Back to Journals » Clinical Ophthalmology » Volume 17
Impact of First Healthcare Provider on Acanthamoeba Keratitis Course: How to Overcome Poor Prognosis in Acanthamoeba Keratitis Treatment? A Single Tertiary Center, Observational Study
Authors Przybek-Skrzypecka J ![]() , Walkden A
, Walkden A ![]() , Brahma A, Chidambaram J, Carley FM
, Brahma A, Chidambaram J, Carley FM
Received 6 September 2023
Accepted for publication 7 December 2023
Published 21 December 2023 Volume 2023:17 Pages 3975—3982
DOI https://doi.org/10.2147/OPTH.S438990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Joanna Przybek-Skrzypecka,1,2 Andrew Walkden,3,4 Arun Brahma,3 Jaya Chidambaram,5 Fiona M Carley3,6
1Department of Ophthalmology, Medical University of Warsaw, Warsaw, Poland; 2SPKSO Ophthalmic University Hospital, Warsaw, Poland; 3Cornea Department, Manchester Royal Eye Hospital, Manchester University NHS Foundation, Manchester, UK; 4School of Biological Science, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK; 5Division of Pharmacy and Optometry, School of Health Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK; 6School of Medical Sciences, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK
Correspondence: Joanna Przybek-Skrzypecka, Department of Ophthalmology, Medical University of Warsaw, Marszałkowska 24/26, Warsaw, 00-576, Poland, Tel +48 22 511 62 37, Email [email protected]; [email protected]
Background: To assess the difference in course and final visual outcome of Acanthamoeba keratitis (AK) patients based on the first healthcare provider (HCP) seen.
Methods: Retrospective observational cohort study of AK patients admitted to the Manchester Royal Eye Hospital between 2003 and 2017. HCPs were grouped (Group 1: Optometrists, Opticians; Group 2: General Practitioners (GPs); Group 3: Ophthalmologists) and the data analyzed on demographics, risk factors, clinical history, clinical features, and Acanthamoeba subspecies.
Results: Forty-one patients with unilateral culture-proven AK were included. Median time to consultation with first HCP was 7 days (IQR 4– 14 days), while mean time to the correct diagnosis of AK was 15 days (IQR 7– 29 days). Patients saw an optician, optometrist or ophthalmologists significantly earlier than GPs (median 4 days, vs 15 or 5 days, respectively, p = 0.04). Bacterial keratitis was the most common initial clinical diagnosis (43%). The shortest time to making the AK diagnosis (median 11 days) and the highest rate of initiating AK treatment started at the first visit (38%) were both in the ophthalmologists’ group. No significant differences were observed in initial and final visual acuity between HCP groups (p = 0.36).
Conclusion: AK patients often seek ocular help earlier from optometrists and opticians than medical doctors. Final clinical outcomes did not significantly differ based on the first HCP seen, but ophthalmologists were more likely to make the diagnosis of AK and initiate anti-amoebal therapy faster than other HCPs. Greater education and collaboration between ophthalmologists and other HCPs to increase awareness of AK are needed.
Keywords: keratitis, Acanthamoeba, corneal ulcer, diagnosis, healthcare providers
Introduction
Acanthamoeba keratitis (AK) is one of the most severe ocular infections with poor treatment outcomes.1 Nearly half of all patients with AK will be severely visually impaired (defined as final visual acuity of 20/80 or less).2 Several risk factors for Acanthamoeba keratitis have been described, with contact lenses being the most prominent, followed by corneal trauma and abrasion with other foreign bodies.3–5 Additionally, there are well-known risk factors for poor final visual outcomes including delayed diagnosis, prior steroid treatment, epithelial defect on presentation and inappropriate primary treatment that does not target Acanthamoeba sp. This supports the promotion of early recognition as a crucial factor for both being able to initiate the correct treatment and also for restoring vision.6–11
Considering the non-specific signs and symptoms that can present in the early stages of the disease, prompt diagnosis remains challenging.12 There is no single 100% sensitive and specific test for AK, but corneal scraping, microbiological testing, PCR, and in vivo confocal microscopy (IVCM) are the mainstay of the diagnostic process.13,14 Incorrect and late diagnoses often result in visual loss and significant healthcare costs due to the burden of treatment and clinical appointments as well as surgical intervention.15
This condition has many masquerades and a delayed diagnosis makes it harder to treat. Delayed diagnosis is an undesirable issue in whole medicine. Several factors for late diagnosis include human error, late referrals, no or limited access to ancillary tests and their expense.16,17 Human error is a most prominent issue in rare disorders with non-specific symptoms, like AK.16 Up to 16–40% of patients with AK require surgical intervention, evisceration included, also due to late or incorrect diagnosis.18,19 However, contrary to many other specialties within medicine, ocular health is managed by both doctors (Ophthalmologists and General Practitioners) and other Allied Healthcare Professionals: optometrists, orthoptists, or opticians. Thus, potentially patients suffering from keratitis might be primarily assessed by a non-ophthalmologist, who may not necessarily have AK as one of their diagnostic differentials. The question raised is whether this model of ophthalmic care impacts the management of patients with AK.
Therefore, our aim was to evaluate whether the success of treatment, defined by the visual outcome, was dependent on the type of healthcare provider to first assess the patient (GP, opticians, optometrists and ophthalmologists-residents and consultants).
Methods
This study was approved by the Institutional Review Board of Manchester Royal Eye Hospital, UK. Due to the retrospective nature of this study, and that it employed the use of anonymous unidentifiable retrospective patient data, the requirement for patient consent for use of this data was deemed to not be required by the IRB. This study adhered to the tenets of the Declaration of Helsinki.
Study Participants
This was a retrospective analysis of 46 adults with culture-positive AK presenting to Manchester Royal Eye Hospital (MREH), UK between 2003 and 2017. Corneal ulcers with mixed microbial pathology were excluded from the study. Forty-one patients reached the criteria for analysis, due to full availability of clinical information (see below).
Data Collection
Information on the following variables was collected: patient demographics, past medical history, past ocular history, history of general medical diseases, risk factors for keratitis (contact lens (CL) wear, type of CL, duration of daily wear, history of ocular trauma, soil contamination, CL misuse: sleeping in CL, taking bath in CL, overuse of CL). CL “overuse” was defined as either sleeping, swimming/bathing in any water type whilst wearing CLs, cleaning CL with tap water or prolonged use of CL.
We also analyzed time from the first symptom to final diagnosis of AK, time from the first symptom to visit any healthcare provider (HCP: general practitioner, optician, optometrist, ophthalmology resident, ophthalmology consultant), type of initial diagnosis (Acanthamoeba, bacterial, viral, fungal, mixed keratitis), time from the first symptom to correct AK treatment implementation, initial treatment (Anti-amoebal, antibiotics, antiviral, antifungal, steroids, mixed treatment – at least two groups of medications implemented prior to correct AK treatment).
Clinical symptoms for which data were collected were as follows: pain (quantified in 1–10 VAS scale and which class of analgesics were required), redness, photophobia, blurred vision, foreign body sensation. Clinical signs from the slit-lamp examination were evaluated including the presence of epitheliopathy, epithelial defect, perineuritis, infiltrate (ring and/or multiple), corneal melting or perforation.
Data were also collected on the following: uncorrected and best-corrected visual acuity upon initial presentation, lowest uncorrected visual acuity recorded during the course of the disease, final visual acuity outcome (assessed at the time of the final treatment visit when treatment was completed) measured as log of the minimum angle of resolution (logMAR) units.
The results of in-vivo confocal microscopy (IVCM) examination for the presence or absence of Acanthamoeba cysts in the IVCM images and HSV swab results were also recorded where available.
Microbiological Diagnosis
The corneal scrapes were obtained and tested at the Manchester Royal Eye Hospital. Standard microbiological testing was used (ie, corneal scrapes obtained and directly placed on to blood agar, chocolate agar, Sabouraud agar, and non-nutrient agar plates overlaid with Escherichia coli). Acanthamoeba subspecies were evaluated based on the morphology of cysts in microbiological examination (by experienced microbiologist: MA).
Statistical Methods
Analysis was carried out using R statistical software, version 4.0.5. Data are presented with n (% of group) for nominal variables and as mean ± SD or median (with interquartile range, IQR) for continuous variables, depending on distribution normality. Verification of normality was made with Shapiro–Wilk test and using skewness and kurtosis values. Equity of variances was assessed using Levene’s test. Group comparison was made with Fisher's exact test for nominal variables, and with ANOVA or Kruskal–Wallis test for continuous variables. Tukey post-hoc test was used in significant results of ANOVA analysis. All tests were based on α = 0.05.
Results
The study included a total of 41 patients (21 females and 20 males) with culture proven, unilateral Acanthamoeba keratitis. Information on the first HCP seen was available for 33 patients: 6 patients (18.2%) visited an optician or optometrist, 5 patients (15.2%) saw their GP, 14 patients (42.4%) saw the ophthalmology resident/fellow in the MREH Eye Emergency Clinic and the remaining 8 patients (24.2%) saw an ophthalmology consultant initially. In further analyses, the last 2 groups were combined and analyzed together. There were no significant differences in demographics between patients seen in the different first healthcare provider groups, Table 1.
 |
Table 1 Demographics of Study Participants |
The mean time from symptom onset to seeing the first HCP was significantly different between groups (p = 0.042). Post-hoc analysis confirmed that it was longer in Group 2 (GPs) with median delay of 14 days (IQR 12–14 days) than for the time to seeing allied HCPs (optometrists, opticians) which was 4.5 days (IQR 3.25–7.25 days) or ophthalmologists, 5 days (IQR 4–9 days). Initial treatment was also significantly related to the type of first HCP seen (p = 0.039; Table 2). AK diagnosis was made at the first visit in 8 patients (38%) in Group 3 (ophthalmologists), while in the Allied HCP group, no patients were diagnosed with AK (0%), and in the GP group, only 1 patient (20%) was appropriately diagnosed with AK at the first visit. In the allied HCP group, antibiotic eyedrop treatment was the most frequently initiated treatment (50% of cases); for GPs mixed treatment (at least one topical antibiotic plus antiviral or antifungal drug) was prescribed in 60% of cases while for ophthalmologists the treatment initiated was either a topical anti-amoebal (38.1%) or an antibiotic (38.1%). Direct appropriate AK treatment was implemented in 0 (0%), 1 (20%) and 8 (38%) of patients for group 1, group 2 and group 3, respectively. Patients who were initially seen by GPs had a longer time from symptom onset to the correct diagnosis of AK being made (medial 17 days), and also 60% (n = 3) had tried sequentially more than 2 therapies before the correct anti-amoebal therapy was commenced. Initial VA and final VA were not significantly different between groups (Table 2). BCVA at the last visit was also compared between the four groups (dividing ophthalmologists into residents and consultants) with no statistical difference observed (p = 0.53). Time to reach the final resolution of the AK was approximately a median of 6 months in patients initially seen by the ophthalmologist or the GP and median of 10 months in patients initially seen by the optometrist/optician group (p = 0.067).
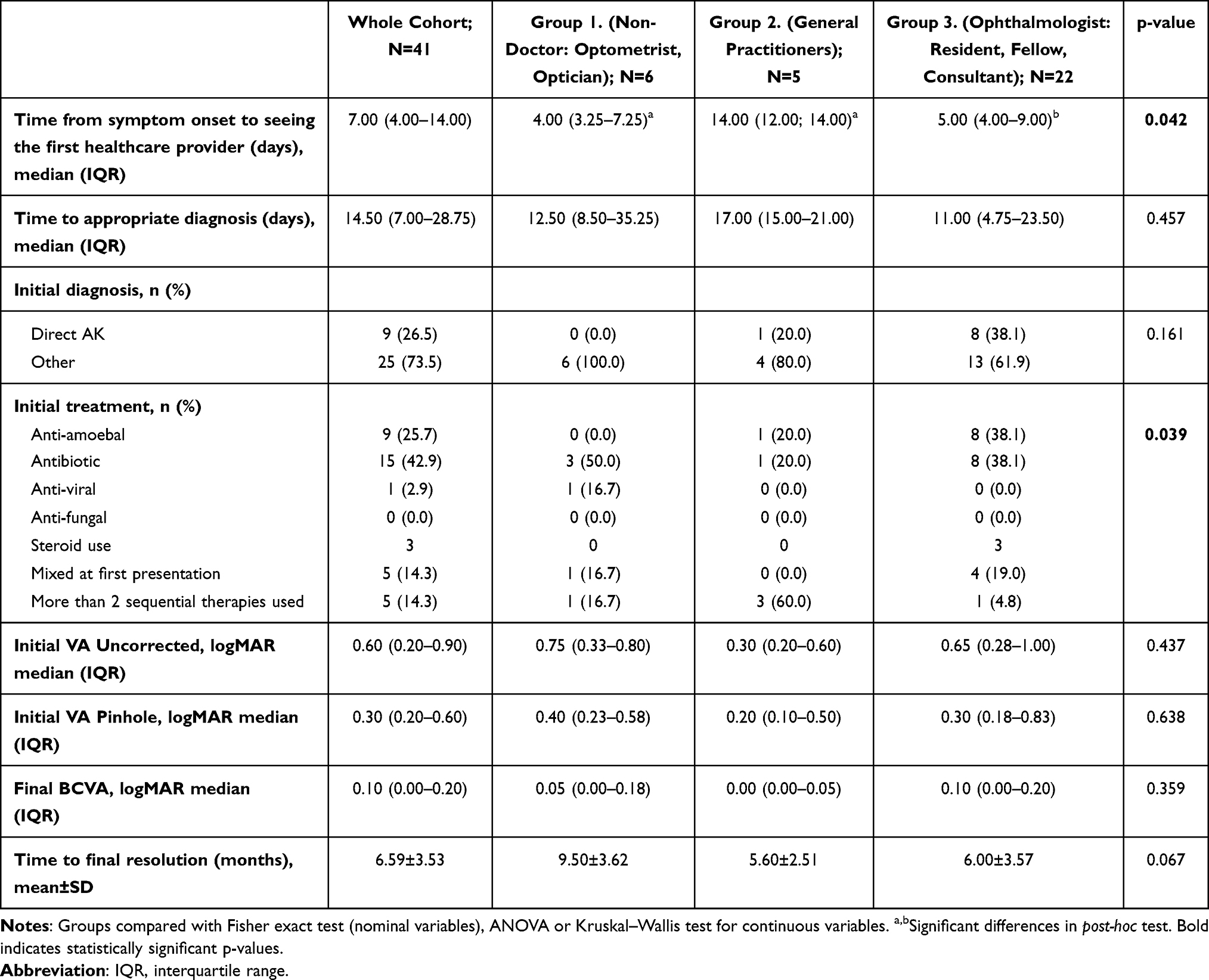 |
Table 2 Initial Diagnosis and Treatment Divided in the Healthcare Providers Groups (Group 1: Non-Doctors, Group 2: General Practitioners, Group 3: Ophthalmologists) |
Among clinical characteristics and risk factors, the only significant difference was observed for CL type (p = 0.031; Table 3). In each group, the majority of patients wore monthly contact lenses. However, a greater proportion of patients seen initially by ophthalmologists were monthly CL-wearers (90%) compared with patients first seen by allied HCPs or GPs (60.0 and 66.7% respectively). Table 3 summarizes risk factors and clinical characteristics of the patients in the subgroups.
 |
Table 3 Clinical Characteristics and Risk Factors for Acanthamoeba Keratitis Cohort |
Acute red eye (77%), eye pain (86%) and photophobia (87%) were the most common initial symptoms bringing the patient to a healthcare provider. Patients with painful AK were more likely to be initially seen by GPs or ophthalmologists rather than by allied HCPs. Almost half of the patients (47%) first seen by ophthalmologists required at least two oral analgesics to alleviate their eye pain.
Discussion
In this cohort of patients with culture-proven unilateral Acanthamoeba keratitis, the average time from symptom onset to the first visit at any healthcare provider was 7 days. The majority of patients decided to visit an ophthalmologist directly, while a smaller proportion opted to be initially evaluated by an optometrist or optician or general practitioner. Whereas the average time to reach the appropriate diagnosis of AK was 15 days for the whole cohort, it was shortest for patients initially seen by an ophthalmologist. In terms of the initial time delay until the first visit to any healthcare provider, the type of HCP seen did not appear to cause any significant difference in the final BCVA. To the best of our knowledge, this is the first report evaluating the impact of multiple healthcare specialists on the course and final visual outcome of AK.
Early diagnosis is widely discussed in the literature as a critical factor for better outcome and is an indicator for better final visual acuity and lower corneal transplant rate.9,19 In this study, the mean time for initiation of appropriate AK treatment was 2 weeks from symptom onset which contributed to the favorable outcomes observed. There is no frank definition of “early” diagnosis, and this is represented differently within the literature, ranging from 14 to 18 days.6,20 Another way to differentiate the “early” stages from “late” stages of AK is to utilize clinical signs of infection that are thought to be more likely to occur in the late stage of disease such as ring infiltrate, total epithelial loss and limbitis.10,13 In AK patients, early diagnosis also reduces the risk of corneal tissue damage, and the incidence of surgical interventions, in particular corneal transplants (both therapeutic and optical), further improving the outcome.21–23 In addition, the transplant failure rate in these cases exceeds that in many other indications for keratoplasty, and so those patients undergoing a corneal transplant are often finally left with a poor visual outcome, due to early failure, rejection or disease recurrence.23
Misdiagnosis in the etiology of infective keratitis may prolong treatment time, cause significant morbidity or lead to visual loss. Acanthamoeba sp., as one of the least common pathogens in infective keratitis, is often inappropriately diagnosed as a bacterial, herpetic or fungal infection.24–28 Almost half of our cohort was primarily treated with topical antibiotics, which is in accordance with previous studies.26,27 However, we showed significantly fewer misdiagnoses of herpetic keratitis than cited in the literature (3% vs 37%).27 Of note, HSV/VZV keratitis shares some clinical features with AK.11,29 Considering the 3–20 times higher prevalence of HSV versus Acanthamoeba keratitis, AK seems to be often missed in the differential diagnosis. The results of our study underline that perineuritis and dendritic-like ulceration in a CL-wearer should raise concern of AK in the first instance.27,29 A high proportion of patients were detected to have perineuritis by the ophthalmologists at MREH at the initial visit which aided in the correct initial diagnosis of AK. This was particularly pleasing to see since the Corneal Unit at MREH has done much to promote education on diagnostic features, such as this, of AK over recent years, especially within the Eye emergency center – using the mantra “beware the dendrite in a contact lens wearer”.
Lack of availability of microbiological and PCR testing services is another limitation for accurate diagnosis and therefore optimal prognosis in AK patients.25,30 The literature shows that apart from GPs’ offices and allied healthcare professionals, 15–20% of ophthalmology practices lack the resources to perform corneal scrapes for microbiology, let alone equipment for IVCM and PCR testing.31–33 Furthermore, more recent literature has shown the value of IVCM in significantly increasing the sensitivity/specificity of AK diagnosis compared to standard microbiology of corneal scrapes.14,34
The favourable outcomes in this study highlight the value of prompt referral to the tertiary center, which has the availability of a wide variety of additional tests and the presence of highly educated and experienced cornea specialists, which overall contributes to a better prognosis. Thus, considering the burden on the patient and the healthcare system of misdiagnosis of AK, non-ophthalmologists involved in first-line eye care for patients should consider the possibility of referring patients with suspected AK to the tertiary ophthalmological center earlier.
This study highlights a key issue to overcoming poor prognosis in AK patients: healthcare providers’ education and collaboration. Even though we perceive AK as an orphan disease, our awareness should be raised by the rising tide of shortsightedness worldwide, followed by the soaring number of contact-lens-wearers and finally a globally higher incidence of AK.10,35,36 Given that AK is a cause of potential medical negligence due to late diagnosis resulting in low visual acuity, all allied healthcare professionals do need to be aware of the potential diagnosis of AK and its predisposing risk factors – this will aid them in prompt referral to tertiary centers. Our results indicate that CL usage, and bathing or sleeping in CLs, followed by pain and/or redness in the affected eye should also raise suspicion of AK. There is a need for education to be incorporated into continuing professional development curricula for optometrists and GPs. Apart from national and international guidelines on corneal ulcer management, our study shows the need for and potential value of local teaching to aid in the recognition of AK on signs and symptoms for early diagnosis.37,38
This study has some limitations. Firstly, the number of patients included is relatively low. However, this is in line with the low corneal scrape positivity rate that is known in AK and also that AK is an orphan disease in our group.34 Secondly, the subgroups are not equal in numbers, but it reflects the trends that the CL-wearer with a red, painful eye may choose to see an ophthalmologist, eg, in the Eye Emergency Center, directly for the first visit. Additionally, our study has shown that keratitis patients do initially visit the GP when in pain. Further studies are needed to follow the patient journey at the GP and other allied healthcare providers in order to develop education for these HCPs on diagnosis of microbial keratitis and the benefits of early referral to the ophthalmologist. Lastly, our cohort presents with relatively good initial visual acuity, significantly better than presenting VA reported in AK the literature. There is also a very low incidence of implementing corticosteroids prior to diagnosis in this study. This might be attributed to a well-educated net of the healthcare specialists in the UK. However, we believe our study findings may pave the way for cross-disciplinary guidelines for proper management of suspected Acanthamoeba keratitis.
Funding
There is no funding to report.
Disclosure
Dr Jaya Chidambaram report is a salaried employee (work unrelated to article content) of Roche Pharmaceuticals, outside the submitted work. Authors declare no other conflicts of interest in this work.
References
1. Niederkorn JY. The biology of Acanthamoeba keratitis. Exp Eye Res. 2021;202:108365. doi:10.1016/j.exer.2020.108365
2. Carnt N, Robaei D, Minassian DC, et al. Acanthamoeba keratitis in 194 patients: risk factors for bad outcomes and severe inflammatory complications. Br J Ophthalmol. 2018;102(10):1431–1435. doi:10.1136/bjophthalmol-2017-310806
3. Lim CH, Carnt NA, Farook M, et al. Risk factors for contact lens-related microbial keratitis in Singapore. Eye. 2016;30(3):447–455. doi:10.1038/eye.2015.250
4. Brown AC, Ross J, Jones DB, et al. Risk factors for acanthamoeba keratitis-a multistate case-control study, 2008–2011. Eye Contact Lens. 2018;44(1):S173–S178. doi:10.1097/ICL.0000000000000365
5. Raghavan A, Baidwal S, Venkatapathy N, et al. The acanthamoeba-fungal keratitis study. Am J Ophthalmol. 2019;201:31–36. doi:10.1016/j.ajo.2019.01.024
6. Claerhout I, Goegebuer A, Van Den Broecke C, et al. Delay in diagnosis and outcome of Acanthamoeba keratitis. Graefes Arch Clin Exp Ophthalmol. 2004;242(8):648–653. doi:10.1007/s00417-003-0805-7
7. Bacon AS, Dart JKG, Ficker LA, et al. Acanthamoeba keratitis. The value of early diagnosis. Ophthalmology. 1993;100(8):1238–1243. doi:10.1016/S0161-6420(93)31499-5
8. Tu EY, Joslin CE. Recent outbreaks of atypical contact lens-related keratitis: what have we learned? Am J Ophthalmol. 2010;150(5):602–608 e2. doi:10.1016/j.ajo.2010.06.045
9. Tu EY, Joslin CE, Sugar J, et al. Prognostic factors affecting visual outcome in Acanthamoeba keratitis. Ophthalmology. 2008;115(11):1998–2003. doi:10.1016/j.ophtha.2008.04.038
10. Varacalli G, Di Zazzo A, Mori T, et al. Challenges in acanthamoeba keratitis: a review. J Clin Med. 2021;10(5):942. doi:10.3390/jcm10050942
11. Robaei D, Carnt N, Minassian DC, et al. The impact of topical corticosteroid use before diagnosis on the outcome of Acanthamoeba keratitis. Ophthalmology. 2014;121(7):1383–1388. doi:10.1016/j.ophtha.2014.01.031
12. Lee MJ, Srikumaran D, Zafar S, et al. Case series: delayed diagnoses of Acanthamoeba keratitis. Am J Ophthalmol Case Rep. 2020;19:100778. doi:10.1016/j.ajoc.2020.100778
13. Dart JK, Saw VP, Kilvington S. Acanthamoeba keratitis: diagnosis and treatment update 2009. Am J Ophthalmol. 2009;148(4):487–499 e2.
14. Chidambaram JD, Prajna NV, Larke NL, et al. Prospective study of the diagnostic accuracy of the in vivo laser scanning confocal microscope for severe microbial keratitis. Ophthalmology. 2016;123(11):2285–2293. doi:10.1016/j.ophtha.2016.07.009
15. Parfitt A, Boxell E, Amoaku WM, et al. Patient-reported reasons for delay in diagnosis of age-related macular degeneration: a national survey. BMJ Open Ophthalmol. 2019;4(1):e000276. doi:10.1136/bmjophth-2019-000276
16. Singh H, Schiff GD, Graber ML, et al. The global burden of diagnostic errors in primary care. BMJ Qual Saf. 2017;26(6):484–494. doi:10.1136/bmjqs-2016-005401
17. Makary MA, Daniel M. Medical error-the third leading cause of death in the US. BMJ. 2016;353:i2139. doi:10.1136/bmj.i2139
18. Radford CF, Lehmann OJ, Dart JK. Acanthamoeba keratitis: multicentre survey in England 1992–6. National acanthamoeba keratitis study group. Br J Ophthalmol. 1998;82(12):1387–1392. doi:10.1136/bjo.82.12.1387
19. Robaei D, Carnt N, Minassian DC, et al. Therapeutic and optical keratoplasty in the management of Acanthamoeba keratitis: risk factors, outcomes, and summary of the literature. Ophthalmology. 2015;122(1):17–24. doi:10.1016/j.ophtha.2014.07.052
20. List W, Glatz W, Riedl R, et al. Evaluation of Acanthamoeba keratitis cases in a tertiary medical care centre over 21 years. Sci Rep. 2021;11(1):1036. doi:10.1038/s41598-020-80222-3
21. Chen WL, Wu C-Y, Hu F-R, et al. Therapeutic penetrating keratoplasty for microbial keratitis in Taiwan from 1987 to 2001. Am J Ophthalmol. 2004;137(4):736–743. doi:10.1016/j.ajo.2003.11.010
22. Szentmary N, Daas L, Shi L, et al. Acanthamoeba keratitis - Clinical signs, differential diagnosis and treatment. J Curr Ophthalmol. 2019;31(1):16–23. doi:10.1016/j.joco.2018.09.008
23. Di Zazzo A, Varacalli G, De Gregorio C, et al. Therapeutic corneal transplantation in acanthamoeba keratitis: penetrating versus lamellar keratoplasty. Cornea. 2022;41(3):396–401. doi:10.1097/ICO.0000000000002880
24. Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite. 2015;22:10. doi:10.1051/parasite/2015010
25. Shah YS, Stroh IG, Zafar S, et al. Delayed diagnoses of Acanthamoeba keratitis at a tertiary care medical centre. Acta Ophthalmol. 2021;99(8):916–921. doi:10.1111/aos.14792
26. Hollhumer R, Keay L, Watson SL. Acanthamoeba keratitis in Australia: demographics, associated factors, presentation and outcomes: a 15-year case review. Eye. 2020;34(4):725–732. doi:10.1038/s41433-019-0589-6
27. Kowalski RP, Nayyar SV, Romanowski EG, et al. The prevalence of bacteria, fungi, viruses, and acanthamoeba from 3004 cases of keratitis, endophthalmitis, and conjunctivitis. Eye Contact Lens. 2020;46(5):265–268. doi:10.1097/ICL.0000000000000642
28. Daas L, Szentmáry N, Eppig T, et al. Das Deutsche Akanthamobenkeratitis- Register. Erste Ergebnisse einer multizentrischen Erhebung [The German Acanthamoeba keratitis register: initial results of a multicenter study]. Ophthalmologe. 2015;112(9):752–763. German. doi:10.1007/s00347-014-3225-7
29. Sheha H, Tighe S, Cheng AMS, et al. A stepping stone in treating dendritic keratitis. Am J Ophthalmol Case Rep. 2017;7:55–58. doi:10.1016/j.ajoc.2017.06.002
30. Carnt N, Stapleton F. Strategies for the prevention of contact lens-related Acanthamoeba keratitis: a review. Ophthalmic Physiol Opt. 2016;36(2):77–92. doi:10.1111/opo.12271
31. Park J, Lee KM, Zhou H, et al. Community practice patterns for bacterial corneal ulcer evaluation and treatment. Eye Contact Lens. 2015;41(1):12–18. doi:10.1097/ICL.0000000000000059
32. McLeod SD, DeBacker CM, Viana MA. Differential care of corneal ulcers in the community based on apparent severity. Ophthalmology. 1996;103(3):479–484. doi:10.1016/S0161-6420(96)30668-4
33. Zimmerman AB, Nixon AD, Rueff EM. Contact lens associated microbial keratitis: practical considerations for the optometrist. Clin Optom. 2016;8:1–12. doi:10.2147/OPTO.S66424
34. Hoffman JJ, Dart JKG, De SK, et al. Comparison of culture, confocal microscopy and PCR in routine hospital use for microbial keratitis diagnosis. Eye. 2022;36(11):2172–2178. doi:10.1038/s41433-021-01812-7
35. Chen M, Wu A, Zhang L, et al. The increasing prevalence of myopia and high myopia among high school students in Fenghua city, eastern China: a 15-year population-based survey. BMC Ophthalmol. 2018;18(1):159. doi:10.1186/s12886-018-0829-8
36. Morgan P, Efron N. Global contact lens prescribing 2000–2020. Clin Exp Optom. 2022;3(105):298–312. doi:10.1080/08164622.2022.2033604
37. Ung L, Wang Y, Vangel M, et al. Validation of a comprehensive clinical algorithm for the assessment and treatment of microbial keratitis. Am J Ophthalmol. 2020;214:97–109. doi:10.1016/j.ajo.2019.12.019
38. Contact lens associated infiltrative keratitis: clinical management guideline. Version 7; 2022. Available from: https://www.college-optometrists.org/clinical-guidance/clinical-management-guidelines/keratitis_cl-associatedinfiltrative.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.