Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Immunomodulators for Non-Melanoma Skin Cancers: Updated Perspectives
Authors Russomanno K ![]() , Abdel Azim S
, Abdel Azim S ![]() , Patel VA
, Patel VA
Received 8 December 2022
Accepted for publication 20 March 2023
Published 18 April 2023 Volume 2023:16 Pages 1025—1045
DOI https://doi.org/10.2147/CCID.S362171
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Kristen Russomanno,1 Sara Abdel Azim,2 Vishal A Patel3
1Department of Dermatology, Medstar Georgetown University Hospital/Medstar Medical Group, Washington, DC, USA; 2School of Medicine, Georgetown University, Washington, DC, USA; 3Department of Dermatology, George Washington University, Washington, DC, USA
Correspondence: Vishal A Patel, Department of Dermatology, George Washington University, 2150 Pennsylvania Avenue NW, 2nd Floor, Washington, DC, 20037, USA, Tel +1 202 741 2600, Email [email protected]
Abstract: Non-melanoma skin cancers (NMSCs) are the most common cancers worldwide and may be associated with significant morbidity and mortality, especially in immunosuppressed populations. Successful management of NMSC must take primary, secondary and tertiary prevention strategies into consideration. In response to an improved understanding of the pathophysiology of NMSC and associated risk factors, multiple systemic and topical immunomodulatory drugs have been developed and integrated into clinical practice. Many of these drugs are efficacious in the prevention and treatment of precursor lesions (actinic keratoses; AKs), low-risk NMSC, and advanced disease. The identification of patients at high risk for the development of NMSC is critical in reducing disease morbidity. Understanding the various treatment options available and their comparative effectiveness is paramount for developing a personalized treatment regimen for such patients. This review article provides an updated overview of the various topical and systemic immunomodulatory drugs available for the prevention and treatment of NMSC, and the published data supporting their use in clinical practice.
Keywords: non-melanoma skin cancer, squamous cell carcinoma, basal cell carcinoma, keratinocyte carcinoma
Introduction
Non-melanoma skin cancers (NMSCs) are the most common cancers worldwide. In the United States (US), the incidence of basal cell carcinoma (BCC) is greater than 2 times that of cutaneous squamous cell carcinoma (cSCC), exceeding the incidence of all other malignancies combined.1 The primary risk factor contributing to the development of NMSC development is chronic exposure to ultraviolet (UV) radiation. UV light leads to direct deoxyribonucleic acid (DNA) damage, free radical production, and cutaneous immunosuppression by way of modifying and suppressing the localized innate and adaptive cytokine profile and cellular surveillance.2 Other risk factors including advanced age, Fitzpatrick skin type I–II, history of ionizing radiation, certain genetic diseases and systemic immunosuppression may also contribute to the development of NMSC. Among the immunosuppressed, the subsets of populations most vulnerable to the development of NMSC include solid organ transplant recipients (SOTRs), patients with hematologic malignancies, and those with other immunosuppressive conditions such as human immunodeficiency virus (HIV). The risk of developing cSCC and BCC in the SOTR population is estimated to be 40–250 and 5–10 times higher than the general population, respectively.3,4 Patients with chronic lymphocytic leukemia (CLL) are 1.86–8.6 times more likely to develop cSCC than the general population.5 The risk of cSCC metastasis in the general population is approximately 4%, but among SOTRs and certain immunosuppressed individuals, the risk may be 2–3 times greater.6,7 In fact, metastatic skin cancer is one of the leading causes of mortality in SOTRs.8 Given the significant morbidity and mortality associated with NMSC in at-risk populations, multi-faceted prevention and treatment approaches are critical.
Destructive and surgical approaches are generally the first-line treatment options for low-risk cSCC and BCC. These include cryosurgery, electrodessication and curettage, and standard surgical excision. Complete margin analysis surgery, such as Mohs micrographic surgery, is generally reserved and preferred for high-risk cSCC and BCC. Treatment selection depends on host risk factors, clinical and histologic features, and anatomic location of the malignancy. Advanced or metastatic disease may not be amenable to surgical and/or destructive therapies, and systemic therapy may be necessary. Aside from the many treatment options for confirmed disease, primary and secondary prevention strategies aimed at reducing overall disease burden are similarly important. This review article will discuss in detail the various immunomodulatory treatment options and the current evidence supporting their use in both the prevention and treatment of NMSC. The safety and efficacy of systemic and topical retinoids, nicotinamide, capecitabine, systemic and topical non-steroidal anti-inflammatories (NSAIDs), mammalian target of rapamycin (mTOR) inhibitors, checkpoint inhibitors, topical 5-fluorouracil (5-FU), topical imiquimod (IMI), topical ingenol mebutate (IMB), and photodynamic therapy (PDT) will be discussed in detail.
Systemic Immunomodulators
Oral Retinoids
Retinoids are natural or synthetic small molecule hormones that mimic the biologic activity of vitamin A, activating nuclear receptors and regulating gene transcription. This ultimately affects the expression of proteins involved in cell growth and regulation.3,9 In addition to their anti-inflammatory and anti-proliferative effects, retinoids have demonstrated immunomodulatory and anti-inflammatory benefits by way of stimulating T cell mediated cytotoxic effects, inhibiting the accumulation of leukocytes in the stratum corneum and inhibiting blastogenesis of lymphocytes.10 Cells infected with human papillomavirus are 10–100 times more sensitive to retinoic acid growth inhibition than uninfected keratinocytes, which may serve as an explanation for the modulation of NMSC development, particularly cSCC.11,12 Retinoids have been studied most extensively in the SOTR population as chemoprophylaxis against keratinocyte carcinomas, but they may also be useful in other high-risk populations.
A double-blind, randomized controlled trial (RCT) published in 1995 by Bavinck et al demonstrated that the administration of acitretin to renal transplant patients at a dose of 30 mg/day for 6 months resulted in a 36% risk reduction in the development of cSCC when compared to placebo.13 A more recent 2002 open-label, randomized crossover trial of renal transplant patients receiving between 25 and 50 mg/day of acitretin demonstrated a statistically significant reduction in cSCC incidence compared to those in the drug-free interval.14 Patients evaluated in this study had either >3 cSCCs or BCCs within the previous 5 years or ≥ 10 or more AKs. Thirty-nine percent of patients withdrew due to side effects including rash, nausea, headache, epistaxis, and elevated serum cholesterol levels.
Many other case series and retrospective studies have reproduced a significant risk reduction in the development of cSCC with the administration of systemic retinoids. A recent systematic literature review published in 2021 by Badri et al reported an overall 54% risk reduction in the annual development of cSCC and a 73% risk reduction in the development of BCC across relevant studies examining the use of acitretin for chemoprophylaxis in renal transplant recipients.15 Some studies report a higher efficacy of acitretin in the prevention of cSCC compared to BCC,14 however a recent RCT investigating 70 non-SOTRs receiving acitretin 25 mg orally 5 days per week suggested a similar efficacy in the prevention of both NMSCs.16
Acitretin is preferred over etretinate, which is no longer available for use in the US due to associated toxicities. Isotretinoin may have some chemopreventive benefit in NMSC, although results from studies are conflicting. A 3-year controlled, prospective study from 1988 demonstrated a statistically significant 63% reduction in skin cancer incidence in patients with xeroderma pigmentosum treated with a high dose (2 mg/kg/day) of isotretinoin compared to a two-year drug-free interval prior to the intervention.17 Protective effects waned within 3 months after treatment withdrawal. One case report from 1996 showed a 50% reduction in NMSC within 2 months with the use of isotretinoin 0.5–1 mg/kg per day in a renal transplant patient,18 however RCTs have failed to show consistent reproducible results.19 Notably, an RCT of 525 patients with ≥ 4 cSCCs or BCCs did not show any statistically significant correlation between 5 and 10 mg/day of isotretinoin or 25,000 units/day of retinol administration and NMSC incidence, though it has been suggested that the low doses administered in this study may have contributed to the lack of effectiveness.20
The current 2.2022 version of the National Comprehensive Cancer Network (NCCN) guidelines for the management of cSCC notes that acitretin and isotretinoin have proven effective in the prevention of both AKs and cSCC in high-risk patients. The guidelines for the management of BCC also note that acitretin might be effective for prevention in high-risk patients.16,21 (Table 1) Common side effects of oral retinoids including hepatotoxicity, teratogenicity, xerosis cutis, and lipid abnormalities may limit clinical use, and therapeutic effects have been shown to diminish within months after discontinuation. Although there are few specific guidelines regarding patient selection and dosing regimens, some experts consider starting oral retinoids in patients who develop ≥ 5 cSCC of any stage over 2–3 years, 1 Brigham and Women’s Hospital (BWH) T2b/T3 cSCC in the setting of diffuse UV damage, or field cancerization responding sub-optimally to PDT or 5-FU.22 The NCCN guidelines for the management of BCC are less specific, however do suggest that individuals at high risk of developing NMSC may benefit from acitretin administration.21
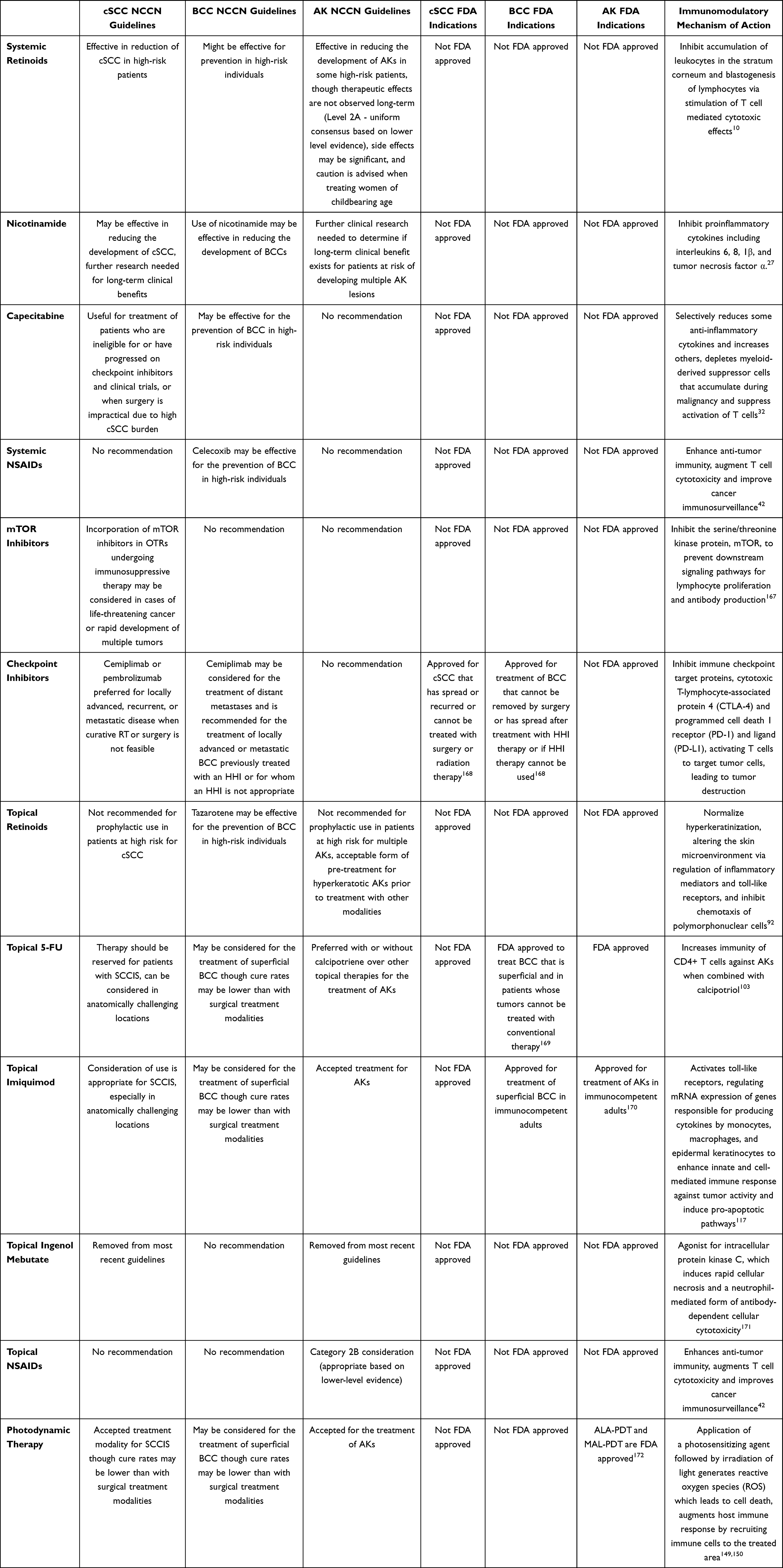 |
Table 1 Immunomodulatory Drug Regulations, FDA Approvals, and Mechanism of Action for Treatment of NMSC |
Nicotinamide
Nicotinamide is a water-soluble amide form of niacin (vitamin B3) and is essential in the production of ATP by way of nicotinamide adenine dinucleotide. Nicotinamide prevents UV radiation induced cellular ATP depletion and reduces UV associated suppression of antitumor immunity, thereby counteracting UV-induced carcinogenesis and the development of NMSC.23–26 Nicotinamide has shown potent in vitro immunomodulatory effects by inhibiting proinflammatory cytokines including interleukins 6, 8, 1β, and tumor necrosis factor α.27 Although the mechanisms are not fully understood, it is thought that nicotinamide exerts a chemoprotective benefit and reduces the immunosuppressive effect of sunlight by modulating DNA repair, regulating apoptosis, and up-regulating immune function-related genes that are typically down-regulated by UV irradiation.28,29
A recent Phase 3 double-blind, randomized, placebo-controlled trial published in 2015 demonstrated a 23% relative rate reduction in the development of new NMSCs when study participants were administered 500 mg of nicotinamide twice daily over a 12-month period when compared to placebo.24 Participants selected for this study were immunocompetent individuals 18 years of age or older, with ≥ 2 histologically confirmed NMSCs in the previous 5 years. Of note, this effect was not maintained by 6 months after drug discontinuation. The study also demonstrated a statistically significant reduction in the development of new AKs (11%), which plateaued after 9 months of treatment, consistent with findings in prior studies. A Phase 2 RCT investigating nicotinamide for chemoprophylaxis in 22 renal transplant recipients with ≥ 2 histologically confirmed NMSCs in the previous 12 months showed a 35% relative difference in the rate of NMSC and 16% reduction in AKs. These results were not statistically significant, possibly owing to a small sample size. Further trials investigating the utility of nicotinamide in SOTRs are underway.25,30
Nicotinamide is generally well tolerated with few side effects at the recommended dosage; however, the therapeutic effects have been shown to wane shortly following cessation. The current NCCN guidelines for the management of cSCC do not give clear specifications on the selection of patients and use of nicotinamide, but there is mention that it may be effective in reducing the development of cSCC.1 Some experts currently recommend nicotinamide to patients who have had >1 cSCC or who display field cancerization.22 The NCCN guidelines for the management of BCC suggest that the use of nicotinamide may be effective, citing data from Chen et al21,24,25 (Table 1) Although the benefits appear to be positive, long-term data is needed to characterize the utility of nicotinamide more fully in at-risk populations.
Capecitabine
Capecitabine is a prodrug of 5′-deoxy-5-fluorouridine, which is ultimately converted to its active metabolite 5-FU by the liver, which subsequently inhibits thymidylate synthase.31 Capecitabine has been shown to selectively reduce inflammatory cytokines, while simultaneously increasing anti-inflammatory cytokines. It has also been hypothesized that fluorouracil, a metabolite of 5-FU, depletes myeloid-derived suppressor cells, which accumulate during the progression of a malignancy and suppress activation of T cells.32
Capecitabine has shown efficacy in the treatment of advanced cSCC in non-SOTRs when used in combination with subcutaneous interferon alpha.33 The drug is most commonly used in its currently approved indications for the treatment of breast and colon malignancies. In patients previously treated with capecitabine for various solid tumor malignancies, inflammation, followed by resolution of AKs occurred incidentally, leading to studies investigating its efficacy in the treatment and prevention of NMSC.34,35
A retrospective, case-observational study published in 2010 investigating the efficacy of oral low dose capecitabine as chemoprophylaxis in 15 SOTRs showed significant reduction in both pre-cancerous lesions and NMSCs. In this study, 1 gm/m2/day of capecitabine was administered to patients with ≥ 2 NMSCs within the prior 6 months or ≥ 10 new AKs requiring treatment within 12 months. The drug was given in two daily doses on days 1–14 of a 21-day cycle, resulting in an individual incidence reduction of cSCC ranging from 56% to 100%. Over half of the participants enrolled in the study also had reductions in AK incidence, and 40% showed a reduction in BCCs, although the pre-intervention incidence was low. One-third of participants discontinued treatment by 1 year, and side effects including fatigue, hand-foot syndrome and diarrhea were common.36
A recent case series published in 2013 by Endrizzi et al reviewed outcomes of systemic capecitabine administration in 10 SOTRs. In this series, patients with high rates of new NMSC were administered a starting dose of 500 to 1500 mg/m2/day (based on body size and renal function) on days 1 and 14 of a 21-day cycle. Over a period of 12 months of treatment, a statistically significant reduction in the rate of cSCC was observed, with a range of 43–100%. A decrease in the number of clinically observable AKs was seen in 9 of 10 patients. There were too few BCCs to draw conclusions about the potential chemoprophylactic effects of capecitabine in this NMSC type.37
Capecitabine may be a useful alternative for reducing the overall burden of AKs and cSCC in the appropriate patient population when other treatments have failed despite optimization. Treatment may be limited by side effects including palmoplantar erythrodysesthesia, which may occur in up to 71% of patients, as well as acral erythema, stomatitis, pyogenic granulomas, hyperpigmentation and hand-foot syndrome.31,38 In the case series by Endrizzi et al, 7 of 10 study participants required dose adjustments, and 2 discontinued treatment as a result of adverse effects (AEs). Use may be limited by renal insufficiency as well as the rare presence of dihydropyrimidine dehydrogenase deficiency, which may cause severe toxicity and death.31,39
Currently, there are no guidelines or recommendations for the use of capecitabine as chemoprophylaxis or treatment of NMSC. The NCCN guidelines for the management of cSCC do suggest that capecitabine may be considered in SOTRs when surgery is impractical due to high tumor burden.1,37 (Table 1) The guidelines for the management of BCC are less specific, although consideration of capecitabine for individuals at high risk for developing NMSC is noted.21 Generally, initiation of capecitabine should be pursued in consultation with medical oncology as intensive monitoring is necessary.
Non-Steroidal Anti-Inflammatory Drugs
NSAIDs decrease prostaglandin synthesis by way of cyclooxygenase-2 (COX-2) inhibition, and overexpression of COX-2 has been suggested to play a role in the pathogenesis of NMSC.40 COX-2 levels increase within the epidermis after UV exposure, and the enzyme has been detected in AKs, cSCCs, and BCCs.41 NSAIDs have gained considerable interest for their immunomodulatory action in the prevention and treatment of various cancers.42 Although not entirely understood, there is evidence supporting the enhancement of anti-tumor immunity, augmentation of T cell cytotoxicity and improvement in cancer immunosurveillance.42 This insight has led to studies investigating the efficacy of both topical and systemic NSAIDs in the treatment of NMSC. To date, there have been conflicting results of studies evaluating the use of systemic NSAIDs for this indication.
A double-blind RCT trial published in 2010 by Elmets et al showed a statistically significant reduction in NMSC in patients administered 200 mg/day of celecoxib when compared to placebo after 11 months of treatment (mean cumulative tumor number per patient 0.14 vs 0.35, respectively). Patients enrolled in this study had 10–40 AKs and ≥ 1 previous histologically confirmed AK and/or NMSC.43 Interestingly, although celecoxib was effective in reducing the incidence of cSCC, the same effect was not seen with AKs.
Although these data are promising, other studies have failed to show a reproducible correlation between NSAIDs and cSCC risk. A retrospective case–control study of 415 patients published in 2010 by Asgari et al did not show any negative correlation between NSAID use and cSCC risk, and a meta-analysis published in 2014 also failed to show any statistically significant protective effect of NSAIDs on NMSC incidence.44
The most recent meta-analysis published in 2015 by Muranushi et al included 2 other studies that were not investigated in the prior meta-analysis by Zhang et al. This meta-analysis included 3 cohort studies and 3 case–control studies for the use of aspirin, and 7 studies (1 RCT, 3 cohort and 3 case control) investigating the use of non-aspirin NSAIDs in the prevention of NMSC.43,45–52 The data from this analysis showed a statistically significant reduction in cSCC risk by 15 and 18% with the use of non-aspirin NSAIDs or any NSAIDs, respectively.53
Although there may be some benefit in the use of systemic NSAIDs, this must be weighed with the risk of side effects and other AEs. The use of COX-2 inhibitors has fallen out of favor due to the increased risk of adverse cardiovascular effects, in addition to other side effects including bleeding risk and adverse gastrointestinal effects.54 Given mixed results, risk for side effects, and availability of other efficacious options, the use of NSAIDs in the chemoprevention of NMSC is currently limited.
mTOR Inhibitors
SOTRs have a risk for NMSC that is well beyond that of other immunosuppressed cohorts, estimated to be up to 10 times greater than HIV positive individuals. This suggests that both the mechanism and level of immunosuppression play a role in the risk of NMSC development and overall tumor burden.8 Studies investigating the relationship between immunosuppressive regimens and the risk of NMSC development in SOTRs have shown variability of the impact of exogenous immunosuppression versus various immunosuppressive conditions (eg HIV, CLL, autoimmune disease, etc.) on overall risk.
Calcineurin inhibitors (cyclosporine and tacrolimus) have historically been a cornerstone of post-transplant immunosuppressive regimens, and although they are efficacious in preventing organ rejection, they are known to enhance tumor development and increase risk for cutaneous malignancies. In contrast, mTOR inhibitors reduce the proliferation and growth of tumors, and have been shown to reduce the risk of NMSC development in SOTRs.55
A recent 9-year retrospective cohort study from 2016 evaluated 329 recipients of various organ transplants and showed an 11.6% reduction in skin cancer risk in SOTRs who were treated with sirolimus following the diagnosis of a posttransplant cancer compared to those not treated with sirolimus.56 A phase 3, multicenter, randomized, open-label trial from 2012 compared the incidence of cSCC in patients taking calcineurin inhibitors compared to those who were transitioned from calcineurin inhibitors to sirolimus. The results demonstrated a cSCC-free survival that was significantly longer in patients taking sirolimus, and a relative risk of 0.56.57 Most of the patients receiving sirolimus experienced an AE, most commonly edema, acneiform eruptions, and aphthous ulcers. The most common serious AEs reported were pneumonitis and diarrhea.57
A prospective, multicenter, open-label RCT from 2012 enrolled 86 renal transplant recipients on calcineurin inhibitor based immunosuppressive regimens for at least 1 year and randomized half of the group to convert their calcineurin inhibitor to sirolimus. The data showed a significantly lower yearly NMSC rate among those taking sirolimus compared to those who remained on calcineurin inhibitors (1.31 vs 2.48 lesions/patient-year, respectively). In the sirolimus group, higher rates of acne, diarrhea, epistaxis, oral ulcers, edema, rash, pneumonitis, and albuminuria were noted. 42.6% of participants discontinued sirolimus due to side effects, most commonly pneumonitis, and diarrhea.58 Notably, no participants in the sirolimus arm experienced rejection of their transplanted kidney, suggesting adequate immunosuppression.
Despite one recent 2016 retrospective cohort study that failed to demonstrate a reduction in cSCC risk with prior sirolimus exposure,59 there are multiple other studies that have reproduced positive results without an increased risk for organ rejection.60–65 Other side effects of sirolimus that may limit its use include cytopenias, lymphedema, mucositis, interstitial lung disease, metabolic syndrome, gastrointestinal side effects, renal toxicity, and thromboembolic disease. Wound healing complications have also been observed with the use of mTOR inhibitors,66 and special consideration must be made to reduce the risk of post-operative complications, especially in patients with other risk factors for poor wound healing.67
Currently, the NCCN guidelines version 2.2022 for the management of cSCC note that consideration should be given to either reduce the level of immunosuppression and/or incorporate mTOR inhibitors into the immunosuppressive regimen of SOTRs in cases of life-threatening skin cancer, or the rapid development of multiple tumors. (Table 1) Expert consensus suggests that revision of immunosuppression should also be considered in SOTRs at risk for significant disease burden or poor outcomes from cSCC.68 The guidelines for the management of BCC do not comment on revision of immunosuppressive regimens for the purpose of BCC prevention.
Checkpoint Inhibitors/Immunotherapy
Checkpoint inhibitors generate an antitumor response by blocking immune checkpoint target proteins cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed cell death 1 receptor and ligand (PD-1 and PD-L1, respectively). This ultimately activates T cells to target tumor cells, leading to tumor destruction. The development of systemic immunotherapy has revolutionized the treatment of multiple different skin cancers, including Merkel cell carcinoma, melanoma, and locally advanced and metastatic NMSC.69,70 There are currently five immune checkpoint inhibitors approved for use in cutaneous malignancies: nivolumab, pembrolizumab, cemiplimab, avelumab, and ipilimumab.
Cemiplimab, an IgG4 monoclonal antibody that inhibits PD-1, was approved by the US Food and Drug Administration (FDA) in 2018 for the treatment of metastatic or locally advanced cSCC in patients who were not candidates for curative surgery or RT. Results published in 2020 from the EMPOWER-CSCC 1 trial, an open-label, phase 2, single-arm study evaluating the safety and efficacy of cemiplimab in 78 patients with locally advanced cSCC who were not candidates for surgery or RT, report an objective response in 44% of patients with complete response (CR) in 13% and partial response (PR) in 31% among patients treated with cemiplimab 3 mg/kg IV every 2 weeks for up to 96 weeks. Forty-four percent of patients experienced grade 3 or 4 AEs, most commonly hypertension and pneumonia.71 Two patients had treatment-emergent AE that resulted in death, one of which was attributable to the study drug.71 A more recent phase 2, confirmatory, multicenter, nonrandomized study evaluated the efficacy of neoadjuvant cemiplimab in patients with resectable Stage II–IV (M0) cSCC.72 Seventy-nine patients received 350 mg of IV cemiplimab every 3 weeks for 4 doses prior to surgical resection. The ORR was 68.4%, with a pathological CR of 50.6% and a major pathologic response in an additional 12.7%.72 17.7% of patients developed AEs that were at least grade 3 in severity, and the most commonly reported AEs were rash, fatigue, nausea and diarrhea.72,73 Four AEs were observed that resulted in death, one of which was possibly related to treatment.72 Durability of response is currently under investigation, showing continued response rates at 3 year follow-up.74
Cemiplimab is currently also FDA approved for the treatment of locally advanced or metastatic BCC previously treated with a hedgehog inhibitor (HHI), or when HHIs are contraindicated.75–78 A open-label, multicenter, single-arm, phase 2 trial evaluated the efficacy of cemiplimab in 84 patients with locally advanced or metastatic BCC who were intolerant to HHIs or who had progressive disease despite HHI therapy.76 Patients received 350mg of IV cemiplimab every 3 weeks for a maximum of 93 weeks. Six percent of patients demonstrated a CR to therapy and 25% demonstrated a PR after a median follow-up duration of 15 months. There were various adverse events reported, and the most common serious AEs that were considered treatment related were adrenal insufficiency and colitis.76 Three treatment-emergent deaths were reported, none of which were attributed to the study drug.76
Pembrolizumab, another PD-1 inhibitor, was approved by the FDA for the treatment of recurrent and metastatic cSCC in June of 2020.79 The KEYNOTE-629 Phase II trial is an ongoing multicenter, nonrandomized, single-arm, open-label trial investigating subjects with histologically confirmed locally advanced, recurrent, and metastatic cSCC who are not eligible for surgical resection, or not cured by surgery or RT. In the second interim analysis published in October 2021, a 50.0% ORR with 16.7% CR and 33.3% PR was reported among a cohort of subjects with locally advanced disease receiving pembrolizumab 200 mg IV every 3 weeks for up to 24 months. The recurrent/metastatic cohort showed a 35.2% ORR with 10.5% CR and 24.8% PR, and an estimated response durability of 77.8% at ≥ 12 months.80–82
CARSKIN, an open-label, uncontrolled, multicenter phase 2 trial also examined the effects of pembrolizumab in subjects with unresectable cSCC. Data showed a statistically significant ORR of 41% at 15 weeks, including 13 PRs and 3 CRs. AEs occurred in 71% of subjects, and 7% were ≥ grade 3 adverse reactions, including diarrhea, colitis, vasculitis, secondary de novo head and neck cancer, cSCC hyper-progression and cholestasis.80 Two treatment-related deaths were reported.80 Other common AEs that may limit the use of pembrolizumab include gastrointestinal symptoms, rash, fatigue, musculoskeletal pain, diminished appetite, pyrexia, and immune-mediated AEs including colitis, hepatitis, nephritis, pneumonitis, and endocrinopathies.83
Notably, in April 2022 the FDA approved a new immunotherapy for the treatment of patients with previously untreated metastatic or unresectable melanoma. The drug, relatlimab, blocks lymphocyte-activation gene 3, an inhibitory immune checkpoint. The drug has shown promise in the treatment of advanced melanoma when combined with nivolumab, a PD-1 inhibitor. It is worthy to note that many immune checkpoint inhibitors have been first approved for melanoma, preceding studies looking into their efficacy for NMSC, and thus future studies are likely to investigate their role in the treatment of these malignancies.84,85
The current 2.2022 NCCN guidelines recommend cemiplimab or pembrolizumab as first-line therapy for the treatment of locally advanced, recurrent, or metastatic cSCC if curative RT or surgery is not feasible.1 (Table 1) Other treatments such as carboplatin, paclitaxel, epidermal growth factor receptor inhibitors, capecitabine, cisplatin, and 5-FU are now recommended for cSCC only if patients progress or do not respond to checkpoint inhibitors. These treatments were historically the only available options for patients with unresectable disease and are generally associated with significant toxicity and low overall survival rates.86,87 The guidelines also recommend cemiplimab for patients with BCC previously treated with an HHI or in which an HHI is not appropriate.75,76 Further studies are currently underway examining the use of immune checkpoint inhibitors for other NMSC indications as well as in the neoadjuvant setting.88,89 Although there are some reports of efficacy in SOTRs, the safety of PD-1 inhibitors in this population is largely unknown, and the risk for organ rejection with immune activation may be high given the mechanism of action.90 Nevertheless, patients who may qualify for treatment with immunotherapy benefit from a multidisciplinary approach to care, with input from dermatology, medical oncology, surgical oncology, and radiation oncology.
Topical Immunomodulators
Topical Retinoids
Topical retinoids, like their systemic counterparts, also bind to nuclear retinoic acid receptors, affecting the transcription of genes that control cell growth and differentiation.91 This mechanism of action renders them useful in the treatment of acne, psoriasis, photoaging, and other dermatologic conditions. Topical retinoids have been thought to have immunomodulatory action by normalizing hyperkeratinization and therefore altering the microenvironment of the skin by regulating inflammatory mediators and toll-like receptors, and by inhibiting chemotaxis of polymorphonuclear cells.92
Topical retinoids are currently not approved by the FDA for the treatment of NMSC or precursor lesions, however studies have demonstrated efficacy in the treatment of facial AKs. A double-blind, controlled, multicenter study from 1991 involving 1265 patients demonstrated that 0.1% tretinoin cream applied twice daily for 15 months reduced the total number of AKs by 73%.93
A more recent RCT from 2003 demonstrated that adapalene gel, a synthetic retinoid, improves AKs, solar lentigines, and other features of photodamaged skin.94 Ninety patients with AKs and solar lentigines were treated daily with adapalene gel 0.1%, 0.3% or a vehicle gel for 4 weeks, followed by twice daily application if tolerated for up to 9 months. At the end of study period, the mean number of AKs reduced by 0.5 ± 0.9 with 0.1% gel and 2.5 ± 0.9 with 0.3% gel.94 A significant increase in the number of AKs was observed in the control group (1.5 ± 1.3, P<0.5). Histologic evaluation demonstrated improved cellular atypia in the treatment group, although differences were not statistically significant.
The role of topical retinoids as an adjunct to other topicals has also been explored. A RCT evaluated the efficacy of daily 0.05% topical tretinoin application to AKs following 5-FU cream application.95 After 3 months, adjunct tretinoin application to the upper extremities showed improved reduction of AKs compared to the control group, suggesting topical retinoids may enhance the efficacy of topical 5-FU in AK reduction.95 Tretinoin and adapalene have also been used to treat AKs or NMSC in conjunction with laser ablation therapy and PDT.96
The efficacy of high dose topical retinoids in preventing NMSC has been investigated, but results supporting chemoprevention are mixed.97 In one randomized, double-blind, vehicle-controlled study, only 6% of patients had a chemopreventive response when tazarotene was used in patients with basal cell nevus syndrome, suggesting against a clinically significant chemopreventive or chemotherapeutic effect.98
Overall, evidence for the use of topical retinoids for the treatment or prevention of NMSC is limited, and other topicals have demonstrated more consistent efficacy for this indication.99–101 The current 2.2022 NCCN guidelines for the management of cSCC recommends against the use of topical retinoids as prophylactic treatment for patients at high risk of NMSC or AKs.1,97 The guidelines for BCC note that tazarotene may be considered for treatment,21 however there is little data to support a significant chemopreventive or curative response98 (Table 1).
5-Fluorouracil
Topical fluorouracil is the most extensively studied topical chemotherapeutic agent and is FDA approved for the treatment of AKs and superficial BCCs.99–101 5-FU is an antimetabolite drug that interferes with DNA synthesis by inhibiting thymidylate synthetase activity. Cancerous cells incorporate pyrimidine uracil into RNA more rapidly than normal cells, and 5-FU is misincorporated into nucleic acid, resulting in cell death.99,102 When combined with calcipotriol, a vitamin D analog, a significant increase in immunity against AKs has been demonstrated among CD4+ T cells.103 It has been suggested that this robust response in addition to lasting T cell immunity may confer a more durable response when the two medications are used synergistically.103
Topical 5-FU has consistently been shown to reduce AKs when applied topically to lesions for 2 to 4 weeks.104 Two RCTs demonstrated that 5-FU application to the dorsum of the hands105 and face106 resulted in a mean reduction of AKs of 70% and 78%, respectively. A recent randomized, double-blinded, placebo-controlled trial published in 2015 compared the application of topical 5-FU cream to a vehicle control twice daily to the face and ears in 932 study subjects who had > 2 NMSC in the 5 years prior to enrollment. The treatment group had higher complete AK clearance rates (38% vs 17% at 6 months) and needed fewer spot treatments at 6-month intervals and other follow-ups during the study interval.107 A systematic review of 4 RCTs assessing 5-FU therapy for AKs published in 2012 showed a total clearance and mean lesion count reduction of 52.6% and 90.2% in the treatment groups, and 0.85% and 28.3% in the vehicle groups, respectively.108
Calcipotriol is an inducer of thymic stromal lymphopoietin, a cytokine that produces antitumor immunity in the skin.109 As discussed previously, when used in combination with 5-FU for the treatment of AKs, a robust T-cell mediated immune response has been shown. An investigator-initiated, randomized, double-blind clinical trial comparing the safety and efficacy of 0.005% calcipotriol ointment + 5-FU cream compared with petroleum jelly + 5-FU cream for a 4 day treatment of AKs on the scalp, face and upper extremities showed a statistically significant 87.8% vs 26.3% mean reduction in the number of AKs in study subjects.103,109 Data from a systematic review published in 2022 reviewing studies investigating calcipotriol plus 5-FU in the treatment of AKs showed a greater reduction in AKs compared to treatment with 5-FU alone, as well as a lowered risk of cSCC on the face and scalp over a 3-year period.103,109–112 The lasting effects may be due in part to resident memory T cells conferring long-term protection against AKs and cSCC following T cell activation during treatment.
A recent systematic literature review from 2009 reviewed results from studies investigating the treatment of NMSC with topical imiquimod and 5-FU.113 Six different studies investigating the use of 5-FU in superficial BCC and cSCC were reviewed. Ninety percent of superficial BCCs were cleared in 31 patients treated for an average of 10.5 weeks with twice daily 5-FU, confirmed 3 weeks after treatment cessation by histologic evaluation.114 Studies with various regimens of 5-FU application (twice daily, once daily under occlusion, once daily for 1 week then twice daily for 3 weeks, etc.) for various durations (4 weeks – 4 months) showed clearance rates ranging from 26% to 85% of cSCC in situ (SCCIS). The study showing the highest clearance rate of 85% was published in 2003 and data was drawn from 26 lesions that were treated for an average of 7.7 weeks with twice daily 5-FU. In this study, 17 of 26 lesions had histopathologic resolution, 6 were clinically clear and 2 lacked sufficient follow-up.115 This is one of the highest clearance rates published, and most other studies cite variable clearance rates in the range of approximately 30–60% of SCCIS. Despite promising results, the use of 5-FU in SCCIS is currently not approved by the FDA.
The NCCN guidelines currently recommend topical 5-FU with or without calcipotriol as an accepted treatment modality for the treatment of diffuse AKs, field cancerization and cSCC prophylaxis (Table 1). The NCCN panel currently prefers 5-FU for treatment of AKs over IMI, methyl aminolevulinate (MAL) PDT or IMB given a higher cumulative probability of remaining free from treatment failure.104 These treatments will be discussed in detail later in this review article. As per the guidelines, topical 5-FU may also be considered for patients with SCCIS, though the cure rate may be lower than that of surgical treatments. Consideration for treatment must also consider the common AEs of treatment which include skin irritation, erythema, dryness, erosions, pain and burning sensations, pruritus, vesicle formation, and ulcerations. Reactions caused by 5-FU monotherapy correlate with the degree of actinic damage present on the treated skin, and therefore patients should be appropriately counseled prior to treatment initiation.104 Improved tolerability and milder AEs have been reported when topical 5-FU is used in conjunction with topical calcipotriol to treat precancerous lesions, without reduction in efficacy.103 The NCCN guidelines for the treatment of BCC recommend consideration of topical 5-FU for patients with superficial BCC with adequate understanding that cure rates may be at least 10% lower than with surgical modalities21,113,116 (Table 1).
Imiquimod
IMI is an immunomodulatory drug that activates toll-like receptors, ultimately regulating mRNA expression of genes responsible for the production of cytokines by monocytes, macrophages, and epidermal keratinocytes.117 The result is an enhanced innate and cell-mediated immune response protective against tumor activity, and induction of pro-apoptotic pathways.117 IMI is currently FDA approved for the use of superficial BCC (5% IMI) and AKs (all concentrations).118
IMI was approved in 2004 for the treatment of superficial BCC after a RCT reported a histologic clearance of 82% for superficial BCC treated topically 5 times per week for 6 weeks. Tumors included in these data were smaller than 2 cm and in low-risk locations.113,119–121 A more recent meta-analysis from 2012 examining both randomized and nonrandomized studies reported a pooled estimate of 86.2% CR of superficial BCC at 12 weeks post treatment with topical IMI, and a tumor-free survival of 87.3% at 1 year.122 Studies examining the efficacy of IMI in nodular BCC, including a phase 2 clinical trial, have reported a response rate of 76% after treatment with 5% IMI cream twice daily for 12 weeks.123 Although surgical approaches remain the standard of care for the treatment of nodular BCCs, IMI may represent an acceptable option for patients who cannot undergo surgery.
Many studies have shown the efficacy of IMI in the treatment of SCCIS, with clearance rates ranging from 70 to 100%.113,124–127 A double-blind, placebo-controlled RCT reported a 75% clinical and histologic clearance rate at 28 weeks following treatment with 5% IMI daily for 16 weeks.128 Patients randomized to receive IMI had various local AEs including pruritus, edema, erosions, and drainage. Other studies investigating the efficacy of IMI in SCCIS report high clearance rates, even in SOTRs and patients with CLL treated in combination with 5-FU and sulindac, respectively.129,130 Generally, studies investigating the efficacy of IMI for SCCIS tumors located on the extremities and the trunk reported improved clearance rates in lower risk anatomic locations.128 In a study examining 829 patients with a total of 7427 AKs treated with IMI 5% cream three times weekly for 4 weeks, followed by repeat treatment if resolution had not occurred, IMI achieved an 85% reduction in the total number of lesions.131 Many other double-blind RCTs have reproduced similar results. Further, improved response rates were noted with application three times weekly when compared to twice weekly application.132–134
The NCCN guidelines recommend the use of topical IMI for SCCIS in anatomically challenging locations for which recurrences would be small and manageable, with the understanding that cure rates may be lower than with surgical treatment modalities. (Table 1) IMI is also recommended for the treatment of superficial BCC in the NCCN guidelines, citing studies that suggest that IMI use is associated with superior results when compared to 5-FU cream, especially when used on large or truncal tumors.21,120,122,135,136
Ingenol Mebutate
IMB is an extract from the plant Euphorbia peplus that induces cell death in dysplastic keratinocytes via necrosis and immune stimulation leading to cytotoxicity.137,138 Through chemoablation, IMB disrupts the plasma membrane of keratinocytes and leads to mitochondrial swelling. Its additional mechanism of action involves induction of neutrophil infiltration and production of tumor-specific antibodies and pro-inflammatory cytokines, leading to an antibody-dependent cellular cytotoxicity that eliminates residual cells.117,139
IMB was first approved by the FDA in 2012 for treatment of AKs of the face and scalp, based on two double-blind RCTs, and later approved for use on the trunk and extremities after data from two further RCTs were published.140–143 However in 2020, drug production was discontinued in the US and other areas of the world after a study comparing the use of IMB to IMI showed increased rates of cSCC in areas treated with IMB.144,145
NSAIDs
As previously discussed, tumorigenesis in NMSC may be linked to expression of COX-2, thus
supporting the theory that inhibitors of this enzyme may be useful in treatment. Further, as noted previously, NSAIDs may enhance anti-tumor immunity, augment T cell cytotoxicity and improve cancer immunosurveillance.42
A RCT of 130 patients published in 1997 studied the tolerability and efficacy of topical 3% diclofenac in hyaluronic acid (HA) gel vs HA gel alone applied twice per day for 24 weeks, and failed to show a statistically significant difference in the reduction of AKs, despite a high rate of PR.146 In contrast, a more recent multicenter, double-blind, placebo-controlled study showed a statistically significant reduction in AKs in patients treated with 3.0% diclofenac in 2.5% HA gel when used twice daily for 60 days.147 A second randomized, double-blind, placebo-controlled study produced similar results at 16 weeks after 12 weeks of treatment with twice daily 3% diclofenac in 2.5% HA gel. In this study, there was a 56.1% reduction of AK lesions in the active treatment group, compared to 23.6% in the placebo group.148
Given the conflicting results of RCTs, the NCCN guidelines for the management of SCCIS accepts topical diclofenac as appropriate, based only upon lower-level evidence and notes it is inferior to other topical treatments as well for the treatment of AKs. (Table 1) There is no current recommendation for its use in the treatment of BCC.21
Photodynamic Therapy
PDT is efficacious in the treatment of NMSC and AKs by way of the production of reactive oxygen species which cause cellular apoptosis.149 Application of a photosensitizing agent followed by exposure to light creates the reactive oxygen species and free radicals which contribute to the mechanism of action. There are several different photosensitizers available on the market. The most common are 5-aminolevulinic acid (ALA), and methyl-5-aminolevulinate (MAL). In addition to local effects, PDT has been shown to augment host immune response by way of recruitment of various immune cells to the treated area.150
ALA-PDT and MAL-PDT are currently FDA approved for the treatment of AKs. A multicenter, investigator-blinded, randomized, vehicle-controlled study published in 2001 showed 88% clearance of AKs 8 weeks after a single PDT treatment, compared to 6% with vehicle only.151 A more recent RCT from 2004 showed 89% of patients had a 75% or more clearance rate of AKs at 12 weeks after treatment. Most of the patients enrolled in this trial experienced either a burning or stinging sensation during treatments, and delayed effects such as edema and erythema of the treated sites.152 Some studies suggest that MAL-PDT may be associated with a shorter duration of pain and discomfortwhen compared to ALA-PDT.153,154 An RCT from 2009 evaluating the efficacy of PDT using MAL and light-emitting diodes for the treatment of AKs showed a CR rate of 83.3%.155 PDT has shown to be effective in delaying the onset of AKs in renal transplant patients when administered at 6-month intervals for 5 years.156 This may represent an alternative method to reducing the overall actinic burden in SOTRs, however studies looking at the development of cSCC over time in this population treated with PDT are conflicting.157
Studies evaluating the efficacy of PDT in the treatment of BCC have shown CR rates ranging from 73 to 99% for superficial BCCs.153 One study comparing ALA and MAL-PDT for the treatment of nodular BCCs showed similar effectiveness of each;158 however, others report improved outcomes with MAL-PDT.159 The results from 2 RCTs showed a CR rate of 73% for the treatment of nodular BCC with MAL-PDT, with the highest effectiveness for lesions of the face (89% CR). Despite variable published efficacy rates, PDT may represent an acceptable non-surgical option for BCCs in patients who cannot undergo surgery. The NCCN guidelines for the treatment of BCC note PDT may have similar effectiveness as cryotherapy but with superior cosmetic outcomes in the treatment of superficial BCC; however, treatment success is inferior to that of IMI.21
Data from studies investigating the efficacy of PDT in the treatment of SCCIS have shown response rates of 90–100%, with an average rate of recurrence of 12% following 1 to 3 PDT treatments.160 A randomized comparison of ALA-PDT to 5-FU in the treatment of SCCIS showed a higher CR in the ALA-PDT group (88%) compared to the 5-FU group (67%).161 One study evaluated cyclical ALA-PDT treatments for SOTRs at 4 to 8-week intervals for a duration of 2 years and showed a 79 and 95% reduction in cSCCs at 12 and 24 months, respectively, when compared to pre-treatment counts.162 The current NCCN guidelines for the treatment of cSCC note that PDT treatment may lead to higher rates of initial clearance and durability of response than 5-FU in the treatment of cSCC, however there is significant variability in effectiveness owing to differences in application and protocols. Therefore, 5-FU is still preferred in the treatment of cSCC.1
Discussion
The carcinogenesis of NMSC relies mainly on UV-induced DNA and oxidative damage, which ultimately leads to various mutations in genes regulating cellular growth and proliferation. Among other risk factors for the development of NMSC, immunosuppression has been shown to confer a substantially higher risk, proving the importance of the immune system in the surveillance of these malignancies. It has been suggested that the high mutational burden in NMSC likely leads to the development of UV-induced neoantigens, which in an immunocompetent host, should trigger an active immune response. In those with suppressed immunity, host surveillance mechanisms are impaired, leading to an increased rate of cancer development.163 It is therefore in accordance that immunomodulatory treatments are often useful in the treatment of NMSC, by way of regulation and activation of the anti-cancerimmune response.
At present, there are many immunomodulatory options with various mechanisms of action for the treatment of both AKs and NMSC. The data supports the use of acitretin in the chemoprevention of NMSC in the SOTR population, as well as other individuals with diffuse actinic damage who have been diagnosed with multiple NMSCs.22 The risk of side effects must be weighed against the potential benefit of preventing the formation of new NMSCs. Other retinoids have less consistent data, or the risk of side effects outweighs the potential benefits.19,20 Nicotinamide shows promising data as an alternative option for chemoprevention, although long-term studies are needed to investigate the durability of response.22,24,30 The current data for nicotinamide in immunocompromised populations is generally lacking, making it difficult to generalize the efficacy to these high-risk groups. Given the low rate of side effects and drug–drug interactions, this supplement is generally well tolerated and may be administered to high-risk patients with increased rate of NMSC development. Capecitabine has shown excellent efficacy in the reduction of AKs and cSCC burden, however side effects are common and may be serious. The use of this drug is therefore limited for chemoprevention, but may be an acceptable salvage option in patients with a heavy burden of disease who are not responding optimally to alternative regimens.38,39 If considered, initiation should occur in a multidisciplinary setting as intensive monitoring is necessary. The use of systemic NSAIDs is generally limited by side effects and risks, as well as the presence of alternatives with superior data to support their use.54 For SOTRs, revision of immunosuppression from calcineurin inhibitors to mTOR inhibitors should be considered in patients with significant disease burden from NMSC or with aggressive, high-risk, or locally advanced/metastatic tumors.68 Although surgical approaches remain the standard of care for the treatment of many cSCCs, checkpoint inhibitors (cemiplimab, pembrolizumab) have become a mainstay of therapy in patients with locally advanced, recurrent, or metastatic cSCC if unresectable or not amenable to curative RT.1 Checkpoint inhibitors also play a role in the treatment of advanced BCCs in select situations. Results from studies examining the utility of checkpoint inhibitors as neoadjuvant treatments are promising and may ultimately lead to a dramatic shift in the standard treatment algorithms for locally advanced and metastatic tumors.72 Significant toxicity and AEs with the use of checkpoint inhibitors may occur, and the risk of organ rejection is still under investigation.90 Collaboration with medical oncology, transplant surgery, radiation oncology and surgical oncology is critical in the initiation of these drugs in most circumstances.
Topical immunomodulators are widely used in clinical practice for both the prevention and treatment of AKs and NMSCs. Topical 5-FU is currently accepted as the superior topical therapy for the treatment of diffuse AKs, field cancerization and for the chemoprevention of cSCC given a higher cumulative probability of successful treatment when compared to IMI, MAL PDT or IMB.104 5-FU is currently not FDA approved for the treatment of SCCIS or superficial BCC; however, off label use may be considered if surgery or other destructive treatment options are contraindicated or not feasible. The addition of calcipotriol has been shown to result in a greater reduction in AKs, improved tolerability, and a lowered risk of future cSCC development on the face and scalp.103,109,110,112 IMI is currently FDA approved for the treatment of superficial BCCs and AKs, with the highest BCC clearance rates in truncal tumors. IMI has been shown to be a more effective superficial therapy for BCCs as compared to 5-FU cream.21 PDT is an efficacious treatment for AKs and is an acceptable and efficacious option for the treatment of cSCC and BCC in patients who cannot undergo surgery. Notably, PDT has been reported to be inferior to IMI in the treatment of BCC especially for large or truncal tumors, however PDT may have better outcomes for elderly patients with lower extremity lesions. For the treatment of SCCIS, PDT has been associated with higher rates of initial complete clearance and higher durable complete response rates when compared to 5-FU.1 Although a reasonable option for the treatment of certain low risk cSCCs and BCCs, PDT is currently only FDA approved for the treatment of AKs. The data to support the use of topical retinoids as well as NSAIDs is limited and conflicting and given superior alternatives for treatment and prevention of NMSC, their use is currently not recommended.21–99,101 Diclofenac gel is appropriate to use for AKs due to a favorable safety profile, however the data supporting its efficacy is weak.21,164 The use of IMB has been largely discontinued after drug production was discontinued out of concern for increased risk of cSCC.165
Conclusion
The immune system plays a critical role in the surveillance of NMSC, and those who have muted immune responses are at much higher risk for the development of these malignancies. Immunomodulatory therapies enhance the immune response to NMSC through various mechanisms and are critical in both the prevention and treatment of these malignancies. The identification of patients at increased risk for field cancerization and NMSC development is crucial to reduce the overall burden of disease. Proactive approaches to reduce the overall disease burden in the immunosuppressed are necessary, especially in the SOTR population. Once identified, a personalized regimen of both systemic and topical immunomodulators may be selected for at-risk individuals, and close ongoing monitoring should be pursued to prevent morbidity and mortality of NMSC. Cyclical multi-modal therapy regimens over extended periods of times may be necessary and key to reverse UV toxicity to the skin and eradicate neoplastic keratinocytes at risk of tumorigenesis and subsequent morbidity and mortality. With ongoing research into the genetics of cutaneous malignancies and various biomarkers signaling susceptibility to disease, stratification of pre-cancerous lesions, and risk for disease progression, it is likely that the future holds revolutionary options for early detection and personalized treatment.166 In the present and as our understanding evolves into the future, dermatologists continue to play a critical role in the prevention and management of AKs and NMSCs, and have many immunomodulatory drugs to choose from to individualize regimens for at-risk patients.
Abbreviations
5-FU, 5-fluorouracil; AKs, actinic keratoses; BCC, basal cell carcinoma; BWH, Brigham and Women’s Hospital; CLL, chronic lymphocytic leukemia; COX-2, cyclooxygenase-2; CR, complete response; cSCC, cutaneous squamous cell carcinoma; CTLA-4, cytotoxic T-lymphocyte-associated protein 4; FDA, Food and Drug Administration; HA, hyaluronic acid; HHI, hedgehog inhibitor; IMB, ingenol mebutate; IMI, imiquimod; MAL, methyl aminolevulinate; mTOR, mammalian target of rapamycin; NCCN, National Comprehensive Cancer Network; NMSC, non-melanoma skin cancer; ORR, objective response rate; PD-1, programmed cell death 1 receptor; PD-L1, programmed cell death receptor 1 ligand; PDT, photodynamic therapy; PR, partial response; RCT, randomized-controlled trial; RT, radiation therapy; SOTR, solid organ transplant recipients; UV, ultraviolet.
Disclosure
Kristen Russomanno and Sara Abdel Azim report no conflicts of interest in this work. Vishal Patel discloses honorarium from Sanofi, Regeneron, PhD Biosciences, Biofrontera and Almirall.
References
1. National Comprehensive Cancer Network. Squamous cell skin cancer (Version 2.2022). Available from: https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf.
2. Didona D, Paolino G, Bottoni U, Cantisani C. Non melanoma skin cancer pathogenesis overview. Biomedicines. 2018;6(1):6. doi:10.3390/biomedicines6010006
3. Carr DR, Trevino JJ, Donnelly HB. Retinoids for chemoprophylaxis of nonmelanoma skin cancer. Dermatol Surg. 2011;37(2):129–145. doi:10.1111/j.1524-4725.2010.01842.x
4. Rigel CC, Carucci J, Wharton. J. Actinic keratoses, basal cell carcinoma, and squamous cell carcinoma. Dermatology. 2008;2008:1641–1659.
5. Lai M, Pampena R, Cornacchia L, et al. Cutaneous squamous cell carcinoma in patients with chronic lymphocytic leukemia: a systematic review of the literature. Int J Dermatol. 2022;61(5):548–557. doi:10.1111/ijd.15813
6. Brantsch KD, Meisner C, Schonfisch B, et al. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: a prospective study. Lancet Oncol. 2008;9(8):713–720. doi:10.1016/S1470-2045(08)70178-5
7. Cooper JZ, Brown MD. Special concern about squamous cell carcinoma of the scalp in organ transplant recipients. Arch Dermatol. 2006;142(6):755–758. doi:10.1001/archderm.142.6.755
8. Wheless L, Jacks S, Mooneyham Potter KA, Leach BC, Cook J. Skin cancer in organ transplant recipients: more than the immune system. J Am Acad Dermatol. 2014;71(2):359–365. doi:10.1016/j.jaad.2014.02.039
9. Wolverton SE. Systemic retinoids. In: Wu JJ, editor. Comprehensive Dermatologic Drug Therapy.
10. Pilkington T, Brogden RN. Acitretin: a review of its pharmacology and therapeutic use. Drugs. 1992;43(4):597–627. doi:10.2165/00003495-199243040-00010
11. Yuan ZF, Davis A, Macdonald K, Bailey RR. Use of acitretin for the skin complications in renal transplant recipients. N Z Med J. 1995;108(1002):255–256.
12. McKenna M, Murphy GM. Skin cancer chemoprophylaxis in renal transplant recipients: 5 years of experience using low-dose acitretin. Br J Dermatol. 1999;140(4):656–660. doi:10.1046/j.1365-2133.1999.02765.x
13. Bavinck JN, Tieben LM, Van der Woude FJ, et al. Prevention of skin cancer and reduction of keratotic skin lesions during acitretin therapy in renal transplant recipients: a double-blind, placebo-controlled study. J Clin Oncol. 1995;13(8):1933–1938. doi:10.1200/JCO.1995.13.8.1933
14. George R, Weightman W, Russ GR, Bannister KM, Mathew TH. Acitretin for chemoprevention of non-melanoma skin cancers in renal transplant recipients. Australas J Dermatol. 2002;43(4):269–273. doi:10.1046/j.1440-0960.2002.00613.x
15. Badri O, Schmults CD, Karia PS, Ruiz ES. Efficacy and cost analysis for acitretin for basal and squamous cell carcinoma prophylaxis in renal transplant recipients. Dermatol Surg. 2021;47(1):125–126. doi:10.1097/DSS.0000000000002423
16. Kadakia KC, Barton DL, Loprinzi CL, et al. Randomized controlled trial of acitretin versus placebo in patients at high-risk for basal cell or squamous cell carcinoma of the skin (North central cancer treatment group study 969251). Cancer. 2012;118(8):2128–2137. doi:10.1002/cncr.26374
17. Kraemer KH, DiGiovanna JJ, Moshell AN, Tarone RE, Peck GL. Prevention of skin cancer in xeroderma pigmentosum with the use of oral isotretinoin. N Engl J Med. 1988;318(25):1633–1637. doi:10.1056/NEJM198806233182501
18. Bellman BA, Eaglstein WH, Miller J. Low dose isotretinoin in the prophylaxis of skin cancer in renal transplant patients. Transplantation. 1996;61(1):173. doi:10.1097/00007890-199601150-00040
19. Levine N, Moon TE, Cartmel B, et al. Trial of retinol and isotretinoin in skin cancer prevention: a randomized, double-blind, controlled trial. Southwest skin cancer prevention study group. Cancer Epidemiol Biomarkers Prev. 1997;6(11):957–961.
20. Jones E, Korzenko A, Kriegel D. Oral isotretinoin in the treatment and prevention of cutaneous squamous cell carcinoma. J Drugs Dermatol. 2004;3(5):498–502.
21. National Comprehensive Cancer Network. Basal cell skin cancer (Version 2.2022). Available from: https://www.nccn.org/professionals/physician_gls/pdf/nmsc.pdf.
22. Que SKT, Zwald FO, Schmults CD. Cutaneous squamous cell carcinoma: management of advanced and high-stage tumors. J Am Acad Dermatol. 2018;78(2):249–261. doi:10.1016/j.jaad.2017.08.058
23. Park J, Halliday GM, Surjana D, Damian DL. Nicotinamide prevents ultraviolet radiation- induced cellular energy loss. Photochem Photobiol. 2010;86(4):942–948. doi:10.1111/j.1751-1097.2010.00746.x
24. Chen AC, Martin AJ, Choy B, et al. A phase 3 randomized trial of nicotinamide for skin- cancer chemoprevention. N Engl J Med. 2015;373(17):1618–1626. doi:10.1056/NEJMoa1506197
25. Chen AC, Martin AJ, Dalziell RA, et al. A phase II randomized controlled trial of nicotinamide for skin cancer chemoprevention in renal transplant recipients. Br J Dermatol. 2016;175(5):1073–1075. doi:10.1111/bjd.14662
26. Surjana D, Halliday GM, Damian DL. Nicotinamide enhances repair of ultraviolet radiation-induced DNA damage in human keratinocytes and ex vivo skin. Carcinogenesis. 2013;34(5):1144–1149. doi:10.1093/carcin/bgt017
27. Ungerstedt JS, Blömback M, Söderström T. Nicotinamide is a potent inhibitor of proinflammatory cytokines. Clin Exp Immunol. 2003;131(1):48–52. doi:10.1046/j.1365-2249.2003.02031.x
28. Yiasemides E, Sivapirabu G, Halliday GM, Park J, Damian DL. Oral nicotinamide protects against ultraviolet radiation-induced immunosuppression in humans. Carcinogenesis. 2009;30(1):101–105. doi:10.1093/carcin/bgn248
29. Sivapirabu G, Yiasemides E, Halliday GM, Park J, Damian DL. Topical nicotinamide modulates cellular energy metabolism and provides broad-spectrum protection against ultraviolet radiation-induced immunosuppression in humans. Br J Dermatol. 2009;161(6):979.e1–979.e12. doi:10.1111/j.1365-2133.2009.09244.x
30. Collins L, Asfour L, Stephany M, Lear JT, Stasko T. Management of non-melanoma skin cancer in transplant recipients. Clin Oncol. 2019;31(11):779–788. doi:10.1016/j.clon.2019.08.005
31. Wolverton SE. Systemic anticancer agents: dermatologic indications and adverse events. In: Wu JJ, editor. Comprehensive Dermatologic Drug Therapy.
32. Asleh K, Brauer HA, Sullivan A, et al. Predictive biomarkers for adjuvant capecitabine benefit in early-stage triple-negative breast cancer in the FinXX clinical trial. Clin Cancer Res. 2020;26(11):2603–2614. doi:10.1158/1078-0432.CCR-19-1945
33. Wollina U, Hansel G, Koch A, Kostler E. Oral capecitabine plus subcutaneous interferon alpha in advanced squamous cell carcinoma of the skin. J Cancer Res Clin Oncol. 2005;131(5):300–304. doi:10.1007/s00432-004-0656-6
34. Peramiquel L, Dalmau J, Puig L, Roe E, Fernandez-Figueras MT, Alomar A. Inflammation of actinic keratoses and acral erythrodysesthesia during capecitabine treatment. J Am Acad Dermatol. 2006;55(5 Suppl):S119–S120. doi:10.1016/j.jaad.2005.11.1100
35. Serrao VV, Feio AB. Inflammation of actinic keratoses with capecitabine therapy for colon cancer. Eur J Dermatol. 2008;18(2):200. doi:10.1684/ejd.2008.0370
36. Jirakulaporn T, Endrizzi B, Lindgren B, Mathew J, Lee PK, Dudek AZ. Capecitabine for skin cancer prevention in solid organ transplant recipients. Clin Transplant. 2011;25(4):541–548. doi:10.1111/j.1399-0012.2010.01348.x
37. Endrizzi B, Ahmed RL, Ray T, Dudek A, Lee P. Capecitabine to reduce nonmelanoma skin carcinoma burden in solid organ transplant recipients. Dermatol Surg. 2013;39(4):634–645. doi:10.1111/dsu.12049
38. Wolf SL, Qin R, Menon SP, et al. Placebo-controlled trial to determine the effectiveness of a urea/lactic acid-based topical keratolytic agent for prevention of capecitabine- induced hand-foot syndrome: north central cancer treatment group study N05C5. J Clin Oncol. 2010;28(35):5182–5187. doi:10.1200/JCO.2010.31.1431
39. O’reilly zwald F, Brown M. Skin cancer in solid organ transplant recipients: advances in therapy and management: part II. Management of skin cancer in solid organ transplant recipients. J Am Acad Dermatol. 2011;65(2):263–279. doi:10.1016/j.jaad.2010.11.063
40. Kuzbicki L, Lange D, Stanek-Widera A, Chwirot BW. Different expression of cyclooxygenase-2 (COX-2) in selected nonmelanocytic human cutaneous lesions. Folia Histochem Cytobiol. 2011;49(3):381–388. doi:10.5603/fhc.2011.0054
41. An KP, Athar M, Tang X, et al. Cyclooxygenase-2 expression in murine and human nonmelanoma skin cancers: implications for therapeutic approaches. Photochem Photobiol. 2002;76(1):73–80. doi:10.1562/0031-8655(2002)076<0073:ceimah>2.0.co;2
42. Hussain M, Javeed A, Ashraf M, Al-Zaubai N, Stewart A, Mukhtar MM. Non-steroidal anti-inflammatory drugs, tumour immunity and immunotherapy. Pharmacol Res. 2012;66(1):7–18. doi:10.1016/j.phrs.2012.02.003
43. Elmets CA, Viner JL, Pentland AP, et al. Chemoprevention of nonmelanoma skin cancer with celecoxib: a randomized, double-blind, placebo-controlled trial. J Natl Cancer Inst. 2010;102(24):1835–1844. doi:10.1093/jnci/djq442
44. Zhang B, Liang X, Ye L, Wang Y, Wei Q-Y. No chemopreventive effect of nonsteroidal anti- inflammatory drugs on nonmelanoma skin cancer: evidence from meta-analysis. PLoS One. 2014;9(5):e96887. doi:10.1371/journal.pone.0096887
45. Clouser MC, Roe DJ, Foote JA, Harris RB. Effect of non-steroidal anti-inflammatory drugs on non-melanoma skin cancer incidence in the SKICAP-AK trial. Pharmacoepidemiol Drug Saf. 2009;18(4):276–283. doi:10.1002/pds.1718
46. Nunes AP, Lapane KL, Weinstock MA, Group VT. Association between non-steroidal anti-inflammatory drugs and keratinocyte carcinomas of the skin among participants in the veterans affairs topical tretinoin chemoprevention trial. Pharmacoepidemiol Drug Saf. 2011;20(9):922–929. doi:10.1002/pds.2142
47. Jeter JM, Han J, Martinez ME, Alberts DS, Qureshi AA, Feskanich D. Non-steroidal anti- inflammatory drugs, acetaminophen, and risk of skin cancer in the nurses’ health study. Cancer Causes Control. 2012;23(9):1451–1461. doi:10.1007/s10552-012-0019-6
48. Asgari MM, Chren MM, Warton EM, Friedman GD, White E. Association between nonsteroidal anti-inflammatory drug use and cutaneous squamous cell carcinoma. Arch Dermatol. 2010;146(4):388–395. doi:10.1001/archdermatol.2009.374
49. Torti DC, Christensen BC, Storm CA, et al. Analgesic and nonsteroidal anti-inflammatory use in relation to nonmelanoma skin cancer: a population-based case-control study. J Am Acad Dermatol. 2011;65(2):304–312. doi:10.1016/j.jaad.2010.05.042
50. Johannesdottir SA, Chang ET, Mehnert F, Schmidt M, Olesen AB, Sorensen HT. Nonsteroidal anti-inflammatory drugs and the risk of skin cancer: a population-based case-control study. Cancer. 2012;118(19):4768–4776. doi:10.1002/cncr.27406
51. Butler GJ, Neale R, Green AC, Pandeya N, Whiteman DC. Nonsteroidal anti- inflammatory drugs and the risk of actinic keratoses and squamous cell cancers of the skin. J Am Acad Dermatol. 2005;53(6):966–972. doi:10.1016/j.jaad.2005.05.049
52. Grau MV, Baron JA, Langholz B, et al. Effect of NSAIDs on the recurrence of nonmelanoma skin cancer. Int J Cancer. 2006;119(3):682–686. doi:10.1002/ijc.21878
53. Muranushi C, Olsen CM, Pandeya N, Green AC. Aspirin and nonsteroidal anti- inflammatory drugs can prevent cutaneous squamous cell carcinoma: a systematic review and meta-analysis. J Invest Dermatol. 2015;135(4):975–983. doi:10.1038/jid.2014.531
54. Schjerning AM, McGettigan P, Gislason G. Cardiovascular effects and safety of (non- aspirin) NSAIDs. Nat Rev Cardiol. 2020;17(9):574–584. doi:10.1038/s41569-020-0366-z
55. Koehl GE, Andrassy J, Guba M, et al. Rapamycin protects allografts from rejection while simultaneously attacking tumors in immunosuppressed mice. Transplantation. 2004;77(9):1319–1326. doi:10.1097/00007890-200405150-00002
56. Karia PS, Azzi JR, Heher EC, Hills VM, Schmults CD. Association of sirolimus use with risk for skin cancer in a mixed-organ cohort of solid-organ transplant recipients with a history of cancer. JAMA Dermatol. 2016;152(5):533–540. doi:10.1001/jamadermatol.2015.5548
57. Euvrard S, Morelon E, Rostaing L, et al. Sirolimus and secondary skin-cancer prevention in kidney transplantation. N Engl J Med. 2012;367(4):329–339. doi:10.1056/NEJMoa1204166
58. Campbell SB, Walker R, Tai SS, Jiang Q, Russ GR. Randomized controlled trial of sirolimus for renal transplant recipients at high risk for nonmelanoma skin cancer. Am J Transplant. 2012;12(5):1146–1156. doi:10.1111/j.1600-6143.2012.04004.x
59. Asgari MM, Arron ST, Warton EM, Quesenberry CP
60. Salgo R, Gossmann J, Schofer H, et al. Switch to a sirolimus-based immunosuppression in long-term renal transplant recipients: reduced rate of (pre-)malignancies and nonmelanoma skin cancer in a prospective, randomized, assessor-blinded, controlled clinical trial. Am J Transplant. 2010;10(6):1385–1393. doi:10.1111/j.1600-6143.2009.02997.x
61. Alberu J, Pascoe MD, Campistol JM, et al. Lower malignancy rates in renal allograft recipients converted to sirolimus-based, calcineurin inhibitor-free immunotherapy: 24- month results from the CONVERT trial. Transplantation. 2011;92(3):303–310. doi:10.1097/TP.0b013e3182247ae2
62. Campistol JM, Eris J, Oberbauer R, et al. Sirolimus therapy after early cyclosporine withdrawal reduces the risk for cancer in adult renal transplantation. J Am Soc Nephrol. 2006;17(2):581–589. doi:10.1681/ASN.2005090993
63. Hoogendijk-van den Akker JM, Harden PN, Hoitsma AJ, et al. Two-year randomized controlled prospective trial converting treatment of stable renal transplant recipients with cutaneous invasive squamous cell carcinomas to sirolimus. J Clin Oncol. 2013;31(10):1317–1323. doi:10.1200/JCO.2012.45.6376
64. Tedesco-Silva H, Peddi VR, Sanchez-Fructuoso A, et al. Open-label, randomized study of transition from tacrolimus to sirolimus immunosuppression in renal allograft recipients. Transplant Direct. 2016;2(4):e69. doi:10.1097/TXD.0000000000000579
65. Nguyen LS, Vautier M, Allenbach Y, et al. Sirolimus and mTOR inhibitors: a review of side effects and specific management in solid organ transplantation. Drug Saf. 2019;42(7):813–825. doi:10.1007/s40264-019-00810-9
66. Manzia TM, Carmellini M, Todeschini P, et al. A 3-month, multicenter, randomized, open-label study to evaluate the impact on wound healing of the early (vs eelayed) introduction of everolimus in de novo kidney transplant recipients, with a follow-up evaluation at 12 months after transplant (NEVERWOUND study). Transplantation. 2020;104(2):374–386. doi:10.1097/TP.0000000000002851
67. Mabood Khalil MA, Al-Ghamdi SMG, Dawood US, et al. Mammalian target of rapamycin inhibitors and wound healing complications in kidney transplantation: old myths and new realities. J Transplant. 2022;2022:6255339. doi:10.1155/2022/6255339
68. Stevenson ML, Carucci J, Colegio OR. Skin cancer in transplant recipients: scientific retreat of the international immunosuppression and transplant skin cancer collaborative and skin care in organ transplant patients-Europe. Clin Transplant. 2019;33(12):e13736. doi:10.1111/ctr.13736
69. Barrios DM, Do MH, Phillips GS, et al. Immune checkpoint inhibitors to treat cutaneous malignancies. J Am Acad Dermatol. 2020;83(5):1239–1253. doi:10.1016/j.jaad.2020.03.131
70. Migden MR, Rischin D, Schmults CD, et al. PD-1 blockade with cemiplimab in advanced cutaneous squamous-cell carcinoma. N Engl J Med. 2018;379(4):341–351. doi:10.1056/NEJMoa1805131
71. Migden MR, Khushalani NI, Chang ALS, et al. Cemiplimab in locally advanced cutaneous squamous cell carcinoma: results from an open-label, phase 2, single-arm trial. Lancet Oncol. 2020;21(2):294–305. doi:10.1016/S1470-2045(19)30728-4
72. Gross ND, Miller DM, Khushalani NI, et al. Neoadjuvant cemiplimab for stage II to IV cutaneous squamous-cell carcinoma. N Engl J Med. 2022;387(17):1557–1568. doi:10.1056/NEJMoa2209813
73. Gross N, Miller DM, Khushanlani N, et al. 789O - neoadjuvant cemiplimab in patients (pts) with stage II–IV (M0) cutaneous squamous cell carcinoma (CSCC): primary analysis of a phase II study. N Engl J Med. 2022;387(17):1557–1568. doi:10.1056/NEJMoa2209813
74. Rischin D, Migden MR, Lim AM, et al. Phase 2 study of cemiplimab in patients with metastatic cutaneous squamous cell carcinoma: primary analysis of fixed-dosing, long- term outcome of weight-based dosing. J Immunother Cancer. 2020;8(1). doi:10.1136/jitc-2020-000775
75. Prescribing information: cemiplimab Libtayo [package insert] Tarrytown, NY: Regeneron Pharmaceuticals, Inc. 2019.
76. Stratigos AJ, Sekulic A, Peris K, et al. Cemiplimab in locally advanced basal cell carcinoma after hedgehog inhibitor therapy: an open-label, multi-centre, single-arm, phase 2 trial. Lancet Oncol. 2021;22(6):848–857. doi:10.1016/S1470-2045(21)00126-1
77. Sekulic A, Migden MR, Oro AE, et al. Efficacy and safety of vismodegib in advanced basal-cell carcinoma. N Engl J Med. 2012;366(23):374–386. doi:10.1056/NEJMoa1113713
78. Wysong A, Aasi SZ, Tang JY. Update on metastatic basal cell carcinoma: a summary of published cases from 1981 through 2011. JAMA Dermatol. 2013;149(5):341–351. doi:10.1001/jamadermatol.2013.3064
79. Food and Drug Administration. FDA approves pembrolizumab for cutaneous squamous cell carcinoma. Available from: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pembrolizumab-cutaneous-squamous-cell-carcinoma.
80. Maubec E, Boubaya M, Petrow P, et al. Phase II study of pembrolizumab as first-line, single-drug therapy for patients with unresectable cutaneous squamous cell carcinomas. J Clin Oncol. 2020;38(26):3051–3061. doi:10.1200/JCO.19.03357
81. Hughes BGM, Munoz-Couselo E, Mortier L, et al. Pembrolizumab for locally advanced and recurrent/metastatic cutaneous squamous cell carcinoma (KEYNOTE-629 study): an open-label, nonrandomized, multicenter, phase II trial. Ann Oncol. 2021;32(10):1276–1285. doi:10.1016/j.annonc.2021.07.008
82. Grob JJ, Gonzalez R, Basset-Seguin N, et al. Pembrolizumab monotherapy for recurrent or metastatic cutaneous squamous cell carcinoma: a single-arm phase II trial (KEYNOTE-629). J Clin Oncol. 2020;38(25):2916–2925. doi:10.1200/JCO.19.03054
83. Keytruda® (pembrolizumab) [package insert]. Whitehouse Station, NY: Merck & Co., Inc.; 2014.
84. García-Sancha N, Corchado-Cobos R, Bellido-Hernández L, et al. Overcoming resistance to immunotherapy in advanced cutaneous squamous cell carcinoma. Cancers. 2021;13(20):5134. doi:10.3390/cancers13205134
85. Tawbi HA, Schadendorf D, Lipson EJ, et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. 2022;386(1):24–34. doi:10.1056/NEJMoa2109970
86. Cowey CL, Robert NJ, Davies K, et al. Treatment patterns and outcomes among patients with advanced cutaneous squamous cell carcinoma (CSCC) in a US community oncology setting. J Clin Oncol. 2019;37(15_suppl):e21033. doi:10.1200/JCO.2019.37.15_suppl.e21033
87. Kim JYS, Kozlow JH, Mittal B, et al. Guidelines of care for the management of cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78(3):560–578. doi:10.1016/j.jaad.2017.10.007
88. Ferrarotto R, Amit M, Nagarajan P, et al. Pilot phase II trial of neoadjuvant immunotherapy in locoregionally advanced, resectable cutaneous squamous cell carcinoma of the head and neck. Clin Cancer Res. 2021;27(16):4557–4565. doi:10.1158/1078-0432.CCR-21-0585
89. Lavaud J, Blom A, Longvert C, Fort M, Funck-Brentano E, Saiag P. Pembrolizumab and concurrent hypo-fractionated radiotherapy for advanced non-resectable cutaneous squamous cell carcinoma. Eur J Dermatol. 2019;29(6):636–640. doi:10.1684/ejd.2019.3671
90. Lipson EJ, Bagnasco SM, Moore J
91. Wolverton SE. Topical retinoids. In: Wu JJ, editor. Comprehensive Dermatologic Drug Therapy.
92. Jones DA. The potential immunomodulatory effects of topical retinoids. Dermatol Online J. 2005;11(1):3.
93. Kligman A, Thorne E. Retinoids in cutaneous malignancy. Blackwell Scientific Publications. 1991;4:66.
94. Kang S, Goldfarb MT, Weiss JS, et al. Assessment of adapalene gel for the treatment of actinic keratoses and lentigines: a randomized trial. J Am Acad Dermatol. 2003;49(1):83–90. doi:10.1067/mjd.2003.451
95. Bercovitch L. Topical chemotherapy of actinic keratoses of the upper extremity with tretinoin and 5-fluorouracil: a double-blind controlled study. Br J Dermatol. 1987;116(4):549–552. doi:10.1111/j.1365-2133.1987.tb05876.x
96. Prens SP, de Vries K, Neumann HA, Prens EP. Non-ablative fractional resurfacing in combination with topical tretinoin cream as a field treatment modality for multiple actinic keratosis: a pilot study and a review of other field treatment modalities. J Dermatolog Treat. 2013;24(3):227–231. doi:10.3109/09546634.2012.687088
97. Weinstock MA, Bingham SF, Digiovanna JJ, et al. Tretinoin and the prevention of keratinocyte carcinoma (Basal and squamous cell carcinoma of the skin): a veterans affairs randomized chemoprevention trial. J Invest Dermatol. 2012;132(6):1583–1590. doi:10.1038/jid.2011.483
98. Tang JY, Chiou AS, Mackay-Wiggan JM, et al. Tazarotene: randomized, double-blind, vehicle-controlled, and open-label concurrent trials for basal cell carcinoma prevention and therapy in patients with basal cell nevus syndrome. Cancer Prev Res. 2014;7(3):292–299. doi:10.1158/1940-6207.CAPR-13-0305
99. Micali G, Lacarrubba F, Dinotta F, Massimino D, Nasca MR. Treating skin cancer with topical cream. Expert Opin Pharmacother. 2010;11(9):1515–1527. doi:10.1517/14656566.2010.481284
100. Micali G, Lacarrubba F, Nasca MR, Ferraro S, Schwartz RA. Topical pharmacotherapy for skin cancer: part II. Clinical applications. J Am Acad Dermatol. 2014;70(6):979e1–12; quiz 9912. doi:10.1016/j.jaad.2013.12.037
101. Micali G, Lacarrubba F, Nasca MR, Schwartz RA. Topical pharmacotherapy for skin cancer: part I. Pharmacology. J Am Acad Dermatol. 2014;70(6):965e1-12; quiz 977–8. doi:10.1016/j.jaad.2013.12.045
102. Longley DB, Harkin DP, Johnston PG. 5-fluorouracil: mechanisms of action and clinical strategies. Nat Rev Cancer. 2003;3(5):330–338. doi:10.1038/nrc1074
103. Rosenberg AR, Tabacchi M, Ngo KH, et al. Skin cancer precursor immunotherapy for squamous cell carcinoma prevention. JCI Insight. 2019;4(6). doi:10.1172/jci.insight.125476
104. Nashan D, Meiss F, Muller M. Therapeutic strategies for actinic keratoses--a systematic review. Eur J Dermatol. 2013;23(1):14–32. doi:10.1684/ejd.2013.1923
105. Kurwa HA, Yong-Gee SA, Seed PT, Markey AC, Barlow RJ. A randomized paired comparison of photodynamic therapy and topical 5-fluorouracil in the treatment of actinic keratoses. J Am Acad Dermatol. 1999;41(3 Pt 1):414–418. doi:10.1016/s0190-9622(99)70114-3
106. Witheiler DD, Lawrence N, Cox SE, Cruz C, Cockerell CJ, Freemen RG. Long-term efficacy and safety of Jessner’s solution and 35% trichloroacetic acid vs 5% fluorouracil in the treatment of widespread facial actinic keratoses. Dermatol Surg. 1997;23(3):191–196. doi:10.1111/j.1524-4725.1997.tb00020.x
107. Pomerantz H, Hogan D, Eilers D, et al. Long-term efficacy of topical fluorouracil cream, 5%, for treating actinic keratosis: a randomized clinical trial. JAMA Dermatol. 2015;151(9):952–960. doi:10.1001/jamadermatol.2015.0502
108. Rahvar M, Lamel SA, Maibach HI. Randomized, vehicle-controlled trials of topical 5- fluorouracil therapy for actinic keratosis treatment: an overview. Immunotherapy. 2012;4(9):939–945. doi:10.2217/imt.12.93
109. Cunningham TJ, Tabacchi M, Eliane JP, et al. Randomized trial of calcipotriol combined with 5-fluorouracil for skin cancer precursor immunotherapy. J Clin Invest. 2017;127(1):106–116. doi:10.1172/JCI89820
110. Mohney L, Singh R, Grada A, Feldman S. Use of topical calcipotriol plus 5-fluorouracil in the treatment of actinic keratosis: a systematic review. J Drugs Dermatol. 2022;21(1):60–65. doi:10.36849/JDD.2022.66321
111. Moore AY, Nguyen M, Moore S. Cyclic calcipotriene 0.005% foam and 1% 5- fluorouracil cream after cryotherapy in treatment of hyperkeratotic actinic keratosis: a retrospective study. J Am Acad Dermatol. 2021;84(4):1148–1150. doi:10.1016/j.jaad.2020.07.010
112. Teresa Sarandeses Diez M, Caral Vanaclocha I, Lemaitre S, Gonzalez Candial M. Topical treatment with calcipotriol combined with 5-fluorouracil for premalignant periocular lesions. J Fr Ophtalmol. 2021;44(1):e27–e29. doi:10.1016/j.jfo.2020.04.030
113. Love WE, Bernhard JD, Bordeaux JS. Topical imiquimod or fluorouracil therapy for basal and squamous cell carcinoma: a systematic review. Arch Dermatol. 2009;145(12):1431–1438. doi:10.1001/archdermatol.2009.291
114. Gross K, Kircik L, Kricorian G. 5% 5-fluorouracil cream for the treatment of small superficial basal cell carcinoma: efficacy, tolerability, cosmetic outcome, and patient satisfaction. Dermatol Surg. 2007;33(4):433–9; discussion 440. doi:10.1111/j.1524-4725.2007.33090.x
115. Bargman H, Hochman J. Topical treatment of bowen’s disease with 5-fluorouracil. J Cutan Med Surg. 2003;7(2):101–105. doi:10.1007/s10227-002-0158-6
116. Algarin YA, Jambusaria-Pahlajani A, Ruiz E, Patel VA. Advances in topical treatments of cutaneous malignancies. Am J Clin Dermatol. 2022. doi:10.1007/s40257-022-00731-x
117. Gupta AK, Paquet M, Villanueva E, Brintnell W. Interventions for actinic keratoses. Cochrane Database Syst Rev. 2012;12:CD004415. doi:10.1002/14651858.CD004415.pub2
118. Wolverton SE. Topical and intralesional antiviral agents. In: Wu JJ, editor. Comprehensive Dermatologic Drug Therapy.
119. Geisse J, Caro I, Lindholm J, Golitz L, Stampone P, Owens M. Imiquimod 5% cream for the treatment of superficial basal cell carcinoma: results from two phase III, randomized, vehicle-controlled studies. J Am Acad Dermatol. 2004;50(5):722–733. doi:10.1016/j.jaad.2003.11.066
120. Geisse JK, Rich P, Pandya A, et al. Imiquimod 5% cream for the treatment of superficial basal cell carcinoma: a double-blind, randomized, vehicle-controlled study. J Am Acad Dermatol. 2002;47(3):390–398. doi:10.1067/mjd.2002.126215
121. Schulze HJ, Cribier B, Requena L, et al. Imiquimod 5% cream for the treatment of superficial basal cell carcinoma: results from a randomized vehicle-controlled Phase III study in Europe. Br J Dermatol. 2005;152(5):939–947. doi:10.1111/j.1365-2133.2005.06486.x
122. Roozeboom MH, Arits AH, Nelemans PJ, Kelleners-Smeets NW. Overall treatment success after treatment of primary superficial basal cell carcinoma: a systematic review and meta-analysis of randomized and nonrandomized trials. Br J Dermatol. 2012;167(4):733–756. doi:10.1111/j.1365-2133.2012.11061.x
123. Shumack S, Robinson J, Kossard S, et al. Efficacy of topical 5% imiquimod cream for the treatment of nodular basal cell carcinoma: comparison of dosing regimens. Arch Dermatol. 2002;138(9):1165–1171. doi:10.1001/archderm.138.9.1165
124. Warshauer E, Warshauer BL. Clearance of basal cell and superficial squamous cell carcinomas after imiquimod therapy. J Drugs Dermatol. 2008;7(5):447–451.
125. Rosen T, Harting M, Gibson M. Treatment of bowen’s disease with topical 5% imiquimod cream: retrospective study. Dermatol Surg. 2007;33(4):427–31;discussion 431–2. doi:10.1111/j.1524-4725.2007.33089.x
126. Mackenzie-Wood A, Kossard S, de Launey J, Wilkinson B, Owens ML. Imiquimod 5% cream in the treatment of bowen’s disease. J Am Acad Dermatol. 2001;44(3):462–470. doi:10.1067/mjd.2001.111335
127. Chitwood K, Etzkorn J, Cohen G. Topical and intralesional treatment of nonmelanoma skin cancer: efficacy and cost comparisons. Dermatol Surg. 2013;39(9):1306–1316. doi:10.1111/dsu.12300
128. Patel GK, Goodwin R, Chawla M, et al. Imiquimod 5% cream monotherapy for cutaneous squamous cell carcinoma in situ (Bowen’s disease): a randomized, double-blind, placebo-controlled trial. J Am Acad Dermatol. 2006;54(6):1025–1032. doi:10.1016/j.jaad.2006.01.055
129. Smith KJ, Germain M, Skelton H. Squamous cell carcinoma in situ (Bowen’s disease) in renal transplant patients treated with 5% imiquimod and 5% 5-fluorouracil therapy. Dermatol Surg. 2001;27(6):561–564. doi:10.1046/j.1524-4725.2001.00149.x
130. Smith KJ, Germain M, Skelton H. Bowen’s disease (squamous cell carcinoma in situ) in immunosuppressed patients treated with imiquimod 5% cream and a cox inhibitor, sulindac: potential applications for this combination of immunotherapy. Dermatol Surg. 2001;27(2):143–146. doi:10.1046/j.1524-4725.2001.00199.x
131. Stockfleth E, Sterry W, Carey-Yard M, Bichel J. Multicentre, open-label study using imiquimod 5% cream in one or two 4-week courses of treatment for multiple actinic keratoses on the head. Br J Dermatol. 2007;157(Suppl 2):41–46. doi:10.1111/j.1365-2133.2007.08272.x
132. Lebwohl M, Dinehart S, Whiting D, et al. Imiquimod 5% cream for the treatment of actinic keratosis: results from two phase III, randomized, double-blind, parallel group, vehicle- controlled trials. J Am Acad Dermatol. 2004;50(5):714–721. doi:10.1016/j.jaad.2003.12.010
133. Szeimies RM, Gerritsen MJ, Gupta G, et al. Imiquimod 5% cream for the treatment of actinic keratosis: results from a phase III, randomized, double-blind, vehicle-controlled, clinical trial with histology. J Am Acad Dermatol. 2004;51(4):547–555. doi:10.1016/j.jaad.2004.02.022
134. Alomar A, Bichel J, McRae S. Vehicle-controlled, randomized, double-blind study to assess safety and efficacy of imiquimod 5% cream applied once daily 3 days per week in one or two courses of treatment of actinic keratoses on the head. Br J Dermatol. 2007;157(1):133–141. doi:10.1111/j.1365-2133.2007.07942.x
135. Peris K, Campione E, Micantonio T, Marulli GC, Fargnoli MC, Chimenti S. Imiquimod treatment of superficial and nodular basal cell carcinoma: 12-week open-label trial. Dermatol Surg. 2005;31(3):318–323. doi:10.1111/j.1524-4725.2005.31081
136. Eigentler TK, Kamin A, Weide BM, et al. A phase III, randomized, open label study to evaluate the safety and efficacy of imiquimod 5% cream applied thrice weekly for 8 and 12 weeks in the treatment of low-risk nodular basal cell carcinoma. J Am Acad Dermatol. 2007;57(4):616–621. doi:10.1016/j.jaad.2007.05.022
137. Samorano LP, Torezan LA, Sanches JA. Evaluation of the tolerability and safety of a 0.015% ingenol mebutate gel compared to 5% 5-fluorouracil cream for the treatment of facial actinic keratosis: a prospective randomized trial. J Eur Acad Dermatol Venereol. 2015;29(9):1822–1827. doi:10.1111/jdv.13063
138. Rosen RH, Gupta AK, Tyring SK. Dual mechanism of action of ingenol mebutate gel for topical treatment of actinic keratoses: rapid lesion necrosis followed by lesion-specific immune response. J Am Acad Dermatol. 2012;66(3):486–493. doi:10.1016/j.jaad.2010.12.038
139. Amini S, Viera MH, Valins W, Berman B. Nonsurgical innovations in the treatment of nonmelanoma skin cancer. J Clin Aesthet Dermatol. 2010;3(6):20–34.
140. Siller G, Gebauer K, Welburn P, Katsamas J, Ogbourne SM. PEP005 (ingenol mebutate) gel, a novel agent for the treatment of actinic keratosis: results of a randomized, double-blind, vehicle-controlled, multicentre, phase IIa study. Australas J Dermatol. 2009;50(1):16–22. doi:10.1111/j.1440-0960.2008.00497.x
141. Siller G, Rosen R, Freeman M, Welburn P, Katsamas J, Ogbourne SM. PEP005 (ingenol mebutate) gel for the topical treatment of superficial basal cell carcinoma: results of a randomized phase IIa trial. Australas J Dermatol. 2010;51(2):99–105. doi:10.1111/j.1440-0960.2010.00626.x
142. Lebwohl M, Swanson N, Anderson LL, Melgaard A, Xu Z, Berman B. Ingenol mebutate gel for actinic keratosis. N Engl J Med. 2012;366(11):1010–1019. doi:10.1056/NEJMoa1111170
143. Anderson L, Schmieder GJ, Werschler WP, et al. Randomized, double-blind, double- dummy, vehicle-controlled study of ingenol mebutate gel 0.025% and 0.05% for actinic keratosis. J Am Acad Dermatol. 2009;60(6):934–943. doi:10.1016/j.jaad.2009.01.008
144. European Medicines Agency. Risks of picato for actinic keratosis outweigh benefits. Available from: https://www.ema.europa.eu/en/medicines/human/referrals/picato.
145. Chabbert C, Levy M, Legrand L. Carcinome épidermoïde cutané multiple après traitement par le mébutate d'ingénol [Multiple cutaneous squamous cell carcinoma after treatment with ingenol mebutate]. Ann Dermatol Venereol. 2019;146(12):823–825. French. doi:10.1016/j.annder.2019.08.005
146. McEwan LE, Smith JG. Topical diclofenac/hyaluronic acid gel in the treatment of solar keratoses. Australas J Dermatol. 1997;38(4):187–189. doi:10.1111/j.1440-0960.1997.tb01693.x
147. Rivers JK, Arlette J, Shear N, Guenther L, Carey W, Poulin Y. Topical treatment of actinic keratoses with 3.0% diclofenac in 2.5% hyaluronan gel. Br J Dermatol. 2002;146(1):94–100. doi:10.1046/j.1365-2133.2002.04561.x
148. Gebauer K, Brown P, Varigos G. Topical diclofenac in hyaluronan gel for the treatment of solar keratoses. Australas J Dermatol. 2003;44(1):40–43. doi:10.1046/j.1440-0960.2002.00635.x
149. Zeitouni NC, Bhatia N, Ceilley RI, et al. Photodynamic therapy with 5-aminolevulinic acid 10% gel and red light for the treatment of actinic keratosis, nonmelanoma skin cancers, and acne: current evidence and best practices. J Clin Aesthet Dermatol. 2021;14(10):E53–E65.
150. Qiang YG, Yow CM, Huang Z. Combination of photodynamic therapy and immunomodulation: current status and future trends. Med Res Rev. 2008;28(4):632–644. doi:10.1002/med.20121
151. Jeffes EW, McCullough JL, Weinstein GD, Kaplan R, Glazer SD, Taylor JR. Photodynamic therapy of actinic keratoses with topical aminolevulinic acid hydrochloride and fluorescent blue light. J Am Acad Dermatol. 2001;45(1):96–104. doi:10.1067/mjd.2001.114288
152. Piacquadio DJ, Chen DM, Farber HF, et al. Photodynamic therapy with aminolevulinic acid topical solution and visible blue light in the treatment of multiple actinic keratoses of the face and scalp: investigator-blinded, phase 3, multicenter trials. Arch Dermatol. 2004;140(1):41–46. doi:10.1001/archderm.140.1.41
153. Lee PK, Kloser A. Current methods for photodynamic therapy in the US: comparison of MAL/PDT and ALA/PDT. J Drugs Dermatol. 2013;12(8):925–930.
154. Moloney FJ, Collins P. Randomized, double-blind, prospective study to compare topical 5-aminolaevulinic acid methylester with topical 5-aminolaevulinic acid photodynamic therapy for extensive scalp actinic keratosis. Br J Dermatol. 2007;157(1):87–91. doi:10.1111/j.1365-2133.2007.07946.x
155. Szeimies RM, Matheson RT, Davis SA, et al. Topical methyl aminolevulinate photodynamic therapy using red light-emitting diode light for multiple actinic keratoses: a randomized study. Dermatol Surg. 2009;35(4):586–592. doi:10.1111/j.1524-4725.2009.01096.x
156. Togsverd-Bo K, Omland SH, Wulf HC, Sørensen SS, Haedersdal M. Primary prevention of skin dysplasia in renal transplant recipients with photodynamic therapy: a randomized controlled trial. Am J Transplant. 2015;15(11):2986–2990. doi:10.1111/ajt.13358
157. de Graaf YG, Kennedy C, Wolterbeek R, Collen AF, Willemze R, Bouwes Bavinck JN. Photodynamic therapy does not prevent cutaneous squamous-cell carcinoma in organ- transplant recipients: results of a randomized-controlled trial. J Invest Dermatol. 2006;126(3):569–574. doi:10.1038/sj.jid.5700098
158. Kuijpers DI, Thissen MR, Thissen CA, Neumann MH. Similar effectiveness of methyl aminolevulinate and 5-aminolevulinate in topical photodynamic therapy for nodular basal cell carcinoma. J Drugs Dermatol. 2006;5(7):642–645.
159. Foley P, Freeman M, Menter A, et al. Photodynamic therapy with methyl aminolevulinate for primary nodular basal cell carcinoma: results of two randomized studies. Int J Dermatol. 2009;48(11):1236–1245. doi:10.1111/j.1365-4632.2008.04022.x
160. de Haas ER, Sterenborg HJ, Neumann HA, Robinson DJ. Response of bowen disease to ALA-PDT using a single and a 2-fold illumination scheme. Arch Dermatol. 2007;143(2):264–265. doi:10.1001/archderm.143.2.264
161. Salim A, Leman JA, McColl JH, Chapman R, Morton CA. Randomized comparison of photodynamic therapy with topical 5-fluorouracil in bowen’s disease. Br J Dermatol. 2003;148(3):539–543. doi:10.1046/j.1365-2133.2003.05033.x
162. Willey A, Mehta S, Lee PK. Reduction in the incidence of squamous cell carcinoma in solid organ transplant recipients treated with cyclic photodynamic therapy. Dermatol Surg. 2010;36(5):652–658. doi:10.1111/j.1524-4725.2009.01384.x
163. Hall ET, Fernandez-Lopez E, Silk AW, Dummer R, Bhatia S. Immunologic characteristics of nonmelanoma skin cancers: implications for immunotherapy. Am Soc Clin Oncol Educ Book. 2020;40:1–10. doi:10.1200/EDBK_278953
164. Nelson CG. Diclofenac gel in the treatment of actinic keratoses. Ther Clin Risk Manag. 2011;7:207–211. doi:10.2147/TCRM.S12498
165. Food and Drug Administration. FDA drug safety communication: FDA warns of severe adverse events with application of Picato (ingenol mebutate) gel for skin condition; requires label changes. Available from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-warns-severe-adverse-events-application-picato-ingenol-mebutate.
166. Trager MH, Geskin LJ, Samie FH, Liu L. Biomarkers in melanoma and non-melanoma skin cancer prevention and risk stratification. Exp Dermatol. 2022;31(1):4–12. doi:10.1111/exd.14114
167. Jung JW, Overgaard NH, Burke MT, et al. Does the nature of residual immune function explain the differential risk of non-melanoma skin cancer development in immunosuppressed organ transplant recipients? Int J Cancer. 2016;138(2):281–292. doi:10.1002/ijc.29450
168. National Cancer Institute. Cemiplimab-rwlc. U.S. Department of Health and Human Services, National Institute of Health. Available from: https://www.cancer.gov/about-cancer/treatment/drugs/cemiplimab-rwlc.
169. National Cancer Institute. Fluorouracil (Topical). U.S. Department of Health and Human Services, National Institute of Health. Available from: https://www.cancer.gov/about-cancer/treatment/drugs/fluorouracil-topical.
170. National Cancer Institute. Imiquimod. U.S. Department of Health and Human Services, National Institutes of Health. Available from: https://www.cancer.gov/about-cancer/treatment/drugs/imiquimod.
171. Alchin DR. Ingenol mebutate: a succinct review of a succinct therapy. Dermatol Ther. 2014;4(2):157–164. doi:10.1007/s13555-014-0061-2
172. American Cancer Society medical and editorial content team. Getting photodynamic therapy. American Cancer Society. Available from: https://www.cancer.org/treatment/treatments-and-side-effects/treatmenttypes/radiation/photodynamictherapy.html#:~:text=PDT%20drugs%20approved%20in%20the%20US%20to%20treat%20cancer&text=It’s%20activated%20by%20red%20light,in%20other%20types%20of%20cancer.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Misdiagnosis of Cutaneous Malignant Tumors as Melanocytic Nevi or Seborrheic Keratosis: A Retrospective Analysis of a Chinese Population
Zhang J, Wang Y, Zhang W, Cai L, Feng J, Zhu Y, Lu H
Clinical, Cosmetic and Investigational Dermatology 2024, 17:465-476
Published Date: 26 February 2024
Epidemiological and Pathological Trends in Skin Cancer: A Hands-On Analysis of 10 Years of Data from the Saudi Cancer Registry
Alqirnas MQ, Arkoubi AY, Alshabnan R, Almughira AI, Alhamadh M, Aldaghri FA, Mortada H, Daghistani W
Cancer Management and Research 2025, 17:2487-2502
Published Date: 27 October 2025