")
Back to Journals » Vascular Health and Risk Management » Volume 19
Impact of Myocardial Ischemia and Revascularization by Percutaneous Coronary Intervention on Circulating Level of Soluble ST2
Authors Alkhateeb A, Mahmoud HEM, AK M , Hassan MH , Muddathir ARM, Bakry AG
Received 7 April 2023
Accepted for publication 30 June 2023
Published 6 July 2023 Volume 2023:19 Pages 411—420
DOI https://doi.org/10.2147/VHRM.S416206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Areej Alkhateeb,1 Hossam Eldin M Mahmoud,1 Mohammed AK,1 Mohammed H Hassan,2 Abdel Rahim Mahmoud Muddathir,3 Ahmed G Bakry1
1Cardiology Division of Internal Medicine Department, South Valley University Hospital, Faculty of Medicine, South Valley University, Qena, 83523, Egypt; 2Department of Medical Biochemistry, Faculty of Medicine, South Valley University, Qena, 83523, Egypt; 3Department of Hematology and Blood Transfusion, Faculty of Medical Laboratory Science, Alzaeim Alazhari University, Khartoum, Sudan
Correspondence: Abdel Rahim Mahmoud Muddathir, Department of Hematology and Blood Transfusion, Faculty of Medical Laboratory Science, Alzaeim Alazhari University, Khartoum, Sudan, Email [email protected]
Background: The prognostic role of the soluble circulating suppression of tumorigenicity 2 marker (sST2) in different cardiovascular diseases (CVD) is still under investigation. This research aimed to assess the serum levels of sST2 in the blood of individuals with ischemic heart disease and its relation to disease severity, also to examine any changes in sST2 levels following a successful percutaneous coronary intervention (PCI) in those patients.
Methods: A total of 33 ischemic patients and 30 non-ischemic controls were included. The plasma level of sST2 was measured using commercially available ELISA assay kit, at baseline and 24– 48 h after the intervention in the ischemic group.
Results: On admission, there was a significant difference between the group of acute/chronic coronary syndrome cases and controls regarding the sST2 plasma level (p < 0.001). There was an insignificant difference between the three ischemic subgroups at the baseline sST2 level (p = 0.38). The plasma sST2 level decreased significantly after PCI (from 20.70 ± 1.71 to 16.51 ± 2.43, p = 0.006). There was a modestly just significant positive correlation between the acute change in post-PCI sST2 level and the severity of ischemia as measured by the Modified Gensini Score (MGS) (r = 0.45, p = 0.05). In spite of the highly significant improvement in the coronary TIMI flow of ischemic group after PCI, there was insignificant negative correlation between the post- PCI delta change in the sST2 level and the post-PCI TIMI coronary flow grade.
Conclusion: A significantly high plasma level of sST2 in patients with myocardial ischemia and controlled cardiovascular risk factors showed an immediate reduction after successful revascularization. The high baseline level of the sST2 marker and the acute post-PCI reduction was mainly related to the severity of ischemia rather than left ventricular function.
Keywords: soluble circulating suppression of tumorigenicity 2 marker, percutaneous coronary intervention, acute/chronic coronary syndrome, severity of ischemia, modified gensini score, revascularization
Introduction
Coronary artery disease (CAD) is one of the leading causes of mortality worldwide.1,2 Therefore, the new research was focused on developing primary and secondary preventive measures to prevent cardiovascular complications and death. Despite advances in healthcare, early detection of ischemic events remains a significant challenge. Many cardiac biomarkers have high sensitivity for detecting myocardial damage, but there are limitations in interpreting the extent of myocardial tissue damage, which is an area of active research. The ST2 gene was first discovered as part of the large IL-1 gene cluster in 1989.3
Two of the four gene isoforms are most relevant for cardiovascular (CV) disease, which is IL1RL1-b or ST2L (a transmembrane ligand belonging to the interleukin-1 receptor family) and the serum-soluble form called IL1RL1-a or sST2 (a truncated receptor).2 When fibroblasts and cardiomyocytes are stretched and deformed, the ST2 gene is abundantly expressed, and ST2L becomes responsive to IL-33.2,4,5 As IL-33 has anti-remodelling features, it prevents cardiomyocyte hypertrophy and fibrosis.2,6,7 Additionally, it appears that the ST2L-IL-33 relationship results in the inhibition of the Mitogen-Activated Protein Kinase (MAPK) pathway brought on by angiotensin II or phenylephrine.5
While sST2 works as a “decoy receptor” for circulating IL-33, it can block IL-33’s positive action.2,8 As a result, many researchers have discovered that the serum sST2 level is one of the early indicators of heart failure (HF), along with a variety of biomarkers such as brain natriuretic peptide (BNP), NT-proBNP, galectin-3, procalcitonin, and growth differentiation factor 15 (GDF15), some of which can be elevated with non-cardiac conditions such as sepsis and renal failure.7,9 Moreover, two reports confirm the diagnostic and prognostic values of sST2 in patients presenting to emergency departments with chest pain and post-myocardial infarction along with other biomarkers, especially NT-proBNP, which consistently improves risk stratification.10,11
In addition, other studies have shown that increased sST2 concentrations (above 35 ng/mL) significantly increase the risk of cardiovascular events, including death, advancing left ventricular (LV) failure, and hospitalization for heart failure.12 Because of sST2’s low biological variability, Wu et al recommend serial monitoring of its level as one of the favourable criteria that are not available in other biomarkers, such as BNP or NT-proBNP.13 Some researches were conducted to find better markers for CAD and HF diseases that are more accurate and comprehensive. Moreover, the ability of the biomarkers to detect the prognosis of ischemia and the outcome of different management techniques adds advantages to some biomarkers over others.14 As a result, this study aimed to identify the role of plasma sST2 as an early marker of myocardial ischemia and a predictor of the severity of ischemia in the presence of cardiac remodelling and left ventricular dysfunction.
Methods
Study Design
This study included two designs:
- Case-control design (baseline comparison between ischemic heart disease and non-ischemic heart disease-control groups)
- Prospective observation study design (follow-up of only ischemic heart disease group)
Inclusion and Exclusion Criteria
In this study, 33 patients aged 40 or older with risk factors for ischemic heart disease (IHD) and acute and chronic coronary syndrome symptoms were enrolled. Routine diagnostic investigations were performed, including an electrocardiogram, cardiac markers, and transthoracic echocardiography (2D-TTE). Acute changes in left ventricular function were assessed using conventional two-dimensional transthoracic echocardiography (2D-TTE), and the severity of ischemia during revascularization was assessed using the Modified Gensini Score. Blood samples for the plasma ST2 level were taken at presentation and 24–48 h after revascularization (angioplasty with stent placement). Additionally, the plasma ST2 levels were obtained from 30 control subjects aged 40 or older with risk factors for IHD but without any ischemic symptoms and normal results on all routine diagnostic investigations. The study group of ischemic patients who underwent coronary angiography with stent placement was divided into three subgroups: group 1: single-vessel disease; group 2: two-vessel disease; and group 3: multivessel disease including left main disease. The Modified Gensini Score (MGS) was measured according to previous research on scores of coronary artery severity.15,16
The following exclusion criteria were used in the study to avoid any systemic diseases that could lead to high plasma levels of sST2: left ventricular dysfunction with ejection fraction (EF) less than 50%, and arrhythmias including atrial fibrillation (AF), valvular or structural heart diseases, uncontrolled hypertension (HTN) or diabetes mellitus (DM), pulmonary diseases (such as chronic obstructive pulmonary disease, obstructive sleep apnea, pulmonary embolism, bronchial asthma, pulmonary hypertension, and respiratory failure), obesity, systemic infection or inflammation, and renal dysfunction.17 Informed consent was obtained from each participant, and the study protocol adhered to the ethical guidelines of the 1975 Declaration of Helsinki. The study protocol was previously approved by South Valley University’s Ethics Committee on Research on Humans (Ethical approval code: SVU-MED-MBC004-4-22-10-469).
Transthoracic Echocardiography
All patients underwent conventional transthoracic echocardiography with standard two-dimensional, M-mode, and Doppler views using an iE33 Philips Healthcare ultrasound machine (Netherlands) equipped with a two-dimensional cardiac probe S5–1 (1–5 MHz). The TTE views were analyzed offline to establish ventricular dimensions and functions and exclude any cases with valvular, structural, and myocardial disorders or significant left ventricular systolic dysfunction (EF < 50%). Additionally, all studies were electrocardiogram (ECG)-gated.
Coronary Angioplasty with Stent Placement and Patients’ Selection
Patients with acute and chronic coronary syndromes were evaluated by the heart team for revascularization options, including optimal medical therapy (OMT), coronary artery bypass graft (CABG), or percutaneous coronary intervention (PCI), according to the 2018 European Society of Cardiology/European Association for Cardio-Thoracic Surgery (ESC/EACTS) guidelines on myocardial revascularization.18 Diagnostic coronary angiography was performed under local anaesthesia with fluoroscopic guidance in angina cases where non-invasive testing was insufficient to provide a suitable diagnosis. A decision for percutaneous coronary intervention was made by two independent cardiologists who were unaware of the research area and any significant lesion with angiographic luminal stenosis of 50% or more of the artery diameter. Selinger’s technique used the right femoral artery puncture for all cases. Selective left and right coronary angiography in multiple views using Judkins left, and right 4F catheters were used, respectively. At the same time, the MGS was used to determine the severity of coronary artery stenosis from angiograms. As mentioned in previous research, the total score of the MGS was divided into two sections. The first section was the percentage of coronary artery stenosis graded from 1 to 4 (grade 1: 1%–49% decrease in the lumen diameter, grade 2: 50%–74% stenosis, grade 3: 75%–99% stenosis, and grade 4: 100% occlusion).16,17 The second section of the score was the factor for each artery according to its significance, as follows: (20) left anterior descending (LAD), (20) left circumflex (LCX), (20) right coronary artery (RCA), (10) main diagonal branch (D1), (10) obtuse marginal branch (OM1), (10) main posterior descending branch (PDA), (5) left main (LM), and (5) first septal perforator (S1).16 The proportion of each stenotic vessel was multiplied by the factor of that vessel. In the case of the lateral wall being supplied mainly by a large obtuse marginal or intermediate vessel, the factor of this vessel would be the same as the LCX, which was 20, and the non-dominant or small LCX would have a small factor of 10.19,20 After an intervention, all hemostatic measures were taken for the patient’s safety.
Biochemical Studies
A total of 5 mL of venous blood samples were obtained from each participant at baseline and 24–72 h after the intervention in the ischemic group using serum separator gel tubes. The samples were allowed to clot at 37 °C for half an hour, then centrifuged at 3500 rpm for 10 min. The separated sera were aliquoted into 1 mL cryotubes and stored at −80 °C until measurement of sST2 using a commercially available ELISA kit supplied by Elabscience, USA (Catalog number E-EL-H6082). The sandwich-ELISA principle was used, with a sensitivity of 0.19 ng/mL, a detection range of 0.31–20 ng/mL, and a coefficient of variation of ˂ 10%. The assays were performed using a microplate ELISA reader (EMR 500, USA) according to the manufacturer’s protocol.
Follow-Up
All patients received the recommended medical treatment, including dual antiplatelet therapy, according to the 2018 ESC/EACTS guidelines on myocardial revascularization.17 Post-PCI follow-up withdrawal of the plasma sST2 and 2-D TTE to assess biventricular remodelling and function was performed by independent, experienced echocardiographers who were blinded to the patient classification.
Statistical Analysis
Statistical analysis was carried out using IBM SPSS version 24. The Shapiro–Wilk test was used to quantitatively test the normality of the data after it had been visually evaluated using histograms and a common Q-Q plot. The mean ± standard error (SEM) was used to express continuous normal data. A comparison of the same group’s data was performed before and after the intervention using a paired t-test and between the two groups using an independent t-test. A one-way ANOVA was used when there were more than two different groups. The difference between values before and after an intervention is known as the delta change (Δ). The Pearson correlation coefficient was used to evaluate the correlation. The authors are fully responsible for the integrity of the data and have full access to it. Significance was defined as p-value ≤ 0.05 and highly significant at p < 0.01.
Results
The demographic and baseline clinical, biochemical, and angiographic data of the patients are presented in (Table 1). There were no statistically significant differences in the frequency of body mass index or controlled risk factors such as hypertension or diabetes between the two groups. However, the ischemic group had higher levels of aging (p < 0.001) and a higher proportion of males (p = 0.005) compared to the control group. Additionally, as measured by EF, left ventricular function was within the normal range up to the lower limit of normality in the ischemic group compared to the control group (EF of ischemic group: from 52.88 ± 1.08% to 59.86 ± 0.67%, p = 0.001).
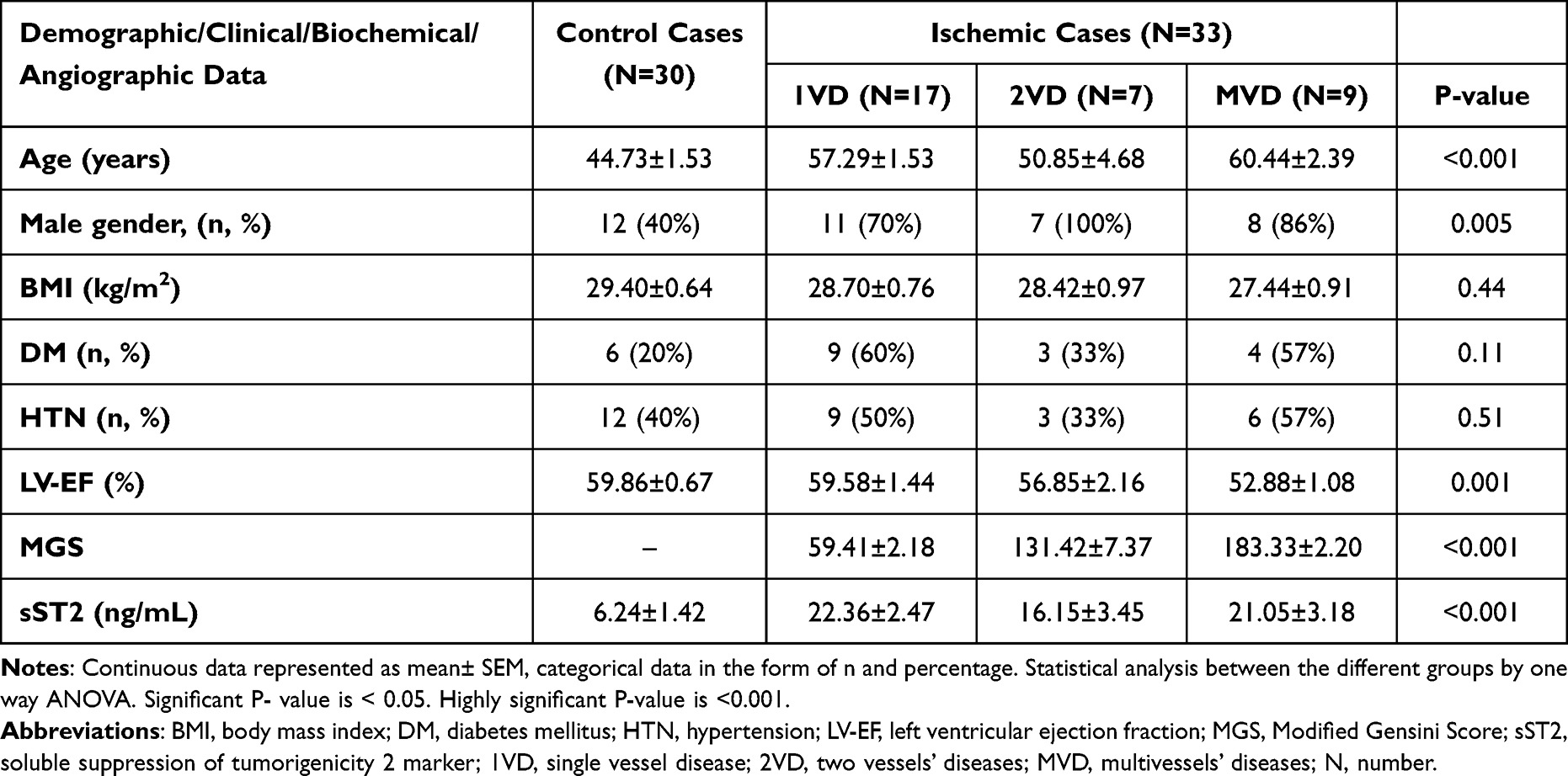 |
Table 1 The Baseline Demographic, Clinical, Biochemical, and Angiographic Characteristics of the Ischemic versus Control Groups |
Angiographic results and Severity of Coronary Artery Stenosis
Out of 33 ischemic patients, 17 (51.5%) had a single diseased vessel, 7 (21.2%) had two diseased vessels, and 9 (27.2%) had multivessel disease. The difference between the single-vessel disease, two-vessel disease, and multivessel disease groups in the mean MGS was highly significant (59.41±2.18, 131.42±7.37, 183.33±2.20, respectively, P < 0.001) as shown in (Table 1).
Baseline Comparison of the Plasma sST2 Levels Between the Study Groups and Controls
The study results indicated a significant increase in the plasma level of sST2 in ischemic patients compared to controls. The ischemic patients had a mean plasma level of sST2 of 20.70 ± 1.71 ng/mL, while the controls had a mean plasma level of sST2 of 6.24 ± 1.42 ng/mL (Figure 1). However, there was no significant difference in the baseline ST2 level between the subgroups of ischemic patients with single-vessel disease, two-vessel disease, and multivessel disease (p = 0.38). This suggests that the degree of vessel disease does not have a significant impact on the baseline level of sST2 in ischemic patients.
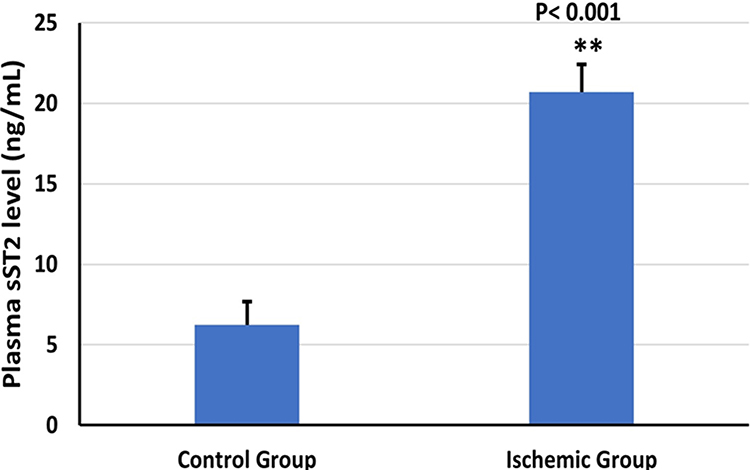 |
Figure 1 The comparative difference in the baseline plasma level of sST2 between ischemic and control groups. Abbreviation: sST2, soluble suppression of tumorigenicity 2 marker. Notes: Highly significant growth in the level of sST2 in the ischemic patients more than control ones. Reported data were expressed as mean values ±SEM. **Highly significant P-value (< 0.001). Statistical analysis between the different 2 groups was done by independent 2-tailed t test. |
Acute Changes in Plasma Level of sST2 and TIMI Coronary Flow After PCI
After 24–48 h of percutaneous coronary artery intervention, there was a significant reduction in the plasma level of sST2 (P = 0.006). The level was 20.70 ± 1.71 ng/mL before the intervention and decreased to 16.52 ± 1.84 ng/mL afterward, as shown in (Figure 2). Moreover, there was a highly significant improvement in the coronary TIMI flow after PCI (P = 0.0001).
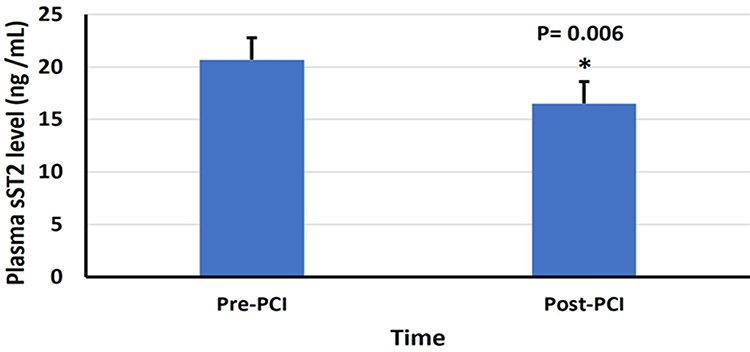 |
Figure 2 Acute changes in the plasma level of sST2 after PCI in the ischemic group. Abbreviations: sST2, soluble suppression of tumorigenicity 2 marker; Pre, before; Post, after; PCI, percutaneous coronary intervention. Notes: Significant reduction in sST2 plasma level after 24–72 hours of intervention (from 20.70±1.71 ng/mL to 16.52±1.84 ng/mL, P= 0.006). *Significant difference between the 2 stages of the ischemic patients. Reported data was expressed as mean values ±SEM. Significant P-value < 0.05. Statistical analysis was done by paired 2-tailed t-test of the same group of patients. |
The Relation of Acute Changes in the Plasma Level of sST2 to the Possible Confounding Risk Factors: MGS, Aging, Left Ventricular Function, Controlled DM and HTN
A linear correlation was performed between the percent change in the ischemic group’s plasma level of sST2 after intervention (∆) and the mean of MGS, LV-EF, aging, and the presence of controlled cardiovascular risks factors such as diabetes mellitus (DM) and hypertension (HTN). The correlation between the acute post-PCI delta change in the plasma level of sST2 (∆) and the mean value of MGS is modest and slightly significant (r = 0.45, p = 0.05). However, there were weak, insignificant negative correlations between the acute post-PCI delta change in the sST2 level (∆) and LV-EF, age, and controlled DM values (r = −0.25, −0.006, −0.13; p = 0.98, 0.30, 0.59, respectively) (Table 2). A weak, insignificant positive correlation was found between the sST2 (∆) level and the presence of a controlled HTN, as shown in Table 2. These results indicated that the acute change in sST2 plasma level after the intervention is mainly affected by the degree of ischemia and revascularization rather than the differences in the presence of controlled risk factors such as DM, HTN, advanced aging, or changes in LV-EF within the normal range.
 |
Table 2 Correlation Table Between the Acute Delta Changes in the Plasma sST2 Level to the MGS, Aging, LV-EF, Controlled DM and HTN |
Furthermore, in spite of the highly significant improvement in the coronary TIMI flow of ischemic group after PCI and the significant correlation between the post- PCI delta change in the sST2 level and the severity of coronary stenosis by using MGS, there was insignificant negative correlation between the post- PCI delta change in the sST2 level and the post-PCI TIMI coronary flow grade (r = −0.18, p = 0.46). Which means that the more reduction in the sST2 level post-PCI was associated with more improvement in the TIMI flow grade.
Discussion
In recent clinical practice guideline updates, the American College of Cardiology/American Heart Association (ACC/AHA) has recommended the measurement of sST2 for risk stratification and prognostic value in heart failure (HF) patients with acute decompensated heart failure (ADHF) and chronic HF.7 Since 2013, there have been two main research groups with opposing views on the relationship of ST2 to cardiovascular disease (CVD). One group has suggested the use of sST2 as a predictor of HF hospitalization and death and 30-day adverse events after myocardial infarction (MI), while the other group has found that despite the prognostic role of sST2 in ischemic heart disease being demonstrated, its pathogenesis still requires further studies and, in some cases, the ability of sST2 to predict HF is limited.7,21
In this study, the researchers reported a statistically significant higher level of sST2 in ischemic patients compared to controls with the same controlled risk factors, including diabetes mellitus (DM) and hypertension (HTN), despite the significant difference in gender between the two groups. In agree with the results of some prior publications, a high sST2 level, significantly more than 28.4 ng/mL, was observed in a study group with a high percentage of men and hypertension.22 Moreover, the Framingham Heart Study demonstrated that male gender and advanced age were related to greater sST2 concentrations (p = 0.0001, 0.004, respectively) after controlling for CAD, HF, AF, diabetes, HTN, obesity, valvular disease, LV systolic dysfunction, and pulmonary and renal dysfunction.17 In other studies, higher sST2 levels could also result from different CVDs such as HF, HTN, diabetes, AF, and valvular heart disease. Some non-cardiac conditions, including inflammation, asthma, fibroproliferative disorders, rheumatoid arthritis, autoimmune conditions, sepsis, and trauma, have been linked to high sST2 levels.3,23
Therefore, all patients with left ventricular dysfunction (EF < 50%), any arrhythmia including AF, valvular or structural heart diseases, uncontrolled hypertension or diabetes, pulmonary diseases (chronic obstructive pulmonary disease, obstructive sleep apnea, bronchial asthma, pulmonary embolism, pulmonary hypertension, and respiratory failure), obesity, systemic infection or inflammation, and renal dysfunction were excluded from the current study to avoid misleading results.
The most interesting finding in the current study was the significant reduction in the plasma level of sST2 after revascularization through PCI (p < 0.001). The same result was observed by Eggers et al as a part of the Global Use of Strategies to Open Occluded Arteries (GUSTO) IV research (a randomized trial of adjunctive treatment of NSTEMI with GIIbIIIa), when 403 of the 7800 patients with ischemic symptoms and either a positive cardiac troponin test or 0.5-mm ST-segment depression in ECG were identified in the serial ST2 monitoring.24 Blood samples were collected 24, 48, and 72 h after randomization. The maximum level of ST2 was found 6 to 17 h following the onset of symptoms, which is consistent with data from patients with STEMI. By 24–48 h after the onset of symptoms, the levels had subsequently dropped to a stable level of around 20 ng/mL.25 In addition, when patients with diabetes had critical limb ischemia, Caporali et al observed that one of the tumor necrosis factor (TNF)-alpha receptor families (neurotrophin p75 receptor) was excessively released in postischemic neovascularization.25 This receptor can enhance the sST2 gene transcription and, in turn, result in the prevention of complete revascularization by endothelial cells.
Contrary to some previous publications, the authors found a positive, modest, and statistically significant correlation between the mean value of MGS and the percentage of sST2 level reduction after revascularization by PCI (r = 0.45, p = 0.05). This meant that the most severe ischemia was associated with the highest plasma level of sST2, which showed a marked drop after successful PCI. Therefore, sST2 can be considered one of the primary indicators of the severity of cardiomyocyte ischemia and recovery. There was a negative, weak, and statistically insignificant correlation between the acute post-PCI change in sST2 plasma level and LV-EF, age, and DM values. In contrast to Dieplinger et al’s study, which assessed the serum level of sST2 in an ischemic study group, 229 patients had the insignificant single-vessel disease (17%), 323 had the significant single-vessel disease (24%), 300 had the significant two-vessel disease (22%), 493 had the significant multivessel disease (37%), and 129 patients had HF; it was found that sST2 level was not linked to the severity of CAD (r = 0.038, p = 0.159).26
The study by Weir et al is in line with the present study, which identified a positive correlation between endocardial, epicardial, and microvascular obstruction on the one hand and sST2 serum concentrations on the other in 100 patients with acute MI.27 Similar results were observed in the CLARITY-TIMI 28 trial in patients with STEMI, where ascending quartiles of serum sST2 were not associated with chronic LV wall stress, aging, hypertension, prior MI, or HF.28 In the post-MI stage, there were differences in the acute temporal changes in serum sST2 and NT-proBNP.22 Most patients had serial monitoring of the serum sST2 for one to four days following MI symptoms and at the time of the angiogram. While the mean NT-proBNP increased by an average of 386 pg/mL, approximately six times as much as sST2, with a minor average drop in sST2 of 0.009 ng/mL after four days of symptoms.22,28
There was a significant three-fold elevation in the sST2 level in ischemic patients with severe coronary artery stenosis than in less severe cases, which was graded by angiographic TIMI flow and TIMI myocardial perfusion.22 At the same time, the natriuretic peptide marker was more closely associated with LVEF than sST2. These results implied that plasma sST2 measures the amount of damaged tissue and the accompanying necrosis and inflammatory processes, while the NT-proBNP level is related to cardiac mechanical stress.22 In contrast to NT-proBNP, ST2 levels at baseline were more accurate at predicting death or heart failure than levels four days later (ie, at angiography).22
In light of the above results, we attribute the positive correlation between post-PCI sST2 acute changes and MGS to the fact that several studies conducted in the lab and on animals have shown how the IL-33/ST2 signaling cascade contributes to the inflammatory process and cellular damage during ischemia.6 Furthermore, the role of IL-33 as a regulator of cardiomyocyte hypertrophy, fibrosis, apoptosis, plaque stability, and cardiac dysfunction following MI has a crucial clinical impact on post-ischemia prognosis, including hospitalization, death, and the best time for revascularization.6
Conclusion
Ischemic patients with controlled risk factors had significantly higher plasma levels of sST2 compared to patients with the same risk factors but without cardiac ischemia. The significant reduction in sST2 plasma levels began as early as one-day post-PCI, regardless of the patient’s age or changes in LVEF within the normal range. After successful revascularization by PCI, there was a positive correlation between the severity of coronary artery stenosis and the acute post-PCI reduction in sST2, suggesting that sST2 is a highly sensitive early indicator of the degree of ischemia and the effectiveness of revascularization.
Limitations and Recommendations
Although this study was based on the opinions of expert cardiologists to avoid the risk of error in assessing the CA stenosis extent, guided by MGS, the risk of subjective measurement of CAD severity is high. We measured all changes in sST2 plasma levels during the acute post-PCI stage, and a more extended follow-up period will likely verify the current findings for prognostic values. The study main limitation is the small sample size, so to further ensure the absence of confounding factors, we recommend increasing the sample size and recruiting individuals from various ages, genders, and LVEF groups. This is because changes in left ventricular diastolic and systolic function, as determined by advanced monitoring techniques, may influence the sST2 level.
Abbreviations
2D, Two-Dimensional; ACC/AHA, American College of Cardiology/American Heart Association; ADHF, Acute Decompensated Heart Failure; AF, Atrial Fibrillation; BNP, Brain Natriuretic Peptide; CA, Coronary Artery; CABG, Coronary Artery Bypass Graft; CAD, Coronary Artery Disease; Chromosome 2q12, Queue (long arm); CV, Cardiovascular; D1, Main Diagonal Branch; DM, Diabetes Mellitus; ECG, Electrocardiogram; EF, Ejection Fraction; ELISA, Enzyme-Linked Immunoassay; EMR, Enzyme-Linked Immunoassay Microplate Reader; ESC/EACTS, European Society of Cardiology/European Association for Cardio-Thoracic Surgery Guidelines; F, French; GIIbIIIa, Glycoprotein IIb/IIIa; GDF15, Growth Differentiation Factor 15; GUSTO, Global Use of Strategies to Open Occluded Arteries; HF, Heart Failure; HTN, Hypertension; IHD, Ischemic Heart Disease; IL, Interleukin; IL1RL1, Interleukin 1 Receptor Ligand 1; LAD, Left Anterior Descending; LCX, Left Circumflex; LM, Left Main; LV-EF, Left Ventricle-Ejection Fraction; MAPK, Mitogen-Activated Protein Kinase; MGS, Modified Gensini Score; MI, Myocardial Infarction; ng/mL, Nanograms per milliliter; NSTEMI, Non-ST-Elevation Myocardial Infarction; NT-proBNP, N-Terminal pro B-type Natriuretic Peptide; OM1, Obtuse Marginal Branch (OM1); PCI, Percutaneous Coronary Intervention; PDA, Posterior Descending Branch; Pg/mL, Picograms per milliliter; RCA, Right Coronary Artery; S1, First Septal Perforator; sST2, Soluble Circulating Suppression of Tumorigenicity 2; ST2L, Suppression of Tumorigenicity 2 Transmembrane Ligand; STEMI, ST-Elevation Myocardial Infarction; TNF, Tumor Necrosis Factor; TIMI, Thrombolysis in Myocardial Infarction; TTE, Transthoracic Echocardiography.
Data Sharing Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Ethical Statement
Informed consent was obtained from each participant. The study protocol was previously approved by South Valley University’s Ethics Committee for research on humans (Ethical approval code: SVU-MED-MBC004-4-22-10-469).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Ahern RM, Lozano R, Naghavi M, Foreman K, Gakidou E, Murray CJ. Improving the public health utility of global cardiovascular mortality data: the rise of ischemic heart disease. Popul Health Metr. 2011;9(1):8. doi:10.1186/1478-7954-9-8
2. Ciccone MM, Cortese F, Gesualdo M, et al. A novel cardiac bio-marker: ST2: a review. Molecules. 2013;18(12):15314–15328. doi:10.3390/molecules181215314
3. Kakkar R, Lee RT. The IL-33/ST2 pathway: therapeutic target and novel biomarker. Nat Rev Drug Discov. 2008;7(10):827–840. doi:10.1038/nrd2660
4. Weinberg EO, Shimpo M, De Keulenaer GW, et al. Expression and regulation of ST2, an interleukin-1 receptor family member, in cardiomyocytes and myocardial infarction. Circulation. 2002;106(23):2961–2966. doi:10.1161/01.cir.0000038705.69871.d9
5. Sanada S, Hakuno D, Higgins LJ, Schreiter ER, McKenzie AN, Lee RT. IL-33 and ST2 comprise a critical biomechanically induced and cardioprotective signaling system. J Clin Invest. 2007;117(6):1538–1549. doi:10.1172/JCI30634
6. Seki K, Sanada S, Kudinova AY, et al. Interleukin-33 prevents apoptosis and improves survival after experimental myocardial infarction through ST2 signaling. Circ Heart Fail. 2009;2(6):684–691. doi:10.1161/CIRCHEARTFAILURE.109.873240
7. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147–e239. doi:10.1016/j.jacc.2013.05.019
8. Sweet MJ, Leung BP, Kang D, et al. A novel pathway regulating lipopolysaccharide-induced shock by ST2/T1 via inhibition of Toll-like receptor 4 expression. J Immunol. 2001;166(11):6633–6639. doi:10.4049/jimmunol.166.11.6633
9. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. doi:10.1093/eurheartj/ehw128
10. Brown AM, Wu AHB, Clopton P, Robey JL, Hollander JE. ST2 in emergency department chest pain patients with potential acute coronary syndromes. Ann Emerg Med. 2007;50(2):153–158.e1. doi:10.1016/j.annemergmed.2007.02.015
11. Aldous SJ, Richards AM, Troughton R, Than M. ST2 has diagnostic and prognostic utility for all-cause mortality and heart failure in patients presenting to the emergency department with chest pain. J Card Fail. 2012;18(4):304–310. doi:10.1016/j.cardfail.2012.01.008
12. Januzzi JL, Pascual-Figal D, Daniels LB. ST2 testing for chronic heart failure therapy monitoring: the International ST2 Consensus Panel. Am J Cardiol. 2015;115(7 Suppl):70B–5B. doi:10.1016/j.amjcard.2015.01.044
13. Wu AH, Wians F, Jaffe A. Biological variation of galectin-3 and soluble ST2 for chronic heart failure: implication on interpretation of test results. Am Heart J. 2013;165(6):995–999. doi:10.1016/j.ahj.2013.02.029
14. Alkhateeb A, Abd Elrady NS, Ali AMS, Hashim AKA. Impact of diabetes mellitus on acute and short term left ventricular longitudinal systolic strain recovery after percutaneous coronary intervention in ischemic hypertensive patients. SVU Int J Med Sci. 2023;6(2):152–159. doi:10.21608/svuijm.2023.202042.1556
15. Gensini GG. Coronary Arteriography / by Goffredo G. Gensini Mount Kisco, N.Y: Futura Pub. Co; 1975.
16. Golabchi A, Sadeghi M, Sanei H, et al. Can timi risk score predict angiographic involvement in patients with st-elevation myocardial infarction? ARYA Atheroscler. 2010;6(2):69–73.
17. Coglianese EE, Larson MG, Vasan RS, et al. Distribution and clinical correlates of the interleukin receptor family member soluble ST2 in the Framingham Heart Study. Clin Chem. 2012;58(12):1673–1681. doi:10.1373/clinchem.2012.192153
18. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization [published correction appears in. Eur Heart J. 2019;40(37):3096. doi:10.1093/eurheartj/ehy394
19. Sullivan DR, Marwick TH, Freedman SB. A new method of scoring coronary angiograms to reflect extent of coronary atherosclerosis and improve correlation with major risk factors. Am Heart J. 1990;119(6):1262–1267. doi:10.1016/s0002-8703(05)80173-5
20. Adams MR, Nakagomi A, Keech A, et al. Carotid intima-media thickness is only weakly correlated with the extent and severity of coronary artery disease. Circulation. 1995;92(8):2127–2134. doi:10.1161/01.cir.92.8.2127
21. Zhang T, Xu C, Zhao R, Cao Z. Diagnostic Value of sST2 in Cardiovascular Diseases: a Systematic Review and Meta-Analysis. Front Cardiovasc Med. 2021;8:697837. doi:10.3389/fcvm.2021.697837
22. Richards AM, Di Somma S, Mueller T. ST2 in stable and unstable ischemic heart diseases. Am J Cardiol. 2015;115(7 Suppl):48B–58B. doi:10.1016/j.amjcard.2015.01.041
23. Crnko S, Printezi MI, Jansen TPJ, et al. Prognostic biomarker soluble ST2 exhibits diurnal variation in chronic heart failure patients. ESC Heart Fail. 2020;7(3):1224–1233. doi:10.1002/ehf2.12673
24. Eggers KM, Armstrong PW, Califf RM, et al. ST2 and mortality in non-ST-segment elevation acute coronary syndrome. Am Heart J. 2010;159(5):788–794. doi:10.1016/j.ahj.2010.02.022
25. Shimpo M, Morrow DA, Weinberg EO, et al. Serum levels of the interleukin-1 receptor family member ST2 predict mortality and clinical outcome in acute myocardial infarction. Circulation. 2004;109(18):2186–2190. doi:10.1161/01.CIR.0000127958.21003.5A
26. Dieplinger B, Egger M, Haltmayer M, et al. Increased soluble ST2 predicts long-term mortality in patients with stable coronary artery disease: results from the Ludwigshafen risk and cardiovascular health study. Clin Chem. 2014;60(3):530–540. doi:10.1373/clinchem.2013.209858
27. Weir RA, Miller AM, Murphy GE, et al. Serum soluble ST2: a potential novel mediator in left ventricular and infarct remodeling after acute myocardial infarction. J Am Coll Cardiol. 2010;55(3):243–250. doi:10.1016/j.jacc.2009.08.047
28. Sabatine MS, Morrow DA, Higgins LJ, et al. Complementary roles for biomarkers of biomechanical strain ST2 and N-terminal prohormone B-type natriuretic peptide in patients with ST-elevation myocardial infarction. Circulation. 2008;117(15):1936–1944. doi:10.1161/CIRCULATIONAHA.107.728022
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.