ali N, Elbarazi I ![]() , Ghazal-Aswad S, Al-Maskari F
, Ghazal-Aswad S, Al-Maskari F ![]() , Al-Rifai RH
, Al-Rifai RH ![]() , Oulhaj A, Loney T
, Oulhaj A, Loney T ![]() , Ahmed LA
, Ahmed LA ![]()
Received 28 May 2020
Accepted for publication 12 October 2020
Published 8 December 2020 Volume 2020:12 Pages 1171—1179
DOI https://doi.org/10.2147/IJWH.S264229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Nasloon Ali,1 Iffat Elbarazi,1 Saad Ghazal-Aswad,2 Fatima Al-Maskari,1,3 Rami H Al-Rifai,1,3 Abderrahim Oulhaj,1,3 Tom Loney,4 Luai A Ahmed1,3
1Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates; 2Obstetrics and Gynecology Department, Tawam Hospital, Al Ain, United Arab Emirates; 3Zayed Centre for Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates; 4College of Medicine, Mohammed Bin Rashid University of Medicine and Health Sciences, Dubai, United Arab Emirates
Correspondence: Luai A Ahmed
Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, PO Box 17666, Al Ain, United Arab Emirates
Tel +971 37137511
Email [email protected]
Purpose: To estimate the prevalence of recurrent miscarriage (RM) and investigate the association between RM and adverse maternal outcomes in subsequent pregnancies.
Participants and Methods: This is an interim analysis of a prospective study of 1737 pregnant women with gravidity of two or more prior to the current pregnancy. These women joined the Mutaba’ah Study between May 2017 and April 2019 and were followed up until they delivered. Hospital medical records were used to extract data on past pregnancy history and the progress and outcomes of the current pregnancy, such as gestational diabetes, preeclampsia, mode of delivery, preterm delivery, and complications at birth.
Results: Amongst pregnant women with at least two previous pregnancies (n=1737), there were 234 (13.5%) women with a history of two or more consecutive miscarriages. Women with RM were slightly older, more parous, and more likely to have had previous infertility treatment (all p-values < 0.05). Women with a history of RM had independently significant increased odds of cesarean section (adjusted odds ratio (aOR) 1.81, 95% CI 1.24– 2.65) and preterm (< 37 weeks, aOR: 2.52, 95% CI 1.56– 4.08) or very preterm delivery (< 32 weeks, aOR: 7.02 95% CI 2.41– 20.46) in subsequent pregnancies than women who did not have a history of RM.
Conclusion: Women with a history of RM were twice as likely to undergo cesarean section and seven times more likely to deliver prior to 32 weeks of gestation than women without a history of RM. The study findings support the need for early pregnancy monitoring or assessment units to ensure better follow-up and customized care for at-risk pregnant women with a history of RM.
Keywords: cesarean section, cohort study, miscarriage, preterm delivery, recurrent miscarriage
Introduction
Recognized miscarriages in clinical settings occur in approximately 15–20% of all pregnancies.1 Recurrent miscarriages (RM), defined as two consecutive miscarriages before the 20th week of gestation,2–6 are less common and affect 1–5% of fertile women.7 The current available literature on RM primarily focuses on the possibility of future loss8 and the psychological distress caused by RM,9 such as poorer mental health outcomes after the loss10 and during subsequent pregnancies.11 While most women who experience RM proceed to have healthy live births,12 studies show that RM is associated with some unfavorable outcomes, such as placental dysfunctions, preterm births, and assisted deliveries, in future pregnancies.13–16 It has also been shown that women with RM are more likely to develop gestational hypertension and gestational diabetes mellitus [GDM] during their subsequent pregnancies.12,17 Furthermore, babies born to women with a history of RM were at an increased risk of low birth weight and being small or large for gestational age.12 Nevertheless, there is a need for further studies that investigate the influence of RM on a wider range of outcomes in future pregnancies.18 Currently, there is a lack of data on RM in the United Arab Emirates (UAE) and the surrounding region.19,20 The limited available research is generally focused on the biochemical processes of RM. Therefore, population-based studies with longitudinal designs are required to assess the epidemiological burden of RM and its influence on maternal health outcomes. This study aims to estimate the prevalence of RM and investigate the association between RM and adverse maternal outcomes in subsequent pregnancies in pregnant women who have had a gravidity of two or more in the UAE.
Participants and Methods
Study Design, Setting, and Participants
Pregnant women who participated in the Mutaba’ah Mother and Child Health Study were included in this analysis. The Mutaba’ah (Arabic for “to follow up”) Study is a prospective cohort study that aimed to systematically recruit 10,000 pregnant women from the Emirati population during their antenatal care visits at three major health institutions in Al Ain, UAE. All pregnant women, and their newborns, from the Emirati population who were aged 18 years and above, resident in Al Ain, and able to provide informed consent were eligible for the study. Recruitment involved completing a baseline survey. Participants were followed up during pregnancy via medical records and other questionnaires. Mothers and their offspring will be subsequently followed up using questionnaires, medical record extractions, and interviews until the child turns 16 years old. More information about the Mutaba’ah Study can be found elsewhere.21,22
Variables and Measurements
Data for the current analysis were extracted from the baseline survey administered during the first point of contact with participants who were recruited between May 2017 and April 2019 and from their medical records. The survey included 67 questions regarding demographics, psychosocial factors, previous pregnancies, and lifestyle behaviors during the current pregnancy. The dataset from the medical records included information about previous pregnancy history and current pregnancy (from the first hospital visit until delivery and postnatal discharge).
A miscarriage was defined as all pregnancy losses from the time of conception (fertilized ovum) to neonate in this study.3 Only data from the medical records on previous pregnancy history were used to confirm the history of miscarriage and form exposure groups. As per inclusion criteria, in this analysis, only women with two or more previous consecutive miscarriages were included in the RM group, while women with a gravidity of two or more and no history of two consecutive losses were included in the comparison group. This definition of quantifying RM (using two or more losses) is as per the European Society of Human Reproduction and Embryology guidelines, the American Society of Reproductive Medicine as well as the American College of Obstetricians and Gynecologists and the Dutch Society of Obstetrics and Gynecology although they have varying definitions of what constitutes a miscarriage.3–6 Other institutions define RM with a diagnostic definition of three or more consecutive losses.7 This definition was used in a supplementary analysis.
Medical records were also used to obtain information about the current pregnancy and delivery. This included information on maternal anthropometry, pregnancy outcomes (eg, diagnoses of GDM and preeclampsia), mode of delivery, and gestational age at delivery. Options for mode of delivery included spontaneous vaginal delivery, assisted vaginal delivery (including the use of vacuum and forceps), and cesarean section. We also extracted data on blood loss during delivery. We were unable to elucidate if the current pregnancy was achieved via assisted conception (eg, via ovulation induction, intrauterine insemination, or any type of in vitro fertilization) as this information was confidential. Information on maternal age, gestational age at booking, body mass at first visit, and blood pressure at first visit were also collected from medical records.
Demographic and other pregnancy-related characteristics obtained from the questionnaire included maternal education, employment, number of people living in the house, number of previous pregnancies (gravidity), number of children (parity), ever been treated for infertility, pregnancy planning status, maternal and paternal smoking status, consanguinity, perceived social support, and childbirth anxiety.
Assuming an exposure level of 10% (a history RM) and an outcome of 30% (for instance, cesarean section) in the unexposed group, a cohort of 1700 pregnant women will allow the detection of as low as 1.6-fold increase in odds of the outcome in the exposed group compared to the unexposed group with 80% power and a 5% Type I error probability.
Statistical Analyses
Descriptive statistics were performed to compare the distribution of characteristics of the study population by RM status. Continuous variables were presented as means and standard deviations, while categorical variables were presented as counts and percentages. Student’s t-tests were used to determine differences between group means for continuous variables, while Pearson Chi-square tests were used for categorical variables. Univariate and multivariate regression models were used to quantify the association between exposure to history of RM (coded as yes/no) and current pregnancy maternal outcomes (cesarean section or preterm or very preterm delivery, preeclampsia and GDM) [all coded as yes/no], and blood loss during delivery (coded as a continuous variable). Factors associated with a history of RM in the crude model and other relevant factors were added to the multivariate model. All models were adjusted for age, gravidity, body weight and gestational age at delivery unless stated otherwise. Crude odds ratio (OR) and adjusted odds ratios (aOR) with 95% confidence intervals (CI) were reported. Stata 16 (Stata Corp, College Station, TX) was used to perform statistical analyses. Statistical significance was defined by a p-value less than or equal to 0.05.
Results
Between May 2017 and April 2019, 2769 women consented and participated in the Mutaba’ah Study and completed their pregnancies at the time of this analysis. Of these 2769 women, 542 (19.6%) were primiparous (did not have a history of pregnancies) and 490 (17.7%) had only one previous pregnancy (gravida = 1). The remaining 1737 women had a gravidity of two or more prior to the current pregnancy and were included in this analysis.
Prevalence of RM and Characteristics of the Study Population
Approximately 13.5% (N = 234) of these women had a history of two or more consecutive miscarriages. They formed the RM group. Table 1 shows the characteristics of women in the RM and non-RM groups. In brief, women with history of RM were slightly older, more gravid, and more likely to have had prior infertility treatment (all p-values <0.05). The mean (±SD) age of women with a history of RM was 33.7 ± 5.6 years, while that of women without a history of RM was 32.6 ± 5.2 years. In general, women with a history of RM had on average two more pregnancies than those without a history of RM (mean ± SD gravidity of 6.2 ± 2.6 versus 4.0 ± 2.0, respectively). However, there was no difference in the number of children (parity) the two groups were having at this index pregnancy (3.3 ± 0.1 versus 3.4 ± 0.05). More than one-fifth (22.1%) of women with RM had self-reported that they had previously undergone infertility treatment during their reproductive career prior to this pregnancy, compared to 8.1% of those without a history of RM. There were no significant differences in the planning status of the current pregnancy, education, or consanguinity between the two groups.
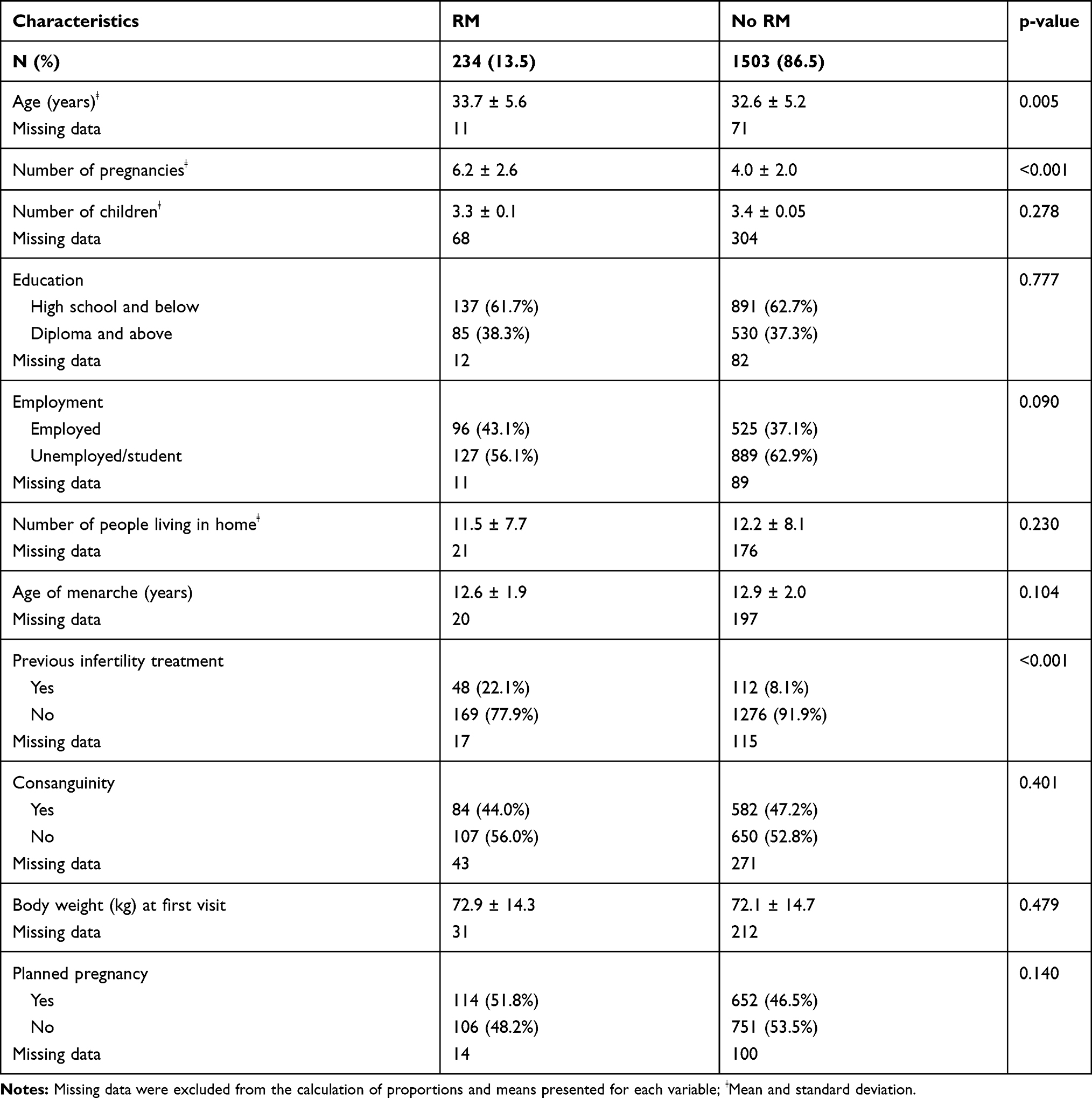 |
Table 1 Characteristics of 1737 Pregnant Women with Gravidity of two or More Prior to the Current Pregnancy According to Their History of Recurrent Miscarriage (RM) Status (Has a History of Two or More Consecutive Miscarriages) in Al Ain, UAE: The Mutaba’ah Study |
History of RM and Adverse Outcomes in the Current Pregnancy
Figure 1 shows adverse outcomes in the current pregnancy by RM status. Women with a history of RM were significantly more likely to deliver via cesarean section (34.2% versus 21.1%, p <0.001) or preterm (<37 weeks’ gestation, 16.2% versus 7.5%, p < 0.001) or very preterm (<32 weeks of gestation, 4.6% versus 0.6%, p < 0.001) and to experience preeclampsia (3.2% versus 1.2%, p = 0.021) than women with no history of RM (Figure 1). The two groups showed no significant difference for GDM in the current pregnancy (24.2% versus 26.1%, p = 0.557). The mean (± SD) blood loss during delivery was 446 ± 306 mL for women with a history of RM and 355 ± 276 mL in women with no history of RM (p <0.05).
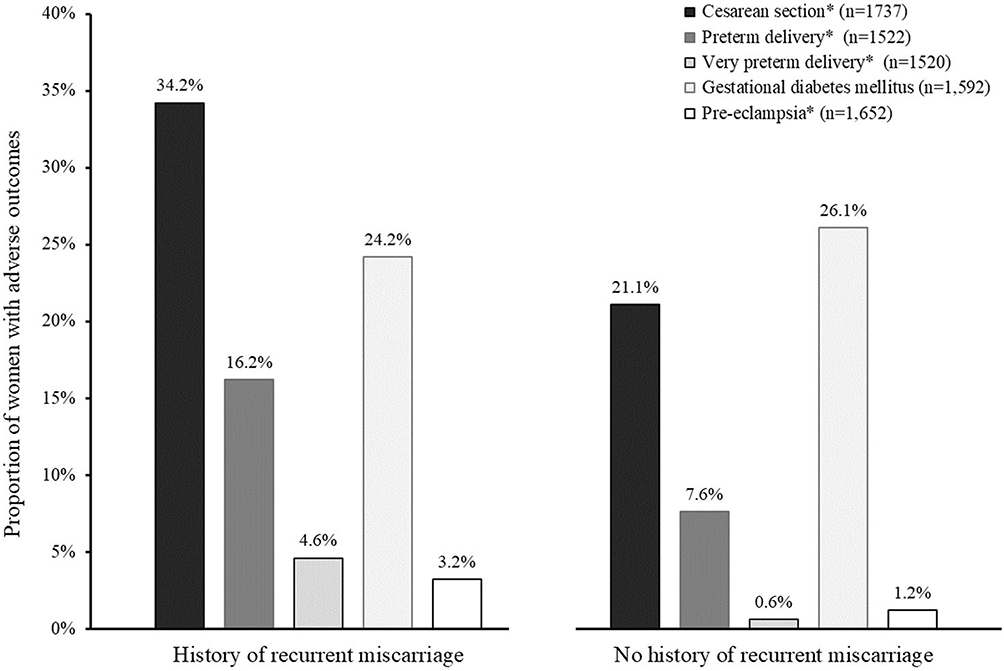 |
Figure 1 Adverse pregnancy outcomes in 1737 pregnant women with gravidity of two or more prior to the current pregnancy by history of recurrent miscarriage (RM) status (history of RM: n = 234, no history of RM: n = 1503) in Al Ain, UAE: The Mutaba’ah Study. Notes: *Adverse outcomes were significantly different between RM and no-RM groups (p <0.05). |
Table 2 shows crude and adjusted associations between RM and maternal outcomes in the current pregnancy. In the crude model, a history of RM was associated with increased odds of cesarean section (OR 1.87, 95% CI 1.39–2.51), preterm (OR 2.39, 95% CI 1.55–3.67) and very preterm delivery (OR 7.92, 95% CI 3.02–20.77), increased blood loss during delivery (OR 1.36, 95% CI 1.13–1.63), and preeclampsia (OR 2.74, 95% CI 1.12–6.67). Some of the associations remained statistically significant after controlling for potential confounding factors, including age, gravidity, body mass, gestational age at delivery. Women with a history of RM had independent associations with cesarean section (aOR 1.81, 95% CI 1.24–2.65), preterm delivery (aOR 2.52, 95% CI 1.56–4.08), and very preterm delivery (aOR 7.02, 95% CI 2.41–20.46) (Table 2).
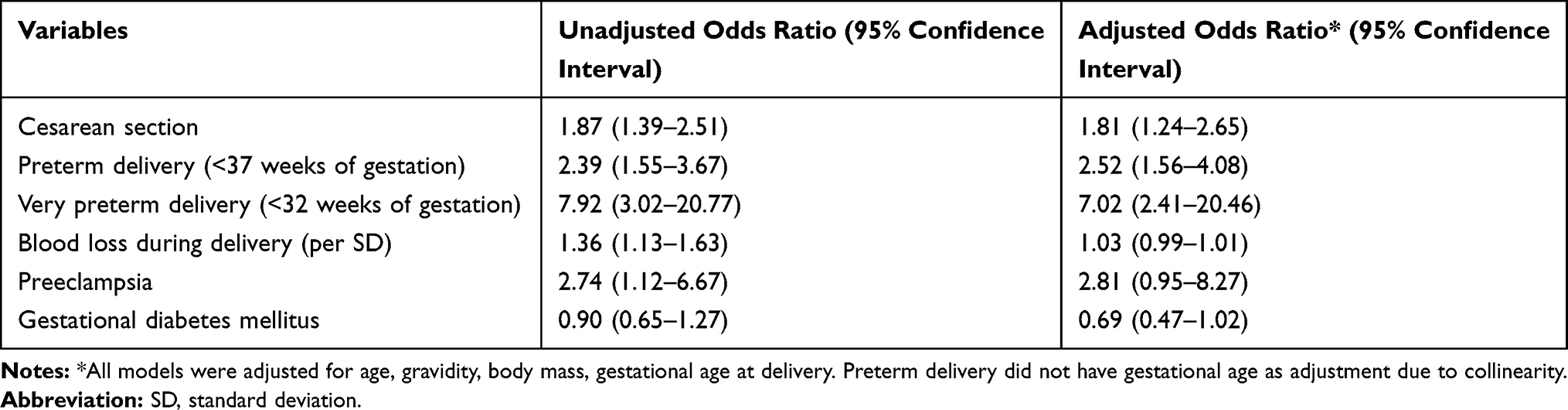 |
Table 2 Crude and Adjusted Associations Between History of Recurrent Miscarriage and Maternal Outcomes in Current Pregnancy Among 1737 Pregnant Women with Gravidity of two or More Prior to the Current Pregnancy in Al Ain, UAE: The Mutaba’ah Study |
Supplementary Analysis
In a supplementary analysis, calculations were repeated with RM defined as three or more consecutive losses (data not shown). Accordingly, 76 (5.8%) women were identified as having a history of RM amongst 1316 pregnant women with gravidity of three or more prior to the current pregnancy. Overall, women with a history of three or more consecutive miscarriages had similar risks for cesarean section, preterm delivery, and very preterm delivery to women identified using the diagnostic definition of RM as two or more consecutive losses.
Discussion
This prospective cohort study provides the first population-based estimates on the prevalence of RM and the maternal obstetric outcomes associated with RM among pregnant women in the UAE and the surrounding region. Approximately 13.5% of the pregnant women with gravidity of two or more prior to the current pregnancy in this study population had a history of RM. Moreover, women with a history of RM were twice as likely to undergo cesarean section and deliver prematurely and seven times more likely to deliver before 32 weeks of gestation than women without a history of RM.
Using the definition of quantifying RM as two or more consecutive pregnancy losses, our study showed that one in eight women with a gravidity of two or more who were pregnant again during the study period had a history of RM. The relatively high prevalence of RM in this population is 2–13 times more common than in other parts of the world (~1–5%)8 and reflects that RM is an important public health and clinical issue in the UAE. However, caution must be made when comparing prevalence estimates of RM between studies due to the use of different definitions, i.e., two versus three miscarriages as the cutoff for RM. Moreover, whether a consecutive or non-consecutive loss pertains to RM also differs between studies.23 The denominator used to calculate RM also varies in many studies and includes either women at risk of having a history of RM (by having had two or more pregnancies), all women in their reproductive years, or women intending to conceive.24 Accurate estimates of these denominators are also difficult to obtain in many countries. While our population comprised pregnant women with gravidity of two or more prior to the current pregnancy, other similar studies tend to exclusively include women with a history of RM or women at the end of their reproductive career.17,24 Nevertheless, it was envisioned that defining RM as two or more miscarriages would facilitate research and shared decision-making and enhance the psychological support available to couples.10 Finally, testing for antiphospholipid syndrome (APS), a treatable autoimmune disorder and a common cause of RM, can be performed after two losses.3 Hence, our study used two or more consecutive losses as the primary definition of RM for this population of pregnant women.
The study findings showed that a history of RM in currently pregnant women was associated with a greater likelihood of cesarean section, preterm delivery, and very preterm delivery. Similar associations were found using different RM definitions.17,25–27 Caregiver bias, where cesarean section is chosen as a simple mode of delivery in high-risk pregnancies, has been postulated to explain the increased likelihood of cesarean section in women with a history of RM.25,28 On the other hand, it has been suggested that both pregnancy loss and preterm delivery may be due to genital infections.29 Other factors such as uterine malformations or endocrine issues such as polycystic ovarian syndrome (PCOS) can also be related to RM as well as poor pregnancy outcomes. Uterine abnormalities have been linked to RM as well as preterm labor and birth and abnormal fetal presentations.30–32 Similarly, endocrine disorders such as PCOS, diabetes and hypothyroidism can be associated with miscarriage as well as poor pregnancy outcomes such as cesarean sections and inductions.33 Unfortunately, due to the lack of availability of data on these factors, we were not able to investigate their effect on the association between RM and the adverse maternal outcomes.
The crude association between history of RM and increased blood loss during delivery was an interesting finding in this study. However, this association seemingly attenuated and did not reach statistical significance in the multivariate model following the addition of cesarean section. Previous research has reported that placental management is usually manual during cesarean section and that spontaneous expulsion of the placenta is known to result in less blood loss compared to manual removal.34 Increased blood loss can be related to cesarean section, but it may also be related to placental and cervical insufficiency and management, as well as trauma and uterine atony,35 which can occur as a result of multiple miscarriages.36 Fortunately, in the case of cervical insufficiency, which might be the primary cause of RM,37 cervical cerclage can be performed to limit the occurrence of RM. Cervical cerclage can also assist in reducing other future negative outcomes, such as placental abruption and preterm labor,38 which was independently associated with a history of RM in this population.
This study highlights the increased risk of adverse maternal outcomes that may occur in women who have had two or more consecutive miscarriages in the form of missed miscarriages, ectopic, molar, or therapeutic abortions. Pre-pregnancy planning in women with a history of RM should include optimizing preconception health. Also, at-risk women with a history of RM should meet with care providers early during pregnancy or even prior to conception to discuss potential risks (eg, fetal growth reduction, placental dysfunction, and spontaneous preterm labor) and the need for increased maternal and fetal monitoring. Managing early pregnancy problems led to the development of early pregnancy monitoring units around the world.39 The implementation of such units has reduced admission times and costs associated with loss.40 The early pregnancy monitoring units can also alert physicians and other healthcare professionals to a history of RM; this can ensure better follow-up and customized care. Health policy makers and hospital management may want to consider introducing and monitoring such services.
As medical records were the basis of this analysis, it is assumed that the pregnancies, their dating, and outcomes were accurate. The relatively large sample size and detailed dataset permitted robust analyses of less common but important outcomes, such as preterm and very preterm delivery. Furthermore, since the sites of recruitment of the study population were the three major health institutions in Al Ain, the Mutaba’ah Study was an apt population to study the impact of RM. This provided a representative pregnant population and hence reduced the chances of selection bias. We were unable to categorize the RM of each participant according to the etiology of the losses as this data was unavailable. Future studies should consider exploring whether the outcomes differed according to the etiology of RM. A common outcome of having a history of RM is the advent of future pregnancy loss in the form of miscarriages and stillbirth.15,41 However, a complete register of miscarriages cannot be captured by the data from this interim analysis. Hence, it was deemed inappropriate to investigate the association of loss after a history of RM. Furthermore, there may have been residual confounding for factors we could not control for such as the use of artificial reproductive technology in the current pregnancy. Future studies can endeavor to understand the impact of such factors.
Conclusion
To the best of our knowledge, this study is the first and largest population-based cohort study to report the prevalence of RM and future maternal outcomes associated with a history of RM in pregnant women in the region. One in eight mothers in our population of pregnant women with gravidity of two or more prior to the current pregnancy had a history of RM. This was independently associated with several serious subsequent maternal complications, such as cesarean section, preterm delivery, and very preterm delivery. The study findings support the need for early pregnancy monitoring or assessment units to ensure better follow-up and customized care for at-risk pregnant women with a history of RM.
Abbreviations
aOR, adjusted odds ratio; APS, anti-phospholipid syndrome; CI, confidence interval; CS, cesarean section; ESHRE, European Society of Human Reproduction and Embryology; GDM, gestational diabetes mellitus; OR, odds ratio; PCOS, polycystic ovarian syndrome; RM, recurrent miscarriage; SD, standard deviation; UAE, United Arab Emirates.
Data Sharing Statement
Data can be made available on reasonable request from the Mutaba’ah Study.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committees of the United Arab Emirates University (ERH-2017-5512), Al Ain Hospital (AAHEC-03-17-058), and Tawam Hospital (IRR–494), and was in complete agreement with the Declaration of Helsinki. All participants provided written informed consent.
Acknowledgments
The authors would like to thank all women who generously agreed to participate in the Mutaba’ah study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by a grant from the Zayed Center for Health Sciences, United Arab Emirates University (31R076).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Macklon NS, Geraedts JP, Fauser BC. Conception to ongoing pregnancy: the ‘black box’ of early pregnancy loss. Hum Reprod Update. 2002;8(4):333–343. doi:10.1093/humupd/8.4.333
2. Stirrat GM. Recurrent miscarriage. Lancet. 1990;336(8716):673–675. doi:10.1016/0140-6736(90)92159-F
3. American College of Obstetricians and Gynecologists. Management of recurrent pregnancy loss. Number 24, February 2001. (Replaces Technical Bulletin Number 212, September 1995). Int J Gynaecol Obstet. 2002;78(2):179–190.
4. ESHRE Guideline Group on RPL; Bender Atik R, Christiansen OB, et al. ESHRE guideline: recurrent pregnancy loss. Hum Reprod Open. 2018;2018(2):hoy004.
5. Practice Committee of the American Society for Reproductive Medicine. Aging and infertility in women: a committee opinion. Fertil Steril. 2002;78(1):215–219. doi:10.1016/S0015-0282(02)03212-0
6. van den Boogaard E, Kaandorp SP, Franssen MT, et al. Consecutive or non-consecutive recurrent miscarriage: is there any difference in carrier status? Hum Reprod. 2010;25(6):1411–1414. doi:10.1093/humrep/deq089
7. Rai R, Regan L. Recurrent miscarriage. Lancet. 2006;368(9535):601–611. doi:10.1016/S0140-6736(06)69204-0
8. Egerup P, Kolte AM, Larsen EC, Krog M, Nielsen HS, Christiansen OB. Recurrent pregnancy loss: what is the impact of consecutive versus non-consecutive losses? Hum Reprod. 2016;31(11):2428–2434. doi:10.1093/humrep/dew169
9. DeBackere KJ, Hill PD, Kavanaugh KL. The parental experience of pregnancy after perinatal loss. J Obstet Gynecol Neonatal Nurs. 2008;37(5):525–537.
10. Kolte AM, Olsen LR, Mikkelsen EM, Christiansen OB, Nielsen HS. Depression and emotional stress is highly prevalent among women with recurrent pregnancy loss. Hum Reprod. 2015;30(4):777–782. doi:10.1093/humrep/dev014
11. McCarthy FP, Moss-Morris R, Khashan AS, et al. Previous pregnancy loss has an adverse impact on distress and behaviour in subsequent pregnancy. BJOG. 2015;122(13):1757–1764. doi:10.1111/1471-0528.13233
12. Shapira E, Ratzon R, Shoham-Vardi I, Serjienko R, Mazor M, Bashiri A. Primary vs. secondary recurrent pregnancy loss–epidemiological characteristics, etiology, and next pregnancy outcome. J Perinat Med. 2012;40(4):389–396. doi:10.1515/jpm-2011-0315
13. Armstrong DS. Impact of prior perinatal loss on subsequent pregnancies. J Obstet Gynecol Neonatal Nurs. 2004;33(6):765–773. doi:10.1177/0884217504270714
14. Edlow AG, Srinivas SK, Elovitz MA. Second-trimester loss and subsequent pregnancy outcomes: what is the real risk? Am J Obstet Gynecol. 2007;197(6):581e581–586. doi:10.1016/j.ajog.2007.09.016
15. McQueen DB, Perfetto CO, Hazard FK, Lathi RB. Pregnancy outcomes in women with chronic endometritis and recurrent pregnancy loss. Fertil Steril. 2015;104(4):927–931. doi:10.1016/j.fertnstert.2015.06.044
16. Rushworth FH, Backos M, Rai R, Chilcott IT, Baxter N, Regan L. Prospective pregnancy outcome in untreated recurrent miscarriers with thyroid autoantibodies. Hum Reprod. 2000;15(7):1637–1639. doi:10.1093/humrep/15.7.1637
17. Jivraj S, Anstie B, Cheong YC, Fairlie FM, Laird SM, Li TC. Obstetric and neonatal outcome in women with a history of recurrent miscarriage: a cohort study. Hum Reprod. 2001;16(1):102–106.
18. Kolte AM, Bernardi LA, Christiansen OB, et al. Terminology for pregnancy loss prior to viability: a consensus statement from the ESHRE early pregnancy special interest group. Hum Reprod. 2015;30(3):495–498. doi:10.1093/humrep/deu299
19. Gowri V, Udayakumar AM, Bsiso W, Al Farsi Y, Rao K. Recurrent early pregnancy loss and consanguinity in Omani couples. Acta Obstet Gynecol Scand. 2011;90(10):1167–1169. doi:10.1111/j.1600-0412.2011.01200.x
20. Saad FA, Jauniaux E. Recurrent early pregnancy loss and consanguinity. Reprod Biomed Online. 2002;5(2):167–170. doi:10.1016/S1472-6483(10)61620-3
21. Al Haddad A, Ali N, Elbarazi I, et al. Mutaba’ah-Mother and Child Health Study: protocol for a prospective cohort study investigating the maternal and early life determinants of infant, child, adolescent and maternal health in the United Arab Emirates. BMJ Open. 2019;9(8):e030937. doi:10.1136/bmjopen-2019-030937
22. Ali N, Elbarazi I, Alabboud S, Al-Maskari F, Loney T, Ahmed LA. Antenatal care initiation among pregnant women in the United Arab Emirates: the Mutaba’ah study. Front Public Health. 2020;8:211. doi:10.3389/fpubh.2020.00211
23. Silver RM, Branch DW, Goldenberg R, Iams JD, Klebanoff MA. Nomenclature for pregnancy outcomes: time for a change. Obstet Gynecol. 2011;118(6):1402–1408. doi:10.1097/AOG.0b013e3182392977
24. Bashiri A, Ratzon R, Amar S, Serjienko R, Mazor M, Shoham-Vardi I. Two vs. three or more primary recurrent pregnancy losses–are there any differences in epidemiologic characteristics and index pregnancy outcome? J Perinat Med. 2012;40(4):365–371. doi:10.1515/jpm-2011-0295
25. Sheiner E, Levy A, Katz M, Mazor M. Pregnancy outcome following recurrent spontaneous abortions. Eur J Obstet Gynecol Reprod Biol. 2005;118(1):61–65.
26. Field K, Murphy DJ. Perinatal outcomes in a subsequent pregnancy among women who have experienced recurrent miscarriage: a retrospective cohort study. Hum Reprod. 2015;30(5):1239–1245. doi:10.1093/humrep/dev044
27. Sugiura-Ogasawara M, Ebara T, Yamada Y, et al. Adverse pregnancy and perinatal outcome in patients with recurrent pregnancy loss: multiple imputation analyses with propensity score adjustment applied to a large-scale birth cohort of the Japan Environment and Children’s Study. Am J Reprod Immunol. 2019;81(1):e13072.
28. Sheiner E, Shoham-Vardi I, Hershkovitz R, Katz M, Mazor M. Infertility treatment is an independent risk factor for cesarean section among nulliparous women aged 40 and above. Am J Obstet Gynecol. 2001;185(4):888–892. doi:10.1067/mob.2001.117308
29. Buchmayer SM, Sparen P, Cnattingius S. Previous pregnancy loss: risks related to severity of preterm delivery. Am J Obstet Gynecol. 2004;191(4):1225–1231. doi:10.1016/j.ajog.2004.02.066
30. Dhont M. Recurrent miscarriage. Curr Womens Health Rep. 2003;3(5):361–366.
31. Mannisto T, Mendola P, Grewal J, Xie Y, Chen Z, Laughon SK. Thyroid diseases and adverse pregnancy outcomes in a contemporary US cohort. J Clin Endocrinol Metab. 2013;98(7):2725–2733. doi:10.1210/jc.2012-4233
32. Homburg R. Pregnancy complications in PCOS. Best Pract Res Clin Endocrinol Metab. 2006;20(2):281–292. doi:10.1016/j.beem.2006.03.009
33. Cocksedge KA, Li TC, Saravelos SH, Metwally M. A reappraisal of the role of polycystic ovary syndrome in recurrent miscarriage. Reprod Biomed Online. 2008;17(1):151–160. doi:10.1016/S1472-6483(10)60304-5
34. McCurdy CM, Magann EF, McCurdy CJ, Saltzman AK. The effect of placental management at cesarean delivery on operative blood loss. Am J Obstet Gynecol. 1992;167(5):1363–1367. doi:10.1016/S0002-9378(11)91717-7
35. Weeks A. The prevention and treatment of postpartum haemorrhage: what do we know, and where do we go to next? BJOG. 2015;122(2):202–210.
36. Gunnarsdottir J, Stephansson O, Cnattingius S, Akerud H, Wikstrom AK. Risk of placental dysfunction disorders after prior miscarriages: a population-based study. Am J Obstet Gynecol. 2014;211(1):34e31–38. doi:10.1016/j.ajog.2014.01.041
37. Sneider K, Christiansen OB, Sundtoft IB, Langhoff-Roos J. Recurrence of second trimester miscarriage and extreme preterm delivery at 16–27 weeks of gestation with a focus on cervical insufficiency and prophylactic cerclage. Acta Obstet Gynecol Scand. 2016;95(12):1383–1390. doi:10.1111/aogs.13027
38. Drakeley AJ, Roberts D, Alfirevic Z. Cervical stitch (cerclage) for preventing pregnancy loss in women. Cochrane Database Syst Rev. 2003;(1):CD003253.
39. Edey K, Draycott T, Akande V. Early pregnancy assessment units. Clin Obstet Gynecol. 2007;50(1):146–153. doi:10.1097/GRF.0b013e3180305ef4
40. Bigrigg MA, Read MD. Management of women referred to early pregnancy assessment unit: care and cost effectiveness. BMJ. 1991;302(6776):577–579. doi:10.1136/bmj.302.6776.577
41. Ford HB, Schust DJ. Recurrent pregnancy loss: etiology, diagnosis, and therapy. Rev Obstet Gynecol. 2009;2(2):76–83.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.