Back to Journals » Journal of Inflammation Research » Volume 18
Immune Response to TB Antigen Stimulation in Type 2 Diabetes Mellitus: Insights from a Cross-Sectional Cytokine Profile Analysis
Authors Soetedjo NNM ![]() , Koesoemadinata RC, Rahmadika N, Indrati AR
, Koesoemadinata RC, Rahmadika N, Indrati AR ![]() , Mudjanarko SW, Permana H, Alisjahbana B, Parwati I
, Mudjanarko SW, Permana H, Alisjahbana B, Parwati I ![]()
Received 28 August 2025
Accepted for publication 21 November 2025
Published 22 December 2025 Volume 2025:18 Pages 17997—18008
DOI https://doi.org/10.2147/JIR.S559756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Quan Zhang
Nanny Natalia Mulyani Soetedjo,1 Raspati Cundarani Koesoemadinata,2 Nofri Rahmadika,3 Agnes Rengga Indrati,4 Sony Wibisono Mudjanarko,5 Hikmat Permana,6 Bachti Alisjahbana,7 Ida Parwati4
1Department of Internal Medicine, Faculty of Medicine, Universitas Padjadjaran, Dr Hasan Sadikin General Hospital, Bandung, Indonesia; 2Research Center for Care and Control of Infectious Disease, Universitas Padjadjaran, Bandung, Indonesia; 3Department of Microbiology, Faculty of Medicine, Universitas Andalas, Padang, Indonesia; 4Department of Clinical Pathology, Faculty of Medicine, Universitas Padjadjaran, Dr Hasan Sadikin General Hospital, Bandung, Indonesia; 5Department of Internal Medicine, Faculty of Medicine, Universitas Airlangga, Dr Soetomo General Hospital, Surabaya, Indonesia; 6Division of Endocrinology and Metabolism, Department of Internal Medicine, Faculty of Medicine, Universitas Padjadjaran, Hasan Sadikin General Hospital, Bandung, Indonesia; 7Division of Tropical Medicine and Infectious Disease, Department of Internal Medicine, Faculty of Medicine, Universitas Padjadjaran, Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Nanny Natalia Mulyani Soetedjo, Department of Internal Medicine, Faculty of Medicine, Universitas Padjadjaran – Dr Hasan Sadikin Hospital, Bandung, Indonesia, Email [email protected]
Purpose: The syndemic of tuberculosis (TB) and type 2 diabetes mellitus (T2DM) presents a growing global health challenge, particularly in high-burden countries. T2DM is known to impair immune responses, increasing susceptibility to TB. However, the cytokine dynamics underlying this interaction remain unclear. This study aimed to explore the differences in ex vivo cytokine responses between individuals with and without T2DM following TB antigen stimulation.
Patients and Methods: In this cross-sectional study, we analyzed plasma samples from 110 individuals with T2DM and 38 without, collected as part of the TANDEM and INFECT cohort studies in Indonesia. Cytokine levels (IL-1β, IL-6, TNF-α, and IFN-γ) were measured using ELISA before and after TB antigen stimulation using the QuantiFERON-TB Gold assay. Demographic, clinical, and metabolic parameters were recorded. Statistical analyses included Mann–Whitney U-tests and Spearman correlation.
Results: Patients with DM showed a higher baseline levels of pro-inflammatory cytokines than non-DM individuals, particularly in IL-1β, IL-6 and TNF-α, suggesting a primed immune response even before TB antigen exposure. After TB antigen stimulation, no significant between-group differences were observed in cytokine levels. However, IL-1β showed a more pronounced median increase in T2DM (124 vs – 54 pg/mL, p = 0.43), while IL-6, TNF-α, and IFN-γ changes were blunted in the T2DM group. Correlation analyses revealed that in T2DM individuals, IL-1β positively correlated with IL-6 and TNF-α both pre- and post-stimulation. IL-6 and IFN-γ showed significant associations with HbA1c and BMI in the non-DM group.
Conclusion: T2DM group exhibited altered immune patterns marked by heightened IL-1β response and disrupted regulation of IL-6, TNF-α, and IFN-γ, although no statistically significant cytokine differences were observed. These findings suggest an immune dysregulation in T2DM that may contribute to TB susceptibility, warranting further investigation using CD4/CD8-responsive assays in larger, more diverse populations.
Keywords: cytokines, chronic inflammation, diabetes mellitus, hyperglycemia, tuberculosis
Introduction
The coexistence of diabetes mellitus (DM) and tuberculosis (TB) resembles a “syndemic” as the two conditions intensify each other’s effects through a synergistic interaction. Individuals with T2DM have a two-to-four fold higher risk of developing active TB, which up to 30% of TB patients may also have diabetes, indicating a strong comorbidity and worse treatment outcomes once infected.1–3 Globally, the prevalence of type 2 diabetes mellitus (T2DM) among TB patients is estimated to be approximately 13.7–16%.4,5 Whereas in Asia, particularly in Indonesia, TB remains the leading cause of death from infectious diseases and the second-highest cause of overall mortality with approximately 1.06 million new TB cases and 134,000 deaths annually according to the WHO Global Tuberculosis Report 2024.6 At the same time, the prevalence of type 2 diabetes is rising sharply, with projections estimate an increase from 9.1 9% in 2020 to 16.09% in 2045, corresponding to nearly 40.7 million diabetes cases nationwide if current trends continue.7 Previous studies in Jakarta found that 13.2% of TB patients also had diabetes, highlighting the substantial overlap between these diseases.8 Combined, these figures illustrate a dual epidemic, making integrated management and prevention strategies essential to mitigate the public health impact of TB-DM comorbidity in Indonesia.9–11
The coexistence TB-DM highlights a bidirectional relationship in which each condition has the potential to worsen the other.12,13 Metabolic dysfunction in type 2 diabetes, including obesity, insulin resistance, and the accumulation of advanced glycation end-products (AGEs), contributes to chronic inflammation and immune dysregulation, thereby influencing host responses to infectious diseases such as tuberculosis.14,15 Alterations in both innate and adaptive immunity within an inflammatory environment may contribute to this cycle. DM can weaken immune defenses, increasing susceptibility to TB, while the inflammation associated with TB can disrupt blood sugar regulation in individuals with diabetes.16–20 Chronic inflammation plays a central role in the pathogenesis of both T2DM and TB. Low-grade systemic inflammation is a key factor in insulin resistance and beta-cell dysfunction, with elevated levels of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) commonly observed.21 Similarly, tuberculosis triggers a strong immune response, characterized by activation of macrophages and T-cells, and the release of inflammatory mediators like interferon-gamma (IFN-γ), IL-6 and interleukin-1β (IL-1β).22–24
Although the established relationship between DM and TB, biological mechanism underlying the relationship remains unclear. Ex vivo stimulation assays such as QuantiFERON have been widely used as immune monitoring tools in TB research, as they provide a clinically relevant model of antigen-specific immune responsiveness and enable the simultaneous measurement of multiple cytokines.25,26 Previous studies have reported altered cytokine profiles in diabetic patients, but findings have been inconsistent, and direct correlations between blood glucose levels and specific cytokine responses, particularly IL-1β, remain unclear.24,27 Notably, no consistent association has been established between glycemic status and IL-1β secretion after TB antigen exposure.20 Other research showed that dysregulated cytokine responses, such as impaired IFN-γ and excessive proinflammatory signaling, have been associated with increased susceptibility to TB progression and poorer treatment outcomes in individuals with diabetes.13,28
Recent systems immunology and transcriptomic analyses have provided a more holistic understanding of TB–DM comorbidity. These studies demonstrated that individuals with diabetes and tuberculosis exhibit altered expression of interferon signaling, inflammatory, and metabolic pathways, suggesting that immune dysfunction in TB–DM reflects a complex network-level alteration rather than isolated cytokine changes.29 This study provides novel insight by examining cytokine responses (IL-1β, IL-6, TNF-α, and IFN-γ) in diabetic and non-diabetic individuals, both before and after stimulation with TB antigens, using an ex vivo model. The findings contribute to a deeper understanding of how hyperglycemia may alter the host’s immune signaling pathways during TB infection, offering potential biomarkers or therapeutic targets for comorbid DM-TB management.
Materials and Methods
Study Design and Setting
This cross-sectional study utilized archived blood samples and data from two previous studies: the TANDEM study,30 which investigated the relationship between tuberculosis (TB) and diabetes mellitus (DM), and the INFECT study,31 which focused on TB household contacts. Diabetic participants were enrolled between December 2013 and February 2015 from 25 community health centers (CHCs) and the outpatient endocrine clinic at Dr. Hasan Sadikin General Hospital in Bandung, Indonesia, where they were screened for TB as part of the TANDEM study. TB patients were recruited from 45 CHCs and the hospital’s outpatient TB clinic between April 2014 and December 2017, and were screened for DM under the same study. Household contacts of TB patients initially enrolled in the TANDEM study were later included in the INFECT study through home visits conducted in Bandung City.
Informed written consent was obtained from all participants prior to enrollment. The TANDEM study received ethical approval from the Health Research Ethics Committee, Faculty of Medicine, Universitas Padjadjaran (Ref No: 05/UN6.C2.1.2/KEPK/PN/2014), as well as from the Research Ethics Committee of the London School of Hygiene and Tropical Medicine (LSHTM Ethics Ref: 6449; Amendment No: A473). The INFECT study was approved by the same Indonesian ethics committee (Ref No: 14/UN6.C2.1.2/KEPK/PN/2014) and by the Health and Disability Ethics Committees in New Zealand (Ref: 13/STH/132). This bioarchive-based study was also approved by the Health Research Ethics Committee at Universitas Padjadjaran (Ref No: 263/UN6.KEP/EC/2019). Ethical clearance for the utilization of archived biological specimens was granted by the Center for Clinical Infection Studies, Faculty of Medicine, Universitas Padjadjaran (Ref. No: 202/UN6.C.7.1/LT/2019). All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments.
Study Procedure
In this study, we focused on four cytokines—IL-1β, IL-6, TNF-α, and IFN-γ—because of their established roles as central proinflammatory mediators in both M. tuberculosis immunity and type 2 diabetes mellitus (T2DM)–associated immune dysregulation. These cytokines have been consistently reported as key markers of innate and adaptive immune responses in the TB–diabetes context, and their dysregulation may contribute to increased susceptibility and worse outcomes in patients with T2DM.17–19
Enrolment procedures for type 2 diabetes mellitus (T2DM) patients were previously reported.32 These individuals were screened for tuberculosis (TB) symptoms and underwent chest X-rays. If symptoms or radiological signs indicated potential TB, sputum samples were collected for microbiological testing. Blood samples were also drawn to perform routine hematological tests—including hemoglobin, white cell count, and differentials—and to conduct an IFN-γ release assay using the QuantiFERON-TB Gold test (QFT). The recruitment of non-diabetic participants was outlined in a more recent publication.31
The samples from DM patients who were 40 years or older and previously diagnosed with T2DM were included in this study. Samples from DM patients who had active pulmonary TB based on bacteriological or radiological examination and which haemoglobin concentration below normal value were excluded. Non-DM subjects were households of TB patients aged ≥40 years, with HbA1c levels <6.5% and no evidence of TB whose samples were available.
Out of 809 diabetic patients, 384 samples met the inclusion and exclusion criteria. Among these, 97 samples were excluded due to issues such as icterus, hemolysis, or insufficient volume (less than 200μL), resulting in 287 eligible samples. Following random selection, 148 participants were included in the final study, comprising 110 individuals with diabetes and 38 without diabetes.
The QuantiFERON-TB Gold Test (QFT)
For the QuantiFERON-TB (QFT) assay, approximately 4 mL of blood was collected from the cubital fossa into heparinized vacutainer tubes. Whole blood samples from selected individuals with type 2 diabetes and those without diabetes were incubated for 20 to 24 hours. Following incubation, plasma was separated, and interferon-gamma (IFN-γ) levels were measured using an enzyme-linked immunosorbent assay (ELISA) method. The assays were performed on plasma/serum/supernatant stored at −80°C and thawed once immediately prior to assay. Assay performance metrics (limit of detection, inter- and intra-assay variability) were added as recommended to ensure reproducibility. One tube served as a negative control (unstimulated), while another contained a peptide cocktail simulating the TB-specific antigens ESAT-6, CFP-10, and TB7.7. IFN-γ concentrations were calculated by subtracting the value from the unstimulated tube, and a threshold of 0.35 IU/mL was applied based on the manufacturer’s guidelines.26
The remaining plasma samples were frozen at −80°C in preparation for further cytokine investigations. Inadequate preserved samples, such as lysed, icteric, or lipemic samples were excluded from analysis. The levels of IL-1β, TNF-α (Human R&D systems), and IL-6 (Sanquin) released in response to antigen stimulation in the QFT cell-free culture supernatants of all samples were determined by ELISA.
HbA1C Measurements
Venous blood samples were analyzed using high-performance liquid chromatography (HPLC) with the Variant II Turbo system (Bio-Rad, USA) at a private diagnostic laboratory, namely “Prodia”. The equipment used is certified by both the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) and the National Glycohemoglobin Standardization Program (NGSP).
Data Collection and Statistical Analysis
Patients’ characteristics were obtained from TANDEM and INFECT electronic databases and merged with cytokines data. Data were presented as means and standard error of the mean or median (interquartile range), as appropriate. Differences in cytokine concentration were evaluated by unpaired t-test if data were normally distributed or the Mann–Whitney test if they were not normally distributed. The correlation between the two variables was analysed using Spearman’s rank correlation coefficient. Confidence intervals and p-values were used to determine statistical significance. A p-value of <0.05 was considered statistically significant. Graphs and statistical analyses were performed using Stata version 13.1 (StataCorp, College Station, TX, USA).
Results
Table 1 summarizes the clinical characteristics of the study participants, comparing individuals with diabetes mellitus (DM, n = 110) to those without diabetes (non-DM, n = 38). The groups were similar in terms of sex distribution (p = 0.40), history of tuberculosis (TB) (p = 0.38), current smoking status (p = 0.008), and positive IGRA results (p = 0.23). However, there were statistically significant differences in median age, BCG vaccination history, number of household members, and body mass index (BMI) distribution. DM participants were significantly older (median age: 58 vs 50 years, p = 0.0004) and more likely to have a BCG scar (67.3% vs 92.1%, p = 0.003). Regarding BMI, DM individuals had a higher proportion of obesity (BMI ≥25), particularly those classified as obese class I and II, compared to non-DM participants (p = 0.03). Median HbA1c among DM participants was 8.2% (IQR: 6.9–10.2), reflecting poor glycemic control. A variety of medications were reported among DM participants, with the most common being metformin (57.3%) and sulfonylureas (29.7%). These findings highlight key clinical and demographic differences between the DM and non-DM groups.
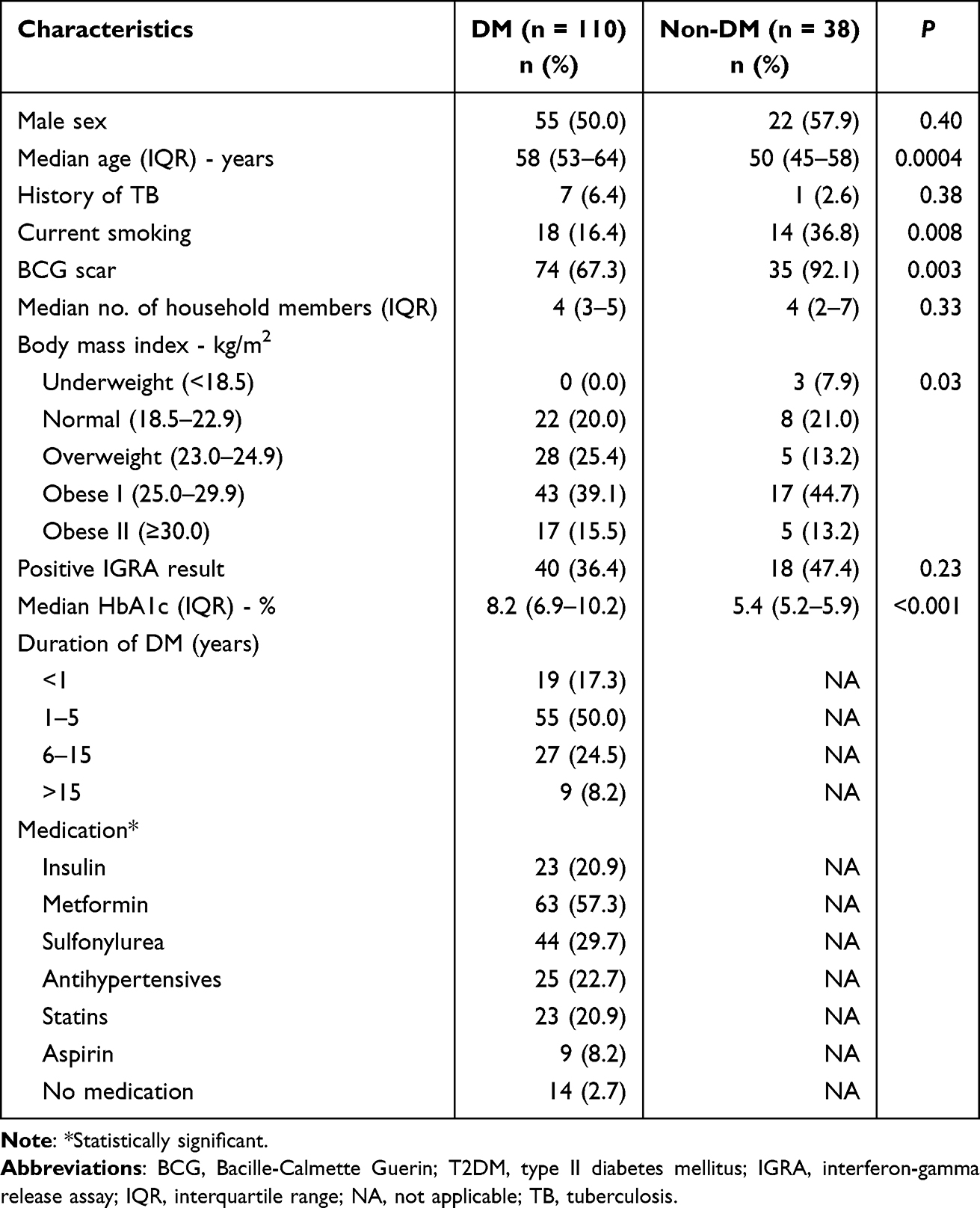 |
Table 1 Clinical Characteristics of the Participants |
Table 2 presents the laboratory findings of DM and non-DM participants. Compared to the non-DM group, participants with diabetes had significantly higher median haemoglobin levels (14.6 vs 14.2 g/dl, p = 0.1), neutrophil counts (5.9 vs 4.2/mm3, p < 0.001), monocyte counts (0.7 vs 0.5/mm3, p < 0.001), lymphocyte counts (3.1 vs 2.2/mm3, p = 0.0001) and leucocyte counts (8.100 vs 7.450/mm3, p = 0.09). Based on the cytokine profile comparison presented in Table 2, patients with DM showed a higher baseline levels of pro-inflammatory cytokines than non-DM individuals. After TB antigen stimulation, no statistically significant differences were observed between the DM and non-DM groups. Although the DM group demonstrated a greater median change in IL-1β levels after stimulation (124 pg/mL vs –54 pg/mL in non-DM), the difference remained statistically non-significant (p = 0.43). Additionally, the median changes in IL-6, IFN-γ, and TNF-α were all lower in the DM group compared to non-DM, but none reached statistical significance (all p > 0.05). These findings suggest possible differences in immune activation patterns among individuals with diabetes, potentially reflecting altered inflammatory or innate immune responses, despite the lack of statistically significant results. All the boxplot visualizations depicting cytokine responses before and after TB antigen stimulation in both DM and non-DM groups are presented in Figure 1. These plots illustrate the distribution and median shifts of IL-1β, IL-6, TNF-α, and IFN-γ levels, supporting the descriptive findings summarized in Table 2.
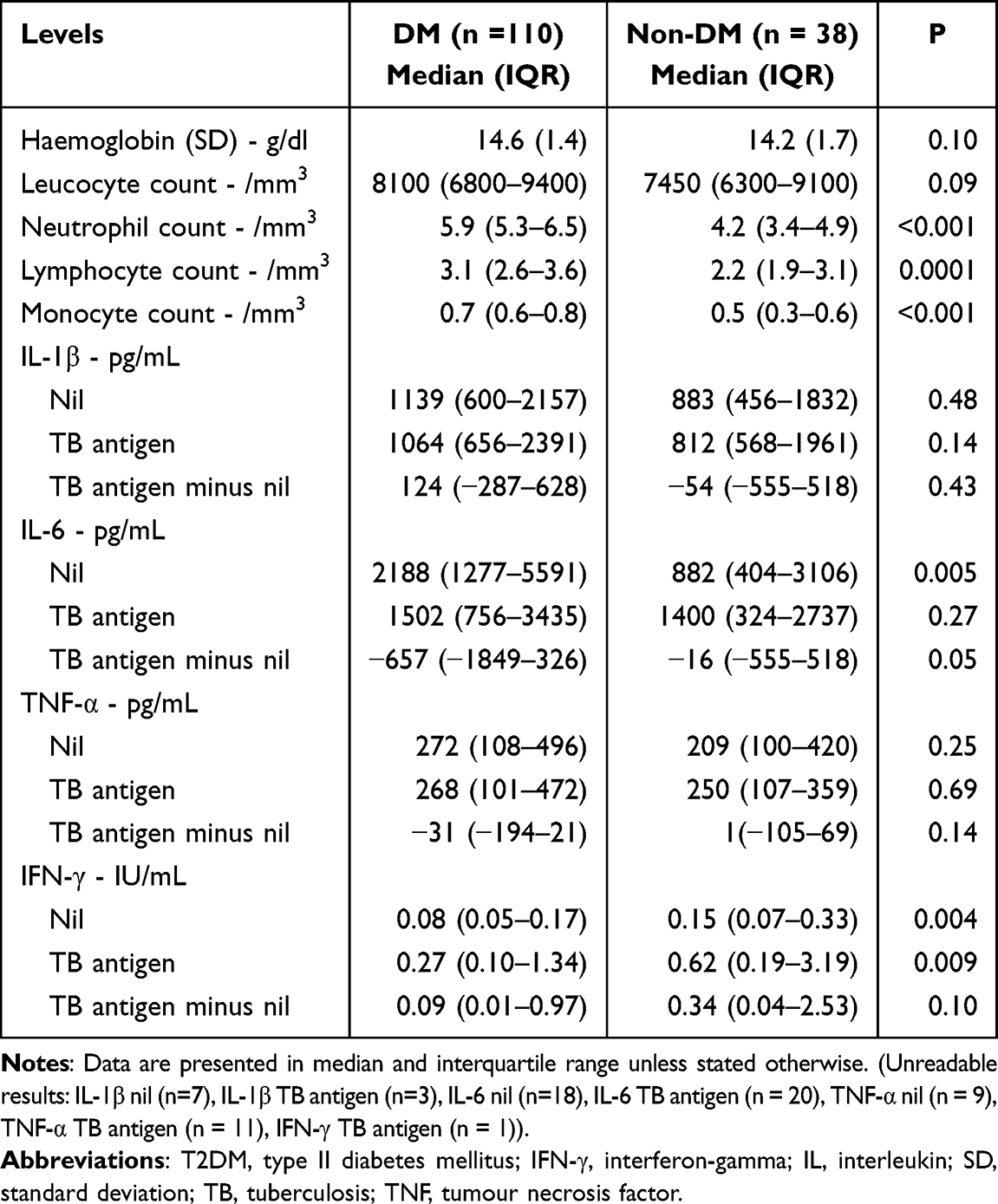 |
Table 2 Laboratory Results of the Participants |
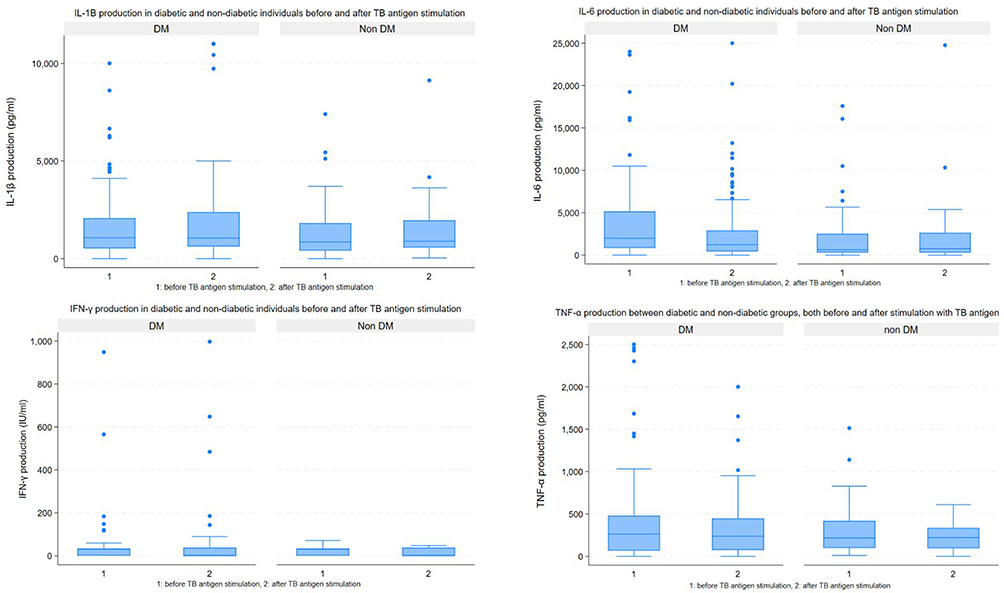 |
Figure 1 Comparison of cytokines response before (1) and after (2) TB antigen stimulation in T2DM and Non-T2DM group (Samples of DM (n=110), and Non-DM (n=38), The y-axis represents cytokine concentration (pg /mL for IL-1β, IL-6, and TNF-α; IU/mL for IFN-γ)). |
Based on Tables 3 and 4, which examine correlations between cytokines (IL-1β, IL-6, TNF-α, IFN-γ), age, BMI, and HbA1c in T2DM and non-T2DM patients before and after TB antigen stimulation, several key patterns emerge. In T2DM patients (Table 3), IL-1β showed significant positive correlations with IL-6 and TNF-α both before and after TB stimulation, suggesting a coordinated inflammatory response. After stimulation, IL-6 and IFN-γ also demonstrated stronger associations with HbA1c and BMI, indicating possible links between immune activation and glycemic control or adiposity in diabetes. In contrast, among non-T2DM individuals (Table 4), the cytokine correlations were generally weaker, although IL-6 and IFN-γ showed statistically significant positive correlations with HbA1c post-stimulation. These findings suggest that TB antigen stimulation may enhance inflammatory responses more markedly in T2DM patients, particularly in relation to metabolic parameters, highlighting a potential interplay between chronic inflammation and metabolic dysfunction in diabetes.
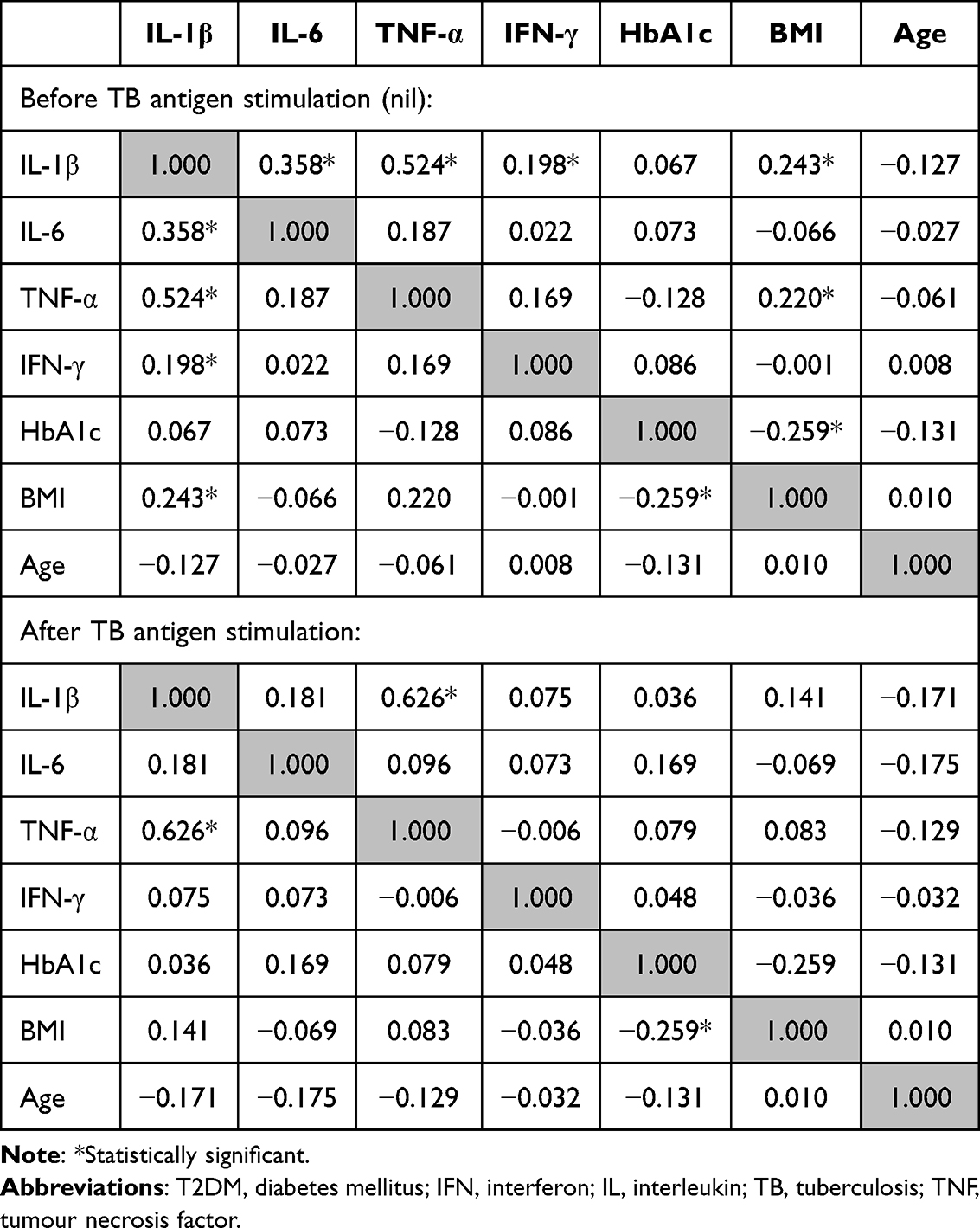 |
Table 3 Correlation Between Cytokines with Age, Body Mass Index, and HbA1c Among T2DM Patients, Before and After TB Antigen Stimulation |
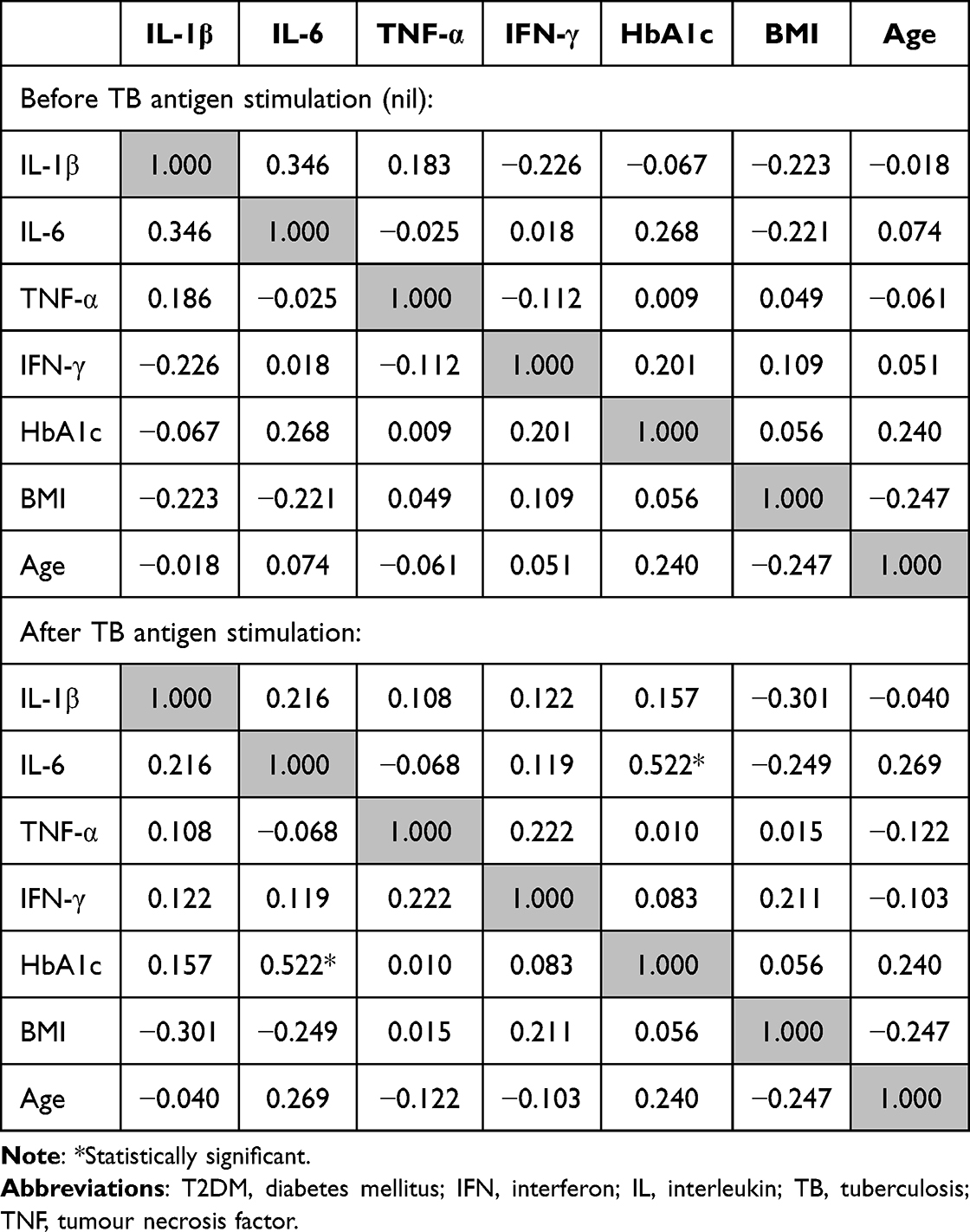 |
Table 4 Correlation Between Cytokines with Age, Body Mass Index, and HbA1c Among Non-T2DM Patients, Before and After TB Antigen Stimulation |
Discussion
This study revealed notable demographic and clinical distinctions between individuals with DM and those without. DM participants were significantly older, had a lower prevalence of BCG vaccination scars, and showed a higher proportion of obesity, particularly in the obese class I and II categories. These differences are important as age, BMI, and vaccination status are known to influence immune function and susceptibility to infection, including tuberculosis (TB) and its immune-mediated responses.33 The presence of poorly controlled glycemia, reflected by a median HbA1c of 8.2% in the DM group, further underscores the metabolic burden in these individuals and may contribute to alterations in immune response profiles.34
There were higher levels of neutrophil, lymphocyte, and monocyte in the T2DM group before and after stimulation with TB antigen. Higher immune response before simulation was probably due to persistent chronic inflammation attributed to the raised glycated end products (AGEs) leading to higher oxidative stress, even if the precise mechanism is yet unknown.35 Previous study found that the ability of neutrophils and macrophages to eradicate infections is decreased by increased oxidative stress.36 This condition favours pathogens to replicate, yielding an increase in immune proliferation to overcome the infection. Meanwhile, Chao et al showed neutrophil dysfunction due to decreased reactive oxygen species production was associated with an increased level of Resistin, protein which inhibits reactive oxygen species (ROS) production and is important in the mycobacterium-induced inflammasome activation.37
Following TB antigen stimulation, there were no significant between-group differences in cytokine levels; however, the DM group exhibited a more trend of median increase in IL-1β levels (124 pg/mL vs –54 pg/mL), suggesting a potentially exaggerated pro-inflammatory response. Although non-significant, lower trend of median differences in IL-6, IFN-γ, and TNF-α in the DM group may indicate an altered cytokine regulatory mechanism post-stimulation. Previous research has shown that individuals with T2DM can display both hyperinflammatory and dysfunctional immune responses to pathogens, including Mycobacterium tuberculosis.13,29 This finding aligns with previous theory that showed asynchronous cytokine release observed in T2DM patients, where dysregulated immune responses—reflected by altered levels of IL-6, IFN-γ, and TNF-α, are driven by the accumulation of toxic advanced glycation end-products and disruptions in cellular metabolism. In particular, hexokinase-1, a key enzyme in glycolysis, has been shown to activate the NLRP3 inflammasome, thereby promoting increased production of IL-1β.38,39 In T2DM individuals, glyceraldehyde 3-phosphate dehydrogenase (GADPH) suppresses TNF expression when the glycolysis process is inhibited.39 Furthermore, on the genomic level, diabetes and intermediate hyperglycemia contribute to immune dysregulation by altering blood transcriptomes and reducing IFN regulation.18
This study showed that there was no significant correlation between plasma cytokine concentrations and HbA1c and diabetes duration. Meanwhile, previous studies have shown the opposite findings.36,40 Plasma concentrations of IFN-γ, TNF-α, IL-17A, and IL-10 were found positively correlated with HbA1c levels, showing a chronic effect of the hyperglycaemic environment to immune regulation.28,35,36 Half of our subjects were diagnosed with diabetes for 1–5 years and no correlation was found between IL-6 levels and HbA1C. Sari et al found uncontrolled diabetic patients, who were diagnosed with diabetes for 8.6 years, had higher IL-6 levels than those of the poorly controlled and controlled diabetic patients. The study presented diabetes duration associated with chronic inflammation and immune dysregulation.41
In this predominantly obese DM population, IL-6 levels showed no significant change before and after TB antigen exposure. Interestingly, this contrasts with previous studies linking obesity to elevated inflammatory cytokines like TNF-α and IL-6, typically produced by adipose tissue. Obesity-related insulin resistance and hyperglycemia, often driven by reactive oxygen species, are also known to promote pro-inflammatory responses.42 Interleukin-6 (IL-6), produced by monocyte-derived macrophages, plays a key role in the immune response to TB and is linked to disease severity. M. tuberculosis regulates IL-6 to suppress type I interferon signaling and promote disease progression. Boni et al suggested that reduced IL-6 levels may help prevent cytokine storms. In our DM group, IL-6 production did not significantly increase after antigen exposure, suggesting that while DM increases TB susceptibility, it may also modulate inflammatory responses, potentially offering both risk and protective effects against severe TB.43 Patients with diabetes produced lower levels of IFN-γ compared to controls, before and after TB antigen exposures. The absence of IFN-γ has been associated with increased risk for mycobacterial disease and worse survival once infected.44 Interferon-gamma activates macrophages and limits PMN inflammation during TB infection. Lower level of IFN-γ also interfere with the granuloma formation, eventually manifesting in fewer BCG scars among T2D patients – although some may not have been vaccinated.44
Although cytokine alterations in T2DM are biologically plausible, our findings should be interpreted cautiously since most differences were not statistically significant. The higher IL-1β levels in T2DM may reflect a pro-inflammatory trend, while the reduced IL-6, TNF-α, and IFN-γ responses suggest possible immune dysregulation. However, these patterns remain exploratory. Consistent with previous reports, our results indicate that diabetes may influence immune reactivity, but larger, powered studies are required to confirm these observations and define their clinical relevance in TB–DM comorbidity. While our findings provide important insights into the immune response to TB antigens in individuals with T2DM, we acknowledge that additional cytokines, particularly Th17-related cytokines such as IL-17A and regulatory cytokines such as IL-10, also play important roles in TB pathogenesis and host immune regulation.45,46 These were not included in the present analysis due to laboratory resource limitations and our intention to focus on the most reproducible and widely studied cytokine markers. Future studies incorporating these additional cytokines could provide a more comprehensive understanding of immune dysregulation in the TB–T2DM syndemic.
This study has several limitations. The inclusion of participants aged ≥40 years may limit the generalizability of the findings to younger T2DM populations. The use of the QuantiFERON-TB Gold assay, which primarily measures CD4⁺ T-cell responses, also restricts assessment of CD8⁺ T-cell activity; future studies employing the QuantiFERON-TB Plus could provide broader insight. The lack of correlation observed between groups may relate to the relatively small sample size, variations in diabetes duration, and differences in medication regimens, which were not adjusted statistically. The influence of antidiabetic drugs such as metformin, known to modulate inflammatory pathways, could also have affected cytokine profiles. In addition, the number of samples excluded due to hemolysis, icterus, or inadequate volume was not recorded, although standardized criteria were applied consistently. Finally, the cross-sectional design precludes causal inference, and no formal power analysis was conducted given the exploratory nature of the study.
Conclusion
This study highlights key differences in immune responses to TB antigen stimulation between individuals with and without T2DM. Patients with DM showed a higher baseline levels of pro-inflammatory cytokines than non-DM individuals. While no statistically significant changes were observed in cytokine levels, T2DM patients showed a trend toward elevated IL-1β and reduced responsiveness in IL-6, TNF-α, and IFN-γ, suggesting underlying immune dysregulation. These patterns, coupled with the altered correlations between cytokines and metabolic parameters, support the hypothesis that T2DM modulates immune responses to TB. Further studies that adjust for potential confounders such as age, BMI, and diabetes medications with broader age ranges and advanced immunological assays (eg, QuantiFERON-TB Plus) are needed to confirm these findings and guide tailored TB prevention strategies in diabetic populations.
Data Sharing Statement
The authors confirm that the data and materials supporting the findings of this study are available in the article.
Ethical Approval
- Approval of the research protocol:
- TANDEM study received ethical approval from the Health Research Ethics Committee, Faculty of Medicine, Universitas Padjadjaran (Ref No: 05/UN6.C2.1.2/KEPK/PN/2014),
- Research Ethics Committee of the London School of Hygiene and Tropical Medicine (LSHTM Ethics Ref: 6449; Amendment No: A473).
- The INFECT study was approved by the same Indonesian ethics committee (Ref No: 14/UN6.C2.1.2/KEPK/PN/2014)
- Health and Disability Ethics Committees in New Zealand (Ref: 13/STH/132).
- Health Research Ethics Committee at Universitas Padjadjaran (Ref No: 263/UN6.KEP/EC/2019)
- Ethical clearance for the utilization of archived biological specimens was granted by the Center for Clinical Infection Studies, Faculty of Medicine, Universitas Padjadjaran. (Ref. No: 202/UN6.C.7.1/LT/2019).
- Approval date of Registry and the Registration No. of the study/trial:
- Health Research Ethics Committee at Universitas Padjadjaran (Ref No: 263/UN6.KEP/EC/2019) – Aproval date: March 6th, 2019
- Ethical clearance for the archived biological specimens by the Center for Clinical Infection Studies, Faculty of Medicine, Universitas Padjadjaran. (Ref. No: 202/UN6.C.7.1/LT/2019) – Aproval date: June 17th, 2019.
Acknowledgments
We thank the TANDEM consortium and INFECT study for the bio-archives.
Author Contributions
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Nanny Natalia Mulyani; Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Raspati Cundarani, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Nofri Rahmadika, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Agnes Rengga Indrati, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Sony Wibisono, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Hikmat Permana, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Ida Parwati, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Bachti Alisjahbana. Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Funding
The authors declare that this study received no funding.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Krishna S, Jacob JJ. Diabetes mellitus and tuberculosis. 2021.
2. Al-Rifai RH, Pearson F, Critchley JA, Abu-Raddad LJ. Association between diabetes mellitus and active tuberculosis: a systematic review and meta-analysis. PLoS One. 2017;12(11):e0187967. doi:10.1371/journal.pone.0187967
3. Huangfu P, Ugarte-Gil C, Golub J, Pearson F, Critchley J. The effects of diabetes on tuberculosis treatment outcomes: an updated systematic review and meta-analysis. Int J Tuberc Lung Dis. 2019;23(7):783–796. doi:10.5588/ijtld.18.0433
4. Li M, Chen T, Hua Z, et al. Global, regional, and national prevalence of diabetes mellitus in patients with pulmonary tuberculosis: a systematic review and meta-analysis. Diabetol Metab Syndr. 2021;13:1–8. doi:10.1186/s13098-021-00743-3
5. Workneh MH, Bjune GA, Yimer SA. Prevalence and associated factors of tuberculosis and diabetes mellitus comorbidity: a systematic review. PLoS One. 2017;12(4):e0175925. doi:10.1371/journal.pone.0175925
6. Asia-Pacific Solidarity Network. Indonesia now second-highest in global tuberculosis cases, with 134,000 annual deaths. Asia-Pacific Solidarity; 2025. (Based on WHO Global Tuberculosis Report 2024 data).
7. Wahidin M, Achadi A, Besral B, et al. Projection of diabetes morbidity and mortality till 2045 in Indonesia based on risk factors and NCD prevention and control programs. Sci Rep. 2024;14(1):5424. doi:10.1038/s41598-024-54563-2
8. Zahrani M, Setiabudi RJ, Hasan H, Wahyunitisari MR. The frequency of multidrug-resistant tuberculosis patient who have history of tuberculosis, HIV, and diabetes mellitus at Dr. Soetomo General Academic Hospital. CIMRJ. 2023;4(1):6–9. doi:10.20473/cimrj.v4i1.42603
9. Amelia R, Fujiati II, Lindarto D, Yunir E, Kusnanto H. Profile of tuberculosis patients with comorbid diabetes mellitus in Medan, Indonesia: a cross-sectional study. Pan Afr Med J. 2024;49:54. doi:10.11604/pamj.2024.49.54.36492
10. Cho NH, Shaw JE, Karuranga S, et al. IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
11. Ruslami R, Aarnoutse RE, Alisjahbana B, Van Der Ven AJ, Van Crevel R. Implications of the global increase of diabetes for tuberculosis control and patient care. Trop Med Int Health. 2010;15(11):1289–1299. doi:10.1111/j.1365-3156.2010.02625.x
12. Yorke E, Atiase Y, Akpalu J, Sarfo-Kantanka O, Boima V, Dey ID. The bidirectional relationship between tuberculosis and diabetes. Tuberc Res Treat. 2017;2017(1):1702578. doi:10.1155/2017/1702578
13. Restrepo BI. Diabetes and tuberculosis. In: Venketaraman V, editor. Understanding the Host Immune Response Against Mycobacterium Tuberculosis Infection. Cham: Springer; 2018:1–21. doi:10.1007/978-3-319-97367-8_1
14. Ssekamatte P, Sitenda D, Nabatanzi R, et al. Metabolic dysfunction impairs Mycobacterium tuberculosis-specific cytokine and chemokine responses in latent tuberculosis and type 2 diabetes mellitus. Sci Rep. 2025;15(1):30474. doi:10.1038/s41598-025-16385-8
15. Abbas U, Masood KI, Khan A, et al. Tuberculosis and diabetes mellitus: relating immune impact of co-morbidity with challenges in disease management in high burden countries. J Clin Tuberc Other Mycobact Dis. 2022;29:100343. doi:10.1016/j.jctube.2022.100343
16. Ronacher K, Joosten SA, van Crevel R, Dockrell HM, Walzl G, Ottenhoff TH. Acquired immunodeficiencies and tuberculosis: focus on HIV/AIDS and diabetes mellitus. Immunol Rev. 2015;264(1):121–137. doi:10.1111/imr.12257
17. Martinez N, Kornfeld H. Diabetes and immunity to tuberculosis. Eur J Immunol. 2014;44(3):617–626. doi:10.1002/eji.201344301
18. Hodgson K, Morris J, Bridson T, Govan B, Rush C, Ketheesan N. Immunological mechanisms contributing to the double burden of diabetes and intracellular bacterial infections. Immunology. 2015;144(2):171–185. doi:10.1111/imm.12394
19. Stalenhoef JE, Alisjahbana B, Nelwan E, et al. The role of interferon-gamma in the increased tuberculosis risk in type 2 diabetes mellitus. Eur J Clin Microbiol Infect Dis. 2008;27:97–103. doi:10.1007/s10096-007-0395-0
20. Lachmandas E, Thiem K, van den Heuvel C, et al. Patients with type 1 diabetes mellitus have impaired IL-1β production in response to Mycobacterium tuberculosis. Eur J Clin Microbiol Infect Dis. 2018;37:371–380. doi:10.1007/s10096-017-3145-y
21. Hossain M, Faruque MO, Kabir G, et al. Association of serum TNF-α and IL-6 with insulin secretion and insulin resistance in IFG and IGT subjects in a Bangladeshi population. Int J Diabetes Mellitus. 2010;2(3):165–168. doi:10.1016/j.ijdm.2010.08.004
22. O’Garra A, Redford PS, McNab FW, Bloom CI, Wilkinson RJ, Berry MP. The immune response in tuberculosis. Ann Rev Immunol. 2013;31(1):475–527. doi:10.1146/annurev-immunol-032712-095939
23. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harbor Perspect Biol. 2014;6(10):a016295. doi:10.1101/cshperspect.a016295
24. Sia JK, Rengarajan J. Immunology of Mycobacterium tuberculosis infections. Microbiol Spectr. 2019;7(4):10–1128.
25. Zhang L, Yang Z, Wu F, et al. Multiple cytokine analysis based on QuantiFERON-TB gold plus in different tuberculosis infection status: an exploratory study. BMC Infect Dis. 2024;24(1):28. doi:10.1186/s12879-023-08943-0
26. Qiagen G. Quantiferon-TB Gold Plus (QFT-Plus) ELISA Package Insert. Germany: Qiagen Hilden; 2017.
27. Jayaraman P, Sada-Ovalle I, Nishimura T, et al. IL-1β promotes antimicrobial immunity in macrophages by regulating TNFR signaling and caspase-3 activation. J Immunol. 2013;190(8):4196–4204. doi:10.4049/jimmunol.1202688
28. Kumar Nathella P, Babu S. Influence of diabetes mellitus on immunity to human tuberculosis. Immunology. 2017;152(1):13–24. doi:10.1111/imm.12762
29. Prada-Medina CA, Fukutani KF, Pavan Kumar N, et al. Systems immunology of diabetes-tuberculosis comorbidity reveals signatures of disease complications. Sci Rep. 2017;7(1):1999. doi:10.1038/s41598-017-01767-4
30. Alisjahbana B, McAllister SM, Ugarte-Gil C, et al. Screening diabetes mellitus patients for pulmonary tuberculosis: a multisite study in Indonesia, Peru, Romania and South Africa. Trans R Soc Trop Med Hyg. 2021;115(6):634–643. doi:10.1093/trstmh/traa100
31. Verrall AJ, Schneider M, Alisjahbana B, et al. Early clearance of Mycobacterium tuberculosis is associated with increased innate immune responses. J Infect Dis. 2020;221(8):1342–1350. doi:10.1093/infdis/jiz147
32. Koesoemadinata RC, McAllister SM, Soetedjo NN, et al. Latent TB infection and pulmonary TB disease among patients with diabetes mellitus in Bandung, Indonesia. Trans R Soc Trop Med Hyg. 2017;111(2):81–89. doi:10.1093/trstmh/trx015
33. Wherry EJ, Kurachi M. Molecular and cellular insights into T cell exhaustion. Nat Rev Immunol. 2015;15(8):486–499. doi:10.1038/nri3862
34. Pickup JC. Inflammation and activated innate immunity in the pathogenesis of type 2 diabetes. Diabetes Care. 2004;27(3):813–823. doi:10.2337/diacare.27.3.813
35. Lachmandas E, Vrieling F, Wilson LG, et al. The effect of hyperglycaemia on in vitro cytokine production and macrophage infection with Mycobacterium tuberculosis. PLoS One. 2015;10(2):e0117941.
36. Ronacher K, van Crevel R, Critchley JA, et al. Defining a research agenda to address the converging epidemics of tuberculosis and diabetes: part 2: underlying biologic mechanisms. Chest. 2017;152(1):174–180. doi:10.1016/j.chest.2017.02.032
37. Chao WC, Yen CL, Wu YH, et al. Increased resistin may suppress reactive oxygen species production and inflammasome activation in type 2 diabetic patients with pulmonary tuberculosis infection. Microb Infect. 2015;17(3):195–204. doi:10.1016/j.micinf.2014.11.009
38. Daryabor G, Atashzar MR, Kabelitz D, Meri S, Kalantar K. The effects of type 2 diabetes mellitus on organ metabolism and the immune system. Front Immunol. 2020;11:1582.
39. Finucane OM, Sugrue J, Rubio-Araiz A, Guillot-Sestier MV, Lynch MA. The NLRP3 inflammasome modulates glycolysis by increasing PFKFB3 in an IL-1β-dependent manner in macrophages. Sci Rep. 2019;9(1):4034. doi:10.1038/s41598-019-40619-1
40. Zhou T, Hu Z, Yang S, Sun L, Yu Z, Wang G. Role of adaptive and innate immunity in type 2 diabetes mellitus. J Diabetes Res. 2018;2018(1):7457269. doi:10.1155/2018/7457269
41. Sari MI, Tala ZZ, Wahyuni DD. Association between glycated hemoglobin with the levels of serum proinflammatory cytokines and antioxidants in patients with type 2 diabetes mellitus in Universitas Sumatera Utara Hospital. Open Access Maced J Med Sci. 2019;7(5):715. doi:10.3889/oamjms.2019.168
42. Shen Q, He T, Li T, et al. Synergistic effects of overweight/obesity and high hemoglobin A1c status on elevated high-sensitivity C-reactive protein in Chinese adults: a cross-sectional study. Front Nutr. 2023;10:1156404. doi:10.3389/fnut.2023.1156404
43. Boni FG, Hamdi I, Koundi LM, Shrestha K, Xie J. Cytokine storm in tuberculosis and IL-6 involvement. Infect Genet Evol. 2022;97:105166. doi:10.1016/j.meegid.2021.105166
44. Domingo-Gonzalez R, Prince O, Cooper A, Khader SA. Cytokines and chemokines in Mycobacterium tuberculosis infection. Microbiol Spectr. 2016;4(5):10–1128.
45. Li H-M, Wang L-J, Huang Q, Pan H-F, Zhang T-P. Exploring the association between Th17 pathway gene polymorphisms and pulmonary tuberculosis. Front Immunol. 2022;13:994247. doi:10.3389/fimmu.2022.994247
46. Lyadova IV, Panteleev AV. Th1 and Th17 cells in tuberculosis: protection, pathology, and biomarkers. Mediators Inflamm. 2015;2015:854507. doi:10.1155/2015/854507
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.