Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Impact of an Inaugural Interprofessional Education Session Among Multidisciplinary Healthcare Students: A Mixed Methods Study from the United Arab Emirates
Authors Al-Ghananeem AM ![]() , Palaian S
, Palaian S ![]() , Kheir N, Khan E
, Kheir N, Khan E ![]() , Hasan S, Jaber M
, Hasan S, Jaber M ![]() , Ahmeda A, Mahasneh D, Ibrahim N
, Ahmeda A, Mahasneh D, Ibrahim N ![]() , Abd Al Magied A
, Abd Al Magied A ![]()
Received 30 June 2025
Accepted for publication 9 October 2025
Published 29 October 2025 Volume 2025:18 Pages 7007—7024
DOI https://doi.org/10.2147/JMDH.S550623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abeer M Al-Ghananeem,1 Subish Palaian,1 Nadir Kheir,1 Erum Khan,2 Sanah Hasan,1 Mohamed Jaber,3 Ahmad Ahmeda,4 Deema Mahasneh,1,5 Nihal Ibrahim,1 Abdallah Abd Al Magied1
1College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates; 2College of Medicine, Ajman University, Ajman, United Arab Emirates; 3College of Dentistry, Ajman University, Ajman, United Arab Emirates; 4Department of Basic Medical Sciences, College of Medicine, University of Sharjah, Sharjah, United Arab Emirates; 5Faculty of Nursing, Mutah University, Karak, Jordan
Correspondence: Abeer M Al-Ghananeem, College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates, Email [email protected]
Purpose: This study assessed attitudes and perception of medicine, dental, pharmacy and nursing students toward their first interprofessional education (IPE), compared interprofessional attitudes scores with demographic characteristics, and evaluated session feedback to identify areas for improvements.
Methods: A mixed method study was conducted among healthcare students participating in an introductory IPE session. The interprofessional attitudes Scale (IPAS) was administered pre-session to evaluate baseline attitudes. Post-session, quantitative feedback was collected and analyzed using non-parametric tests (Mann–Whitney U, Kruskal–Wallis). Quantitative data were obtained through structured discussions with nine facilitators (Medicine/Dentistry/Pharmacy), recorded and analyzed until thematic saturation was reached.
Results: Among 218 respondents (Dentistry 30%, Nursing 25.3%, Medicine 22.6%, Pharmacy 21.2%), 88% had no prior IPE exposure. Median IPAS scores were positive (IQR-5), with significant variations by discipline, cumulative GPA, and academic year (p< 0.001). Post session, the “community-Centeredness” domain showed significant improvement (p< 0.001). Student feedback (n=131) yielded median satisfactory scores of 52 (IQR 48– 55), with prior IPE exposure influencing perceptions (p< 0.05). Facilitators acknowledged IPE’s value but identified key areas for enhancement: pre-session team-building to improve engagement, structured facilitator training for clearer role definition, more balanced clinical case designs to ensure equitable participation, incorporation of visual/high-fidelity simulation elements and stronger integration into core curricula.
Conclusion: Both students and facilitators perceive IPE positively, reinforcing its role in fostering collaborative practice readiness. The significant improvement in community-centered attitudes and overall satisfaction support IPE implementation across healthcare programs. However, optimizing its impact requires addressing critical gaps particularly in facilitators preparation, session design, and curricular alignment. This research provides a conceptual framework and methodological outline to initiate IPE sessions within the university and elsewhere in the country and the region.
Keywords: interprofessional education, diabetes mellitus, health profession students, United Arab Emirates, Pharmacy, Nursing, Medicine, Dentistry, Case-based learning
Introduction
Growing international attention is given to interprofessional education (IPE) in health science disciplines. Scholars argue that today’s patients have complex health needs, and thus, no single discipline can address issues regarding their health status to achieve optimal health.1,2 It is argued that IPE should be introduced to students at the start of their professional education in healthcare, which may prevent the formation of negative interprofessional attitudes.1 IPE is a prerequisite to building a collaborative practice environment and optimising patient care.3 Kitto et al provided a review on the evolution of IPE in the past few years and evaluated various evidence-based IPE interventions on understanding the delivery and evaluation of IPE activities.4
Though the core set competencies in IPE established by Interprofessional Education and Collaboration (IPEC), are values and ethics, roles and responsibilities, communication, teams and teamwork,4 the dominant approach to medical education is based on a profession-specific and disciplinary philosophy. Such philosophy often resulted in limited collaboration and poor communication skills; hence, the primary focus is on eliciting patients’ needs rather than enhancing teamwork among students.2 In many countries, current curricula and practices limit opportunities for interprofessional collaboration, preventing health science students from mastering essential communication and teamwork skills. For example, in Indonesia, medical students were hesitant to share knowledge with other healthcare professionals, opposing the idea of Interprofessional Education.5 This, in turn, reinforces stereotyped perceptions among them.6
In clinical settings, the absence of interprofessional teams means that each team operates within its discipline, which hinders the collaboration and integration of knowledge and perspectives across professions to achieve a high standard of patient care.7,8 A systematic review examining the impact of IPE on students’ learning outcomes revealed statistically significant improvements in seven of the reviewed studies.3 The barriers included a lack of team effort, inadequate communication within the institute, and insufficient administrative support, despite the availability of resources and infrastructure at the university.9
In the UAE, although the concept of IPE is still emerging, earlier studies have shown that students’ readiness scores for this medical education approach were high.10 Other researchers have identified several barriers to implementing IPE in the UAE, including gender segregation due to cultural barriers and the limited dedicated time allocated for faculty members to establish IPE activities.1 However, to date, much of what is known about the implementation of IPE within the context of health sciences has been derived from the West.2,11 Given the differences in educational philosophies, culture, and university infrastructures, the applicability of existing evidence to the UAE’s context may be questionable.
In the UAE, while local evidence is valuable, it is based on small-scale research using exclusively quantitative methodologies,1,10 which often require follow-up research to compare the impact of institutional efforts on students’ behavioral and perceptual changes.7 Interprofessional education is not yet part of the formal curriculum at the Colleges of Health Sciences at Ajman University. Thus, a multidisciplinary team led a project to examine the impact of an interprofessional education session among multidisciplinary healthcare students.
This study aims to equip educators and decision-makers with the critical insights necessary for designing, executing, and assessing impactful IPE initiatives. As healthcare systems continue to evolve, cultivating collaborative competencies within our workforce becomes increasingly crucial. By prioritising effective IPE, we can prepare teams to deliver outstanding, patient-centred care. Understanding the dynamics of IPE is not only beneficial but also essential for creating a robust healthcare environment that meets the complex needs of patients.2,6
Study Objectives
The objectives of this study are to assess the baseline attitudes and perceptions of medicine, nursing, dental, and pharmacy students regarding their first interprofessional education session, to compare the interprofessional attitude scores with respondents’ demographic characteristics, and to obtain quantitative and qualitative feedback from participants (students and facilitators) on the interprofessional education session.
Methodology
Study Design
A mixed-methods study was conducted using both quantitative and qualitative assessments of an IPE session among students from medicine, nursing, dental, and pharmacy programs. The qualitative part employed focus group discussions (FGDs) and the quantitative part employed pre-post assessments using questionnaires. The student part included quantitative assessments, while the facilitator’s feedback was qualitative.
Ethical Approval
The Research Ethics Committee at Ajman University approved the research with the number P-F-H-11-Feb, dated 11th February 2025.
Informed Consent
Written Informed consent was obtained from each student participant before enrolling in the study and separately before receiving the survey response. Similarly, written consent was obtained from the instructors before enrolling them in the qualitative interviews. The researchers strictly followed all the ethical principles laid down by the ethical approval body. The participants informed consent included publication of anonymized responses and direct quotes.
Overview of the IPE Session
An IPE session was conducted on 13th February 2025, involving senior students from Ajman University’s colleges of medicine, nursing, dentistry, and pharmacy. The IPE session was based on a case study of a“‘diabetic patient with trauma”’ wherein a total of 35 groups of students, each consisting of eight students (two from each of the colleges of medicine, nursing, dentistry, and pharmacy), worked together. The session ran for two hours, and each group had one faculty facilitator who moderated the session to ensure that the students learned from, with, and about each other (IPE core principle). The organization of the event was taken care of by the events committee of the College of Pharmacy and Health Sciences, and the fundamental learning outcome of“‘learning together for working together”’ was kept in mind. The learning outcomes were discussed during multiple face-to-face meetings among the research team members under the leadership of the principal investigator.
Study Subjects and Sampling
Final-year students from the medicine, nursing, dentistry, and pharmacy programs at Ajman University were enrolled using a convenience sampling method on a first-come, first-served basis. To maintain uniformity among the participants’ level of competency, only “senior” students were enrolled. However, in the case of the nursing discipline, students from the second year were enrolled since that was the highest level present in the university, and a few of the first-year self-motivated students (n=20) volunteered to participate and were allowed to participate in the IPE event and hence the study.
Method of Data Collection
Quantitative Assessment
The baseline interprofessional attitudes of the participants were measured before the start of the IPE session using the interprofessional attitudes scale (IPAS).12 Written permission was obtained from the authors prior to using the survey tool. The IPAS tool has 27, 5-point Likert-type items measuring each of the respondent’s agreement with statements grouped under five domains: teamwork roles and responsibilities, patient-centred care, interprofessional biases, diversity and ethics, and community-centeredness. All participating students were requested to complete the survey, along with informed consent. Upon completion of the IPE session, post-session interprofessional attitudes were collected using the IPAS.
The participants’ quantitative feedback was collected using a “Student Feedback Form”, which consisted of 11 items measured on a 5-point Likert-type scale, along with two open-ended questions (Supplementary Appendix 1).
Qualitative Assessment
The qualitative part of the study employed heterogeneous FGDs to explore the session facilitators’ experiences with the IPE exercise using an interview guide (Supplementary Appendix 2). The heterogeneous approach was chosen to capture shared and contrasting facilitation experiences across professions while promoting richer discussions on the interprofessional dynamics of the exercise. The mixed group composition allowed for efficient data collection, reducing the number of sessions required to reach thematic saturation while ensuring a robust exploration of key issues. Adopting a phenomenological approach, the qualitative study aimed to uncover facilitators’ perceptions, observations, and suggestions following the IPE sessions. Participant facilitators were purposively selected from the colleges of Medicine, Pharmacy, and Health Sciences, as well as Dentistry.
Recruitment of facilitators in the FGDs was conducted via Email invitations sent to college representatives at the IPE task force, who then provided names of candidate participants. Data collection continued until thematic saturation was achieved, with each FGD comprising 4 and 5 facilitators to foster in-depth discussions. Sessions, lasting between 60 and 90 minutes, were guided by a semi-structured framework centred on predetermined themes: facilitators’ experiences with IPE sessions, in-group interprofessional dynamics, perceived benefits of IPE for students and facilitators, challenges encountered during IPE facilitation, and recommendations for future IPE sessions. A trained moderator led the discussions, supported by a co-moderator responsible for note-taking and logistical management. With participants’ consent, all sessions were audio-recorded and transcribed verbatim for subsequent analysis. Finally, a total of 9 facilitators participated in the FGDs, with representation of 3 facilitators from each college: College of Medicine (COM), College of Pharmacy and Health Sciences (COPHS), and College of Dentistry (COD).
Data Analysis (Quantitative and Qualitative)
The IPAS scale was scored as strongly disagree (1) to strongly agree (5). Filled IPAS scores were transferred to SPSS, and the normality of the data was assessed using the Shapiro–Wilk test (α = 0.05). The median (IQR) scores of the individual statements, each domain, and the total scores were tested using the Mann–Whitney U-Test (for variables with two groups) and the Kruskal–Wallis test (for variables with more than two groups), at α = 0.05. The same analysis was followed for student feedback. The pre-post median (IQR) total IPAS scores were compared using the Wilcoxon-Signed Rank test. The qualitative interview recording was transcribed using “Microsoft Transcribe” and assessed using the content analysis method. The coding was generated using ATLAS.ti program.
For the qualitative data, thematic analysis, guided by Braun and Clarke’s six-step framework, was employed to interpret the data.13 This process involves familiarization with the data, generating initial codes, identifying and reviewing themes, defining and naming themes, and compiling a comprehensive report enriched with direct participant quotations. To ensure the credibility and reliability of the findings, the study incorporated triangulation by comparing findings across different facilitators and professions, member checking, where participants will be invited to review preliminary findings to validate interpretations, peer debriefing with other qualitative researchers to enhance objectivity, and thick description, providing rich contextual details to enhance transferability.
Results
Part A: Quantitative Results
A total of 218 students responded to the baseline survey, and their demographic details are mentioned in Table 1.
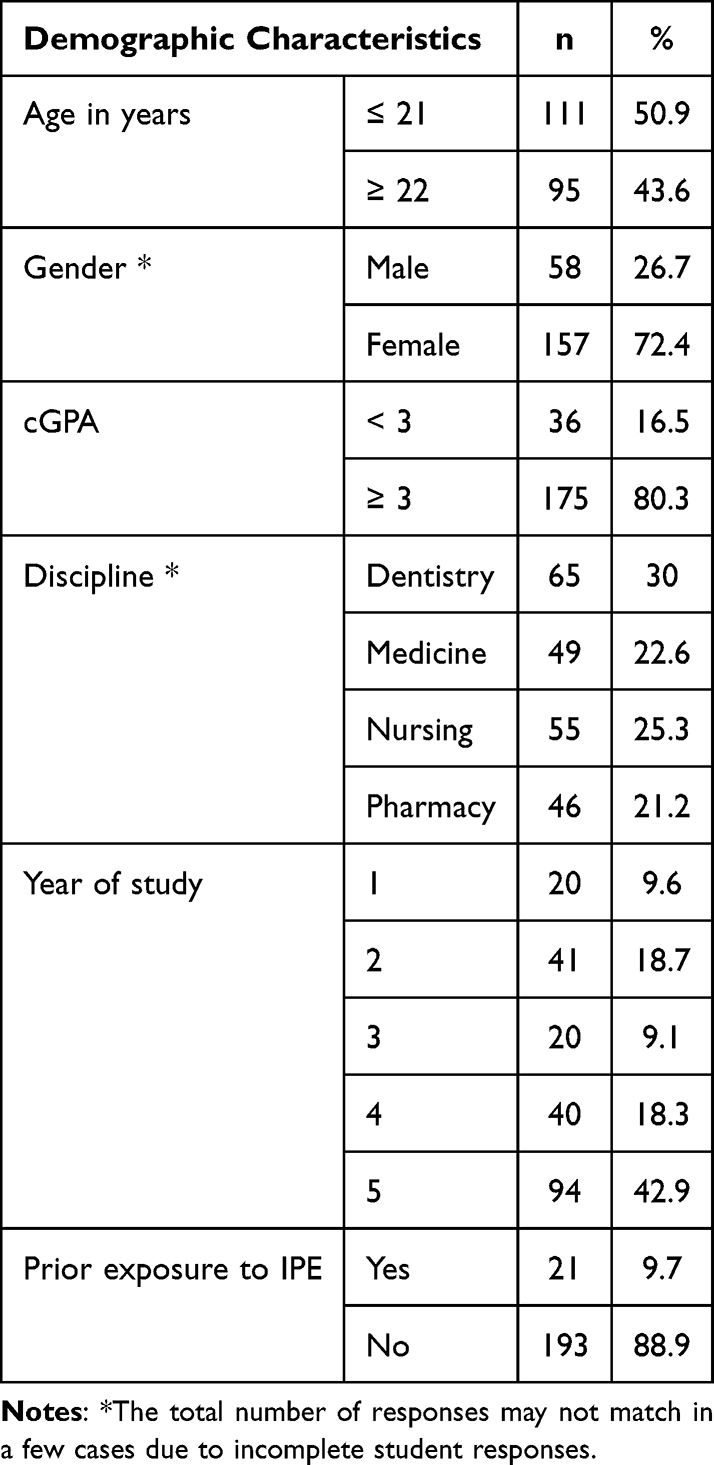 |
Table 1 Demographic Distribution of the Respondents at Baseline |
Baseline Assessment of Interprofessional Attitude Among Students
The median (IQR) and mean ± SD scores for individual statements under the IPAS tool are presented in Table 2. Overall, for most statements, the median score was five. However, for a few statements, such as “It is not necessary for health sciences students to learn together” and “I have prejudices or make assumptions about health professionals/students from other disciplines”, the median scores were in the range of 3.
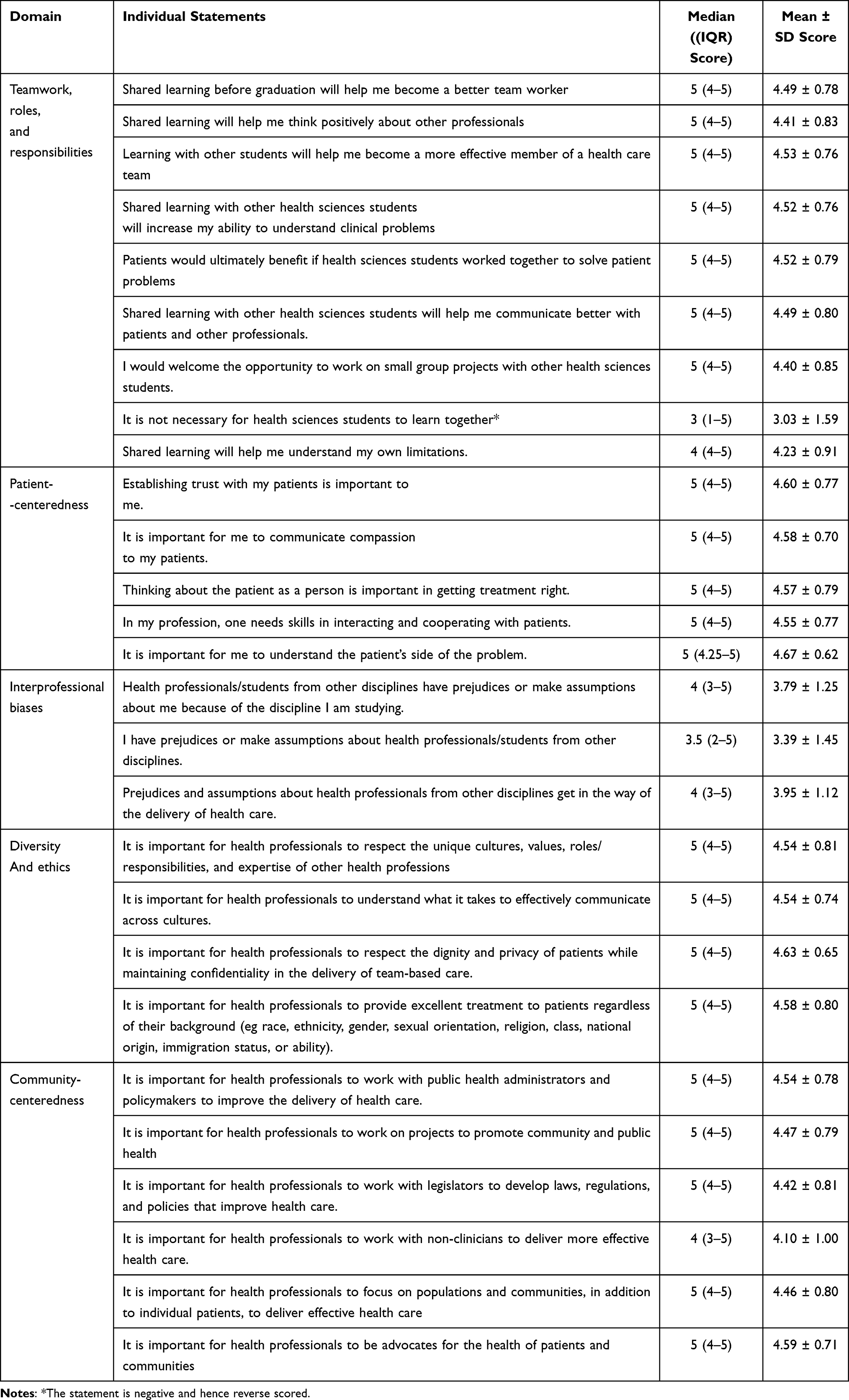 |
Table 2 Baseline Scores for Individual IPAS Statements |
Comparison of Students’ Attitudes at Baseline with Their Demographic Characteristics
The median (IQR) baseline scores were compared within demographic intervals, and no statistically significant associations were noted (Table 3). Though not statistically significant, there were noticeable differences in the scores between cGPA, discipline, and year of study.
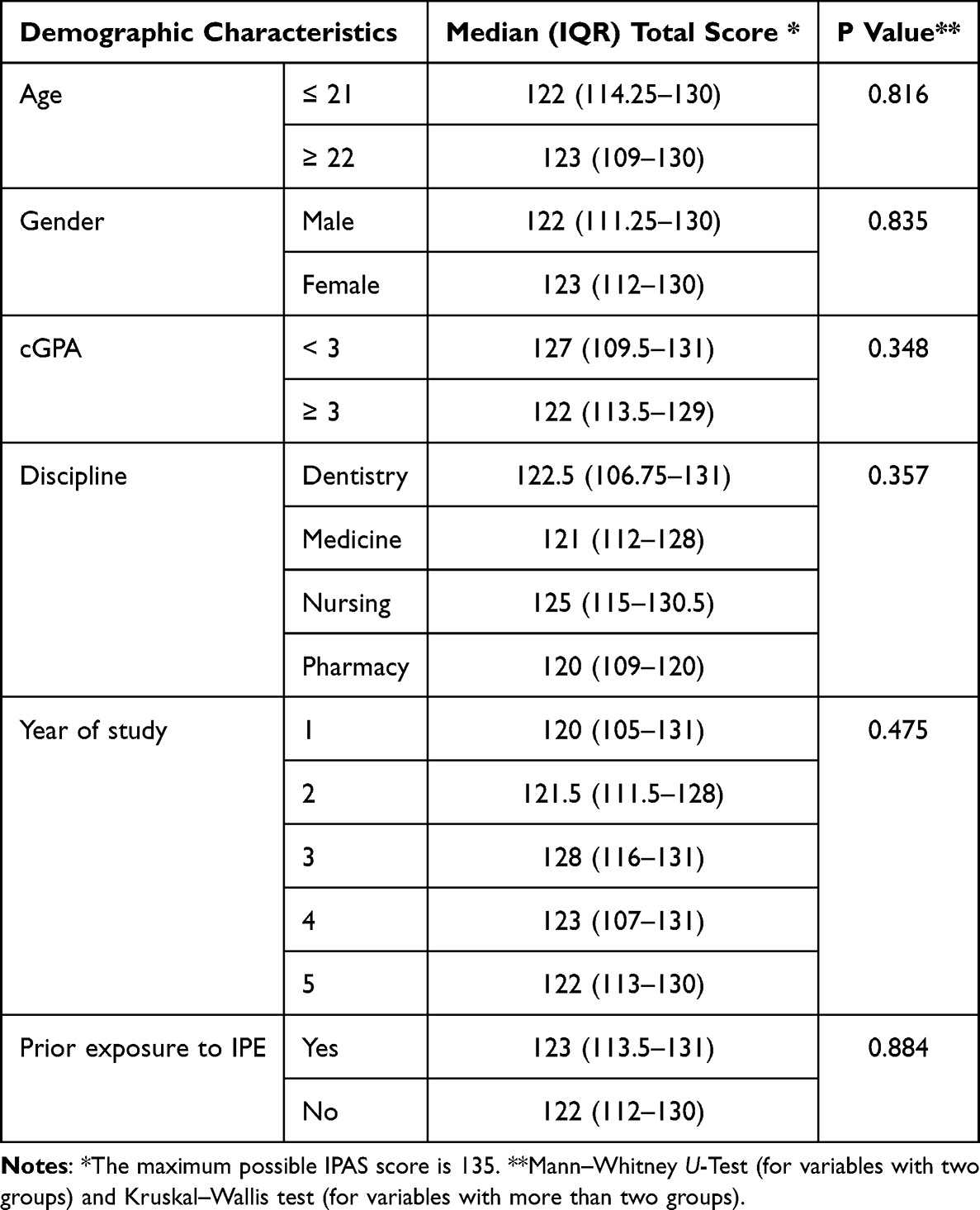 |
Table 3 Comparison of Total Baseline IPAS Scores with Demographic Characteristics of Student Respondents |
The Influence of the IPE Session on Overall and Specific Domains of Students’ Attitudes
The median (IQR) IPAS scores at baseline and post-intervention are presented in Table 4. The pre-post comparison of total scores showed statistical significance (p < 0.001), and among the scores under specific domains, a statistically significant improvement was noted for the domain “Community-Centeredness” (p < 0.001). Furthermore, improvements were reported in the total scores of the following domains: interprofessional biases and community-centeredness.
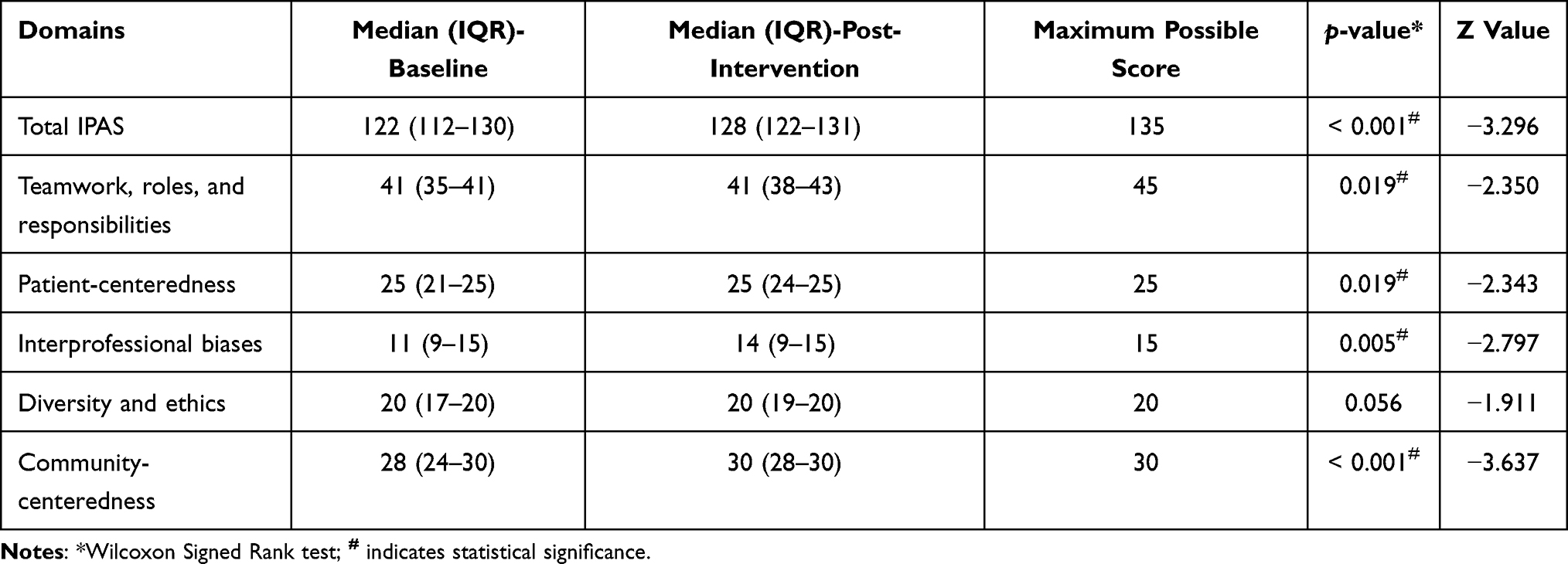 |
Table 4 Total Scores Achieved in IPAS and Its Specific Domains Pre- and Post-IPE Activity |
Pre-Post Comparison of Total IPAS Scores Concerning Specific Demographic Characteristics
The improvements in the IPAS scores, concerning respondents’ demographics, are presented in Table 5. There were noticeable improvements in the total median scores across all segments.
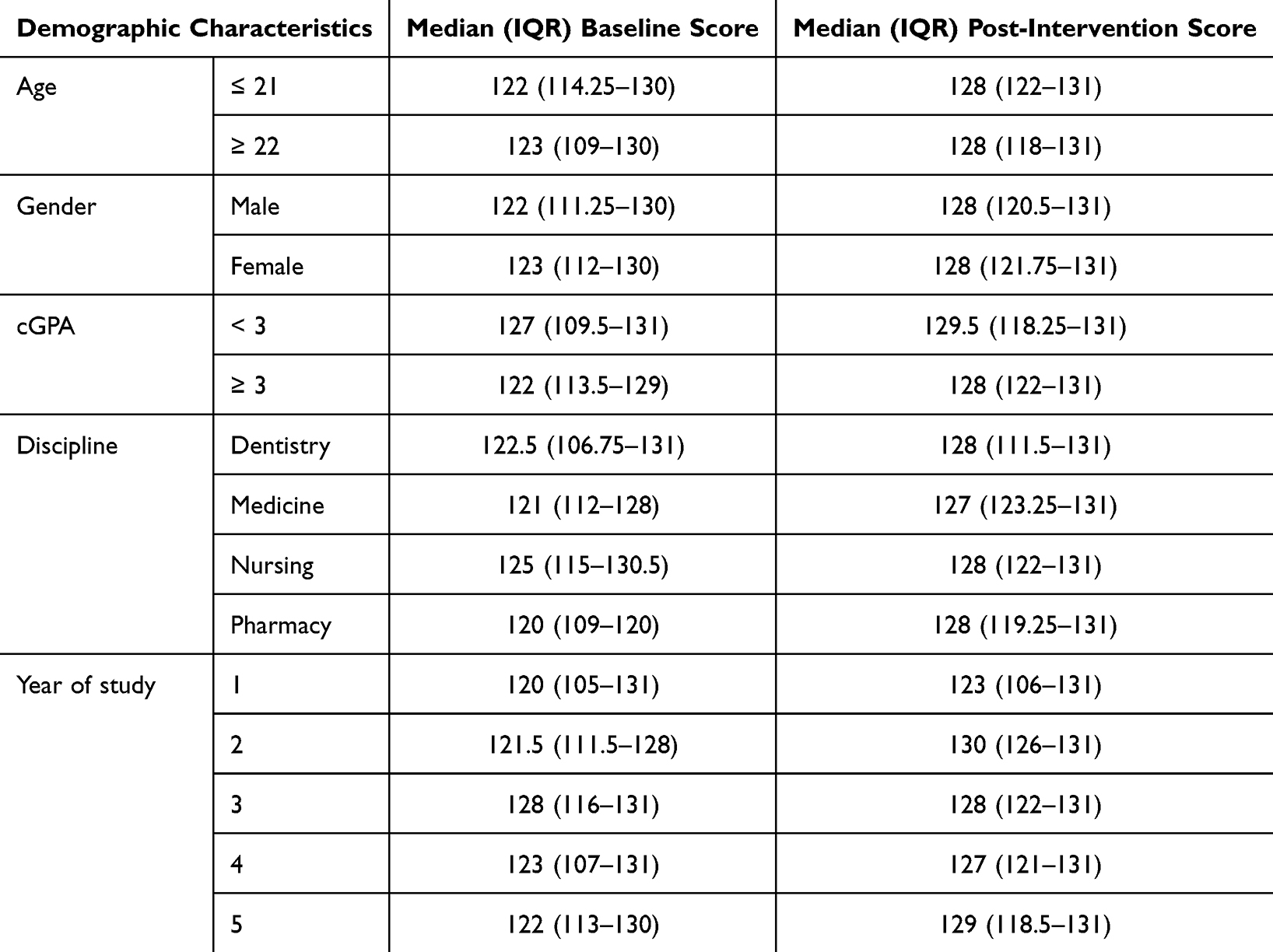 |
Table 5 Pre-Post Total IPAS Scores Concerning Participant Demographic Characteristics |
Correlation Between Demographic Characteristics and Specific Domains at Baseline
A statistically significant positive correlation was observed between “Teamwork, roles, and responsibilities” versus “student discipline” and their “cGPA”. Further, a significant correlation was observed between “Patient-centeredness” and “cGPA”. However, the observed correlations are “weak”. More details are available in Table 6.
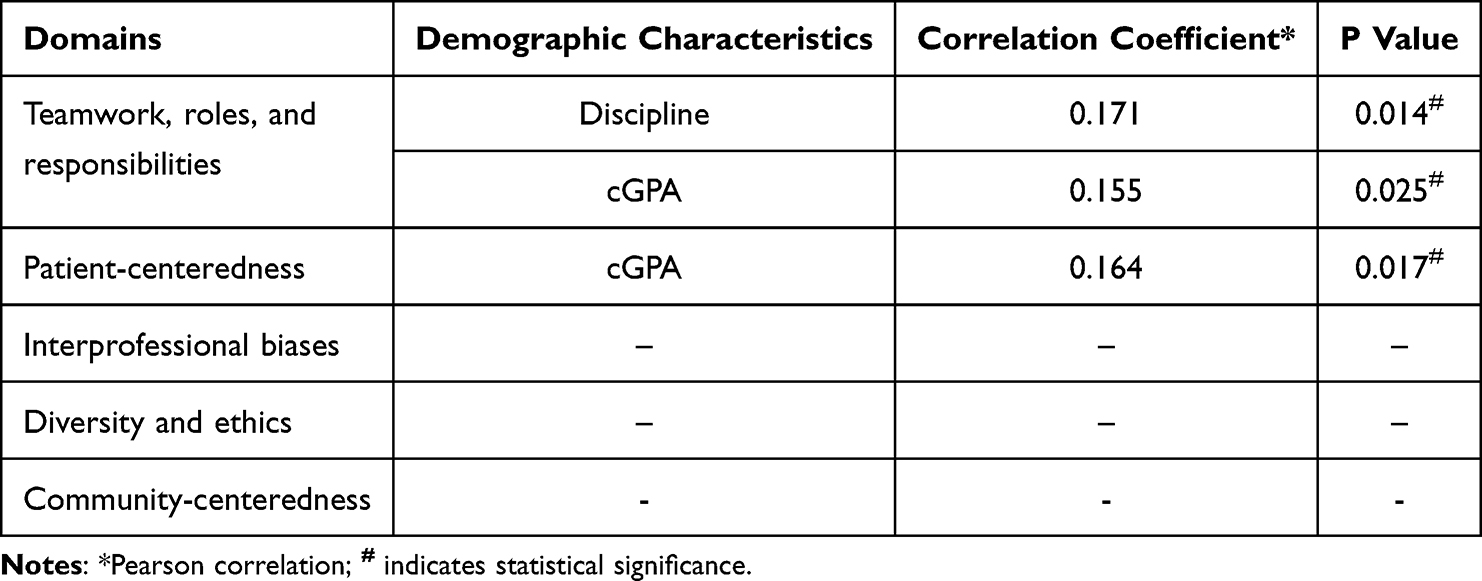 |
Table 6 Correlation Assessment Between Demographic Characteristics and Specific Domains at Baseline |
Feedback on IPE Session
The post-session feedback was provided by 131 students [medicine (n = 37, 28.9%); dentistry (n = 29, 22.7%); pharmacy (n = 35, 27.3%); and nursing (n = 37, 28.9%)]. The total median (IQR) and mean ± SD scores were 52 (48–55) and 50.33 ± 5.30, respectively, out of a maximum possible score of 55. Analysis of the individual feedback statements showed a highly positive trend, as indicated by high median and mean scores (Table 7).
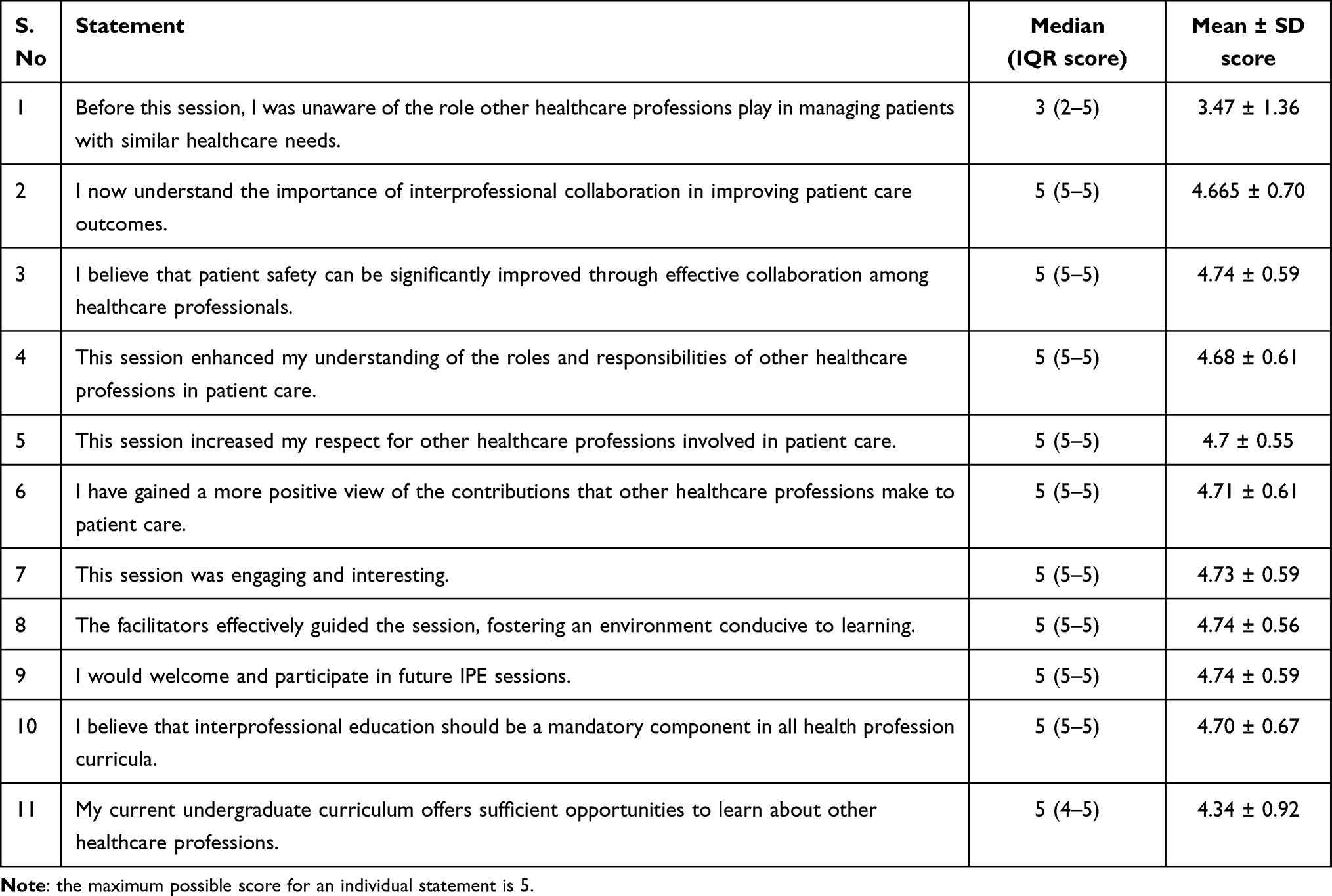 |
Table 7 Student Feedback on Individual Statements (n = 131) |
Comparison of Total Feedback Scores with Students’ Demographic Characteristics
Upon comparing the student feedback scores, it was observed that “Prior exposure to IPE” had a significant association with the total feedback scores (Table 8).
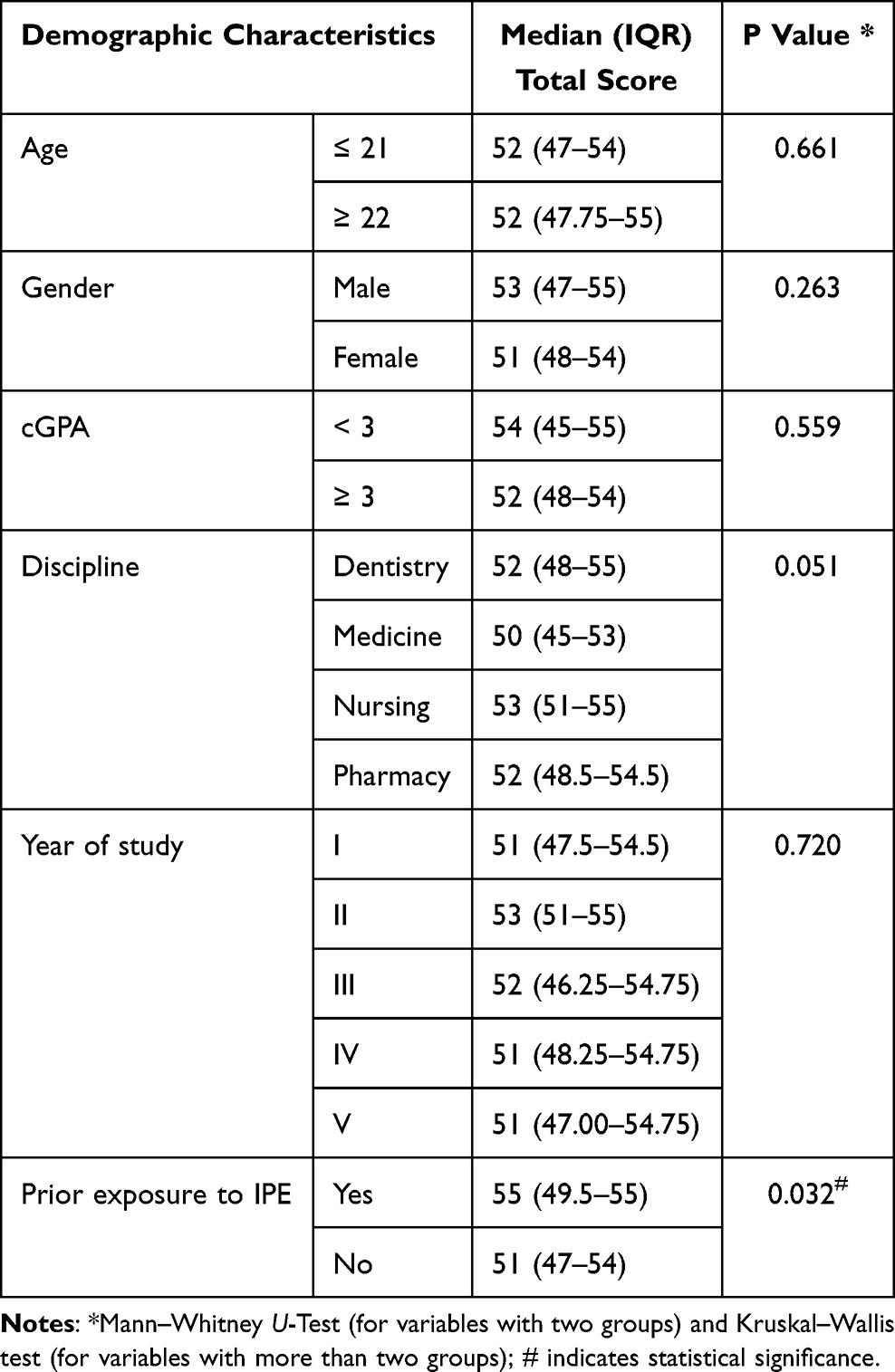 |
Table 8 Comparison of Total Feedback Scores with Demographic Characteristics of Student Respondents |
Correlation of Total Feedback Score with Demographic Variables
There was no statistically significant correlation between feedback total score and demographic characteristics (Pearson’s correlation test at α = 0.05). However, the linear regression between age and total feedback score showed R square=0.008 (95% CI = 49.28–51.28).
Students’ Open-Ended Feedback on the IPE Session
Students’ responses to the two open-ended questions on the feedback questionnaire are presented in Supplementary Appendix 3. File 1. Figures 1 and 2 depict the word cloud of the feedback statements.
 |
Figure 1 Word cloud of the most valuable aspect of the IPE session. |
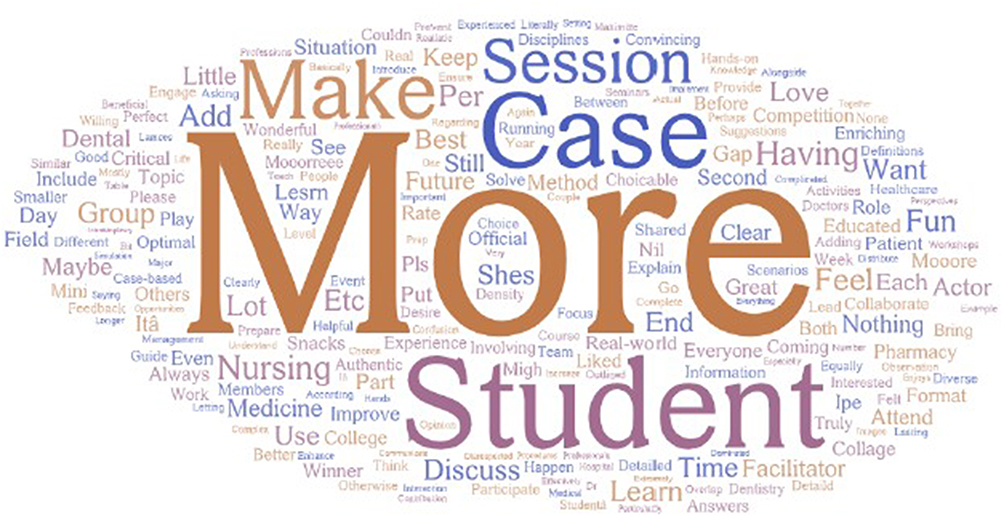 |
Figure 2 Word cloud of the students’ suggestions for future IPE sessions. |
a. What was the most valuable aspect of this IPE session?
b. What suggestions do you have for improving future IPE sessions?
Part B: Qualitative Results
Facilitator Focus Group Discussions
Participants’ demographics and group compositions are illustrated in Table 9.
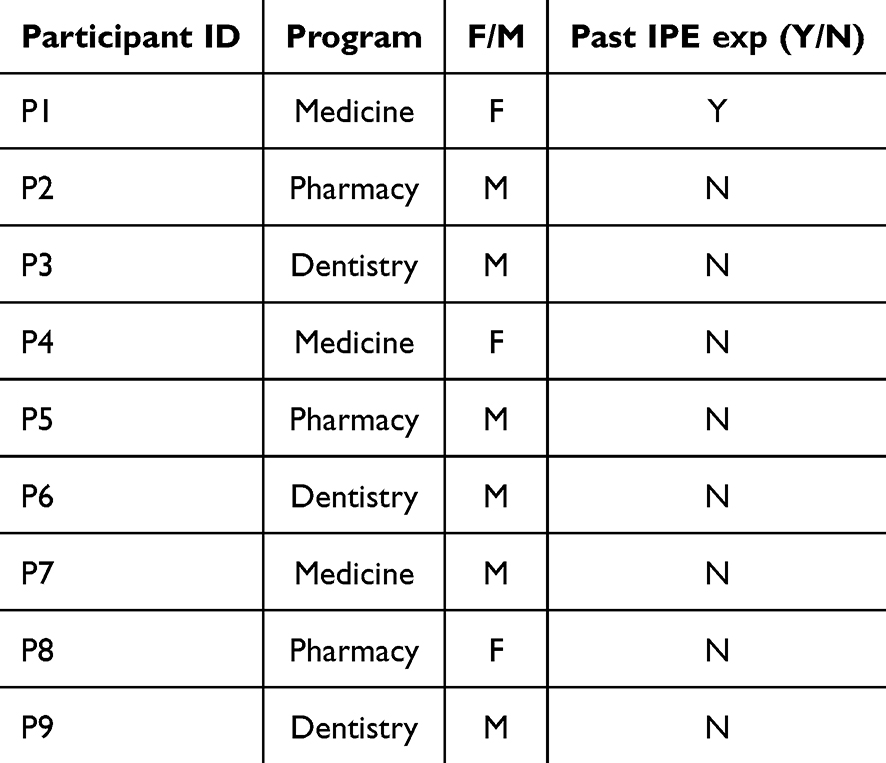 |
Table 9 Participants’ Programs and Demographics |
Thematic analysis focused on key areas, including the facilitators’ roles, student engagement and communication dynamics, leadership patterns, case study design, and challenges encountered during the facilitation process. The following results present the key themes that emerged from the focus group discussions with the facilitators.
Thematic Analysis Results
Across all focus groups, facilitators highlighted varied levels of enthusiasm, preparedness, clarity about roles, and confidence in guiding interprofessional discussions. Some were experienced in facilitation or had received orientation materials, while others desired more structured pre-event training and clearer role expectations. The following is a summary of the themes emerging, and the associated codes and categories which were supported by quotes from participants:
Theme 1: Facilitator Preparedness and Role Clarity
Codes extracted from the transcripts were: “Received orientation document”, “confused table assignment”, “brief outline before session”, “case document sent in advance”, and “mediation role.”
Categories
Preparedness level; Clarity of facilitation role; Logistics.
Variability in Preparedness
Some facilitators received adequate materials (eg, case documents, briefings) and felt prepared. Others requested a formal pre-event meeting with case developers.
More explicit role allocation (eg, which table or team a facilitator belonged to) was identified as a logistical improvement area.
We were given the PPT and the text document of the case, but I think it could be better if we could sit together and have a short discussion before the actual event starts. (P9, COD)
I had enough time to go through the case... there was an orientation session... that was more than adequate to prepare. (P6, COD)
Students or us as faculty, we didn’t know, like we have to go to a specific table I was confused. (P7, COM)
Role Understanding and Expectations
Facilitators generally understood their role was to prompt discussions and ensure equal participation, but some felt unsure of how directive they should be.
I believe my role was simply to mediate communication between them... to encourage them to think a little bit laterally. (P6, COD)
My role was to be a co-facilitator or a hopper, depending on the situation... balancing out the dynamics. (P8, COPH)
Theme 2: Student Induction and Group Dynamics
Description
A recurring theme was the lack of structured student induction, which impacted communication and comfort. Facilitators emphasized the importance of pre-session orientation, team-building, and breaking hierarchical tendencies in discussions.
Codes extracted from the transcripts were: “students didn’t know each other”, “first meeting between specialities”, “medical students led”, “shy pharmacy student”, and “condescending behaviour.”
Categories
Icebreaking and team-building; Hierarchical roles; Group communication.
Lack of Student Orientation
Many students did not know each other and were hesitant at first. A formal orientation would help set expectations and encourage cross-disciplinary respect.
Supporting Quotes
They don’t have a rapport. I had to encourage them to talk to each other. (P6, COD)
This was the first meeting between these specialities... everyone was [wondering] what we are going to do. (P7, COM)
Hierarchical Influence and Group Dominance
Medical students often took the lead, sometimes naturally due to case relevance or confidence, but at times, overshadowed others.
Some facilitators noted condescending behaviour and the reinforcement of professional hierarchies.
All participants just put the ball in the playground of the medicine... they were asking, “Okay, you are the leader”. (P7, COM)
The medicals are the one who always have the hierarchy... they themselves feel that we are boss” (P9, COD)
Theme 3: Experiential and Collaborative Learning
Description
The majority of facilitators praised the experiential learning aspect and appreciated how the case allowed students to understand their roles and those of others. However, they suggested further integration of simulation and visual aids to enhance realism.
Codes extracted from the transcripts included: “students collaborating”, “interdisciplinary interaction”, “discussion without prompt”, “used simulation before”, and “suggested pictorials/videos.”
Categories
Team-based learning; Simulation and visual tools; Peer-to-peer engagement.
Interprofessional Teamwork and Role Awareness
Facilitators observed that students began to collaborate more organically as the session progressed. With guidance, they started consulting one another based on their respective areas of expertise.
By the second and third stage of the case, they were talking to each other without prompts. (P6, COD)
I tried to have the dentistry and pharmacy students discuss antibiotic dosing together. (P8, COPH)
Realism and Simulation
Facilitators advocated for more realistic or multimedia-driven cases (eg, pictorials, simulations, or videos).
Supporting Quotes
We need to include more pictorials or videos... so students get more engaged. (P6, COD)
We should involve high-fidelity simulation, especially in universities with hospital access. (P4, COM)
Theme 4: Case Design and Interdisciplinary Balance
Description: While most facilitators felt the trauma case worked well, many believed future cases should involve a broader range of disciplines to encourage more equal participation.
Codes extracted from the transcripts were: “case too medical”, “pharmacy helped a lot”, “dental had minimal role”, “case extension needed”, and “more follow-up care.”
Categories
Case inclusiveness; Speciality relevance; Longitudinal patient care.
Case Inclusiveness
Some disciplines, especially medicine and pharmacy, had a clearer and more active role. Others felt less relevant depending on the scenario.
The case was very medical... pharmacy helped a lot, but dental had minimal opportunity. (P9, COD)
We need case scenarios from different situations... to allow all specialities to participate equally. (P7, COM)
Referral, Discharge, and Continuity of Care
Facilitators suggested that cases should be extended to cover community care, follow-up, and referrals, thereby including all health professions in a meaningful way.
There should have been a trigger for a referral to dental... and an extension to discharge planning. (P8, COPH)
Pharmacy students already exposed the discharge and counseling role in my group. (P7, COM)
Discussion
In an increasingly complex healthcare system, members of the health service delivery team need to collaborate to accomplish common goals to improve patient experience and outcomes.14,15 There is international agreement that health professional students should be prepared for practice by experiencing IPE.14 As the core of IPE lies in collaborative training among healthcare professionals and preparing them with the skills needed for managing a complex healthcare setting.16 The success of this training is vastly dependent on attitudes and readiness of healthcare students towards this learning.17 Student attitudes have been identified as the most important element in defining the success of IPE,18 as these attitudes eventually can affect behaviour towards collaboration with other professions.19 We utilised the IPAS as a validated instrument to measure baseline and post IPE activity attitudes towards collaboration amongst students of four health professions (Pharmacy, medicine, nursing and dentistry). The tool is comprehensive as it not only links the assessment of IPE to the core competencies established by the IPEC,20 but it also adds assessments related to diversity and ethics, community-centeredness, and interprofessional biases, which are domains unique to the IPAS.
A Collaborative case-based discussion was utilised in our study to teach IPE, providing a comprehensive approach to patient case management. Collaborative learning focuses on both content and social skills, including communication, mutual respect, and team building.21 However, feedback provided by the students highlighted their preference for “authentic” assessments, simulations, and real patients, which underscores the importance of intentional, real-world-oriented tasks that simulate clinical collaboration, allowing them to explore how different health professions contribute to shared goals. Given the timeframe for conducting the IPE activity within the semester, collaborative case discussions were determined to require less manpower, time, and training resources, as it served as an extension of the regular classroom flow.
In our study, at baseline, students rated all items within the domains of the IPAS positively; only two items were rated neutrally: “It is not necessary for health sciences students to learn together” within the domain of Teamwork, Roles, and Responsibilities and the item “I have prejudices or make assumptions about health professionals/students from other disciplines” within the domain Interprofessional Biases. The scores of this domain were the lowest among the other domain scores. This reflected the raw nature of the attitude some students had regarding the roles other professions have in caring for patients and, therefore, the need for increased awareness and modelling of these roles early in the career of the students. Lowest scores on the Interprofessional biases domain were reported in previous studies from the UAE 22 and Lebanon.21 However, no such comparison was made with studies from Western countries since the implementation of IPE and collaborative practice in the healthcare settings is vastly different. Positively, post-intervention data identified that the total scores on the IPAS and all scores under its specific domains, such as “Community-Centeredness” and “Interprofessional Biases”, increased in a statistically significant fashion. It was clear that even though the academic/experiential background of the students had not prepared them for the professional roles of other members in the healthcare team, a simple single activity that involved engaging students from different professions had a positive impact on their awareness and appreciation of other professions.
Post activity student feedback about their experience undergoing an IPE activity was very positive in all items of measurement. Similar experiences were reported post IPE activities in Saudi Arabia, Qatar and Lebanon.23–25 Specifically, collaboration perception and interprofessional identity have been shown to strengthen after participating in IPE.26 Students’ positive perception of collaboration directly contributes to the development of their interprofessional identity. As interprofessional identity strengthens, students’ perception of collaboration becomes more positive, reinforcing the desire and competence to work across disciplines. Professional identity has been defined as:
the development of a robust cognitive, psychological, and emotional sense of belonging to an interprofessional community, necessary to achieve shared context-dependent goals.27
The open-ended text from the student feedback survey and echoed by the word cloud generated several themes that confirm the quantitative data and align with Reinders’ interprofessional identity model,28 comprising three dimensions: belonging, commitment, and reliance. Students reported that the IPE session fostered interprofessional belonging by providing opportunities to meet, learn from, and collaborate with peers from other health disciplines. This experience was reflected in the theme of Multidisciplinary Learning and Broader Clinical Perspective, as students developed a deeper appreciation for how different healthcare professions approach clinical care. Students also demonstrated a strong sense of interprofessional commitment, which corresponded with the theme of Teamwork and Group Dynamics, where they expressed enthusiasm for working collaboratively and recognised the importance of team roles and mutual support. As reported by the facilitators, over time, students developed interprofessional reliance, gaining confidence in their ability to depend on the contributions of other disciplines. This shift was mirrored in the themes of Communication and Role Clarity and Collaboration and Contribution in Patient Care, as participants increasingly valued effective communication, role understanding, and integrated decision-making as essential to optimising patient outcomes.
Students highlighted the need for better training in IPE through improved preparation and the establishment of clear expectations. The literature proposes the flipped classroom model in interprofessional education to offer several advantages, which can be easily adapted in the early stages of IPE within curricula. It promotes a more equitable learning environment by ensuring that all students receive the same preparatory materials in advance, arriving at class with a shared foundation of knowledge. This structure allows class time to be dedicated to student-centred activities, enabling facilitators to focus on guiding skill development and deeper learning through interactive engagement.26
The focus group findings affirm the value of interprofessional education in promoting collaboration, mutual respect, and communication among students from diverse healthcare disciplines. Facilitators described overall positive experiences, despite initial unequal participation, often influenced by traditional hierarchies. Confident students, usually those with stronger subject mastery, tended to lead discussions, reinforcing perceived professional dominance. Facilitators play a vital role in addressing this intentionally by ensuring all voices are heard and valued. Importantly, facilitators noted that students became more engaged as the session progressed; over time, students grew more comfortable working across disciplines, especially when facilitators actively encouraged balanced participation. The establishment of a supportive and inclusive learning environment should be evident from the onset of any teaching activity.29,30 Facilitator training is essential in promoting inclusive participation leading to success of IPE as role modelling of “interprofessional leadership” by facilitators, allows students to witness the collaborative nature of joint leadership, promoting trust and acceptance of interprofessional practice.31
Integrating IPE more consistently into curricula, through orientation sessions and cross-disciplinary collaboration, will help prepare students to practice as effective, patient-centered healthcare teams. It has been suggested that emphasis on early curricular integration is particularly significant and requires thoughtful curriculum design that embeds IPE sequentially, not as one-off workshops but as longitudinal, scaffolded experiences. The qualitative responses from students confirm this, indicating that students perceive sequential, collaboration-oriented activities as helpful for shaping positive attitudes toward teamwork and for solidifying their identity as contributors to interprofessional healthcare teams.31
Limitations
This study had a few limitations. The generalizability of these findings is limited due to the use of a convenience sampling technique, which may have introduced selection bias and may not truly represent the broader student population from various disciplines. Additionally, the participating nursing students were from the second year of the program, as the first cohort of the nursing undergraduate program had only reached the second year. This may not only have affected the uniformity of the group (since all other participating students were from the senior years of their respective programs), but also the homogeneity of competency and engagement across the groups. Another limitation of the study is that 20 of the first-year students participated in the study, though the study was aimed at final year students who can easily understand and interpret the case. Moreover, the study was conducted at a single university in the UAE, limiting the generalizability of the findings to other institutions or regions.
The assessment of students’ attitudes and perceptions about the IPE session relied heavily on self-reporting instruments, posing the risk of socially desirable responses instead of deeper reflection and sincere self-assessment.
Moreover, the study focused primarily on attitudinal outcomes, which, while necessary, represent only one dimension of interprofessional competence. The study did not assess behavioural or cognitive aspects of interprofessional learning, nor did it examine patient or system-level outcomes that might result from improved collaboration.
The trauma and diabetes case scenario was aligned more closely with the training and scope of practice of medicine and pharmacy students. This could have facilitated their dominant participation in the case discussion, potentially marginalizing the contributions from other disciplines (dental and nursing), and limiting the opportunity for equitable engagement across the interprofessional group.
While these limitations constrain the generalizability and definitive interpretation of the findings, they do not negate the importance of the study’s contributions. Instead, they highlight the complexity of implementing and evaluating IPE initiatives, pointing to valuable opportunities for methodological refinement in future research.
Recommendations
The recommendations were generated from data-driven insights and facilitator experiences expressed during the focus group meetings.
Facilitators across all focus groups expressed genuine enthusiasm for the IPE initiative and highlighted valuable insights to help enhance future sessions. These suggestions build on what worked well and offer practical ways to improve the experience for both students and faculty. Facilitator preparation can benefit from structured, pre-event briefings that include both case developers and facilitators. These meetings would help align expectations, clarify roles, and provide valuable strategies for managing group dynamics. A brief facilitator guide could also support consistency across sessions. For students, a more interactive orientation would help ease initial hesitation and promote better teamwork. Activities focused on team-building, role awareness, and addressing professional hierarchies can encourage more balanced participation and mutual respect. Case design was widely praised, though facilitators suggested Proper case design to serve the involvement of all disciplines. To enrich the learning experience, simple simulations and digital tools, like pictorial case prompts or brief clinical videos, can make discussions more engaging, especially in large group settings. Finally, embedding IPE into the curriculum through joint communication modules or interdisciplinary electives would reinforce collaboration as a core professional value, not just a one-off event. These reflections offer clear, achievable steps to build on the success of the current IPE model and support its continued growth into a meaningful, student-centered experience.
Conclusions
This study emphasizes the substantial value of interprofessional education (IPE) among medical, pharmacy, dental, and nursing students. The overwhelmingly positive students’ Pre-post total IPAS quantitative scores, along with the facilitators’ qualitative responses, suggest that IPE can play a pivotal role in preparing future healthcare professionals for effective teamwork in the real-world clinical settings. The findings of the study demonstrate enhanced collaboration, improved communication, and a deeper understanding of each profession’s unique contributions to patient care. Future studies should aim to address these limitations and explore long-term outcomes of IPE initiatives. Overall, integrating IPE into the health curricula not only fosters mutual respect and cooperation but also equips students with the essential skills needed for delivering high-quality, patient-centered care. The positive outcomes observed in this study provide a strong foundation for the continued implementation and development of IPE programs across the different healthcare disciplines. Further, being one of the earlier researches in the country and region, this research provides a conceptual framework and operational method to initiate IPE sessions within the country and the region.
Acknowledgments
The Authors would like to acknowledge all the students who spent their valuable time participating in the study. The authors also thank Ms. Alaa Farajallah, Senior Instructor at the College of Pharmacy and Health Sciences, Ajman University, Ajman, for her help in performing statistical analysis for this research. A special thanks to Dr. Jeffrey Norris for permitting us to use the study questionnaire. The authors would like to extend their appreciation to Ajman University for paying the article processing fee.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zaher S, Otaki F, Zary N, Al Marzouqi A, Radhakrishnan R. Effect of introducing interprofessional education concepts on students of various healthcare disciplines: a pre-post study in the United Arab Emirates. BMC Med Educ. 2022;22(1):517. doi:10.1186/s12909-022-03571-9
2. de Camargo JC, Finkler M, Campagnoni JP, et al. Interprofessional education in traditional and complementary medicine: a scoping review. J Interprof Care. 2024;38(6):1127–1139. doi:10.1080/13561820.2024.2395978
3. Spaulding EM, Marvel FA, Jacob E, et al. Interprofessional education and collaboration among healthcare students and professionals: a systematic review and call for action. J Interprof Care. 2021;35(4):612–621. doi:10.1080/13561820.2019.1697214
4. Kitto S, Wondwossen Fantaye A, Davies N, et al. The evidence base for interprofessional education within health professions education: a protocol for an update review. J Interprof Care. 2023;37(3):515–518. doi:10.1080/13561820.2022.2097651
5. Lestari E, Stalmeijer RE, Widyandana D, Scherpbier A. Understanding students’ readiness for interprofessional learning in an Asian context: a mixed-methods study. BMC Med Educ. 2016;16:179. doi:10.1186/s12909-016-0704-3
6. Shuyi AT, Zikki LYT, Mei Qi A, Koh Siew Lin S. Effectiveness of interprofessional education for medical and nursing professionals and students on interprofessional educational outcomes: a systematic review. Nurse Educ Pract. 2024;74:103864. doi:10.1016/j.nepr.2023.103864
7. Hintenach AM, Howe JL. Interprofessional care: why teamwork matters. In: Geriatric Practice: A Competency Based Approach to Caring for Older Adults. Cham: Springer International Publishing; 2019:491–500.
8. Earl SR, Thweatt L, Parkes E, et al. Bridging disciplines: an evaluation of learning about Interprofessional roles and responsibilities through an interactive group activity. Curr Pharm Teach Learn. 2025;17(4):102268. doi:10.1016/j.cptl.2024.102268
9. Gillani SW, Azhar A, Shadab A, Gulam SM. Perceptions and barriers of health-care professionals to develop and implement interprofessional education in UAE: a qualitative study. J Educ Health Promot. 2022;11:313. doi:10.4103/jehp.jehp_384_21
10. Yasin H, Palaian S, Shankar PR, Nallamilli S. Readiness for interprofessional education among health profession students in a University in the United Arab Emirates. J Multidiscip Healthc. 2023;16:1141–1149. doi:10.2147/JMDH.S395320
11. Murphy JE, Liles AM, Bingham AL, et al. Interprofessional education: principles and application. An update from the American College of Clinical Pharmacy. J Am Coll Clin Pharm. 2018;1(1):e17–28. doi:10.1002/jac5.1025
12. Norris J, Carpenter JG, Eaton J, et al. The development and validation of the interprofessional attitudes scale: assessing the interprofessional attitudes of students in the health professions. Acad Med. 2015;90(10):1394–1400. doi:10.1097/ACM.0000000000000764
13. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psych. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
14. Buring SM, Bhushan A, Brazeau G, Conway S, Hansen L, Westberg S. Keys to successful implementation of interprofessional education: learning location, faculty development, and curricular themes. Am J Pharm Educ. 2009;73(4):60. doi:10.1016/S0002-9459(24)00555-2
15. Gilbert JH, Yan J, Hoffman SJ. A WHO report: framework for action on interprofessional education and collaborative practice. J Allied Health. 2010;39(Suppl 1):196–197.
16. Abu-Rish E, Kim S, Choe L, et al. Current trends in interprofessional education of health sciences students: a literature review. J Interprof Care. 2012;26(6):444–451. doi:10.3109/13561820.2012.715604
17. El-Zubeir M, Rizk DE, Al-Khalil RK. Are senior UAE medical and nursing students ready for interprofessional learning? Validating the RIPL scale in a Middle Eastern context. J Interprof Care. 2006;20(6):619–632. doi:10.1080/13561820600895952
18. Milutinović D, Lovrić R, Simin D. Interprofessional education and collaborative practice: psychometric analysis of the readiness for interprofessional learning scale in undergraduate Serbian healthcare student context. Nurse Educ Today. 2018;65:74–80. doi:10.1016/j.nedt.2018.03.002
19. Mackay S. The role perception questionnaire (RPQ): a tool for assessing undergraduate students’ perceptions of the role of other professions. J Interprof Care. 2004;18(3):289–302. doi:10.1080/13561820410001731331
20. Panel IE. Core competencies for interprofessional collaborative practice: report of an expert panel. Interprofessional Educ Collab Expert Panel; 2011.
21. Sakr CJ, Fakih L, Dejong J, et al. Can interprofessional education change students’ attitudes? A case study from Lebanon. BMC Med Educ. 2022;22(1):570. doi:10.1186/s12909-022-03608-z
22. Dennis V, Craft M, Bratzler D, et al. Evaluation of student perceptions with 2 interprofessional assessment tools-the Collaborative Healthcare Interdisciplinary Relationship Planning instrument and the interprofessional attitudes scale-following didactic and clinical learning experiences in the United States. J Educ Eval Health Prof. 2019;16:35. doi:10.3352/jeehp.2019.16.35
23. Zeeni N, Zeenny R, Hasbini-Danawi T, et al. Student perceptions towards interprofessional education: findings from a longitudinal study based in a Middle Eastern university. J Interprof Care. 2016;30(2):165–174. doi:10.3109/13561820.2015.1117060
24. El-Awaisi A, Awaisu A, El Hajj MS, et al. Delivering tobacco cessation content in the Middle East through interprofessional learning. Am J Pharm Educ. 2017;81(5):91. doi:10.5688/ajpe81591
25. Al-Shaikh GK, Al-Madi EM, Masood J, et al. Interprofessional learning experiences: exploring the perception and attitudes of Saudi Arabian medical and dental students. Med Teach. 2018;40(sup1):S43–S48. doi:10.1080/0142159X.2018.1465180
26. He Q, Dizon JIWT, Ganotice FA, et al. Unveiling the impact of interprofessional education on shaping students’ interprofessional identity and collaboration perception: a mixed-method study. BMC Med Educ. 2024;24(1):855. doi:10.1186/s12909-024-05833-0
27. Tong R, Brewer M, Flavell H, Roberts LD. Professional and interprofessional identities: a scoping review. J Interprof Care. 2020;13:1–9.
28. Reinders JJ, Lycklama À, Nijeholt M, Van Der Schans CP, Krijnen WP. The development and psychometric evaluation of an interprofessional identity measure: Extended Professional Identity Scale (EPIS). J Interprof Care. 2020;3:1–13.
29. Burgess A, Roberts C, van Diggele C, Mellis C. Peer teacher training (PTT) program for health professional students: interprofessional and flipped learning. BMC Med Educ. 2017;17(1):239. doi:10.1186/s12909-017-1037-6
30. Burgess A, van Diggele C, Mellis C. Faculty development for junior health professionals. Clin Teach. 2019;16(3):189–196. doi:10.1111/tct.12795
31. Diggele C, Roberts C, Burgess A, Mellis C. Interprofessional education: tips for design and implementation. BMC Med Educ. 2020;20(Suppl 2):455. doi:10.1186/s12909-020-02286-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.