Back to Journals » ImmunoTargets and Therapy » Volume 14
Immune Microenvironment on the Molecular Mechanisms and Therapeutic Targets of MAFLD
Authors Jiang Z ![]() , Qian B, Xu T
, Qian B, Xu T ![]() , Bai J, Fu W
, Bai J, Fu W
Received 14 April 2025
Accepted for publication 23 June 2025
Published 11 July 2025 Volume 2025:14 Pages 719—733
DOI https://doi.org/10.2147/ITT.S530451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jadwiga Jablonska
Zhonghao Jiang,1,* Baolin Qian,1,* Tongjie Xu,1,2 Junjie Bai,1 Wenguang Fu1,3
1Department of Biliary-Pancreatic Center, The Affiliated Hospital of Southwest Medical University, Luzhou, People’s Republic of China; 2Department of Vascular Surgery, The Affiliated Hospital, Southwest Medical University, Luzhou, 646000, People’s Republic of China; 3Metabolic Hepatobiliary and Pancreatic Diseases Key Laboratory of Luzhou City, The Affiliated Hospital, Southwest Medical University, Luzhou, 646000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenguang Fu, Department of General Surgery (Hepatopancreatobiliary Surgery), The Affiliated Hospital, Southwest Medical University, Luzhou, 646000, People’s Republic of China, Email [email protected]
Abstract: Metabolic dysfunction-associated fatty liver disease (MAFLD) is one of the most prevalent chronic liver diseases worldwide. It is characterized by hepatic steatosis in the absence of significant alcohol consumption, and can progress to liver fibrosis, cirrhosis, and even hepatocellular carcinoma (HCC). Despite its widespread impact, treatment options remain limited, and effective therapies targeting the underlying disease mechanisms are lacking. Recent studies have highlighted the critical role of the liver’s immune microenvironment in the onset and progression of MAFLD. However, research into immune-based therapies remains in its early stages. Most existing studies have focused on understanding the immune mechanisms involved, but specific immune targets and therapeutic strategies have yet to be fully explored. This gap has hindered the development of targeted immunotherapies for MAFLD. This review aims to examine the molecular mechanisms of the immune microenvironment in MAFLD and identify potential therapeutic targets, offering insights for future clinical and scientific advancements.
Keywords: MAFLD, immune microenvironment, pathway, therapeutic targets
Metabolic dysfunction-associated fatty liver disease (MAFLD), characterized by liver steatosis, is one of the most prevalent chronic liver diseases globally.1 The disease was redefined in 2023, with the name changing from non-alcoholic fatty liver disease (NAFLD) to MAFLD. This change was made to better reflect the link between metabolic dysfunction and fatty liver disease, a relationship that was not fully captured by the previous term.2,3 MAFLD’s incidence is rising rapidly, with recent epidemiological data projecting a global prevalence of over 30% by 2025. In the United States, the number of affected individuals is expected to reach 27 million by the 2030s, with approximately half of these patients likely to develop significant liver fibrosis.4 The Asia-Pacific region, particularly mainland China and India, is considered the epicenter of MAFLD, with both high and increasing prevalence rates.5–7 The pathogenesis of MAFLD is complex, involving factors such as hepatic stellate cell reprogramming, hepatocyte-endothelial interactions, alterations in the liver’s immune environment, remodeling of the hepatic microvascular and interstitial environments, and disruptions in metabolic homeostasis.8,9
We conducted literature searches using two databases: PubMed (“metabolic associated fatty liver disease” OR “MAFLD”) AND (“immune” OR “immune system” OR “inflammation” OR “immune response” OR “immune pathways” OR “immune-based interventions”), and Web of Science TS=(“metabolic associated fatty liver disease” OR “MAFLD”) AND TS=(“immune” OR “immune system” OR “inflammation” OR “immune response” OR “immune pathways” OR “immune-based interventions”). The search was limited to the past 10 years, yielding a total of 775 documents. We then systematically reviewed the potential mechanisms that contribute to or inhibit the development of MAFLD, with a focus on immune microenvironment-related research targets. Specifically, we examined their key regulatory roles, associated molecular pathways, and potential therapeutic strategies. This review aims to provide strategic insights for future MAFLD therapies, particularly by identifying underexplored targets, mechanisms, and directions for drug development in both clinical and scientific contexts.
Mechanistic Insights in MAFLD
The pathological mechanisms of MAFLD are multifaceted, involving lipid metabolism disorders, oxidative stress, granulomal dysfunction, insulin resistance, and inflammatory responses. Additionally, factors such as intestinal flora imbalances and endoplasmic reticulum stress play significant roles in the disease’s progression (Figure 1).10,11
 |
Figure 1 Fat accumulation can lead to an increase in DNL, FFA and TG. High pressure in the endoplasmic reticulum can lead to the expression of eIF2α, etc and insulin resistance, mitochondrial damage and intestinal secretion of LPS can all increase the amount of ROS, exacerbate liver inflammation and promote the development of MAFLD. Created in BioRender. Jiang, Z. (2025) https://BioRender.com/yttgsjt. |
In MAFLD, excessive fat accumulation in the liver (hepatic steatosis >5% of liver weight) leads to the oxidation of fatty acids via the beta-oxidation pathway. This process induces endoplasmic reticulum (ER) stress, oxidative stress, and activation of Kupffer cells (KCs),12 which generate large amounts of reactive oxygen species (ROS).13 Some lipid peroxidation products can activate hepatic stellate cells (HSCs), which, due to their phagocytic activity and expression of NADPH oxidase, fail to efficiently eliminate ROS, thereby exacerbating oxidative stress.14–16
Mitochondria are the primary source of reactive oxygen species (ROS),17 producing approximately 90% of cellular ROS. When mitochondria are damaged, oxidative phosphorylation is impaired, leading to an increase in ROS production. Excess ROS activate mitochondrial quality control (MQC) mechanisms, including biogenesis, fission, fusion, and autophagy.18 If these processes fail, mitochondrial dysfunction occurs, which may contribute to the progression of MAFLD.19 Moore et al reported a 40–50% reduction in beta-oxidation in MASH patients, which correlated with increased ROS production in the liver and decreased markers of mitochondrial biogenesis, autophagy, and mitochondrial dynamics (fission and fusion).20–22
Insulin resistance (IR) is characterized by decreased insulin sensitivity in the body, liver, and adipose tissues. In the presence of IR, elevated blood glucose levels and gluconeogenesis trigger metabolic disorders and inflammatory responses, which can lead to liver cell damage and fibrosis. Additionally, reduced adiponectin levels in MAFLD increase free fatty acids (FFAs), disrupting the insulin response and further promoting IR, creating a vicious cycle.23
Gut microbes play a key role in bile acid metabolism, and dysbiosis can disrupt the composition of bile acids, affecting their interaction with receptors.24 This imbalance can impair the intestinal barrier, increase permeability, and allow bacterial endotoxins to enter the bloodstream, triggering a systemic inflammatory response.25,26 At the same time, it activates Kupffer cells in the liver, leading to the production of pro-inflammatory molecules such as trimethylamine N-oxide (TMAO), secondary bile acids (SBAs), and bacterial 16sDNA.27,28 These molecules exacerbate liver inflammation and fibrosis, potentially accelerating the progression of MAFLD.29
Liver Immune Microenvironment
Kupffer cells are activated, releasing pro-inflammatory cytokines that trigger inflammatory responses and hepatocellular injury in MAFLD.30 The reactive oxygen species (ROS) produced by these activated Kupffer cells also promote hepatic stellate cell (HSC) activation. HSCs, in turn, secrete chemokines that recruit monocytes and other immune cells to the liver, exacerbating inflammation.31 Once activated, HSCs release cytokines and growth factors, such as TGF-β,32 which further enhance Kupffer cell activity, creating a positive feedback loop that accelerates both MAFLD progression and liver fibrosis.33 Neutrophils worsen hepatocyte injury and inflammation by secreting elastase, ROS, and various pro-inflammatory cytokines, as well as chemokines like IL-8, which recruit additional immune cells to the liver.34,35 Natural killer (NK) cells and natural killer T (NKT) cells, which are both pro-inflammatory and cytotoxic, also contribute to disease progression.36 NKT cells release TNF superfamily member 14 (TNFSF14), which increases free fatty acid (FFA) uptake by hepatocytes, promoting steatosis.37 Dendritic cells (DCs), as potent antigen-presenting cells, secrete pro-inflammatory cytokines such as IL-12 and TNF-α upon activation, promoting Th1 cell differentiation and enhancing liver inflammation.38 Finally, dysfunction in liver endothelial cells (LECs), which regulate blood flow and metabolism, may further exacerbate liver injury (Figure 2).39–41
 |
Figure 2 Free fatty acids stimulate Kupffer cells to produce inflammatory factors such as TNF and aggravate liver inflammatory response and injury through NF-κB and JNK signaling pathways, while immune cells such as monocytes, macrophages, and neutrophils promote the activation of HSCs through inflammatory factors such as TGF-β1, TNF, and IL-1β; on the other hand, Kupffer cells also promote lipid deposition in hepatocytes, further aggravating MAFLD. Created by Medpeer. Zhonghao J (2025) www.medpeer.cn. |
Immune Microenvironment and Pathways of MAFLD
Involvement of Intrinsic Immune Cells
As discussed in Liver Immune Microenvironment, innate immune cells play a multifaceted role in MAFLD, contributing to liver cell damage clearance, activation of fibrosis, and regulation of the immune microenvironment balance at various stages of the disease.
Role of Adaptive Immune Cells
In MAFLD, Th1 and Th17 cells exacerbate liver damage by activating innate immune cells and secreting pro-inflammatory cytokines such as interferon gamma (IFN-γ) and IL-17. Th2 cells produce IL-4 and IL-13, which, under certain conditions, can promote fibrosis.35,42 In contrast, Tregs secrete IL-10 and TGF-β,43 which help inhibit inflammation and maintain immune homeostasis. However, in MAFLD, the number and function of Tregs are diminished, leading to worsened inflammation.30,31,33 Additionally, CD8+ T-cells contribute to MASH by directly attacking liver cells. B cells further aggravate liver fibrosis and inflammation by producing antibodies, activating the complement system, and presenting antigens.
Release of Pro-Fibrotic Factors
Transforming growth factor-beta (TGF-β) is the primary profibrotic factor driving the progression of MAFLD to fibrosis. It activates hepatic stellate cells (HSCs) and stimulates the synthesis of extracellular matrix (ECM) proteins through the Smad signaling pathway, contributing to fibrosis. Other factors, including platelet-derived growth factor (PDGF), tumor necrosis factor-alpha (TNF-α), insulin-like growth factor-1 (IGF-1), and endothelin-1 (ET-1), also promote HSC proliferation, migration, and ECM synthesis through various signaling pathways. TNF-α further enhances fibrosis by indirectly inducing other pro-fibrogenic factors, such as TGF-β and interleukin-1β (IL-1β), which worsen inflammation. ET-1 exacerbates the hypoxic environment in the liver through vasoconstriction, further promoting fibrosis. Additionally, chemokines like CCL2 (MCP-1) and stromal cell-derived factor-1 (SDF-1) activate HSCs by attracting monocytes and macrophages to the liver, creating a local inflammatory microenvironment that accelerates fibrosis.44 These profibrogenic factors form complex molecular networks that drive the progression of fatty liver disease to fibrosis and cirrhosis.43
Effects of Disorders of Lipid Metabolism
In MAFLD, insulin resistance leads to excessive free fatty acid (FFA) accumulation, causing fat buildup in liver cells, triglyceride formation, and the production of toxic substances like malondialdehyde (MDA) and 4-hydroxy-2-nonenal (4-HNE),45 which activate liver immune cells. This also triggers inflammatory pathways, such as toll-like receptor 4 (TLR4), and the release of pro-inflammatory cytokines like TNF-α and IL-6.46,47 Lipid metabolism disorders and sustained inflammation activate hepatic stellate cells (HSCs), which secrete extracellular matrix components, contributing to liver fibrosis.48 Additionally, excess lipids impair autophagy and disrupt the intestinal barrier, allowing endotoxins to enter the liver, further promoting inflammation and fibrosis.
Role of the Gut-Liver Axis
Patients with MAFLD often exhibit imbalances in their intestinal flora, with an increase in harmful bacteria and a decrease in beneficial ones. This disrupts intestinal barrier function, leading to increased permeability and allowing bacterial products and metabolites to enter the bloodstream. These substances are then transported to the liver via the portal vein, where they activate immune cells and trigger an inflammatory response.49 Additionally, bile acids, short-chain fatty acids (such as butyric acid and propionic acid), and tryptophan derivatives produced by gut microbiota metabolism can directly influence liver metabolism and immune function, thereby modulating inflammation and lipid accumulation.28
Autophagy and Oxidative Stress
Autophagy plays a protective role in MAFLD by reducing ROS production through the removal of damaged mitochondria, thus alleviating oxidative stress.50,51 It also degrades lipid droplets in hepatocytes (lipophagy), reducing fat accumulation and mitigating hepatic steatosis. Additionally, autophagy exerts an anti-inflammatory effect by clearing necrotic cells and the danger-associated molecular patterns (DAMPs) they release, inhibiting immune activation.52 However, during MAFLD progression, excessive ROS generated by oxidative stress can impair the autophagy pathway, disrupting its function and worsening oxidative stress in a vicious cycle that accelerates liver damage.53–55 Therefore, combining antioxidants with autophagy activators may provide a more effective treatment approach for MAFLD, offering improved therapeutic options for patients.
Remodeling of the Immune Microenvironment
The remodeling of the immune microenvironment is a key factor in the progression of MAFLD. Studies indicate that the immune profile in MAFLD patients differs significantly from that of healthy controls, with notable changes in immune cell subpopulations and cytokine secretion. For example, CD4+ T-cells exhibit abnormal function in MAFLD, and their absence in the liver microenvironment is closely associated with the progression to fibrosis and hepatocellular carcinoma (HCC). γδ T-cells also play a crucial role in MAFLD; gut microbiota influence liver inflammation and fibrosis by modulating the activation of these cells.56 Akkermansia muciniphila (Akk bacteria), a beneficial gut bacterium, inhibits the development of MAFLD by regulating the polarization of γδ T-cells and macrophages, which not only affects liver inflammation but also influences fibrosis by modulating hepatic stellate cell activation.57,58
The interaction between changes in the liver’s immune microenvironment and the molecular mechanisms underlying MAFLD drives its progression to MASH, fibrosis, and liver cancer. Additionally, metabolic signaling pathways such as AMPK,59 mTOR,59,60 and PI3K/AKT61 influence immune cells and interact with immune signaling pathways like NF-κB62,63 and JNK/MAPK,64,65 collectively regulating inflammation and disease progression in MAFLD66,67 (Table 1 and Figure 3). Therefore, targeting the liver immune microenvironment through these signaling pathways to inhibit pro-inflammatory factors, modulate immune cell subsets, and improve the gut-liver axis may provide new therapeutic strategies for MAFLD.
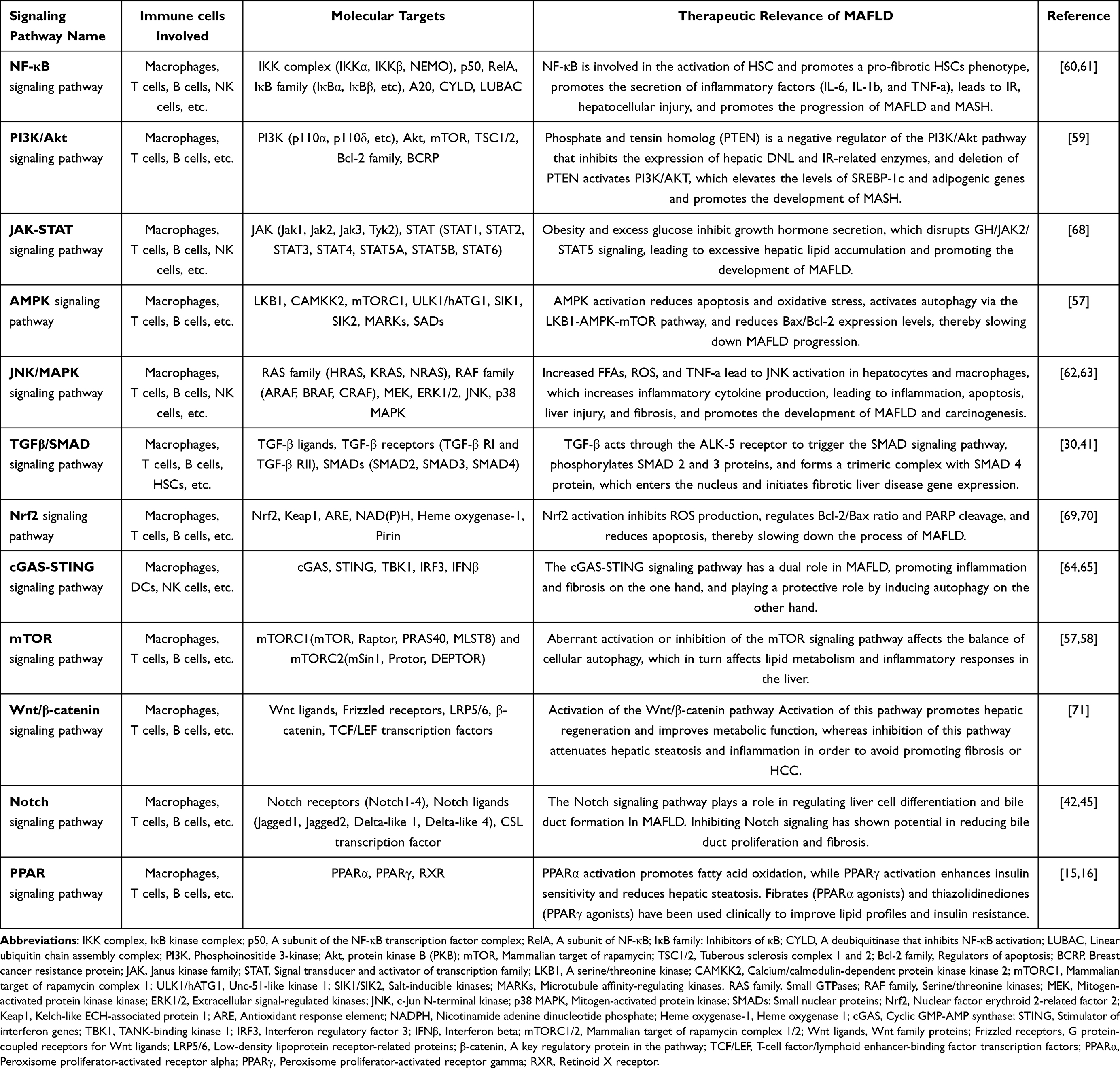 |
Table 1 Relevant Signaling Pathways in and for MAFLD |
 |
Figure 3 Eight key signaling pathways and related targets affecting the development of MAFLD, as well as providing suitable options for subsequent targeted therapies. Created in BioRender. Jiang, Z. (2025) https://BioRender.com/5mu5xru. Abbreviations: ADAM 10, A member of the ADAM family of proteins; GDP/GTP, Guanosine diphosphate/guanosine triphosphate; AMPK, AMP-activated protein kinase; Rag A/B, Rag C/D, Proteins involved in the regulation of mTORC1 signaling; mTORC1/mTORC2, Mammalian target of rapamycin complex 1 and complex 2; TSC1/2, Tuberous sclerosis complex 1/2; Rheb, Ras homolog enriched in brain; PI3K, Phosphatidylinositol-3-kinase; PIP₂/PIP₃, Phosphatidylinositol-4,5-bisphosphate/phosphatidylinositol-3,4,5-trisphosphate; AKT, protein kinase B; PTEN, Phosphatase and tensin homolog; TCF/LEF, T-cell factor/lymphoid enhancer-binding factor; AP1, Activator protein 1; ATF2, Activating transcription factor 2; Nrf2, Nuclear factor-erythroid 2-related factor 2; Keap1, Kelch-like ECH-associated protein 1; ARE, Antioxidant response element; PPAR, Peroxisome proliferator-activated receptor; RXR, Retinoid X receptor; EGFR, Epidermal growth factor receptor; GPCR, G protein-coupled receptor; TNFR, Tumor necrosis factor receptor; IL-1R, Interleukin-1 receptor; BMP, Bone morphogenetic protein; TGFβ, Transforming growth factor beta; TLR, Toll-like receptor; JAK, Janus kinase; STAT, Signal transducer and activator of transcription; SMAD, A family of proteins involved in TGFβ signaling; IKK, IκB kinase; NF-κB, Nuclear factor kappa-B; IRF3, Interferon regulatory factor 3; STING, Stimulator of interferon genes; cGAS, Cyclic GMP-AMP synthase; cGAMP, Cyclic GMP - AMP. |
Therapeutic Strategies
Anti-Dyslipidemia Therapy
Triglyceride transferase 2 (DGAT2) catalyzes triglyceride formation and plays a crucial role in triglyceride accumulation in the liver. A Phase II trial assessed the safety, efficacy, and tolerability of PradiGastat (a DGAT1 inhibitor).58,72 The results demonstrated that liver fat content was reduced by at least 30% in the high-dose (35.29%) and low-dose (30%) groups, compared to a 10.53% reduction in the placebo group.73
Microsomal triglyceride transfer protein (MTTP) plays a critical role in the assembly and secretion of very-low-density lipoprotein (VLDL). Inhibiting MTTP reduces VLDL formation, thereby decreasing liver lipid accumulation.74
The TRIM56-FASN axis has also been identified as a potential therapeutic target for MAFLD. Researchers at the University of Science and Technology of China found that TRIM56, an E3 ubiquitin ligase, slows MAFLD progression by promoting the degradation of FASN, a key enzyme involved in fatty acid synthesis.75
Farnesoid X receptor (FXR) activation, primarily in hepatocytes and intestinal epithelial cells, inhibits bile acid (BA) synthesis, reduces liver fat production and gluconeogenesis, and prevents liver inflammation, fibrosis, and cell death.76–78 Obeticholic acid, the first FXR agonist to enter Phase III clinical trials, showed significant promise in lowering liver fat content and improving liver function, though it was not FDA-approved due to efficacy and side effects.79,80
Retinol-binding protein-4 (RBP-4) exacerbates insulin resistance and liver damage by interfering with the insulin signaling pathway, promoting lipogenesis, and activating pro-inflammatory and pro-fibrotic signaling pathways. Inhibiting RBP-4 synthesis or targeting its function with novel delivery systems could provide a new treatment strategy for MAFLD.81 Additionally, circulating RBP-4 levels correlate with MAFLD severity and may serve as an early biomarker for high-risk patients. Researchers at Peking University proposed the “Fibrotic Overexpression and Retention (FORT)” strategy, using mRNA lipid nanoparticles (LNPs) to deliver therapeutic proteins directly to liver lesions. This method leverages the high expression of RBP-4 in fibrotic livers, enhancing protein retention and efficacy for precise liver fibrosis treatment.69,70
Osteocalcin (OCN) regulates fatty acid uptake through the AMPK-FOXO1/BCL6-CD36 signaling pathway, reduces liver lipid accumulation, activates the Nrf2 pathway to combat oxidative stress,68,82 inhibits the JNK pathway to mitigate inflammation,64,83 and improves insulin resistance, thereby regulating glucose and lipid metabolism.84 In clinical studies, chemically synthesized osteocalcin (csOCN) has been shown to alleviate liver damage in MAFLD mouse models by reducing fatty acid uptake via CD36 regulation.
Anti-Inflammatory Treatment
Chemokine receptors CCR2/CCR5 mediate the recruitment of monocytes and macrophages, which release pro-inflammatory factors that promote liver inflammation and fibrosis.85 Berberine (BBR) has been shown to improve MAFLD by modulating the chemokine/CMKLR1 signaling pathway, thereby reducing liver inflammation and lipid deposition.86
High-mobility group box 1 protein (HMGB1) activates pro-inflammatory responses through the HMGB1/RAGE signaling pathway, contributing to liver damage.87 A novel RG-I pectin-like polysaccharide, YJ3A1, purified from roses, may inhibit MAFLD progression by suppressing the expression and release of HMGB1.88
Cyclooxygenase-2 (COX-2), a key enzyme in the production of prostaglandin E2 (PGE2), activates inflammatory pathways, including NF-κB and PI3K-AKT, through its receptors (EP1-4). This promotes the release of pro-inflammatory factors such as TNF-α and IL-6, exacerbating liver inflammation.89 Inhibitors of the COX-2/PGE2 axis could provide more comprehensive metabolic improvements in MAFLD patients.90
NLRP3 inflammasomes contribute to MAFLD progression by activating inflammation, inducing oxidative stress, and regulating lipid metabolism.91 Inhibitors such as MCC950 and OLT1177 reduce the release of inflammatory factors (eg, IL-1β and IL-18) by blocking NLRP3 activation, alleviating liver inflammation and fibrosis.71
Mitochondrial antiviral signaling protein (MAVS) plays a critical role in mitochondrial function, protecting cells from metabolic stress by interacting with the VDAC2 protein on the outer mitochondrial membrane. In MAFLD models, the absence of MAVS exacerbates mitochondrial dysfunction, leading to increased fat accumulation and heightened inflammatory responses. MAVS also regulates lipid metabolism pathways, reducing liver fat production and accumulation.92
Antifibrotic Therapy
The PDGF, NLRP3-caspase-1, and Wnt/β-catenin signaling pathways are key regulators of HSC activation and fibrogenic progression in MAFLD.93 Targeting these pathways may inhibit HSC activation and mitigate liver fibrosis.94 For instance, PDGF receptor inhibitors such as imatinib have demonstrated promising results in liver fibrosis models.95
Lysyl oxidase-like protein 2 (LOXL2) catalyzes the cross-linking of collagen, enhancing the stability and stiffness of the extracellular matrix (ECM) and promoting liver fibrosis. Consequently, the LOXL2 inhibitor simtuzumab represents a potential new treatment for MAFLD.96
ASK1 inhibitors, such as GS-4997, reduce oxidative stress, inhibit inflammatory responses, and block ASK1-mediated p38 and JNK signaling pathways, leading to decreased stellate cell activation.97 These inhibitors have shown significant anti-fibrotic and anti-inflammatory effects in MAFLD treatment.98
Galectin-3 is a crucial mediator in liver fibrosis and inflammation. Inhibitors like GR-MD-02 can reduce stellate cell activation and collagen deposition, thereby alleviating fibrosis. Combining such treatments with FXR agonists or immune checkpoint inhibitors could further enhance their anti-fibrotic and anti-inflammatory effects.99,100
Immunomodulation
Immunological checkpoint molecules such as CTLA-4, PD-1/PD-L1, and Tim-3 play essential roles in regulating immune responses. Inhibiting these checkpoints can enhance the immune system’s ability to detect and clear liver lesions. For example, PD-1 inhibitors like pembrolizumab have demonstrated potential efficacy in clinical studies of MAFLD.101–103
Additionally, the m6A methyltransferase METTL3, which has been identified as a potential therapeutic target for MAFLD-associated hepatocellular carcinoma (MAFLD-HCC),104 promotes cholesterol biosynthesis by modulating m6A-modified SCAP. This, in turn, affects the function of CD8+ T-cells within the tumor microenvironment, thereby enhancing anti-tumor responses.105
Intestinal Flora
Akkermansia muciniphila (Akk bacteria) enhances immune function, reduces inflammation, and improves both intestinal immunity and metabolism.106 Probiotics, such as Bifidobacteria and Lactobacilli, along with short-chain fatty acids (SCFAs), have been shown to decrease the production of inflammatory factors.107 Fecal microbiota transplantation (FMT), which involves transplanting healthy gut flora, helps restore intestinal microecology.108 These approaches have demonstrated promise in clinical trials and offer novel strategies for treating MAFLD.
Targeted therapies also contribute to improving the immune microenvironment in MAFLD through various mechanisms. These include inhibiting adipogenesis, promoting the oxidative breakdown of fat, regulating macrophage subpopulations, enhancing T-cell function, suppressing immunosuppressive cells, reducing the release of inflammatory factors, and modulating the gut microbiome (Figure 4). Together, these mechanisms open up new therapeutic targets and treatment strategies for MAFLD.
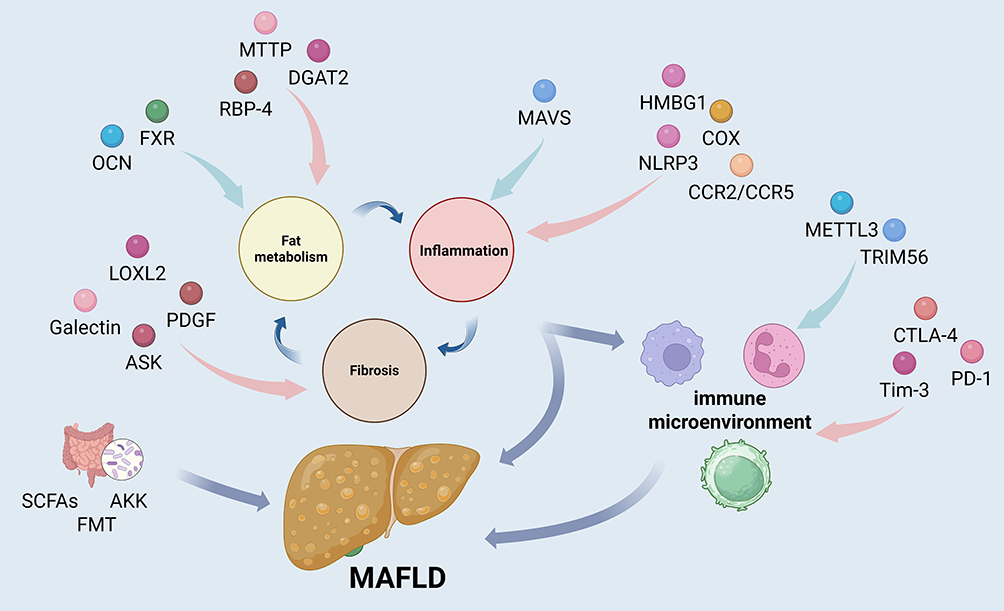 |
Figure 4 Relevant targets (red for promotion, blue for inhibition) affect MAFLD either directly by influencing lipid metabolism, inflammation, and fibrosis or by acting on the immune microenvironment. Created in BioRender. Jiang, Z. (2025) https://BioRender.com/6t6ta22. Abbreviations: MTTP, Microsomal Triglyceride Transfer Protein; DGAT2, Diacylglycerol O-acyltransferase 2; RBP-4, Retinol-binding protein 4; FXR, Farnesoid X Receptor; OCN, Osteocalcin; MAVS, Mitochondrial Antiviral Signaling Protein; HMGB1, High Mobility Group Box 1; COX, Cyclooxygenase; NLRP3, NLR Family Pyrin Domain Containing 3; CCR2/CCR5, Chemokine receptors key for immune cell chemotaxis and migration; LOXL2, Lysyl Oxidase Like 2; Galectin, A family of proteins binding carbohydrates; PDGF, Platelet-Derived Growth Factor, a multifunctional cytokine; ASK, Apoptosis Signal-Regulating Kinase; METTL3, Methyltransferase-Like 3; TRIM56, Tripartite Motif Containing 56; CTLA-4, Cytotoxic T-Lymphocyte Associated Protein 4; Tim-3, T-cell Immune Receptor with Ig and ITIM Domains; PD-1, Programmed Cell Death Protein 1; SCFAs, Short-Chain Fatty Acids; AKK, Akkermansia; FMT, Fecal Microbiota Transplantation. |
Conclusion and Outlook
MAFLD is a global chronic liver disease with a complex pathogenesis involving multiple factors such as lipid accumulation, insulin resistance, and oxidative stress. A decade-long analysis of the immune microenvironment in MAFLD reveals that imbalances in immune cell subpopulations, abnormal activation of immune pathways, and disrupted immune-metabolic interactions play key roles in its development and progression. However, research into immune-based therapeutic interventions remains limited.
Currently, the US Food and Drug Administration (FDA) has not approved any drugs specifically for the treatment of simple fatty liver disease or MAFLD. Ongoing clinical trials, such as the Phase III trials of Rezdiffra by Madrigal Pharmaceuticals, Aramchol by Galmed Pharmaceuticals, and Semaglutide by Novo Nordisk, primarily focus on metabolic targets, with few studies targeting immune regulation.
Though some immunomodulatory treatments have shown promise in animal studies—such as FGF-21 therapy, which reduces liver fat and improves insulin resistance—questions remain about their long-term effects on inflammation and fibrosis, their interaction with immune cells, and their efficacy across varying metabolic states. CCR2/CCR5 inhibitors, like cenicriviroc, have improved insulin resistance in mouse models, but large-scale clinical trials are necessary for validation.
Adoptive cell therapies targeting immune cells such as Tregs and NKT cells show limited clinical progress, with small sample sizes and low-quality evidence. Immune checkpoint inhibitors (ICIs) hold promise in MAFLD-associated hepatocellular carcinoma (MAFLD-HCC), but the evidence is still limited. Similarly, while dietary fiber supplementation has shown potential to improve gut microbiota and regulate immune responses, studies have been small and lack long-term follow-up.
To establish effective immunotherapies for MAFLD, large-scale, multicenter clinical trials are essential. These should aim to validate the efficacy and safety of immunomodulatory drugs, precisely target affected areas, minimize systemic immunosuppression, reduce adverse reactions, and optimize treatment regimens.
Future studies should focus on investigating the dynamic changes and interactions of various immune cell subpopulations (eg, different T-cell types and macrophage subpopulations) at different stages of MAFLD, such as simple steatohepatitis, MASH, and liver fibrosis. These studies should aim to clarify the specific mechanisms by which these cells contribute to disease progression and identify early diagnostic markers and prognostic indicators that reflect immune microenvironmental reorganization. By detecting changes in immune cell subpopulations, cytokines, chemokines, and other biomarkers in blood or liver tissue, we can enable precise assessment of MAFLD disease status and develop personalized treatment plans.
For instance, lipid-associated macrophages (LAMs) gradually replace resident Kupffer cells during MAFLD progression. These LAMs activate hepatic stellate cells by secreting factors like SPP1, promoting liver fibrosis. Additionally, studying how metabolic products such as fatty acids and bile acids in the local liver microenvironment influence immune cell activity, differentiation, and function—and vice versa—could provide insights into the complex interplay between metabolism and immunity in MAFLD.
Strengthening interdisciplinary collaboration and integrating advanced technologies like genomics and metabolomics will allow for a more comprehensive assessment of the immune status and disease progression in MAFLD patients. This approach could also enable the exploration of combined treatment strategies, such as combining immunotherapy with anti-inflammatory therapies, metabolic regulation, and anti-fibrotic treatments, to synergistically improve the immune microenvironment and enhance treatment efficacy.
Moreover, targeted therapies that focus on specific immune cell subpopulations or signaling pathways, combined with lifestyle interventions (eg, dietary control and exercise), and interventions aimed at modulating the gut microbiota (eg, probiotics, prebiotics, and fecal microbiota transplantation), may provide novel therapeutic strategies to treat MAFLD.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by The National Natural Science Foundation of China (Grant No. 82170587, Grant No. 82400740). The Sichuan Provincial Natural Science Foundation for Outstanding Youth Foundation (Grant No. 2024NSFJQ0054). Research Start-up Funded Project of the Affiliated Hospital of Southwest Medical University (Grant No 24353, 24354). Southwest Medical University Natural Science General Program (Grant No 2024ZKY050).
Disclosure
The authors declare that they have no competing interests.
References
1. De A, Bhagat N, Mehta M, Taneja S, Duseja A. Metabolic dysfunction-associated steatotic liver disease (MASLD) definition is better than MAFLD criteria for lean patients with NAFLD. J Hepatol. 2024;80(2):e61–e62. doi:10.1016/j.jhep.2023.07.031
2. Yuan S, Chen J, Li X, et al. Lifestyle and metabolic factors for nonalcoholic fatty liver disease: Mendelian randomization study. Eur J Epidemiol. 2022;37(7):723–733. doi:10.1007/s10654-022-00868-3
3. Chan SL, Schuler M, Kang YK, et al. A first-in-human Phase 1/2 study of FGF401 and combination of FGF401 with spartalizumab in patients with hepatocellular carcinoma or biomarker-selected solid tumors. J Exp Clin Cancer Res. 2022;41(1):189. doi:10.1186/s13046-022-02383-5
4. Song R, Li Z, Zhang Y, Tan J, Chen Z. Comparison of NAFLD, MAFLD and MASLD characteristics and mortality outcomes in United States adults. Liver Int. 2024;44(4):1051–1060. doi:10.1111/liv.15856
5. Gofton C, Upendran Y, Zheng MH, George J. MAFLD: how is it different from NAFLD? Clin Mol Hepatol. 2023;29(Suppl):S17–s31. doi:10.3350/cmh.2022.0367
6. Paik JM, Duong S, Zelber-Sagi S, Lazarus JV, Henry L, Younossi ZM. Food insecurity, low household income, and low education level increase the risk of having metabolic dysfunction-associated fatty liver disease among adolescents in the United States. Am J Gastroenterol. 2024;119(6):1089–1101. doi:10.14309/ajg.0000000000002749
7. Pipitone RM, Ciccioli C, Infantino G, et al. MAFLD: a multisystem disease. Therapeut Adv Endocrinol Metabol. 2023;14:20420188221145549. doi:10.1177/20420188221145549
8. Pouwels S, Sakran N, Graham Y, et al. Non-alcoholic fatty liver disease (NAFLD): a review of pathophysiology, clinical management and effects of weight loss. BMC Endocr Disord. 2022;22(1):63. doi:10.1186/s12902-022-00980-1
9. Rong L, Zou J, Ran W, et al. Advancements in the treatment of non-alcoholic fatty liver disease (NAFLD). Front Endocrinol. 2022;13:1087260. doi:10.3389/fendo.2022.1087260
10. Guo X, Yin X, Liu Z, Wang J. Non-alcoholic fatty liver disease (NAFLD) pathogenesis and natural products for prevention and treatment. Int J Mol Sci. 2022;23(24):15489. doi:10.3390/ijms232415489
11. Le P, Payne JY, Zhang L, et al. Disease state transition probabilities across the spectrum of NAFLD: a systematic review and meta-analysis of paired biopsy or imaging studies. Clin Gastroenterol Hepatol. 2023;21(5):1154–1168. doi:10.1016/j.cgh.2022.07.033
12. Wei S, Wang L, Evans PC, Xu S. NAFLD and NASH: etiology, targets and emerging therapies. Drug Discovery Today. 2024;29(3):103910. doi:10.1016/j.drudis.2024.103910
13. Mózes FE, Lee JA, Selvaraj EA, et al. Diagnostic accuracy of non-invasive tests for advanced fibrosis in patients with NAFLD: an individual patient data meta-analysis. Gut. 2022;71(5):1006–1019. doi:10.1136/gutjnl-2021-324243
14. Sunny NE, Bril F, Cusi K. Mitochondrial adaptation in nonalcoholic fatty liver disease: novel mechanisms and treatment strategies. Trend Endocrinol Metabol. 2017;28(4):250–260. doi:10.1016/j.tem.2016.11.006
15. Lin RT, Sun QM, Xin X, et al. Comparative efficacy of THR-β agonists, FGF-21 analogues, GLP-1R agonists, GLP-1-based polyagonists, and Pan-PPAR agonists for MASLD: a systematic review and network meta-analysis. Metabolism. 2024;161:156043. doi:10.1016/j.metabol.2024.156043
16. Peiseler M, Schwabe R, Hampe J, Kubes P, Heikenwälder M, Tacke F. Immune mechanisms linking metabolic injury to inflammation and fibrosis in fatty liver disease - novel insights into cellular communication circuits. J Hepatol. 2022;77(4):1136–1160. doi:10.1016/j.jhep.2022.06.012
17. Begriche K, Massart J, Robin MA, Bonnet F, Fromenty B. Mitochondrial adaptations and dysfunctions in nonalcoholic fatty liver disease. Hepatology. 2013;58(4):1497–1507. doi:10.1002/hep.26226
18. Roca-Portoles A, Tait SWG. Mitochondrial quality control: from molecule to organelle. Cell Mol Life Sci. 2021;78(8):3853–3866. doi:10.1007/s00018-021-03775-0
19. Krishnasamy Y, Gooz M, Li L, Lemasters JJ, Zhong Z. Role of mitochondrial depolarization and disrupted mitochondrial homeostasis in non-alcoholic steatohepatitis and fibrosis in mice. Int J Physiol Pathophysiol Pharmacol. 2019;11(5):190–204.
20. Moore MP, Cunningham RP, Meers GM, et al. Compromised hepatic mitochondrial fatty acid oxidation and reduced markers of mitochondrial turnover in human NAFLD. Hepatology. 2022;76(5):1452–1465. doi:10.1002/hep.32324
21. Sinha RA, Yen PM. Thyroid hormone-mediated autophagy and mitochondrial turnover in NAFLD. Cell Biosci. 2016;6:46. doi:10.1186/s13578-016-0113-7
22. Cable EE, Finn PD, Stebbins JW, et al. Reduction of hepatic steatosis in rats and mice after treatment with a liver-targeted thyroid hormone receptor agonist. Hepatology. 2009;49(2):407–417. doi:10.1002/hep.22572
23. Fujii H, Kawada N, Japan Study Group Of Nafld J-N. The role of insulin resistance and diabetes in nonalcoholic fatty liver disease. Int J Mol Sci. 2020;21(11):3863. doi:10.3390/ijms21113863
24. Long J, Xu Y, Zhang X, Wu B, Wang C. Role of FXR in the development of NAFLD and intervention strategies of small molecules. Arch Biochem Biophys. 2024;757:110024. doi:10.1016/j.abb.2024.110024
25. Ravaioli F, Dajti E, Mantovani A, Newsome PN, Targher G, Colecchia A. Diagnostic accuracy of FibroScan-AST (FAST) score for the non-invasive identification of patients with fibrotic non-alcoholic steatohepatitis: a systematic review and meta-analysis. Gut. 2023;72(7):1399–1409. doi:10.1136/gutjnl-2022-328689
26. Zamani M, Alizadeh-Tabari S, Chitkara P, Singh S, Loomba R. Prevalence of nonalcoholic fatty liver disease in patients with rheumatoid arthritis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2023;21(11):2789–2796. doi:10.1016/j.cgh.2023.02.021
27. Zhou D, Zhang J, Xiao C, Mo C, Ding BS. Trimethylamine-N-oxide (TMAO) mediates the crosstalk between the gut microbiota and hepatic vascular niche to alleviate liver fibrosis in nonalcoholic steatohepatitis. Front Immunol. 2022;13:964477. doi:10.3389/fimmu.2022.964477
28. Schoeler M, Caesar R. Dietary lipids, gut microbiota and lipid metabolism. Rev Endocr Metab Disord. 2019;20(4):461–472. doi:10.1007/s11154-019-09512-0
29. Zheng C, Wang L, Zou T, et al. Ileitis promotes MASLD progression via bile acid modulation and enhanced TGR5 signaling in ileal CD8(+) T cells. J Hepatol. 2024;80(5):764–777. doi:10.1016/j.jhep.2023.12.024
30. Zhou Y, Zhang H, Yao Y, Zhang X, Guan Y, Zheng F. CD4(+) T cell activation and inflammation in NASH-related fibrosis. Front Immunol. 2022;13:967410. doi:10.3389/fimmu.2022.967410
31. Moreno-Fernandez ME, Giles DA, Oates JR, et al. PKM2-dependent metabolic skewing of hepatic Th17 cells regulates pathogenesis of non-alcoholic fatty liver disease. Cell Metab. 2021;33(6):1187–1204.e1189. doi:10.1016/j.cmet.2021.04.018
32. Yan M, Li H, Xu S, et al. Targeting endothelial necroptosis disrupts profibrotic endothelial-hepatic stellate cells crosstalk to alleviate liver fibrosis in nonalcoholic steatohepatitis. Int J Mol Sci. 2023;24(14):11313. doi:10.3390/ijms241411313
33. Wabitsch S, McCallen JD, Kamenyeva O, et al. Metformin treatment rescues CD8(+) T-cell response to immune checkpoint inhibitor therapy in mice with NAFLD. J Hepatol. 2022;77(3):748–760. doi:10.1016/j.jhep.2022.03.010
34. Pfister D, Núñez NG, Pinyol R, et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature. 2021;592(7854):450–456. doi:10.1038/s41586-021-03362-0
35. Parola M, Pinzani M. Liver fibrosis in NAFLD/NASH: from pathophysiology towards diagnostic and therapeutic strategies. Mol Aspect Med. 2024;95:101231. doi:10.1016/j.mam.2023.101231
36. Ye Q, Liu Y, Zhang G, et al. Deficiency of gluconeogenic enzyme PCK1 promotes metabolic-associated fatty liver disease through PI3K/AKT/PDGF axis activation in male mice. Nat Commun. 2023;14(1):1402. doi:10.1038/s41467-023-37142-3
37. Rohm TV, Meier DT, Olefsky JM, Donath MY. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55(1):31–55. doi:10.1016/j.immuni.2021.12.013
38. Marques V, Afonso MB, Bierig N, et al. Adiponectin, leptin, and IGF-1 are useful diagnostic and stratification biomarkers of NAFLD. Front Med. 2021;8:683250. doi:10.3389/fmed.2021.683250
39. Schinzari F, Cardillo C. Intricacies of the endothelin system in human obesity: role in the development of complications and potential as a therapeutic target. Can J Physiol Pharmacol. 2020;98(9):563–569. doi:10.1139/cjpp-2019-0651
40. Liu Y, Hao L, Wang L, Lu M, Yin C, Xiao Y. Serum stromal cell-derived factor-1 concentrations are increased and associated with nonalcoholic fatty liver disease in children with obesity. BMC Endocr Disord. 2024;24(1):67. doi:10.1186/s12902-024-01597-2
41. Loomba R, Abdelmalek MF, Armstrong MJ, et al. Semaglutide 2·4 mg once weekly in patients with non-alcoholic steatohepatitis-related cirrhosis: a randomised, placebo-controlled Phase 2 trial. Lancet Gastroenterol Hepatol. 2023;8(6):511–522. doi:10.1016/S2468-1253(23)00068-7
42. Pan Y, Chen H, Zhang X, et al. METTL3 drives NAFLD-related hepatocellular carcinoma and is a therapeutic target for boosting immunotherapy. Cell Rep Med. 2023;4(8):101144. doi:10.1016/j.xcrm.2023.101144
43. Rom O, Liu Y, Liu Z, et al. Glycine-based treatment ameliorates NAFLD by modulating fatty acid oxidation, glutathione synthesis, and the gut microbiome. Sci Trans Med. 2020;12(572). doi:10.1126/scitranslmed.aaz2841.
44. Kang J, Postigo-Fernandez J, Kim K, et al. Notch-mediated hepatocyte MCP-1 secretion causes liver fibrosis. JCI Insight. 2023;8(3). doi:10.1172/jci.insight.165369.
45. Tong J, Lan XT, Zhang Z, et al. Ferroptosis inhibitor liproxstatin-1 alleviates metabolic dysfunction-associated fatty liver disease in mice: potential involvement of PANoptosis. Acta Pharmacol Sin. 2023;44(5):1014–1028. doi:10.1038/s41401-022-01010-5
46. Jiang B, Wang D, Hu Y, et al. Serum amyloid A1 exacerbates hepatic steatosis via TLR4-mediated NF-κB signaling pathway. Mol Metabol. 2022;59:101462. doi:10.1016/j.molmet.2022.101462
47. Yu J, Zhu C, Wang X, et al. Hepatocyte TLR4 triggers inter-hepatocyte Jagged1/Notch signaling to determine NASH-induced fibrosis. Sci Trans Med. 2021;13(599). doi:10.1126/scitranslmed.abe1692.
48. Chen J, Yang S, Luo H, et al. Polysaccharide of Atractylodes macrocephala Koidz alleviates NAFLD-induced hepatic inflammation in mice by modulating the TLR4/MyD88/NF-κB pathway. Int Immunopharmacol. 2024;141:113014. doi:10.1016/j.intimp.2024.113014
49. Ge Y, Wang X, Guo Y, et al. Gut microbiota influence tumor development and Alter interactions with the human immune system. J Exp Clin Cancer Res. 2021;40(1):42. doi:10.1186/s13046-021-01845-6
50. Hou X, Yin S, Ren R, et al. Myeloid-cell-specific IL-6 signaling promotes MicroRNA-223-enriched exosome production to attenuate NAFLD-associated fibrosis. Hepatology. 2021;74(1):116–132. doi:10.1002/hep.31658
51. Skuratovskaia D, Komar A, Vulf M, et al. IL-6 reduces mitochondrial replication, and IL-6 receptors reduce chronic inflammation in NAFLD and type 2 diabetes. Int J Mol Sci. 2021;22(4):1774. doi:10.3390/ijms22041774
52. Ma DW, Ha J, Yoon KS, Kang I, Choi TG, Kim SS. Innate immune system in the pathogenesis of non-alcoholic fatty liver disease. Nutrients. 2023;15(9):2068. doi:10.3390/nu15092068
53. Vogli S, Naska A, Marinos G, Kasdagli MI, Orfanos P. The effect of vitamin E supplementation on serum aminotransferases in non-alcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis. Nutrients. 2023;15(17):3733. doi:10.3390/nu15173733
54. Alwadani AH, Almasri SA, Aloud AA, Albadr NA, Alshammari GM, Yahya MA. The synergistic protective effect of γ-Oryzanol (OZ) and N-acetylcysteine (NAC) against experimentally induced NAFLD in rats entails hypoglycemic, antioxidant, and PPARα stimulatory effects. Nutrients. 2022;15(1):106. doi:10.3390/nu15010106
55. Ding Q, Guo R, Pei L, et al. N-Acetylcysteine alleviates high fat diet-induced hepatic steatosis and liver injury via regulating the intestinal microecology in mice. Food Funct. 2022;13(6):3368–3380. doi:10.1039/D1FO03952K
56. Shi J, Liu Y, Zhang Z, et al. Zexie-Baizhu Decoction ameliorates non-alcoholic fatty liver disease through gut-adipose tissue crosstalk. J Ethnopharmacol. 2025;337(Pt 1):118700. doi:10.1016/j.jep.2024.118700
57. Newsome PN, Sanyal AJ, Neff G, et al. A randomised Phase IIa trial of amine oxidase copper-containing 3 (AOC3) inhibitor BI 1467335 in adults with non-alcoholic steatohepatitis. Nat Commun. 2023;14(1):7151. doi:10.1038/s41467-023-42398-w
58. Xu J, Xia Q, Wu T, et al. Prophylactic treatment with Bacteroides uniformis and Bifidobacterium bifidum counteracts hepatic NK cell immune tolerance in nonalcoholic steatohepatitis induced by high fat diet. Gut Microbes. 2024;16(1):2302065. doi:10.1080/19490976.2024.2302065
59. Du D, Liu C, Qin M, et al. Metabolic dysregulation and emerging therapeutical targets for hepatocellular carcinoma. Acta pharmaceutica Sinica B. 2022;12(2):558–580. doi:10.1016/j.apsb.2021.09.019
60. Biao Y, Li D, Zhang Y, et al. Wulingsan alleviates MAFLD by activating autophagy via regulating the AMPK/mTOR/ULK1 signaling pathway. Can J Gastroenterol Hepatol. 2024;2024:9777866. doi:10.1155/2024/9777866
61. He Y, Wang H, Lin S, et al. Advanced effect of curcumin and resveratrol on mitigating hepatic steatosis in metabolic associated fatty liver disease via the PI3K/AKT/mTOR and HIF-1/VEGF cascade. Biomed Pharmacothe. 2023;165:115279. doi:10.1016/j.biopha.2023.115279
62. Wang YF, Zhang WL, Li ZX, et al. METTL14 downregulation drives S100A4(+) monocyte-derived macrophages via MyD88/NF-κB pathway to promote MAFLD progression. Signal Transduction Targeted Ther. 2024;9(1):91. doi:10.1038/s41392-024-01797-1
63. Liu B, Xiang L, Ji J, et al. Sparcl1 promotes nonalcoholic steatohepatitis progression in mice through upregulation of CCL2. J Clin Invest. 2021;131(20). doi:10.1172/JCI144801.
64. Chu Y, Yang S, Chen X. Fibroblast growth factor receptor signaling in metabolic dysfunction-associated fatty liver disease: pathogenesis and therapeutic targets. Pharmacol Ther. 2025;269:108844. doi:10.1016/j.pharmthera.2025.108844
65. Fang Z, Xu H, Duan J, et al. Short-term tamoxifen administration improves hepatic steatosis and glucose intolerance through JNK/MAPK in mice. Signal Transduction Targeted Ther. 2023;8(1):94. doi:10.1038/s41392-022-01299-y
66. Donne R, Saroul-Ainama M, Cordier P, et al. Replication stress triggered by nucleotide pool imbalance drives DNA damage and cGAS-STING pathway activation in NAFLD. Dev Cell. 2022;57(14):1728–1741.e1726. doi:10.1016/j.devcel.2022.06.003
67. Chen R, Du J, Zhu H, Ling Q. The role of cGAS-STING signalling in liver diseases. JHEP Rep. 2021;3(5):100324. doi:10.1016/j.jhepr.2021.100324
68. Yang Q, Shen X, Luo Y, et al. ELANE enhances KEAP1 protein stability and reduces NRF2-mediated ferroptosis inhibition in metabolic dysfunction-associated fatty liver disease. Cell Death Dis. 2025;16(1):266. doi:10.1038/s41419-025-07603-2
69. Guo Z, Yao Z, Huang B, et al. MAFLD-related hepatocellular carcinoma: exploring the potent combination of immunotherapy and molecular targeted therapy. Int Immunopharmacol. 2024;140:112821. doi:10.1016/j.intimp.2024.112821
70. Armstrong MJ, Okanoue T, Sundby Palle M, Sejling AS, Tawfik M, Roden M. Similar weight loss with semaglutide regardless of diabetes and cardiometabolic risk parameters in individuals with metabolic dysfunction-associated steatotic liver disease: post hoc analysis of three randomised controlled trials. Diab Obes Metab. 2025;27(2):710–718. doi:10.1111/dom.16065
71. Wang XX, Song YY, Jin R, et al. Hepatic steatosis analysis in metabolic dysfunction-associated steatotic liver disease based on artificial intelligence. Diagnostics. 2024;14(24):2889. doi:10.3390/diagnostics14242889
72. Armandi A, Bespaljko H, Mang A, et al. Short-term reduction of dietary gluten improves metabolic-dysfunction associated steatotic liver disease: a randomised, controlled proof-of-concept study. Aliment Pharmacol Ther. 2024;59(10):1212–1222. doi:10.1111/apt.17941
73. Amin NB, Saxena AR, Somayaji V, Dullea R. Inhibition of diacylglycerol acyltransferase 2 versus diacylglycerol acyltransferase 1: potential therapeutic implications of pharmacology. Clin Ther. 2023;45(1):55–70. doi:10.1016/j.clinthera.2022.12.008
74. Tan S, Liu X, Chen L, et al. Fas/FasL mediates NF-κBp65/PUMA-modulated hepatocytes apoptosis via autophagy to drive liver fibrosis. Cell Death Dis. 2021;12(5):474. doi:10.1038/s41419-021-03749-x
75. Xu S, Wu X, Wang S, et al. TRIM56 protects against nonalcoholic fatty liver disease by promoting the degradation of fatty acid synthase. J Clin Invest. 2024;134(5). doi:10.1172/JCI166149.
76. Parlati L, Régnier M, Guillou H, Postic C. New targets for NAFLD. JHEP Rep. 2021;3(6):100346. doi:10.1016/j.jhepr.2021.100346
77. Adorini L, Trauner M. FXR agonists in NASH treatment. J Hepatol. 2023;79(5):1317–1331. doi:10.1016/j.jhep.2023.07.034
78. Clifford BL, Sedgeman LR, Williams KJ, et al. FXR activation protects against NAFLD via bile-acid-dependent reductions in lipid absorption. Cell Metab. 2021;33(8):1671–1684.e1674. doi:10.1016/j.cmet.2021.06.012
79. Lu Q, Yu J, Xia N, et al. Obeticholic acid aggravates liver fibrosis by activating hepatic farnesoid X receptor-induced apoptosis in cholestatic mice. Chem Biol Interact. 2025;406:111364. doi:10.1016/j.cbi.2024.111364
80. Adorini L, Rigbolt K, Feigh M, Roth J, Erickson M. Increased hepatoprotective effects of the novel farnesoid X receptor agonist INT-787 versus obeticholic acid in a mouse model of nonalcoholic steatohepatitis. PLoS One. 2024;19(4):e0300809. doi:10.1371/journal.pone.0300809
81. Chen H, Chen S, Liu D, et al. Associations between multiple metabolic biomarkers with steatotic liver disease subcategories: a 5-year Chinese cohort study. Cell Rep Med. 2025;6(1):101884. doi:10.1016/j.xcrm.2024.101884
82. Abulikemu A, Zhao X, Xu H, et al. Silica nanoparticles aggravated the metabolic associated fatty liver disease through disturbed amino acid and lipid metabolisms-mediated oxidative stress. Redox Biol. 2023;59:102569. doi:10.1016/j.redox.2022.102569
83. Annadurai P, Isaac AE. Unveiling the role of IL7R in metabolism-associated fatty liver disease leading to hepatocellular carcinoma through transcriptomic and machine learning approaches. Discover Oncol. 2025;16(1):873. doi:10.1007/s12672-025-02638-5
84. Zhang M, Dong K, Du Q, et al. Chemically synthesized osteocalcin alleviates NAFLD via the AMPK-FOXO1/BCL6-CD36 pathway. J Transl Med. 2024;22(1):782. doi:10.1186/s12967-024-05592-y
85. Krenkel O, Puengel T, Govaere O, et al. Therapeutic inhibition of inflammatory monocyte recruitment reduces steatohepatitis and liver fibrosis. Hepatology. 2018;67(4):1270–1283. doi:10.1002/hep.29544
86. Lu Z, Lu F, Wu L, He B, Chen Z, Yan M. Berberine attenuates non-alcoholic steatohepatitis by regulating chemerin/CMKLR1 signalling pathway and Treg/Th17 ratio. Naunyn-Schmiedeberg’s Arch Pharmacol. 2021;394(2):383–390. doi:10.1007/s00210-020-01914-1
87. Chandrashekaran V, Seth RK, Dattaroy D, et al. HMGB1-RAGE pathway drives peroxynitrite signaling-induced IBD-like inflammation in murine nonalcoholic fatty liver disease. Redox Biol. 2017;13:8–19. doi:10.1016/j.redox.2017.05.005
88. Jing X, Zhou G, Zhu A, Jin C, Li M, Ding K. RG-I pectin-like polysaccharide from Rosa chinensis inhibits inflammation and fibrosis associated to HMGB1/TLR4/NF-κB signaling pathway to improve non-alcoholic steatohepatitis. Carbohydr Polym. 2024;337:122139. doi:10.1016/j.carbpol.2024.122139
89. Lee Y, Gu EJ, Song HY, et al. Exploring the anti-inflammatory potential of novel chrysin derivatives through cyclooxygenase-2 inhibition. ACS Omega. 2024;9(51):50491–50503. doi:10.1021/acsomega.4c07938
90. Ali G, Omar H, Hersi F, Abo-Youssef A, Ahmed O, Mohamed W. The protective role of etoricoxib against diethylnitrosamine/2-acetylaminofluorene- induced hepatocarcinogenesis in Wistar rats: the impact of NF-κB/COX-2/PGE2 signaling. Current Mol Pharmacol. 2022;15(1):252–262. doi:10.2174/1874467214666210708103752
91. Yu T, Luo L, Xue J, Tang W, Wu X, Yang F. Gut microbiota-NLRP3 inflammasome crosstalk in metabolic dysfunction-associated steatotic liver disease. Clin Res Hepatol Gastroenterol. 2024;48(8):102458. doi:10.1016/j.clinre.2024.102458
92. Fu J, Hu F, Ma T, et al. A conventional immune regulator mitochondrial antiviral signaling protein blocks hepatic steatosis by maintaining mitochondrial homeostasis. Hepatology. 2022;75(2):403–418. doi:10.1002/hep.32126
93. Tian Y, Mok MT, Yang P, Cheng AS. Epigenetic activation of Wnt/β-Catenin signaling in NAFLD-associated hepatocarcinogenesis. Cancers. 2016;8(8):76. doi:10.3390/cancers8080076
94. Wu X, Zhang F, Xiong X, et al. Tetramethylpyrazine reduces inflammation in liver fibrosis and inhibits inflammatory cytokine expression in hepatic stellate cells by modulating NLRP3 inflammasome pathway. IUBMB Life. 2015;67(4):312–321. doi:10.1002/iub.1348
95. AlAsfoor S, Rohm TV, Bosch AJT, et al. Imatinib reduces non-alcoholic fatty liver disease in obese mice by targeting inflammatory and lipogenic pathways in macrophages and liver. Sci Rep. 2018;8(1):15331. doi:10.1038/s41598-018-32853-w
96. Chen W, Yang A, Jia J, Popov YV, Schuppan D, You H. Lysyl oxidase (LOX) family members: rationale and their potential as therapeutic targets for liver fibrosis. Hepatology. 2020;72(2):729–741. doi:10.1002/hep.31236
97. Li C, Fang L, Su X, et al. Macrophage miR-4524a-5p/TBP promotes β-TrCP -TIM3 complex activation and TGFβ release and aggravates NAFLD-associated fibrosis. Cell Death Dis. 2025;16(1):315. doi:10.1038/s41419-025-07574-4
98. He M, Wang J, Deng W, et al. Exploring novel indazole derivatives as ASK1 inhibitors: design, synthesis, biological evaluation and docking studies. Bioorg Chem. 2024;147:107391. doi:10.1016/j.bioorg.2024.107391
99. Kram M. Galectin-3 inhibition as a potential therapeutic target in non-alcoholic steatohepatitis liver fibrosis. World J Hepatol. 2023;15(2):201–207. doi:10.4254/wjh.v15.i2.201
100. Jin H-L, Feng X-Y, Feng S-L, Dai L, Zhu W-T, Yuan Z-W. Isoquercitrin attenuates the progression of non-alcoholic steatohepatitis in mice by modulating galectin-3-mediated insulin resistance and lipid metabolism. Phytomedicine. 2024;123:155188. doi:10.1016/j.phymed.2023.155188
101. Sawada K, Hayashi H, Nakajima S, Hasebe T, Fujiya M, Okumura T. Non-alcoholic fatty liver disease is a potential risk factor for liver injury caused by immune checkpoint inhibitor. J Gastroenterol Hepatol. 2020;35(6):1042–1048. doi:10.1111/jgh.14889
102. Sauer N, Janicka N, Szlasa W, et al. TIM-3 as a promising target for cancer immunotherapy in a wide range of tumors. Cancer Immunol Immunother. 2023;72(11):3405–3425. doi:10.1007/s00262-023-03516-1
103. Du X, Wu Z, Xu Y, et al. Increased Tim-3 expression alleviates liver injury by regulating macrophage activation in MCD-induced NASH mice. Cell Mol Immunol. 2019;16(11):878–886. doi:10.1038/s41423-018-0032-0
104. Li Y, He X, Lu X, et al. METTL3 acetylation impedes cancer metastasis via fine-tuning its nuclear and cytosolic functions. Nat Commun. 2022;13(1):6350. doi:10.1038/s41467-022-34209-5
105. Lian S, Lu M, Jiajing L, et al. Conjugated lithocholic acid activates hepatic TGR5 to promote lipotoxicity and MASLD-MASH transition by disrupting carnitine biosynthesis. Adv Sci 2025;12(20):e2410602. doi:10.1002/advs.202410602
106. Higarza SG, Arboleya S, Arias JL, Gueimonde M, Arias N. Akkermansia muciniphila and environmental enrichment reverse cognitive impairment associated with high-fat high-cholesterol consumption in rats. Gut Microbes. 2021;13(1):1–20. doi:10.1080/19490976.2021.1880240
107. Pinanga YD, Pyo KH, Shin EA, et al. Association between hepatocyte TM4SF5 expression and gut microbiome dysbiosis during non-alcoholic fatty liver disease development. Life Sci. 2024;358:123164. doi:10.1016/j.lfs.2024.123164
108. Saeed H, Díaz LA, Gil-Gómez A, et al. Microbiome-centered therapies for the management of metabolic dysfunction-associated steatotic liver disease. Clin Mol Hepatol. 2025;31(Suppl):S94–s111. doi:10.3350/cmh.2024.0811
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.