Back to Journals » Advances in Medical Education and Practice » Volume 16
Impact of an Educational Intervention on Nurses’ Knowledge and Practice in Early Detection of Acute Kidney Injury at Mbarara Regional Referral Hospital, Western Uganda
Authors Phiona W, Murungi EB ![]() , Kasozi J
, Kasozi J ![]()
Received 3 February 2025
Accepted for publication 26 March 2025
Published 31 March 2025 Volume 2025:16 Pages 503—514
DOI https://doi.org/10.2147/AMEP.S516379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Were Phiona,1 Eric Baluku Murungi,2 Jannat Kasozi1
1Department of Nursing, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara City, Uganda; 2Department of Emergency Nursing, Faculty of Nursing and Midwifery, Lira University, Lira, Uganda
Correspondence: Eric Baluku Murungi, Department of Emergency Nursing, Faculty of Nursing and Midwifery, lira university, lira University, Uganda, Tel +256773595259, Email [email protected]
Introduction: Acute Kidney Injury (AKI) is a common, often undocumented disorder causing significant morbidity and high mortality. It affects 20% of hospitalized patients, with over 50% incidence in ICUs. Nurses play a crucial role in AKI management, particularly in in-patient care. Early detection and management depend on nurses’ knowledge and practice, impacting outcomes. AKI is a global concern, with over 2.3 million projected annual deaths worldwide.
Aim: To examine the impact of an educational intervention on nurses’ knowledge and practice in early detection of AKI at Mbarara Regional Referral Hospital.
Methods: A quasi-experimental study was conducted at Mbarara Regional Referral Hospital in the Accident and Emergency and Intensive Care Units. It involved a pre-test, intervention, and post-test. Thirty nurses completed self-administered questionnaires to assess knowledge, while 25 medical charts were reviewed using a checklist to evaluate practice. Paired t-tests and Chi-square tests were used to analyse changes in knowledge and practice before and after an educational intervention.
Results: The findings revealed that the knowledge and practices in early detection of AKI among the nurses was inadequate with only 3.3% of the nurses having excellent knowledge in the early identification of AKI while most of the medical charts had incorrectly performed practices. However, after the educational intervention the knowledge and practice in detection of AKI improved. The mean knowledge scores were 43.0333 (SD = 16.9) pre-test and 68.3 (12.8) post-test. There were significant differences in mean knowledge and practice scores before and after intervention, mean of (t (29) with 18.7018– 31.96487 (95% confidence interval) and P-value of < 0.0001.
Conclusion: There is a need to organize regular sessions on AKI to improve the knowledge and practices of nurses in early detection of AKI.
Keywords: acute kidney injury, RIFLE, NICE, KDIGO, early detection
Background
Acute Kidney Injury (AKI) is a common, frequently undocumented disorder which causes significant morbidity and a high projected annual mortality of greater than 2.3 million worldwide.1 It is a rapid loss in kidney function over a period of hours to days, resulting in a buildup of creatinine, urea, and other waste products in the blood.2,3 According to the RIFLE (Risk, Injury, Failure, Loss and End stage kidney disease) classification, AKI is defined as an increase in serum creatinine (SCr) or decreased estimated glomerular filtration rate (eGFR) and/or a decrease in urine output (UO). RIFLE identifies three severity levels (risk, injury, and failure) and two outcomes (loss of kidney function and end-stage kidney disease) in AKI.4 This was modified by the AKI Network (AKIN) to include an absolute change of SCr consequently defining AKI as an increase in SCr by 0.3 mg/dl within 48 hours or by a decrease in UO lower than 0.5 mL/kg/hr for more than 6 hours.5 Finally, the Kidney Disease: Improving Global Outcomes group, a global non-profit organization, unified RIFLE and AKIN definitions. This includes an increase in serum creatinine by 0.3 mg/dL or more within 48 hours, or an increase in serum creatinine to 1.5 times baseline or more within the last 7 days, or urine output less than 0.5 mL/kg/h for 6 hours, improving AKI definition.6
Timely recognition of patients at risk or with possible AKI is essential for early intervention to minimize further damage that is refractory to fluid resuscitation and circumvent the need for renal replacement therapy (RRT).7
In high and low resource limited countries, AKI is a common complication affecting 20% of hospitalized patients. It is more pronounced in the Intensive Care Units (ICU), where the incidence is over 50% in critically ill patients. This develops at some point during the progression of their critical illness with greater than 50% mortality.3,8
In high resource countries, early patient identification and progressive treatment are regularly available.9 However, this does not happen in low resource countries due to the limited resources and misdiagnosis of the condition.10,11 This limits awareness and early recognition, delaying implementation of measures that permit early and adequate management.12 In low resource countries guidelines by the KDIGO group to improve early detection of AKI has not been implemented because of economic disparities, resource limitation and shortage of trained personnel.7,13
There are two types of AKI, namely hospital acquired AKI (h-AKI) and community acquired AKI (c-AKI). The h-AKI occurs as a complication during a hospital stay, resulting from post-surgical complications, hemorrhage, infections, septic shock and drug toxicity while c-AKI, in the low resource settings, commonly results from infections such as malaria, obstetric complications, intake of herbal remedies and traumatic injury (Ponce, 2016).
Therefore, AKI detection necessitates nurses’ awareness of the risk factors, which include the age of the patient, comorbidities such as hypertension, diabetes mellitus and chronic kidney disease (CKD) with knowledge of common causes. Additionally, continuous monitoring of urine output and obtaining serum creatinine levels are important for diagnosis of AKI, and therefore ensures early fluid resuscitation which improves outcomes and decreases mortality.14
Currently, mortality from AKI is higher than prostate cancer, breast cancer, heart failure and diabetes. Awareness of prevention or management of AKI by relatively simple measures such as fluid resuscitation, identification and treatment of underlying condition, and discontinuing nephrotoxic drugs can timely salvage abnormal renal function. This might prevent development of CKD which requires Renal replacement therapy (RRT) that is not widely available in Uganda.15,16
According to Adejumo, Akinbodewa17 nurses play a key role in management of patients, more so those receiving in-patient care. Early detection of AKI, its management, and outcomes are all dependent on nurses’ knowledge of AKI. Educating nurses about AKI is important in attaining the International Society of Nephrology (ISN) vision of zero mortality from AKI by the year 2025, especially in developing countries like Uganda.
Methodology
Study Design
A descriptive quantitative, quasi-experimental study was used. It included a pre-test, intervention and post-test. An intervention was employed, to create awareness about AKI screening tools for early detection and management of AKI. A quasi experiment design uses quantitative research to explain relationships, clarify why certain events happen, and examine causality between selected independent and dependent variables in conditions not conducive for experimental controls.18
Study Site
The study was conducted at Mbarara Regional Referral Hospital (MRRH) in the Accident and Emergency Unit (A&E) and Intensive Care Unit (ICU). The A&E unit is subdivided into four areas; the triage area has a two-bed capacity and receives all the emergency cases, stabilizes, then transfers to their respective areas. The resuscitation area has only one bed, the surgical area is an eight bed capacity that handles only surgical emergency cases and finally the medical area which is also an eight bed capacity that handles all the medical emergencies. On the other hand, the ICU is a fully equipped eight bed capacity. MRRH is the biggest public hospital in the southwestern region of Uganda, located in Kamukuzi division, Mbarara Municipality, Mbarara district, about 265 km from Kampala city. It was founded in 1940 and receives patients from several districts including Mbarara, Ibanda, Isingiro, Kiruhura, Mitooma, Ntugamo, Bushenyi, Buhweju, Rubirizi, Sheema and also countries like Rwanda, Burundi, Congo, Kenya and Tanzania. It serves as a teaching hospital for Mbarara University of Science and Technology. It has a bed capacity of 600 and provides both inpatient and outpatient services.
Study Population
The study population included all nurses working in the accident and emergency wards and intensive care unit. A total of 30 nurses were located in these two units with 15 nurses in the accident and emergency unit and 15 nurses in the intensive care unit. These 2 areas were selected because they care for the critically ill patients who may develop AKI.
Inclusion Criteria
All staff nurses presently employed by the MRRH including intern nurses with more than three months experience in the intensive care and accident and emergency units who consented to participate at time of the study.
Exclusion Criteria
Nurse who were on leave or absent due to other commitments during the time of data collection.
Sample Size
The intensive care unit (ICU) had a total of 15 nurses, and the accident and emergency had also total of 15 nurses, which led to a total of 30 nurses. For a planned t-test analysis, a priori power analysis indicated a total sample size of 22 to detect a large effect (Cohen’s d=0.5) with α =0.05 and 1-β=0.95.19 To all for an anticipated attrition of ten percent, the researcher aimed at having all 30 nurses participate in the study.
Sampling Technique
All staff nurses and intern nurses working in the intensive care, accidents and emergency units were invited to participate in the, educational intervention and a posttest.
Data Collection Tools
The study utilized two tools, one to measure knowledge and one to examine practice.
a) A pre-test self-administered questionnaire was adapted from two sources to assess nurses’ knowledge. The first source was a questionnaire from a prospective multi-center study conducted in Brazil related to AKI prevention, diagnosis, and treatment20 and the second source was a questionnaire from a cross-sectional survey conducted in the United Kingdom to enable recognition of AKI.21 The questionnaire consisted of 14 multiple choice or true/false questions related to nurse’s knowledge on AKI detection and management.
b) Practice was measured using a checklist that was developed by the investigator using available literature with the assistance of two supervisors who are affluent in research. The checklist was used by the investigator to review the patient’s medical charts and observe nurses to ascertain whether the nurses were practicing the protocols for early detection of AKI.
Data Collection Procedure
The investigator contacted the in-charges of those units and organized meetings with the nursing staff in which the investigator explained the purpose of the study and the relevant details. All nurses who consented to the study were given a pre-test questionnaire to fill and later interventional education training was conducted. A post-test was then given after a period of one month from the intervention to assess the change in knowledge. A non-participant structured observational screening tool was adapted and used in this study to obtain briefly what was happening in practice in early detection of AKI among nurses and then an educational training was conducted. One month later a similar tool was implemented to check if participants’ (nurses) knowledge and practice had changed.
The following was a description of how data was collected in different phases:
- Pre-intervention phase: participants’ demographic data and pre-intervention knowledge about AKI using a questionnaire that was written based on the National Institute for Health and Care Excellence (NICE) guidelines for AKI was assessed. Participants were assured of confidentiality of their information. A check list was also completed on 25 medical charts for the patients currently admitted on the units/wards and observation on nurses was done to measure current practices related to AKI identification and monitoring and it took 30 minutes to answer the questionnaire and checklist.
Intervention phase: an education intervention was conducted immediately on completion of the pre-intervention assessment. The investigator conducted a face to face teaching session on nurses for each of the involved units/wards lasting for one hour for one week and also five minute audio-visual video. This was done in the afternoon hours to avoid disrupting the hospital activities since in the morning hours the unit/wards were quite busy. The researcher also used audio-visual aids to ensure a deeper understanding of the sessions. The participating nurses were given a folder containing the information taught about AKI. The training session aimed to increase nurses’ knowledge on early detection of AKI, a detailed overview of the NICE AKI guidelines, including key recommendations for prevention, early detection, and management of AKI and practical examples of how to apply the NICE guidelines in real-world clinical scenarios.
- Post-intervention phase: After the intervention, a post intervention evaluation was done after one month had elapsed to assess the outcome of the education interventions on the nurses’ knowledge on the use of the NICE guidelines for AKI. Patients’ files were also reviewed to examine whether the taught NICE guidelines have been followed in patient management.
Data Analysis
Data were analyzed using STATA version 14 for statistical analysis. Descriptive statistics were used. A paired t-test was used to test the null hypothesis, and compared participants’ knowledge in regards to early detection of AKI before and after intervention. Data on knowledge and practice were as analyzed and presented in the form of frequencies and percentages, means and standard deviations (SD). The mean knowledge scores were calculated out of a set maximum score points for both pre- and post-test intervention, and this was done after the assumption of normality was fulfilled using skewness and kurtosis test. Pre-intervention test was done to assess nurses’ knowledge gaps in early identification of patients at risk or with AKI using the NICE guidelines for AKI which indicated the need for the educational intervention.
Scores for the recorded practices was assessed both pre- and post-test. A Chi-square test was used to test the comparison of the participants’ practices before and after the intervention. This was done to determine whether nurses’ practices are consistent with the recommended NICE guidelines for AKI.22
Ethical Consideration
Initially approval was obtained from the nursing department, Faculty Research Committee (FRC) and MUST Research Ethics Committee (REC). Then administration clearance was obtained from the Hospital Director of Mbarara Regional Referral Hospital. A written informed consent was obtained from the nurses before participation in the study. This included the pre-test and posttest for knowledge and practice of the AKI screening tools. Confidentiality was maintained using numbers instead of participants names and privacy enabled throughout the study. We ensured the information obtained from the questionnaires was kept safe and only accessible by the researcher.
Results
This study was conducted in three units that included: The Intensive Care Unit and Accident and Emergency (Medical Unit and Surgical Unit). The period of data collection was from 1st October 2020 to 12rd November 2020. Self-administered questionnaires were distributed to 30 participants. The target population was nurses in the above mentioned units. Research results are categorized according to the sections of data collection instrument which are: Demographic data, knowledge of nurses’ in early detection of AKI and their practices in early detection of AKI.
Demographic Characteristics of the Participants
Table 1 summarizes the demographic data of the participants. The results indicate that the female participants were slightly higher 17 (56.7%) than the male. The mean age of the participants was 38.3 years ranging from 25 years to 52 years and the dominant age group was between 31–40 years 11 (36. 7%). The level of experience varied from 2 years to 21 years with more than fifteen years taking up the highest percentage 10 (33. 3%). Regarding the unit majority of the participants 15 (50%) worked in ICU. Level of education was also questioned in the sample characterization study. Of all 30 nurses that participated in the study, the highest number were 13 (43.3%) with a Diploma. It was vital to determine if the nurses had any previous AKI training however, only 3 (10%) of the nurses had received AKI training before the study.
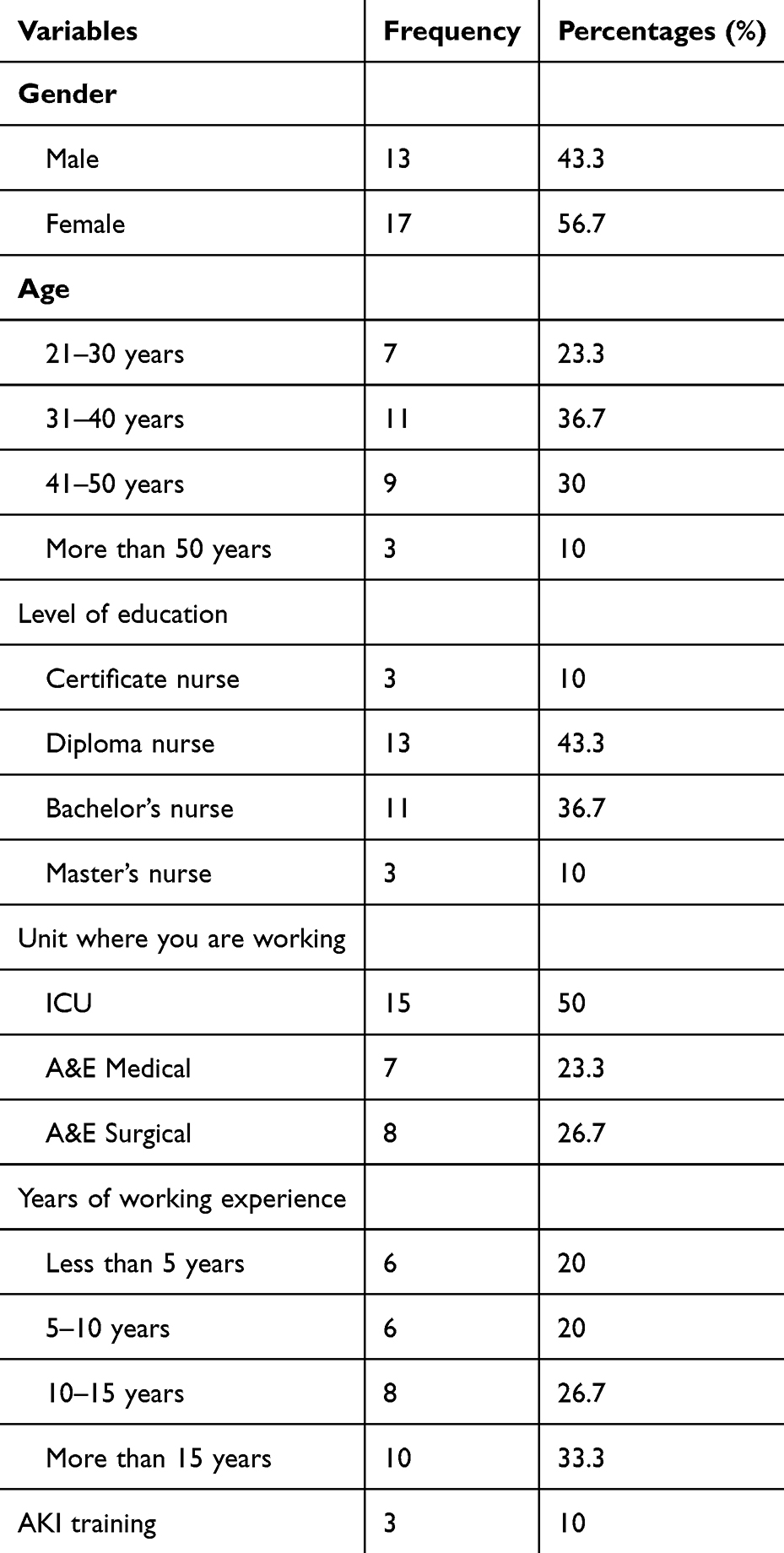 |
Table 1 Demographic Data of the Participants (n=30) |
Knowledge in the Early Detection of AKI (n=30)
The participants’ knowledge in early detection of AKI were categorized according to the scores. From Table 2, the majority 20 (66.7%) of the participants had poor knowledge in early detection. The total average score of all the participants was calculated to determine the performance prior to an educational intervention. The average score was 43.0% with a standard deviation of 16.9%.
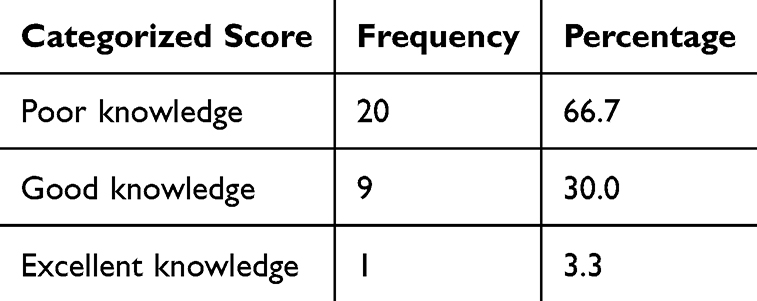 |
Table 2 Showing the Nurses’ Knowledge Score in Early Detection of AKI at Baseline |
Practice in Early Detection of AKI (n=25)
From Table 3, most of the patient medical charts had fluid input 20 (80%) and systolic blood pressure 18 (72%) fully performed and documented. Additionally, the infection prevention measures were inadequately done where only 15 (50%) of the participants could correctly perform handwashing. The least performed practice was use of protective gear with 21 (70%) of the participants incorrectly performing it.
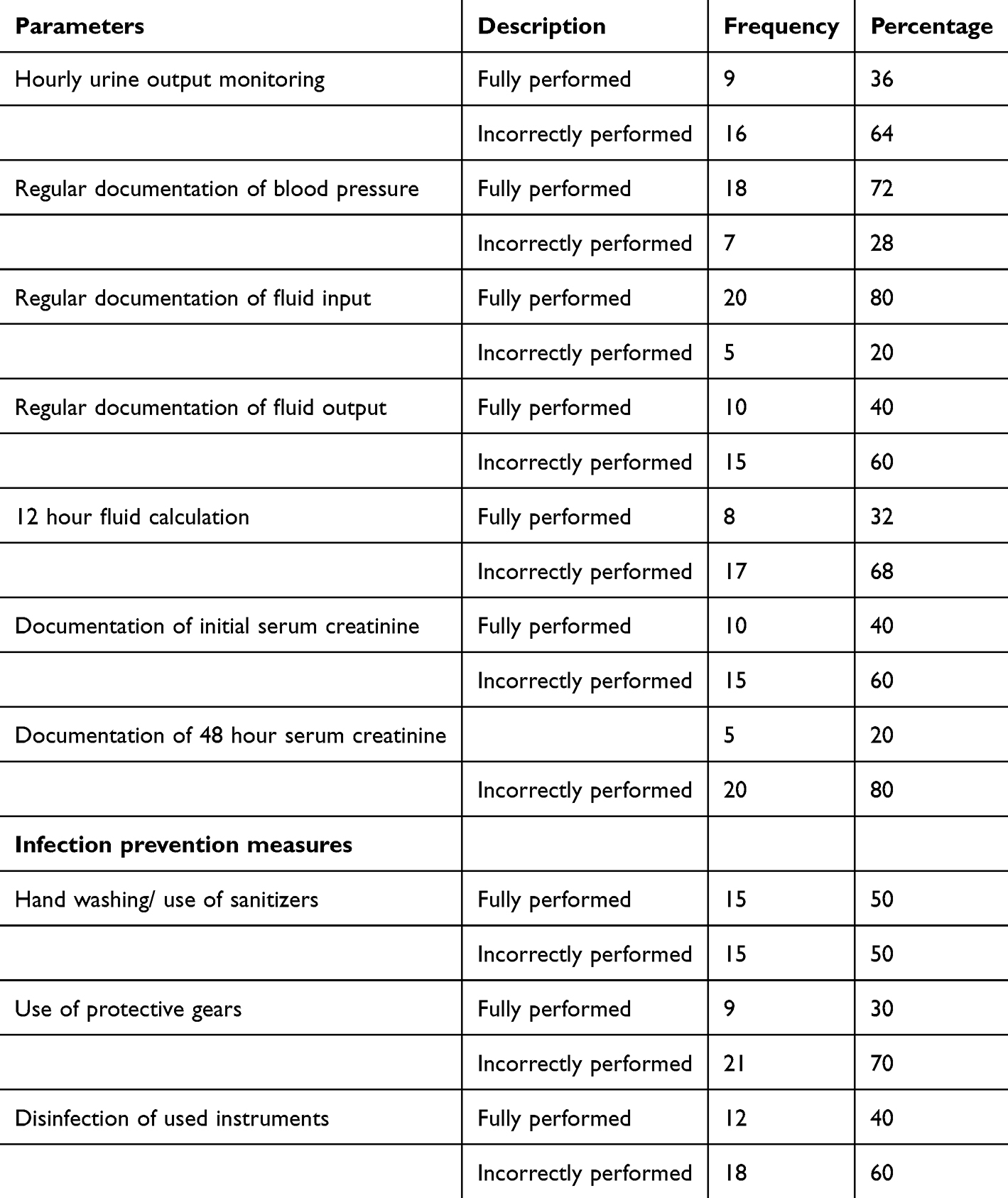 |
Table 3 Showing Practice at Baseline |
Outcome of an Educational Intervention on Nurses’ Knowledge and Practice in Early Detection of AKI
Outcome of an Educational Intervention in Early Detection of AKI
The same questionnaire was used to assess the nurses’ knowledge after the educational intervention. This was done to determine if the nurses’ knowledge in early detection of AKI had improved or remained the same.
Table 4 shows the participants’ categorized score on knowledge in early detection of AKI after the education intervention. After the educational intervention majority of the participants 17 (56.7%) had good knowledge. The total average score of all the participants on knowledge was also calculated to determine the general performance of the participants after the educational intervention. The average score was 68.3% with a standard deviation of 12.8%.
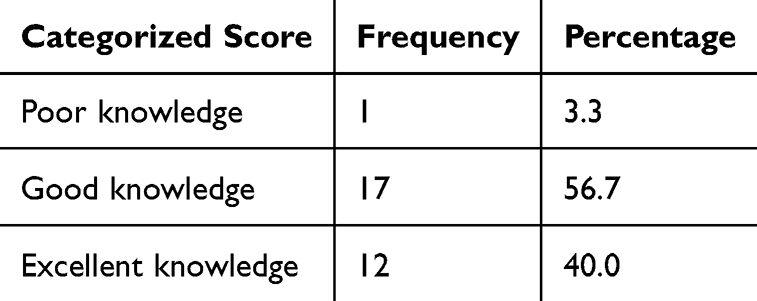 |
Table 4 Showing the Nurses’ Knowledge Score in Early Detection of AKI After the Educational Intervention |
A paired t test was also done to determine if the average score of all participants before and after the educational intervention had a statistically significant difference.
From Table 5, the mean of the pre-score and post-score is different since the confidence interval of the two means are not overlapping and also thep value is less than 0.0001, showing that the difference in the two means is statistically significant. Therefore, the null hypothesis stating that there is no difference in the two means was rejected. This suggests that the educational intervention had an impact on the nurses’ knowledge in early detection of AKI as reflected by the increase in the post score average of all the participants in the study.
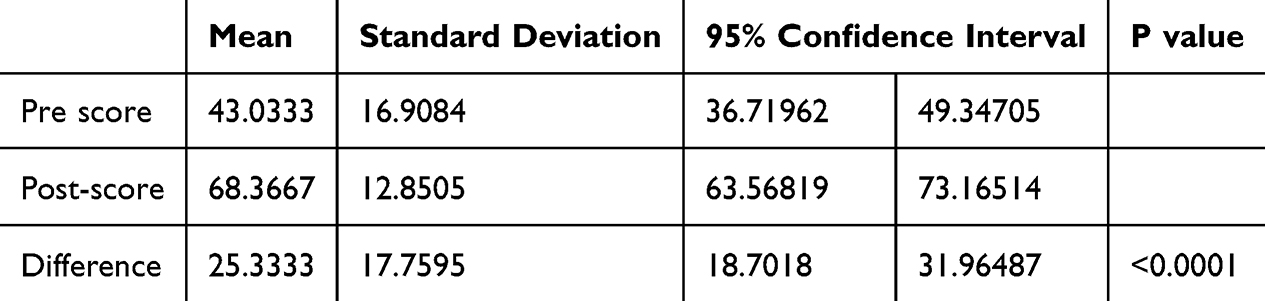 |
Table 5 Shows a Paired t Test Done on the Pre-Score and Post-Score Mean to Test if They are Statistically Different |
Outcome of Educational Intervention on Nurses Practice in Early Detection of AKI
For the assessment of post intervention practices 25 medical charts were reviewed after the educational intervention. Table 6 shows the comparison between pre-intervention and post-intervention practices performed to enable early detection of AKI.
From Table 6 it was observed that the performed practices improved after the educational intervention. The P values of each parameter observed was statistically significant showing that the practices before the educational intervention were different from the practices performed after the educational intervention.
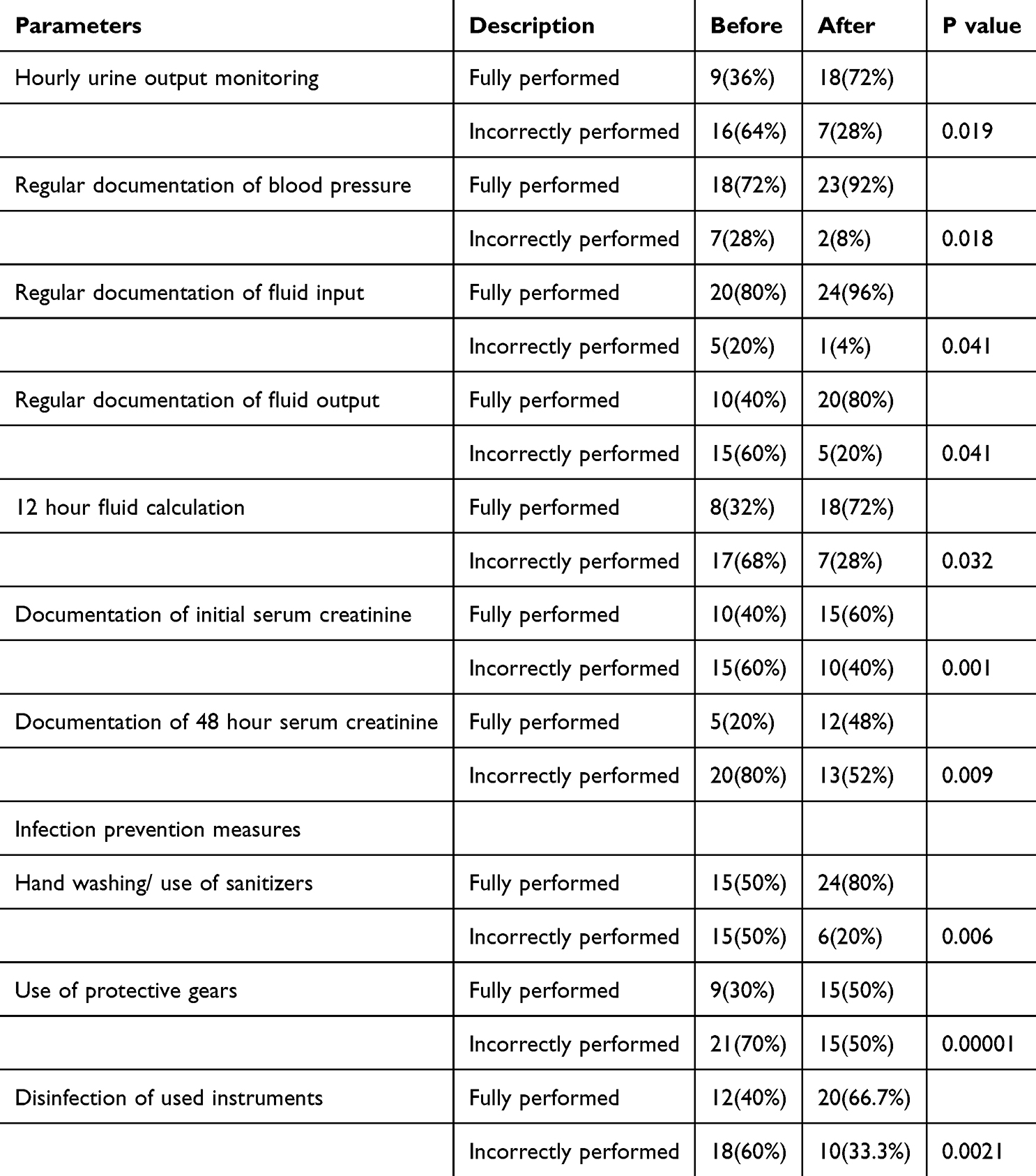 |
Table 6 Comparing the Practice Before and After Intervention |
Discussion
The results of this study showed that the female participants were slightly higher than the male participants within the middle age. On the level of education, most participants were diploma holders with majority having more than fifteen years of working experience.
The findings highlighted that nurses had inappropriate knowledge and practices regarding early detection of AKI. However, after the educational intervention the nurses’ knowledge and practice in early identification of AKI improved.
Nurses Knowledge in the Early Detection of AKI
According to the study findings, participants had inadequate knowledge on early identification of AKI. These findings are similar to a study done on health workers in Malawi which found that all had inadequate knowledge and confidence in management of AKI with 100% of the nurses who were involved in the study lacking knowledge.15 In line with this study, two other studies in South Nigeria and Rwanda reported that only 12% and 5.4% of the nurses had good knowledge on AKI respectively.17,23 Nurses play a key role in patients’ management, especially those receiving in-patient care. Their knowledge on various aspects of AKI would have effect on early diagnosis, management, and outcome of AKI.17 Nurses are required to be able to identify patients at risk of AKI: such as those with excessive bleeding or have had severe trauma, hypovolemic, edematous, hypotensive, those taking nephrotoxic drugs, critically ill patients and those with heart failure then report the unusual findings to the physician to enable quick and correct response taken and prevent kidney failure. In most health facilities, nurses are very essential because they spend more time with the patients than any other health worker. So it is vital for them to be properly equipped with correct information about AKI to enable early detection of AKI.
This finding therefore indicate that the overall patient care would be affected with the inadequate knowledge of nurses in early detection of AKI.
Nurses’ Practices on Early Detection of AKI
The findings on practices done by nurses to enable early detection of AKI were found to be inadequate. Reviewing the 25 medical charts of the patients that were admitted at the time of study showed that most of the parameters such as urine output monitoring, systolic blood pressure monitoring, fluid input and output monitoring, fluid balance calculation and creatinine documentation were not done as recommended. Only 9 (36%) of the medical charts had hourly urine output documented. These findings were similar to a study done in west African countries that showed that the majority of the nurses did not monitor the urine output of critically ill patients and worse still did not know that hourly urine output monitoring and recording was associated with early identification of AKI. Similarly, obtaining serum creatinine levels are important for diagnosis of AKI, and therefore ensures early fluid resuscitation which improves outcomes and decreases mortality.14
Although 18 (72%) of the medical charts had the systolic blood pressure documented this was only done on physician’s recommendation. Nurses ought to know that intensive blood pressure monitoring is associated with early detection of AKI since it shows the amount of blood flow to the kidneys.24 It was also observed that only 8 (32%) of the medical charts had a 12-hour fluid balance calculated. Fluid balance calculation is vital in early identification of AKI in the critically ill. In a study done to determine the association of fluid balance and mortality of critically ill patients with AKI indicated that daily fluid balance was higher in the patients who had AKI.25 Optimal fluid balance management is essential for the prevention of AKI. In non-AKI studies, a positive fluid balance was strongly associated with increased mortality and other unfavourable outcomes in some subgroups of ICU patients, including worse lung function, longer duration of mechanical ventilation, increased post-operative complications and longer ICU stay.26
Infection prevention measures were also observed among the nurses using a checklist which included handwashing practices, use of protective gear and disinfection of instruments. It was observed that the majority of the nurses performed the practices inadequately. Hand washing or use of sanitizers was only done appropriately by 15 (50%) of the nurses in the three units with the least performed practice being use of protective gear during the procedures being done by only 9 (30%) of the nurses. A recent systematic review done on incidence of AKI in COVID-19 infection showed that AKI has been reported as a severe complication of COVID-19 with a higher risk of mortality.27 Therefore the nurses need to adhere to the infection prevention measures to prevent development of AKI from infections.
Outcome of an Educational Intervention on Nurses’ Knowledge and Practice in Early Detection of AKI
Following the educational intervention, there was a significant overall increase in correct response rate with the majority of participants answering most of the questions correctly on knowledge in relation to early detection of AKI. This mean knowledge score for the nurses improved from 43.0% before the educational intervention to 68.3% after the educational intervention. Xu, Baines28 assessed clinicians’ knowledge on AKI and found that only 26% of them were aware of AKI guidelines compared to 64% after the educational intervention. This also correlates to a study done in two large acute teaching hospital in England where they found that education improved AKI guidelines awareness and also patient outcomes.28 Concurrently, the nurses’ practices towards early detection of AKI had improved after the educational intervention in the study area. Nurses had improved in hourly urine output documentation as majority of the medical charts had hourly urine output monitored after the education intervention. This was also true for systolic blood pressure monitoring, fluid input and output documentation, fluid balance calculation and creatinine documentation as the P- values were statistically significant. It was found that AKI was poorly managed in a district general hospital with the ABCDE: steps (address drugs, boost blood pressure of less than 90 mmHg, calculate fluid balance, dip urine and exclude obstruction) only being implemented in 20% of the cases. This was improved by educating the entire multidisciplinary team to identify three key early warning signs. A rise in serum creatinine, urine output of less than 500mls in 24 hours and systolic blood pressure of less than 90mmHg. In addition the use of ABCDE checklist led to an improvement in care of critically ill patients.29
Conclusion
The results found that nurses had inadequate knowledge and practices in regards to AKI timely identification prior to the educational intervention but after the educational intervention their knowledge and practice in early detection of AKI was improved.
Acute Kidney Injury is a very common and fatal condition that requires timely identification to prevent the patients from developing chronic kidney disease that has a high mortality rate. Equipping nurses with knowledge in early detection of AKI is important because they remain the most forefront health care providers who spend more time with the ill patients and are able to detect the slightest change in the condition of patient sthey are managing and immediately inform the physician to enable quick response.
Recommendation
There is a need to ensure nurses receive comprehensive educational interventions on AKI to improve their knowledge and practices in early detection.
The educators need to be kept updated on current trends of AKI in relation to the prevalence, incidence, mortality rate of AKI and ensure that they emphasize these when educating nurses. Students need to be aware of the risk factors, clinical manifestations and management of AKI.
Study Limitations
The main study limitation was the small sample size that limited generalizability. The hospital departments studied were representative of other general hospitals and the results may be of use to other clinicians. Due to the nature of the study design as applied to this study, there was no control group to compare the results to and this may have affected the internal validity of the study. Intervention studies generally recommend a minimum of 6 weeks to collect data post-intervention. In this study, however, we performed post-intervention data collection at 4 weeks, as adopted from some studies that considered a minimum of 4 weeks post-intervention to be sufficient. The argument is that the participants’ memories of the training content may have been quite fresh, with seemingly very good results.
Nursing Implications
The study reinforces the importance of established frameworks like KDIGO in defining and managing AKI. It highlights the gap between these guidelines and their implementation in low-resource settings.
The study provides evidence for the effectiveness of educational interventions in improving nurses’ knowledge and practices related to AKI. This supports the implementation of regular training sessions and the use of tools like the NICE guidelines.
Conducting studies with larger sample sizes and across multiple sites would enhance the generalizability of the findings and also longitudinal studies to assess the long-term impact of educational interventions on nurses’ practices and patient outcomes.
Abbreviations
AKI, Acute Kidney Injury; AKIN, Acute Kidney Injury Network; CKD, Chronic Kidney Disease; c- AKI, community acquired Acute Kidney Injury; eGFR, estimated Glomerular Filtration Rate; ESKD, End Stage Kidney Disease; h-AKI, hospital acquired Acute Kidney Injury; ICU, Intensive care unit; ISN, International Society of Nephrology; KDIGO, Kidney Disease: Improving Global Outcomes; MRRH, Mbarara Regional Refferal Hospital; NICE, National institute for health and care excellence; PCI, Percutaneous Coronary Interventions; RIFLE, Risk, Injury, Failure, Loss and End stage kidney disease; RRT, Renal Replacement Therapy; SCr, Serum Creatinine; UO, Urine output.
Acknowledgments
The research reported in this publication was supported by the first Mile project. The content is solely the responsibility of the authors and does not necessarily reflect the official views of the First Mile Project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Directorate of Research and Graduate Training Mbarara Grants Office. The content is solely the responsibility of the authors and does not represent the official opinion of the Directorate of Research and Graduate Training Mbarara Grants Office.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Mehta R, Bagga A, Patibandla R, Chakravarthi R, et al. Detection and management of AKI in the developing world: the 18th acute disease quality initiative (ADQI) international consensus conference. Kidney Int Rep. 2017;2(4):515–518. doi:10.1016/j.ekir.2017.03.013
2. Hertzberg D, Rydén L, Pickering JW, Sartipy U, Holzmann MJ. Acute kidney injury—an overview of diagnostic methods and clinical management. Clin Kidney J. 2017;10(3):323–331.
3. Mohsenin V. Practical approach to detection and management of acute kidney injury in critically ill patient. J Intensive Care. 2017;5(1):57. doi:10.1186/s40560-017-0251-y
4. Gameiro J, Agapito Fonseca J, Jorge S, Lopes JA. Acute kidney injury definition and diagnosis: a narrative review. J Clin Med. 2018;7(10):307.
5. Singbartl K, Kellum JA. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int. 2012;81(9):819–825.
6. Kellum JA, Lameire N; KDIGO AKI Guideline Work Group. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care. 2013;17(1):204.
7. Kher V, Srisawat N, Noiri E, et al. Prevention and therapy of acute kidney injury in the developing world. Kidney Int Rep. 2017;2(4):544–558.
8. Silver SA, Adu D, Agarwal S, et al. Strategies to enhance rehabilitation after acute kidney injury in the developing world. Kidney Int Rep. 2017;2(4):579–593. doi:10.1016/j.ekir.2017.04.005
9. Bouchard J, Acharya A, Cerda J, et al. A prospective international multicenter study of AKI in the intensive care unit. Clin J Ame Soc Nephrol. 2015;10(8):1324–1331.
10. Bagasha P, Nakwagala F, Kwizera A, et al. Acute kidney injury among adult patients with sepsis in a low-income country: clinical patterns and short-term outcomes. BMC Nephrol. 2015;16(1):4. doi:10.1186/1471-2369-16-4
11. Cerdá J, Mohan S, Garcia-Garcia G, et al. Acute kidney injury recognition in low-and middle-income countries. Kidney Int Rep. 2017;2(4):530–543. doi:10.1016/j.ekir.2017.04.009
12. Hulse C, Davies A. Acute kidney injury: prevention and recognition. Nurs Times. 2015;111(30–31):12–15.
13. Kathuria D, Singh N. Prevention and management of acute kidney injury: what a physician should know. J Assoc Phys Ind. 2017;65:74.
14. Bouchard J, Acharya A, Cerda J. A nurse‐led intervention improves detection and management of AKI in Malawi. Clin J Ame Soc Nephrol. 2016;42(4):196–204.
15. Evans R, Rudd P, Hemmila U, Dobbie H, Dreyer G. Deficiencies in education and experience in the management of acute kidney injury among Malawian healthcare workers. Malawi Med J. 2015;27(3):101–103.
16. Li PKT, Burdmann EA, Mehta RL. Acute kidney injury: global health alert. Arab J Nephrol Transplant. 2013;6(2):75–81.
17. Adejumo OA, Akinbodewa AA, Alli OE, Pirisola OB, Abolarin OS. Knowledge of acute kidney injury among nurses in two government hospitals in Ondo City, Southwest Nigeria. Saudi J Kidney Dis Transpl. 2017;28(5):1092.
18. Grove SK, Burns N, Gray J. The Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence. Elsevier Health Sciences; 2012.
19. Buchner A, et al. G* power (version 3.1. 2)[computer program]. 2009.
20. Nascimento RA, Assunção MS, Silva Junior JM. Nurses’ knowledge to identify early acute kidney injury. Revista da Escola de Enfermagem da USP. 2016;50(3):399–404.
21. Blakemore N, Bhandari S. Increasing knowledge of Acute Kidney Injury (AKI). Metric J. 2016. 1(4).
22. Ftouh S, Thomas M. Acute kidney injury: summary of NICE guidance. BMJ. 2013;347:f4930. doi:10.1136/bmj.f4930
23. Knowledge of nurses in early detection and management of a te kidney injury in a selected hospital in Rwanda. 2017.
24. Rocco MV, Sink KM, Lovato LC. Effects of intensive blood pressure treatment on acute kidney injury events in the systolic blood pressure intervention trial (SPRINT). Ame J Kidney Dis. 2018;71(3):352–361.
25. Fluid balance and mortality in critically ill patients with acute kidney injury: a multicenter prospective epidemiological study. Crit Care. 2015;19(1):371.
26. Teixeira C, Garzotto F, Piccinni P. Fluid balance and urine volume are independent predictors of mortality in acute kidney injury. Critical Care. 2013;17(1):R14. doi:10.1186/cc12484
27. Chen YT, Shao SC, Hsu CK, Wu IW, Hung MJ, Chen YC. Incidence of acute kidney injury in COVID-19 infection: a systematic review and meta-analysis. Crit Care. 2020;24(1):1–4.
28. Xu G, Baines R, Westacott R, Selby N, Carr S. An educational approach to improve outcomes in acute kidney injury (AKI): report of a quality improvement project. BMJ Open. 2014;4(3):e004388. doi:10.1136/bmjopen-2013-004388
29. Forde C, McCaughan J, Leonard N. Acute kidney injury: it’s as easy as ABCDE. BMJ Qual Improvement Rep. 2012;11:u200370.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.