Back to Journals » Cancer Management and Research » Volume 18

Impact of Evolving Antiemetic Prophylaxis on Chemotherapy-Induced Nausea and Vomiting (CINV): A Five-Year Comparative Study in Sichuan, China (2018–2023)
Authors Xiong W, Zhang W ![]() , Zhao Q, Zheng Y, Xie K, Miao J, Chen L, Li T, Cao W, Zhu D, Huang M, Li C, Wang Y, Gui Y, Li Q, Cao C, Yang Y, Du C, Gao Y, Zhou Y, Zhang H, Le X, Chen P, Jiang M, Li P, Yang J, Wang Y, Zhu J, He L
, Zhao Q, Zheng Y, Xie K, Miao J, Chen L, Li T, Cao W, Zhu D, Huang M, Li C, Wang Y, Gui Y, Li Q, Cao C, Yang Y, Du C, Gao Y, Zhou Y, Zhang H, Le X, Chen P, Jiang M, Li P, Yang J, Wang Y, Zhu J, He L
Received 3 December 2025
Accepted for publication 9 May 2026
Published 22 May 2026 Volume 2026:18 579784
DOI https://doi.org/10.2147/CMAR.S579784
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bilikere Dwarakanath
Weijie Xiong,1,* Weiwei Zhang,1,* Quande Zhao,2,* Yuzhu Zheng,3,* Ke Xie,4,* Jidong Miao,5 Li Chen,6 Ting Li,7 Wei Cao,8 De Zhu,9 Mengjun Huang,10 Cheng Li,11 Youhua Wang,12 Yan Gui,13 Qingcong Li,14 Chun Cao,15 Yunxiao Yang,16 Chi Du,17 Yan Gao,18 Yangang Zhou,19 Huiling Zhang,20 Xiaoyan Le,21 Ping Chen,22 Ming Jiang,23 Peng Li,24 Jinping Yang,25 Yang Wang,26 Jiang Zhu,27 Lang He1
1Department of Oncology, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), Cancer Prevention and Treatment Institute of Chengdu, Chengdu, Sichuan Province, People’s Republic of China; 2Department of Oncology, Langzhong People’s Hospital, Nanchong, Sichuan Province, People’s Republic of China; 3Department of Oncology, The Third People’s Hospital of Chengdu, Chengdu, Sichuan Province, People’s Republic of China; 4Department of oncology, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, Sichuan Province, People’s Republic of China; 5Department of Oncology, The Fourth People’s Hospital of Zigong, Zigong, Sichuan Province, People’s Republic of China; 6Department of Oncology, Wusheng People’s hospital, Guang’an, Sichuan Province, People’s Republic of China; 7Department of Oncology, The Second People’s Hospital of Yibin, Yibin, Sichuan Province, People’s Republic of China; 8Department of Oncology, the People’s Hospital of Jianyang City, Chengdu, Sichuan Province, People’s Republic of China; 9Department of Oncology, Bazhong Central hospital, Bazhong, Sichuan Province, People’s Republic of China; 10Department of Oncology, Du Jiang Yan Medical Center, Chengdu, Sichuan Province, People’s Republic of China; 11Department of Oncology, Guang’an People’s Hospital, Guang’an, Sichuan Province, People’s Republic of China; 12Department of Oncology, Gulin People’s hospital, Luzhou, People’s Republic of China; 13Department of Oncology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan Province, People’s Republic of China; 14Department of Oncology, Ya’an People’s Hospital, Chengdu, Sichuan Province, People’s Republic of China; 15Department of Oncology, Zigong First People’s Hospital, Zigong, Sichuan Province, People’s Republic of China; 16Department of Oncology, The Affiliated Hospital of Panzhihua University, Panzhihua, Sichuan, People’s Republic of China; 17Department of Oncology, The Hospital of Zizhou, Neijiang, Sichuan Province, People’s Republic of China; 18Department of Oncology, Pidu District People’s Hospital, Chengdu, Sichuan Province, People’s Republic of China; 19Department of Oncology, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan Province, People’s Republic of China; 20Department of Oncology, Ziyang Central Hospital, Chengdu, Sichuan Province, People’s Republic of China; 21Department of Oncology, Chengdu Shi Wenjiang Qu Renmin Yiyuan, Chengdu, Sichuan Province, People’s Republic of China; 22Department of Oncology, Chengdu Seventh People’s Hospital, Chengdu, Sichuan Province, People’s Republic of China; 23Head & Neck Oncology Ward, Cancer Center, West China Hospital of Sichuan University, Chengdu, Sichuan Province, People’s Republic of China; 24Department of Oncology, Dayi People’s Hospital, Chengdu, Sichuan Province, People’s Republic of China; 25Department of Oncology, People’s Hospital of Guangyuan, Chengdu, Sichuan Province, People’s Republic of China; 26Department of Oncology, China Aviation Industry Chengdu 363 Hospital, Chengdu, Sichuan Province, People’s Republic of China; 27Department of Thoracic Oncology, West China Hospital of Sichuan University, Chengdu, Sichuan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiang Zhu, Department of Thoracic Oncology, West China Hospital of Sichuan University, Chengdu, Sichuan Province, People’s Republic of China, Email [email protected] Lang He, Department of Oncology, Chengdu Fifth People’s Hospital (The Second Clinical Medical College, Affiliated Fifth People’s Hospital of Chengdu University of Traditional Chinese Medicine), Chengdu, Sichuan province, People’s Republic of China, Email [email protected]
Background: A baseline study conducted in 2018 revealed suboptimal guideline adherence and high chemotherapy-induced nausea and vomiting (CINV) burden in Sichuan, China. Since then, concerted efforts have been made to enhance CINV management through guideline promotion and physician education. This study aimed to evaluate temporal changes in CINV incidence and antiemetic prophylaxis patterns by comparing 2023 real-world data with the 2018 baseline.
Methods: In this prospective, multicenter study, we enrolled 1985 cancer patients receiving moderately or highly emetogenic chemotherapy (MEC/HEC) across Sichuan in 2023. We employed methodologies consistent with the baseline study to ensure direct comparability. Primary endpoints were the overall, acute, and delayed CINV incidence. Secondary endpoints included complete control (CC) rates and antiemetic regimen adherence.
Results: Compared with the 2018 baseline, significant improvements were observed in 2023. The overall CINV incidence decreased from 82.97% to 57.3% (P < 0.001). Acute CINV decreased from 55.3% to 43.9%, and delayed CINV showed the most substantial decline from 62.3% to 30.4% (P < 0.001 for both). For patients receiving HEC, CC rates in the overall, acute, and delayed phases increased from 30.1% to 58.4%, from 52.8% to 64.1%, and from 60.6% to 75.6%, respectively. For MEC patients, CC rates in the overall, acute, and delayed phases increased from 32.1% to 68.5%, from 47.5% to 83.4%, and from 55.4% to 91.9%, respectively (P < 0.001 for all comparisons). Guideline-concordant antiemetic prophylaxis increased from 21.5% to 52%. The most notable increase was observed in the utilization of neurokinin-1 receptor antagonists (NK-1 RAs) for HEC. Regarding NCDs, guideline-compliant management resulted in significantly more CINV-free days compared with non-compliant management (19.88 days vs. 17.05 days, P < 0.0001), highlighting the critical role of standardized antiemetic prophylaxis in improving patient outcomes.
Conclusion: Over the five-year period, CINV management in Sichuan has demonstrated significant, measurable progress, evidenced by a notable decline in incidence and substantially improved complete control rates, especially in high-risk HEC patients. This positive trend is strongly associated with the increased implementation of evidence-based antiemetic guidelines. However, the persistent CINV burden underscores the need for continued quality improvement efforts to fully translate guideline recommendations into universal best practice.
Keywords: chemotherapy-induced nausea and vomiting, CINV, no CINV days, NCDs, guideline adherence, real-world evidence, China
Introduction
Chemotherapy-induced nausea and vomiting (CINV) persist as a formidable obstacle in oncology, profoundly influencing the quality of life of patients undergoing treatment and potentially compromising their overall survival rates. Furthermore, CINV can induce metabolic disturbances, malnutrition, and weight loss among cancer patients, significantly augmenting their physical and psychological burdens and leading to decreased treatment adherence.1,2 Despite advancements in antiemetic therapies, CINV remains prevalent, with its incidence remaining notably high and influenced by a multitude of intricate factors. A real-world study encompassing 45,324 patients with CINV revealed that only 24%, 18%, and 7% of patients on anthracycline and cyclophosphamide (AC), cisplatin, and carboplatin regimens, respectively, adhered to the three antiemetic regimens recommended by the Multinational Association of Supportive Care in Cancer (MASCC) and European Society for Medical Oncology (ESMO) guidelines.3,4 However, studies have demonstrated that, in the absence of effective interventions, highly emetogenic chemotherapy (HEC) regimens can induce CINV in approximately 90% of patients, highlighting the pressing need for enhanced management strategies.5,6
The real-world occurrence of both acute and delayed CINV appears to be substantially higher than often reported in clinical trials, although the underlying causes of this discrepancy remain elusive. Previous randomized clinical trials (RCTs) have shown that with effective preventive measures, the incidence of acute CINV is approximately 10%, and delayed CINV is about 25–30%.7 However, in real-world settings, the incidence of acute CINV is about 40–55%, and the incidence of delayed CINV can reach as high as 50–60%.7,8 Factors such as patient demographics, prior chemotherapy experiences, and specific agents used can all interplay to influence the severity and frequency of CINV.9–11 Standardized treatment protocols utilizing antiemetic medications have proven crucial in reducing the incidence of CINV, yet challenges persist.12
Regional-specific factors may substantially influence CINV management. In Sichuan, healthcare resources are unevenly distributed between urban and rural areas, potentially delaying adoption of updated antiemetic guidelines in primary care.13 Economic constraints and variations in insurance reimbursement limit access to costly but effective NK-1 receptor antagonists.14 Additionally, clinical practice inertia persists, as real-world data show guideline-concordant antiemetic prophylaxis remains suboptimal in routine practice.15 These region-specific factors are essential to consider when interpreting local CINV trends and developing targeted supportive care strategies.
Current research has predominantly concentrated on the incidence trajectories of acute and delayed CINV associated with single-agent chemotherapy, while comprehensive data throughout the entire chemotherapy cycle—particularly for multiday cisplatin regimens—remain notably scarce.16 Defining the temporal boundaries of acute and delayed CINV in this context introduces additional complexities that warrant further methodological consideration.17 Furthermore, conventional endpoints such as complete control (CC) rates capture only the binary presence or absence of vomiting and rescue therapy at discrete time points, failing to adequately reflect the cumulative burden of CINV over the entire cycle.18 In response, the concept of “no CINV days” (NCDs) has emerged as a patient-centered metric that quantifies the total number of days patients remain free from both nausea and vomiting, offering incremental value by capturing overall symptom burden and providing greater sensitivity to detect differences in antiemetic effectiveness—particularly in real-world settings where symptom fluctuations are common.13,15 Notwithstanding substantial progress, numerous factors influencing CINV occurrence remain to be fully elucidated, warranting further research to optimize therapeutic outcomes in this critical domain of oncology supportive care.19
To investigate the actual incidence of CINV in cancer patients in Sichuan, China, our team discovered in 2018 that the most critical factor affecting CINV incidence was the non-use of standardized antiemetic drugs, primarily due to the non-utilization of neurokinin-1 receptor antagonists (NK-1 RAs).13 In response, cancer experts in Sichuan Province, through continuous learning and communication, not only established a vomit-free ward but also formulated guidelines for CINV prevention and control in Sichuan Province.20 To ascertain whether these studies and efforts have reduced the incidence of CINV in cancer patients in Sichuan, China, this study conducted a secondary investigation and analysis of CINV in the real world, building upon previous research.
Patients and Methods
Study Design
This observational prospective study was devised and executed under the expert guidance of clinicians specializing in the prevention and management of CINV in Sichuan Province, China. Within this framework, questionnaires were collaboratively designed through joint decision-making among advocates, oncology clinicians, psychologists, and nursing specialists. By the study’s conclusion, a total of 27 cancer research institutions across Sichuan had contributed to this forward-looking clinical investigation. Between March 2023 and October 2023, patients diagnosed with malignant tumors who underwent MEC/HEC at these institutions, along with their oncologists and nurses, participated in the survey. The research proposal has undergone rigorous review and has been approved by the ethics committees of all participating institutions. In addition, all patients underwent a comprehensive informed consent procedure and signed a written informed consent form approved by the Ethics Committee of Chengdu Fifth People’s Hospital.
Patients
The main inclusion criteria were as follows: 1) age 18 years or older; 2) a histologically confirmed malignant tumor; and 3) currently scheduled to receive MEC or HEC.
Patients will be excluded based on any of the following criteria: chronic digestive system diseases, persistent chronic nausea and vomiting, a history of dizziness or Ménière’s syndrome, uncontrolled cancerous pain necessitating titration or adjustment of opioid analgesic dosage, cognitive impairment (including mental disorders or severe learning disabilities), long-term corticosteroid therapy, use of illegal drugs (including medicinal marijuana), or significant cognitive impairment due to excessive alcohol consumption; patients with poor compliance and inability to complete the study as planned; current participation in any other clinical trials or observational studies.
Methods
The main study tools consisted of two parts: investigator’s questionnaires (part 1) and patients’ diaries (part 2). Once eligible patients have signed the informed consent form, the research physician will proceed to register their demographic and clinical characteristics on the electronic case report form, henceforth referred to as the patient information collection form in this context. The recorded clinical features include the patient’s age, gender, tumor type, tumor metastasis site, presentation status of the Eastern Cooperative Oncology Group (ECOG), chemotherapy regimen, chemotherapy cycle, chemotherapy line, antiemetic medication regimen, alcohol consumption, and pregnancy related nausea or vomiting. Furthermore, detailed notes will be taken on the rescue measures administered to each patient experiencing nausea or vomiting during the acute, delayed, and high-risk phases. Based on established emetic standards, chemotherapy regimens are categorized into high emetic chemotherapy (HEC) and moderate emetic chemotherapy (MEC). Physician-reported data were available for all 1985 enrolled patients. Patient diary data, recording daily nausea and vomiting, were completed by 1726 patients (87.0%). These two data sources were analyzed separately for their respective endpoints; thus, no imputation for missing diary data was required.
In accordance with the NCCN Clinical Practice Guidelines in Oncology for Antiemesis (Version 2.2018 for the baseline study; Version 1.2023 for the current study),21–23 the standard antiemetic prophylaxis for HEC involves a triple-drug combination of an NK-1 receptor antagonist (NK-1 RA), a serotonin-3 receptor antagonist (5-HT3 RA), and dexamethasone (DEX). For MEC, the standard antiemetic prophylaxis consists of a 5-HT3 RA plus DEX.4,23 Olanzapine may be considered as an additional option for selected high-risk patients receiving HEC. For patients at higher risk or receiving certain MEC regimens, a triple-drug regimen (as used for HEC) may be adopted for both acute and delayed phase prevention. Antiemetic regimens were considered guideline-adherent if they complied with the recommendations of the NCCN guidelines, including appropriate selection and dosing of antiemetic agents based on chemotherapy emetogenicity risk level.
The patient diary, designed using the Multinational Association for Cancer MASCC antiemetic tool (MAT) version,24,25 meticulously logs the occurrence of nausea and vomiting from the first to the twenty-first day of chemotherapy. A Visual Analog Scale (VAS), featuring a 10-centimeter line ranging from 0 (no nausea) to 10 (most severe nausea), is employed to document the severity of nausea. Patients are instructed to record their nausea intensity and vomiting frequency on a daily basis.
Definition of Key Terms
CINV Incidence: A patient was considered to have experienced CINV if they reported any nausea episode or vomiting event from chemotherapy initiation until the end of the overall phase.
Phase Definitions:
Acute Phase: The first 24 hours following chemotherapy infusion (D1–3 was recorded if cisplatin was administered for 3 days).
Delayed Phase: Days 2 through 5 post chemotherapy (D4–7 was recorded if cisplatin was administered for 3 days).
Risk Phase: The combined high-risk interval (acute and delayed phases, days 1–5; day 1–7 was recorded if cisplatin was administered for 3 days).
Beyond the Risk Phase: The subsequent observation period from days 6 to 21 (D8–21 was recorded if cisplatin was administered for 3 days).
Overall Phase: The complete study duration (days 1–21).
Efficacy Endpoints:
No CINV Days (NCDs): The cumulative count of days within the observation period during which a patient experienced no vomiting and no nausea.
Complete Control (CC): Defined as no vomiting, no use of salvage therapy, and no significant nausea (ie, nausea not interfering with daily activities as per patient diary).
Statistical Analysis
Statistical analysis was performed using SPSS 25.0 software, and bar charts were generated with GraphPad Prism 9.0. Continuous data were expressed as mean ± standard deviation (SD), and count data were expressed as numbers (rates or percentages). For comparisons between two groups, independent sample t-tests or Mann–Whitney U-tests were used for continuous variables depending on normality, and chi-square tests or Fisher’s exact tests were used for categorical variables. Specifically, for subgroup analyses (eg, comparing CINV incidence and CC rates between patients receiving MEC and HEC), the chi-square test or Fisher’s exact test (when expected frequencies were <5) was applied. For continuous variables such as age and NCDs, comparisons between groups were performed using independent sample t-tests or Mann–Whitney U-tests based on the distribution of the data. Additionally, to control for potential confounding factors, multivariate logistic regression models were used to evaluate the independent impact of different antiemetic regimens on CINV outcomes. A P-value of less than 0.05 was considered statistically significant.
Results
Patient Characteristics
Between March 2023 and October 2023, a comprehensive total of 2078 patients were enrolled in the study. Upon revising the intended population, five individuals who withdrew their informed consent, along with 88 patients with incomplete information, were excluded, resulting in the inclusion of 1985 patients for analysis. The average age of the patients was 61 years, with ages ranging from 18 to 90 years. The gender distribution comprised 1177 males (59.3%) and 808 females (40.7%). Regarding ECOG scores, 85.6% of patients scored 0–1, while 14.4% scored 2. Among the primary tumor locations, lung cancer topped the list with 540 cases (27.2%), followed by colorectal cancer with 394 cases (19.8%), and esophageal cancer with 240 cases (12.1%). In terms of chemotherapy regimens, 840 patients (42.3%) received the MEC regimen, while 1145 patients (57.7%) received the HEC regimen. A total of 1243 patients (62.6%) were undergoing first-line chemotherapy (Table 1).
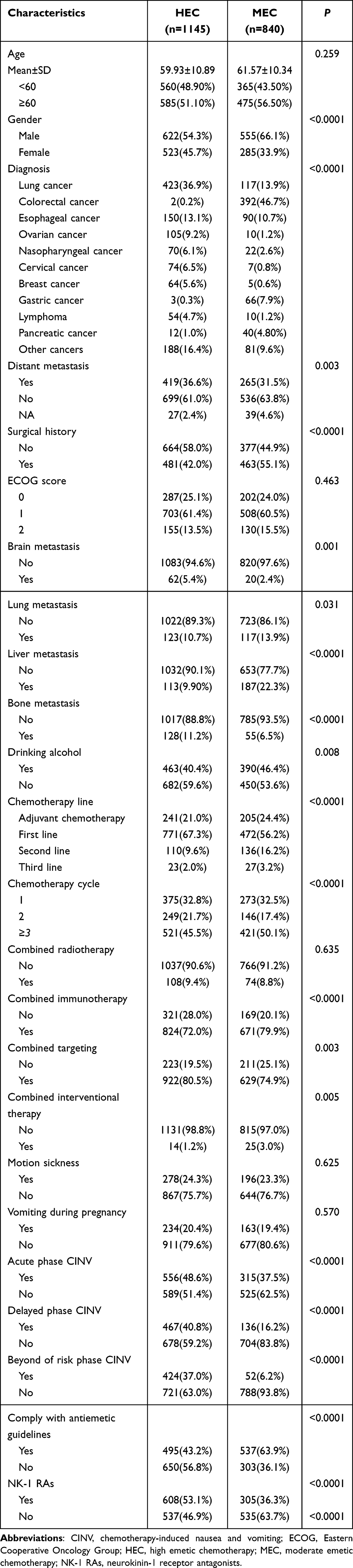 |
Table 1 Baseline Patient Demographic and Clinical Characteristics |
Comparative Analysis of HEC and MEC Patient Cohorts
The distribution of chemotherapy regimens was consistent with prior characterization, with 1145 patients (57.7%) receiving HEC and 840 (42.3%) receiving MEC (Table 1). Comparative analysis revealed no significant differences between HEC and MEC groups in age, ECOG performance status, concurrent radiotherapy, history of motion sickness, or vomiting during pregnancy.
However, statistically significant differences were observed across multiple clinical parameters. The groups differed significantly in gender distribution, cancer type, presence of distant metastases (including specific sites such as brain, lung, liver, and bone), alcohol consumption, chemotherapy line, cycle number, and concurrent treatments (targeted therapy, interventional therapy, and prior surgical intervention).
Notably, CINV incidence patterns diverged substantially between regimens. Patients receiving HEC demonstrated significantly higher rates of acute, delayed, and beyond the risk period CINV compared to MEC recipients. Furthermore, distinct antiemetic management patterns emerged: guideline-compliant prophylaxis was more frequently administered in the MEC subgroup (63.9% vs. 43.2%), while NK-1 RAs utilization was significantly higher in HEC patients (53.1% vs. 36.3%) (Table 1).
Comparative Analysis of Overall and Phase-Specific CINV Incidence
Compared with the 2018 baseline, the 2023 survey demonstrated a significant decrease in CINV incidence across all phases. The overall CINV rate declined from 82.97% (921/1110) to 57.33% (1138/1985), representing an absolute reduction of 25.64% (95% CI: 22.42% to 28.86%, P < 0.0001). Acute phase CINV decreased from 55.32% (614/1110) to 43.88% (871/1985), with an absolute reduction of 11.44% (95% CI: 7.91% to 14.97%, P < 0.0001). Delayed phase CINV showed the most pronounced reduction, declining from 62.25% (691/1110) to 30.38% (603/1985), an absolute reduction of 31.87% (95% CI: 28.54% to 35.20%, P < 0.0001). CINV occurrence beyond the conventional risk period decreased from 36.04% (400/1110) to 23.98% (476/1985), an absolute reduction of 12.06% (95% CI: 8.73% to 15.39%, P < 0.0001) (Figure 1).
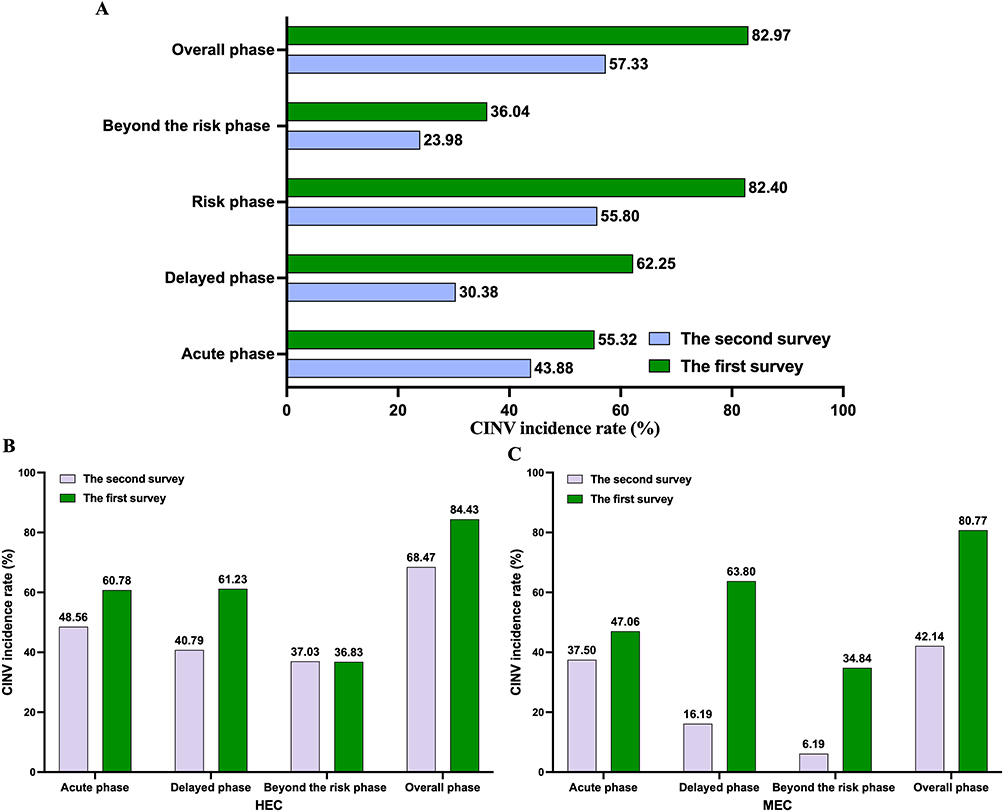 |
Figure 1 Comparison chart of CINV incidence rate in two investigations. (A) Comparative Analysis of Overall and Phase-Specific CINV Incidence. (B) The incidence of CINV in the HEC subgroup population. (C) The incidence of CINV in the MEC subgroup population. Abbreviations: CINV, chemotherapy-induced nausea and vomiting; HEC, high emetic chemotherapy; MEC, moderate emetic chemotherapy. |
The Relationship Between Chemotherapy Drugs and the Incidence of CINV
Analysis of patients receiving HEC demonstrated significant temporal changes in CINV patterns. The current study revealed an overall CINV incidence of 68.47% (784/1145) in the HEC group, representing a substantial decline from the 84.43% (564/668) reported in the 2018 cohort, representing an absolute reduction of 15.96% (95% CI: 11.96% to 19.96%, P < 0.0001).13 Acute phase CINV decreased from 60.78% (406/668) to 48.56% (556/1145) (absolute reduction: 12.22%, 95% CI: 7.59% to 16.85%, P < 0.0001). Delayed phase CINV showed the most pronounced improvement, declining from 61.23% (409/668) to 40.79% (467/1145) (absolute reduction: 20.44%, 95% CI: 15.89% to 24.99%, P < 0.0001). However, CINV occurrence beyond the conventional risk period remained relatively stable, with no significant change (36.83% vs. 37.03%; absolute reduction: 0.20%, 95% CI: −4.27% to 4.67%, P = 0.93) (Figure 1).
Among MEC patients, the overall CINV incidence decreased significantly from 80.77% (357/442) in 2018 to 42.14% (354/840) in 2023, representing an absolute reduction of 38.63% (95% CI: 33.65% to 43.61%, P < 0.0001). Acute phase CINV decreased from 47.06% (208/442) to 37.50% (315/840) (absolute reduction: 9.56%, 95% CI: 3.96% to 15.16%, P < 0.001). Delayed phase CINV showed the most pronounced improvement, declining from 63.80% (282/442) to 16.19% (136/840) (absolute reduction: 47.61%, 95% CI: 42.71% to 52.51%, P < 0.0001). CINV occurrence beyond the conventional risk period also decreased substantially from 34.84% (154/442) to 6.19% (52/840) (absolute reduction: 28.65%, 95% CI: 24.21% to 33.09%, P < 0.0001) (Figure 1).
In addition, χ2-test analysis showed that the incidence of CINV in the HEC group was significantly higher than that in the MEC group during the acute, delayed, and high-risk phases, and the difference was statistically significant (Table 1).
CINV Incidence and Guideline Compliance Rates
The results showed that the compliance rate of all antiemetic regimens was 52.0% (1032/1985), within which the rate was 24.9% in the MEC group and 27.1% in the HEC group. Within this guideline-compliant group, 63.9% were undergoing MEC and 43.2% HEC. The utilization of neurokinin-1 receptor antagonists (NK-1 RAs) was observed in 45.9% of all patients, with higher rates in the HEC subgroup (53.1%) compared to the MEC subgroup (35.3%) (Table 1).
When comparing with the 2018 baseline, substantial improvements in CINV management were observed in the 2023 cohort. As shown in Table 2, guideline adherence increased significantly from 21.50% in 2018 to 52.00% in 2023 (P < 0.001). Notably, despite the 2023 cohort having older age (60.62 vs. 56.67 years, P < 0.001) and a higher proportion of ECOG score 2 patients (14.36% vs. 7.12%, P < 0.001)—factors associated with increased CINV risk—the overall CINV incidence decreased significantly from 82.97% in 2018 to 57.33% in 2023 (P < 0.0001).
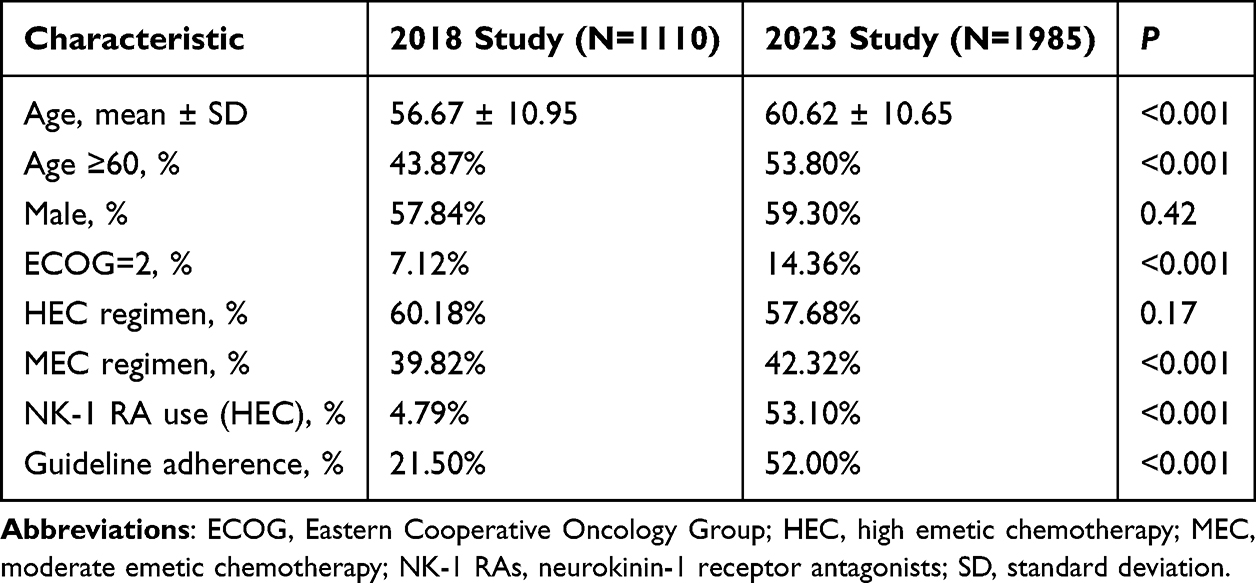 |
Table 2 Comparison of Patient Characteristics Between the 2018 Baseline Cohort and the 2023 Current Cohort |
In the entire patient cohort, the incidences rates of CINV in acute phase (35% vs. 53.5%), delayed phase (12.4% vs. 49.8%), beyond the risk period (4.7% vs. 44.9%), and overall phase (39.4% vs. 76.7%) were significantly lower in patients who received guideline-compliant prophylaxis compared to those who did not (all P < 0.05) (Figure 2). This significant protective effect of guideline adherence was consistently observed across both HEC and MEC subgroups. Among HEC patients, the guideline-compliant group demonstrated markedly lower CINV incidences across all phases (acute: 38% vs. 56.6%; delayed: 10.5% vs. 63.8%; beyond risk period: 3.8% vs. 62.3%; overall: 41.8% vs. 88.8%; all P < 0.05). Similarly, in the MEC subgroup, patients receiving guideline-compliant regimens also reported significantly reduced incidences (acute: 32.3% vs. 46.9%; delayed: 14.2% vs. 19.8%; beyond risk period: 5.4% vs. 7.6%; overall: 37.2% vs. 50.8%; all P < 0.05) (Figure 2).
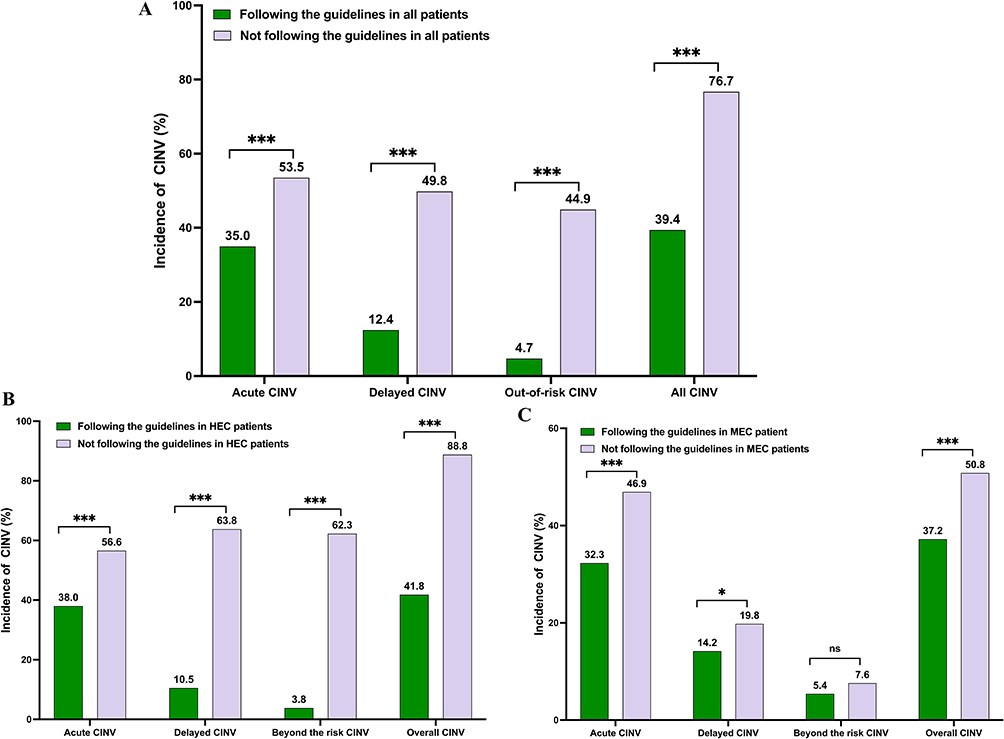 |
Figure 2 Incidence rate of CINV in patients with compliance with antiemetic guidelines. (A) Incidence rate of CINV in all patients. (B) Incidence rate of CINV in HEC patients. (C) Incidence rate of CINV in MEC patients. *P < 0.05; *** P < 0.001; ns, not significant (P ≥ 0.05). Abbreviations: CINV, chemotherapy-induced nausea and vomiting; HEC, high emetic chemotherapy; MEC, Moderate emetic chemotherapy |
Further statistical analysis within the HEC subgroup revealed no significant association between guideline adherence and patient age, gender, alcohol consumption, line of chemotherapy, or metastasis status (all P > 0.05). Conversely, guideline adherence demonstrated significant associations with ECOG performance status, history of vomiting during pregnancy, tumor type, utilization of NK-1 RAs, and number of chemotherapy cycles (all P < 0.05) (Table 3).
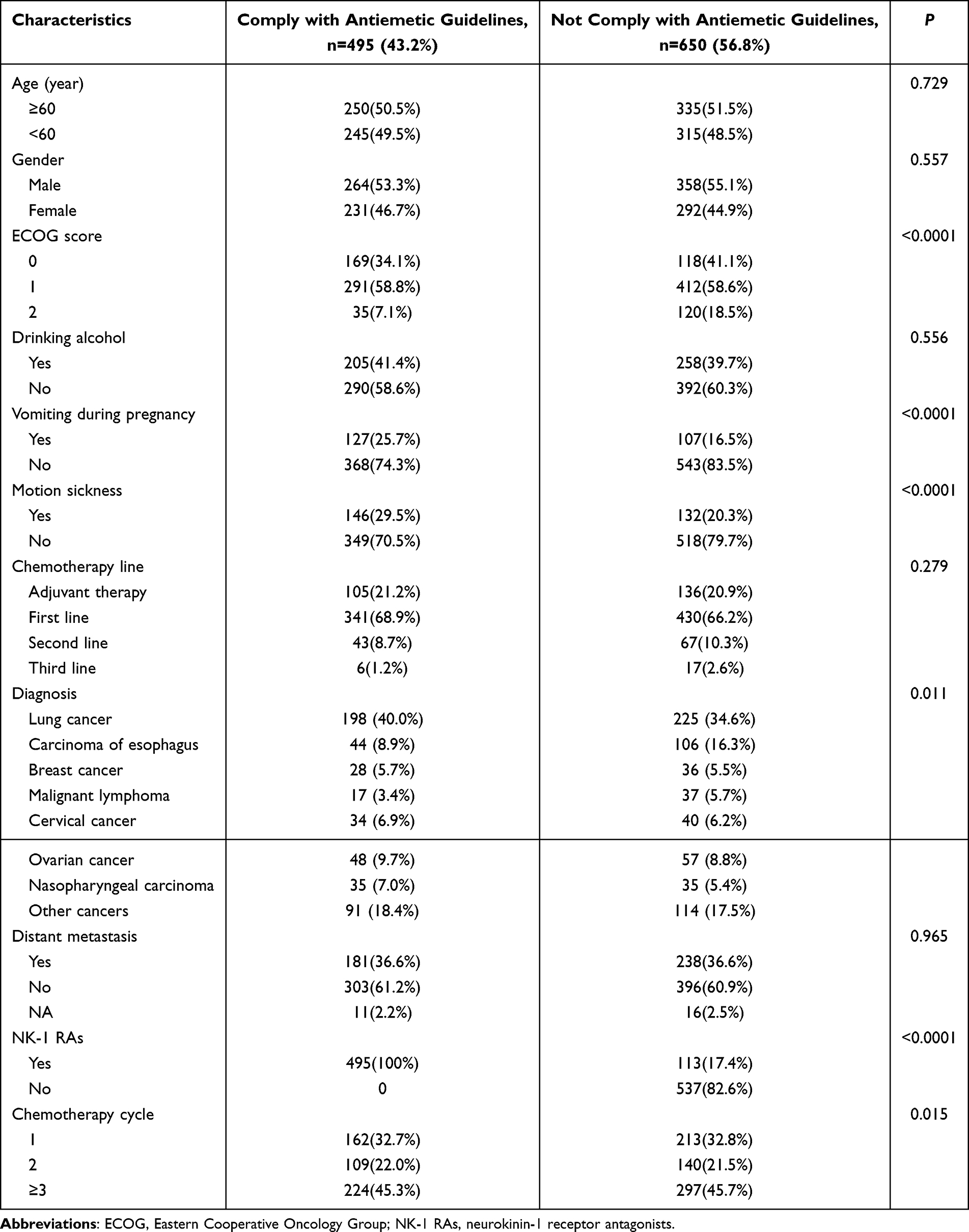 |
Table 3 Baseline Characteristics of Compliance with Antiemetic Guidelines in the HEC Subgroup |
Evolution of Antiemetic Prophylaxis Regimens
A comparative analysis with the inaugural 2018 survey13 was conducted to evaluate the progress in standardized CINV management in Sichuan. The results demonstrate a substantial evolution in antiemetic prescribing patterns, accompanied by two key factors: a marked increase in the utilization of NK-1 RAs and significantly improved adherence to guideline-recommended antiemetic regimens.
The current study found that the overall NK-1 RAs utilization rate surged to 54.0%, a profound increase from the previously reported 3.42%. As shown in Table 2, NK-1 RA use in HEC patients increased dramatically from 4.79% in 2018 to 53.10% in 2023, representing a nearly 11-fold increase (P < 0.001). This upward trend was consistently observed in subgroup analyses, where NK-1 RAs usage rose to 53.1% (from 4.79%) in patients receiving HEC and to 36.3% (from 1.36%) in those receiving MEC (Figure 3).
 |
Figure 3 Comparison of NK-1 RAs usage rate and compliance with antiemetic guidelines in two survey studies. (A) Comparison of NK-1 RAs usage rates in two survey studies. (B)Comparison of compliance with antiemetic guidelines in two survey studies. Abbreviations: CINV, chemotherapy-induced nausea and vomiting; HEC, high emetic chemotherapy; MEC, moderate emetic chemotherapy; NK-1 RAs, neurokinin-1 receptor antagonists. |
Concurrently, the overall rate of guideline-compliant antiemetic prophylaxis significantly improved, reaching 52.0% compared to 21.5% in the 2018 baseline (P < 0.001). Table 2 further confirms this substantial improvement, with guideline adherence increasing from 21.50% to 52.00% over the five-year period. This enhancement in adherence was also evident in both the HEC subgroup (43.2% vs. 4.64%) and the MEC subgroup (63.9% vs. 47.06%) (Figure 3).
Analysis of Complete Control Rates
Comparative analysis demonstrated substantial improvements in complete control (CC) rates across all phases and emetogenic categories in the current study compared with the 2018 baseline.13 In the HEC subgroup, CC rates increased from 30.1% to 58.4% in the overall phase, from 52.8% to 64.1% in the acute phase, from 60.6% to 75.6% in the delayed phase, and from 85.6% to 91.9% beyond the conventional risk period (Figure 4).
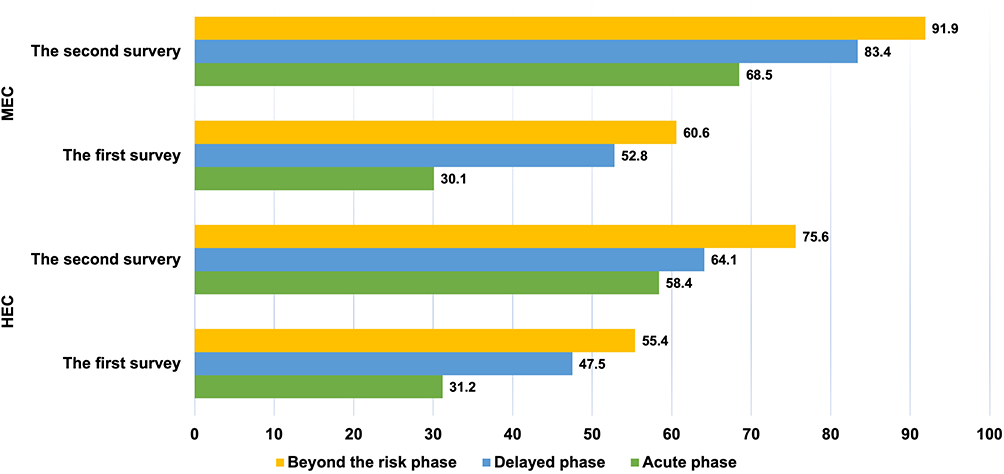 |
Figure 4 Comparison of complete control rates in different emetic chemotherapy regimens and two survey studies. Abbreviations: HEC, high emetic chemotherapy; MEC, moderate emetic chemotherapy. |
In the MEC subgroup, even more pronounced improvements were observed. CC rates increased from 32.1% to 68.5% in the overall phase, from 47.5% to 83.4% in the acute phase, from 55.4% to 91.9% in the delayed phase, and from 79.0% to 93.2% beyond the risk period (Figure 4).
The magnitude of improvement was particularly notable in the acute phase for both HEC and MEC groups, with CC rates approximately doubling compared with the 2018 baseline. Additionally, MEC patients consistently achieved higher final CC rates than HEC patients across all evaluated timeframes in the current study.
Analysis of No CINV Days (NCDs)
Among the 1985 enrolled patients, 1726 patients (87.0% of the enrolled cohort) completed all 21 days of diary records and were included in the NCDs analysis. The mean number of no CINV days in the current chemotherapy cycle was 18.50 ± 3.51 days.
Patients receiving MEC regimens experienced significantly more NCDs across all phases compared to those receiving HEC (all P < 0.0001). The overall NCDs were 20.10 ± 1.53 days for the MEC group versus 17.26 ± 4.06 days for the HEC group (mean difference: 2.84 days, 95% CI: 2.56 to 3.12 days). This pattern persisted in the acute phase (0.62 ± 0.49 vs. 0.50 ± 0.50 days; mean difference: 0.12 days, 95% CI: 0.07 to 0.17 days), delayed phase (3.64 ± 0.91 vs. 2.48 ± 1.70 days; mean difference: 1.16 days, 95% CI: 1.04 to 1.28 days), and beyond the risk period (15.85 ± 0.67 vs. 14.28 ± 2.62 days; mean difference: 1.57 days, 95% CI: 1.40 to 1.74 days) (all P < 0.0001) (Figure 5).
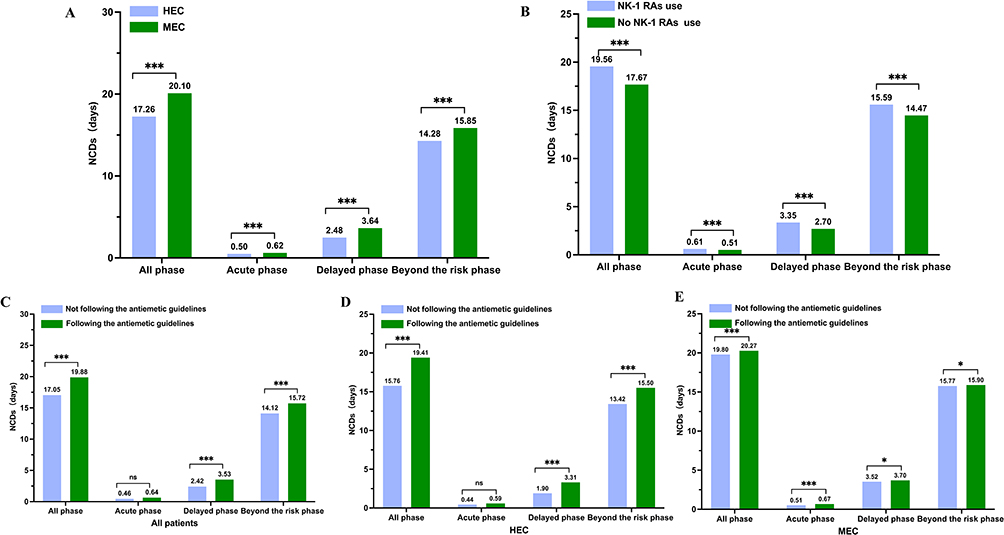 |
Figure 5 Comparative analysis of no CINV Days (NCDs) in different subgroups. (A) Comparison of NCDs between HEC and MEC subgroups. (B) Comparison of NCDs between subgroups using NK-1 RAs or not. (C) Comparison of standardized antiemetic regimens and subgroups of NCDs. (D) Comparison of standardized antiemetic regimens and NCDs in the HEC subgroup. (E) Comparison of standardized antiemetic regimens and non-standardized treatment for NCDs in MEC subgroups. *P < 0.05; *** P < 0.001; ns, not significant (P ≥ 0.05). Abbreviations: HEC, high emetic chemotherapy; MEC, moderate emetic chemotherapy; NCDs, no chemotherapy-induced nausea and vomiting days; NK-1 RAs, neurokinin-1 receptor antagonists |
The administration of NK-1 RAs was associated with increased NCDs throughout the observation period. Patients who received NK-1 RAs demonstrated higher NCDs in the acute phase (0.61 days), delayed phase (3.35 days), beyond the risk period (15.59 days), and overall (19.56 days) compared to those who did not receive NK-1 RAs (0.51, 2.70, 14.47, and 17.67 days, respectively) (all P<0.0001) (Figure 5).
Adherence to guideline-directed antiemetic prophylaxis consistently correlated with improved NCD outcomes. In the overall population, guideline-compliant management resulted in higher NCDs across all phases (acute: 0.64 days, delayed: 3.53 days, beyond risk period: 15.72 days, total: 19.88 days) compared to non-compliant management (0.46, 2.42, 14.12, and 17.05 days, respectively). This advantage was maintained in both HEC and MEC subgroups, with patients following guidelines exhibiting superior NCDs at each stage of analysis. However, there was no significant difference in the number of NCDs in the acute phase among the HEC subgroup patients (Figure 5).
Discussion
CINV is a prevalent and distressing adverse effect experienced by cancer patients undergoing treatment, significantly impacting their quality of life and, ultimately, their overall survival rates. This debilitating condition not only hampers patients’ ability to complete their prescribed chemotherapy regimens but also exacerbates their emotional and physical burden, impeding their recovery journey. Consequently, the management of CINV has emerged as a pivotal aspect of cancer care, necessitating a multifaceted approach encompassing preventive strategies, prompt interventions, and continuous monitoring.
The incidence of CINV is alarmingly high, with numerous factors contributing to its variable manifestation across different patients. The complex pathophysiology of CINV, involving multiple neurotransmitter systems including serotonin, dopamine, and substance P, may explain why current strategies remain imperfect.26 In the absence of effective prophylactic measures, HEC regimens can induce nausea and vomiting in nearly 90% of patients, posing a considerable challenge to clinicians. The intricate interplay between individual patient characteristics, such as age, gender, and genetic predispositions, as well as regimen-specific factors, including drug type, dosage, and route of administration, further complicates the prediction and management of CINV. So, this complexity underscores the need for continued research into novel therapeutic targets and approaches for patients with breakthrough symptoms despite standard prophylaxis.
This comparative longitudinal study demonstrates substantial improvements in CINV management across Sichuan cancer centers since the initial 2018 survey.13 The significant reduction in overall CINV incidence from 82.97% to 57.33%, particularly the pronounced decline in delayed CINV from 62.3% to 30.4%, represents meaningful progress in supportive care quality. However, the persistent high CINV burden, especially in patients receiving HEC treatment, underscores the ongoing challenges in comprehensive symptom control.
Our subgroup analysis reveals differential improvement patterns across risk categories. Patients receiving MEC demonstrated remarkable gains, with delayed CINV incidence decreasing dramatically from 63.8% to 16.2%, suggesting successful implementation of delayed-phase antiemetic strategies for this population. In contrast, HEC patients maintained substantially higher CINV rates (68.4% overall), highlighting the inherent challenges of highly emetogenic regimens and validating the risk-stratified approach to antiemetic prophylaxis.27 The particularly high incidence of CINV extending beyond the conventional risk period in HEC patients (37.03%) warrants special attention in future management strategies.
The most compelling finding of our study is the robust association between guideline-compliant antiemetic prophylaxis and significantly improved clinical outcomes across all evaluation endpoints. Patients receiving guideline-adherent regimens demonstrated nearly halved CINV risk (39.4% vs 76.7%) in the overall population, with consistent therapeutic benefits maintained across both HEC and MEC subgroups. These results provide substantial real-world validation for current antiemetic recommendations established by major oncology organizations including ASCO, MASCC/ESMO, and CSCO.22,28,29
Nevertheless, the suboptimal overall guideline adherence rate of 52.0% in our cohort, despite remarkable improvement from the 21.5% baseline in 2018, likely explains the persistently elevated CINV rates observed in clinical practice. This implementation gap is consistent with global patterns, as evidenced by international reports demonstrating concerningly low adherence rates: a Swedish study revealed only 61% guideline compliance with 89% of patients receiving suboptimal delayed CINV prevention;30 similarly, United States data indicated merely 29–39% adherence among HEC patients.31,32 Identified barriers to optimal adherence include insufficient knowledge of updated guidelines, concerns about medication costs, particularly regarding NK-1 RAs utilization, and inadequate assessment of individual patient risk factors.18,33–35
The Chinese context reflects similar challenges, though comparative data remain limited by sample size constraints. A retrospective analysis documented guideline compliance rates of 11.41% and 53.89% for HEC and MEC, respectively.36 More encouragingly, a 2022 investigation across 16 tertiary hospitals in Shanghai demonstrated substantial improvement in HEC guideline adherence, increasing from 21.6% to 67.0% over five years.37 This positive trajectory aligns with our observed advancements in Sichuan, suggesting that nationwide initiatives including standardized antiemetic protocols and the establishment of vomit-free wards are effectively enhancing CINV management quality across Chinese medical institutions.
The dramatic increase in NK-1 RAs utilization from 3.42% to 54.0% was closely associated with the observed clinical improvements. The superior CC rates and increased NCDs among NK-1 RAs recipients are consistent with the effectiveness of this drug class in preventing delayed CINV through its specific mechanism of substance P antagonism.38 The association between NK-1 RAs use and better outcomes even in MEC patients provides real-world evidence for considering expanded use in selected moderate-risk settings, particularly for patients with additional risk factors.
Our study introduces “No CINV Days” (NCDs) as a novel patient-centered outcome measure, offering a refined perspective for evaluating antiemetic efficacy. This metric-shifts focus from merely counting emetic episodes to quantifying symptom-free periods, thereby providing a more comprehensive assessment of how CINV management impacts patients’ daily functioning and quality of life. The data demonstrate that patients achieving an average of 18.5 NCDs per cycle experienced meaningful clinical benefits, translating reduced symptom burden into tangible quality-of-life improvements.
Analysis revealed that guideline-compliant antiemetic regimens significantly increased NCD counts across all evaluation periods (acute, delayed, and beyond-risk phases; all P<0.0001). While both HEC and MEC patients benefited from standardized prophylaxis, the therapeutic advantage was particularly pronounced in the HEC subgroup. Notably, even with optimal prevention, the number of completely asymptomatic days during acute and delayed phases remained limited, highlighting the persistent challenge of breakthrough CINV. These findings suggest the need to elevate our therapeutic goals from simply reducing emetic episodes toward maximizing asymptomatic days—a higher standard that better aligns with comprehensive symptom control and quality-of-life optimization.
One strength of the study lies in the large sample size of the multicenter prospective observational study, which enhances the robustness of this registry and its potential applicability to clinical practice in China. This study once again highlights the remarkable value of adhering to guidelines for improving CINV prevention. Furthermore, it is important to delve deeper into CINV management and patient education. However, there are some limitations to this study. Firstly, it did not consider patients’ mental health status, thus precluding an understanding of the relationship between mental health status and the incidence of CINV. Secondly, it did not further explore biomarkers and genetic molecular mechanisms of CINV.
Several limitations warrant consideration. As a non-randomized real-world observational study, the findings should be interpreted with caution. The absence of randomization means that we cannot entirely exclude the possibility of selection bias or unmeasured confounding. Although we performed multivariable logistic regression adjusting for key confounders (age, sex, ECOG performance status, cancer type, chemotherapy line, and comorbidities), residual confounding may still exist. Consequently, the observed associations between guideline adherence and improved CINV outcomes should be interpreted as strong correlations rather than causal effects. Regarding generalizability, our findings are derived from 17 cancer centers across Sichuan Province—a region with diverse healthcare infrastructure ranging from tertiary referral centers to county-level hospitals. While this diversity supports the applicability of our findings to similar real-world settings in western China, caution is warranted when extrapolating to healthcare systems with substantially different resources, patient populations, or practice patterns. It is also noteworthy that the 2023 cohort had older age and a higher proportion of ECOG score 2 patients—factors associated with increased CINV risk—yet we observed substantial improvements, suggesting that our findings may actually underestimate the true impact of guideline implementation. Future prospective studies with more detailed data collection in other regions and healthcare contexts are warranted to further validate these findings and confirm external validity. Nevertheless, the persistent CINV burden (57.33%) underscores the need for continued efforts to fully translate evidence-based guidelines into universal best practice.
Several limitations warrant consideration. First, as a non-randomized real-world observational study with a descriptive, comparative design, the findings should be interpreted with caution. The absence of randomization means that we cannot entirely exclude the possibility of selection bias or unmeasured confounding. Moreover, the lack of individual-level data from the 2018 cohort precluded multivariate adjustment for inter-cohort differences. Consequently, the observed improvements should be interpreted as associations with temporal trends in clinical practice rather than causal effects. Second, regarding generalizability, our findings are derived from 17 cancer centers across Sichuan Province—a region with diverse healthcare infrastructure ranging from tertiary referral centers to county-level hospitals. While this diversity supports the applicability of our findings to similar real-world settings in western China, caution is warranted when extrapolating to healthcare systems with substantially different resources, patient populations, or practice patterns. Third, it is noteworthy that the 2023 cohort had older age and a higher proportion of ECOG score 2 patients—factors associated with increased CINV risk—yet we observed substantial improvements. This suggests that our findings may actually underestimate the true impact of guideline implementation. Future prospective studies with individual-level data across multiple time points and more detailed data collection in other regions are warranted to further validate these findings and confirm external validity. Nevertheless, the persistent CINV burden (57.33%) underscores the need for continued efforts to fully translate evidence-based guidelines into universal best practice.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Chengdu Fifth People’s Hospital (the ethics approval number is 2023-004-01). All patients in this study provided informed written (or verbal) consent and must adhere to the Declaration of Helsinki: https://www.wma.net/policies-post/wma-declaration-of-helsinki. Participation in the study was voluntary, and participants had the right to withdraw from the study at any time without any adverse consequences.
Acknowledgment
We would like to express our special thanks to the Grassroots Cancer Prevention and Control Committee of the Sichuan Preventive Medicine Association, the Tumor Targeting and Immunotherapy Committee of the Chengdu Anti-Cancer Association, and the Cancer Psychology and Health Management Committee of the Sichuan Cancer Society for their strong support. Special thanks to all participating doctors, nurses, and patients for their support and assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported in part by the Chengdu Fifth People’s Hospital Scientific Research Project (KYJJ2021-05), Chengdu Fifth People’s Hospital Teaching Reform Research Project (JGZX202214), Sichuan Science and Technology Program (2026NSFSC1906), 2021 Sichuan Medical Association (2021HR79), 2022 Xicisco Nestle Health Science Cancer Nutrition Research Fund Project (Y-NESTLE2022QN-0486), Chengdu Medical Research Project (2023484), The second batch of cancer pain management projects for the National Health Commission’s Capacity Building and Continuing Education Center (PMT1002-2), China Youth Entrepreneurship and Employment Foundation (P241121108690) and Cancer Prevention and Treatment Institute of Chengdu.
Disclosure
The authors declare no conflict of interest.
References
1. Aapro M. CINV: still troubling patients after all these years. Support Care Cancer. 2018;26(Suppl 1):5–17. doi:10.1007/s00520-018-4131-3
2. Seyedfatemi N, Ghezeljeh TN, Bolhari J, et al. Effects of family-based dignity intervention and expressive writing on anticipatory grief of family caregivers of patients with cancer: a study protocol for a four-arm randomized controlled trial and a qualitative process evaluation. Trials. 2021;22(1):751. doi:10.1186/s13063-021-05718-3
3. Aapro M, Scotté F, Escobar Y, et al. Practice patterns for prevention of chemotherapy-induced nausea and vomiting and antiemetic guideline adherence based on real-world prescribing data. Oncologist. 2021;26(6):e1073–e1082. doi:10.1002/onco.13716
4. Herrstedt J, Clark-Snow R, Ruhlmann CH, et al. 2023 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting. ESMO Open. 2024;9(2):102195. doi:10.1016/j.esmoop.2023.102195.
5. Jordan K, Jahn F, Aapro M. Recent developments in the prevention of chemotherapy-induced nausea and vomiting (CINV): a comprehensive review. Ann Oncol. 2015;26(6):1081–1090. doi:10.1093/annonc/mdv138
6. Wu F, Lin X, Yang Z, et al. Phase III randomized trial of palonosetron and dexamethasone with or without aprepitant to prevent nausea and vomiting induced by full-dose single-day cisplatin-based chemotherapy in lung cancer. Clin Lung Cancer. 2018;19(6):e913–e918. doi:10.1016/j.cllc.2018.08.006
7. Aapro M, Carides A, Rapoport BL, et al. Aprepitant and fosaprepitant: a 10-year review of efficacy and safety. Oncologist. 2015;20(4):450–458. doi:10.1634/theoncologist.2014-0229
8. Liau CT, Chu NM, Liu HE, et al. Incidence of chemotherapy-induced nausea and vomiting in Taiwan: physicians’ and nurses’ estimation vs. patients’ reported outcomes. Support Care Cancer. 2005;13(5):277–286. doi:10.1007/s00520-005-0788-5
9. Neefjes ECW, Van Der Vorst M. Nausea and vomiting after chemotherapy: an ongoing problem for patients] [J. Ned Tijdschr Geneeskd. 2023;167.
10. Mosa ASM, Hossain AM, Lavoie BJ, et al. Patient-related risk factors for chemotherapy-induced nausea and vomiting: a systematic review. Front Pharmacol. 2020;11:329. doi:10.3389/fphar.2020.00329
11. Dranitsaris G, Molassiotis A, Clemons M, et al. The development of a prediction tool to identify cancer patients at high risk for chemotherapy-induced nausea and vomiting. Ann Oncol. 2017;28(6):1260–1267. doi:10.1093/annonc/mdx100
12. Aapro M, Molassiotis A, Dicato M, et al. The effect of guideline-consistent antiemetic therapy on chemotherapy-induced nausea and vomiting (CINV): the Pan European Emesis Registry (PEER). Ann Oncol. 2012;23(8):1986–1992. doi:10.1093/annonc/mds021
13. Sun Y, Zheng Y, Yang X, et al. Incidence of chemotherapy-induced nausea and vomiting among cancer patients receiving moderately to highly emetogenic chemotherapy in cancer centers in Sichuan, China. J Cancer Res Clin Oncol. 2021;147(9):2701–2708. doi:10.1007/s00432-021-03554-1
14. Xu X, Bao Y, Xu K, et al. Economic value of fosaprepitant-containing regimen in the prevention of chemotherapy-induced nausea and vomiting in china: cost-effectiveness and budget impact analysis. Front Public Health. 2022;10:913129. doi:10.3389/fpubh.2022.913129
15. Si X, Zhang H, Ding Q, et al. Retrospective analysis of real-world prescribing data for managing cisplatin-based chemotherapy-induced nausea and vomiting in China. Cancer Med. 2024;13(6):e7121. doi:10.1002/cam4.7121
16. Herrstedt J, Clark-Snow R, Ruhlmann CH, et al. MASCC/ESMO antiemetic guidelines: introduction to the 2023 guidelines update. Support Care Cancer. 2023;32(1):57. doi:10.1007/s00520-023-08219-y
17. Rapoport BL, Herrstedt J, Snow RC, et al. 2023 updated MASCC/ESMO consensus recommendations: prevention of nausea and vomiting following multiple-day chemotherapy, high-dose chemotherapy, and breakthrough nausea and vomiting. Support Care Cancer. 2023;32(1):36. doi:10.1007/s00520-023-08224-1
18. Navari RM, Aapro M. Antiemetic prophylaxis for chemotherapy-induced nausea and vomiting. N Engl J Med. 2016;374(14):1356–1367. doi:10.1056/NEJMra1515442
19. Scotté F, Schwartzberg L, Iihara H, et al. 2023 updated MASCC/ESMO Consensus recommendations: prevention of nausea and vomiting following moderately emetic risk antineoplastic agents. Support Care Cancer. 2023;32(1):45. doi:10.1007/s00520-023-08222-3
20. Expert Group for the Development of the Sichuan Provincial Expert Consensus on the Prevention and Management of Antineoplastic Drug-Induced Nausea and Vomiting. Expert consensus on prevention and control of nausea and vomiting related to anti tumor drug treatment in sichuan province, 2024 edition. Chin J Evidence-Based Med. 2024;10:1129–1136. doi:10.7507/1672-2531.202407066.
21. Network N C C. NCCN clinical practice guidelines in antiemesis. NCCN, 2018, Version 2.
22. Kennedy SKF, Goodall S, Lee SF, et al. 2020 ASCO, 2023 NCCN, 2023 MASCC/ESMO, and 2019 CCO: a comparison of antiemetic guidelines for the treatment of chemotherapy-induced nausea and vomiting in cancer patients. Support Care Cancer. 2024;32(5):280. doi:10.1007/s00520-024-08462-x
23. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Antiemesis (Version 1.2023). 2023. https://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf.
24. Matsuda Y, Okita K, Furuhata T, et al. Evaluation of the validity of chemotherapy-induced nausea and vomiting assessment in outpatients using the Japanese version of the MASCC antiemesis tool. Support Care Cancer. 2015;23(11):3331–3339. doi:10.1007/s00520-015-2780-z
25. Eghbali M, Negarandeh R, Ebadi A, et al. Psychometric assessment of the Persian version of short clinical scale to measure chemotherapy-induced nausea and vomiting: the MASCC antiemetic tool. Support Care Cancer. 2020;28(9):4353–4359. doi:10.1007/s00520-019-05281-3
26. Janelsins MC, Tejani MA, Kamen C, et al. Current pharmacotherapy for chemotherapy-induced nausea and vomiting in cancer patients. Expert Opin Pharmacother. 2013;14(6):757–766. doi:10.1517/14656566.2013.776541
27. Hesketh PJ, Kris MG, Basch E, et al. Antiemetics: ASCO Guideline Update. J Clin Oncol. 2020;38(24):2782–2797. doi:10.1200/JCO.20.01296
28. Roila F, Molassiotis A, Herrstedt J, et al. 2016 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting and of nausea and vomiting in advanced cancer patients. Ann Oncol. 2016;27(suppl 5):v119–v133. doi:10.1093/annonc/mdw270
29. Berger MJ, Ettinger DS, Aston J, et al. NCCN guidelines insights: antiemesis, version 2.2017. J Natl Compr Canc Netw. 2017;15(7):883–893. doi:10.6004/jnccn.2017.0117
30. Burmeister H, Aebi S, Studer C, et al. Adherence to ESMO clinical recommendations for prophylaxis of chemotherapy-induced nausea and vomiting. Support Care Cancer. 2012;20(1):141–147. doi:10.1007/s00520-010-1079-3
31. Gilmore JW, Peacock NW, Gu A, et al. Antiemetic guideline consistency and incidence of chemotherapy-induced nausea and vomiting in US community oncology practice: INSPIRE Study. J Oncol Pract. 2014;10(1):68–74. doi:10.1200/JOP.2012.000816
32. Yu S, Burke TA, Chan A, et al. Antiemetic therapy in Asia Pacific countries for patients receiving moderately and highly emetogenic chemotherapy--a descriptive analysis of practice patterns, antiemetic quality of care, and use of antiemetic guidelines. Support Care Cancer. 2015;23(1):273–282. doi:10.1007/s00520-014-2372-3
33. Mosa ASM, Hossain AM, Yoo I. A dynamic prediction engine to prevent chemotherapy-induced nausea and vomiting. Artif Intell Med. 2020;109:101925. doi:10.1016/j.artmed.2020.101925
34. Grunberg SM, Deuson RR, Mavros P, et al. Incidence of chemotherapy-induced nausea and emesis after modern antiemetics. Cancer. 2004;100(10):2261–2268. doi:10.1002/cncr.20230
35. Affronti ML, Schneider SM, Herndon JE, et al. Adherence to antiemetic guidelines in patients with malignant glioma: a quality improvement project to translate evidence into practice. Support Care Cancer. 2014;22(7):1897–1905. doi:10.1007/s00520-014-2136-0
36. Xu YH, Zhou JQ, Zhou SS, et al. Adherence analysis of the antiemetic guidelines for chemotherapy-induced nausea and vomiting. China Pharm. 2021;30(24):125–127.
37. Zeng C, Jin YZ, Li T, et al. Chemotherapy-induced nausea and vomiting among cancer patients in Shanghai: a cross-sectional study. China Oncol. 2023;33(11):1009–1017. doi:10.19401/j.cnki.1007-3639.2023.11.006.
38. Hesketh PJ, Grunberg SM, Gralla RJ, et al. The oral neurokinin-1 antagonist aprepitant for the prevention of chemotherapy-induced nausea and vomiting: a multinational, randomized, double-blind, placebo-controlled trial in patients receiving high-dose cisplatin--the aprepitant protocol 052 study group. J Clin Oncol. 2003;21(22):4112–4119. doi:10.1200/JCO.2003.01.095
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.