Back to Journals » Nature and Science of Sleep » Volume 11
Immune-mediated comorbidities in Saudi patients with narcolepsy
Authors Alomar M, Almeneessier AS ![]() , Olaish AH
, Olaish AH ![]() , Alshiban A, Alomar A, BaHammam AS
, Alshiban A, Alomar A, BaHammam AS ![]()
Received 22 November 2018
Accepted for publication 16 February 2019
Published 3 May 2019 Volume 2019:11 Pages 35—43
DOI https://doi.org/10.2147/NSS.S195650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sutapa Mukherjee
Majed Alomar,1 Aljohara S Almeneessier,1,2 Awad H Olaish,1 Abdulrahman Alshiban,1 Abdullah Alomar,1 Ahmed S BaHammam1,3
1The University Sleep Disorders Center, Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2Family and Community Medicine Department, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 3The Strategic Technologies Program of the National Plan for Sciences and Technology and Innovation in the Kingdom of Saudi Arabia, King Saud University, Riyadh, Saudi Arabia
Background: Autoimmunity has been proposed as a cause of narcolepsy. A few studies have assessed comorbid autoimmune diseases in patients with narcolepsy, with conflicting results; however, no study has assessed autoimmune diseases in Arab narcolepsy patients. This study aimed to assess the coexistence of immune-mediated conditions such as allergies, autoimmune diseases, and autoinflammatory diseases in patients with narcolepsy type 1 (with cataplexy) (NT1) and narcolepsy type 2 (without cataplexy) (NT2).
Methods: Personal and family history of autoimmune/autoinflammatory and allergic disorders was collected using a questionnaire in 80 consecutive Saudi patients with narcolepsy (46 NT1 and 24 NT2), who were diagnosed according to the International Classification of Sleep Disorders, Third Edition. The control group comprised 222 adults from the general population.
Results: Comorbid autoimmune/autoinflammatory diseases were reported by 21.4% of the NT1 patients, and 12.2% of the controls, with no significant difference between cases and controls in a model adjusted for confounding covariates. However, allergic disorders were significantly more prevalent among NT1 patients. Both comorbid autoimmune/autoinflammatory and allergic disorders were significantly more prevalent among NT2 patients compared to controls. No differences in demographic and clinical characteristics were detected between narcolepsy patients with and without autoimmune/autoinflammatory diseases.
Conclusion: NT1 is not associated with increased comorbid autoimmune diseases in the studied sample of Saudi patients. However, autoimmune diseases are associated with NT2, and allergic disorders are associated with both NT1 and NT2. These findings suggest the existence of dysregulation in the immune system of narcolepsy patients that requires further research.
Keywords: cataplexy, hypersomnolence, hypersomnia, allergy, narcolepsy
Introduction
Narcolepsy is a lifelong disabling sleep disorder, caused by the selective degeneration of hypocretin (orexin)-producing neurons in the lateral hypothalamus.1 Hypocretin is involved in many physiological functions such as the sleep–wakefulness cycle, appetite, autonomic regulation, and neuroendocrine homeostasis.2 Narcolepsy is characterized by irresistible attacks of sleep. In addition, other symptoms can be present such as cataplexy, hypnagogic or hypnopompic hallucinations, sleep paralysis, and sleep-maintenance insomnia.3 Narcolepsy can be divided into two types, narcolepsy type 1 (with cataplexy) (NT1) and narcolepsy type 2 (without cataplexy) (NT2). Narcolepsy affects around 0.02% of the adults worldwide, with huge variations in prevalence attributed to differences in genetic background.4
NT1 is deeply associated with two HLA-DQ loci—DQA1*01:02, and DQB1*06:02.5 DQB1*06:02 is found in 76–95% of the patients with NT1 and 40–60% of the patients with NT2, but only in 12–38% of the general population.6,7 Other HLA alleles, such as DQB1*03:01 and DQA1*06, are also related to narcolepsy, but to a lesser extent. Using a genome-wide association (GWA) analysis among different ethnic groups, an association was found between polymorphisms in the TCRα (T-cell receptor alpha) locus and narcolepsy.8 The TCR has a critical role in the recognition of antigens bound to HLA molecules. HLA class II molecules (eg, DQB1*06:02) present antigenic peptides to CD4+ T cells, a fact that may indicate a similarity to diabetes and celiac disease, which are T-cell-mediated autoimmune diseases. The fact that the concordance rate of narcolepsy among monozygotic twins is 25–31% implies that other important mechanisms such as environmental factors have a crucial role in the development of the disease.
Although the exact cause of NT1 is not known, the leading hypothesis involves autoimmunity.9 However, it has been shown that autoimmune disease rates are affected by race, ethnicity, socioeconomic status, occupation, and geographic location.10,11 On the other hand, our understanding of the pathophysiology of NT2 and other hypersomnolence disorders with normal hypocretin levels is limited.12
Autoimmune diseases tend to coexist with a prevalence higher than anticipated rates by chance.13 GWA studies have demonstrated that some loci are associated with more than one autoimmune disorder.14 This could be related to shared pathways for T‑cell and B‑cell activation and cytokine signaling.14 It is possible that certain subgroups of autoimmune diseases share etiological similarities and underlying mechanisms of disease.14 Therefore, autoimmune disorders may co-occur in the same individual, which has led researchers to consider different terms such as autoimmune diathesis or kaleidoscope of autoimmunity, both of which point to a common genetic background of autoimmune disorders.15 A few studies have assessed comorbid autoimmune diseases in patients with narcolepsy, with conflicting results;16–18 however, no study has assessed autoimmune diseases in Arab narcolepsy patients. We hypothesized that autoimmune diseases will be higher in Saudi Arabian patients with narcolepsy. Therefore, this case–control study aimed to assess the coexistence of immune-mediated conditions such as allergies, autoimmune diseases, and autoinflammatory diseases in patients with narcolepsy (NT1 and NT2).
Methods
Study design
An observational case–control study was conducted at the University Sleep Disorders Center (USDC) of King Saud University Medical City. Narcolepsy patients and controls were matched for age, sex, and body mass index (BMI).
Both written and informed consent was obtained from all participants, and ethics approval was obtained from the Institutional Review Board in the College of Medicine at King Saud University. The study was conducted in accordance with the Declaration of Helsinki.
Participants
The study included 80 consecutive patients (84% male), with a mean age of 34.6±1.6 years, attending the narcolepsy clinic in the USDC of King Saud University Medical City between September 2016 and December 2017.
A control group of 222 subjects matched for sex, age, and BMI was recruited from the general population, from public places, during the same period. Table 1 presents the demographics on cases and controls.
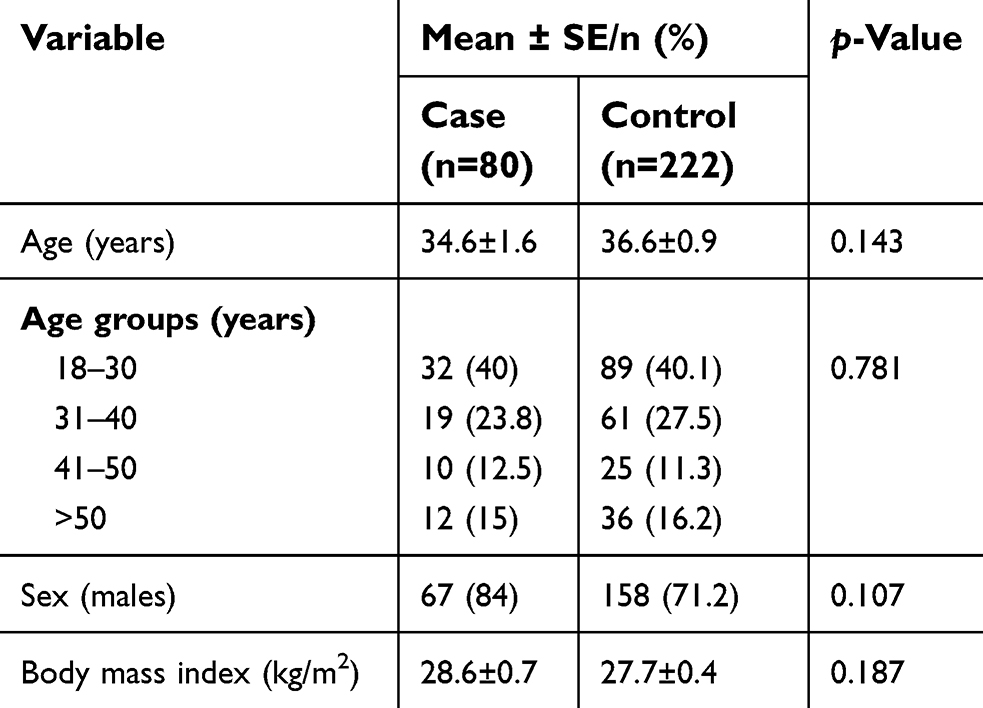 | Table 1 Demographics of narcolepsy patients and controls |
Narcolepsy was diagnosed based on the International Classifications of Sleep Disorders-third edition.19 All patients underwent full polysomnography (PSG) followed by a multiple sleep latency test (MSLT).19 In addition to irresistible attacks of sleep, NT1 was diagnosed by a mean latency of <8 mins on the MSLT with evidence of sleep-onset rapid eye movement periods (SOREMPs) and clear cataplexy (“more than one episode of generally brief (<2 mins), usually bilaterally symmetrical, sudden loss of muscle tone with retained consciousness”).19 NT2 was diagnosed by a mean latency of <8 mins on the MSLT and two SOREMPs (or one SOREMP on PSG and one or more on MSLT), but without cataplexy.19
Data collection
The investigators interviewed the participants using a prestructured questionnaire. The questionnaire items were formulated to evaluate comorbidities chosen on the basis of previous studies.16–18,20–24 Specifically, the questionnaire was used to assess personal or family history of autoimmune diseases and allergic disorders. Additionally, past medical history and the medical reports from other specialists were reviewed. The search included the following autoimmune/autoinflammatory diseases: diabetes mellitus type 1, alopecia areata, Crohn’s disease, primary biliary cirrhosis, autoimmune hepatitis, polymyositis/dermatopolymyositis, myasthenia gravis, Guillain–Barré syndrome, pemphigus, rheumatoid arthritis, systemic lupus erythematosus, Sjögren’s syndrome, autoimmune thyroiditis (Hashimoto’s disease), Addison disease, acute anterior uveitis, Behçet disease, and arthritis. Allergic disorders included asthma, allergic rhinitis, atopic dermatitis, and eczema. Family (first and second degree) history of autoimmune/autoinflammatory diseases and allergic disorders was obtained as well.
Pilot study
A pilot study with 10 patients was conducted to test the clarity of the questions and to estimate the interview time. The interview mean time was 15 mins, and none of the subjects in the pilot group had difficulty understanding the questions.
Statistical analysis
Data were expressed as means±standard error for continuous data and percentages for categorical data. For comparing groups, Pearson’s Chi-squared or two-sided Fisher’s exact test was used for categorical variables, and Student’s t-test for continuous variables with normal distribution. If the normality test failed, we used the Mann–Whitney U test for continuous variables.
We compared personal and family history of autoimmune diseases and allergies, between controls and each narcolepsy type, NT1 and NT2. A univariate logistic regression analysis was used to compare between cases and controls (or NT1 and NT2) for immune-based disease exposure variables. The results of logistic regression analysis were expressed by odds ratios (OR) and their 95% CIs. Adjustments for covariates were performed based on the results of variable comparisons: the adjustments were done only if the univariate analysis showed significant differences. Specifically, for the comparison of NT2 vs NT1, we defined a “model 0” as crude associations and “model 1” adjusted for age and BMI. For the comparison between NT1 and controls, we defined a “model 1” adjusted for age and a “model 2” adjusted for age and BMI. In all comparisons, “model 0” reported only the crude associations.16 The analysis was performed using the Statistical Package for Social Sciences software version 22.0 (SPSS Inc., Chicago, IL, USA). p-Values <0.05 were considered significant.
Ethics statement
Participants were informed about the research aims, objectives, and the mean time of the interview. Both written and informed consent was taken from all participants before beginning the interview. Anonymity was preserved. Ethics approval was obtained from the Institutional Review Board in the College of Medicine at King Saud University. The study was conducted in accordance with the Declaration of Helsinki.
Results
NT1 patients were 56 patients and NT2 were 24 patients. Sleep latency was 2.4±0.1 mins in NT1 patients and 2.8±0.1 mins in NT2 patients (p-value=0.2), and SOREMs occurred in 3.1±0.1 of NT1 patients and 2.8±0.1 of NT2 patients (p-value=0.20).
There were no differences between narcolepsy (NT1+NT2) patients and controls regarding age, sex, and BMI (Table 1). However, when narcolepsy patients were divided into NT1 and NT2, there were some differences between controls and NT1 in age and BMI (Table 2). The mean age at onset of narcolepsy was 19.8±1.1 years.
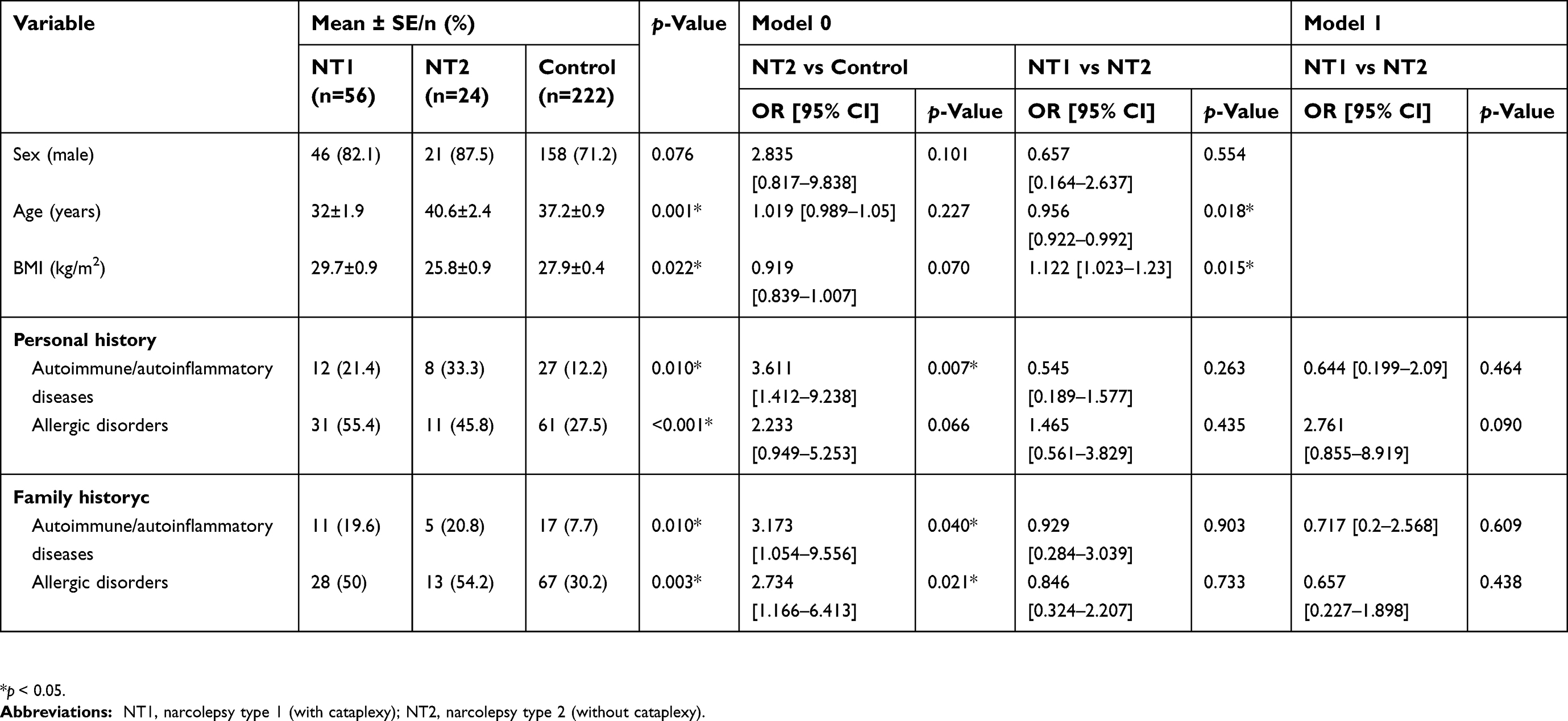 | Table 2 A comparison between the demographic characteristics and personal and family history of autoimmune diseases and allergic disorders in narcolepsy NT1, NT2, and controls |
Comorbid autoimmune diseases in patients with NT1
Table 3 presents the number of autoimmune/autoinflammatory diseases and allergic disorders in patients with NT1, NT2, and controls. History of autoimmune/autoinflammatory diseases and allergic disorders was reported by 21.4% and 55.4% of the NT1 patients and 12.2% and 27.5% of the controls, respectively. Compared with controls, patients with NT1 were older and had higher BMI. After adjusting for age and BMI, allergic disorders were significantly more prevalent among patients with NT1 in the crude and adjusted analysis (OR 3.208, 95% CI 1.724–5.97, model 2) (Table 4). With regard to autoimmune disease comorbidity, after adjusting for age and BMI, there was no significant difference between NT1 patients and controls. However, family history of autoimmune diseases and allergic disorders was significantly more prevalent in patients with NT1 in both the crude and the adjusted analysis.
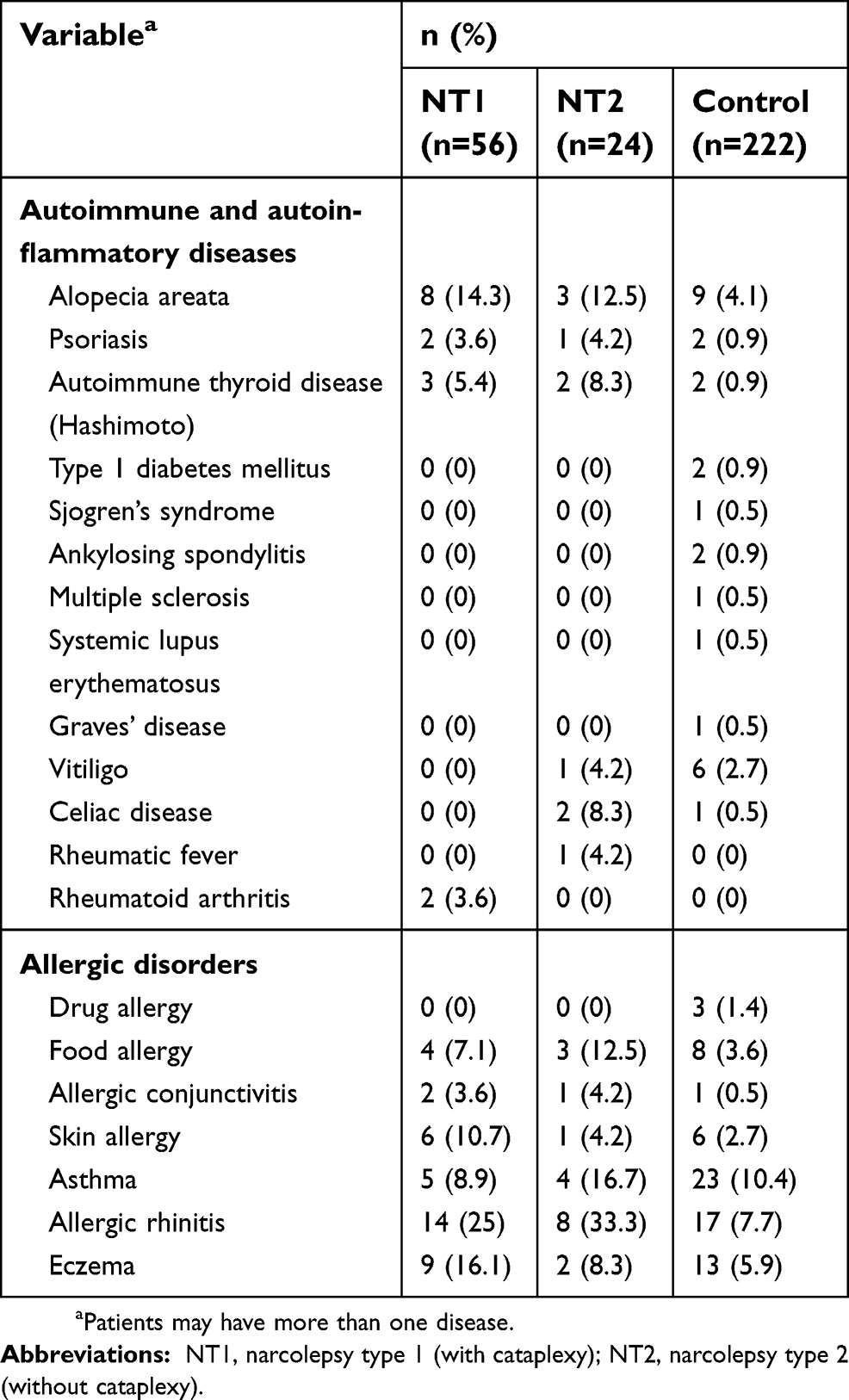 | Table 3 Number of autoimmune/autoinflammatory diseases and allergic disorders in NT1, NT2, and control groups |
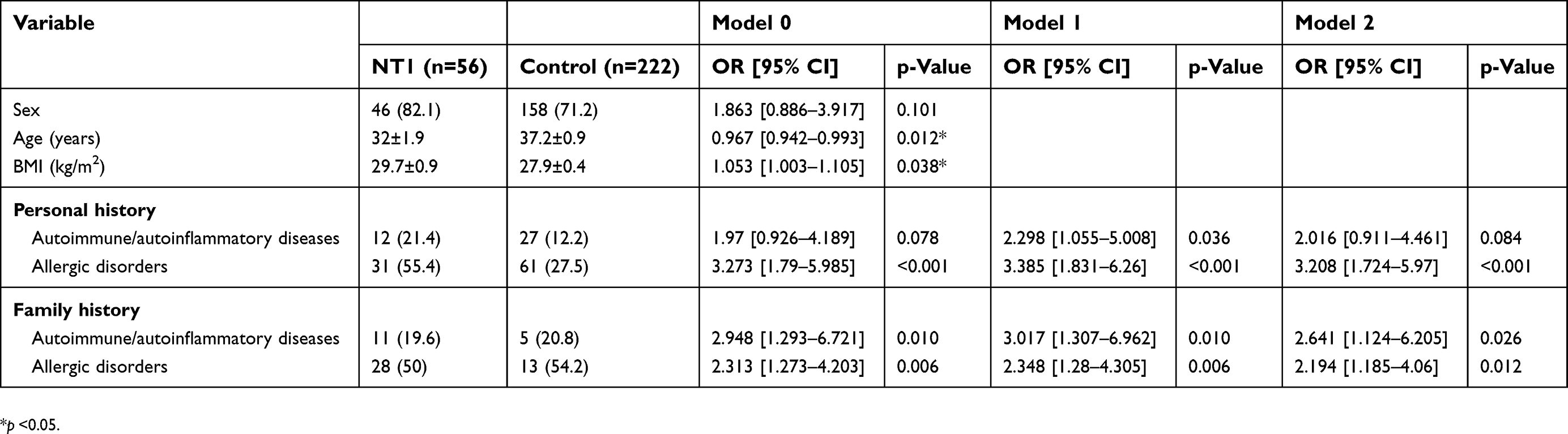 | Table 4 A comparison between the demographic characteristics and personal and family history of autoimmune diseases and allergic disorders in narcolepsy type 1 (NT) and controls |
Comorbid autoimmune diseases in patients with NT2
Among patients with NT2, autoimmune/autoinflammatory diseases were reported by 33.3% and allergic disorders in 45.8% of the cases (Table 2). Compared with controls, history of autoimmune/autoinflammatory diseases, history of allergic disorders, family history of autoimmune/autoinflammatory diseases, and family history of allergic disorders were all significantly associated with NT2.
Comparison between narcolepsy patients with and without autoimmune disorders
Table 5 presents a comparison between narcolepsy patients with and without autoimmune disorders. No significant differences were found regarding sex, BMI, or the presence of cataplexy.
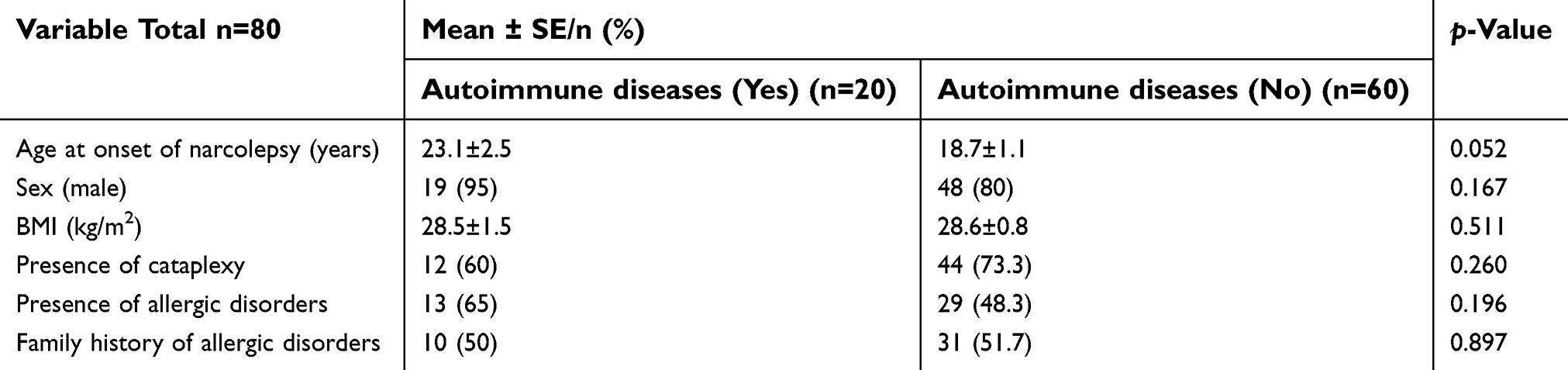 | Table 5 Comparison between narcolepsy patients with and without autoimmune/autoinflammatory diseases |
Discussion
Patients with NT2 showed significantly higher prevalence of allergies and autoimmune/autoinflammatory diseases compared to controls, and NT1 patients showed higher prevalence of allergic disorders compared to controls. However, after adjusting for age and BMI, there was no association between NT1 and autoimmune/autoinflammatory diseases.
Three recent studies have evaluated the association between narcolepsy and autoimmune diseases.16–18 Our findings concur with those by Barateau et al and are in contrast with those by Martínez-Orozco et al.16–18 In a French case–control study, Barateau et al compared the frequencies of personal and family history of autoimmune diseases and allergies in consecutive patients, adults and children, with NT1, NT2, and idiopathic hypersomnia, and healthy controls.16 The results demonstrated that NT1 is not associated with increased risk of autoimmune disorders. However, similar to our data, the investigators reported higher frequency of autoimmune diseases in NT2 patients compared to controls.16 In their first retrospective study, Martínez-Orozco et al reviewed the past medical history and the medical reports of patients with narcolepsy.18 They did not divide the study group into NT1 and NT2. The investigators reported that narcolepsy patients are more predisposed to immunopathological diseases (autoimmune diseases and allergies).18 In the studied sample, 16% of the patients had at least one immunopathological disease, with the predominance of allergic disorders over autoimmune conditions.18 However, the study had no control group. In their second observational retrospective case–control study, Martínez-Orozco et al studied 158 Caucasians NT1 patients with associated autoimmune diseases and those without any association within the same series, and 151 control subjects matched by gender and age.17 Thirty out of 158 patients had one or more coexisting autoimmune diseases. Analysis of data revealed a higher frequency of autoimmune diseases in NT1 patients compared with controls (OR 3.17; 95% CI: 1.01–10.07; p=0.04).17 The differences between these studies may reflect genetic and racial differences between the populations. Additionally, there is growing evidence suggesting that autoimmune diseases likely result from interactions between genetic and environmental factors, and that environmental factors may significantly contribute to the risk of disease initiation and propagation.25
The exact cause of NT1 is not clear; however, current indirect evidence suggests that an autoimmune mechanism is the likely cause.26 Our results concur with those of Barateau et al, suggesting that NT1 may not have the same risk and susceptibility as other autoimmune diseases.16 It is possible that NT1 has a unique pathophysiology that is not associated with an increased risk of other autoimmune diseases.16 Nevertheless, family history of autoimmune diseases was higher in NT1 patients than in controls, pointing to a possible increase in family susceptibility to autoimmune diseases that could be related to the HLA genotype.16 The association between NT2 (a disorder with unknown underlying pathophysiology) and autoimmune diseases in our study and in that by Barateau et al suggests a propensity to activate the immune system in NT2.16,27 More studies from different parts of the world are needed to confirm these findings and to explore the underlying mechanisms.
Although the prevalence of psoriasis and autoimmune thyroid disease in the current study was higher in patients with narcolepsy than in controls, it actually lies within the prevalence reported in the general Saudi population.28,29 On the other hand, alopecia areata was common among patients with narcolepsy (both NT1 [14.3%] and NT2 [12.5%]). Several case reports have described the coexistence of alopecia areata and narcolepsy.30–32 A recent study reported a prevalence of alopecia areata in Saudi men and women of 6.750% and 6.375%, respectively.33 The association between alopecia areata and narcolepsy needs further research to elucidate the underlying mechanisms.
In the current study, allergic disorders were more common among NT1 and NT2 patients compared to controls. A retrospective chart review of childhood narcolepsy pediatric patients was conducted at three major pediatric sleep centers in the US, France, and Taiwan and included 468 children with narcolepsy.34 The investigators reported an increased frequency of allergic disorders.34 Interestingly, the study found that allergic disorders, particularly asthma and allergic rhinitis, were markedly lower in NT1 compared to NT2.34 However, the study had no control group. The authors suggest that T-helper-2 (Th2) cellular hyperactivation against autoantigens would cause IgE-mediated allergy.34 The authors also hypothesize that the presence of a shift toward Th2 in the Th1:Th2 balance, as indicated by the presence of allergic conditions, may modify the severity of the disorder in childhood narcolepsy, reduce the prevalence of cataplexy in these patients, and potentially dampen the severity of the disorder even among the patients with cataplexy.34 Although autoimmune and allergic disorders both represent immunological dysregulations, it remains controversial whether allergies tend to co-occur with autoimmune diseases.35
The current study has some merits and limitations. The patients were diagnosed in a major referral central for patients with central hypersomnolence disorders in the country. Additionally, this is the first study to report comorbid autoimmune diseases and allergic disorders in an Arab population. Limitations include the fact that the age of onset of autoimmune diseases was not documented in this study. Additionally, HLA typing was not reported. Moreover, immune diseases and allergic disorders were self-reported, although we also reviewed medical records and specialists reports to check for documented disorders. Previous studies that assessed comorbid autoimmune disorders used a similar method.16–18 Finally, the sample size is relatively small, which may not have adequate power to address differences between the narcolepsy and control groups.
Conclusions
In summary, this study showed that NT1 was not associated with increased comorbid autoimmune/autoinflammatory diseases in the studied sample. This finding concurs with a recent French study and may reflect a unique pathophysiology of NT1.16 However, larger studies are needed to confirm the current findings.
On the other hand, autoimmune diseases were associated with NT2, and allergic disorders were associated with both NT1 and NT2. This result suggests a dysregulation in the immune system in narcolepsy patients, which needs further research to explore the clinical and genetic associations between narcolepsy and autoimmune and allergic disorders. Moreover, prospective multiethnic studies from different geographical regions of the world are needed to explore the immunophenotype and potential associations with HLA markers such as DQB1*06:02.
Abbreviation list
NT1, narcolepsy type 1; NT2, narcolepsy type 2; GWA, genome-wide association; BMI, body mass index; ICSD-3, International Classifications of Sleep Disorders-third edition; PSG, polysomnography; MSLT, multiple sleep latency test; SOREMP, sleep-onset rapid eye movement period; SD, standard deviation; OR, odds ratio; CI, confidence interval.
Acknowledgments
This study was supported by a grant from the College of Medicine Research Center, Deanship of Scientific Research, King Saud University Project, Saudi Arabia. The grant was obtained by Prof. Ahmed S. BaHammam. The study sponsors played no role in the study design; collection, analysis, or interpretation of the data; writing of the manuscript; or decision to submit the manuscript.
Author contributions
MA: Conception of idea, data collection, writing the manuscript. ASA: Data analysis, writing the manuscript, final edit and approval of the manuscript. AHO: Data analysis, writing the manuscript. ASB: Conception of idea, data collection, securing grant, data analysis, writing the manuscript, final edit and approval of the manuscript. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Savvidou A, Knudsen S, Olsson-Engman M, Gammeltoft S, Jennum P, Palm L. Hypocretin deficiency develops during onset of human narcolepsy with cataplexy. Sleep. 2013;36(1):147–148. doi:10.5665/sleep.2320
2. Dalal J, Roh JH, Maloney SE, et al. Translational profiling of hypocretin neurons identifies candidate molecules for sleep regulation. Genes Dev. 2013;27(5):565–578. doi:10.1101/gad.207654.112
3. Arango M-T, Kivity S, Shoenfeld Y. Is narcolepsy a classical autoimmune disease? Pharmacol Res: official J Italian Pharmacol Society. 2015;92:6–12. doi:10.1016/j.phrs.2014.10.005
4. Dauvilliers Y, Arnulf I, Mignot E. Narcolepsy with cataplexy. Lancet (London, England). 2007;369(9560):499–511. doi:10.1016/S0140-6736(07)60237-2
5. Mignot E, Hayduk R, Black J, Grumet FC, Guilleminault C. HLA DQB1*0602 is associated with cataplexy in 509 narcoleptic patients. Sleep. 1997;20(11):1012–1020.
6. Hor H, Kutalik Z, Dauvilliers Y, et al. Genome-wide association study identifies new HLA class II haplotypes strongly protective against narcolepsy. Nat Genet. 2010;42(9):786–789. doi:10.1038/ng.647
7. Al Shareef SM, AlAnbay E, AlKhathlan MA, et al. HLA-DQB1*06:02 allele frequency and clinic-polysomnographic features in Saudi Arabian patients with narcolepsy. Sleep Breath. 2018;1–7.
8. Hallmayer J, Faraco J, Lin L, et al. Narcolepsy is strongly associated with the T-cell receptor alpha locus. Nat Genet. 2009;41(6):708–711. doi:10.1038/ng.372
9. De la Herran-Arita AK, Garcia-Garcia F. Narcolepsy as an immune-mediated disease. Sleep Disord. 2014;2014:792687. doi:10.1155/2014/792687
10.
11. Hughes JW, Riddlesworth TD, DiMeglio LA, et al. Autoimmune diseases in children and adults with type 1 diabetes from the T1D Exchange Clinic Registry. J Clin Endocrinol Metab. 2016;101(12):4931–4937. doi:10.1210/jc.2016-2478
12. Mignot E, Lammers GJ, Ripley B, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch Neurol. 2002;59(10):1553–1562.
13. Somers EC, Thomas SL, Smeeth L, Hall AJ. Are individuals with an autoimmune disease at higher risk of a second autoimmune disorder? Am J Epidemiol. 2009;169(6):749–755. doi:10.1093/aje/kwn408
14. Richard-Miceli C, Criswell LA. Emerging patterns of genetic overlap across autoimmune disorders. Genome Med. 2012;4(1):6. doi:10.1186/gm305
15. Rojas-Villarraga A, Amaya-Amaya J, Rodriguez-Rodriguez A, Mantilla RD, Anaya JM. Introducing polyautoimmunity: secondary autoimmune diseases no longer exist. Autoimmune Dis. 2012;2012:254319.
16. Barateau L, Lopez R, Arnulf I, et al. Comorbidity between central disorders of hypersomnolence and immune-based disorders. Neurology. 2017;88(1):93–100. doi:10.1212/WNL.0000000000003432
17. Martinez-Orozco FJ, Vicario JL, De Andres C, Fernandez-Arquero M, Peraita-Adrados R. Comorbidity of narcolepsy type 1 with autoimmune diseases and other immunopathological disorders: a case-control study. J Clin Med Res. 2016;8(7):495–505. doi:10.14740/jocmr2569w
18. Martínez-Orozco FJ, Vicario JL, Villalibre-Valderrey I, De Andrés C, Fernández-Arquero M, Peraita-Adrados R. Narcolepsy with cataplexy and comorbid immunopathological diseases. J Sleep Res. 2014;23(4):414–419. doi:10.1111/jsr.12143
19.
20. Jennum P, Ibsen R, Knudsen S, Kjellberg J. Comorbidity and mortality of narcolepsy: a controlled retro- and prospective national study. Sleep. 2013;36(6):835–840. doi:10.5665/sleep.2706
21. Ohayon MM. Narcolepsy is complicated by high medical and psychiatric comorbidities: a comparison with the general population. Sleep Med. 2013;14(6):488–492. doi:10.1016/j.sleep.2013.03.002
22. Vignatelli L, Plazzi G, Peschechera F, Delaj L, D’Alessandro R. A 5-year prospective cohort study on health-related quality of life in patients with narcolepsy. Sleep Med. 2011;12(1):19–23. doi:10.1016/j.sleep.2010.07.008
23. Kok SW, Overeem S, Visscher TLS, et al. Hypocretin deficiency in narcoleptic humans is associated with abdominal obesity. Obes Res. 2003;11(9):1147–1154. doi:10.1038/oby.2003.156
24. Fortuyn HAD, Mulders PC, Renier WO, Buitelaar JK, Overeem S. Narcolepsy and psychiatry: an evolving association of increasing interest. Sleep Med. 2011;12(7):714–719. doi:10.1016/j.sleep.2011.01.013
25. Jorg S, Grohme DA, Erzler M, et al. Environmental factors in autoimmune diseases and their role in multiple sclerosis. Cell Mol Life Sci. 2016;73(24):4611–4622. doi:10.1007/s00018-016-2311-1
26. Barateau L, Liblau R, Peyron C, Dauvilliers Y., Narcolepsy type 1 as an autoimmune disorder: evidence, and implications for pharmacological treatment. CNS Drugs. 2017;31(10):821–834. doi:10.1007/s40263-017-0464-6
27. Baumann CR, Mignot E, Lammers GJ, et al. Challenges in diagnosing narcolepsy without cataplexy: a consensus statement. Sleep. 2014;37(6):1035–1042. doi:10.5665/sleep.3756
28. Fatani MI, Abdulghani MH, Al-Afif KA. Psoriasis in the eastern Saudi Arabia. Saudi Med J. 2002;23(2):213–217.
29. Akbar DH, Ahmed MM, Al-Mughales J. Thyroid dysfunction and thyroid autoimmunity in Saudi type 2 diabetics. Acta Diabetol. 2006;43(1):14–18. doi:10.1007/s00592-006-0204-8
30. Dominguez Ortega L. [Narcolepsy and alopecia areata: a new association?]. An Med Interna. 1992;9(5):234–236.
31. King LE
32. Nigam G, Pathak C, Riaz M. Alopecia areata and narcolepsy: a tale of obscure autoimmunity. BMJ Case Rep. 2016;2016:bcr2015211523.
33. Ama AE, Maghrabi IA. Prevalence and treatment of Alopecia areata in Taif area, KSA. Saudi J Health Sci. 2015;4:125–128. doi:10.4103/2278-0521.157891
34. Aydinoz S, Huang Y-S, Gozal D, Inocente CO, Franco P, Kheirandish-Gozal L., Allergies and disease severity in childhood narcolepsy: preliminary findings. Sleep. 2015;38(12):1981–1984. doi:10.5665/sleep.5254
35. Shah A. The pathologic clinical intersection of atopic and autoimmune disease. Curr Allergy Asthma Rep. 2012;12(6):520–529. doi:10.1007/s11882-012-0293-0
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.