Back to Journals » International Journal of General Medicine » Volume 14
Impact of Computed Tomography-Quantified Emphysema Score on Clinical Outcome in Patients with COVID-19
Authors Lim JK ![]() , Park B
, Park B ![]() , Park J, Choi KJ, Jung CY, Kim YH, Kim JY, Moon S
, Park J, Choi KJ, Jung CY, Kim YH, Kim JY, Moon S ![]() , Lee YH, Lee J
, Lee YH, Lee J ![]()
Received 24 April 2021
Accepted for publication 28 June 2021
Published 12 July 2021 Volume 2021:14 Pages 3327—3333
DOI https://doi.org/10.2147/IJGM.S317295
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jae-Kwang Lim,1 Byunggeon Park,1 Jongmin Park,1 Keum-Ju Choi,2 Chi-Young Jung,2 Young Hwan Kim,3 Jin Young Kim,4 Sungjun Moon,5 Yong Hoon Lee,6 Jaehee Lee6
1Department of Radiology, School of Medicine, Kyungpook National University, Daegu, Republic of Korea; 2Department of Internal Medicine, Daegu Catholic University School of Medicine, Daegu, Republic of Korea; 3Department of Radiology, Daegu Catholic University School of Medicine, Daegu, Republic of Korea; 4Department of Radiology, Dongsan Hospital, Keimyung University School of Medicine, Daegu, Republic of Korea; 5Department of Radiology, College of Medicine, Yeungnam University, Daegu, Republic of Korea; 6Department of Internal Medicine, School of Medicine, Kyungpook National University, Daegu, Republic of Korea
Correspondence: Jaehee Lee
Department of Internal Medicine, School of Medicine, Kyungpook National University, 680 Gukchaebosang-ro, Jung-gu, 41944, Daegu, Republic of Korea
Tel +82-53-420-5536
Fax +82-53-426-2046
Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is considered a risk factor for poor outcomes in patients with coronavirus disease 2019 (COVID-19). However, data on the prognostic impact of radiological emphysema extent on patients with COVID-19 are limited. Thus, this study aimed to examine whether computed tomography (CT)-quantified emphysema score is associated with a worse clinical outcome in patients with COVID-19.
Methods: Volumetric quantitative analyses of CT images were performed to obtain emphysema scores in COVID-19 patients admitted to four tertiary referral hospitals in Daegu, South Korea, between February 18 and March 25, 2020. Patients were divided into three groups according to emphysema score (emphysema score ≤ 1%, 1%< emphysema score ≤ 5%, and emphysema score > 5%).
Results: A total of 146 patients with confirmed SARS-CoV-2 infection were included. The median emphysema score was 1.0% (interquartile range, 0.5– 1.8%). Eight patients (6%) had a previous COPD diagnosis. Eighty (55%), 55 (38%), and 11 (8%) patients had emphysema scores ≤ 1%, between 1% and 5%, and > 5%, respectively. The number of patients who received oxygen therapy two weeks after admission was significantly higher in the group with emphysema scores > 5% than in other groups (p=0.025). The frequency of deaths was three (27%) in the group with emphysema scores > 5% and tended to be higher than that in other groups. Multivariate analysis revealed that age, COPD, and serum lactate dehydrogenase levels were associated with a greater risk of in-hospital mortality in patients with COVID-19.
Conclusion: The current study demonstrated that patients with CT-quantified emphysema scores > 5% tended to progress to severe disease over time; however, they did not exhibit an increased risk of mortality in our COVID-19 cohort. Further studies with consideration of both emphysema extent and airflow limitation degree are warranted.
Keywords: COVID-19, emphysema, computed tomography, COPD, mortality
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has culminated in a global health emergency. The clinical spectrum of COVID-19 ranges from asymptomatic infection to critical and fatal illness. Cough, fever, and dyspnea are the most common symptoms, whereas diarrhea, sore throat, and smell or taste abnormalities are less commonly described.1 Older patients with comorbidities are at a high risk of poor COVID-19 outcomes.2–5 Chronic obstructive pulmonary disease (COPD), a common chronic respiratory disease, is reasonably expected to have a significant impact on the risk of severe COVID-19. Although there are conflicting data on COVID-19 in patients with COPD, recent studies have reported a significant association between COPD and an increased risk of severe COVID-19.5–8 However, COPD has been under-represented among comorbidities reported in patients with COVID-19 compared with the estimated COPD prevalence in the general population.9–11 Thus, the additional risk of more severe manifestations of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in patients with COPD requires further clarification.
Emphysema is easily and accurately detected using chest computed tomography (CT). The extent of emphysema has been associated with an increased risk of the subsequent development of pneumonia in patients with COPD.12 However, emphysema is often present on CT scan in those without airflow obstruction.13 Further, the severity of emphysema documented on CT scans is a strong independent predictor of respiratory mortality in ever-smokers irrespective of COPD diagnosis.14 To date, little attention has been directed to the clinical implications of CT-diagnosed emphysema extent on pneumonia outcomes regardless of COPD diagnosis.15 Likewise, data regarding the prognostic impact of radiological emphysema extent on patients with COVID-19 are limited. Therefore, this study aimed to examine whether CT-quantified emphysema score is associated with an increased risk of poor outcomes in patients with COVID-19.
Patients and Methods
Study Design and Patients
This was a multicenter, retrospective study on patients with confirmed SARS-CoV-2 infection at four tertiary referral hospitals (Daegu Catholic Medical Center, Keimyung University Dongsan Medical Center, Kyungpook National University Hospital, and Yeungnam University Hospital) in Daegu, South Korea. Patients with COVID-19 who were admitted to the study hospitals between February 18 and March 25, 2020, and underwent chest CT within five days of admission were included in this study. COVID-19 diagnosis was confirmed using the real-time reverse-transcriptase polymerase chain reaction test for SARS-CoV-2 based on nasopharyngeal swabs. The study protocols were reviewed and approved by the Daegu Joint Institutional Review Board and performed in accordance with the principles of the Declaration of Helsinki. The requirement for written informed consent from each patient was waived because of the observational, retrospective nature of this study. Patient information was anonymized and unidentifiable.
Data Collection
Demographic, clinical, and laboratory data were obtained from the patients’ electronic medical records. Comorbidity data included that on hypertension, diabetes mellitus (DM), COPD, coronary artery disease, chronic liver disease, and chronic kidney disease. Clinical outcomes were assessed in terms of oxygen-therapy requirement, intensive care unit (ICU) admission, and in-hospital death.
Quantitative CT Emphysema Analysis
Emphysema scores were calculated using commercially available segmentation software (syngo.via; Siemens Healthineers, Erlangen, Germany). A chest radiologist (B.P.) with 5 years’ experience in chest CT interpretation who was blinded to the patients’ other data evaluated the acquired images by loading them manually into the software program for emphysema quantification. Whole-lung parenchyma were automatically segmented after removing the chest wall, mediastinum, diaphragm, and airway in the CT image. Emphysema percentage was calculated by determining the percentage of lung voxels between −1000 and −950 Hounsfield units for whole-lung voxels.12 All segmented images were reviewed by two independent chest radiologists (B.P. and J.K.L. with 13 years of experience in chest CT interpretation) to consensually certify the accuracy of segmentation.
Statistical Analysis
Data were expressed as medians (interquartile ranges, IQRs) for continuous variables and numbers and percentages for categorical variables. In bivariate analysis, the Mann–Whitney U-test or t-test was used for continuous variables and the χ2 or Fisher’s exact test for categorical variables. To identify factors associated with in-hospital mortality in patients with COVID-19, variables with p values <0.1 in the univariate analysis were included in the multivariate logistic regression analysis. All statistical procedures were performed using SPSS software (version 24.0; SPSS Inc., Chicago, IL, USA).
Results
During the study period, 236 patients with confirmed SARS-CoV-2 infection underwent chest CT scans. Among them, 146 patients with available chest CT scans obtained within five days of admission were analyzed. The median emphysema score was 1.0% (IQR, 0.5–1.8%). Representative images of emphysema quantification are shown in Figure 1. Patients were divided into three groups according to emphysema score (emphysema score ≤1%, 1%< emphysema score ≤5%, and emphysema score >5%) based on a previous study.16 Among the 146 patients, 80 (55%), 55 (38%), and 11 (8%) had emphysema scores ≤1%, between 1% and 5%, and >5%, respectively. The median emphysema scores were 0.5% (IQR, 0.2–0.9%), 1.8% (IQR, 1.2–2.0%), and 8.0% (IQR, 5.0–13.0%) in groups with emphysema scores ≤1%, >1% and ≤5%, and >5%, respectively (Table 1).
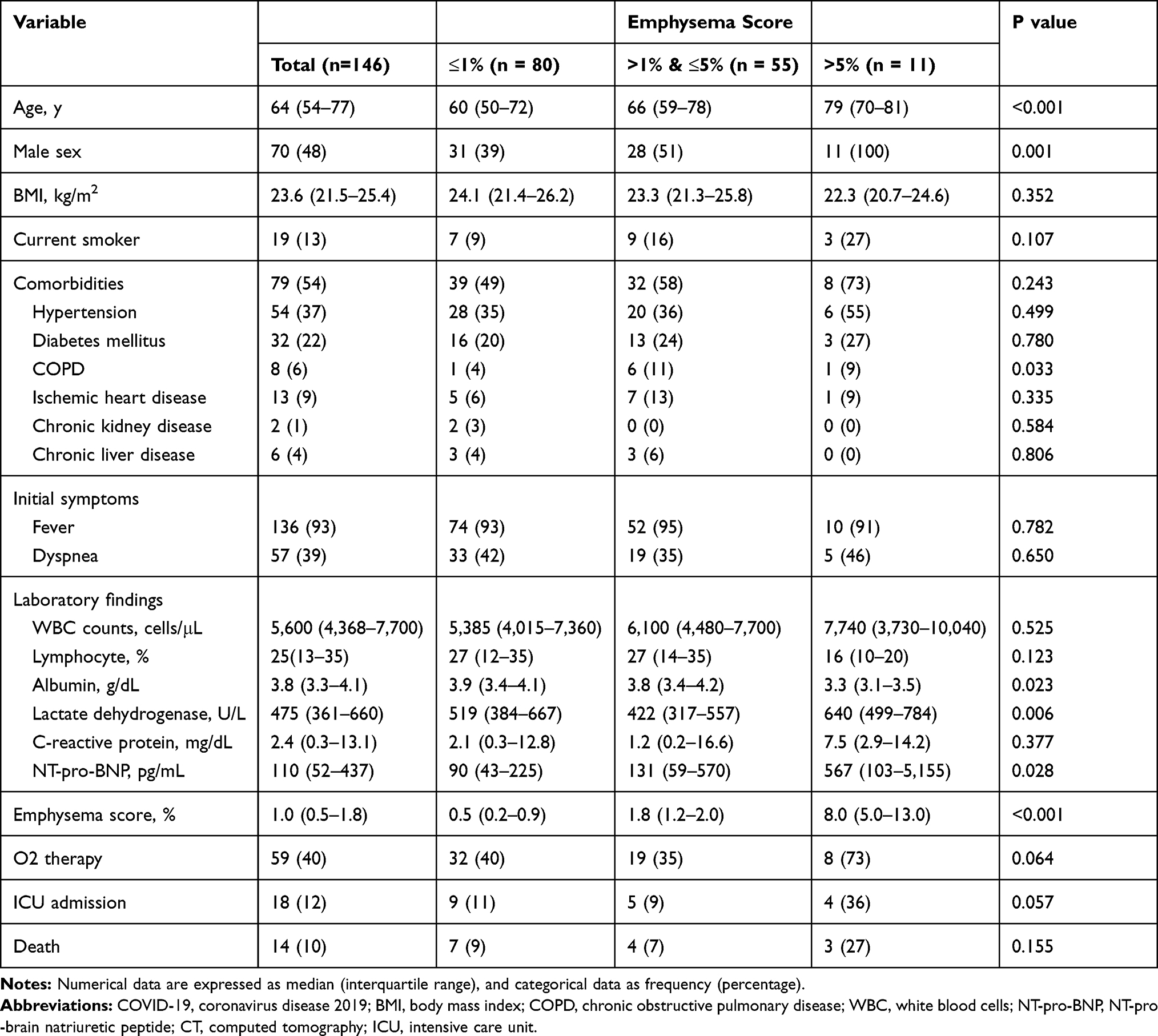 |
Table 1 Comparison of Clinical and Laboratory Findings and Clinical Outcomes in Patients with COVID-19 According to Quantitative Emphysema Scores by Computed Tomography |
 |
Figure 1 Representative images of emphysema quantification: Emphysema area (green color) was automatically calculated under thresholds of –950 HU on computed tomography axial images. Application of quantification software revealed that the percentage of emphysema was 1.0% of the entire lung tissue in a 53-year-old woman (A), 6.0% in an 82-year-old man (B), and 13.0% in a 73-year-old man (C). |
Comparison of Clinical and Laboratory Findings in Patients with COVID-19 According to CT-Quantified Emphysema Scores
Clinical and laboratory findings were compared between the emphysema-score groups (Table 1). The median age and proportion of male subjects of the overall study population were 64 years (IQR, 54–77) and 48%, respectively, and increased with increasing emphysema-score category (p<0.001 and p=0.001, respectively). There were no significant differences in body mass index; frequency of comorbidities, except COPD; and initial symptoms between the groups. In total, eight patients (6%) had a previous diagnosis of COPD. COPD frequency was higher in the group with emphysema scores >1% and ≤5% and that with scores >5% than in the group with emphysema scores ≤1% (p=0.033).
White blood cell counts, C-reactive protein (CRP) levels, and lymphocyte proportions were comparable between the three groups (Table 1). Meanwhile, the group with emphysema scores >5% exhibited relatively lower albumin levels (p=0.023) and higher lactate dehydrogenase (LDH) and N-terminal fragment B-type natriuretic peptide (NT-proBNP) levels (p=0.006 and p=0.028, respectively).
Comparison of Clinical Outcomes in Patients with COVID-19 According to CT-Quantified Emphysema Scores
In total, there were 59 (40%) patients with severe COVID-19 requiring oxygen therapy during hospitalization. There was no significant difference in the proportion of patients requiring oxygen therapy on admission between the three groups (Figure 2). However, the number of patients who received oxygen therapy two weeks after admission was significantly higher in the group with emphysema scores >5% than in the group with emphysema scores >1% and ≤5% and that with scores ≤1% (55% vs 26% vs 18%, p=0.025).
 |
Figure 2 The proportion of patients who received oxygen therapy during hospitalization in the groups with different emphysema scores *p < 0.05. |
There were 18 (12%) patients with severe COVID-19 requiring ICU admission and 14 (10%) deaths, respectively, in the whole study population. Four (36%) cases required ICU admission in the group with emphysema scores >5%, a figure that was relatively higher than that in other groups (p=0.057). Similarly, three deaths (27%) occurred in the group with emphysema scores >5%, a figure that was relatively higher than that in other groups but without statistical significance.
Among the eight patients with previous diagnoses of COPD, those who required oxygen therapy and ICU admission were 7 (88%) and 4 (50%), respectively. Significant differences were observed in the numbers requiring oxygen therapy and ICU admission between patients with COPD and those without (oxygen therapy: 7 [88%] vs 52 [38%], p=0.008; ICU admission: 4 [50%] vs 14 [10%], p=0.008). In addition, in-hospital death occurred in four patients (50%) with COPD and 10 (7%) without COPD, indicating a significant difference (p=0.003).
Analysis of Factors Associated with in-Hospital Mortality in Patients with COVID-19
From univariate analysis, variables associated with increased mortality in patients with COVID-19 included age; male sex; DM; COPD; the proportion of lymphocytes; and levels of serum albumin, LDH, CRP, and NT-proBNP (Table 2). CT emphysema scores >5% tended to be associated with an increased risk of mortality in patients with COVID-19 (p=0.053). However, multivariate analysis revealed that age (odds ratio [OR] = 1.069 [CI, 1.001–1.141]), COPD (OR = 8.068 [CI, 1.195–54.486]), and serum LDH levels (OR = 1.002 [CI, 1.001–1.004]) were independently associated with a greater risk of in-hospital mortality in patients with COVID-19.
 |
Table 2 Univariate and Multivariate Analyses for Factors Associated with in-Hospital Mortality of Patients with COVID-19 |
Discussion
In this study, we initially evaluated whether the CT-quantified emphysema score is associated with an increased risk of in-hospital mortality in patients with COVID-19, given the altered local and systemic immunity of emphysema.17 We found that the CT emphysema score itself was not associated with an increased risk of mortality in patients with COVID-19. However, COVID-19 patients with CT emphysema scores >5% initially presented relatively lower albumin and higher LDH levels and were more likely to require oxygen therapy and ICU admission during hospitalization than those with relatively lower emphysema scores. In addition, patients with emphysema scores >5% and those with relatively lower emphysema scores exhibited increased and decreased proportions of oxygen-therapy requirement over time during hospitalization, respectively. This finding is consistent with that of a recent study, which revealed more severe community-acquired pneumonia in patients with emphysema than that in those without emphysema regardless of COPD diagnosis.15 In addition, this previous study reported a higher 30-day mortality rate in the severe emphysema group than that in the control group. However, the CT-quantified emphysema score was not an independent risk factor for mortality in our COVID-19 cohort. A relatively lower degree of emphysema of our study population might have had negative effects on the evaluation of the clinical significance of emphysema. We could not identify the presence of airflow limitation using spirometry. Given that approximately 6% of the patients with COVID-19 had a previous diagnosis of COPD in this study, most of the study population would not have airflow limitations. Radiological mild emphysema without airflow limitation might have had a relatively lower impact on poor outcomes in patients with COVID-19. Thus, further research is required to evaluate the clinical significance of both emphysema extent and airflow limitation in COVID-19 using large patient samples.
There is growing evidence that indicates a significant association of COPD with COVID-19 severity and mortality.5–8,18 The frequency of previous COPD diagnoses in our COVID-19 cohort was consistent with the pooled prevalence of COPD in hospitalized COVID-19 patients.19 Similarly, the present study revealed an association between COPD and the increased risk of in-hospital mortality, corroborating previous study findings. COPD patients are usually older and have more comorbidities, thus predisposing them to an increased risk of worse outcomes from COVID-19. In the future, different COPD phenotypes should be studied to identify differences in clinical manifestations of SARS-CoV-2 infection. Additionally, age and serum LDH levels, well-known risk factors for mortality in patients with COVID-19, were found to be associated with an increased risk of in-hospital COVID-19 mortality in this study.5,18 Careful monitoring for disease deterioration is required in those with these risk factors for mortality.
Our study has certain limitations. First, it is highly probable that the most severe patients were excluded from this analysis because they were too ill to be transferred to the x-ray department for CT scans. Second, data regarding pulmonary function tests and COPD medications were not available due to the overburdening of the healthcare system posed by the COVID-19 outbreak; hence, the association between airflow obstruction and quantitative CT emphysema scores or between mortality and COPD drug use could not be assessed.
In conclusion, the current study demonstrated that patients with CT-quantified emphysema scores >5% were more likely to progress to severe disease over time, whereas the CT-quantified emphysema score was not an independent risk factor for mortality in our COVID-19 cohort. Further, this study’s findings provide additional evidence that corroborates previous study findings in which age, COPD, and LDH level were found to be risk factors for poor COVID-19 outcomes. Further assessments with consideration of both emphysema extent and airflow limitation degree are required using larger COVID-19-patient samples.
Abbreviations
COVID-19, coronavirus disease 2019; COPD, chronic obstructive pulmonary disease; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; CT, computed tomography; ICU, intensive care unit; DM, diabetes mellitus; LDH, lactate dehydrogenase; CRP, C-reactive protein; NT-proBNP, N-terminal fragment B-type natriuretic peptide.
Author Contributions
Each author made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; participated in drafting, revising, or critically reviewing the article; provided final approval of the version to be published; agreed on the journal to which the article has been submitted; and agrees to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare regarding the publication of this manuscript.
References
1. De Vito A, Fiore V, Princic E, et al. Predictors of infection, symptoms development, and mortality in people with SARS-CoV-2 living in retirement nursing homes. PLoS One. 2021;16:e0248009. doi:10.1371/journal.pone.0248009
2. Hu L, Chen S, Fu Y, et al. Risk factors associated with clinical outcomes in 323 Coronavirus Disease 2019 (COVID-19) hospitalized patients in Wuhan, China. Clin Infect Dis. 2020;71:2089–2098. doi:10.1093/cid/ciaa539
3. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–1062. doi:10.1016/S0140-6736(20)30566-3
4. Du RH, Liang LR, Yang CQ, et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: a prospective cohort study. Eur Respir J. 2020;55.
5. Parohan M, Yaghoubi S, Seraji A, et al. Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: a systematic review and meta-analysis of observational studies. Aging Male. 2020;1–9.
6. Lippi G, Henry BM. Chronic obstructive pulmonary disease is associated with severe coronavirus disease 2019 (COVID-19). Respir Med. 2020;167:105941. doi:10.1016/j.rmed.2020.105941
7. Zhao Q, Meng M, Kumar R, et al. The impact of COPD and smoking history on the severity of Covid-19: a systemic review and meta-analysis. J Med Virol. 2020;92(10):1915–1921. doi:10.1002/jmv.25889
8. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: a rapid systematic review and meta-analysis. PLoS One. 2020;15:e0233147. doi:10.1371/journal.pone.0233147
9. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323:1061–1069. doi:10.1001/jama.2020.1585
10. Guan WJ, Liang WH, Zhao Y, et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. Eur Respir J. 2020;55.
11. Halpin DMG, Faner R, Sibila O, et al. Do chronic respiratory diseases or their treatment affect the risk of SARS-CoV-2 infection? Lancet Respir Med. 2020;8:436–438. doi:10.1016/S2213-2600(20)30167-3
12. Gevenois PA, De Vuyst P, de Maertelaer V, et al. Comparison of computed density and microscopic morphometry in pulmonary emphysema. Am J Respir Crit Care Med. 1996;154:187–192. doi:10.1164/ajrccm.154.1.8680679
13. Omori H, Nakashima R, Otsuka N, et al. Emphysema detected by lung cancer screening with low-dose spiral CT: prevalence, and correlation with smoking habits and pulmonary function in Japanese male subjects. Respirology. 2006;11:205–210. doi:10.1111/j.1440-1843.2006.00827.x
14. Johannessen A, Skorge TD, Bottai M, et al. Mortality by level of emphysema and airway wall thickness. Am J Respir Crit Care Med. 2013;187:602–608. doi:10.1164/rccm.201209-1722OC
15. Seo H, Cha SI, Shin KM, et al. Clinical relevance of emphysema in patients hospitalized with community-acquired pneumonia: clinical features and prognosis. Clin Respir J. 2021. doi:10.1111/crj.13370
16. Labaki WW, Xia M, Murray S, et al. Quantitative emphysema on low-dose CT imaging of the chest and risk of lung cancer and airflow obstruction: an analysis of the National Lung Screening Trial. Chest. 2021;159:1812–1820. doi:10.1016/j.chest.2020.12.004
17. Farr BM, Bartlett CL, Wadsworth J, et al. Risk factors for community-acquired pneumonia diagnosed upon hospital admission. British Thoracic Society Pneumonia Study Group. Respir Med. 2000;94:954–963. doi:10.1053/rmed.2000.0865
18. Liu W, Tao ZW, Wang L, et al. Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin Med J (Engl). 2020;133:1032–1038. doi:10.1097/CM9.0000000000000775
19. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382:1708–1720. doi:10.1056/NEJMoa2002032
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.