Back to Journals » Risk Management and Healthcare Policy » Volume 18
Impact of Artificial Intelligence-Assisted Closed-Loop Mobile Nursing Information Management on Nursing Quality Indicators and Work Efficiency
Authors Yuan X, Zhu L, Jiang K, Chen J
Received 2 July 2025
Accepted for publication 4 October 2025
Published 5 November 2025 Volume 2025:18 Pages 3581—3591
DOI https://doi.org/10.2147/RMHP.S548275
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Xing Yuan,* Lihong Zhu,* Kaili Jiang, Jinyan Chen
Department of Pediatric Surgery, Anqing Municipal Hospital, Anqing, Anhui Province, 246000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xing Yuan, Department of Pediatric Surgery, Anqing Municipal Hospital, NO. 87 Tianzhushan East Road, Anqing, 246000, Anhui Province, People’s Republic of China, Tel +86 0556 5836117, Fax +8605565223906, Email [email protected]
Objective: This study aimed to construct and evaluate an AI-assisted mobile nursing information closed-loop management model.
Methods: This study adopted a prospective before-after control design to compare nursing indicators before and after model implementation, conducted in the Pediatric Surgery Department of Anqing Municipal Hospital Affiliated with China Pharmaceutical University, where an information management system was implemented. A statistical analysis was conducted on the quality control data of 3891 cases (from 438 hospitalized patients) before model implementation (March to May 2024) and 3697 cases (from 417 patients) after implementation (July to September 2024) to evaluate its effectiveness. Existing quality control indicators were reviewed, and new/updated metrics generated from the implementation of new nursing closed-loop management measures were evaluated. AI-driven tools were leveraged to enhance the early warning capabilities of mobile nursing information systems through data acquisition, collection, and interpretation, and establishing a closed-loop management model for mobile nursing information.
Results: Following the model implementation, significant improvements were observed in all evaluated indicators. The bedside settlement completion rate rose from 66.16% to 83.3% (χ²=61.63, *p*< 0.001), and the critical value reception rate increased from 51.72% to 93.55% (χ²=21.78, *p*< 0.001). The nursing plan and workflow completion rates improved to 98.17% and 94.89% (both *p*< 0.001), respectively. Nursing work efficiency surged from 3.03 to 25 tasks per hour, and overall patient satisfaction increased from 83.3% to 97.65%, confirming the model’s effectiveness in enhancing nursing quality and patient experience.
Conclusion: The AI-assisted mobile nursing information closed-loop management model presented here was found to enhance nursing work efficiency, improve patient experience, and optimize workflow processes, contributing to a more effective and structured nursing management system.
Keywords: AI-assisted, mobile nursing information system, nursing closed-loop management, nursing quality, process optimization
Introduction
Artificial Intelligence (AI) refers to the technology of simulating human intelligent behavior through computers, enabling machines to possess the capabilities of learning, reasoning, problem-solving, and decision-making. In recent years, AI has been widely applied in the healthcare field. By combining AI-driven tools with nursing information systems through the steps of pre-input training, writing instructional prompts, and inputting commands, it can automatically identify abnormal patterns through data processing and analysis, reduce human errors, and thus improve work efficiency and nursing quality.1,2
Closed-loop management originates from automatic control theory, where it refers to a continuous improvement cycle of “decision-control-feedback”.3 In healthcare, closed-loop management has been widely used in clinical blood use, safe drug use, and critical value management.4,5 For instance, Zhang et al (2021) demonstrated that closed-loop management significantly reduced nursing interruption risks by 24.6% in a quasi-experimental study, improving medication administration accuracy and workflow efficiency.6 Bhangu et al (2022) further applied closed-loop management in trauma care, identifying team performance improvements through closed-loop communication analysis.7 The core principle of this approach involves establishing clear objectives, implementing real-time monitoring and feedback mechanisms, and promptly identifying and addressing issues to enhance overall management effectiveness.2,8
The advancement of health information technology (HIT), including clinical decision support systems (CDSS) and electronic health records (EHR), has significantly contributed to the transformation and innovation of nursing service delivery models.9 For example, an acute abdominal pain patient admitted via emergency, registration creates EMPI on evaluation platform. Ward physician issues e-orders linked to hospital-wide dictionary, synced to nursing/pharmacy. Nursing station generates assessment template, retrieving past allergy/medication history from EHR. Nurses use mobile terminals to scan wristbands, access order executions, record vitals. System compares vitals with KB thresholds, alerts for abnormalities (eg, HR>100bpm), links lab reports for evaluation. At discharge, physician generates summary with auto-extracted records. Nursing updates discharge instructions, links to meds module. System verifies record completeness.
In 2023, the hospital underwent evaluation and achieved the fifth level of electronic health record application, continuously enhancing the informatization of nursing care. This progress has facilitated dynamic monitoring of nursing quality indicators and supported the transition towards a more digitalized, refined, and comprehensive nursing quality management model. AI has emerged as a key technology in nursing informatics, with studies highlighting its potential in data analysis and risk prediction. For example, Wei et al (2025) reviewed AI applications in nursing, emphasizing its role in clinical decision-making and patient education.10 Ruksakulpiwat et al (2024) conducted a systematic review and identified AI-driven tools for nursing care, though noted challenges in data privacy and technical reliability.11 McGrow (2025) further discussed AI’s transition from data processing to wisdom generation in nursing, advocating for enhanced nurse-AI collaboration.12 Gonzalez-Garcia et al (2024) reported that AI-based systems improved nurse management efficiency by 18.3% in a systematic review.13 Benefiting from these changes, AI has enabled nurses to shift from routine tasks to patient-centered advanced care, such as clinical decision-making, personalized patient education, and emotional support. Meanwhile, it has homogenized nursing quality across departments and improved management efficiency. Consequently, nursing quality control indicators and management frameworks have undergone continuous optimization and refinement.
By analyzing data generated through the AI-assisted mobile nursing information closed-loop management model, consisting of an AI-driven keyboard that integrating intelligent functions (including data statistical analysis, charting, table creation, mind mapping, AI Q&A) with the nursing information system, data-driven decision-making has been enhanced, contributing to the refinement of nursing quality control standards and the establishment of a closed-loop quality management system tailored to mobile nursing.14 This approach enhances the efficiency of nursing quality control, improves the quality of care, increases nursing work efficiency, and optimizes the overall patient experience.
Information and Methods
General Data
In March 2024, the Pediatric Surgery Department of Anqing Municipal Hospital Affiliated with Anhui Medical University initiated the implementation of a mobile nursing information closed-loop management system using mobile nursing terminals. Nursing quality control data collected from March to May 2024, prior to full implementation of the mobile nursing terminal system, were designated as the pre-implementation group. Data collected from July to September 2024, after the system had been fully implemented, constituted the post-implementation group for comparative analysis. Quality control data of 3891 patient admissions (or 3891 instances of patient care) from 438 hospitalized patients before model implementation (March to May 2024) and 3697 instances from 417 patients after implementation (July to September 2024) were statistically analyzed to evaluate its effectiveness.
Methods
Establishment of the Nursing Information Quality Management Team
A mobile nursing information management team was established based on the department’s existing nursing quality control management team (Figure 1). The organizational structure for quality control and mobile nursing information management was refined, with a clearly defined division of responsibilities across decision-making, support, and implementation levels. An AI-driven keyboard that covered intelligent functions (such as data statistics and analysis, charting, table creation, mind mapping, and AI Q&A) was leveraged and integrated with the nursing information system.
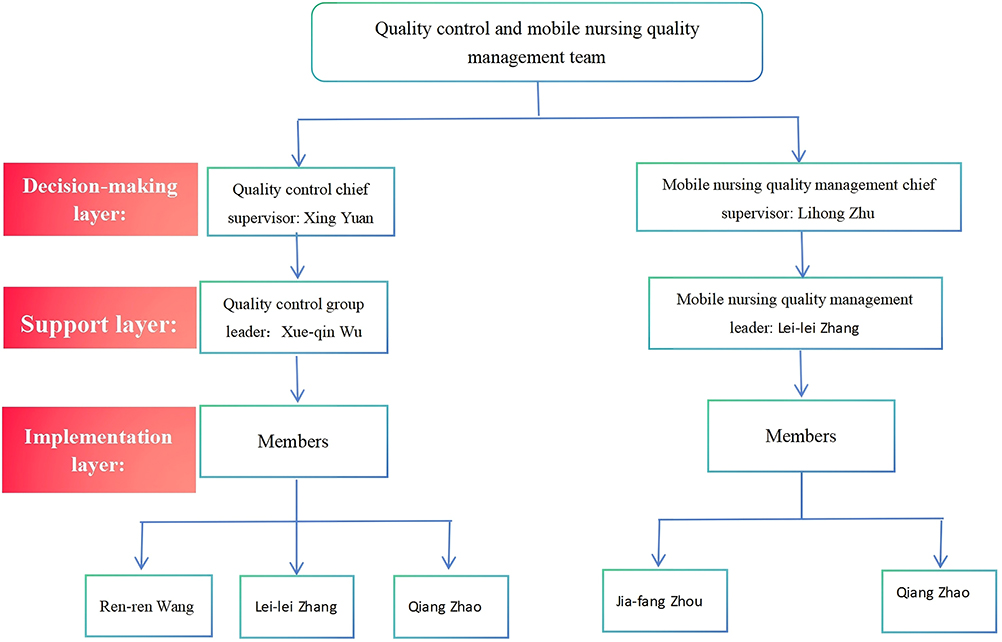 |
Figure 1 Construction of the mobile nursing information management team. Decision-making layer: This layer is responsible for team creation, development of work systems, overseeing overall coordination, and organizational management coordination. Support layer: This layer is responsible for coordinating decisions, coordinating organizational activities, personnel management, task guidance and allocation. Implementation layer: This layer is responsible for implementing mobile nursing information closed-loop management processes. |
Training programs on information system-related knowledge and practical applications were conducted in various formats. An emergency response protocol for the department’s information system was established, and emergency drills were implemented to enhance preparedness. Additionally, a mobile nursing information evaluation standard was formulated, incorporating key monitoring points for nursing procedures and closed-loop management processes.
The management team assumed responsibility for data analysis, process optimization, and standard development, in addition to overseeing staff training, performance assessment, system application, decision-making, control, and feedback. Continuous quality improvement measures were implemented to enhance the efficiency and effectiveness of mobile nursing information management.15
Establishment of Quality Control Indicators
Completion Rate of Nursing Information Data Closed-Loop Management
The completion rate of nursing information data closed-loop management refers to the proportion of information management processes successfully completed within the nursing information system during a specified period.
It is calculated using the following formula: The completion rate of nursing information data closed-loop management = (Number of cases with completed closed-loop management in the nursing information system, including critical value effective receipt, specimen collection, effective rounds, and bedside settlement, within the specified period) / (Total number of cases of all information data (including critical value effective receipt, specimen collection, effective rounds, and bedside settlement) in the nursing information system within the specified period) * 100%.
Bedside Settlement Completion Rate
The bedside settlement completion rate assesses the proportion of patient discharge settlements conducted through the bedside settlement system, which facilitates discharge procedures and enhances the patient experience.
It is calculated as follows: Bedside settlement completion rate = (Number of patients who completed bedside settlement per month) / (Total number of patients discharged per month) * 100%.
Effective Follow-up Completion Rate
The effective follow-up completion rate reflects the extent to which health education and post-discharge care are provided to discharged patients, as documented in the electronic follow-up system.
The calculation formula is as follows: Effective follow-up completion rate = (Number of patients who responded normally to follow-up calls per month) / (Total number of discharged patients per month) * 100%.
Critical Value Effective Receipt Rate
The critical value effective receipt rate measures the efficiency of the early warning mechanism for significantly abnormal test results that indicate potentially severe or life-threatening conditions. This metric reflects the timeliness of notifying the responsible physician for prompt intervention.
It is calculated as follows: Critical value effective receipt rate = (Number of critical values received within 5 minutes per month) / (Total number of critical values reported per month) * 100%.
Specimen Collection Execution Rate
The specimen collection execution rate measures adherence to standardized procedures for medical order execution following patient identification using mobile nursing terminals (personal digital assistants, PDAs) during specimen collection. Strict implementation of the verification system ensures patient safety throughout the process.
It is calculated as follows: Specimen collection execution rate = (Number of cases with completed closed-loop management for specimen collection per month) / (Total number of specimen collection cases per month) * 100%.
Effective Rounds Completion Rate
The effective rounds completion rate evaluates the implementation of graded nursing rounds based on patient conditions, incorporating mobile nursing terminals for infusion rounds.
It is calculated as follows: Effective rounds completion rate = (Number of timely rounds per month) / (Total number of rounds per month) * 100%.
Data Analysis and Current Status Assessment
Data were extracted from the electronic health record (EHR) system to evaluate the execution status of key monitoring indicators in the department’s mobile nursing information system. Statistical analyses were conducted using SPSS 25.0 software. The chi-squared (χ²) test was applied to compare categorical variables between groups with p < 0.05, indicating a statistically significant difference. All outcome indicators in this study (such as bed-side settlement completion rate, critical value reception rate, etc.) were categorical variables (dichotomous: completed / not completed), and the data between groups were independent samples (pre-implementation vs post-implementation). The chi-square test was suitable for comparing differences in categorical variables between independent samples, so this method was selected for inter-group comparison. When applying the chi-square test in this study, the following assumptions were satisfied: (1) All observations are independent of each other (there is no overlap in nursing data of different patients); (2) The expected frequency is ≥ 5 (the sample size of each group is > 30, and it was verified through SPSS that the expected frequency of all cells is > 5); (3) The categorical variables are mutually exclusive and exhaustive (outcomes are only divided into two categories: “completed” and “not completed”).
AI-Assisted Development of a Mobile Nursing Information Closed-Loop Management System
The mobile nursing information closed-loop management system is designed with a patient-centric approach, integrating all stages of nursing care into a cohesive process. The system incorporated a customized AI-driven keyboard equipped with terminal SoC chips, which provide internal flash storage and intelligent voice audio support. This keyboard may enable functions such as intelligent writing, speech recognition, speech translation, and OCR recognition, specifically designed for clinical data analysis, organization, and personalized care customization. By reducing data statistics errors caused by manual entry and homogenizing data analysis, it significantly may enhance nursing work efficiency and supports the digital transformation of care processes. This system enhances the efficiency of nursing quality control, minimizes nursing-related errors, and improves overall care quality, facilitating a transition to a more digitalized and refined management model. To address potential vulnerabilities and safety risks, modifications, reorganizations, and enhancements have been made to the existing workflow. The nursing process has been redesigned and optimized by incorporating continuous data collection, analysis, evaluation, and feedback from process monitoring points. These iterative improvements strengthen the execution of nursing interventions, ensuring the achievement of quality control objectives (Figure 2).
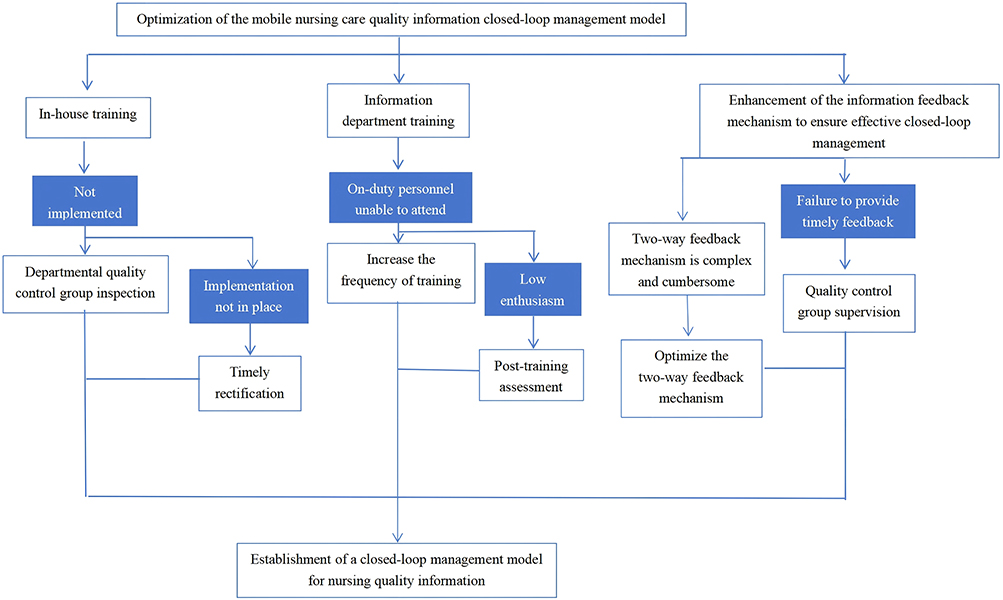 |
Figure 2 AI-assisted mobile nursing information closed-loop management model. Abbreviation: AI, Artificial Intelligence. |
Optimization of the Specimen Collection Process
Prior to specimen collection, patient identity verification is conducted by asking the patient’s name and scanning the barcode on their wristband using a personal digital assistant (PDA). Accurate patient identification is ensured by cross-referencing medical order details and scanning the specimen barcode. Following verification, the specimen tube is labeled and subjected to a secondary confirmation using the PDA. Once accuracy is confirmed, the specimen is collected. After this, the specimen is promptly recorded in the emergency laboratory specimen tracking log, and test results are continuously monitored and reported in real-time for effective result management and oversight.
Optimization of the Bedside Settlement Process
When the attending physician issues a discharge order, the hospital discharge procedure is initiated through digital payment platforms such as WeChat or Alipay by scanning to activate the medical insurance code. During hospitalization, nursing staff ensure that family members complete the required pre-binding of their family account in accordance with the hospital’s procedural guidelines. The head nurse verifies the final charges, initiates the discharge process, and notifies the family members to proceed with payment. Upon settlement, family members present the discharge records and diagnosis certificates at the nursing station, where the head nurse verifies the information. Once the correct refund amount is credited, the final discharge summary is printed and reviewed for accuracy before completing the discharge process.
Optimization of the Critical Value Reporting Process
When critical values are identified and confirmed by auxiliary departments, they are communicated to the relevant departments via telephone and the Hospital Information System (HIS). Upon receiving the notification, the relevant nurse promptly confirms receipt within the HIS system and informs the attending physician. The physician then verifies the critical value and initiates the appropriate medical treatment. The nurse continuously monitors the patient’s condition, follows medical orders, and documents all relevant actions in the nursing records. To ensure continuity of care, the information is effectively communicated during shift handovers, and ongoing follow-up is conducted as necessary. Additionally, all critical values are systematically documented in the temporary “Critical Value Registration Log” for record-keeping and quality control.
Development of Standardized Flowcharts
After the process optimization and protocol formulation, a standardized flowchart is developed to ensure procedural consistency and serve as an operational guide and training reference. The flowchart incorporates decision-making algorithms for data interpretation and process flow adjustments. Additionally, protocols for addressing anomalies, such as data discrepancies or mismatches, are established, outlining whether the operation should be terminated or redirected to the verification process. Furthermore, contingency measures for managing network disruptions or equipment malfunctions are integrated to maintain continuity and accuracy in nursing operations.
Implementation of AI-Based Retrieval in Quality Management
Clinical quality management presents significant complexities, with notable variability in data analysis proficiency among nurses at different levels of expertise. Nurses often lack a thorough understanding of quality analysis tools, resulting in ineffective analysis. Furthermore, the extensive workload associated with clinical nursing, combined with numerous quality supervision tasks, adversely affects efficiency. Traditional quality audits involve manual compilation of inspection results, scoring, issue categorization, and report generation, a process that is both labor-intensive and susceptible to manual entry errors, potentially compromising data accuracy.
To address these challenges, an AI-driven retrieval model was integrated into the mobile nursing information management system, accompanied by AI retrieval training for nursing staff. The adoption of AI retrieval technology facilitates real-time monitoring and assessment of nursing quality, providing objective data to support continuous improvements in clinical practice. This approach standardizes data statistics, reduces workload, and enhances work efficiency (Figure 3).
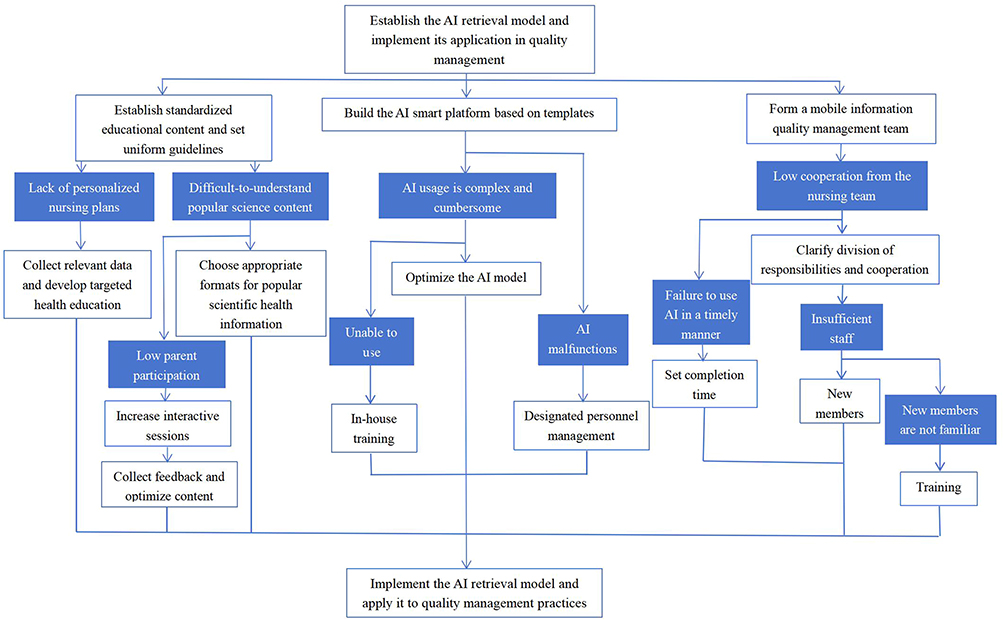 |
Figure 3 Application of the AI retrieval model in nursing quality management. Abbreviation: AI, Artificial Intelligence. |
Additionally, AI-driven analytics enable the development of personalized nursing plans based on patient-specific information, including medical history and behavior patterns, thereby optimizing nursing interventions. Patient health education is a key component in enhancing nursing effectiveness. Through AI technology, customized health education materials can be tailored to individual patient conditions and cognitive levels, ensuring appropriate content delivery in accessible formats.16 This approach enhances patient awareness of health conditions, promotes self-management skills, supports recovery, and aligns with individualized patient needs, ultimately enhancing the overall patient experience.
Results
Bedside Settlement Completion Rate
Data on bedside settlement execution between March 2024 and September 2024 were analyzed to assess the impact of process optimization (Table 1). The bedside discharge settlement completion rate increased from 66.16% prior to implementation to 83.3% post-implementation (χ2 = 61.6284, p < 0.001), significantly reducing the wait time for discharge procedures and further enhancing the patient care experience.
 |
Table 1 Bedside Settlement Completion Rate |
Critical Value Reception Rate
Data on the execution of critical value reception between March 2024 and September 2024 were analyzed (Table 2). The critical value acknowledgment rate improved from 51.72% pre-implementation to 93.55% post-implementation (χ2 = 21.78172195, p < 0.001), demonstrating timely clinician notification of critical patient status, facilitating immediate interventions, and ultimately enhancing patient safety.
 |
Table 2 Critical Value Reception Rate |
Nursing Plan Completion Rate
Data on nursing plan execution between March 2024 and September 2024 were analyzed (Table 3). The nursing care plan completion rate increased from 90.53% pre-implementation to 98.17% post-implementation (χ2 = 114.7585793, p < 0.001), demonstrating the implementation of comprehensive, standardized nursing interventions and improving overall care quality.
 |
Table 3 Nursing Plan Completion Rate |
Nursing Workflow Completion Rate
Data on nursing workflow execution from March 2024 to September 2024 were analyzed (Table 4). The nursing workflow completion rate rose from 73.17% pre-implementation to 94.89% post-implementation (χ2 = 61.30296852, p < 0.001), demonstrating optimized patient needs fulfillment and elevating holistic care quality.
 |
Table 4 Nursing Workflow Completion Rate |
Nursing Work Efficiency
The implementation of AI-assisted nursing quality supervision, feedback, and rectification was associated with an increase in the number of tasks completed per hour, rising from 3.03 tasks per hour pre-implementation to 25 tasks per hour post-implementation.
Patient Experience
A patient experience survey was conducted to evaluate six dimensions: medical environment, admission and discharge services, nursing techniques, humanistic care, effective communication, respect for patient privacy and legal rights, and payment methods. The survey included 20 items, with overall patient satisfaction increasing from 83.3% before implementation to 97.65% after implementation.
Discussion
Effective nursing quality management requires the systematic application of quality control indicators to facilitate evaluation, assessment, and performance measurement. These indicators serve as foundational tools for implementing scientifically grounded quality management systems across healthcare settings. While nursing quality information systems are well-established, previous research indicates that monitoring nursing workflows and control points within closed-loop frameworks remains insufficiently addressed in practice.2,17,18
In this study, AI technology was integrated into nursing quality control processes through structured staff training, real-time data tracking, and intelligent data processing. This integration aligns with prior findings by Wang et al (2024) and Lee and Yoon (2021), who noted the potential of AI to reduce human error and optimize clinical workflows.1,2 Additionally, AI-assisted closed-loop mechanisms enabled timely supervision and feedback on various nursing tasks, as supported by Bhangu et al (2022) and Wei et al (2022), who demonstrated the efficacy of AI-embedded closed-loop systems in clinical environments.19,20
The study employed multiple key indicators, including bedside settlement completion rate, effective follow-up completion rate, critical value receipt rate, specimen collection execution rate, nursing plan completion rate, and workflow execution rate. The improvements observed mirror those of Tsan et al (2021), who reported enhanced nursing workflow effectiveness through mobile app-based interventions.21 These enhancements also corroborate findings from recent research showing that AI-enabled systems streamline patient discharge, reduce nursing documentation time, and improve patient education outcomes.15,22,23
Furthermore, our findings reinforce the importance of data-driven decision-making in nursing management. This perspective is echoed by Chew et al (2022), who highlighted the utility of AI-powered chatbots in tailoring patient education, and McGrow (2025), who emphasized the transition from data to actionable insights in AI-supported nursing environments.16,24 Importantly, these optimizations not only elevate clinical outcomes but also support the shift toward more patient-centered and emotionally supportive care, as noted by Vasquez et al (2023).25
The broader implications of this study suggest that AI-assisted closed-loop systems represent a transformative innovation in nursing quality management. These systems minimize human error, enhance operational efficiency, and allow nurses to reallocate time to direct patient care. Our results echo those of Gonzalez-Garcia et al (2024), who found that AI-based platforms improved nurse task efficiency by over 18%.26
Nonetheless, challenges remain. Some AI tools used in clinical nursing are still in the conceptual or early validation phases, with concerns related to data privacy, interoperability, and user trust. Future research should focus on refining AI algorithms, improving interpretability, and enhancing nurses’ AI literacy to ensure meaningful human–AI collaboration.27–29
This study has several limitations. First, the single-center design (conducted only in the Pediatric Surgery Department of one hospital) may limit the generalizability of findings, as nursing workflows and AI adoption vary across institutions. Second, the short observation period (3 months pre- and post-implementation) prevents assessment of long-term effectiveness, such as system stability over 6 months or more. Third, potential confounding factors (eg, nurse training intensity) were not controlled, which may have influenced outcome improvements. Future studies should address these by conducting multi-center trials with extended follow-up and adjusting for confounding variables.
Conclusion
The implementation of an AI-assisted mobile nursing information closed-loop management model has the potential to transform nursing practices by enhancing the efficiency of nursing quality control, improving overall nursing quality, increasing work productivity, and optimizing the healthcare experience for pediatric patients and their families. Additionally, this model contributes to improved patient safety. The integration of AI represents not only a technological advancement but also an opportunity to introduce fundamental improvements in nursing workflows.
The seamless incorporation of AI into nursing practice facilitates the development of a more efficient, high-quality, and patient-centered nursing service model. To further enhance nursing management, ongoing advancements in AI technology application are essential, fostering the continued evolution of intelligent and efficient nursing processes.
In summary, the integration of AI is not only a technological upgrade but also a crucial opportunity to drive profound changes in nursing work models. The deep integration of AI and nursing practice can jointly shape a more efficient, high-quality, and humanized nursing service model. However, the application of AI in the nursing field has not been smooth sailing. Some AI tools are still in the proof-of-concept stage and face numerous challenges in practical application, such as data privacy protection and technical reliability. At the same time, AI also puts forward new requirements for nurses’ professional capabilities. Nurses need to possess certain AI knowledge and skills to better collaborate with intelligent systems. In the future, we will focus on specific steps: conducting multi-site clinical validation in 2–3 other hospitals to test the model’s adaptability; integrating uncertainty quantification and collecting systematic user feedback from nurses via monthly questionnaires to optimize AI functions like the intelligent keyboard; promoting integration with hospital EHR and LIS systems to achieve automatic data synchronization, and to optimize AI tools to better meet clinical needs, while strengthening AI knowledge training for nurses to ensure that nursing staff can provide higher-quality nursing services for patients in the era of intelligent nursing.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Xing Yuan, upon reasonable request.
Ethics Approval
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Anqing Municipal Hospital.
Funding
No funding was received.
Disclosure
None of the authors have any financial disclosure or conflict of interest.
References
1. Lee D, Yoon SN. Application of artificial intelligence-based technologies in the healthcare industry: opportunities and challenges. Int J Environ Res Public Health. 2021;18(1):271. doi:10.3390/ijerph18010271
2. Wang Q, Ding XT, Luo ZC, et al. Advances of artificial intelligence in nursing quality management. Chin J Nurs. 2024;59(23):2933–2939. doi:10.3761/j.issn.0254-1769.2024.23.019
3. Shao -L-L, Zhang Y, Shi J-M, et al. Research on the application value of closed-loop management mode in the risk management of patients with artificial airway in respiratory monitoring. Cardiovasc Dis Electron J Integr Trad Chin West Med. 2020;8(32):23–26.
4. Hu S-Z. Application of closed-loop information system construction in nursing management of critical patients in ICU. Contemp Med. 2017;23(30):168–170.
5. Lu C, Yi-jun J, Xie S. Construction and application of the closed-loop process management of medical examination. Chin Digit Med. 2020;15(03):41–43.
6. Zhang WG, Liu JW, Yang SY, et al. A study on the improvement of nursing interruption risk by a closed-loop management model. Risk Manag Healthc Policy. 2021;14:2945–2952. doi:10.2147/RMHP.S301108
7. Bhangu A, Notario L, Pinto RL, et al. Closed loop communication in the trauma bay: identifying opportunities for team performance improvement through a video review analysis. Can J Emerg Med. 2022;24:419–425. doi:10.1007/s43678-022-00295
8. Weng YQ, Zhou LT. Exploration and practice of closed loop management of medical new technologies and projects in a third class hospital. Chin Health Stand Manag. 2023;14(21):46–49.
9. National Health Commission. Notice on Issuing the Management Measures for Grading and Evaluating the Application Level of Electronic Medical Record Systems (Trial) and Evaluation Standards (Trial). Medical Letter from the National Health Office. 1079. 2018.
10. Wei Q, Pan S, Liu X, et al. The integration of AI in nursing: addressing current applications, challenges, and future directions. Front Med Lausanne. 2025;12:1545420. doi:10.3389/fmed.2025.1545420
11. Ruksakulpiwat S, Thorngthip S, Niyomyart A, et al. A systematic review of the application of artificial intelligence in nursing care: where are we, and what’s next? J Multidiscip Healthc. 2024;17:1603–1616. doi:10.2147/JMDH.S459946
12. McGrow K. Artificial intelligence in nursing: a journey from data to wisdom. Nursing. 2025;55(4):16–24. doi:10.1097/NSG.0000000000000165
13. Gonzalez-Garcia A, Pérez-González S, Benavides C, et al. Impact of artificial intelligence-based technology on nurse management: a systematic review. J Nurs Manag. 2024;2024:3537964. doi:10.1155/2024/3537964
14. Jost SG. Nurses as knowledge work agents: measuring the impact of a clinical decision support system on nurses’ perceptions of their practice and the work environment [EB/OL]. Available from: https://repository.upenn.edu/edissertations/2375.
15. Hidayat AAA, Uliyah M, Haryanti T. Mobile nursing care plan information system for nursing service in hospitals. Eur Rev Med Pharmacol Sci. 2023;27(1):13–19. doi:10.26355/eurrev_202301_30848
16. Chew HSJ. The use of artificial intelligence-based conversational agents (Chatbots) for weight loss: scoping review and practical recommendations. JMIR Med Inform. 2022;10(4):e32578. doi:10.2196/32578
17. Donabedian A. The quality of care: how can it be assessed? JAMA. 1988;260(12):1743–1748. doi:10.1001/jama.1988.03410120089033
18. Weng YQ, Zhou LT. Exploration and practice of closed-loop management of medical technologies. Chin Health Stand Manag. 2023;14(21):46–49.
19. Bhangu A, Søreide K, Di Saverio S, et al. Perioperative care for trauma patients: global strategies and future directions. Lancet. 2022;399(10330):1627–1638. doi:10.1016/S0140-6736(22)00391-2
20. Wei K, Xie X, Huang T, et al. Drug closed-loop management system using mobile technology. BMC Med Inform Decis Mak. 2022;22(1):311. doi:10.1186/s12911-022-02067-2
21. Tsan CY, Chen MC, Wen JC, Wang YC. Develop a mobile nursing app to improve nursing workflow and effectiveness assessment. Stud Health Technol Inform. 2021;284:356–358. doi:10.3233/SHTI210744
22. Zqp N, Ling LYJ, Chew HSJ, Lau Y. The role of artificial intelligence in enhancing clinical nursing care: a scoping review. J Nurs Manag. 2022;30(8):3654–3674. doi:10.1111/jonm.13425
23. Pan W, Ji Y, Zhou Y, Wang L, Zhou L. Research on the construction of information-based nursing quality control system based on deep learning model under the lean perspective. Technol Health Care. 2024;32(4):2081–2090. doi:10.3233/THC-230730
24. McGrow T. From data to wisdom: integrating AI in clinical nursing decision-making. Nurse Educ Today. 2025;126:105648. doi:10.1016/j.nedt.2024.105648
25. Vasquez B, Moreno-Lacalle R, Soriano GP, et al. Technological machines and artificial intelligence in nursing practice. Nurs Health Sci. 2023;25(3):474–481. doi:10.1111/nhs.13029
26. Gonzalez-Garcia N, Perez-Fernandez E, Aranda-Gallardo M, Pousette A, Törner M. Effectiveness of artificial intelligence applications in nursing management: a systematic review. J Adv Nurs. 2024;80(3):765–778. doi:10.1111/jan.15567
27. Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56. doi:10.1038/s41591-018-0300-7
28. Yu KH, Beam AL, Kohane IS. Artificial intelligence in healthcare. Nat Biomed Eng. 2018;2(10):719–731. doi:10.1038/s41551-018-0305-z
29. Davenport T, Kalakota R. The potential for AI in healthcare. Future Healthc J. 2019;6(2):94–98. doi:10.7861/futurehosp.6-2-94
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.