Back to Journals » Infection and Drug Resistance » Volume 19
Impact of a Pharmacist-Led Grid-Based Stewardship Program on the Association Between Antimicrobial Use and Resistance: A 7.5-Year Interrupted Time-Series Analysis in a Chinese Tertiary Hospital
Authors Mei Z ![]() , Zhou L
, Zhou L ![]() , Tan Y, Xu B, Wu J
, Tan Y, Xu B, Wu J ![]() , Zheng T, Guan T, Xi W, Jin G
, Zheng T, Guan T, Xi W, Jin G
Received 15 February 2026
Accepted for publication 18 May 2026
Published 26 May 2026 Volume 2026:19 603756
DOI https://doi.org/10.2147/IDR.S603756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Zhao Mei,1,2 Li Zhou,1,2 Yueqing Tan,1,2 Bang Xu,1,2 Jinhua Wu,1,2 Tieqi Zheng,1,2 Tao Guan,3 Wei Xi,1,2 Guilan Jin1,2,4
1Department of Pharmacy, The First College of Clinical Medical Science, China Three Gorges University, Yichang, People’s Republic of China; 2Department of Pharmacy, Yichang Central People’s Hospital, Yichang, People’s Republic of China; 3Department of Clinical Laboratory, Yichang Central People’s Hospital, Yichang, People’s Republic of China; 4Institute of Pharmaceutic Preparation, China Three Gorges University, Yichang, People’s Republic of China
Correspondence: Zhao Mei, Department of Pharmacy, The First College of Clinical Medical Science, China Three Gorges University, Yichang, People’s Republic of China, Email [email protected]
Background: Whether antimicrobial stewardship programs (ASPs) modulate the association between antimicrobial use and resistance remains uncertain. Long-term evidence for precision stewardship models in Chinese tertiary hospitals is scarce.
Methods: A 7.5-year interrupted time-series analysis (2018– 2025) was conducted at a 1900-bed Chinese tertiary hospital. A pharmacist-led, grid-based precision ASP—stratifying 29 departments via Boston Matrix and integrating four synergistic pillars—was implemented in July 2020. Segmented regression models, adjusted for seasonality and autocorrelation, evaluated changes in antimicrobial use density (AUD), clinical/economic outcomes, and the temporal association (R2) between AUD and multidrug-resistant organism (MDRO) detection rates.
Results: The ASP was associated with an immediate AUD reduction (− 25.6%, β2 = − 14.55 DDDs/100 patient-days, P < 0.001) and a sustained decline in antimicrobial use rate (β3 = − 0.003, P < 0.001). Key antimicrobial classes showed marked reductions (fluoroquinolones: − 40.2%; carbapenems: − 16.1%). The ASP was also associated with improved clinical outcomes, including shorter median length of stay (10.9 to 8.8 days), 52% lower all-cause mortality (0.79% to 0.38%, P < 0.001), and declining per capita antimicrobial costs (β3 = − 19.39 CNY/month, P < 0.001). Notably, the AUD-MDRO temporal association varied across pathogens: R2 for MRSA, CREco, and CRAB decreased by 71.8% to 87.0%, moderately weakened for CRKP (49.8%), but paradoxically strengthened for CRPA (+78.3%).
Conclusion: This grid-based precision ASP was associated with sustained reductions in antimicrobial use and costs, and improved clinical outcomes. It was also associated with changes in the temporal relationship between AUD and MDRO detection rates. These alterations suggest this approach may mitigate selective pressure driving resistance, although causality cannot be established in this observational study. This framework may serve as a policy-aligned reference for large tertiary hospitals and provide useful insights to inform local and national antimicrobial stewardship initiatives.
Keywords: temporal association, antimicrobial stewardship, pharmacist-led intervention, grid-based precision management, interrupted time-series analysis, multidrug-resistant organism
Introduction
Antimicrobial resistance (AMR) constitutes a paramount global public health threat, with projections estimating over 39 million cumulative deaths and an economic burden of up to US$100 trillion by 2050.1,2 As a leading consumer of antimicrobials, China’s healthcare system, particularly its tertiary hospitals, faces intense pressure to curb inappropriate use—a primary driver of resistance.3,4 In response, national policies mandate the implementation of antimicrobial stewardship programs (ASPs) in tertiary hospitals, with pharmacist-led, multidisciplinary models recognized as a cornerstone strategy.5,6
Despite this policy impetus, critical evidence gaps in ASP evaluation persist. Most published evaluations of ASPs are limited to short follow-up durations, predominantly employ simple pre-post designs, and rarely account for inter-departmental heterogeneity in clinical practice.7–9 More critically, evidence remains limited regarding whether ASPs are associated with changes in the temporal relationship between antimicrobial consumption and resistance.10 Exploring potential shifts in the temporal correlation between antimicrobial use density (AUD) and multidrug-resistant organism (MDRO) detection rates may provide additional observational insights into antimicrobial resistance patterns.
To address these gaps, we designed and implemented a novel, pharmacist-led ASP structured around a grid-based framework for precision management. This model stratifies clinical departments into distinct risk categories using the validated Boston Matrix—which has proven feasible for identifying high-priority departments11—with pre-intervention AUD and guideline compliance rates as two core dimensions directly linked to stewardship optimization. We hypothesized that this precision, stratified approach would be associated with optimized antimicrobial use and changes in clinical and economic indicators, while also potentially altering temporal correlations between antimicrobial consumption and MDRO detection at the institutional level.
We employed a 7.5-year interrupted time-series (ITS) analysis, a robust quasi-experimental design well-suited for evaluating sustained, policy-driven interventions in healthcare settings while controlling for underlying secular trends.12 This study evaluated intervention effects across four sequential domains: (1) antimicrobial consumption (AUD and antimicrobial use rate [AUR]); (2) department-level heterogeneity; (3) clinical safety and economic impact; and (4) ecological patterns, including observational changes in the temporal correlation between AUD and MDRO detection. This structured assessment thus aims to provide a replicable framework for large tertiary hospitals and empirical evidence to inform the refinement of national stewardship policies.
Materials and Methods
Study Design
A retrospective, single-center ITS analysis was conducted at Yichang Central People’s Hospital, a 1900-bed tertiary Grade A teaching hospital in central China. The study period spanned 90 months from January 2018 to June 2025, divided into a pre-intervention phase (January 2018–June 2020) and a post-intervention phase (July 2020–June 2025). The intervention—a hospital-wide, pharmacist-led, grid-based precision ASP—was implemented in July 2020. We included discharged inpatients who received at least one dose of systemic antibacterial or antifungal agents (therapeutic or prophylactic). Excluded were outpatients, emergency visits not resulting in hospitalization, and records with missing discharge dates.
ASP Intervention
The ASP was built upon four synergistic, interdependent pillars, with the overall workflow and risk stratification framework visualized in Figure 1.
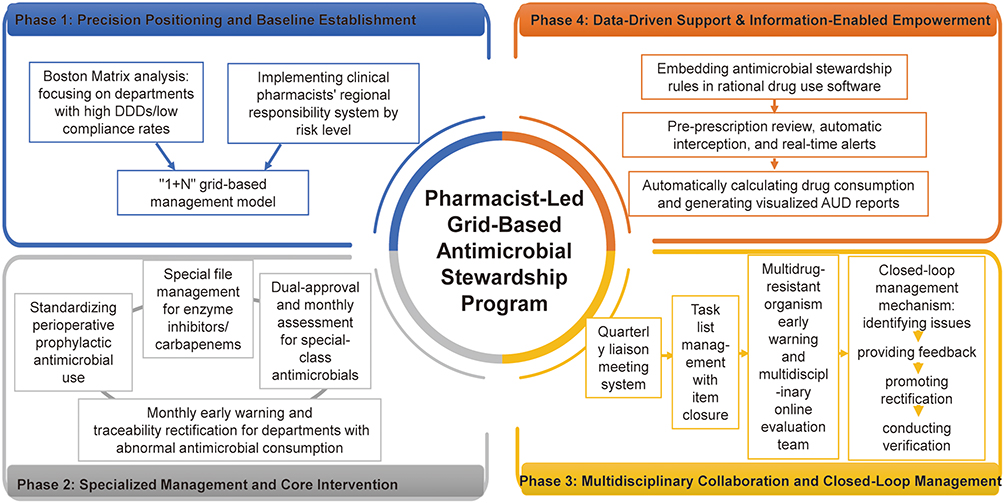 |
Figure 1 Four-Phase Implementation Framework of the Pharmacist-Led Grid-Based Antimicrobial Stewardship Program (ASP) for the 7.5-Year Interrupted Time Series (ITS) Study. |
Grid-Based Precision Management
Clinical departments (n=29) were stratified into a 2×2 matrix using two dimensions derived from 30 months of pre-intervention data: AUD (Defined Daily Doses [DDDs] per 100 patient-days [PD]) and institutional antimicrobial guideline compliance rate. High/low thresholds were defined at the 75th and 25th percentiles, respectively, creating four risk grids: High-Use/Low-Compliance (key target), High-Use/High-Compliance (optimization focus), Low-Use/Low-Compliance, and Low-Use/High-Compliance. Dedicated clinical pharmacists provided tailored education, differentiated audit intensity, and targeted feedback based on the specific profile of each risk grid.
Targeted Control of Key Antimicrobials and High-Risk Processes
Standardized, evidence-based protocols for perioperative antimicrobial prophylaxis were implemented and enforced across all surgical departments.13 For broad-spectrum and restricted agents (eg, carbapenems, enzyme-inhibitor combinations), a mandatory prospective audit-and-feedback (PAF) process with a dual-approval system (requiring authorization from both the prescribing physician and a clinical pharmacist) was instituted prior to therapy initiation, ensuring real-time review of antimicrobial indications, dosage, and duration.
Multidisciplinary Closed-Loop Feedback Cycle
A stewardship multidisciplinary team (MDT) was established, convened and chaired by a chief clinical pharmacist, with representation from medical administration, infection control, and clinical departments. The MDT met quarterly to perform three key activities: review department-level performance dashboards, analyze electronic alerts for non-compliant prescriptions, and investigate units with elevated MDRO rates. Findings were translated into action via a structured “task-list system,” which formally mandated corrective actions from respective department heads. These actions were then followed by a pharmacist-led re-audit, thereby closing the feedback loop. An MDRO early-warning mechanism was integrated into this cycle to trigger immediate MDT consultations for mitigating emerging resistance risks.
IT-Enabled Stewardship
Customized stewardship rules developed by the pharmacy team were embedded within the hospital’s computerized physician order entry (CPOE) system. This integration enabled prospective, pharmacist-led prescription review and triggered real-time alerts for non-compliant orders (eg, missing indications, excessive duration, guideline deviations). Furthermore, the system generated dynamic, visualized dashboards that displayed key metrics—including AUD, AUR, MDRO detection rates, and cost data—to support continuous quality improvement and data-driven decision making.
Data Collection
De-identified monthly aggregate data (January 2018–June 2025) were independently extracted by two investigators from the hospital’s electronic medical record and microbiology laboratory systems. To protect patient privacy, all personal identifiers were permanently de-identified, and dates were generalized to month and year. Discrepancies in data extraction were resolved by consensus between investigators, and a random 10% sample was cross-checked to validate extraction accuracy.
Collected variables included: (1) Demographic and clinical characteristics: age, sex, surgical status, length of stay (LOS), discharge status (cured, improved, died, others); (2) Antimicrobial use: agent name, formulation, quantity, and DDDs for systemic antibacterial and antifungal agents; (3) Economic indicators: per capita total hospitalization cost and antimicrobial cost (Chinese Yuan, CNY); (4) Microbiological surveillance: monthly detection rates of methicillin-resistant Staphylococcus aureus (MRSA) and carbapenem-resistant Gram-negative bacilli (CR-GNB), including Escherichia coli (CREco), Klebsiella pneumoniae (CRKP), Pseudomonas aeruginosa (CRPA), and Acinetobacter baumannii (CRAB). Susceptibility testing followed CLSI M100-S35 standards.14 Only the first non-duplicate clinical isolate per patient per hospitalization was included. Monthly MDRO detection rates were calculated as the percentage of non-duplicate targeted multidrug-resistant isolates among the total number of isolates for the same bacterial species (the complete raw datasets of all collected variables are provided in Supplementary Table S1.1–S1.5).
Outcome
Primary outcomes were AUD and AUR. AUD was calculated as (total cumulative DDDs of systemic antimicrobials / total PD) × 100, consistent with the WHO ATC/DDD index (2025 edition).15 Total PD was defined as the sum of daily inpatient counts at midnight for the month. AUR was defined as (number of discharged inpatients receiving at least one systemic antimicrobial agent / total discharged inpatients) × 100%.
Secondary outcomes included the consumption of key antimicrobial classes (fluoroquinolones, third-/fourth-generation cephalosporins, enzyme-inhibitor combinations, carbapenems); clinical outcomes (median LOS, all-cause in-hospital mortality rate); economic outcomes (per capita antimicrobial cost, proportion of total hospitalization costs attributed to antimicrobials); and monthly MDRO detection rates.
Statistical Analysis
Descriptive statistics were used to summarize participant characteristics, with continuous variables presented as median (interquartile range, IQR) and categorical variables as frequencies (percentages). Between-group comparisons were performed using the Wilcoxon rank-sum test for continuous variables and Pearson’s χ2 test or Fisher’s exact test for categorical variables.
The impact of the ASP was assessed using segmented linear regression for ITS data. The model was specified as:

where:  = outcome at month t;
= outcome at month t;  = baseline intercept;
= baseline intercept;  = pre-intervention trend;
= pre-intervention trend;  = immediate level change following intervention;
= immediate level change following intervention;  = post-intervention trend change;
= post-intervention trend change;  = monthly dummy variables for seasonal adjustment (January as the reference month);
= monthly dummy variables for seasonal adjustment (January as the reference month);  = random error term. Autocorrelation was assessed using the Durbin–Watson statistic and residual ACF/PACF plots, while heteroskedasticity was examined via the Breusch–Pagan test. Newey–West standard errors (lag order 4, selected by comparing fit across lags 1–8) were applied to address violations, with sensitivity analyses confirming robustness to alternative lags and seasonal specifications (monthly dummies vs unadjusted).16,17 Given the aggregated data structure, conventional multivariable adjustment for case-mix shifts was not feasible. We therefore compared key demographic and clinical characteristics between periods and performed a quantitative bias analysis to assess confounding related to observed differences. Model fit was assessed using R2, and standardized effect sizes were quantified with Cohen’s d (interpreted as small [< 0.5], moderate [0.5–0.8], or large [≥ 0.8]).18
= random error term. Autocorrelation was assessed using the Durbin–Watson statistic and residual ACF/PACF plots, while heteroskedasticity was examined via the Breusch–Pagan test. Newey–West standard errors (lag order 4, selected by comparing fit across lags 1–8) were applied to address violations, with sensitivity analyses confirming robustness to alternative lags and seasonal specifications (monthly dummies vs unadjusted).16,17 Given the aggregated data structure, conventional multivariable adjustment for case-mix shifts was not feasible. We therefore compared key demographic and clinical characteristics between periods and performed a quantitative bias analysis to assess confounding related to observed differences. Model fit was assessed using R2, and standardized effect sizes were quantified with Cohen’s d (interpreted as small [< 0.5], moderate [0.5–0.8], or large [≥ 0.8]).18
For exploratory department-level analysis, annual AUD values (pre- vs post-intervention) were compared using the Wilcoxon rank-sum test, reporting unadjusted P values without correction for multiple testing.
To evaluate the impact of stewardship on the ecological dynamics between antimicrobial use and MDRO detection rates, the temporal association between AUD and MDRO detection rates was assessed using simple linear regression (MDRO rate as the dependent variable and AUD as the independent variable). The primary outcome was the change in the strength of this association before and after the intervention. The optimal lag period (1–6 months) was selected via cross-correlation analysis to maximize model fit. We quantified changes in the strength of the association by calculating the percentage change in R2: [(R2 post − R2 pre) / R2 pre] × 100%. A substantial reduction in R2 reflected a change in the temporal correlation between AUD and MDRO rates, indicating a shift in the co-occurrence trends of antimicrobial consumption and resistance.
All analyses were performed using STATA/MP 17.0 (Stata Corp LLC, College Station, TX, USA). A two-tailed P value < 0.05 was considered statistically significant.
Results
Participant Characteristics
A total of 427,619 inpatient admissions were analyzed (126,356 pre-intervention; 301,263 post-intervention). The post-intervention cohort was significantly older (median age, 56 vs 53 years; P < 0.001) with a higher proportion of surgical patients (42.49% vs 36.71%; P < 0.001), reflecting increasing case complexity over time. Sex distribution was comparable between periods (P = 0.591). Key characteristics are summarized in Table 1.
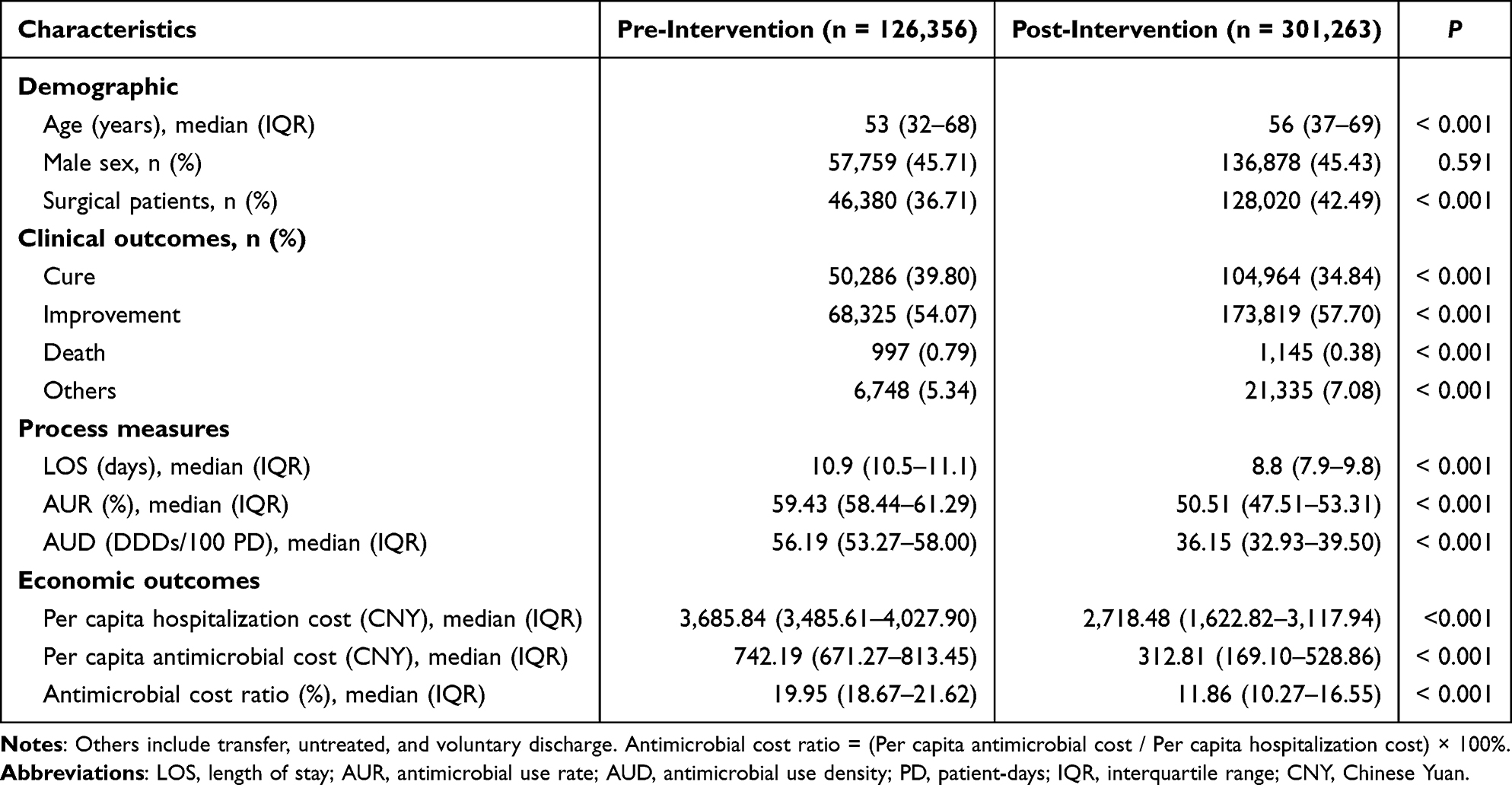 |
Table 1 Baseline Characteristics and Key Outcomes Pre- vs Post-ASP Intervention |
Hospital-Wide Antimicrobial Use
ITS analysis showed immediate and sustained reductions in antimicrobial use: AUD decreased by 25.6% (β2 = −14.55 DDDs/100 PD, P < 0.001) with no significant post-intervention trend shift, while AUR declined by 8.6% immediately (β2 = −0.052, P < 0.001) and continued to decrease (β3 = −0.003, P < 0.001). Both models, adjusted for seasonality and autocorrelation, demonstrated excellent fit (R2 = 0.81) with large effect sizes (Cohen’s d: 2.60–3.74) (Table 2 and Figure 2; see Supplementary Table S2 for model adjustment details).
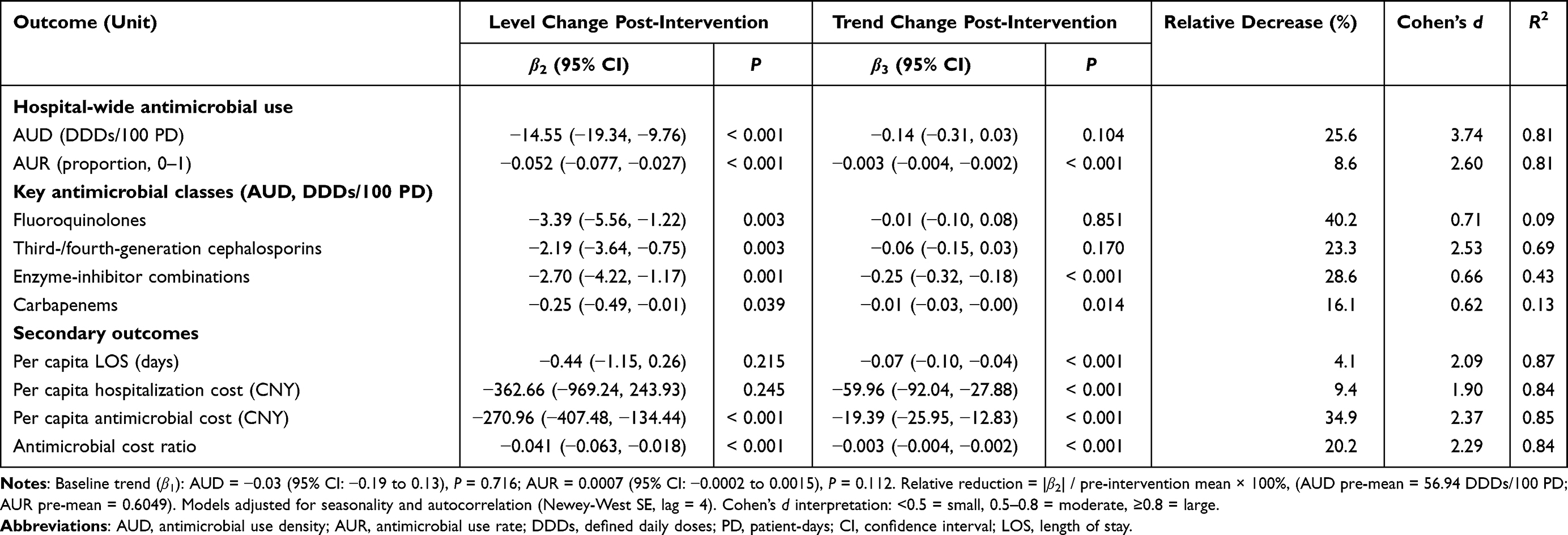 |
Table 2 Segmented Regression Analysis Results for Antimicrobial Use, Key Class, and Secondary Outcomes |
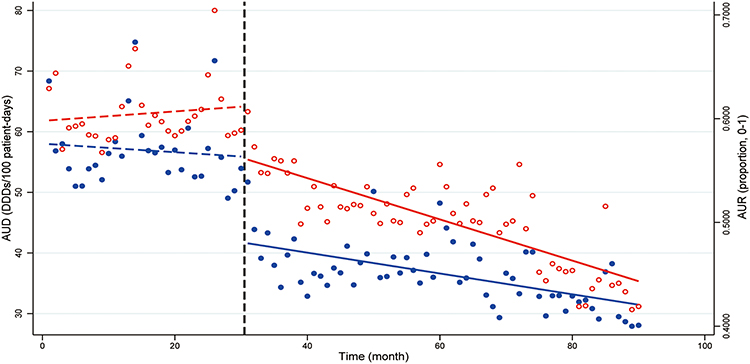 |
Figure 2 ITS Analysis of Hospital-Wide Antimicrobial Use Density (AUD) and Antimicrobial Use Rate (AUR). Blue: AUD; red: AUR. Points: monthly observed values; dashed lines: pre-intervention fitted trends; solid lines: post-intervention fitted trends. Vertical dashed line: ASP implementation (Month 30). |
Department-Level Heterogeneity
Exploratory analysis showed heterogeneous AUD changes across 29 clinical departments: 19 (65.5%) exhibited significant reductions, with the most pronounced decreases observed in Otorhinolaryngology (−72.8%), Ophthalmology (−68.6%), and Endocrinology (−48.3%). Hematology showed a non-significant reduction (−7.4%, P = 0.302). In contrast, the intensive care unit (ICU) demonstrated a significant AUD increase (+34.2%, P = 0.020), alongside its high-acuity case mix characterized by severe sepsis and multi-organ dysfunction, while Stomatology showed a non-significant upward trend (+24.0%, P = 0.302) (Table 3 and Figure 3).
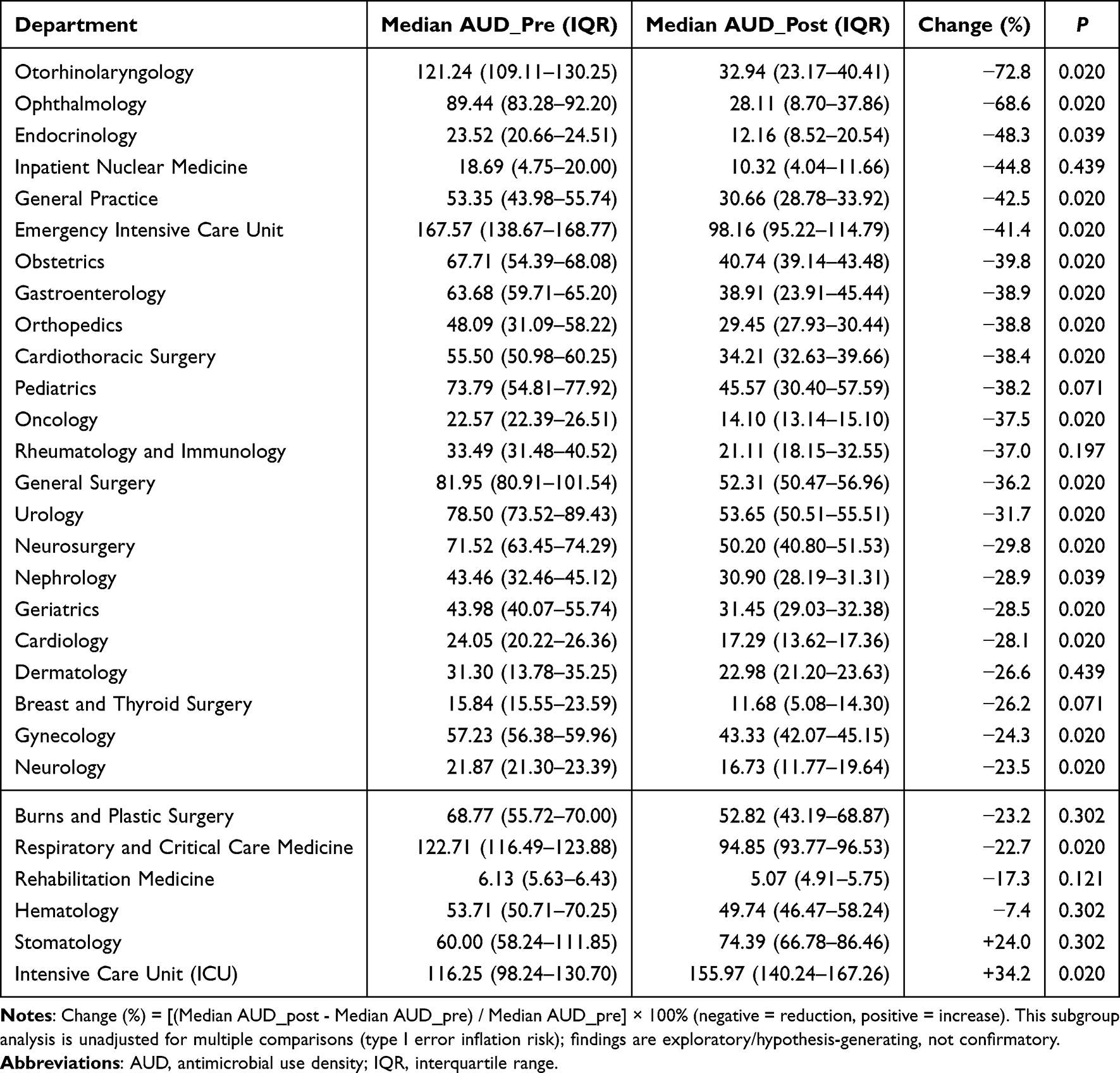 |
Table 3 Changes in Annual Antimicrobial Use Density (AUD) Across 29 Clinical Departments |
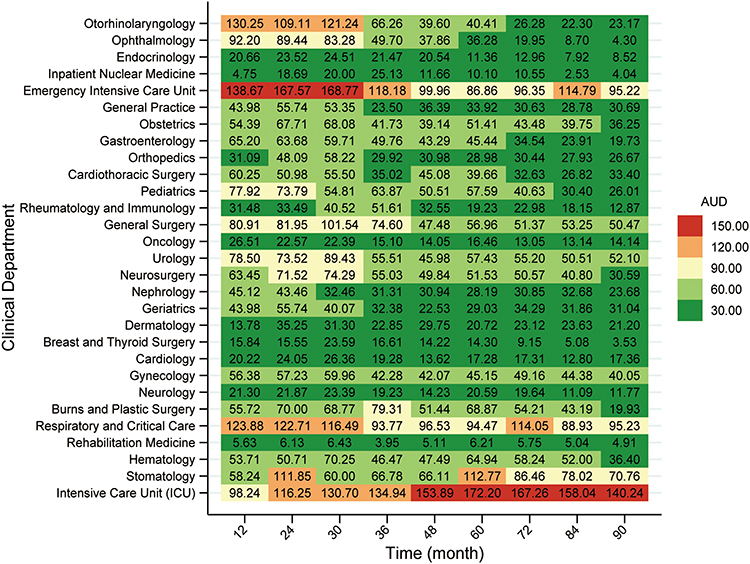 |
Figure 3 Heatmap of Heterogeneous Antimicrobial Use Density (AUD) Changes Across 29 Clinical Departments. Color gradient (blue = low AUD, red = high AUD) shows heterogeneous ASP effects. AUD unit: Defined Daily Doses (DDDs)/100 patient-days. |
Key Antibacterial Class Consumption
Significant immediate reductions were observed in the use of key antibacterial classes: fluoroquinolones (−40.2%, β2 = −3.39 DDDs/100 PD, P = 0.003), third-/fourth-generation cephalosporins (−23.3%, β2 = −2.19 DDDs/100 PD, P = 0.003), enzyme-inhibitor combinations (−28.6%, β2 = −2.70 DDDs/100 PD, P = 0.001), and carbapenems (−16.1%, β2 = −0.25 DDDs/100 PD, P = 0.039). Furthermore, enzyme-inhibitor combinations and carbapenems exhibited significant sustained downward trends in the post-intervention period (both P < 0.05) (Table 2 and Figure 4).
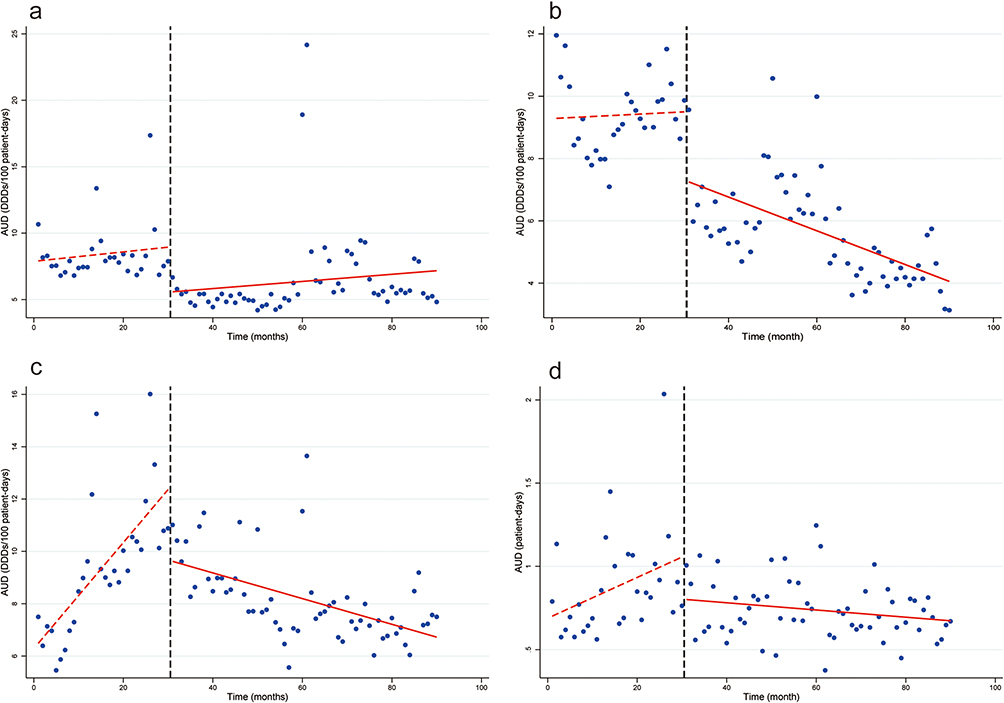 |
Figure 4 ITS Analysis of Consumption Trends for Key Antimicrobial Classes. (a) Fluoroquinolones; (b) Third-/fourth-generation cephalosporins; (c) Enzyme-inhibitor combinations; (d) Carbapenems. Points: monthly observed values; dashed lines: pre-intervention fitted trends; solid lines: post-intervention fitted trends. Vertical dashed line: ASP implementation (Month 30). |
Clinical and Economic Outcomes
Concurrent changes were observed in secondary outcomes: a sustained monthly reduction in LOS (β3 = −0.07 days/month, P < 0.001), per capita antimicrobial cost (β3 = −19.39 CNY/month, P < 0.001), and the ratio of antimicrobial cost to total hospitalization cost (β3 = −0.003/month, P < 0.001). A 52% reduction in all-cause in-hospital mortality was observed (from 0.79% to 0.38%, P < 0.001). Models for these outcomes showed high goodness-of-fit (R2 = 0.84–0.87) and moderate-to-large effect sizes (Cohen’s d = 1.90–2.37) (Table 2 and Figure 5).
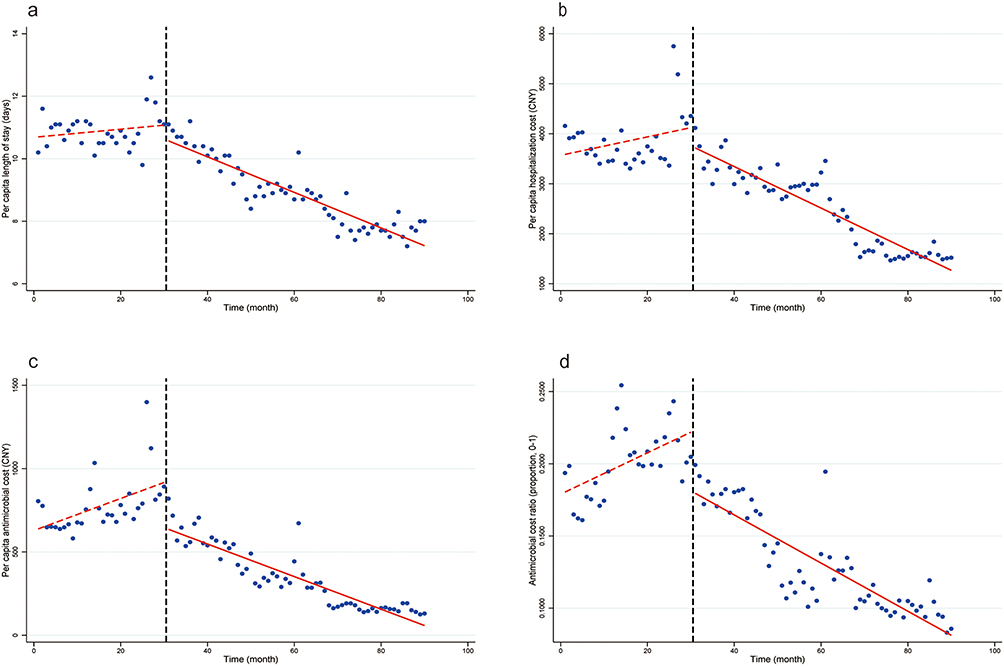 |
Figure 5 ITS Analysis of Secondary Clinical and Economic Outcomes. (a) Length of stay; (b) Total hospitalization cost; (c) Per capita antimicrobial cost; (d) Antimicrobial cost ratio (0–1). Points: monthly observed values; dashed lines: pre-intervention fitted trends; solid lines: post-intervention fitted trends. Vertical dashed line: ASP implementation (Month 30). |
MDRO Detection and AUD-MDRO Association
The explanatory power of AUD on MDRO detection rates was markedly reduced in the post-intervention period. Linear regression analysis revealed altered temporal correlations across key pathogens: MRSA, CREco, and CRAB showed the most pronounced reduction in R2 (a 71.8–87.0% decrease), reflecting that AUD explained much less of the variance in detection rates post-intervention. CRKP showed a moderate reduction in association strength (49.8% decrease in R2). In contrast, the association for CRPA paradoxically strengthened (+78.3% change in R2), with an observed shift in temporal correlation despite stable detection rates. Concurrently, crude monthly detection rates decreased significantly for MRSA (P = 0.016) and CRAB (P = 0.008), while no significant changes were observed for CREco (P = 0.127), CRKP (P = 0.800), and CRPA (P = 0.273) (Table 4 and Figure 6).
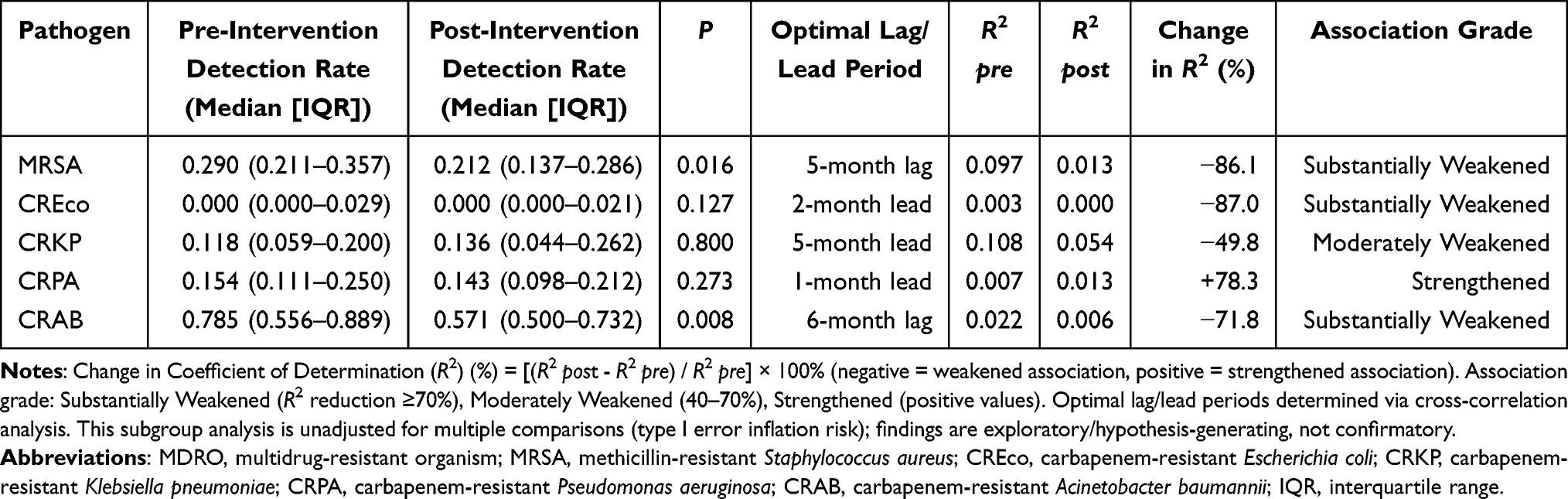 |
Table 4 MDRO Detection Rates and Temporal Association with Antimicrobial Use Density (AUD) |
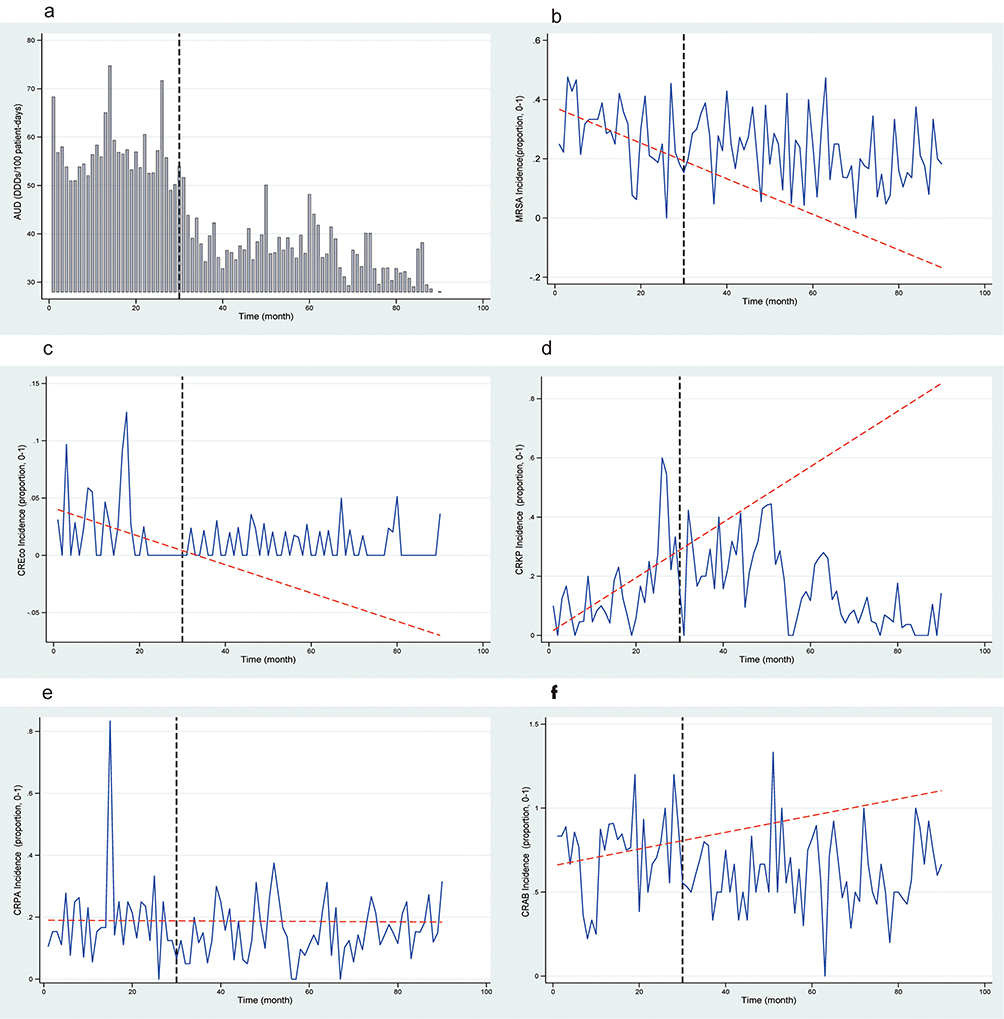 |
Figure 6 Temporal Association between Antimicrobial Use Density (AUD) and Multidrug-Resistant Organism (MDRO) Detection Rates. (a) AUD; (b) Methicillin-resistant Staphylococcus aureus (MRSA); (c) Carbapenem-resistant Escherichia coli (CREco); (d) Carbapenem-resistant Klebsiella pneumoniae (CRKP); (e) Carbapenem-resistant Pseudomonas aeruginosa (CRPA); (f) Carbapenem-resistant Acinetobacter baumannii (CRAB). Blue lines: monthly observed values; red lines: counterfactual trends (expected values without ASP intervention). Vertical dashed line: ASP implementation (Month 30). |
Discussion
This 7.5-year ITS analysis reveals that a pharmacist-led, grid-based precision ASP was associated with sustained reductions in antimicrobial use and an altered temporal association between antimicrobial consumption and MDRO detection rates. Four key findings emerged: (1) sustained reductions in antimicrobial use were observed despite increasing patient complexity; (2) substantial department-level heterogeneity was noted, consistent with adaptive, targeted stewardship; (3) parallel changes in clinical and economic outcomes were identified; and (4) the temporal association between AUD and MDRO detection rates was markedly altered. These findings address key gaps in the long-term observational evaluation of hospital-based antimicrobial stewardship programs.
Our key contribution lies in the empirical observation of a shift in temporal association patterns between antimicrobial consumption and MDRO detection rates. Unlike most ASP studies, which only report declines in antimicrobial use or MDRO prevalence and fail to address the dynamic temporal relationship between antimicrobial consumption and MDRO detection rates—the core relationship that ASPs seek to influence—our analysis reveals a notable change in this long-term relationship.10 For example, Xia et al reported optimized pre-therapy pathogen identification and corresponding CRKP declines but observed no consistent correlation shifts for other MDROs.19 Similarly, Zhang et al documented a 15.2% AUD reduction over 3 years in a Chinese hospital but did not quantify such ecological associations.20 In contrast, our grid-based ASP was associated with a marked reduction in R2 (explanatory power) for MRSA, CREco, and CRAB (71.8–87.0%), suggesting that antimicrobial use became less predictive of MDRO detection trends. These findings highlight that precision stewardship can mitigate inappropriate antimicrobial exposure rather than promote indiscriminate antimicrobial restriction—a critical distinction rarely quantified in long-term ASP evaluations.12,21,22
In comparison with international experiences, the present intervention documents sustained trends over an extended follow-up period. Ford et al achieved 24–47% azithromycin reduction via clinical decision support, but only for a single drug class and over a short follow-up.21 Sangiorgi et al reported 11% inappropriate carbapenem reduction in Italy, but without departmental stratification—resulting in uneven effectiveness across care areas.22 By contrast, our 7.5-year intervention was associated with sustained reductions across multiple high-priority antimicrobial classes (fluoroquinolones: −40.2%; carbapenems: −16.1%) while accounting for departmental heterogeneity. The 34.2% increase in ICU AUD—rather than indicating an undesired outcome—reflects the adaptive, tailored design of the intervention: in this high-acuity setting (characterized by severe sepsis and multi-organ dysfunction), antimicrobial use was guided by clinical appropriateness rather than blanket restriction, illustrating a “precision over restriction” approach23 and addressing known limitations of uniform restriction strategies.24 This pattern of heterogeneous response—reductions in low-acuity departments and appropriateness-driven adjustments in the ICU—supports the potential value of grid-based stratification in supporting sustainable program implementation.
Moving beyond one-size-fits-all strategies enables more efficient and targeted resource allocation. Substantial reductions in lower-complexity, high-use departments—Otorhinolaryngology (−72.8%) and Ophthalmology (−68.6%)—paired with appropriateness-focused ICU management, illustrate the value of tailored stewardship. Such heterogeneity, often masked in hospital-wide aggregate analyses, is critical to sustaining frontline clinician engagement and long-term compliance. Targeted interventions for “High-Use/Low-Compliance” departments (eg, General Surgery), including monthly pharmacist-led education and real-time prescription auditing, contributed to a 36.2% AUD reduction—further validating the practical utility of grid-based stratification.
The program’s four-pillar synergistic design—supported by a modest resource investment (≈ 1 full-time equivalent pharmacist per 100–300 beds),25 consistent with international sustainable ASP staffing benchmarks—was key to its sustained performance. Mandatory prospective audit and dual approval for restricted antimicrobials balanced consumption reduction with continued appropriate access for high-risk patients26—an approach more durable than rigid restriction alone.24 The pharmacist-chaired multidisciplinary team and closed-loop feedback mechanism drove a 23.3% sustained reduction in third-/fourth-generation cephalosporin use (β2 = −2.19 DDDs/100 PD; 95% CI: −3.64 to −0.75; P = 0.003; Table 2 and Figure 4). Embedding stewardship rules into the CPOE system enabled scalable real-time decision support and dynamic performance dashboards,27 curbing non-compliant prescribing. This multifaceted integrated approach likely explains five years of durable post-implementation effectiveness, with large effect sizes (Cohen’s d = 1.90–3.74) that compare favorably with other long-term ITS evaluations,21,22,28 and these findings were corroborated by sensitivity analyses (Supplementary Table S2).
The paradoxical 78.3% strengthening of the AUD–CRPA association—despite stable crude detection rates—may arise from three interrelated mechanisms. First, PA has an intrinsic resistance profile, including efflux pump overexpression and OprD porin deficiency, which reduces its responsiveness to volume-focused stewardship.29,30 Second, shifts in pathogen distribution may have occurred: the significant reduction in CRAB (P = 0.008) likely opened a niche favorable to CRPA expansion.31 Of note, CRPA isolates were concentrated in respiratory and neurosurgical ICUs, where continued appropriate broad-spectrum antipseudomonal use may have altered local microbial dynamics. Third, the environmental persistence of CRPA and prolonged antipseudomonal courses for ventilator-associated pneumonia can inadvertently support ongoing transmission. These observations highlight important limitations of antimicrobial stewardship alone: pathogen-specific strategies and enhanced infection control—including rigorous environmental disinfection and contact precautions—are necessary to control persistent environmental pathogens such as CRPA.32
This study has several limitations. First, as an ecological time-series analysis, we cannot establish individual-level causality or adjust for patient-specific confounders such as disease severity. However, the increased proportion of surgical patients after intervention represents a negative confounder that biases results toward the null, suggesting our findings are conservative. Second, the linear ITS model cannot fully capture the complex non-linear biological dynamics of antimicrobial resistance evolution, though our results still provide valuable population-level observational trends. Third, subgroup and pathogen-specific analyses were not adjusted for multiple comparisons, which may inflate type I error; these findings should therefore be interpreted as exploratory and hypothesis-generating rather than confirmatory. Finally, the single-center, retrospective design limits generalizability, although the 7.5-year duration and ICU’s divergent trend help reduce bias from secular trends.
This grid-based precision ASP may offer preliminary policy and clinical translational insights. Observations from this single-center program suggest potential alignment with tertiary hospital quality improvement initiatives and DRG-based payment reform, as the intervention was associated with reduced unnecessary antimicrobial consumption and improved key quality metrics.7,33 For tertiary care settings, this framework may warrant further evaluation for potential scalability, given its relatively modest resource requirements, compatibility with existing CPOE systems, and adaptability to local antimicrobial prescribing guidelines.
Three priorities for future research emerge: (1) to conduct the planned multi-center stepped-wedge randomized controlled trial (RCT) to evaluate generalizability across diverse healthcare settings;34 (2) to implement AI-powered real-time decision support in high-risk units, integrating machine learning models to predict CRPA risk and personalize antipseudomonal therapy;35 and (3) to use whole-genome sequencing to clarify whether the altered AUD—CRPA association reflects evolutionary adaptation, unmeasured confounding, or differential transmission dynamics.36 For future translational research, we will develop a DRG-aligned pharmacoeconomic framework and implement targeted infection control bundles for high-priority MDROs such as CRPA.
Conclusion
This pharmacist-led, grid-based precision ASP was associated with sustained reductions in antimicrobial consumption, concurrent shifts in clinical and economic indicators, and altered temporal correlations between antimicrobial use and MDRO detection at a single tertiary hospital. These observational findings reflect parallel resistance trends alongside decreased antimicrobial consumption, without implying causal ecological relationships. This integrated, data-driven stewardship model merits further evaluation for scalability and may inform local and national antimicrobial stewardship strategies targeting antimicrobial resistance and rational prescribing.
AI-Assisted Statement
Limited AI-assisted language editing and grammatical refinement were performed using Doubao solely to improve manuscript readability. No artificial intelligence tools were used for study design, data analysis, result interpretation, or core manuscript writing. All authors retain full responsibility for the final content and conclusions of this study.
Data Sharing Statement
The complete primary raw datasets supporting the conclusions of this study are available as Supplementary Table S1 with this manuscript, and supplementary materials for ITS model adjustment and robustness tests are provided in Supplementary Table S2.
Ethics Approval and Informed Consent
The study was approved by the Medical Ethics Committee of Yichang Central People’s Hospital (Approval No. 2026-021-01). Informed consent was waived due to the retrospective nature of the study and use of fully anonymized, aggregated data. All procedures were conducted in accordance with the ethical standards outlined in the Declaration of Helsinki, with strict patient data confidentiality maintained.
Consent for Publication
The study used fully anonymized, aggregated data with all personal identifiers permanently removed. Informed consent for publication was waived by the Medical Ethics Committee of Yichang Central People’s Hospital, consistent with the study’s ethical approval.
Acknowledgments
The authors thank the clinical pharmacists, physicians, and nursing staff at Yichang Central People’s Hospital for their commitment to antimicrobial stewardship. We also thank Dr. H. Ruan (Department of Critical Care Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China) for valuable comments and statistical guidance during manuscript preparation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no competing interests.
References
1. GBD 2021 Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. Lancet. 2024;404(10459):1199–15. doi:10.1016/S0140-6736(24)01867-1
2. O’Neill J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. London: Review on Antimicrobial Resistance; 2016.
3. Zhao H, Wei L, Li H, et al. Appropriateness of antibiotic prescriptions in ambulatory care in China: a nationwide descriptive database study. Lancet Infect Dis. 2021;21(6):847–857. doi:10.1016/S1473-3099(20)30596-X
4. Song H, Liu X, Zou K, et al. Assessment of antibiotic consumption patterns in hospital and primary healthcare using WHO Access, Watch and Reserve classification (AWaRe) in Sichuan Western China: 2020. Arch Public Health. 2024;82(1):182. doi:10.1186/s13690-024-01391-5
5. Yang D, Dyar OJ, Yin J, Ma W, Sun Q, Lundborg CS. Antimicrobial resistance in China across human, animal, and environment sectors–a review of policy documents using a governance framework. Lancet Reg Health West Pac. 2024;48:101111. doi:10.1016/j.lanwpc.2024.101111
6. Wenhao L. Role of clinical pharmacists in antimicrobial stewardship programs: a multicenter study. J Appl Pharm. 2025;17:468. doi:10.35248/1920-4159.25.17.468
7. Yu J, Liu Y, Qu R, et al. Evaluation of a clinical pharmacist-led antimicrobial stewardship program in a neurosurgical intensive care unit: a pre-and post-intervention cohort study. Front Pharmacol. 2023;14:1263618. doi:10.3389/fphar.2023.1263618
8. Kuijpers SME, de la Court JR, Prins JM, Schade RP, Heijmans J, Sigaloff KCE. Impact of an antimicrobial stewardship bundle on the outcome of high-risk neutropenic patients with fever: a pre-post study. JAC Antimicrob Resist. 2025;7(5):dlaf191. doi:10.1093/jacamr/dlaf191
9. Son H-J, Bae S, Cho K, et al. Impact of carbapenem-targeted antimicrobial stewardship interventions: an interrupted time-series analysis. J Hosp Infect. 2023;140:132–138. doi:10.1016/j.jhin.2023.07.019
10. Laffont-Lozes P, Larcher R, Salipante F, et al. Usefulness of dynamic regression time series models for studying the relationship between antimicrobial consumption and bacterial antimicrobial resistance in hospitals: a systematic review. Antimicrob Resist Infect Control. 2023;12(1):100. doi:10.1186/s13756-023-01302-3
11. Shu L, Luo ZD, He MC, Wang S. Antimicrobial drug use and changing trends from 2021 to 2023—a case study of a general hospital in Sichuan Province. J Eval Clin Pract. 2025;31(1):e14306. doi:10.1111/jep.14306
12. Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. 2017;46(1):348–355. doi:10.1093/ije/dyw098
13. National Health Commission of the People’s Republic of China. Guiding Principles for Clinical Application of Antimicrobials (2015 Edition). Beijing: People’s Medical Publishing House; 2015.
14. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing.
15. World Health Organization Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2025 [Internet]. Oslo: WHOCC; 2025. Available from: https://atcddd.fhi.no/atc_ddd_index/.
16. Newey WK, West KD. A simple, positive semi-definite, heteroskedasticity and autocorrelation consistent covariance matrix. Econometrica. 1987;55:703–708.
17. Newey WK, West KD. Automatic lag selection in covariance matrix estimation. Rev Econ Stud. 1994;61:631–653.
18. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
19. Xia S, Jiang Q, Liu Y, et al. Impact of an antimicrobial stewardship program on pre-therapy pathogen detection specimen submission, antimicrobial use, and resistant pathogens: an interrupted time series analysis. Infect Drug Resist. 2025;18:6561–6575. doi:10.2147/IDR.S561879
20. Zhang X, Zhou L, Peng P, Zhang W, Liang C. Role of antimicrobial stewardship in modulating antibiotic use and mitigating bacterial resistance in a tertiary care setting during COVID-19. Infect Drug Resist. 2025;18:1647–1656. doi:10.2147/IDR.S500379
21. Ford JS, Morgan Bustamante BL, Virk MK, et al. Use of clinical decision support for antibiotic stewardship in the emergency department and outpatient clinics: an interrupted time-series analysis. Antimicrob Steward Healthc Epidemiol. 2023;3:e80. doi:10.1017/ash.2023.140
22. Sangiorgi F, Del Vecchio P, Magrini E, et al. Impact of a post-prescription audit and feedback antimicrobial stewardship intervention on inappropriate carbapenem prescribing: an interrupted time series analysis. JAC Antimicrob Resist. 2025;7(6):dlaf236. doi:10.1093/jacamr/dlaf236
23. Pickens CI, Wunderink RG. Principles and practice of antibiotic stewardship in the ICU. Chest. 2019;156:163–171. doi:10.1016/j.chest.2019.01.013
24. López-Viñau T, Peñalva G, García-Martínez L, et al. Impact of an antimicrobial stewardship program on the incidence of carbapenem resistant gram-negative bacilli: an interrupted time-series analysis. Antibiotics. 2021;10:586. doi:10.3390/antibiotics10050586
25. Nelson GE, Narayanan N, Onguti S, Stanley K, Newland JG, Doernberg SB. Principles and practice of antimicrobial stewardship program resource allocation. Infect Dis Clin North Am. 2023;37:683–714. doi:10.1016/j.idc.2023.07.002
26. Ronda M, Padullés A, Grau I, et al. Impact of a prospective audit and feedback antimicrobial stewardship programme on carbapenem consumption: a quasi-experimental study (IPANEMA study). J Antimicrob Chemother. 2023;78:1705–1710. doi:10.1093/jac/dkad160
27. Fortier M, Pistre P, Ferreira V, et al. Impact of a checklist used by pharmacists on hospital antimicrobial use: a patient-level interrupted time series study. J Hosp Infect. 2019;103:251–258. doi:10.1016/j.jhin.2019.06.009
28. Lee LW, Lim SYC, Zhou YP, et al. Impact of the ABxSG mobile application on antibiotic prescribing: an interrupted time series study. Antibiotics. 2025;14(9):933. doi:10.3390/antibiotics14090933
29. Lorusso AB, Carrara JA, Barroso CDN, Tuon FF, Faoro H. Role of efflux pumps on antimicrobial resistance in Pseudomonas aeruginosa. Int J Mol Sci. 2022;23:15779. doi:10.3390/ijms232415779
30. Wang M, Zhang Y, Pei F, Liu Y, Zheng Y. Loss of OprD function is sufficient for carbapenem-resistance-only but insufficient for multidrug resistance in Pseudomonas aeruginosa. BMC Microbiol. 2025;25(1):218. doi:10.1186/s12866-025-03935-3
31. Banerji A, Jahne M, Herrmann M, Brinkman N, Keely S. Bringing community ecology to bear on the issue of antimicrobial resistance. Front Microbiol. 2019;10:2626. doi:10.3389/fmicb.2019.02626
32. Męcik M, Stefaniak K, Harnisz M, Korzeniewska E. Hospital and municipal wastewater as a source of carbapenem-resistant Acinetobacter baumannii and Pseudomonas aeruginosa in the environment: a review. Environ Sci Pollut Res Int. 2024;31(36):48813–48838. doi:10.1007/s11356-024-34436-x
33. Zheng N, Li J, Liu Y, et al. Evaluation of implementation and effectiveness of China’s antibiotic stewardship in the First Affiliated Hospital of Sun Yat-sen University. Antibiotics. 2023;12(4):770. doi:10.3390/antibiotics12040770
34. Kennedy-Shaffer L, de Gruttola V, Lipsitch M. Novel methods for the analysis of stepped wedge cluster randomized trials. Stat Med. 2020;39(7):815–844. doi:10.1002/sim.8451
35. Jiang Y, Wang HW, Tian FY, Guo Y, Wang XM. Predicting carbapenem-resistant Pseudomonas aeruginosa infection risk using XGBoost model and explainability. Sci Rep. 2025;15(1):19737. doi:10.1038/s41598-025-04028-x
36. Guo Y, Hao Y, Huang M, et al. Whole-genome sequencing reveals resistance mechanisms and molecular epidemiology of carbapenem-resistant Pseudomonas aeruginosa bloodstream infections. BMC Microbiol. 2025;25(1):679. doi:10.1186/s12866-025-04293-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.