")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Impact of Patient Safety Culture on Job Satisfaction and Intention to Leave Among Healthcare Workers: Evidence from Middle East Context
Authors Al-Surimi K , Almuhayshir A, Ghailan KY, Shaheen NA
Received 15 September 2022
Accepted for publication 13 December 2022
Published 31 December 2022 Volume 2022:15 Pages 2435—2451
DOI https://doi.org/10.2147/RMHP.S390021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Khaled Al-Surimi,1– 4 Amirah Almuhayshir,1 Khalid Y Ghailan,5 Naila A Shaheen6– 8
1College of Public Health and Health Informatics, King Saud Bin Abdul-Aziz University for Health Sciences, Riyadh, Saudi Arabia; 2School of Health and Environmental Studies, Hamdan Bin Mohammed Smart University, Dubai, United Arab Emirates; 3Community Medicine and Public Health, Faculty of Medicine and Health Sciences, Thamar University, Dhamar, Yemen; 4King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 5Faculty of Public Health and Tropical Medicine, Jazan University, Jazan, Saudi Arabia; 6Department of Biostatistics and Bioinformatics, King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 7King Saud Bin Abdul-Aziz University for Health Sciences, Riyadh, Saudi Arabia; 8Ministry of National Guard-Health Affairs, Riyadh, Saudi Arabia
Correspondence: Naila A Shaheen, Department of Biostatistics and Bioinformatics, King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Ministry of National Guard-Health Affairs, P.O. Box 22490, Mail Code 1515, Riyadh, 11426, Saudi Arabia, Tel +966-11-4294472, Fax +966-11-4294466, Email [email protected]
Background: The association between patient safety culture and staff outcomes remains unclear to date. This study aimed to identify the relationship between patient safety culture/job satisfaction and intention to leave among healthcare workers.
Methods: A cross-sectional study was conducted using an online survey. Multinomial logistic regression analysis was used to investigate the association between the safety culture dimensions and the outcomes in terms of job satisfaction and intention to leave.
Results: Majority were females (77.2%); age between (20– 30) years were (66.1%). 1– 5 years work experience was reported by (98.2%); nurses accounted for (75.7%). (62.1%) reported very good patient safety grade. (78.3%) of respondents had no intention to leave; (84.3%) reported they like their job, (70.5%) stated that working in this hospital is like being part of a large family. However, (38%) said the hospital is not a good place to work, and morale in their clinical area is low. The overall composite scores were highest for “teamwork within hospital units (81.4)”, and “organizational learning (79.4)”, while lowest for “communication openness (37)“,staffing (26.5)”, and “non-punitive response to error (22.1)”. Females were two times more likely to leave their jobs compared to males (AOR: 2.36, 95% CI: 1.24– 3.46); intention to leave was 3.35 (95% CI = 2.19– 5.09). As for job satisfaction, ages between 31– 40 years tend to like their job two times more than other age groups (AOR: 1.90, 95% CI = 1.02– 3.55). The safety culture domains “staffing” and “hospital management support for patient safety” were linked to a higher odds ratio for job satisfaction.
Conclusion: Aside from gender and age, the dimensions of safety culture, including staffing, hospital management support, hospital handover, and transition, may have a signification impact on job satisfaction and intention to leave among healthcare workers.
Keywords: patient safety culture, staff outcomes, job satisfaction, intention to leave, healthcare workers
Plain Language Summary
This study focuses on assessing the relationship between patient safety culture with job satisfaction and intention to leave the job among healthcare workers. More than half of the participants were females (77.2%), age group 20–30 years (66%), and having a nursing background (76%). Majority of the participants had responded they had no intention to leave their job; they like their job, and stated that working in this hospital is like being part of a large family. Female participants had reported more intention to leave their job compared with males. Few factors affect healthcare workers intent to leave their job ie sex, age, and factors related to patient safety culture.
Introduction
Patient Safety Culture (PSC) is one of the key quality indicators in a healthcare organization. Patient safety means preventing harm to patients.1 PSC is a concept defined as “the product of individual and group values, attitudes, perceptions, competencies, and patterns of behavior that determine the commitment to, and the style and proficiency of, an organization’s health and safety management2” The required elements for building PSC in an organization were described as (i) environmental structure (ii) employee perception, and (iii) individual behavior. PSC is primarily based on the individual commitment. Studies had reported job satisfaction as an important factor affecting patient safety culture.3,4
Studies have shown the effect of PSC on staff outcomes, including adverse event reporting, medication error reporting, and staff injury rates.5–7 The turnover intention or intention to leave has been described as employee’s perception of job dissatisfaction and planning to leave the job or look for other job opportunities. The intention to leave is considered a proxy for actual turnover behavior among healthcare workers.8,9 Several factors, including work pressure, psychological issues, low pay, and a lack of career opportunities, have been reported to influence intent to leave.10–14 The rate of physician and nurse turnover in the healthcare system is increasing. According to Degen et al physicians have high turnover and inter-departmental change. Similarly, nursing staff turnover and job satisfaction have received considerable attention.15
Given that service quality and patient safety are heavily reliant on the healthcare workforce, it is essential to explore factors that may influence staff turnover.16 Healthcare worker shortage stems mainly from high turnover. This issue has been reported primarily, but not exclusively, among nurses.17 As a result, healthcare organizations face reduced organizational productivity, performance and efficiency.15 Additionally, higher costs are incurred in the areas of separation costs, recruitment and training. The reported adverse consequences of physician turnover are patient dissatisfaction, financial loss, and organizational instability.18
Employee turnover can also lead to organizational loss of experience and knowledge, higher workloads, and lower team morale, causing more staff to leave.15 When continuity of care is compromised, adverse events and prolonged length of stay are often reported in hospitals as a consequence.19,20
The perception of patient safety culture, job satisfaction and intention to leave have been studied extensively in the healthcare industry. However, few studies have examined the relationship between PSC, job satisfaction, and intention to leave. One study found a negative correlation between patient safety domains, such as “teamwork, safety climate, working conditions and safe behavior”, and intention to leave.21 Further, healthcare worker job satisfaction has been positively associated with PSC.4,22 However, the impact of PSC on job satisfaction remains unclear. Therefore, the aim of this study was to address the gap in the literature by exploring the influence of patient safety culture measures on healthcare workers’ (i) job satisfaction and (ii) intention to leave, along with predictors in a tertiary care hospital.
Methods
Study Design, Settings, and Participants
An electronic self-report survey available in two languages (Arabic and English) was emailed to all healthcare workers (clinical and non-clinical), including doctors, nurses, therapists, technicians, and other health professionals working in a tertiary care hospital. This hospital is a governmental tertiary care center, with a capacity of 1000 beds and more than 65 departments. A list of all healthcare workers was provided by the employee relation office. An email introducing the study and providing informed consent was sent to all the healthcare workers (male/female, full-time, and directly involved in patient care).
Data Collection Tools
Two well-known, validated patient safety culture surveys were utilized in this study: AHRQ’s “The Hospital Survey on Patient Safety”23 and “Safety Attitudes Survey”. The hospital’s patient safety culture, as perceived by healthcare workers, was assessed using “Hospital Survey on Patient Safety Culture”. This instrument consists of twelve dimensions of patient safety with a total of 42 items.24 Each dimension consists of 3/4 items. In addition, we focused on two employee outcomes, namely “job satisfaction” and “intonation to leave”. Twelve dimensions of safety culture were measured, including (1) Teamwork within units, (2) Supervisor/manager expectations and actions promoting patient safety, (3) Organizational learning, (4) Management support for patient safety, (5) Overall perceptions of patient safety, (6) Feedback and communication about error, (7) Communication openness, (8) Frequency of events reported, (9) Teamwork across units, (10) Staffing, (11) Handover & transitions, and (12) Non Punitive response to errors. Responses to all items in the twelve dimensions were rated as agree or disagree on a five-point Likert scale. Agreement response answers included options; (“strongly disagree”, “disagree”, “neutral”, “agree”, to “strongly agree”). Frequency response answers included options (“never”, “rarely”, ‘sometimes’, “most of the times” to “always”). In addition, the tool contains two individual items on patient safety outcomes; patient safety grade and number of events reported, which were assessed as single item outcomes. The patient safety grade responses included, (“excellent”, “very good”, “acceptable”, “poor and failing”). The number of events was measured on a categorical scale with responses that can be grouped into six categories. Some items in the tool were worded negatively.
Questions pertaining to job satisfaction were taken from the Job Satisfaction domain of the Survey Attitudes Survey,25 a well-known and widely used validated tool adapted for use in various clinical settings to assess caregivers’ attitudes towards PSC. The job satisfaction domain consists of five items. The questions assess respondents’ preferences for how much they like their job; co-workers; work environment; overall perceived morale in the clinical area; and perceived pride in working in the hospital. Responses were collected on an agreement scale (“strongly disagree”, “disagree”, “neutral”, “agree”, to “strongly agree”). The second outcome, intention to leave, was assessed by a single question, “Have you ever thought about leaving the hospital?” Response options for this item included (“never”, “rarely”, “sometimes”, “most of the time” and “always”).
Scoring of Responses
All item responses, measured on a Likert scale, were coded with scores from 1–5. For example, the lowest score of 1 corresponded to strongly disagree, 2= disagree, 3= neutral, 4 =agree, and 5=strongly agree. For the response options “Never, Rarely, Sometimes, Most of the time and Always”, points were assigned in a similar fashion, so that never =1, while always= 5. Negatively worded items were reverse scored/coded to ensure that the scores assigned to negatively worded statements were consistent and adequately reflected the meaning of terms, such as “agree” or “disagree”, to respondents. The lowest score of one was assigned to “strongly agree”, while the highest score of 5 was assigned to “strongly disagree”.
The total number of responses for each composite item was recorded, and the overall percentage scores for positive, negative and neutral response rates were presented. Positive % responses were calculated from the sum of strongly agree and agree responses. Negative % responses were calculated from the sum of strongly disagree and disagree responses. The total score for each response parameter (negative, neutral, positive) per patient safety culture dimension was calculated by adding the total score for each response and dividing the sum by the total number of items in each dimension. The higher the percentage of positive responses, the more positive staff attitudes toward patient safety in their work environment. Moreover, data were collected on the demographic characteristics of healthcare staff, job position, and length of service at the hospital and in a particular specialty or department and level of direct patient contact have been collected.
Ethical Considerations
Ethical approval for this study was obtained by King Abdullah International Medical Research Center Institutional Review Board (IRB) (number SP15/117). All ethical considerations including confidentiality and privacy of the respondents’ personal information and getting the informed consent were displayed at the beginning of the electronic survey as an introductory paragraph explaining the study objectives.
Statistical Analysis
All data were analyzed using SPSS version 22 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as frequencies / percentages. The continuous variables were reported as means and standard deviation. The chi-square test was used to explore the association between the safety culture domains and job satisfaction and intention to leave. Logistic regression was used to determine the association between patient safety culture domains, job satisfaction and intention to leave. P-value <0.05 and 95% confidence interval were used to indicate statistical significance.
Results
Study Sample Characteristics
Out of 1500 hospital employees, 800 subjects responded to the survey, but 137 of these responses (17%) were excluded from the final analysis due to not fulfilling the AHRQ inclusion criteria, resulting in 663/800 (82.8%) valid responses. The majority of respondents were female (77.2%); over half of them aged between 20–30 years old (66.1%); 87.6% hold a bachelor’s degree. Nearly all respondents (98.2%) had been working within the study hospital for a period between 1–5 years and had been working within the hospital unit for the same period. Most of the respondents (85%) worked between 40–59 hours per week. Nurses constitute the majority of respondents (75.7%). Most of the participants (82%) reported their work required direct contact with patients. About two-thirds (62.1%) of the respondents graded the hospital patient safety as very good (62.1%), and over the half of the study participants (58%) stated that no adverse events have been reported compared with (34%) stated they had reported 1 to 5 adverse events (Table 1).
 |
Table 1 Socio-Demographic and Occupation Related Characteristics, and Patient Safety Grades Reported by Healthcare Workers |
Patient Safety Culture Assessment
The overall composite scores were highest among the following safety culture dimensions: Organizational Learning (79.4) and Teamwork within Hospital Units (81.4). The Positive Response Rate (PRR) in these two dimensions exceeded the cut-off value of 75% as described by AHRQ. The overall composite scores for “communication openness”, “staffing” and “non-punitive response to error” had the lowest scores among all 12 safety culture dimensions (36.9, 26.5, and 22.1), respectively. The particular items in which respondents scored very low included “Staff are afraid to ask questions when something does not seem right”, “We are given feedback about changes put into place based on event reports”, “Staff are worried that mistakes they make are kept in their personnel file” and “Staff in this unit work longer hours than is best for patient car”. In general, low overall composite scores for; “teamwork across hospital units (49.5)”, “handoffs and transitions (39.7)” and “hospital management support for patient safety (56.6)” were summarized in Table 2. The dimension: handovers and transitions scored below (50).
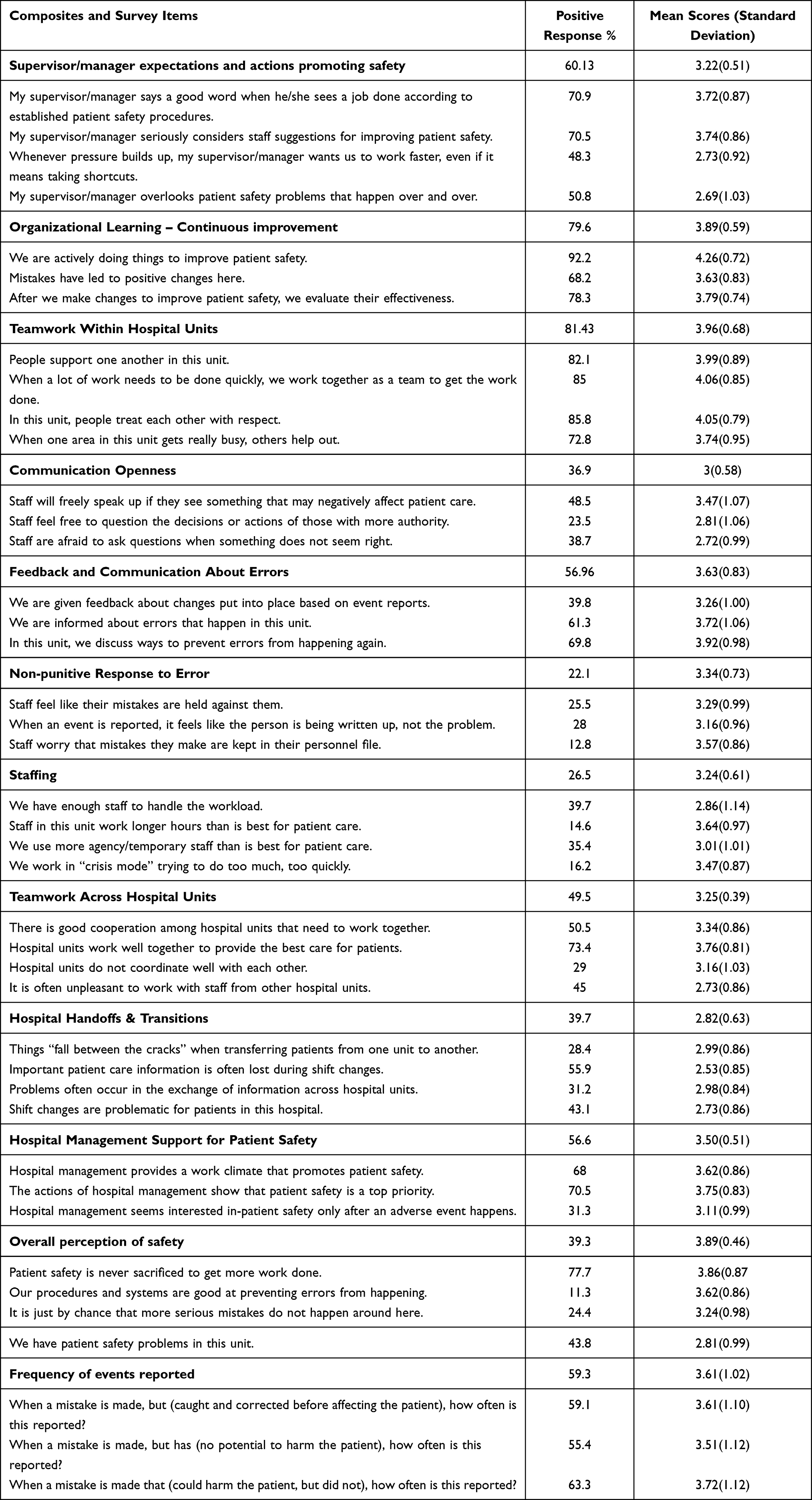 |
Table 2 Distribution of Positive Responses and Mean Scores for Safety Culture Composites/Items |
Staff Outcomes Measures: Intention to Leave and Job Satisfaction
The Outcomes measures in terms of intention to leave and job satisfaction level have been displayed in Table 3. More than two-thirds (78.3%) of the healthcare workers reported they had no intention to leave. As for the job satisfaction, about three-thirds (84.3%) reported that they like their job, and about three-fifths (70.5%) stated that working in this hospital is like being part of a large family. However, about (38%) think this hospital is not a good place to work, and moral in this clinical area is not high.
 |
Table 3 Staff Outcomes Measures, Intention to Leave and Job Satisfaction Level |
Factors Associated with Staff Outcomes of Intention to Leave and Job Satisfaction
The predictor of intention to leave and job satisfaction are summarized in Table 4. Female were two times more likely to leave their job compared to male respondents (AOR: 2.36, 95% CI: 1.24–3.46). The PSC composites that were significantly associated with lower odds of intention to leave the job were: supervisor/manager expectations and actions promoting safety, teamwork within hospital units, staffing, and hospital management support for patient safety. The study results showed that intention to leave were 3.35 times (95% CI = 2.19–5.09) more likely for every unit increase in hospital hand-offs and transitions. Logistic regression analysis showed that respondents aged between 31–40 years tend to like their job two times more than other age groups (AOR: 1.90, 95% CI = 1.02–3.55). The other domains associated with an increased odds ratio for liking the job by healthcare workers were staffing domain and hospital management support for patient safety.
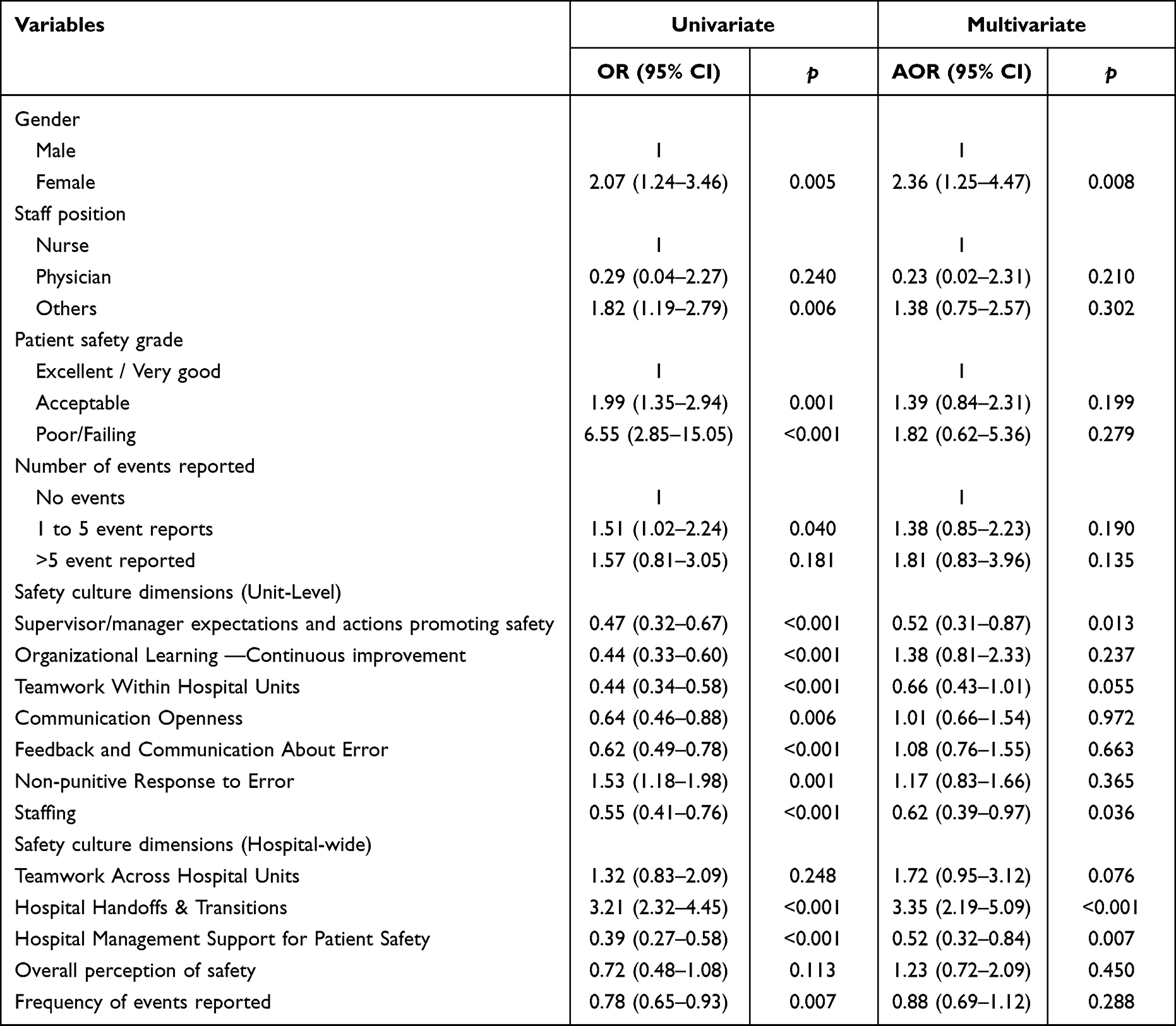 |
Table 4 Predictors of Healthcare Workers’ Intention to Leave |
Table 5 shows the factors associated with job satisfaction. The respondents who have been working in the hospital for more than 11 years were about six times more likely to think that working here is like being part of a large family. Other composites that were associated with higher odds of thinking that being part of a large family were: supervisor/manager expectations and actions promoting safety, teamwork within hospital units, and hospital management support for patient safety. The odds of thinking this hospital is a good place to work at and feeling proud of working here are two times higher for males than females. For those who spent over 11 years in current position are more likely to think this hospital is a good place to work. Also, feeling proud of working in this hospital was increased by 4.87 times (95% CI = 1.37–17.34) for older healthcare workers more than others. There were other composites associated with higher odds of job satisfaction domains which were: supervisor/manager expectations and actions promoting safety, teamwork within hospital units, staffing, and hospital management support for patient safety, unlike hospital handoffs and transitions domain which are associated with a lower odds ratio of job satisfaction domains.
 | 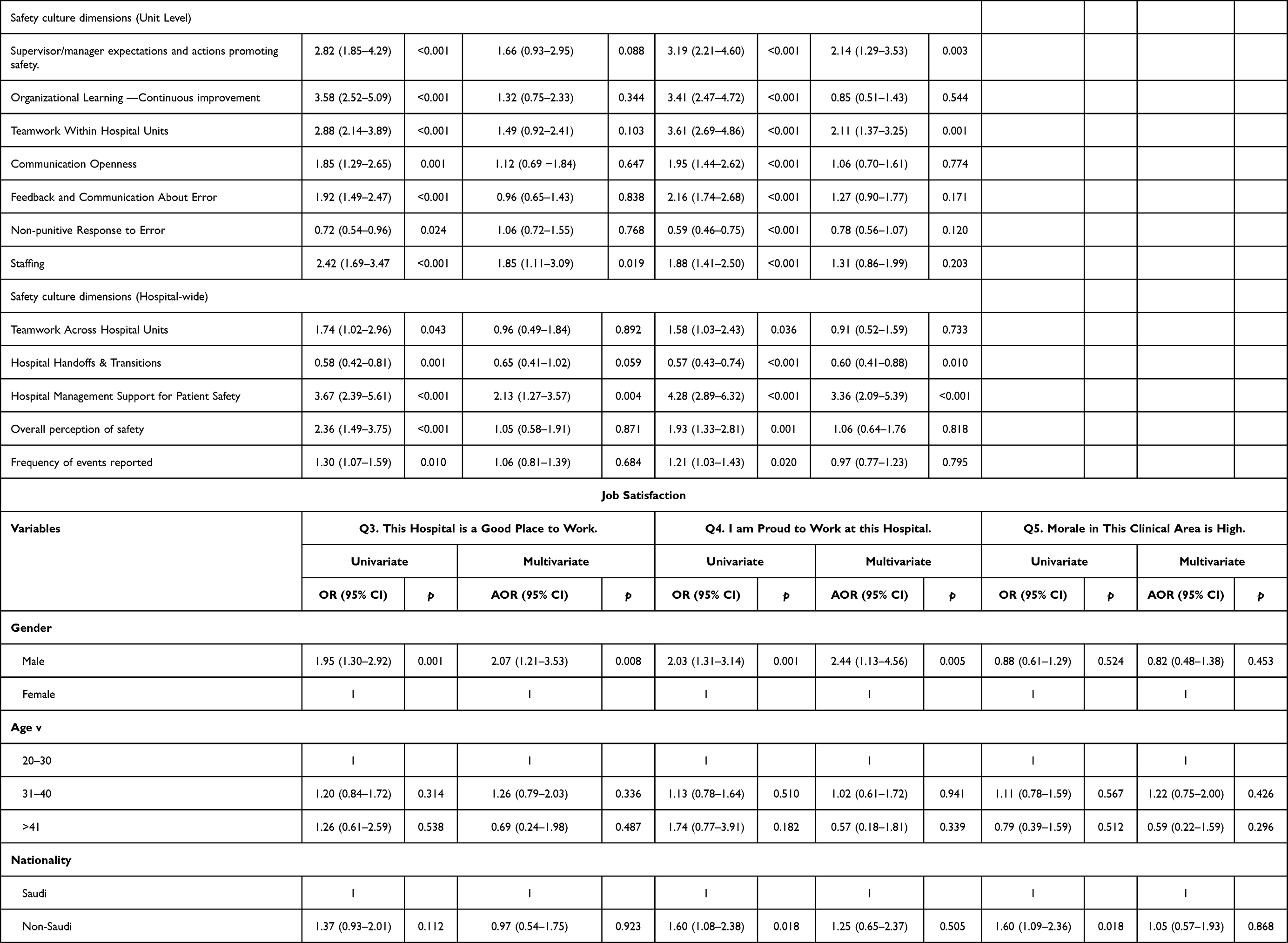 |  |
Table 5 Predictors of Healthcare Workers’ Job Satisfaction |
Discussion
This paper aimed to address the gap in the literature by exploring the influence of PSC measures on staff outcomes in terms of employee’s job satisfaction and intention to leave in healthcare settings. Healthcare workers are the foundation of the healthcare organization. It is necessary to understand the relationship that may influence healthcare workers turnover given the global challenge of healthcare workers shortage and the resulting impact on healthcare system and delivery of health services. It has been reported that job satisfaction is linked to the intention to leave, staff turnover, absenteeism, and perceived stress.26
Patient Safety Culture
The current study identifies PSC areas of strength like organizational learning and continuous improvement (79.4%), and teamwork within hospital units (81.4%). However, some areas in need of improvement that received the lowest rating were “communication openness; 36.9%”, “staffing; 26.5%”, and “non-punitive response to error; 22%”. In particular, “lack of coordination between hospital units”, “things falling between cracks during transitions and handovers” and “hospital management shows interest in patient safety only after the occurrence of adverse events” were items that had a negative impact on the overall rating of the three dimensions. Although organizational learning has been studied from different aspects in the past years, it has not been clearly defined. Most researchers define organizational learning as a process that grows over time and is associated with acquired knowledge and improved performance. Managers are responsible for developing systems and processes to sustain learning activities and incorporating them into daily performance to improve the learning process.27 The findings of the current study show that the organizational learning domain received one of the highest scores (79.4) and exceeded the cut-off score of 75%, indicating that the measure was positive. Most respondents agreed that unified staff actively take action to improve patient safety and evaluate its effectiveness. The findings are consistent with previous studies, in which organizational learning was cited as the most positively rated composite.28,29 However, a more recent study in Saudi Arabia reported lower scores on organizational learning/continuous improvement (65%), compared to the current study.30
Teamwork within units can be defined as the staff understanding of the efficiency of collaboration and support between unit members.24 One of the strengths of the current findings is teamwork within hospital units; the PRR (81.4%) was the highest among other domains. The findings are consistent with other studies on teamwork within hospital units. Studies conducted in Saudi Arabia concluded that the item “teamwork within hospital units” was positively rated (more than 70%) by healthcare workers.30,31 Consistent with our findings, with respect to the element “teamwork within the unit”, supportive staff, teamwork environment, and a mutual respect were rated significantly high with more than 80% positive ratings. In contrast, the element “when one area in this unit gets really busy, others help out” was reported as low (7.1%) compared to the current results (72%).30 Other studies have reported that teamwork within units, mutual support among employees, the ability to work as a team under pressure, and mutual respect were the strongest domains in PSC.28,29,32,33
The climate of teamwork and safe behavior domains received a high score of 73.8%; a value very close to the concept of positive safety climate for patient safety.21 This finding is important because studies on climate and safety culture indicate that teamwork developed through effective communication can be reflected in mutual collaboration among professionals, leading to positive outcomes such as job satisfaction and efficiency in activities.34
A non-punitive response to errors means that healthcare workers understand that their errors will be dealt with, and consequently, will not be used against them or recorded in their personnel file.23 The composite score for non-punitive response to errors had the lowest score of all 12 dimensions of safety culture (22.1%), indicating that these aspects of PSC require the most improvement efforts. Studies conducted in Saudi Arabia have shown similar results to the current study. The non-punitive response to error was 22%, while under-reporting of events over the past 12 months was 43%. In addition, staffing (22%), and teamwork across hospital units (27%) were cited as aspects that needed improvement.30,31 Furthermore, studies have shown that non-punitive response to errors, in addition to staffing, were considered the weak areas of PSC, while other items and the overall PSC score were described as neutral. The item of non-punitive response to error has shown the weakest association with the outcome variable of measuring perceptions of patient safety.33,35 Another study found similar findings, with the lowest positive mean score (19.5%) for a non-punitive response to an error.28 Staffing is a significant predictor of PSC. As can be seen from the results, staffing is one of the composites with the lowest value, receiving only one positive value (26.5%). A significant challenge for the hospital today is providing a robust and capable workforce.29 A workforce shortage can cause employees to suffer from stress and lack of sleep. This finding leads to a drop in performance due to a shortage in the workforce. Therefore, errors may occur, affecting quality and performance.36 Our results suggest that more positive staffing ratings increases the likelihood of positive perceptions of job satisfaction and decreases the likelihood that an employee will leave his or her job. Numerous studies found very low positive scores for the staffing dimension. The staffing dimension suggests that the number of employees getting the job done is very low and that work schedules are adequate to provide excellent patient care. Staffing is one of the factors studied that have not been shown to be predictors of patient safety.31 This may be due to a lack of equipment and facilities that meet achievable standards, an inadequate time structure, a heavy workload, and hospital staff shortage. It is interesting to note that all items within the composites measuring staffing and non-punitive responses to errors were rated as areas in need of improvement in the participating hospitals.33 Staffing levels indicate that there are not enough staff to handle the workload and that work hours are appropriate to provide the best possible care to patients.28,30,35
Openness of communication was one of the areas in need of improvement, with a low score of only 26.5% positive responses. Because openness of communication is highly correlated with feedback and communication about errors, it could help eliminate threats to patient safety. Communication problems have been identified as major contributing factors to adverse events.7 In line with our findings, there are many studies that have identified very low scores for communication openness.28,31,35 A published systematic review showed that openness in communication had the lowest positive score (29.7%) and the highest positives score (68%).35
The composite of hand-offs and transitions in the hospital refers to staff perceptions of the importance of hand-offs within hospital departments, as most information about patient care is transferred during shift changes.23 One study showed that hospital hand-offs and transitions were viewed positively by only 14.2%, which is similar to our findings.30 The lowest scores were found for the dimensions of hand-offs and transitions in the hospital (49.7%), staffing (36.8%), and non-punitive response to errors (24.3%).33,37 The highest positives responses for the hospital hand-offs and transitions domain were (69%), while the lowest positive response was (0).32
As the results of current study indicate, focusing on specific cultural composites when planning and training healthcare workers is essential to improving certain types of patient hand-offs and transactions. For example, in large hospitals or complex medical systems, it is increasingly challenging to plan proper hand-offs. In the current study, hospital hand-offs and transitions play a significant role in job dissatisfaction and employee’s intent to leave. Over half of the respondents stated that “Important patient care information is often lost during shift changes.” As for overall perception of safety, only 10% agreed that procedures and systems do a good job of preventing errors. A previous study conducted at the United States Department of Health and Human Services asserted that a strong communication culture only partially ensures the effective sharing and transmission of patient information.38
The current findings show that scores for lack of proper communication were high. Less than half of the healthcare workers said they were afraid to ask questions when something did not seem right to them. The findings also concur with a study that demonstrated that work-related contacts with supervisors have significant direct effects on healthcare workers’ turnover intentions.39
Staff Outcomes: Job Satisfaction
In the current study, job satisfaction was reported by 84%, meaning employees liked their jobs. Healthcare workers who had more than 11 years of work experience indicated that working here was like belonging to a large family. Other composites that were associated with a higher likelihood of feeling like part of a large family were: Supervisor/manager expectations and actions to promote safety, teamwork within hospital units, and hospital management support for patient safety. Predictors of job satisfaction were described as internal and external. The external factors such as pay, working hours and working conditions are listed as key factors in job dissatisfaction. The internal factors (eg recognition of accomplishments) lead to high job satisfaction.40 Researchers have found that job dissatisfaction decreases with higher levels of education.41,42
Staff Outcomes: Intention to Leave
The current study found that more than two-thirds (78.3%) of respondents said they had no intention of leaving. The PSC composites that were significantly associated with lower intention to leave were: Supervisor/manager expectations and actions to promote safety, teamwork within hospital units, staffing, and hospital management support for patient safety. The study results showed that the odds of leaving the workplace were 3.35 higher when the number of hand-offs and transitions in the hospital increased by one unit. Few studies have examined the relationship between PSC, job satisfaction, and intention to leave the hospital. A study conducted in Saudi Arabia found that a transformational leadership style increased nurses’ job satisfaction and intention to stay in the profession.37 A study found a negative relationship between patient safety domains such as “safety climate, teamwork, safe behavior and the variables of time in the facility, time in the institution” and intention to leave the profession. This finding suggests that there is a negative correlation between the time spent working in the facility and the institution, and the intention to leave the profession, and scores in these domains.21
Of all participants, 21.7% intended to leave their jobs. Among the study participants who had the intention to leave, the percentage is lower than some earlier reports: (55.2%) among doctors,43 (47%) among general practitioners,44 (42.3%) among primary care physicians.45 The factors associated with this high turnover intention among general practitioners were lower income level, lower job, and heavy workload.44 Workload and stress were also found among nurses and doctors.17,44 In the current study, female healthcare workers, and the 31–40 age group indicated they were more likely to leave their jobs. A similar age group was reported as a predictor of intention to leave the workplace in a study in the region. Other reported factors included low job satisfaction, working more than 40 hours per week, and conflict with supervisors.43 However, job dissatisfaction has been reported to be a key factor in turnover.46–48
Findings at the bivariate and multi-variate levels suggest several areas of improvement within the composites that may increase job satisfaction and perception of patient safety and decrease intention to leave. Studies conducted among nurses have examined the relationship between job satisfaction and quality of patient care. Job satisfaction predicts intention to stay or leave an organization.49–51 Hospital hand-offs and transitions play a leading role in high healthcare staff turnover and low job satisfaction. Studies have reported several factors associated with nurses’ intention to stay, such as work environment,52–54 and working in a public hospital.55
Job satisfaction is a key predictor of employee turnover. The relationship has been extensively studied among nurses and described as inversely related to intention to quit.49,56,57 Factors such as job satisfaction, job security, pay, work hours, and work stress play a critical role in employee turnover.58 However, job satisfaction is one of the most important predictors59, and the likelihood of leaving the job is higher among dissatisfied employees.60,61 Studies have summarized the inverse relationship between job satisfaction and turnover intentions.48,59,62,63
Staff turnover is one of the key factors leading to shortages in the healthcare workforce. The relationship between job satisfaction and turnover has been well studied among nurses.15 The turnover rate decreases as job satisfaction increases.64 Turnover intention or intention to leave is a prominent predictor of actual turnover.43 Stress has been reported to have a significant impact on turnover;65 and to have a negative relationship with job satisfaction41 and a strong relationship with intention to leave.66,67 A systematic review conducted in Saudi Arabia had reported factors affecting PSC; situational, local working conditions, organizational, external, and general factors.68
Strengths and Limitations
Among the strenghths first, the sample size was sufficient to draw the conclusions and increased the statistical power.
Second, because this study included all healthcare workers, it provides a more comprehensive picture of the staff working in a tertiary care hospital. Third, we investigated two outcomes associated with PSC: intention to leave and job satisfaction. Finally, because the responses were anonymous, we anticipate they were not biased. The current study had several limitations. The recall bias could not be excluded due to self-reporting. We have not analyzed the possible influence of the types of professions on intention to leave and job satisfaction. We were unable to analyze the difference between respondents and those who refrained from participation due to a lack of data. Lastly, results cannot be generalized since the participants were enrolled from one hospital only.
Conclusion
The patient safety culture scores were highest in “organizational learning” and “teamwork”. However, low scores were observed in the domains of “openness in communication”, “staffing”, “non-punitive response to error”, and “handoffs and transitions” domains, which warrant improvement. Only a few healthcare workers had expressed a desire to leave their jobs. The study findings support the notion that, in addition to age and gender, the dimensions of safety culture, including the staffing, hospital management support, hospital handover, and transition, can have a signification impact on job satisfaction and intention to leave among healthcare workers. The dimensions of patient safety culture mentioned above are closely related to healthcare workers’ job satisfaction, intention to leave, and can play a significant role in developing administrative policies and interventions to improve staff outcomes.
Data Sharing Statement
The dataset supporting the conclusions of this article are not available publicly due to the institutional rules and regulations, but are available from the first author on a reasonable request.
Ethics Approval and Consent to Participate
The ethical approval was obtained by King Abdullah International Medical Research Center (KAIMRC) Institutional Review Board (IRB) with approval number (number SP15/117). All participants were adequately informed of the aims, methods, and risks of the study as well as of voluntary participation and confidentiality of the responses at the introduction of the survey. The responses were anonymous and participants’ confidentiality was maintained.
Consent for Publication
This is not applicable, as participants’ personal details were not recorded.
Acknowledgments
We would like to thank all healthcare workers participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Disclosure
The authors declare no conflicts of interest.
References
1. Wilson RM, Michel P, Olsen S, et al. Patient safety in developing countries: retrospective estimation of scale and nature of harm to patients in hospital. BMJ. 2012;344:e832. doi:10.1136/bmj.e832
2. Lee JY, Shin JH. Why do they stay? Intention to stay among registered nurses in nursing homes. Int J Environ Res Public Health. 2020;17:8485. doi:10.3390/ijerph17228485
3. Wang K-Y, Chou CC, Lai JCK. A structural model of total quality management, work values, job satisfaction and patient-safety-culture attitude among nurses. J Nurs Manag. 2019;27:225–232. doi:10.1111/jonm.12669
4. Ooshaksaraie M, Azadehdel MR, Sadowdi FJ. The relationship between nurses job satisfaction and patient safety culture in the hospitals of Rasht city. Heal Saf Work. 2016;6:91–102.
5. Najjar S, Nafouri N, Vanhaecht K, Euwema M. The relationship between patient safety culture and adverse events: a study in Palestinian hospitals. Saf Heal. 2015;1:16. doi:10.1186/s40886-015-0008-z
6. Kavanagh C. Medication governance: preventing errors and promoting patient safety. Br J Nurs. 2017;26:159–165.
7. Birk K, Pađen L, Markič M. Adverse event reporting in Slovenia: the influence of safety culture, supervisors and communication. Vojnosanit Pregl. 2016;73:714–722.
8. Beecroft PC, Dorey F, Wenten M. Turnover intention in new graduate nurses: a multivariate analysis. J Adv Nurs. 2008;62:41–52.
9. Hann M, Reeves D, Sibbald B. Relationships between job satisfaction, intentions to leave family practice and actually leaving among family physicians in England. Eur J Public Health. 2011;21:499–503.
10. Schwarzkopf D, Rüddel H, Thomas-Rüddel DO, et al. Perceived nonbeneficial treatment of patients, burnout, and intention to leave the job among ICU nurses and junior and senior physicians. Crit Care Med. 2017;45:e265–73. doi:10.1097/CCM.0000000000002081
11. Lehmann U, Dieleman M, Martineau T. Staffing remote rural areas in middle- and low-income countries: a literature review of attraction and retention. BMC Health Serv Res. 2008;8:19. doi:10.1186/1472-6963-8-19
12. Stone PW, Larson EL, Mooney-Kane C, Smolowitz J, Lin SX, Dick AW. Organizational climate and intensive care unit nurses’ intention to leave. Crit Care Med. 2006;34:1907–1912. doi:10.1097/01.CCM.0000218411.53557.29
13. Eastwood JB, Conroy RE, Naicker S, West PA, Tutt RC, Plange-Rhule J. Loss of health professionals from sub-Saharan Africa: the pivotal role of the UK. Lancet. 2005;365:1893–1900. doi:10.1016/S0140-6736(05)66623-8
14. Keane S, Lincoln M, Smith T. Retention of allied health professionals in rural New South Wales: a thematic analysis of focus group discussions. BMC Health Serv Res. 2012;12:175. doi:10.1186/1472-6963-12-175
15. Coomber B, Barriball KL. Impact of job satisfaction components on intent to leave and turnover for hospital-based nurses: a review of the research literature. Int J Nurs Stud. 2007;44:297–314. doi:10.1016/j.ijnurstu.2006.02.004
16. A universal truth: no health without a workforce third global forum on human resources for health report; 2013. Available from: https://www.who.int/workforcealliance/knowledge/resources/hrhreport2013/en/.
17. Hayes LJ, O’Brien-Pallas L, Duffield C, et al. Nurse turnover: a literature review - an update. Int J Nurs Stud. 2012;49:887–905. doi:10.1016/j.ijnurstu.2011.10.001
18. Misra-Hebert AD, Kay R, Stoller JK. A review of physician turnover: rates, causes, and consequences. Am J Med Qual Off J Am Coll Med Qual. 2004;19:56–66. doi:10.1177/106286060401900203
19. Martsolf GR, Auerbach D, Benevent R, et al. Examining the value of inpatient nurse staffing: an assessment of quality and patient care costs. Med Care. 2014;52:982–988. doi:10.1097/MLR.0000000000000248
20. Thungjaroenkul P, Cummings GG, Embleton A. The impact of nurse staffing on hospital costs and patient length of stay: a systematic review. Nurs Econ. 2007;25:255.
21. Tondo J, de Brito Guirardello E. Perception of nursing professionals on patient safety culture. Rev Bras Enferm. 2017;70:1284–1290. doi:10.1590/0034-7167-2016-0010
22. Merino-Plaza MJ, Carrera-Hueso FJ, Roca-Castelló MR, Morro-Martín MD, Martínez-Asensi A, Fikri-Benbrahim N. Relationship between job satisfaction and patient safety culture. Gac Sanit. 2018;32:352–361. doi:10.1016/j.gaceta.2017.02.009
23. Sorra J, Nieva VF. Hospital Survey on Patient Safety Culture. Agency for Healthcare Research and Quality; 2004.
24. Rockville M; Agency for Healthcare Research and Quality. Hospital survey on patient safety culture; 2013. Available from: https://www.ahrq.gov/sops/surveys/hospital/index.html.
25. Sexton JB, Helmreich RL, Neilands TB, et al. The safety attitudes questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. 2006;6:44. doi:10.1186/1472-6963-6-44
26. Kumar R, Ahmed J, Shaikh BT, Hafeez R, Hafeez A. Job satisfaction among public health professionals working in public sector: a cross sectional study from Pakistan. Hum Resour Health. 2013;11:2. doi:10.1186/1478-4491-11-2
27. Garvin DA. Building a learning organization. Harv Bus Rev. 1993;71(4):1.
28. Aboul Fotouh AM, Ismail NA, Ez Elarab HS, Wassif GO. Assessment of patient safety culture among health-care providers at a teaching hospital in Cairo, Egypt. EMHJ. 2012;18(4):372–377. doi:10.26719/2012.18.4.372
29. El-Jardali F, Jamal D, Abdallah A, Kassak K. Human resources for health planning and management in the Eastern Mediterranean region: facts, gaps and forward thinking for research and policy. Hum Resour Health. 2007;5:9. doi:10.1186/1478-4491-5-9
30. Alharbi W, Cleland J, Morrison Z. Assessment of patient safety culture in an adult oncology department in Saudi Arabia. Oman Med J. 2018;33:200–208. doi:10.5001/omj.2018.38
31. Alahmadi HA. Assessment of patient safety culture in Saudi Arabian hospitals. Qual Saf Heal Care. 2010;19:e17–e17.
32. Damayanti RA, Bachtiar A. Outcome of patient safety culture using the hospital survey on patient safety culture (HSOPSC) in Asia: a systematic review with meta analysis. Proc Int Conf Appl Sci Heal. 2019;2019:849–863.
33. El-Jardali F, Jaafar M, Dimassi H, Jamal D, Hamdan R. The current state of patient safety culture in Lebanese hospitals: a study at baseline. Int J Qual Heal Care. 2010;22:386–395. doi:10.1093/intqhc/mzq047
34. Han K, Trinkoff AM, Gurses AP. Work‐related factors, job satisfaction and intent to leave the current job among United States nurses. J Clin Nurs. 2015;24:3224–3232. doi:10.1111/jocn.12987
35. Ghahramanian A, Rezaei T, Abdullahzadeh F, Sheikhalipour Z, Dianat I. Quality of healthcare services and its relationship with patient safety culture and nurse-physician professional communication. Heal Promot Perspect. 2017;7:168. doi:10.15171/hpp.2017.30
36. Baldwin DC, Daugherty SR, Tsai R, Scotti MJ. A national survey of residents’ self-reported work hours: thinking beyond specialty. Acad Med. 2003;78:1154–1163. doi:10.1097/00001888-200311000-00018
37. Abualrub RF, Alghamdi MG. The impact of leadership styles on nurses’ satisfaction and intention to stay among Saudi nurses. J Nurs Manag. 2012;20:668–678. doi:10.1111/j.1365-2834.2011.01320.x
38. Lee S-H, Phan PH, Dorman T, Weaver SJ, Pronovost PJ. Handoffs, safety culture, and practices: evidence from the hospital survey on patient safety culture. BMC Health Serv Res. 2016;16:254. doi:10.1186/s12913-016-1502-7
39. Kim H, Lee SY. Supervisory communication, burnout, and turnover intention among social workers in health care settings. Soc Work Health Care. 2009;48:364–385.
40. Sachau DA. Resurrecting the motivation-hygiene theory: herzberg and the positive psychology movement. Hum Resour Dev Rev. 2007;6:377–393. doi:10.1177/1534484307307546
41. Yin J-CT, Yang K-PA. Nursing turnover in Taiwan: a meta-analysis of related factors. Int J Nurs Stud. 2002;39:573–581. doi:10.1016/S0020-7489(01)00018-9
42. Rambur B, Palumbo MV, McIntosh B, Mongeon J. A statewide analysis of RNs’ intention to leave their position. Nurs Outlook. 2003;51:182–188. doi:10.1016/S0029-6554(03)00115-5
43. Ali Jadoo SA, Aljunid SM, Dastan I, et al. Job satisfaction and turnover intention among Iraqi doctors - a descriptive cross-sectional multicentre study. Hum Resour Health. 2015;13:21. doi:10.1186/s12960-015-0014-6
44. Shen X, Jiang H, Xu H, et al. The global prevalence of turnover intention among general practitioners: a systematic review and meta-analysis. BMC Fam Pract. 2020;21:21. doi:10.1186/s12875-020-1095-4
45. Wen T, Zhang Y, Wang X, Tang G. Factors influencing turnover intention among primary care doctors: a cross-sectional study in Chongqing, China. Hum Resour Health. 2018;16:10. doi:10.1186/s12960-018-0274-z
46. Peters DH, Chakraborty S, Mahapatra P, Steinhardt L. Job satisfaction and motivation of health workers in public and private sectors: cross-sectional analysis from two Indian states. Hum Resour Health. 2010;8:27. doi:10.1186/1478-4491-8-27
47. Ojakaa D, Olango S, Jarvis J. Factors affecting motivation and retention of primary health care workers in three disparate regions in Kenya. Hum Resour Health. 2014;12:33. doi:10.1186/1478-4491-12-33
48. Steinmetz S, de Vries D, Tijdens K. Should I stay or should I go? The impact of working time and wages on retention in the health workforce. Hum Resour Health. 2014;12(1):23. doi:10.1186/1478-4491-12-23
49. Currie EJ, Hill RAC. What are the reasons for high turnover in nursing? A discussion of presumed causal factors and remedies. Int J Nurs Stud. 2012;49:1180–1189.
50. Tao H, Ellenbecker CH, Wang Y, Li Y. Examining perception of job satisfaction and intention to leave among ICU nurses in China. Int J Nurs Sci. 2015;2:140–148.
51. Freund A. Commitment and job satisfaction as predictors of turnover intentions among welfare workers. Adm Soc Work. 2005;29:5–21.
52. Friese CR. Nurse practice environments and outcomes: implications for oncology nursing. Oncol Nurs Forum. 2005;32:765–772.
53. Aiken LH, Clarke SP, Sloane DM, Lake ET, Cheney T. Effects of hospital care environment on patient mortality and nurse outcomes. J Nurs Adm. 2008;38:223–229.
54. El-Jardali F, Dimassi H, Jamal D, Jaafar M, Hemadeh N. Predictors and outcomes of patient safety culture in hospitals. BMC Health Serv Res. 2011;11:45. doi:10.1186/1472-6963-11-45
55. Al‐Hamdan Z, Manojlovich M, Tanima B. Jordanian nursing work environments, intent to stay, and job satisfaction. J Nurs Scholarsh. 2017;49:103–110.
56. Blaauw D, Ditlopo P, Maseko F, et al. Comparing the job satisfaction and intention to leave of different categories of health workers in Tanzania, Malawi, and South Africa. Glob Health Action. 2013;6:19287.
57. Suadicani P, Bonde JP, Olesen K, Gyntelberg F. Job satisfaction and intention to quit the job. Occup Med. 2013;63:96–102.
58. Clark A. What really matters in a job? Hedonic measurement using quit data. Labour Econ. 2001;8:223–242.
59. Shader K, Broome ME, Broome CD, West ME, Nash M. Factors influencing satisfaction and anticipated turnover for nurses in an academic medical center. J Nurs Adm. 2001;31:210–216.
60. Seston E, Hassell K, Ferguson J, Hann M. Exploring the relationship between pharmacists’ job satisfaction, intention to quit the profession, and actual quitting. Res Social Adm Pharm. 2009;5:121–132.
61. Parsons SK, Simmons WP, Penn K, Furlough M. Determinants of satisfaction and turnover among nursing assistants. The results of a statewide survey. J Gerontol Nurs. 2003;29:51–58.
62. Bonenberger M, Aikins M, Akweongo P, Wyss K. The effects of health worker motivation and job satisfaction on turnover intention in Ghana: a cross-sectional study. Hum Resour Health. 2014;12:43.
63. Liu J, Zhu B, Wu J, Mao Y. Job satisfaction, work stress, and turnover intentions among rural health workers: a cross-sectional study in 11 western provinces of China. BMC Fam Pract. 2019;20:9.
64. Cavanagh SJ, Coffin DA. Staff turnover among hospital nurses. J Adv Nurs. 1992;17:1369–1376.
65. Fang Y. Turnover propensity and its causes among Singapore nurses: an empirical study. Int J Hum Resour Manag. 2001;12:859–871.
66. Blegen MA. Nurses’ job satisfaction: a meta-analysis of related variables. Nurs Res. 1993;42:36–41.
67. Hinshaw AS, Smeltzer CH, Atwood JR. Innovative retention strategies for nursing staff. J Nurs Adm. 1987;17:8–16.
68. Albalawi A, Kidd L, Cowey E. Factors contributing to the patient safety culture in Saudi Arabia: a systematic review. BMJ Open. 2020;10:e037875–e037875.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.