Back to Journals » Orthopedic Research and Reviews » Volume 17
Impact of Preoperative and Residual Alpha Angle on Outcomes After Hip Arthroscopy
Authors Puria J ![]() , Puczko D
, Puczko D ![]() , Frey CS, Rogers JL, Hymel AM, Mathews III CG
, Frey CS, Rogers JL, Hymel AM, Mathews III CG ![]() , Spears TM, Sullivan JP
, Spears TM, Sullivan JP
Received 22 May 2025
Accepted for publication 22 October 2025
Published 11 November 2025 Volume 2025:17 Pages 531—538
DOI https://doi.org/10.2147/ORR.S542143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Clark Hung
Jasmine Puria,1,* Daniel Puczko,2,* Christopher S Frey,3,4 James L Rogers,2 Alicia M Hymel,5 Candler G Mathews III,3,6 Thomas M Spears,7 Jaron Paul Sullivan3
1College of Medicine, University of Tennessee Health Science Center, Memphis, TN, USA; 2School of Medicine, Vanderbilt University, Nashville, TN, USA; 3Department of Orthopaedic Surgery, Vanderbilt University Medical Center, Nashville, TN, USA; 4Department of Orthopaedic Surgery, University of Texas Health Science Center at Houston, Houston, TX, USA; 5Center for Musculoskeletal Research, Vanderbilt University Medical Center, Nashville, TN, USA; 6Medical University of South Carolina Health Orthopaedics, Medical University of South Carolina, Columbia, SC, USA; 7Department of Orthopaedic Surgery, Naval Medical Center Portsmouth, Falls Church, VA, USA
*These authors contributed equally to this work
Correspondence: Christopher S Frey, Department of Orthopaedic Surgery, Vanderbilt University Medical Center, 1215 21 st Ave S, Suite 4200, Nashville, TN, 37232, USA, Tel +1 615 322 5000, Email [email protected]
Purpose: Femoroacetabular impingement syndrome (FAIS) can lead to pain, decreased mobility, and difficulty in performing activities of daily living. Symptoms can improve with surgery, often hip arthroscopy with osteoplasty. Radiological parameters such as the alpha angle can be utilized to determine the degree of cam morphology and assess resection after surgery. This study sought to evaluate the relationship between pre-operative alpha angle and the change in alpha angle on patient satisfaction post-surgical correction using the 12-item International Hip Outcome Tool (iHOT-12).
Patients and Methods: Patients that underwent primary or revision hip arthroscopy with osteoplasty for FAIS by a single fellowship-trained surgeon at a tertiary academic center from September 1, 2014 to April 1, 2024 were eligible for this retrospective cohort study. Data collected included type of operation, preoperative and postoperative alpha angle, 6-month iHOT-12 scores, and demographic data. Multivariate proportional odds regression analyses were conducted to assess whether preoperative alpha angle and the change in alpha angle from pre- to post-operative were predictive of 6-month iHOT-12 scores. Additionally, Pearson correlation coefficients were reported for 6-month iHOT-12 association with preoperative alpha angle and alpha angle delta.
Results: 507 patients and 541 operative hips were identified during the study period. 99 (18%) hips were included in the final analysis. Mean alpha angle was 60.9 (SD = 9.8) preoperatively and 44.4 (SD = 6.1) postoperatively with a mean absolute change of 16.5 (SD = 8.6). The mean 6-month iHOT-12 score was 62.0 (SD = 26.9). Multivariate proportional odds regression analyses did not reveal significant predictors of 6-month iHOT-12 scores including preoperative alpha angle and alpha angle change.
Conclusion: This study found no association between preoperative alpha angle or postoperative change in alpha angle and 6-month iHOT-12 scores. Future research on other factors such as three-dimensional morphology may be warranted.
Keywords: femoroacetabular impingement syndrome, radiographic measurements, international hip outcome tool, arthroscopic surgery
Introduction
Femoroacetabular impingement syndrome (FAIS) is a hip disorder due to abnormal contact between the proximal femur and the acetabulum. Ganz et al first described this disorder in 2003 and characteristic symptoms include anterior hip and groin pain and restricted range of motion (ROM).1 This disorder commonly affects young, active adults and has become an increasingly prevalent source of hip pain over the years.2 Notzli et al initially developed the alpha angle to represent the structural abnormality characteristic of FAIS in 2002, and this radiographic measurement has been widely used as an objective diagnostic indicator since.3 The use of subjective tools or patient-reported outcome measures (PROMs) is also common and allows physicians to evaluate how their patients’ abnormal hip morphology limits them functionally. The 12-item International Hip Outcome Tool (iHOT-12) is one such tool. It is a shorter version of its predecessor, the iHOT-33, and shares at least 96% of the variability with it.4 Griffin et al developed it so clinicians could measure changes in quality of life and function following treatment with greater ease and efficiency.4
A plethora of research has been done to identify preoperative variables that constitute clinically meaningful outcomes, and the associations between these variables and postoperative outcome measures have been examined as well. Greater age at the time of surgery, elevated body mass index (BMI), positive history of tobacco use, and past medical history significant for mental health disease have all been found to significantly impact postoperative PROMs.5–20 The association between the alpha angle and PROMs has been mixed. Some investigators found that larger preoperative alpha angles were associated with lower scores on postoperative PROMs, but some did not find any significant relationship at all.6,7,9,10,14,21–26 This could be because the alpha angle, which is typically measured from plain radiographs, is not a sufficient predictor of postoperative outcomes given that FAIS is a structurally complex disorder that requires three-dimensional (3-D) imaging, such as reconstructed computer tomography (CT), to give clinicians the full picture of their patients’ pathology.27 It is worth noting that Beck et al did find that patients with larger preoperative alpha angles achieved superior clinical satisfaction compared to those with smaller values.17 Investigators, however, discovered this finding in the context of visual analog scale (VAS) satisfaction scores only, and they ultimately concluded that the alpha angle is not a predictor of postoperative outcomes because this finding represented an outlier in the literature.17
It seems logical that patients with larger preoperative deformities and/or greater areas resected would report more positive improvements after surgery compared to those with smaller deformities. We expect patients’ postoperative iHOT-12 responses to reflect that change. We thus hypothesized that patients with larger preoperative alpha angles and those who had greater changes between preoperative and postoperative alpha angles would report more positive changes in function as measured by a greater postoperative iHOT-12 score. We hope that the results of this study will establish a clearer relationship between these two variables and ultimately allow clinicians to better predict how their patients will respond to surgery.
Materials and Methods
Patient Selection
This retrospective cohort study received approval from the institutional review board of Vanderbilt University Medical Center (VUMC), and the requirement for informed consent was waived given the retrospective nature of the study. Retrospective data on patients who underwent a primary or revision hip arthroscopy with osteoplasty from September 1, 2014 to April, 1 2024 for the treatment of FAIS by a single fellowship-trained surgeon (J.P.S.) were collected and stored in a secure web platform (Redcap, Nashville, TN). All patient data was deidentified to maintain confidentiality, and this study was performed in compliance with the “Declaration of Helsinki.” Patients were selected for this study using the following CPT codes: 29914, 29915, and 29916 (Box: Summary of Procedures Performed). If present, concurrent labral tears were managed with surgical debridement or repair. Patients were given an oral non-steroidal anti-inflammatory medication (NSAID) for 4 weeks postoperatively to minimize the development of heterotopic ossification. Patients were included in the study based on the following criteria: having received hip arthroscopy and osteochondroplasty for FAIS, received heterotopic ossification prophylaxis per protocol, had postoperative follow up of at least 6 months, and iHOT-12 completed 6 months postoperatively. Patients were excluded from this study based on the following criteria: age of 18 years or younger at the time of surgery, surgical indications for a hip arthroscopy other than FAIS, did not receive surgery by J.P.S., no preoperative radiographs, no 3 month or longer postoperative radiographs, and pre-existing heterotopic ossification.
 |
Box Summary of Procedures Performed |
Radiographic Analysis and Measurements
Patients received a set of radiographs of the symptomatic hip preoperatively upon initial clinical evaluation and postoperatively at 6 months. Each set of radiographs consisted of standing low anteroposterior pelvis, 45-degree Dunn lateral, false profile, and frog-leg lateral views. Patients also received CT scans with 3-D reconstruction for surgical planning. Preoperative alpha angles were independently measured twice during retrospective data collection using the 45-degree Dunn radiographs. The alpha angle was measured as described by Notzli.3 Measurements were performed by a musculoskeletal radiology attending, orthopaedic sports medicine fellow, or medical student. The average of the two measurements was used. In situations where alpha angle measurements differed by 7 degrees (2 SD), a third reviewer consisting of either an orthopaedic sports medicine fellow or radiology attending performed an independent measurement and the average of the two closest measurements was used.
Surgical Technique and Postoperative Rehabilitation Protocol
The surgeries were performed by the senior author (J.P.S)., a sports medicine fellowship-trained surgeon at a tertiary referral center. In short, patients underwent general anesthesia and were placed supine on a post-less traction table Anterolateral, anterior, and distal anterolateral accessory (DALA) portals were used. An interportal capsulotomy was utilized for the central compartment and a T-capsulotomy for the peripheral compartment. The capsule was repaired at the end of the case. Femoroplasty was performed for cam-type impingement, acetabuloplasty for pincer-type impingement, and either debridement, repair, or allograft reconstruction for labral pathology depending on tissue quality and patient factors.
Patients received a 4-week course of NSAIDs postoperatively for heterotopic ossification prophylaxis. Patients were typically allowed to weight bear as tolerated after surgery. Postoperative rehabilitation started 1–3 days after surgery working on passive and gentle active ROM. Patients were instructed to ambulate with crutches to minimize fall risk for 2 weeks and progressed through a five-phase rehabilitation protocol over the following 16 weeks.
Functional Outcome Evaluation
Preoperative patient demographics were collected retrospectively from electronic medical record chart review. In the present study, each patient completed the iHOT-12 preoperatively at the initial clinical evaluation and subsequently at 6 months. Scoring of the iHOT-12 was based off the methods described by Mohtadi et al and Griffin et al.4,28
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics and PROMs. Categorical variables were reported using frequencies and percentages, and continuous variables were reported using means and standard deviations.
Multivariate proportional odds regression analyses were conducted to assess whether preoperative alpha angle and the change in alpha angle from pre- to post-operative were predictive of postoperative iHOT-12 scores while controlling for BMI, autoimmune disease, diabetes, and procedure type (labral repair, arthroscopic psoas tenotomy or labral reconstruction with semi-T, and/or other surgery). Model covariates were selected a priori. The unadjusted Pearson’s correlation between alpha angle and iHOT-12 scores were also reported. All analyses were run in R version 4.2.
Results
In total, 507 patients and 541 operative hips were identified. After exclusion criteria were applied, there were 323 (59%) hips eligible for analysis. 99 (18%) completed the postoperative iHOT-12 assessments and are included in this analysis (Figure 1).
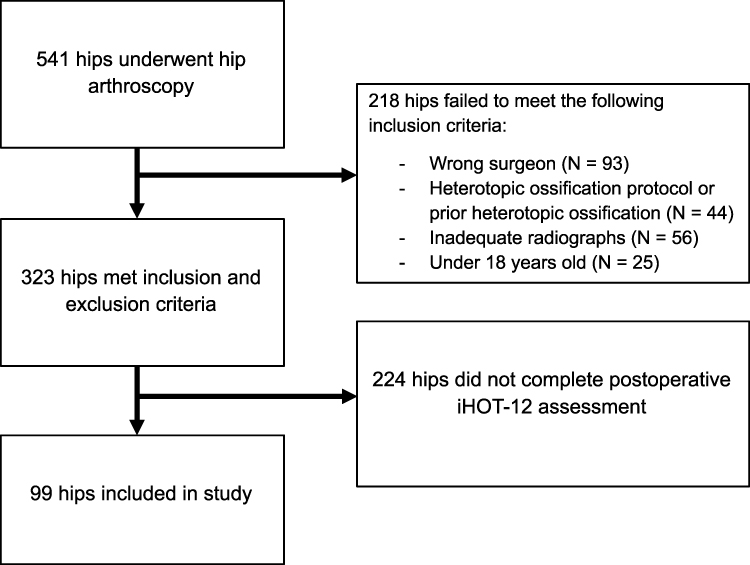 |
Figure 1 Patient Selection. |
The mean age was 33.0 years (SD = 9.3) and the mean BMI was 27.7 (SD = 4.2). 47.5% of patients were male. 4.04% of the sample had diabetes and 6.06% had an autoimmune disease. 43.4% of surgeries were performed on the left side, 40.4% on the right, and 16.2% were bilateral (Table 1).
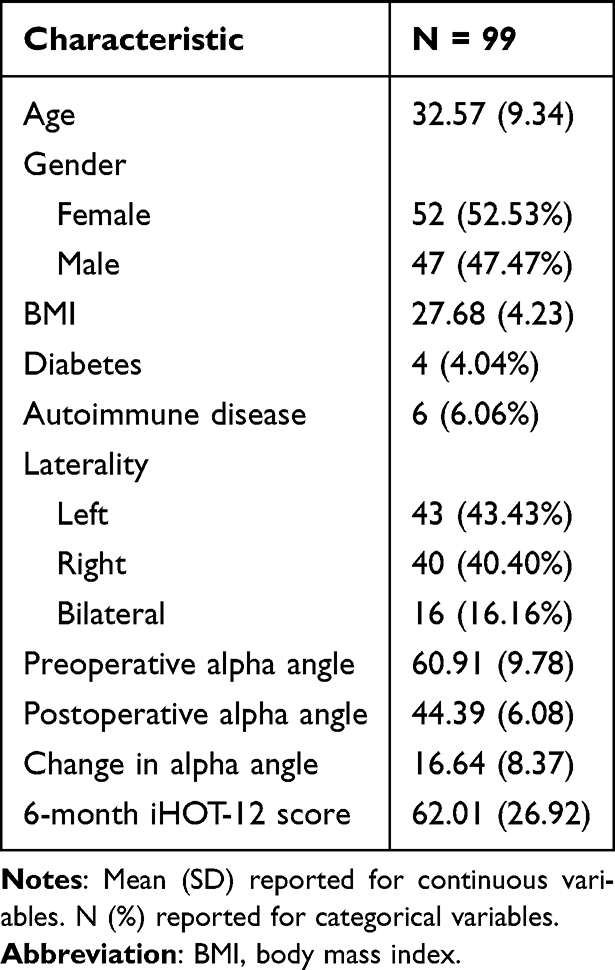 |
Table 1 Patient Characteristics |
All cases underwent hip arthroscopy with femoral osteoplasty while labral repair was performed in 83 (84%) hips, and arthroscopic psoas tenotomy or labral reconstruction with semi-T was performed in 10 (10.1%) hips (Box: Summary of Procedures Performed). Procedures other than labral repair or reconstruction (eg, acetabular osteoplasty, microfracture, loose body removal, core decompression of femoral head, debridement of the ligamentum teres) were performed in 17 (17.2%) hips (Box: Summary of Procedures Performed).
Radiographic measurements of the alpha angle demonstrated high inter-rater reliability. Intraclass correlation coefficients (ICCs) using a two-way model for agreement yielded an ICC of 0.966 for the first two raters, with a 95% confidence interval from 0.955 to 0.975. The ICCs for the final two ratings utilized in computing the analytic value was 0.983, with a 95% confidence interval from 0.977 to 0.987. The mean alpha angle was 60.9 (SD = 9.8) preoperatively and 44.4 (SD = 6.1) postoperatively. The mean of the absolute value of the difference between preoperative and postoperative alpha angle was 16.5 (SD = 8.6) (Table 1).
The mean 6-month iHOT-12 score was 62.0 (SD = 26.9) (Table 1). Multivariate proportional odds regression analyses were run to determine whether preoperative alpha angle was predictive of 6-month iHOT-12 scores when controlling for patient and surgical characteristics. Neither preoperative alpha angle nor the absolute value of change in alpha angle from pre- to post-operative were significant predictors of 6-month iHOT-12 scores when controlling for patient and surgical characteristics (Table 2). Unadjusted analyses similarly failed to demonstrate a relationship between alpha angle and postoperative iHOT-12 scores. Neither preoperative alpha angle (r = 0.05, p = 0.60) nor the absolute value of change in alpha angle (r = −0.03, p = 0.76) were significantly correlated with 6-month iHOT-12 scores.
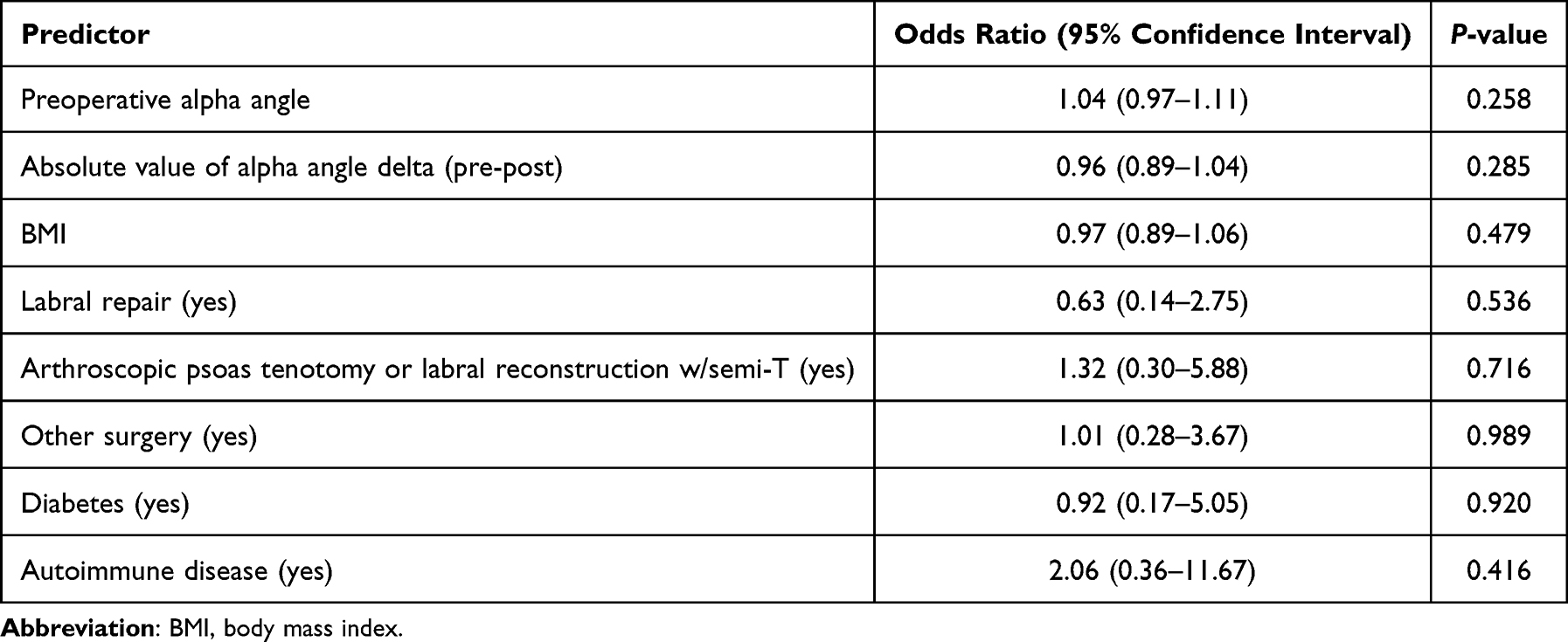 |
Table 2 Multivariate Proportional Odds Regression Model Predicting 6-Month iHOT-12 Score |
Discussion
In the present study, we sought to assess the impact of alpha angles on postoperative outcomes after hip arthroscopy for FAIS. We hypothesized that larger preoperative alpha angles and greater changes in alpha angles from pre- to post-operatively would be associated with greater iHOT-12 scores after hip arthroscopy. The mean iHOT-12 score was found to be 62.0 at 6 months after surgery. This approaches the patient acceptable symptomatic state (PASS) threshold of 63.0 and 59.5 determined in prior studies.9,29 It should be noted that researchers in both articles administered the iHOT-12 one year after the operation, allowing for an additional six months of recovery. However, we found that there was no statistically significant correlation between iHOT-12 scores and preoperative alpha angle or the change in alpha angle.
In the literature, data is mixed with regards to the impact of preoperative alpha angle and change in alpha angle with respect to outcomes. Multiple cohort and case series found no association with preoperative alpha angle and outcome scores including the iHOT-12.7,26 Postoperative alpha angle was also determined to have no significant impact on outcomes by several studies.23,25 Additionally, a retrospective study by Ellis et al determined that the total volume of a preoperative cam lesion on CT predicted worse outcomes for patients.21 On the other hand, there have been multiple reports of patients with smaller preoperative alpha angles having better postoperative outcomes.6,14,22 The cause for discrepancy in results is likely multifactorial. While this study included possible confounding factors such as concomitant procedures, they were relatively infrequent and did not significantly predict 6-month iHOT-12 scores (Table 2). BMI could additionally pose as a confounding factor in the present study, but other important determinants of outcomes such as sport participation, patient expectation, or prior history of mental health disorders could have had an impact as well. For example, prior studies found that a history of psychiatric diagnoses was a significant predictor of persistent postoperative pain after hip arthroscopy, which could have influenced outcomes in the present study.5,7,8,19 Moreover, alpha angle alone is not a complete assessment of femoroacetabular pathology as there are other factors, such as cartilage status and 3-D morphology, that can influence outcomes.27 The deformity exists in three dimensions on both the acetabular and femoral sides, and the alpha angle found on one image may not capture a lesion most pronounced in a different plane. In addition to 3-D morphology, femoral retroversion is also important in predicting postoperative outcomes. However, the association between the two is still debated as femoral retroversion has been shown to have a negative impact on postoperative outcomes.30
The findings of our study may have several clinical implications. When counseling patients on the management of femoroacetabular impingement, surgeons may consider multiple factors, not just alpha angle alone. Although cam morphology should be addressed intraoperatively when present, radiographic improvement alone may not dictate outcomes. Thus, surgeons should be thoughtful when determining the degree of femoral osteoplasty in the context of global impingement morphology.
There are some inherent limitations to this retrospective study. Only 99 of 323 (31%) eligible patients and 541 screened (18%) completed the 6-month postoperative iHOT-12 assessments and were included in the study. Such loss of follow-up allows for potential selection bias. This study did not utilize preoperative or 12-month iHOT-12 scores. Preoperative values would have been helpful in providing the total improvement in patient outcomes as prior studies have observed positive functional differences in outcome measures when comparing them pre- vs post-operatively.7,8,10,15–17,20,22,23,25 As patients have been reported to improve for up to two years after surgery, later postoperative assessments may have had different outcomes as well.31 This study focused on radiographic alpha angle as a marker for hip impingement morphology. Given the 3-D nature of femoroacetabular impingement, measurements using reconstructed CT imaging can add value.27 Additionally, the alpha angle does not factor in acetabular morphology or femoral version, which may also play a role in impingement symptoms. The patients in this study were all treated at a single institution by a single high volume, fellowship trained hip arthroscopist, so the conclusions drawn from the data may not apply to the general population as there can be intraoperative variability among surgeons. Considering that patients were collected over a period of nearly 10 years, surgical techniques may have changed as well.
Conclusion
In this study, patients were found to have postoperative iHOT-12 scores meeting or approaching PASS scores. There was no significant association between preoperative alpha angle or the change in alpha angle and iHOT-12 scores. This suggests that the alpha angle alone should not be used solely to predict surgical success when making decisions clinically. There is thus a need for further robust prospective research to elaborate upon the relationship between 3-D resection and outcomes.
Acknowledgments
We would like to thank Katherine D Van Schaik MD, PhD and Jessica R Leschied MD for their contributions in measuring alpha angles. The current affiliation for Christopher S Frey, MD is Department of Orthopaedic Surgery, University of Texas Health Science Center at Houston, Houston, TX, USA. Contact information for Christopher S Frey, MD is (713) 486-8800. The current affiliation for Candler G Mathews III, MD is Medical University of South Carolina Health Orthopaedics, Medical University of South Carolina, Columbia, SC, USA. Contact information for Candler G Mathews III is (803) 865-4500.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the Hip. Clin Orthop Relat Res. 2003;417:112–20. doi:10.1097/01.blo.0000096804.78689.c2
2. Gomez-Verdejo F, Alvarado-Solorio E, Suarez-Ahedo C. Review of femoroacetabular impingement syndrome. J Hip Preserv Surg. 2024;11(4):315–322. doi:10.1093/jhps/hnae034
3. Notzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002;84(4):556–560. doi:10.1302/0301-620x.84b4.12014
4. Griffin DR, Parsons N, Mohtadi NG, Safran MR. Multicenter Arthroscopy of the Hip Outcomes Research N. A short version of the International Hip Outcome Tool (iHOT-12) for use in routine clinical practice. Arthroscopy. 2012;28(5):611–6;quiz616–8. doi:10.1016/j.arthro.2012.02.027
5. Ernat JJ, Song DJ, Brugman SC, Shaha SH, Tokish JM, Lee GY. Mental health medication use correlates with poor outcome after femoroacetabular impingement surgery in a military population. J Bone Joint Surg Am. 2015;97(15):1272–1277. doi:10.2106/JBJS.O.00043
6. Lansdown DA, Kunze K, Ukwuani G, Waterman BR, Nho SJ. The importance of comprehensive cam correction: radiographic parameters are predictive of patient-reported outcome measures at 2 years after hip arthroscopy. Am J Sports Med. 2018;46(9):2072–2078. doi:10.1177/0363546518780311
7. Steiner Q, Watson AM, Mosiman SJ, Spiker AM. Association between symptoms of anxiety and depression, hip pathology, and patient-reported outcomes after hip arthroscopy for femoroacetabular impingement. Am J Sports Med. 2024;52(7):1728–1734. doi:10.1177/03635465241252821
8. Stone AV, Malloy P, Beck EC, et al. Predictors of persistent postoperative pain at minimum 2 years after arthroscopic treatment of femoroacetabular impingement. Am J Sports Med. 2019;47(3):552–559. doi:10.1177/0363546518817538
9. Nwachukwu BU, Chang B, Beck EC, et al. How should we define clinically significant outcome improvement on the iHOT-12? HSS J. 2019;15(2):103–108. doi:10.1007/s11420-018-9646-0
10. Nwachukwu BU, Chang B, Fields K, et al. Defining the “substantial clinical benefit” after arthroscopic treatment of femoroacetabular impingement. Am J Sports Med. 2017;45(6):1297–1303. doi:10.1177/0363546516687541
11. Martin RL, Kivlan BR, Christoforetti JJ, et al. Defining variations in outcomes of hip arthroscopy for femoroacetabular impingement using the 12-item international hip outcome tool (iHOT-12). Am J Sports Med. 2020;48(5):1175–1180. doi:10.1177/0363546520906408
12. Bodendorfer BM, DeFroda SF, Clapp IM, Newhouse A, Nwachukwu BU, Nho SJ. Defining clinically significant improvement on the patient-reported outcomes measurement information system test at 1-year follow-up for patients undergoing hip arthroscopy for the treatment of femoroacetabular impingement syndrome. Am J Sports Med. 2021;49(9):2457–2465. doi:10.1177/03635465211015687
13. Westermann RW, Lynch TS, Jones MH, et al. Predictors of hip pain and function in femoroacetabular impingement: a prospective cohort analysis. Orthop J Sports Med. 2017;5(9):2325967117726521. doi:10.1177/2325967117726521
14. Beck EC, Nwachukwu BU, Kunze KN, Chahla J, Nho SJ. how can we define clinically important improvement in pain scores after hip arthroscopy for femoroacetabular impingement syndrome? minimum 2-year follow-up study. Am J Sports Med. 2019;47(13):3133–3140. doi:10.1177/0363546519877861
15. Maimaitimin M, Yang F, Huang HJ, et al. Outcomes after hip arthroscopy for femoroacetabular impingement syndrome in chinese patients: a minimum 2-year follow-up study. Orthop J Sports Med. 2022;10(11):23259671221135218. doi:10.1177/23259671221135218
16. Maldonado DR, George T, Padmanabhan S, Curley AJ, Domb BG. Defining thresholds and predictors for achieving the patient acceptable symptom state for patient-reported outcome measures after revision hip arthroscopy. Am J Sports Med. 2023;51(14):3772–3780. doi:10.1177/03635465231209320
17. Beck EC, Nwachukwu BU, Mehta N, et al. Defining meaningful functional improvement on the visual analog scale for satisfaction at 2 years after hip arthroscopy for femoroacetabular impingement syndrome. Arthroscopy. 2020;36(3):734–742e2. doi:10.1016/j.arthro.2019.09.028
18. Jimenez AE, Lee MS, Owens JS, et al. Effect of cigarette smoking on midterm outcomes after arthroscopic surgery for femoroacetabular impingement syndrome: a propensity-matched controlled study with minimum 5-year follow-up. Orthop J Sports Med. 2022;10(5):23259671221090905. doi:10.1177/23259671221090905
19. Sogbein OA, Shah A, Kay J, et al. Predictors of outcomes after hip arthroscopic surgery for femoroacetabular impingement: a systematic review. Orthop J Sports Med. 2019;7(6):2325967119848982. doi:10.1177/2325967119848982
20. Cvetanovich GL, Weber AE, Kuhns BD, et al. Clinically meaningful improvements after hip arthroscopy for femoroacetabular impingement in adolescent and young adult patients regardless of gender. J Pediatr Orthop. 2018;38(9):465–470. doi:10.1097/BPO.0000000000000852
21. Ellis SH, Perriman DM, Burns AWR, Neeman TM, Lynch JT, Smith PN. Total volume of cam deformity alone predicts outcome in arthroscopy for femoroacetabular impingement. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1283–1289. doi:10.1007/s00167-019-05383-9
22. Richter C, Ishoi L, Kraemer O, Holmich P, Thorborg K. Association of 5-year hip arthroscopy outcomes with hip morphology and cartilage status at time of surgery: a national registry study with HAGOS outcomes in 281 patients with femoroacetabular impingement syndrome. Orthop J Sports Med. 2024;12(3):23259671241238742. doi:10.1177/23259671241238742
23. Ha YC, Lim JY, Won YS, Lee YK, Koo KH, Kim JW. Outcomes of arthroscopic femoroplasty in patients with cam lesions: minimum 2-year follow-up. J Orthop Surg (Hong Kong). 2020;28(2):2309499020942049. doi:10.1177/2309499020942049
24. Larson JH, Chapman RS, Allahabadi S, et al. Patients with lateral and anterolateral cam morphology have greater deformities versus typical anterolateral deformity alone but no differences in postoperative outcomes: a propensity-matched analysis at minimum 5-year follow-up. Arthroscopy. 2025;41(1):55–65. doi:10.1016/j.arthro.2024.03.020
25. McGovern RP, Martin RL, Christoforetti JJ, et al. Relationship of average outcomes scores and change in status requires further interpretation between 1 and 2 years following hip arthroscopy. Am J Sports Med. 2022;50(12):3184–3189. doi:10.1177/03635465221122769
26. Tjong VK, Gombera MM, Kahlenberg CA, et al. Isolated acetabuloplasty and labral repair for combined-type femoroacetabular impingement: are we doing too much? Arthroscopy. 2017;33(4):773–779. doi:10.1016/j.arthro.2016.10.022
27. Ekhtiari S, Fairhurst O, Mainwaring L, Khanduja V. The Alpha Angle. J Bone Joint Surg Am. 2024;106(20):1910–1921. doi:10.2106/JBJS.23.01089
28. Mohtadi NG, Griffin DR, Pedersen ME, et al. The Development and validation of a self-administered quality-of-life outcome measure for young, active patients with symptomatic Hip disease: the International Hip Outcome Tool (iHOT-33). Arthroscopy. 2012;28(5):595–605;quiz606–10e1. doi:10.1016/j.arthro.2012.03.013
29. Robinson PG, Maempel JF, Rankin CS, Gaston P, Hamilton DF. Evaluation of the patient acceptable symptom state following Hip arthroscopy using the 12 item international hip outcome tool. BMC Musculoskelet Disord. 2020;21(1):5. doi:10.1186/s12891-019-3026-x
30. Sinkler MA, Magister SJ, Su CA, Salata MJ. Femoral version may impact hip arthroscopy outcomes in select patient populations: a systematic review. Arthroscopy. 2023;39(1):114–127. doi:10.1016/j.arthro.2022.06.026
31. Lee MS, Nam-Woo Kim D, Moran J, et al. Patients undergoing primary hip arthroscopy report favorable outcomes at minimum 10 year follow-up: a systematic review. Arthroscopy. 2023;39(2):459–475. doi:10.1016/j.arthro.2022.10.040
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.