Back to Journals » Journal of Pain Research » Volume 11
Immune function after major surgical interventions: the effect of postoperative pain treatment
Authors Amodeo G ![]() , Bugada D
, Bugada D ![]() , Franchi S, Moschetti G
, Franchi S, Moschetti G ![]() , Grimaldi S, Panerai A
, Grimaldi S, Panerai A ![]() , Allegri M
, Allegri M ![]() , Sacerdote P
, Sacerdote P ![]()
Received 27 November 2017
Accepted for publication 1 April 2018
Published 10 July 2018 Volume 2018:11 Pages 1297—1305
DOI https://doi.org/10.2147/JPR.S158230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Giada Amodeo,1 Dario Bugada,2–4 Silvia Franchi,1 Giorgia Moschetti,1 Stefania Grimaldi,5 Alberto Panerai,1 Massimo Allegri,2 Paola Sacerdote1
1Department of Pharmacological and Biomolecular Sciences, University of Milano, Milano, Italy; 2Study In Multidisciplinary Pain Research Group, 3Department of Anesthesia and ICU, ASST Papa Giovanni XXIII, Bergamo, Italy; 4Department of Anesthesia and ICU, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy; 5Department of Anesthesia, IRCCS Humanitas Research Center, Rozzano, Italy
Introduction: Impaired immune function during the perioperative period may be associated with worse short- and long-term outcomes. Morphine is considered a major contributor to immune modulation.
Patients and methods: We performed a pilot study to investigate postoperative immune function by analyzing peripheral blood mononuclear cells’ functionality and cytokine production in 16 patients undergoing major abdominal surgery. All patients were treated with intravenous (i.v.) patient-controlled analgesia with morphine and continuous wound infusion with ropivacaine+methylprednisolone for 24 hours. After 24 hours, patients were randomized into two groups, one continuing intrawound infusion and the other receiving only i.v. analgesia. We evaluated lymphoproliferation and cytokine production by peripheral blood mononuclear cells at the end of surgery and at 24 and 48 hours postoperatively.
Results: A significant reduction in TNF-α, IL-2, IFN-γ and lymphoproliferation was observed immediately after surgery, indicating impaired cell-mediated immunity. TNF-α and IFN-γ remained suppressed up to 48 hours after surgery, while a trend to normalization was observed for IL-2 and lymphoproliferation, irrespective of the treatment group. A significant inverse correlation was present between age and morphine and between age and lymphoproliferation. No negative correlation was present between morphine and cytokine production. We did not find any differences within the two groups between 24 and 48 hours in terms of morphine consumption and immune responses.
Conclusion: A relevant depression of cell-mediated immunity is associated with major surgery and persists despite optimal analgesia. Even though morphine may participate in immunosuppression, we did not retrieve any dose-related effect.
Keywords: opioids, postoperative pain, cytokines, immunomodulation, lymphoproliferation, surgery
Introduction
The perioperative period of any major surgery is accompanied by immune suppression that results from the interaction of several factors, including drugs used for postoperative pain control.1–4 An impaired immune system in the perioperative period has important clinical implications because it is associated with an increased risk of developing postoperative infections and sepsis.4,5 Furthermore, the cell-mediated immunity is important in cancer surgery for reducing metastatic spread.3,6–9 On one hand, surgical stress can activate the sympathetic nervous system (SNS) and the hypothalamic–pituitary–adrenal (HPA) axis to induce the neuroendocrine response,1,4 which inhibits T-cell responses; following major surgery, cellular immunity remains suppressed for several days and cytokine production is profoundly affected.4,10 On the other hand, pain itself is immune depressant; appropriate postoperative pain control is therefore mandatory, and opioids are often used as intra- and postoperative analgesics.
However, opioids (morphine in particular) have consistently been considered as important factors responsible for immune modulation in the perioperative period.8,11–16
Experimental and clinical data indicate that morphine exerts immunosuppressive activity, decreasing innate and both cell-mediated and humoral adaptive immunity, acting on lymphocytes and macrophages. Opioids have been shown to affect nearly all aspects of the immune system including macrophages, neutrophils, T cells and NK cells.11 Cellular immunity, the system primarily responsible for host antitumor defense, is suppressed with both acute and chronic opioid exposure. Opioids modulate immune function by either interacting directly in the periphery with mu-opioid receptors (MOR) expressed by lymphocytes and mononuclear phagocytes or activating central MOR that can stimulate HPA axis.17–20
Since opioid-induced immune effects are dose related,21,22 reduced morphine intake toward opioid-sparing perioperative care could be beneficial, especially in oncologic surgery.21–26
For these reasons, in this pilot study (included in a larger clinical trial on multimodal analgesia), functional measurement of immune responses (lymphoproliferation, T-helper 1/2 – Th1/Th2 and macrophage cytokine production) was performed in patients undergoing major surgery to investigate the effects of surgical stress and opioids on perioperative immune function.
Patients and methods
Patients
This pilot study was performed on a smaller sample of patients enrolled in a Phase III, double-blind, randomized clinical trial investigating the efficacy and safety of prolonged continuous wound infusion (CWI) after major abdominal surgery. A total of 16 patients, American Society of Anesthesiologists’ I–II–III, scheduled to use patient-controlled analgesia (PCA) with morphine for postoperative pain control after major abdominal surgery for cancer (biliopancreatic, hepatic, bowel cancers) were enrolled. Regular use of opioid analgesics and immunosuppressant drugs, history of drugs and/or alcohol abuse, postoperative hospitalization in intensive care with sedation and/or mechanical ventilation, neurological disorders, any heart conduction disease, any cognitive or mental disorder hindering to sign an informed consent, body mass index >30, diabetes (type I or II), allergy to study drugs and use of epidural analgesia were exclusion criteria.
On the day of surgery, patients were provided with standard monitoring (electrocardiography [ECG], oxygen saturation, noninvasive blood pressure) plus invasive pressure monitoring.
The study was approved by the ethical committee of each participating center (Fondazione IRCCS Policlinico San Matteo, Pavia; University Hospital, Parma and Humanitas Research Center, Milan), and all patients signed a written informed consent. The trial was registered on Clinicaltrials.gov (NCT02002663 – Principal Investigator Massimo Allegri, MD).27
Three centers were involved, but all the analyses that are part of the current study were carried on consecutive patients enrolled between April 2015 and July 2016 at Humanitas Research Center, Milan.
Since functional measures need fresh blood to be reliable, this choice was made to quickly deliver fresh blood samples from the closest hospital to the research laboratory (Milan University).
The primary end point of this pilot study was to evaluate immune responses and their correlation with opioid consumption in the first 24 hours. The secondary end point was to evaluate immune response in the second day of treatment according to the allocation group, and its correlation with opioid consumption.
We also investigated correlation between immune responses and age or sex.
Treatments
Details about the main randomized controlled trial (RCT), including inclusion and exclusion criteria, treatments, clinical evaluations and randomization/allocation/blinding are included in our previously published article.27 We summarize here only those information that are relevant to the current study.
Patients received general anesthesia and intraoperative analgesia with opioids (either fentanyl 0.2 µg/kg and/or remifentanil 0.1–0.25 mg/kg/min). All patients received morphine (0.15 mg/kg) 30–45 minutes before the end of surgery and were then all treated with an intravenous PCA with morphine and ketorolac (8 mg) for the next 48 hours, regardless of the allocation group. An infusion catheter (Plan1-Health PAINfusor®; Plan1Health s.r.l. Udine, Italy) was placed by the surgeon in the fascial plane between peritoneum and transversalis fascia, and 10 mL of 0.2% ropivacaine was administered immediately after muscular plane closure; the catheter was then connected to an electronic pump (CADD®-Solis; Smith’s Medical Italia, Latina Scalo, Italy). All patients were infused with the same active treatment (ropivacaine 0.2%+methylprednisolone 1 mg/kg, 10 mL/h) for 24 hours and were then randomized to receive either active treatment (Group A: ropivacaine 0.2%+methylprednisolone 1 mg/kg, 10 mL/h) or placebo (Group B: saline 10 mL/h). On a daily basis, all patients were evaluated after surgery by the acute pain service (APS) and twice a day by the surgeons as part of their current clinical practice. Pain values, analgesic consumption, any drug-related side effect and catheter-related complication (such as occlusion and dislodgment) were recorded. Pain at rest and pain at movement (i.e., coughing and deep inspiration) were evaluated by Numeric Rating Scale (NRS; 11-point scale, from 0=no pain to 10=worst imaginable pain).
Blood sample collection
Blood samples were taken before anesthesia induction, at the end of surgery and at 24 and 48 hours from the end of surgery and collected in EDTA-containing vials. All blood samples were analyzed within 24 hours of collection.
Mononuclear cell cultures
Peripheral blood mononuclear cells (PBMC) were isolated using Ficoll-Paque Premium (GE Healthcare Bio-Sciences AB, Uppsala, Sweden). Cells viability was checked by trypan blue exclusion test.
PBMC were diluted in Roswell Park Memorial Institute (RPMI)-1640+10% fetal calf serum (FCS) at the final concentration of 2×106 (1 mL/well) and dispensed into 24-well culture plates. PBMC were incubated with or without 1 μg/mL lipopolysaccharide, which is considered as a preferential activator of the monocyte/macrophage lineage, for IL-1β, IL-10 and TNF-α stimulation and with 10 µg/mL phytohemagglutinin (PHA) for Th1 (IL-2, IFN-γ) and Th2 (IL-4, IL-10) cytokine stimulation. The stimuli were added to cultures in a final volume of 1 mL/well in RPMI-1640 plus 10% FCS, 1% glutamine, 2% streptomycin solution and 0.1% 2-mercaptoethanol (complete RPMI). After 24 hours of culture at 37°C in 5% CO2 and 95% air, the supernatants were collected and stored at -80°C for cytokine evaluation.28
Enzyme-linked immunosorbent assay (ELISA)
Cytokine concentration was determined using ultra-sensitive ELISA kits according to the manufacturer’s instructions. ELISA Ready-Set-Go! systems for human IL-1β, IL-10, TNF-α, IL-2, IFN-γ and IL-4 were purchased from eBioscience (San Diego, CA, USA). Cytokines produced are reported as concentrations in culture media of stimulating cells (pg/mL).
Lymphocyte proliferation
Lymphoproliferation was assessed before surgery, at the end of surgery and 48 hours postoperatively.
In vitro lymphocyte proliferation was analyzed using 5-bromo-2′-deoxyuridine (BrdU) labeling of DNA-synthesizing cells using FITC BrdU Flow Kit (BD PharmingenTM, San Diego, CA, USA). In all, 106 lymphocytes were seeded in complete RPMI with or without 10 µg/mL PHA at the final volume of 1 mL in 5 mL sterile tubes. All samples were tested in duplicate. After 48 hours of culture at 37°C in 5% CO2 and 95% air in the presence or absence of PHA, BrdU labeling reagent (final concentration: 10 μM) was added and cells were cultured for further 24 hours. Cells were processed according to manufacturer’s instructions and then fixed for 30 minutes and incubated with anti-BrdU for 30 minutes at room temperature. Cells were resuspended in 1 mL of staining buffer (Dulbecco’s PBS+3% FCS+0.09% sodium azide) and analyzed by cytofluorimetric analysis. Culture medium, cells cultured without PHA and cells incubated with anti-BrdU in the absence of BrdU were used as controls.
A cytofluorimetric analysis of fluorescent cells (FITC-BrdU positive cells) evaluated the percentage of cells that have incorporated BrdU. All flow cytometry analysis was performed by FACS Calibur flow cytometer (488Ex/620Em; Becton Dickinson, San Jose, CA, USA) acquiring a maximum of 20×105 cells/sample.
Statistical analysis
Results are presented as mean±standard error of mean (SEM). Normality of data distribution was assessed by the Jarque–Bera test. Statistical analyses were performed using one-way analysis of variance (ANOVA) for parametric results, when indicated follow-up analysis was performed using Bonferroni post tests for multiple comparisons. Paired Student’s t-test was used for the comparison between two groups; to assess possible correlations, Pearson correlation test was used. All the statistical analysis were performed using GraphPad Prism 5 Software (GraphPad Software, Inc., La Jolla, CA, USA). Differences were considered as significant at p<0.05.
Since treatment was the same in both groups in the first 24 hours, we considered all patients as one group and differentiated between two groups only for the second postoperative day (24–48 hours from surgery).
Results
A total of 16 patients were included in the study (mean age 64±11 years, mean±SD; eight males/eight females): nine patients were randomized to Group A (mean age 63.8±11.7 years; six males/three females) and seven patients to Group B (mean age 63.4±12.74 years; two males/five females). Duration of surgery for each patient is reported in Table 1. Only one of the 16 patients needed blood transfusions preoperatively (Group A), while three patients received intraoperative transfusion (two in Group A and one in Group B). Since immune parameters of transfused patients were never different from those of non-transfused one (data not shown), we did not exclude them from the analysis. Patients reported good pain relief all along the postoperative period, as shown by NRS values at rest and movement (Figure 1). No significant differences between groups were observed.
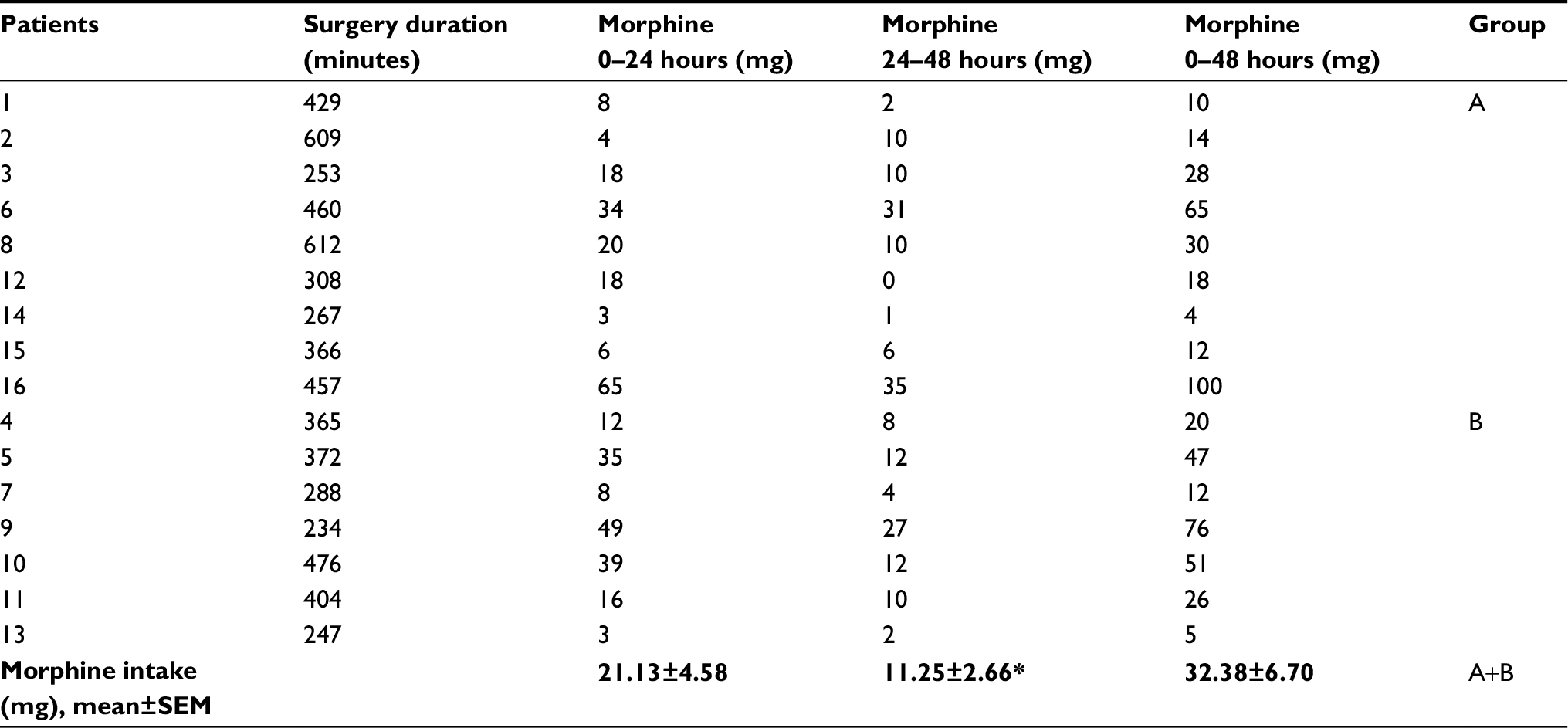 | Table 1 Duration of surgery and individual morphine consumption of patients at the different times of the study Notes: *p<0.05 v.s. 0–24 hours (paired t-test). Active treatment (Group A: ropivacaine 0.2%+methylprednisolone 1 mg/kg, 10 mL/h); placebo (Group B: saline 10 mL/h). Abbreviation: SEM, standard error of mean. |
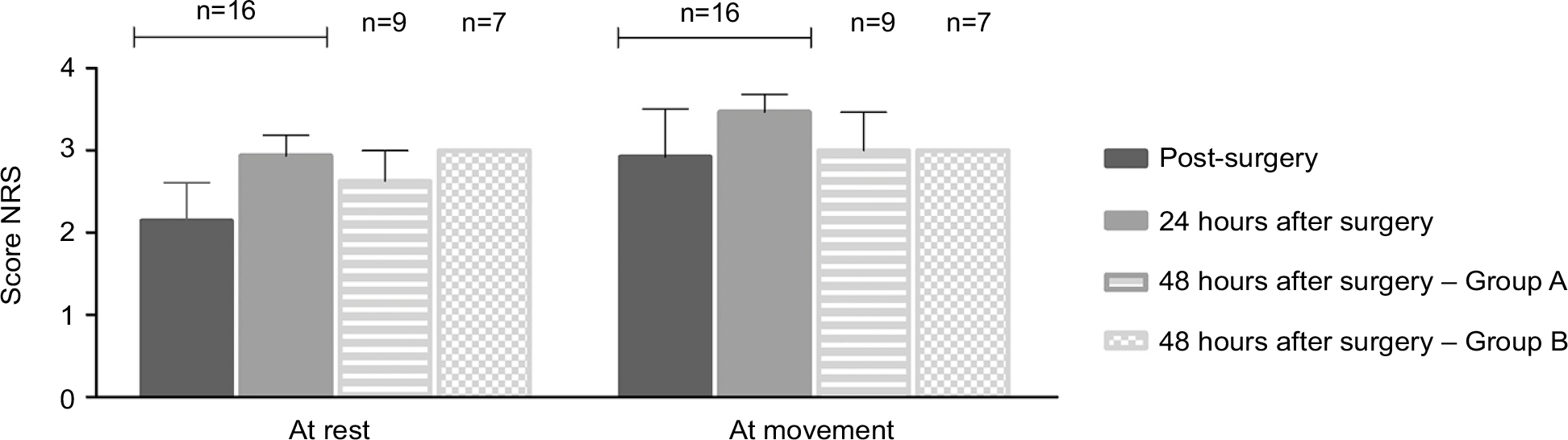 | Figure 1 At rest and movement NRS values recorded immediately after the end of surgery and 24 and 48 hours later. Notes: Data from post- and 24 hours after surgery include all patients (n=16), while data at 48 hours represent patients divided into Group A (n=9) or Group B (n=7). Values are mean±SEM. Active treatment (Group A: ropivacaine 0.2%+methylprednisolone 1 mg/kg, 10 mL/h); placebo (Group B: saline 10 mL/h). Abbreviations: NRS, Numeric Rating Scale; SEM, standard error of mean. |
Cytokines
Figure 2 reports the production of cytokines after in vitro stimulation with lipopolysaccharide.
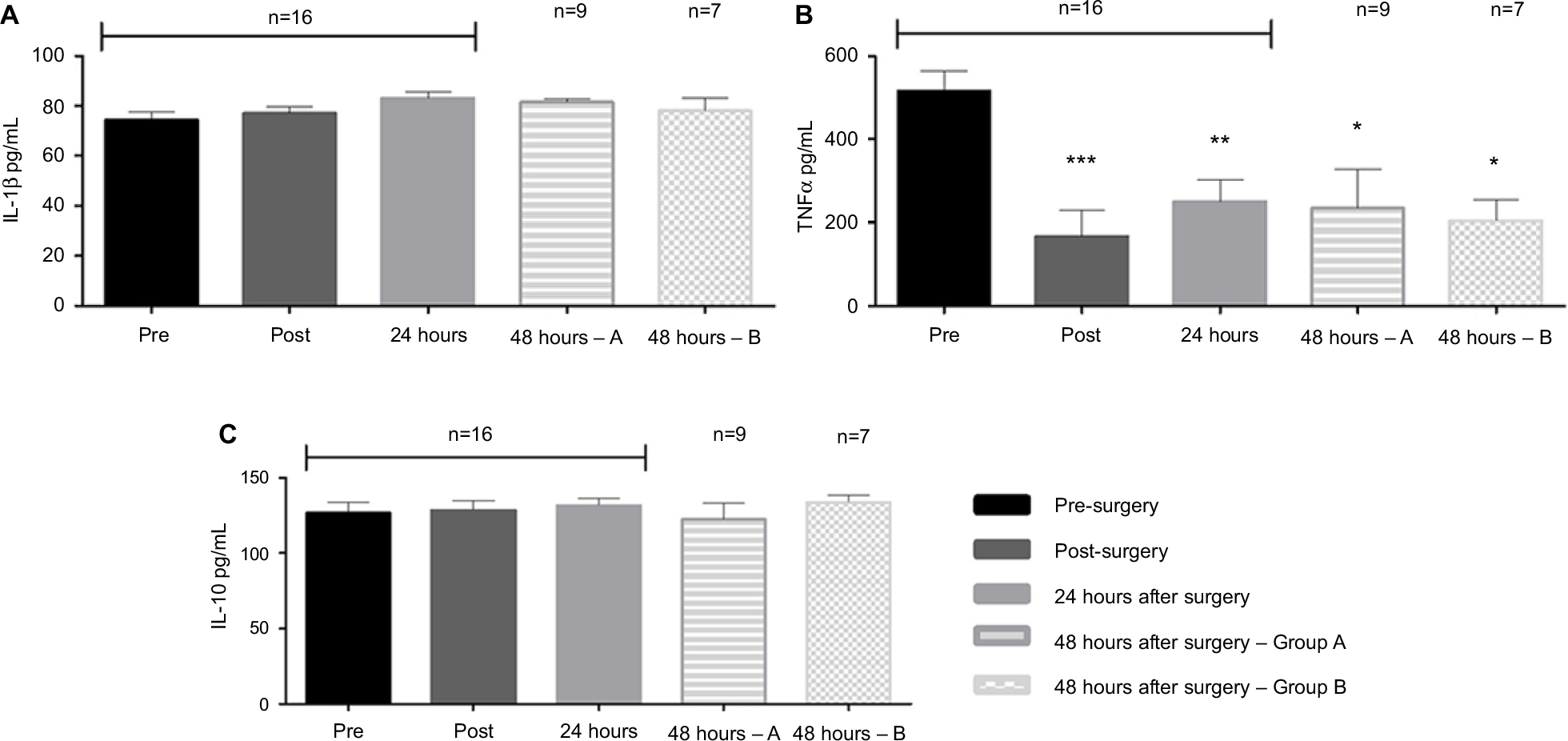 | Figure 2 Cytokine levels released by PBMC after LPS stimulation. Notes: Blood samples were obtained before surgery, immediately after the end of surgery and 24 and 48 hours later. PBMC were stimulated in vitro for 24 hours with 1 µg/mL LPS, and IL-β (A), TNF-α (B) and IL-10 (C) released in media were evaluated by ELISA. Data from pre-, post- and 24 hours after surgery include all patients (n=16), while data at 48 hours represent patients divided into Group A (n=9) or Group B (n=7) (refer the “Patients and methods” section). Values are mean±SEM. *p<0.05, **p<0.01 and ***p<0.001 v.s. presurgery cytokine levels. Active treatment (Group A: ropivacaine 0.2%+methylprednisolone 1 mg/kg, 10 mL/h); placebo (Group B: saline 10 mL/h). Abbreviations: PBMC, peripheral blood mononuclear cells; LPS, lipopolysaccharide; ELISA, enzyme-linked immunosorbent assay; SEM, standard error of mean. |
As reported in Figure 2A, surgery does not influence the production of the proinflammatory cytokine IL-1β, which remains unmodified along the 48 hours of observation, without any significant difference between the two groups. In contrast, the other relevant proinflammatory cytokine TNF-α (Figure 2B) is significantly decreased after the surgery, and the levels remained lower than preoperatively also at 24 and 48 hours in both Group A and Group B. Figure 2C shows the production of the anti-inflammatory cytokine IL-10, which is not altered at any time.
Data on Th1 and Th2 cytokine production are reported in Figure 3. Both IFN-γ (Figure 3A) and IL-2 (Figure 3B), typical Th1 cytokines, are significantly reduced at the end of surgery. IFN-γ remains reduced after 24 and 48 hours, irrespective of the allocation group, while a trend toward normalization was observed for IL-2 at 24 and 48 hours in both groups.
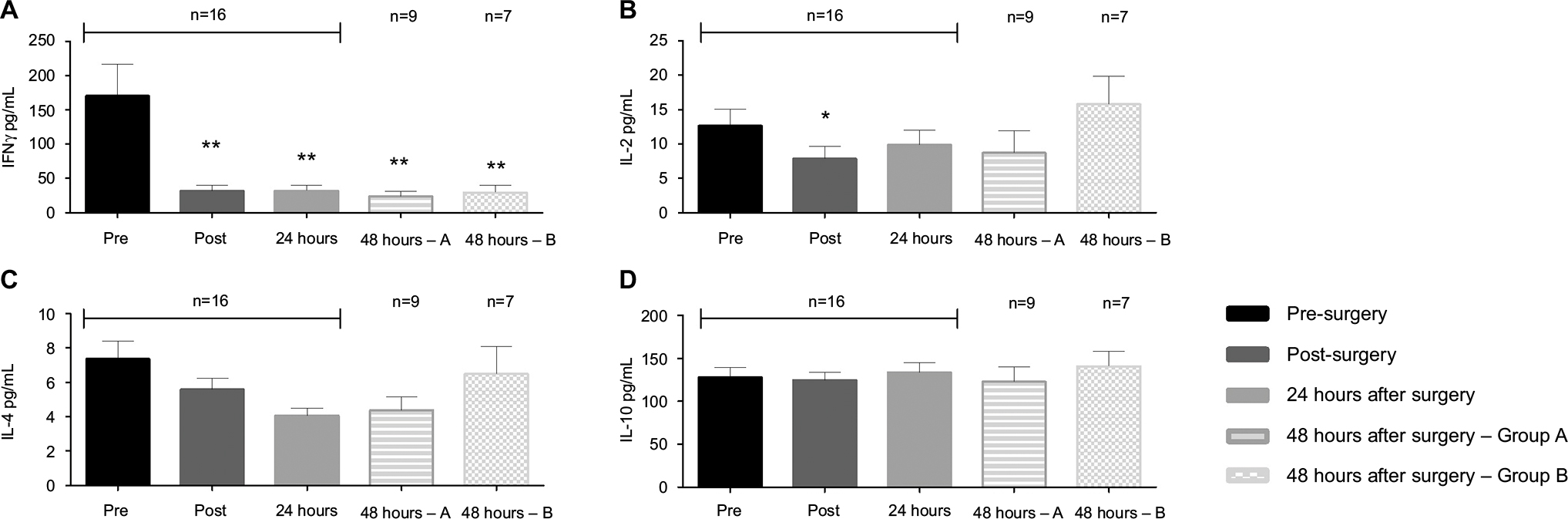 | Figure 3 Cytokine levels released by PBMC after PHA stimulation. Notes: Blood samples were obtained before surgery, immediately after the end of surgery and 24 and 48 hours later. PBMC were stimulated in vitro for 24 hours with 10 µg/mL PHA, and INF-γ (A), IL-2 (B), IL-4 (C) and IL-10 (D) released in media were evaluated by ELISA. Data from pre-, post- and 24 hours after surgery include all patients (n=16), while data at 48 hours represent patients divided into Group A (n=9) or Group B (n=7; refer the “Patients and methods” section). Values are mean±SEM. *p<0.05 and **p<0.01 v.s. presurgery cytokine levels. Active treatment (Group A: ropivacaine 0.2%+methylprednisolone 1 mg/kg, 10 mL/h); placebo (Group B: saline 10 mL/h). Abbreviations: PBMC, peripheral blood mononuclear cells; PHA, phytohemagglutinin; ELISA, enzyme-linked immunosorbent assay; SEM, standard error of mean. |
On the other hand, the Th2 cytokines IL-4 and IL-10 do not appear to be altered either by surgery or postoperative pain treatments (Figure 3C and D).
Lymphoproliferation
As reported in Figure 4, a significant reduction in lymphoproliferation was observed immediately after surgery in all patients; a trend toward a return to presurgical lymphoproliferation was retrieved at 48 hours, without statistically significant difference.
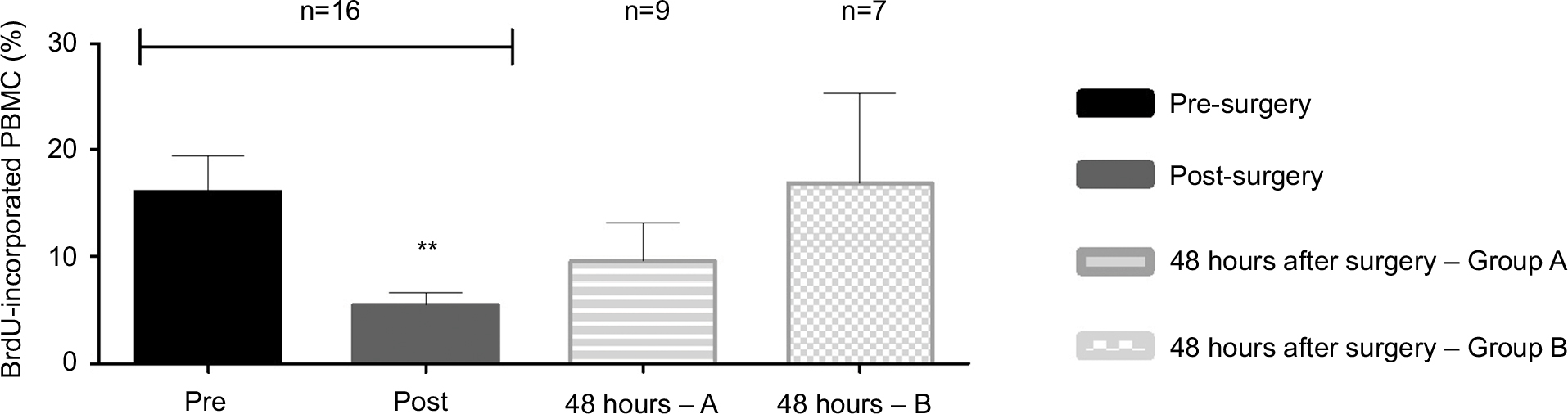 | Figure 4 Lymphocyte proliferation. Notes: Blood samples were obtained before surgery, immediately after the end of surgery and 48 hours later. Cells were stimulated in vitro for 72 hours with 10 µg/mL PHA. Proliferation is expressed as percentage of PBMC that incorporated BrdU in 24 hours. Data from pre- and post-surgery include all patients (n=16), while data at 48 hours represent patients divided into Group A (n=9) or Group B (n=7; refer the “Patients and methods” section). **p<0.01 vs. Pre-surgery. Active treatment (Group A: ropivacaine 0.2%+methylprednisolone 1 mg/kg, 10 mL/h); placebo (Group B: saline 10 mL/h). Abbreviations: PHA, phytohemagglutinin; PBMC, peripheral blood mononuclear cells; BrdU, 5-bromo-2′-deoxyuridine. |
Morphine consumption, immune responses and age
The amount of morphine consumption was different among patients, as reported in Table 1. Morphine intake was significantly higher in the first 24 hours than in the second postoperative day (21.13±4.58 mg vs. 11.25±2.66 mg, mean±SEM; p<0.05 according to paired t-test). In our cohort, we did not find any statistical significant difference in opioid consumption (Group A: 11.7±4.3 mg; Group B: 10.7±3.1 mg, mean±SEM; p=0.83 according to t-test) in the second day after surgery (24–48 hours) between the two groups.
We therefore correlated morphine consumption and the immune response within the whole sample, without looking at possible differences between the two groups. No inverse correlation was determined for any cytokine and morphine intake (data not shown). A significant correlation was found between total (0–48 hours) morphine consumption and lymphoproliferation at 48 hours (Figure 5A).
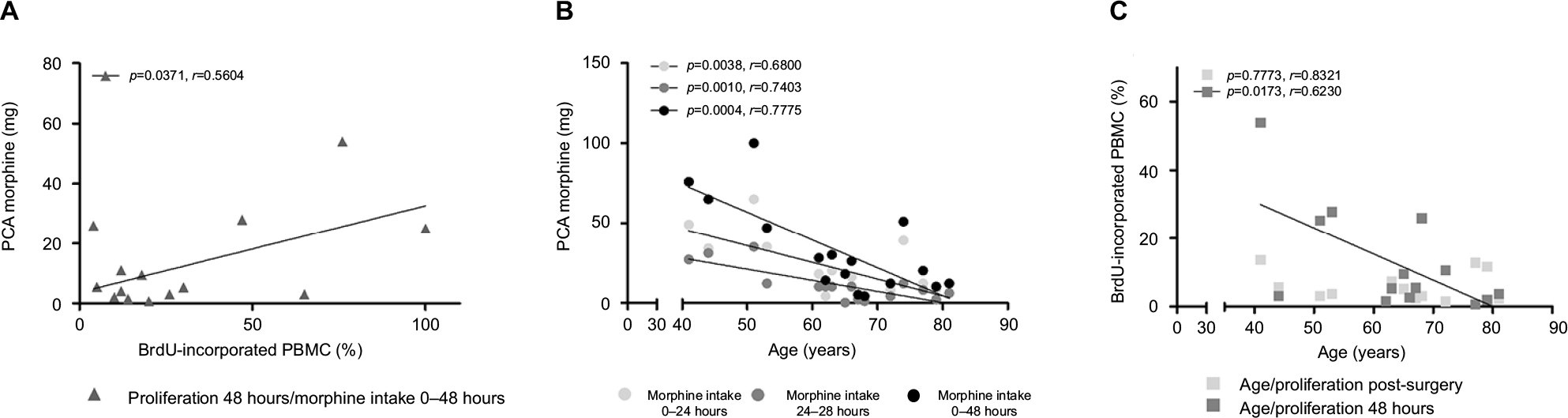 | Figure 5 Correlation analysis between (A) total morphine intake and lymphocyte proliferation at 48 hours, (B) morphine intake at 0–24 hours, 24–48 hours and 0–48 hours and patients’ age and (C) lymphoproliferation post surgery and at 48 hours after surgery and age. Notes: Correlations were investigated using the Pearson correlation test. Calculated regression lines are shown. Abbreviations: BrdU, 5-bromo-2′-deoxyuridine; PBMC, peripheral blood mononuclear cells; PCA, patient-controlled analgesia. |
We found a significant inverse correlation between age and morphine intake at all times of evaluation, i.e., 0–24 hours, 24–48 hours and 0–48 hours (Figure 5B). A significant inverse correlation was also evident between age and lymphoproliferation (Figure 5C) only when measured 48 hours after surgery. Duration of surgery did not significantly correlate with either any immune parameter studied or morphine intake (data not shown).
Discussion
Immune response is severely damaged during the perioperative period, with systemic inflammatory responses accompanied by immune depression.3,11 However, it is still unclear whether the perioperative analgesic treatment can affect this response or not and how postoperative and persistent pain do correlate with it.
In this pilot study, we investigated how the cellular immune response is affected within the postoperative period and how it correlates with opioid consumption in a multimodal analgesic approach.
Since a balance between Th1 and Th2 cells is needed for a correct homeostasis of the immune system in normal conditions,29,30 we measured representative Th1 and Th2 cytokines.28,31 Furthermore, also the proinflammatory cytokines TNF-α and IL-1β were evaluated, considering their relevance in antimicrobial immunity and in immune surveillance against tumors.32
The results obtained clearly confirm that a relevant suppression of cellular immune responses happens after major surgery.
Among the investigated cytokines, TNF-α and the Th1 cytokines IFN-γ and IL-2 are the most affected, suggesting a global reduction in cellular immune response. In contrast, anti-inflammatory and Th2 cytokines are not altered in our cohort. Since IFN-γ/IL-4 ratio is frequently used as index for determining T helper profile, a reduction in Th1 activity can be hypothesized after surgery.
One of the more relevant points of this study is the observation that the immune response has not fully recovered 48 hours after surgery. Some of the cytokines are still significantly reduced, while an improvement in IL-2 production and lymphoproliferation starts, although not complete. Immune dysfunction is therefore partially maintained at 48 hours, potentially increasing the risk of postoperative infection, sepsis or eventually favoring cancer recurrence.
Several factors are known to contribute to immunodepression. Both surgical stress (with HPA activation) and drugs that are used for anesthesia and analgesia can impact immune response. Pain itself has a negative impact on immune response.33,34 In the postoperative period, an optimal control of pain is auspicable, and it is fully achieved in the patients of the study. Extensive preclinical studies from ours and other groups have demonstrated that postoperative immune function is usually more rapidly recovered34–36 when pain control is obtained with drugs devoid of intrinsic immunomodulatory activity; similar results were also reported in a clinical study where the intrinsic immunosuppressive morphine was compared with the non-immunosuppressive tramadol in a group of patients receiving minor surgery.36
All our patients received fentanyl/remifentanil intraoperatively and a morphine bolus immediately before the end of surgery, just before blood withdrawal for immune evaluation. Both fentanyl and morphine are generally considered to be immunosuppressive, and it can be supposed that they participate in the reduction of cytokine production and lymphoproliferation that we observed after surgery.11,23,37,38
Some authors suggested that the effects of opioids such as fentanyl and morphine on immune responses could be dose related.11,21,37 A possible bias of our study is related to the fact that we do not have two groups with different intraoperative opioids intake, but in order to specifically rule out the effect of opioids v.s. surgical stress in giving immune dysregulation, an intraoperative complete opioid-free approach would be needed.39 Postoperative morphine, as well, may account for further immune dysfunction and its duration. Patients enrolled in the current cohort are part of a larger multicenter study, which was designed to reduce morphine intake from 24 hours after surgery in the treatment group. The results on morphine consumption of the whole sample will be published separately. As no difference in morphine consumption was observed between the two groups of patients specifically included in the current study, we decided to consider the amount of morphine for each patient, independent of the allocation group. Morphine did not result to be mainly responsible for the observed decrease in cytokine production: no negative correlation was found between morphine intake and any of the immune parameter, indeed. Again, it is difficult to dissect the actual perioperative impact of morphine on immune function, but since patients were exposed to different amounts of morphine and no differences in immunity were observed, morphine-induced immunomodulation observed in our cohort is unlikely to be dose related.
In addition, no significant difference was found for any of the immune parameters in the two groups at 48 hours from surgery, despite the saline group displayed a slightly better lymphoproliferation. Therefore, although treatment (local anesthetic/methylprednisolone) does not have a strong impact on immune functionality, potential benefit in terms of analgesia should be balanced with the possible harms (namely, steroid-associated immune suppression).
Another important result derived by our study is the confirmation of an inverse correlation between age and morphine intake: older patients self-administered less morphine, with similar pain control but without an impact on immune function. Factors that may contribute could be related to either pharmacokinetic or pharmacodynamic aspects.40–42 It is well known that morphine pharmacokinetic (especially morphine metabolism) plays an important role in the final analgesic effect, and morphine pharmacokinetic may be different in older subjects.43 Different sensitivities to morphine, as well as the psychological attitude of decreased self-administration of morphine, may be part of the aging process in some patients. Finally, the “age” variable may differently impact on opioid consumption according to the genetic profile: in our recent study on patients undergoing abdominal surgery, a model including age and nine single nucleotide polymorphisms (SNPs) of genes associated with pain sensitivity and opioid response explained the highest variability of morphine consumption.44
Age also seems to play a role in patients’ ability to recover from decreased lymphoproliferation: significant inverse correlation exists between lymphoproliferation at 48 hours and patient’s age. Since this correlation is absent immediately after surgery, we suggest that patients are equally sensitive to surgical stress, but younger patients have higher potential of recovery.45,46
Surprisingly, we found a positive correlation between morphine and lymphoproliferation at 48 hours after surgery. However, since older patients had both lower morphine intake and lower recovery of lymphoproliferation, we cannot definitely rule out whether there is a direct relationship between morphine and proliferation or rather the “age” variable prevails.
In contrast, no differences were found considering male or female subjects.
We are aware that other variables or procedures, such as the duration of surgery and blood transfusions, could impact on immune responses.3,47 Although the duration of surgery was different among patients, in our patients’ groups we could not find any correlation between the duration of surgery and the studied parameters. Moreover, due to the limited number of transfused patients in our study, we could not draw any conclusion on this aspect.3,47
We acknowledge that the study has some limitations.
The small number of patients is inherent with the nature of the study; we wanted to perform a pilot evaluation to detect differences in immune function worth to be analyzed in further studies, hopefully comparing patients with opioid-based v.s. non-opioid analgesia. Second, we stopped our evaluations at 48 hours after surgery; future studies should follow-up for a longer period of time, to evaluate whether and when immune function returns to preoperative values.
The strength of our research is that we investigated functional responses of immune cells and not only a differential counting of lymphocytes or serum cytokine measurements as in the majority of published works.13
Conclusion
This small study indicates that functional immune activity is depressed with surgery and that alterations persist despite a good postoperative pain control. We also confirmed that morphine consumption is modified by age, meanwhile showing that recovery of immune depression is more difficult in older patients. It is difficult to extrapolate the role of morphine in the postoperative period, but it can be suggested that the impact of the opioid on immunity is an “all or nothing” effect rather than being dose related. Further therapeutic approaches must be envisaged in order to more effectively prevent or revert postoperative immunosuppression.
Acknowledgment
The current study is supported by a grant from the Italian Health Ministry (“New nanotechnology and biomedical approaches to improve postoperative pain treatment reducing risks related to opioids” – GR-2010-2318370; Principal Investigator Massimo Allegri).
Disclosure
The authors report no conflicts of interest in this work.
References
Desborough JP. The stress response to trauma and surgery. Br J Anaesth. 2000;85:109–117. | ||
Colacchio TA, Yeager MP, Hildebrandt LW. Perioperative immunomodulation in cancer surgery. Am J Surg. 1994;167(1):174–179. | ||
Cata JP, Bauer M, Sokari T, et al. Effects of surgery, general anesthesia, and perioperative epidural analgesia on the immune function of patients with non-small cell lung cancer. J Clin Anesth. 2013;25(4):255–262. | ||
O’Dwyer MJ, Owen HC, Torrance HDT. The perioperative immune response. Curr Opin Crit Care. 2015;21(4):336–342. | ||
Albertsmeier M, Prix NJ, Winter H, Bazhin A, Werner J, Angele MK. Monocyte-dependent suppression of T-cell function in postoperative patients and abdominal sepsis. Shock. 2017;48(6):651–656. | ||
Day A, Smith R, Jourdan I, Fawcett W, Scott M, Rockall T. Retrospective analysis of the effect of postoperative analgesia on survival in patients after laparoscopic resection of colorectal cancer. Br J Anaesth. 2012;109(2):185–190. | ||
Das J, Kumar S, Khanna S, Mehta Y. Are we causing the recurrence-impact of perioperative period on long-term cancer prognosis: Review of current evidence and practice. J Anaesthesiol Clin Pharmacol. 2014;30(2):153–159. | ||
Kaye AD, Patel N, Bueno FR, et al. Effect of opiates, anesthetic techniques, and other perioperative factors on surgical cancer patients. Ochsner J. 2014;14(2):216–228. | ||
Chen WK, Ren L, Wei Y, Zhu DX, Miao CH, Xu JM. General anesthesia combined with epidural anesthesia ameliorates the effect of fast-track surgery by mitigating immunosuppression and facilitating intestinal functional recovery in colon cancer patients. Int J Colorectal Dis. 2015;30(4):475–481. | ||
Kimura F, Shimizu H, Yoshidome H, Ohtsuka M, Miyazaki M. Immunosuppression following surgical and traumatic injury. Surg Today. 2010;40(9):793–808. | ||
Sacerdote P, Franchi S, Panerai AE. Non-analgesic effects of opioids: mechanisms and potential clinical relevance of opioid-induced immunodepression. Curr Pharm Des. 2012;18(37):6034–6042. | ||
Meserve JR, Kaye AD, Prabhakar A, Urman RD. The role of analgesics in cancer propagation. Best Pract Res Clin Anaesthesiol. 2014;28(2):139–151. | ||
Boland JW, Pockley AG. Influence of opioids on immune function in patients with cancer pain: from bench to bedside. Br J Pharmacol. Epub 2017 Jun 8:doi: 10.1111/bph.13903. | ||
Al-Hashimi M, Scott SWM, Thompson JP, Lambert DG. Opioids and immune modulation: more questions than answers. Br J Anaesth. 2013;111(1):80–88. | ||
Vallejo R, de Leon-Casasola O, Benyamin R. Opioid therapy and immunosuppression: a review. Am J Ther. 2004;11(5):354–365. | ||
Cata JP, Bugada D, Marchesini M, De Gregori M, Allegri M. Opioids and cancer recurrence: A brief review of the literature. Cancer Cell Microenviron. 2016;3:e1159. | ||
Gaveriaux-Ruff C, Matthes HW, Peluso J, Kieffer BL. Abolition of morphine-immunosuppression in mice lacking the mu-opioid receptor gene. Proc Natl Acad Sci U S A. 1998;95(11):6326–6330. | ||
Roy S, Liu HC, Loh HH. mu-Opioid receptor-knockout mice: the role of mu-opioid receptor in gastrointestinal transit. Brain Res Mol Brain Res. 1998;56(1–2):281–283. | ||
Wang J, Charboneau R, Balasubramanian S, Barke RA, Loh HH, Roy S. The immunosuppressive effects of chronic morphine treatment are partially dependent on corticosterone and mediated by the mu-opioid receptor. J Leukoc Biol. 2002;71(5):782–790. | ||
Fecho K, Maslonek KA, Dykstra LA, Lysle DT. Evidence for sympathetic and adrenal involvement in the immunomodulatory effects of morphine treatments in rats. J Pharmacol Exp Ther. 1996;277:633–645. | ||
Yardeni IZ, Beilin B, Mayburd E, Alcalay Y, Bessler H. Relationship between fentanyl dosage and immune function in the postoperative period. J Opioid Manag. 2008;4(1):27–33. | ||
Shavit Y, Ben-Eliyahu S, Zeidel A, Beilin B. Effects of fentanyl on natural killer cell activity and on resistance to tumor metastasis in rats. Dose and timing study. Neuroimmunomodulation. 2004;11(4):255–260. | ||
Beilin B, Bessler H, Mayburd E, et al. Effects of preemptive analgesia on pain and cytokine production in the postoperative period. Anesthesiology. 2003;2003:151–155. | ||
Ben-Eliyahu S, Page GG, Yirmiya R, Shakhar G. Evidence that stress and surgical interventions promote tumor development by suppressing natural killer cell activity. Int J Cancer. 1999;80(6):880–888. | ||
Tedore T. Regional anaesthesia and analgesia: relationship to cancer recurrence and survival. Br J Anaesth. 2015;115(suppl 2):ii34–ii45. | ||
Cata JP, Kurz A. Challenges in research related to perioperative cancer care and cancer outcomes. Best Pract Res Clin Anaesthesiol. 2013; 27(4):457–464. | ||
Bugada D, De Gregori M, Compagnone C, et al. Continuous wound infusion of local anesthetic and steroid after major abdominal surgery: study protocol for a randomized controlled trial. Trials. 2015; 16:357. | ||
Sacerdote P, Franchi S, Gerra G, Leccese V, Panerai AE, Somaini L. Buprenorphine and methadone maintenance treatment of heroin addicts preserves immune function. Brain Behav Immun. 2008;22(4):606–613. | ||
Charlton B, Lafferty KJ. The Th1/Th2 balance in autoimmunity. Curr Opin Immunol. 1994;7:793–798. | ||
Mosman TR, Sad S. The expanding universe of T-cell subsets; Th1,Th2 and more. Immunol Today. 1996;17(3):138–146. | ||
Sacerdote P, Manfredi B, Gaspani L, Panerai AE. The opioid antagonist naloxone induces a shift from type 2 to type 1 cytokine pattern in BALB/cJ mice. Blood. 2000;95(6):2031–2036. | ||
Beutler B. Innate immunity, an overview. Mol Immunol. 2004;40(12):845–849. | ||
Page GG. Immunologic effects of opioids in the presence or absence of pain. J Pain Symptom Manage. 2005;29(5 suppl):S25–S31. | ||
Franchi S, Panerai AE, Sacerdote P. Buprenorphine ameliorates the effect of surgery on hypothalamus-pituitary-adrenal axis, natural killer cell activity and metastatic colonization in rats in comparison with morphine or fentanyl treatment. Brain Behav Immun. 2007;21(6):767–774. | ||
Gaspani L, Bianchi M, Limiroli E, Panerai AE, Sacerdote P. The analgesic drug tramadol prevents the effect of surgery on natural killer cell activity and metastatic colonization in rats. J Neuroimmunol. 2002;129(1–2):18–24. | ||
Sacerdote P, Bianchi M, Gaspani L, et al. The effects of tramadol and morphine on immune responses and pain after surgery in cancer patients. Anesth Analg. 2000;90(6):1411–1414. | ||
Beilin B, Shavit Y, Trabekin E, et al. The effects of postoperative pain management on immune response to surgery. Anesth Analg. 2003;97(3):822–827. | ||
Brack A, Rittner HL, Stein C. Immunosuppressive effects of opioids-clinical relevance. Neuroimmune Pharmacol. 2011;6:490–502. | ||
Cata JP, Bugada D, de Andrés J. Opioid-less perioperative care. Minerva Anestesiol. 2017;83(3):315–320. | ||
Pergolizzi J, Böger RH, Budd K, et al. Opioids and the management of chronic severe pain in the elderly: consensus statement of an International Expert Panel with focus on the six clinically most often used World Health Organization Step III opioids (buprenorphine, fentanyl, hydromorphone, methadone, morphine, oxycodone). Pain Pract. 2008;8(4):287–313. | ||
Galicia-Castillo M. Opioids for persistent pain in older adults. Cleve Clin J Med. 2016;83(6):443–451. | ||
Karp JF, Shega JW, Morone NE, Weiner DK. Advances in understanding the mechanisms and management of persistent pain in older adults. Br J Anaesth. 2008;101:111–120. | ||
Gupta DK, Avram MJ. Rational opioid dosing in the elderly: dose and dosing interval when initiating opioid therapy. Clin Pharmacol Ther. 2012;91(2):339–343. | ||
De Gregori M, Diatchenko L, Ingelmo PM, et al. Human genetic variability contributes to postoperative morphine consumption. J Pain. 2016;17(5):628–636. | ||
Yao X, Li H, Leng SX. Inflammation and immune system alterations in frailty. Clin Geriatr Med. 2011;27(1):79–87. | ||
Castle SC, Uyemura K, Fulop T, Makinodan T. Host resistance and immune responses in advanced age. Clin Geriatr Med. 2007;23(3):463–479. | ||
Youssef LA, Spitalnik SL. Transfusion-related immunomodulation: a reappraisal. Curr Opin Hematol. 2017;24(6):551–557. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.