")
Back to Journals » Open Access Emergency Medicine » Volume 15
Impact of Prehospital Antibiotics on in-Hospital Mortality in Emergency Medical Service Patients with Sepsis
Authors Kotnarin R , Sirinawee P, Supasaovapak J
Received 23 March 2023
Accepted for publication 22 May 2023
Published 26 May 2023 Volume 2023:15 Pages 199—206
DOI https://doi.org/10.2147/OAEM.S413791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Rujabhorn Kotnarin, Penpischa Sirinawee, Jirapong Supasaovapak
Department of Emergency Medicine, Rajavithi Hospital, College of Medicine, Rangsit University, Bangkok, Thailand
Correspondence: Rujabhorn Kotnarin, Department of Emergency Medicine, Rajavithi Hospital, College of Medicine, Rangsit University, Bangkok, 10400, Thailand, Tel +66 90464 6554, Email [email protected]
Background: Sepsis is a life-threatening medical condition that requires early recognition and timely management to improve patient outcomes and reduce mortality rates. Administering antibiotics in the prehospital setting can be effective to reduce the time to antibiotic therapy, which may be crucial for sepsis patients. However, the impact of prehospital antibiotics on mortality in sepsis patients remains uncertain, and the current evidence to support this practice in middle-income countries is particularly limited.
Methods: This was a single-center, retrospective-prospective cohort study aimed at determining the impact of prehospital antibiotics on in-hospital mortality rates among adult patients with sepsis. The study included patients who received care from the advanced level of Emergency Medical Service between June 2020 and October 2022 and compared the mortality rates of patients who received prehospital antibiotics with those of their counterparts who did not.
Results: In this study, 180 patients with a mean age of 71.6 ± 15.7 years were included, of whom 68.9% experienced respiratory infections. The results demonstrated that the prehospital antibiotic group had a significantly lower in-hospital mortality rate (32.2%) than the non-prehospital antibiotic group (47.8%; p=0.034). After adjusting for confounding factors, the odds ratio was 0.304 (95% CI: 0.11, 0.82; p=0.018), indicating a 69.6% lower incidence of in-hospital mortality in the prehospital antibiotic group. Furthermore, the prehospital antibiotic group received antibiotics significantly earlier (16.0 ± 7.4 minutes) than the non-prehospital group (50.9 ± 29.4 minutes; p< 0.001).
Conclusion: This study provides evidence to support the administration of antibiotics to sepsis patients in the prehospital setting, as this practice can reduce mortality rates. However, larger, multicenter studies are required to confirm these findings and to further investigate the potential benefits of prehospital antibiotics in improving patient outcomes.
Keywords: sepsis, prehospital, emergency medical services, antibiotic
Introduction
Sepsis is a life-threatening and time-sensitive condition resulting from a dysregulated immune response to an infection.1 Its impact is significant; it affects millions of individuals worldwide annually and results in a mortality rate of up to one-third of those affected. In 2017, there were 48.9 million cases and 11 million deaths globally from infections, accounting for 20% of all global deaths.2 In Thailand, sepsis is a major public health problem, and it is the leading cause of in-hospital deaths, with approximately 175,000 cases and 45,000 deaths reported in 2021, accounting for 32% of all mortality. Even in Bangkok, a city with a diverse population and access to advanced healthcare facilities, sepsis mortality rates have been found to rise to as high as 54%.3 The development of more effective treatments for sepsis continues to pose a challenge in terms of improving patient outcomes and reducing the global burden of mortality.
The recent update of the Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021 (SSC2021) recommended early antibiotic therapy, ideally within 1 to 3 hours of diagnosis of sepsis and within the first hour in cases of septic shock.4 According to evidence-based medicine, emergency medical services play a crucial role in the delivery of sepsis care bundles5–10 and reducing the time to antibiotic therapy;7,11,12 however, a recent randomized controlled trial which evaluated the effect of early prehospital antibiotic therapy administration in patients with suspected infection showed negative results in terms of reducing mortality.13 Nonetheless, several studies have found that prehospital antibiotic administration is associated with lower mortality, particularly in patients with septic shock.14–16
As mentioned above, the impact of prehospital antibiotic therapy on sepsis patient outcomes remains a topic of debate. There are differences in the organization of emergency medical services worldwide,17 and there is limited evidence to support the benefit of prehospital antibiotic therapy in middle-income countries such as Thailand. To address this issue, our study aimed to investigate the impact of prehospital antibiotic therapy on in-hospital mortality rates for sepsis patients. Our investigation focused on sepsis patients who received care from Narenthorn EMS Center, a hospital-based ambulance center located at Rajavithi Hospital. In this study, we aim to provide insights into the potential benefits of prehospital antibiotic therapy for sepsis management in Thailand and other similar settings.
Materials and Methods
Study Design and Population
This was a single-center, retrospective-prospective cohort study focused on sepsis patients treated by Narenthorn EMS center, which performs an average of approximately 1300 EMS operations annually. The research was conducted between June 2020 and October 2022, with the Narenthorn prehospital sepsis protocol being implemented on Dec 13, 2021.18 The prehospital sepsis protocol provides a screening checklist that uses the SIRS, NEWS, and MEWS criteria,4 which were the sepsis screening tools recommended by the SSC2021 guidelines, as well as an initial patient assessment checklist. On-scene treatment involved administering intravenous fluid and antibiotics (specifically ceftriaxone for community-acquired infections and ceftazidime for hospital-acquired infections), as well as screening for drug allergies. A blood draw was obtained for septic workup, including hemocultures and lactic acid analyses, which were then sent to the Rajavithi Hospital laboratory. Pre-arrival notification for sepsis alert was also included in the protocol. The study population consisted of all sepsis patients transported to the Emergency Department of Rajavithi Hospital, a tertiary care facility in Bangkok, Thailand, during the study period. In the retrospective group, sepsis patients were diagnosed individually by the on-scene EMS physician, while in the prospective group, the screening checklist based on the SIRS, NEWS, and MEWS criteria was used to assist in sepsis screening, and diagnosis was made based on individual judgement. The inclusion criteria were patients aged 18 years or older, while exclusion criteria were sepsis patients who required cardiopulmonary resuscitation, were pregnant, had been involved in an accident, required emergency surgery, or had documented antibiotic allergies, which were determined based on on-site interviews with patients and their relatives.
Data Collection and Sample Size
The sample size for this study was calculated using the ratio comparison formula.19 The estimated proportion of interest (P) was derived from data obtained in a previously published study.14 To achieve adequate statistical power, at least 76 participants were required for each of the two groups being compared. Data were collected using both Electronic EMS Medical records and emergency medical records. The variables of interest included patients’ demographic characteristics (age, gender, comorbidities), suspected origin of sepsis, prehospital vital signs (mean blood pressure, diastolic and systolic blood pressure, heart rate, pulse oximetry, respiratory rate, temperature, and Glasgow coma scale), severity scores (NEWS, MEWS), duration of prehospital care, prehospital treatments administered (antibiotic therapy type and dose, initial intravenous fluid type, time to antibiotic therapy), and laboratory parameters such as serum lactate and WBC. The primary outcome measure was in-hospital mortality, while secondary outcomes included ICU admission, hospital length of stay (LOS), and ICU LOS.
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice Guidelines, and it was approved by the Rajavithi Hospital Ethics Committee for Human Research (approval number 64269). For the prehospital antibiotic group, informed consent was obtained from patients or their direct relatives. For the non-prehospital antibiotic group, the requirement for informed consent was waived by the ethics committee. Participants were allowed to drop out of the study at any time by informing the on-scene EMS physician, and withdrawal from the study did not affect their right to receive the usual treatment. To protect the privacy of the participants, their names were replaced with hospital numbers, and all data used in the study was de-identified.
Statistic and Data Analysis
Patient demographic data were presented as percentage for baseline data and mean for normally distributed qualitative data. Standard deviation, median, minimum, maximum, and interquartile ranges were also reported. Categorical data were compared using Chi-square and Fisher’s exact tests, while continuous data from two uncorrelated populations were compared using the Student’s t-test for normally distributed data and the Mann–Whitney U-test for non-normally distributed data.
The primary outcome of this study was evaluation of the proportion of in-hospital mortality, with secondary outcomes consisting of ICU admission rates, hospital length of stay (LOS), and ICU LOS. The data were analyzed using logistic regression for the primary outcome, and median regression analysis was employed for hospital LOS and ICU LOS. Inferential results were reported with 95% confidence intervals (CIs), and a p-value<0.05 was considered statistically significant for all tests. Overall, these statistical analyses provided a comprehensive assessment of the relationship between the variables and the primary outcome of in-hospital mortality.
Results
General Characteristics and Clinical Features of the Subjects
A total of 194 patients from the Narenthorn Emergency Medical Services (EMS) database fulfilled the criteria between June 2020 and October 2022. Fourteen patients were excluded, leaving 180 patients included in the study (Figure 1). The study population had a mean age of 71.63 ± 15.73 years, 103 of the participants (53%) were female, and a total of 157 (87.2%) had at least one comorbidity. The majority of the population had respiratory infections (68.90%), while 14.40% and 12.80% had infections of the GU and GI tracts, respectively.
 |
Figure 1 Study flow chart. |
The prehospital antibiotic group had a significantly shorter time to receiving antibiotics (16.04 ± 7.41 minutes) than the non-prehospital group (50.97 ± 29.44 minutes; p-value <0.001). However, the median operative interval was significantly longer in the prehospital antibiotic group 47.00 min, IQR: 39.87–58.09) than in the t non-prehospital group (39.16 min, IQR: 24.78–48.74) (p-value <0.001).
In the overall population, initial fluid administration consisted of crystalloids in 91.67% of cases, while patients who did not receive fluid administration had fluid overload status. Of the 180 patients included in the study, 101 (56.11%) received vasopressor administration, and there was no statistically significant difference between the prevalence of vasopressor use in patient resuscitation in the two groups. Further details of the clinical characteristics of the population are provided in Table 1.
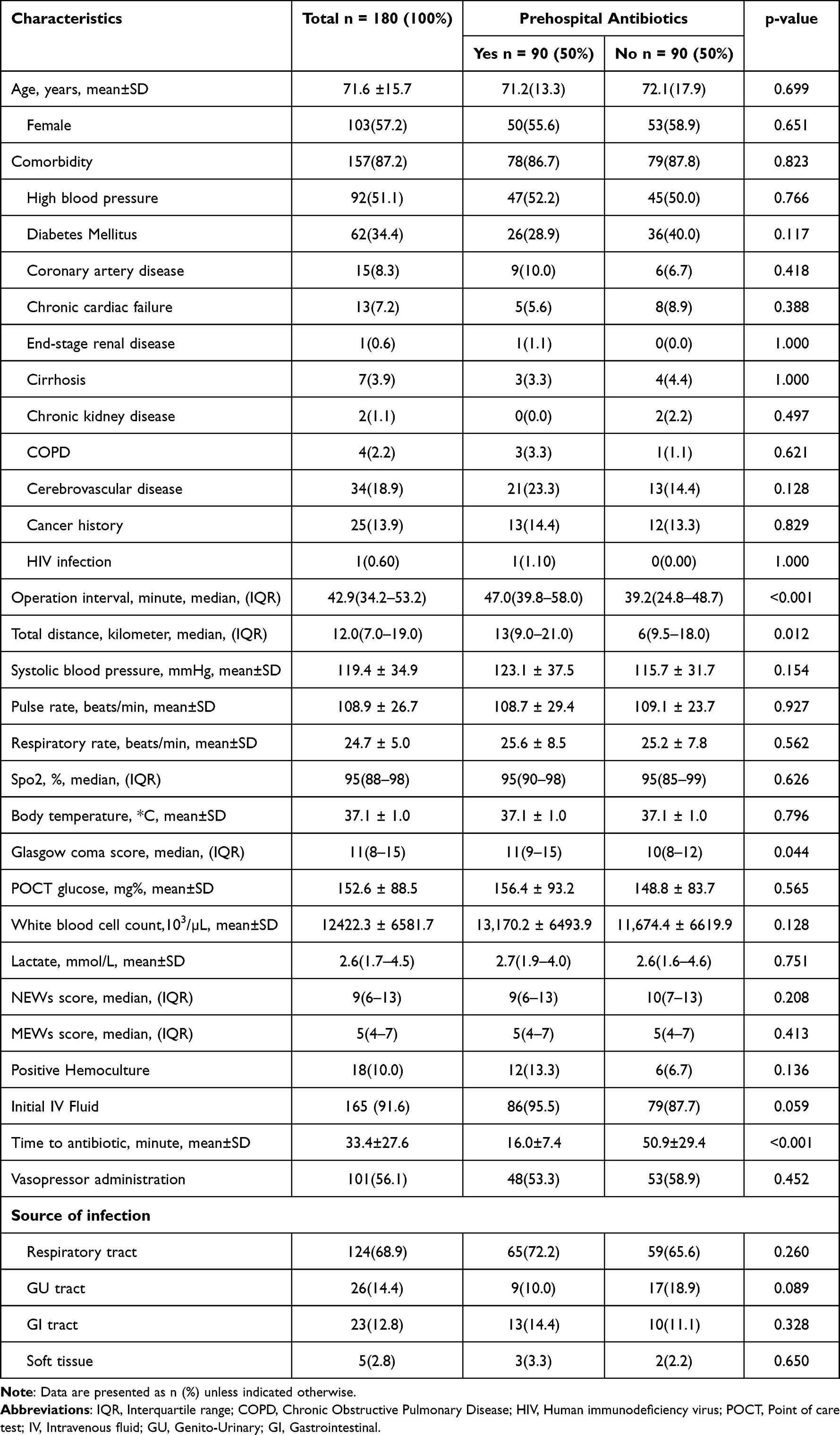 |
Table 1 Demographic and Clinical Characteristics of Participants |
Clinical Outcomes
There was a significant difference between mortality in the prehospital antibiotic and the non-prehospital antibiotic groups, with mortality rates of 32.20% and 47.80% respectively. The prehospital antibiotic group’s mortality rate was significantly lower, with an odds ratio of 0.52 (95% CI: 0.28, 0.95; p=0.034), an approximately 48% lower in-hospital mortality rate. The results of multiple logistic regression analysis revealed that the prehospital antibiotic group had a significant reduction in mortality after adjusting for multiple variables that are potential confounding factors (including Age, Gender, Comorbidities, Operation Interval, Systolic Blood Pressure, Pulse Rate, Respiratory Rate, SpO2, Body Temperature, Glasgow Coma Score, POCT Glucose, White Blood Cell Count, Serum Lactate, and Positive Hemoculture in the model. The adjusted odds ratio was 0.304 (95% CI: 0.11, 0.82; p=0.018), meaning that the prehospital antibiotic group had 69.6% lower in-hospital mortality compared to the non-prehospital antibiotic group, after allowing for other potential confounding factors.
The prehospital antibiotic group had a median hospital length of stay of 9.5 days (IQR: 5.0–16.0) compared with the non-prehospital antibiotic group’s 8.0 days (IQR: 3.0–22.0). The absolute difference between the two groups, estimated by median regression analysis, was not statistically significant (95% CI: −23.84, 7.84 p-value =0.357).
In terms of ICU admission, the prehospital antibiotic group had a rate of 7.80% compared with their non-prehospital antibiotic counterparts’ 6.70%, and there was no statistically significant difference between these rates in the two groups, with an odds ratio of 1.18 (95% CI: 0.38, 3.66 p-value = 0.774). The ICU lengths of stay for the prehospital antibiotic and non-prehospital antibiotic groups were 7.0 days (IQR: 6.0–14.0) and 13.50 days (IQR: 6.0–14.0) respectively, and the absolute difference between the two groups, estimated by median regression analysis, was not statistically significant (95% CI: −23.84, 7.84 p-value =0.290). The outcomes are summarized in Table 2.
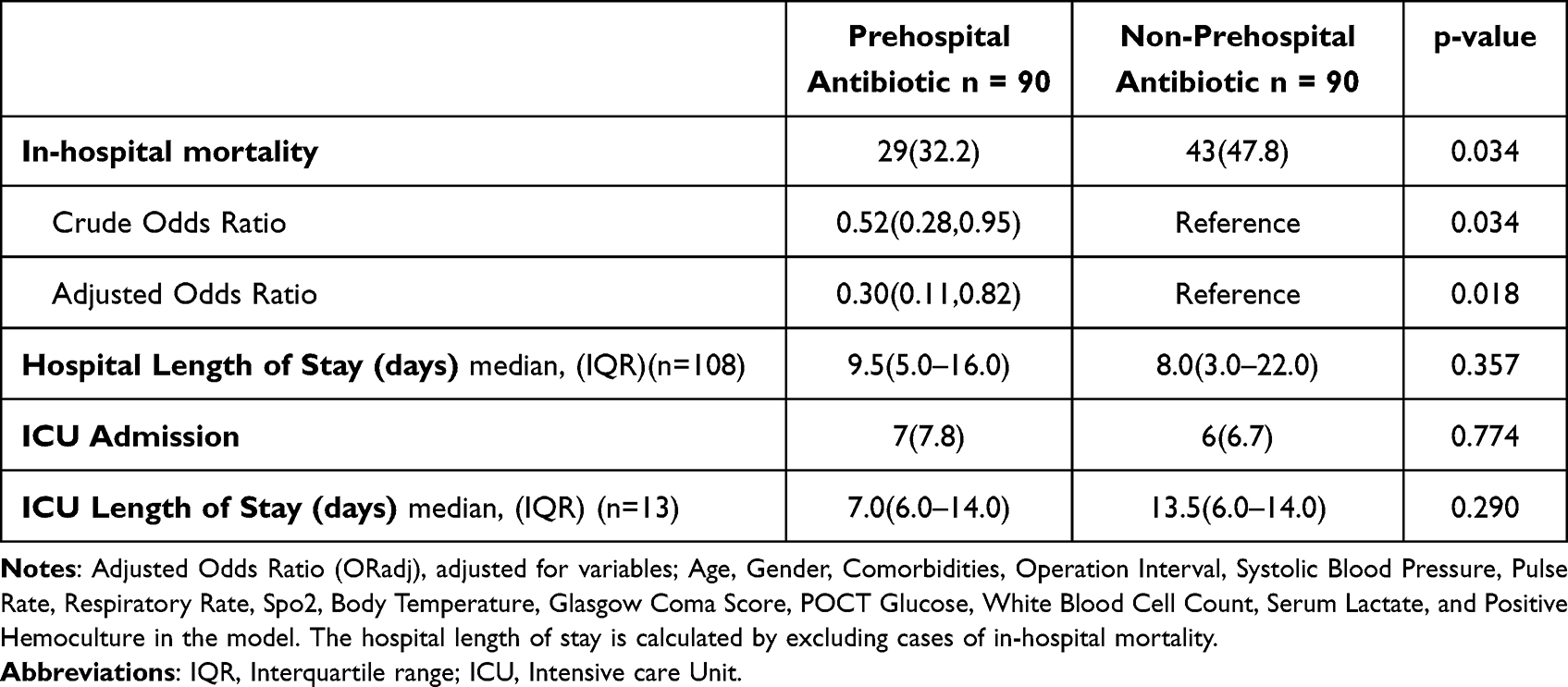 |
Table 2 Outcomes of Prehospital Antibiotics in Emergency Medical Service Patients with Sepsis |
Discussion
The present study provides evidence to support the use of prehospital antibiotics by EMS providers for patients with suspected sepsis. This retro-prospective observational study showed that prehospital antibiotic therapy was associated with significantly lower mortality rates than those of patients who did not receive antibiotics. This is consistent with most prior research,14 despite the fact that a recent randomized controlled trial evaluating the effect of early prehospital antibiotic therapy administration in patients with suspected infection showed negative results in terms of reducing mortality.13 The study also demonstrated that prehospital antibiotic administration reduced the time to antibiotic therapy, emphasizing the importance of timely treatment in sepsis management.
The study also revealed a high mortality rate, which may have been influenced by various factors; for instance, the study was conducted in the Bangkok area, where the mortality rate of sepsis is approximately 54%.3 Additionally, there was a large number of elderly participants with a high prevalence of comorbidities,20 and the study was conducted during the COVID-19 pandemic, which may have adversely affected sepsis outcomes for patients due to co-infection and secondary infection, which can aggravate this condition and perpetuate organ dysfunction, leading to high mortality rates.21 Changes in healthcare delivery, hospital protocols, resource allocation, patient behavior, and demographics may also have contributed to these findings. To further investigate these results and rule out the potential impact of COVID-19 infection, future studies should consider controlling the underlying conditions and external factors affecting sepsis outcomes.
The study’s findings regarding ICU admission probability showed that the rate of admission and the number of hospital days in the two groups were not significantly different because of a high bed occupancy rate in the intensive care unit, which may have limited the admission to ICU of patients with suspected sepsis. The fact that the hospital’s limited ICU capacity may have prevented the admission of eligible patients highlights the need to consider healthcare system capacity and resources when assessing the impact of interventions on patient outcomes. Transferring patients who are no longer in a critical phase to secondary hospitals because of limitations in ICU capacity could have affected ICU length of stay.
The implementation of a prehospital sepsis protocol, initiated in December 2021, was associated with a reduction in hospital mortality among EMS sepsis patients compared to that of a retrospective group of non-prehospital antibiotic-treated patients. The prehospital sepsis protocol consisted of several key components, including a screening checklist that utilizes the SIRS, NEWS, and MEWS criteria,4 which are the sepsis screening tools recommended by the SSC2021 guidelines, an initial patient assessment checklist, on-scene treatment with intravenous fluid and antibiotics, a blood draw for septic workup and pre-arrival notification of sepsis alert to the Emergency department. These findings suggest that the prehospital sepsis bundle of care may be an effective strategy for reducing delays in the diagnosis and treatment of sepsis in emergency departments, particularly in settings with high levels of crowding. Our study highlights the importance of initiating the sepsis bundle of care in the prehospital setting.
However, it is essential to consider the limitations of single-center studies, which are conducted in one particular hospital and EMS center, meaning that the results may not be generalizable to other healthcare settings. Furthermore, these studies are more prone to bias and may be influenced by confounding factors that could affect the results. Therefore, the study’s findings should be confirmed by larger, multi-center studies to determine their generalizability to diverse healthcare settings. Overall, the study provides important insights into the use of prehospital antibiotics for suspected sepsis and highlights the need for further research in this area.
Limitations
This study has several limitations that should be considered when interpreting the results. Firstly, it was conducted at a single center, which may limit the generalizability of the findings to other healthcare settings. In order to test the external validity of the results, further research using multi-center studies is needed regarding the impact of prehospital antibiotics on patients with suspected sepsis in emergency medical systems.
Secondly, the retrospective data collection was performed during the early stages of the COVID-19 pandemic, and this may have affected the in-hospital mortality rate. Although the data collection for the prospective study period was conducted when more treatments and vaccinations for COVID-19 were available, this may not have fully combated the impact of COVID-19 on the study results. Despite these limitations, the study provides valuable insights into the effects of prehospital antibiotics on patients with suspected sepsis.
Finally, the study was conducted in a hospital with high bed occupancy rates in the intensive care unit during a period of high levels of emergency unit crowding, and this may have limited the admission of patients with suspected sepsis to the ICU, potentially affecting the outcomes of the study, as some patients were treated in a general ward instead of receiving intensive care. To address this limitation, future studies should consider conducting research at hospitals with lower bed occupancy rates to ensure that all patients receive the appropriate level of care.
Conclusion
Our study indicates that administering antibiotics in prehospital settings can potentially reduce in-hospital mortality and shorten the duration of antibiotic treatments for patients with suspected sepsis. These findings highlight the potential benefits of implementing prehospital antibiotic protocols in resource-limited settings, particularly in middle-income countries. However, given the limitations of our small sample size, further research with larger, multicenter samples is necessary to provide more evidence on the effectiveness of prehospital antibiotic protocols for sepsis treatment in prehospital settings. Healthcare providers and policymakers should consider the feasibility and effectiveness of implementing such protocols to enhance sepsis care in these settings.
Acknowledgments
The authors would like to express their gratitude to Rajavithi Hospital and the College of Medicine, Rangsit University, for their financial support for this research. The authors also acknowledge the assistance of the Department of Emergency Medicine and Narenthorn EMS center for providing access to the data used in this study, as well as Rajavithi Research Center staff for statistical analysis consultation and manuscript preparation. The authors extend their sincere appreciation to the emergency medicine residents, nurses, paramedics, and emergency medical technicians at Narenthorn EMS center for their participation in this research.
Funding
The College of Medicine, Rangsit University funded this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fernando SM, Rochwerg B, Seely AJE. Clinical implications of the third international consensus definitions for sepsis and septic shock (sepsis-3). CMAJ. 2018;190(36):E1058–E1059. doi:10.1503/cmaj.170149
2. Fleischmann C, Scherag A, Adhikari NK, et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med. 2016;193(3):259–272. doi:10.1164/rccm.201504-0781OC
3. Bureau of Medical system supervision. Inspections Report 2021. Thailand: Bureau of Medical system supervision, department of medical services, Thailand ministry of public health; 2021.
4. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
5. Walchok JG, Pirrallo RG, Furmanek D, et al. Paramedic-initiated CMS sepsis core measure bundle prior to hospital arrival: a stepwise approach. Prehosp Emerg Care. 2017;21(3):291–300. doi:10.1080/10903127.2016.1254694
6. Hunter CL, Silvestri S, Stone A, et al. Prehospital sepsis alert notification decreases time to initiation of CMS sepsis core measures. Am J Emerg Med. 2019;37(1):114–117. doi:10.1016/j.ajem.2018.09.034
7. Cudini D, Smith K, Bernard S, et al. Can pre-hospital administration reduce time to initial antibiotic therapy in septic patients?. Emerg Med Australas. 2019;31(4):669–672.
8. Borrelli G, Koch E, Sterk E, Lovett S, Rech MA. Early recognition of sepsis through emergency medical services pre-hospital screening. Am J Emerg Med. 2019;37(8):1428–1432. doi:10.1016/j.ajem.2018.10.036
9. Moore C, Bulger J, Morgan M, et al. Prehospital recognition and antibiotics for 999 patients with sepsis: protocol for a feasibility study. Pilot Feasibility Stud. 2018;4:64. doi:10.1186/s40814-018-0258-8
10. Chippendale J, Lloyd A, Payne T, Dunmore S, Stoddart B. The feasibility of paramedics delivering antibiotic treatment pre-hospital to ‘red flag’ sepsis patients: a service evaluation. Br Paramed J. 2018;2(4):19–24. doi:10.29045/14784726.2018.03.2.4.19
11. Mixon M, Dietrich S, Floren M, et al. Time to antibiotic administration: sepsis alerts called in emergency department versus in the field via emergency medical services. Am J Emerg Med. 2021;44:291–295. doi:10.1016/j.ajem.2020.04.008
12. Peltan ID, Mitchell KH, Rudd KE, et al. Prehospital care and emergency department door-to-antibiotic time in sepsis. Ann Am Thorac Soc. 2018;15(12):1443–1450. doi:10.1513/AnnalsATS.201803-199OC
13. Alam N, Oskam E, Stassen PM, et al. Prehospital antibiotics in the ambulance for sepsis: a multicentre, open label, randomised trial. Lancet Respir Med. 2018;6(1):40–50. doi:10.1016/S2213-2600(17)30469-1
14. Martel T, Melmer MN, Leaman SM, et al. Prehospital antibiotics improve morbidity and mortality of emergency medical service patients with sepsis. HCA Healthcare J Med. 2020;1:3. doi:10.36518/2689-0216.1063
15. Jouffroy R, Gilbert B, Tourtier JP, et al. Impact of prehospital antibiotic therapy on septic shock mortality. Prehosp Emerg Care. 2021;25(3):317–324. doi:10.1080/10903127.2020.1763532
16. Nannan Panday RS, Wang S, Schermer EH, Cooksley T, Alam N, Nanayakkara PWB. Septic patients with cancer: do prehospital antibiotics improve survival? A sub-analysis of the PHANTASi trial. Neth J Med. 2020;78(1):3–9.
17. Al-Shaqsi S. Models of international Emergency Medical Service (EMS) systems. Oman Med J. 2010;25(4):320–323. doi:10.5001/omj.2010.92
18. Prehospital Sepsis Protocol [Homepage on the Internet]. Narenthorn EMS center; 2021. Available form: https://www.narenthorn.or.th.
19. Rosner B. Fundamentals of Biostatistics.
20. Yang Y, Yang KS, Hsann YM, Lim V, Ong BC. The effect of comorbidity and age on hospital mortality and length of stay in patients with sepsis. J Crit Care. 2010;25(3):398–405. doi:10.1016/j.jcrc.2009.09.001
21. da Silva Ramos FJ, de Freitas FGR, Machado FR. Sepsis in patients hospitalized with coronavirus disease 2019: how often and how severe? Curr Opin Crit Care. 2021;27(5):474–479. doi:10.1097/MCC.0000000000000861
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.