Back to Journals » Clinical Ophthalmology » Volume 20
Immediate Versus Delayed Sequential Bilateral Cataract Surgery: A Systematic Review
Authors Al-Swailem S ![]() , Ahmad K
, Ahmad K ![]() , AlJbreen AJ, AlHilali S
, AlJbreen AJ, AlHilali S ![]()
Received 13 November 2025
Accepted for publication 27 January 2026
Published 12 March 2026 Volume 2026:20 581259
DOI https://doi.org/10.2147/OPTH.S581259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Samar Al-Swailem,1 Khabir Ahmad,2 Abdulaziz Jabr AlJbreen,3 Sara AlHilali1
1Anterior Segment Division, King Khaled Eye Specialist Hospital and Research Center, Riyadh, Saudi Arabia; 2Research Department, King Khaled Eye Specialist Hospital and Research Center, Riyadh, Saudi Arabia; 3Ophthalmology Department, Security Force Hospital, Riyadh, Saudi Arabia
Correspondence: Sara AlHilali, Anterior Segment Division, King Khaled Eye Specialist Hospital and Research Center, P.O. Box 7191, Riyadh, 11462, Saudi Arabia, Tel +966544017155, Email [email protected]
Objective: To compare the visual outcomes, safety, and patient-reported outcomes of ISBCS versus DSBCS in adults undergoing cataract surgery.
Evidence Review: A systematic search of PubMed, Embase, CENTRAL, Web of Science, and gray literature (conference abstracts, registries) was conducted for studies published up to March 2023. Eligible studies directly compared ISBCS and DSBCS in adults, reporting best corrected visual acuity (BCVA), complications, or patient-reported outcomes. Two reviewers independently screened studies, extracted data, and resolved discrepancies by consensus.
Findings: Nine studies were included (3 randomized controlled trials, 5 retrospective cohorts, 1 review), encompassing sample sizes ranging from 298 patients to over 496,000 eyes. Both ISBCS and DSBCS resulted in significant improvements in BCVA, with comparable refractive accuracy. No significant differences were observed in serious complications such as endophthalmitis, cystoid macular edema, or posterior capsular rupture. Some studies reported a trend toward slightly higher patient satisfaction and faster rehabilitation in the ISBCS group.
Conclusions and Relevance: ISBCS appears to be a safe and effective alternative to DSBCS in carefully selected patients, offering potential benefits in efficiency, recovery time, and patient satisfaction. Rigorous randomized controlled trials with standardized outcome measures and long-term follow-up are needed to further validate these findings.
Keywords: cataract surgery, immediate sequential bilateral cataract surgery, ISBCS, delayed sequential bilateral cataract surgery, DSBCS, visual acuity, complications, outcomes, safety or satisfaction
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Surico has been published for this article.
Introduction
Advances in cataract surgery have evolved over decades, progressing from earlier techniques such as intracapsular and extracapsular extraction to modern phacoemulsification. These ongoing improvements have resulted in surgical methods that significantly decrease patient complications and shorten recovery periods.1 Cataracts remain a major cause of vision loss, and with an aging global population, the need for treatment is increasing. Approximately 65.2 million individuals are estimated to require cataract surgery.2 Immediately Sequential Bilateral Cataract Surgery (ISBCS) offers a potential solution to address this growing demand. Several countries have integrated ISBCS into their standard cataract care. For example, it accounts for 80% of cataract surgeries in the Canary Islands and up to 50% in Finland. While ISBCS is performed in other nations like Sweden, the USA, the UK, Germany, Spain, Australia, India, Korea, and Chile, the adoption rate is currently lower.3,4
Traditionally, cataract surgery has been performed on one eye at a time, with a delay between surgeries, known as Delayed Sequential Bilateral Cataract Surgery (DSBCS). However, advancements in surgical techniques, anesthesia, and infection control have led to the emergence of Immediately Sequential Bilateral Cataract Surgery (ISBCS), where both eyes are operated on during the same surgical session. ISBCS offers potential benefits, including reduced recovery time, fewer hospital visits, and lower healthcare costs, but it also raises concerns about the risk of bilateral complications, such as endophthalmitis, and logistical challenges in postoperative care.5 In the published literature, ISBCS has generally been offered to carefully selected patients, typically those with bilateral uncomplicated cataracts, absence of significant ocular comorbidities, and suitability for standardized surgical protocols, including strict aseptic measures and intracameral antibiotic use.5 While Delayed Sequential Bilateral Cataract Surgery (DSBCS) remains the more prevalent approach to cataract treatment, ISBCS is not yet widely considered standard practice.6 Exceptions to this general preference include specific cases, such as pediatric patients or those requiring general anesthesia.7 The limited availability of research comparing the benefits and risks of ISBCS and DSBCS makes it challenging to advocate for the widespread adoption of ISBCS as the new standard of care.
The debate over the safety and efficacy of ISBCS versus DSBCS has gained significant attention in ophthalmology. Proponents of ISBCS argue that modern protocols, including strict aseptic techniques and intracameral antibiotics, have minimized risks, making it a viable option for appropriately selected patients.8 On the other hand, critics emphasize the importance of maintaining DSBCS as the gold standard, citing its long-standing safety record and ability to mitigate the rare but serious risk of bilateral complications.9 Understanding the comparative outcomes of these two approaches are critical for optimizing patient care, improving resource utilization, and addressing growing demands for cataract surgery in aging populations.
Despite increasing interest in immediately sequential bilateral cataract surgery, its adoption remains variable across regions, largely due to concerns regarding bilateral complications and the absence of universal guideline endorsement. Existing evidence is derived from heterogeneous study designs and populations, making interpretation challenging. A systematic synthesis of comparative outcomes is therefore necessary to inform clinical practice and policy decisions.
Methodology
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A comprehensive search was conducted in PubMed, Embase, Cochrane CENTRAL, and Web of Science using terms related to “cataract surgery,” “immediate sequential,” “same-day” and “delayed sequential.” No date restrictions were applied. Gray literature, including conference proceedings and clinical trial registries, was also searched. Reference lists of included studies were screened for additional eligible reports.
Two reviewers (SH, AJ) independently screened titles and abstracts, and full texts of potentially relevant studies were reviewed against predefined inclusion criteria. Disagreements were resolved by discussion or consultation with a third reviewer. Eligible studies included randomized controlled trials and comparative observational studies of adults undergoing cataract surgery, in which ISBCS was compared with DSBCS. Outcomes of interest included BCVA at specified follow-up intervals, intraoperative and postoperative complications, refractive accuracy, and patient-reported outcomes. Studies not directly comparing ISBCS with DSBCS, or those with insufficient outcome data, were excluded.
Data extraction was performed independently using a standardized form, capturing study design, sample size, patient demographics, surgical technique, intraocular lens type, and outcome measures. A qualitative synthesis of findings was undertaken. Meta-analysis was initially considered but not performed due to significant heterogeneity in study designs, populations, and outcome reporting. This study did not involve direct participation of human subjects. All data analyzed during this study are included in this published article and its references. Ethical approval and informed consent were not required as this work is based on previously published studies.
Results
Study Characteristics
The PRISMA flow diagram shows the systematic review process, beginning with the identification of 355 records through database searching across Medline (n=100), PubMed (n=152), Embase (n=67), and CINAHL (n=36). Following the removal of duplicates, a count of 272 records remained. Of these, 95 records were screened by title and abstract, resulting in the exclusion of 82 records that did not meet the inclusion criteria. The remaining 13 full-text articles were assessed for eligibility. Of these, 4 were excluded, because they focused on another outcome. The results of this systematic review were reported by the PRISMA guidelines [Figure 1]. The systematic review included a total of 9 studies published between 2011 and 2023, spanning the Netherlands, USA, Sweden, South Korea, Pakistan, Canada, Spain, and Finland. Different study designs were included, with three randomized controlled trials (RCTs), five retrospective cohort studies, and one systematic review [Table 1].
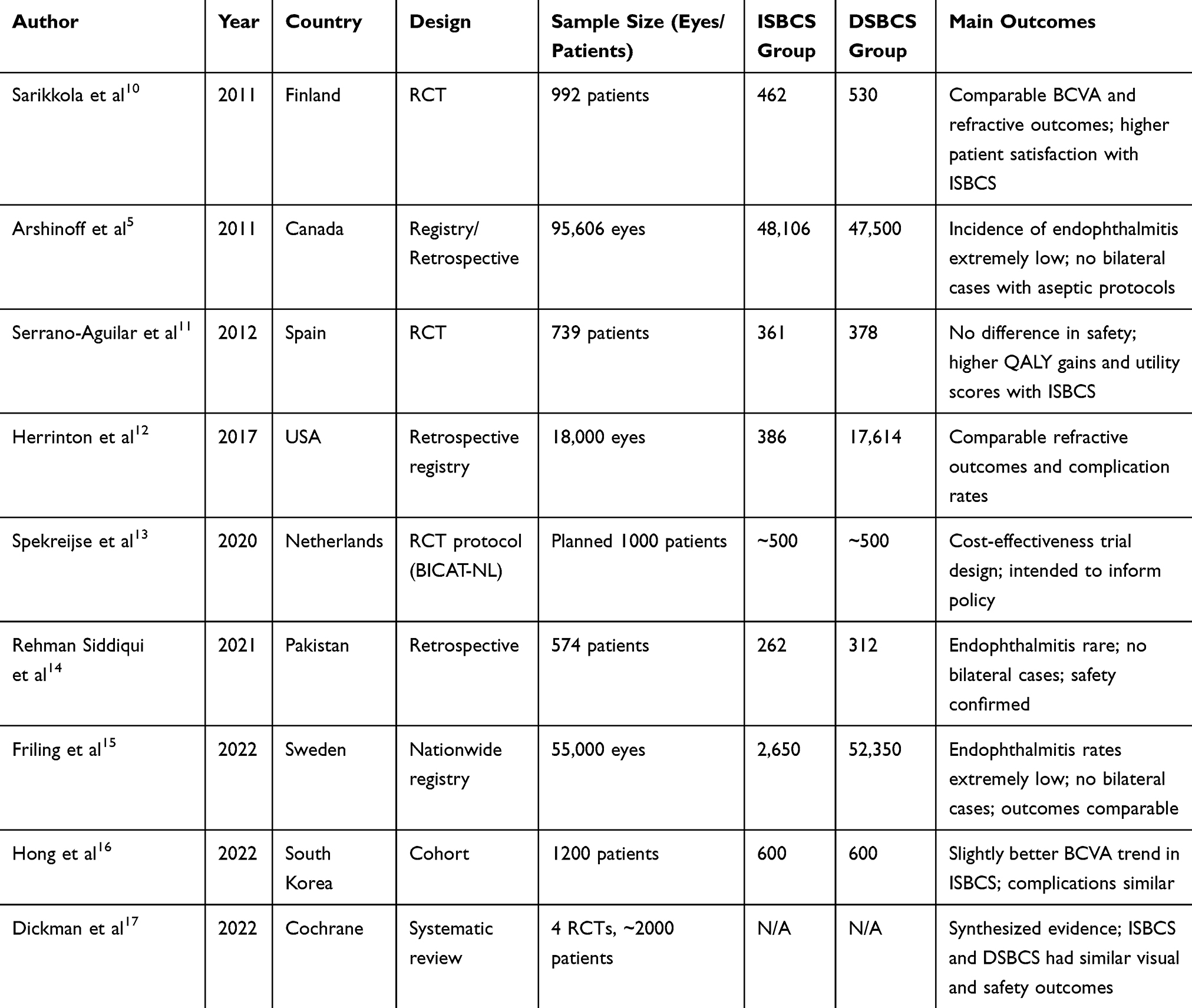 |
Table 1 Summary of Studies Comparing ISBCS and DSBCS |
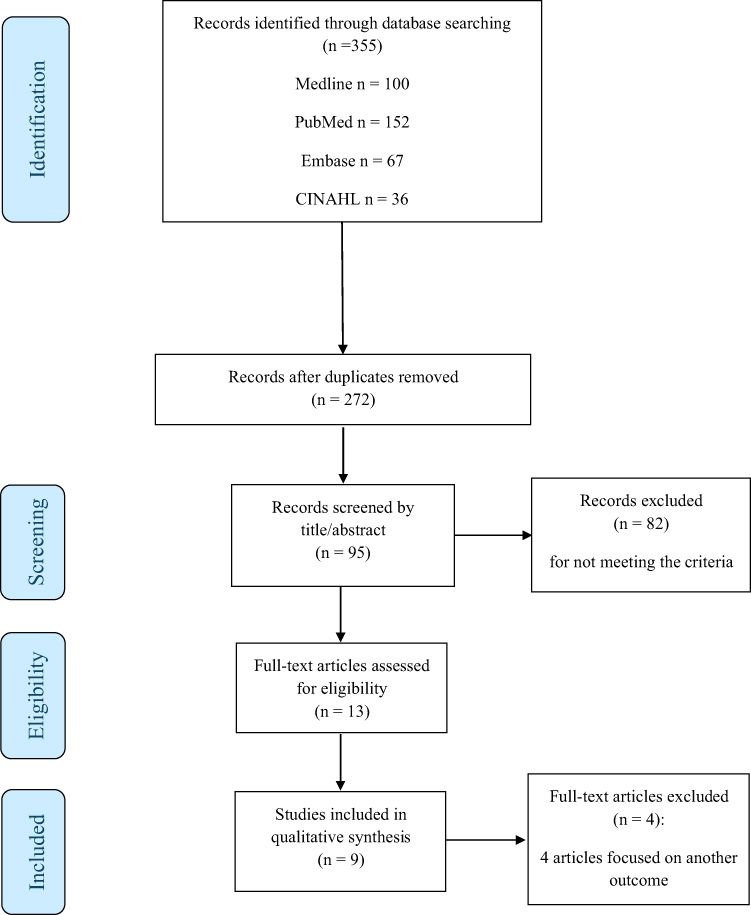 |
Figure 1 PRISMA flow diagram of study selection process. Notes: Flowchart illustrating the identification, screening, eligibility assessment, and inclusion of studies comparing immediate sequential bilateral cataract surgery (ISBCS) and delayed sequential bilateral cataract surgery (DSBCS) in this systematic review. A total of 355 records were identified through database searching, 272 records remained after duplicate removal, 95 records were screened by title and abstract, and 9 studies met the inclusion criteria for qualitative synthesis. |
The sample sizes ranged from 298 patients in a single-center study to 95,606 eyes in a large-scale review. The study populations primarily consisted of patients undergoing cataract surgery, with a focus on comparing immediate sequential bilateral cataract surgery (ISBCS) and delayed sequential bilateral cataract surgery (DSBCS). The age of participants differed across studies, with some reporting mean ages of 73.5 years in Serrano-Aguilar et al11 and others providing wide age ranges for ISBCS (21.4–100.6 years) and DSBCS (18.0–112.5 years) reflecting the inclusion of diverse patient demographics.17
The study populations were predominantly composed of patients with bilateral cataracts, with some studies specifically excluding complex cases or those with significant comorbidities. Retrospective cohort studies, such as those by Friling et al13 and Hong et al18 focused on large datasets from national registries or hospital records, providing insights into real-world outcomes. Geographically, the studies were distributed across high-income countries, with a notable concentration in the USA and Europe.
Pre-Operative Assessment
This systematic review examined the outcomes of immediate sequential bilateral cataract surgery (ISBCS) compared to delayed sequential bilateral cataract surgery (DSBCS) and unilateral cataract surgery. Several studies investigated the impact of ISBCS versus DSBCS on visual acuity and other outcomes. Herrinton et al15 reported preoperative utility scores and BCVA for both ISBCS and DSBCS groups, finding an average preoperative BCVA of 20/53 (0.42 logMAR) for ISBCS and 20/55 (0.44 logMAR) for DSBCS.
Spekreijse et al16 outlined a study protocol comparing ISBCS and DSBCS, including planned assessments of visual acuity and patient-reported outcomes. Dickman et al17 reported preoperative BCVA ranges for both ISBCS and DSBCS, with ISBCS ranging from 20/60 to 20/25 and DSBCS from 20/100 to 20/25. Serrano-Aguilar et al11 and Sarikkola et al12 also compared ISBCS and DSBCS using standard phacoemulsification procedures. Friling et al13 reported a lower percentage of patients with visual acuity of 20/200 or worse in the ISBCS group (10.03%) compared to the unilateral group (17.05%). Hong et al18 found statistically significant differences in postoperative logMAR BCVA, with the ISBCS group demonstrating better visual acuity (0.28 ± 0.30 logMAR) compared to the unilateral group (0.40 ± 0.45 logMAR). Siddiqui et al10 and Arshinoff et al5 investigated ISBCS procedures, including phacoemulsification and IOL implantation, but did not report comparative data.
Outcomes
The systematic review provides a comprehensive comparison between immediate sequential bilateral cataract surgery (ISBCS) and delayed sequential bilateral cataract surgery (DSBCS) across multiple outcomes, including visual acuity, refractive accuracy, complications, and patient-reported outcomes. Several studies, such as Spekreijse et al16 and Dickman et al17 reported that both ISBCS and DSBCS achieved similar refractive outcomes, with a high proportion of patients attaining target refraction within ±1.0 diopter. Herrinton et al15 and Hong et al18 further confirmed that postoperative best-corrected visual acuity (BCVA) was comparable between the two techniques, with ISBCS demonstrating a slightly higher percentage of eyes achieving 20/20 vision. The safety profile of ISBCS was also confirmed by Friling et al13 who found no significant difference in the incidence of postoperative endophthalmitis, the absolute risk of unilateral endophthalmitis with ISBCS was estimated at 0.019% and 0.029% respectively. No cases of bilateral endophthalmitis were reported.
Although risk factors such as capsule complications and the absence of intracameral antibiotics were associated with higher infection rates. Additionally, complications like cystoid macular edema and posterior capsular rupture were reported at similar rates in both surgical approaches.10,11 However, some studies indicated a slightly higher incidence of intraoperative complications in DSBCS, as noted by Dickman et al17 Regarding patient-reported outcomes, studies like Sarikkola et al12 and Dickman et al17 suggested a marginally higher post-operative utility score for ISBCS (0.97) compared to DSBCS (0.89), reflecting greater patient satisfaction.
Discussion
This systematic review analyzed data from nine studies published between 2011 and 2023 and provides insights into the comparative effectiveness and safety of immediate sequential bilateral cataract surgery (ISBCS) and delayed sequential bilateral cataract surgery (DSBCS). The heterogeneity observed in sample sizes, ranging from small single-center studies to large-scale reviews involving hundreds of thousands of eyes, as well as variability in patient demographics, may limit the ability to draw definitive conclusions applicable to all patients. However, this diversity also strengthens the review by encompassing a broader spectrum of patient populations and surgical practices, thereby enhancing its external validity. Most included studies were conducted in high-income healthcare systems with established infection-control protocols. Caution is therefore warranted when extrapolating these findings to low-resource settings, where surgical infrastructure and postoperative follow-up may differ.
Preoperative assessments, as documented by Herrinton et al15 and Dickman et al17 revealed generally comparable baseline visual acuity between the ISBCS and DSBCS groups. However, the wider ranges reported by Dickman et al17 suggest potentially greater variability in preoperative visual function within these groups. Establishing clear baseline characteristics is essential for accurately interpreting postoperative outcomes and discerning the true impact of each surgical approach. This is particularly important given that cataract surgery is primarily performed to improve visual function, and any comparison between techniques must account for pre-existing visual impairment.
In terms of refractive outcomes, the review indicates that both ISBCS and DSBCS achieve similar levels of accuracy, with a high proportion of patients attaining target refraction within ±1.0 diopter.16,17 This finding is consistent with the broader literature on modern cataract surgery, which generally reports excellent refractive outcomes with contemporary techniques such as phacoemulsification and intraocular lens implantation.14,19,20 The comparable refractive results suggest that both ISBCS and DSBCS can effectively correct refractive errors associated with cataracts.
Postoperative best-corrected visual acuity (BCVA) also appears to be similar between the two groups, with some studies suggesting a trend toward slightly better vision in the ISBCS group.15,18 This subtle difference, while potentially clinically relevant, requires further investigation in larger, rigorously designed studies with standardized visual acuity testing protocols. It is important to determine whether this observed trend is statistically significant and whether it translates into meaningful improvements in patients’ daily lives.
The safety of ISBCS is a critical consideration, and this review offers reassuring evidence in this regard. Study Friling et al13 found no significant difference in the incidence of postoperative endophthalmitis between ISBCS and DSBCS. This finding is in line with large-scale studies and national registry data that have consistently demonstrated low rates of endophthalmitis after cataract surgery.21,22 While the overall risk of endophthalmitis is low, it is crucial to emphasize that adherence to strict aseptic techniques and the use of intracameral antibiotics are essential to minimize this devastating complication in both ISBCS and DSBCS.23
Regarding other complications, such as cystoid macular edema and posterior capsular rupture, the review suggests similar rates in both surgical approaches.10,11 However, the observation of potentially higher intraoperative complication rates in DSBCS by Dickman et al17 warrants further investigation. It is important to understand the specific types of intraoperative complications that may be more common in DSBCS and to identify any modifiable risk factors.
Patient-reported outcomes, while assessed in only a few studies, hint at a potential advantage for ISBCS in terms of patient satisfaction.12,17 This is likely attributable to the convenience of undergoing a single surgical procedure and the potential for faster visual rehabilitation. However, more research is needed to comprehensively evaluate the impact of ISBCS on various patient-reported outcomes, including quality of life, visual function, and overall satisfaction. Such studies should employ validated questionnaires and assess outcomes at multiple time points after surgery.
A limitation of this review is that a meta-analysis could not be conducted due to the heterogeneity of study designs, populations, and outcome measures. In addition, direct comparison between randomized controlled trials and observational studies was limited by heterogeneity in design and outcome reporting, and excluded studies were not analyzed as they did not meet predefined inclusion criteria. While this limits the ability to provide pooled quantitative estimates, the qualitative synthesis still offers meaningful insights into the comparative safety and effectiveness of ISBCS and DSBCS.
Conclusions and Recommendations
In conclusion, this systematic review indicates that immediate sequential bilateral cataract surgery (ISBCS) is a safe and effective alternative to delayed sequential bilateral cataract surgery (DSBCS) in carefully selected patients when strict safety protocols are followed. Patients with bilateral uncomplicated cataracts, those at risk of significant postoperative anisometropia, and individuals requiring general anesthesia may particularly benefit from this approach. Successful outcomes rely on appropriate patient selection, meticulous surgical technique, and adherence to established infection-control measures.
Future research should focus on standardizing outcome measures, particularly patient-reported outcomes, and on conducting larger, well-designed studies with longer follow-up to further define the role of ISBCS across different healthcare settings.
Ethics and Consent Statements
This study is a systematic review based entirely on previously published data. No new human participants were enrolled, and therefore, ethics approval and patient consent were not required.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alio JL, Gessa-Sorroche M, Nowrouzi A, Maldonado MJ. Cirugía de catarata bilateral secuencia e inmediata. Archiv Sociedad Española Oftalmol. 2022;97(7):402–7. doi:10.1016/j.oftal.2021.06.007
2. Chen X, Xu J, Chen X, Yao K. Cataract: advances in surgery and whether surgery remains the only treatment in future. Adv Ophthalmol Pract Res. 2021;1(1). doi:10.1016/j.aopr.2021.100008
3. Beatty S, Aggarwal RK, David DB, Guarro M, Jones H, Pearce JL. Simultaneous bilateral cataract extraction in the UK. Br J Ophthalmol. 1995;79(12):1111–1114. doi:10.1136/BJO.79.12.1111
4. Malvankar-Mehta MS, Filek R, Iqbal M, et al. Immediately sequential bilateral cataract surgery: a cost-effective procedure. Can J Ophthalmol. 2013;48(6):482–488. doi:10.1016/J.JCJO.2013.05.004
5. Arshinoff SA, Bastianelli PA. Incidence of postoperative endophthalmitis after immediate sequential bilateral cataract surgery. J Cataract Refract Surg. 2011;37(12):2105–2114. doi:10.1016/J.JCRS.2011.06.036
6. Singh R, Dohlman TH, Sun G. Immediately sequential bilateral cataract surgery: advantages and disadvantages. Curr Opin Ophthalmol. 2017;28(1):81–86. doi:10.1097/ICU.0000000000000327
7. Singh G, Grzybowski A. Evolution of and developments in simultaneous bilateral cataract surgery. Update 2020. Ann Transl Med. 2020;8(22):1554. doi:10.21037/ATM-20-3490
8. Barry P, Cordovés L, Gardner S. ESCRS Guidelines for Prevention and Treatment of Endophthalmitis Following Cataract Surgery: prevention & Treatment Endophthalmitis. 2013. Available from: www.escrs.org.
9. Lundström M, Dickman M, Henry Y, et al. Changing practice patterns in European cataract surgery as reflected in the European Registry of Quality Outcomes for Cataract and Refractive Surgery 2008 to 2017. J Cataract Refract Surg. 2021;47(3):373–378. doi:10.1097/J.JCRS.0000000000000457
10. Rehman Siddiqui MA, Maroof Hussain SZ, Jeeva I. Post-operative endophthalmitis after immediate sequential bilateral cataract Surgery: a retrospective study from Pakistan. J Pak Med Assoc. 2021;71(10):2359–2363. doi:10.47391/JPMA.02-1072
11. Serrano-Aguilar P, Ramallo-Fariña Y, Cabrera-Hernández JM, et al. Immediately sequential versus delayed sequential bilateral cataract surgery: safety and effectiveness. J Cataract Refract Surg. 2012;38(10):1734–1742. doi:10.1016/J.JCRS.2012.05.024
12. Sarikkola AU, Uusitalo RJ, Hellstedt T, Ess SL, Leivo T, Kivelä T. Simultaneous bilateral versus sequential bilateral cataract surgery: helsinki Simultaneous Bilateral Cataract Surgery Study Report 1. J Cataract Refract Surg. 2011;37(6):992–1002. doi:10.1016/J.JCRS.2011.01.019
13. Friling E, Johansson B, Lundström M, Montan P. Postoperative Endophthalmitis in Immediate Sequential Bilateral Cataract Surgery: a Nationwide Registry Study. Ophthalmology. 2022;129(1):26–34. doi:10.1016/j.ophtha.2021.07.007
14. De Vries NE, Webers CAB, Montés-Micó R, Ferrer-Blasco T, Nuijts RMMA. Visual outcomes after cataract surgery with implantation of a +3.00 D or +4.00 D aspheric diffractive multifocal intraocular lens: comparative study. J Cataract Refract Surg. 2010;36(8):1316–1322. doi:10.1016/J.JCRS.2010.01.036
15. Herrinton LJ, Liu L, Alexeeff S, Carolan J, Shorstein NH. Immediate Sequential vs. Delayed Sequential Bilateral Cataract Surgery: retrospective Comparison of Postoperative Visual Outcomes. Ophthalmology. 2017;124(8):1126–1135. doi:10.1016/J.OPHTHA.2017.03.034
16. Spekreijse LS, Spekreijse LS, Simons RWP, et al. Cost-effectiveness of immediate versus delayed sequential bilateral cataract surgery in the Netherlands (the BICAT-NL study): study design of a prospective multicenter randomised controlled trial. BMC Ophthalmol. 2020;20(1). doi:10.1186/S12886-020-01521-X
17. Dickman MM, Spekreijse LS, Winkens B, et al. Immediate sequential bilateral surgery versus delayed sequential bilateral surgery for cataracts. Cochrane Database Syst Rev. 2022;2022(4). doi:10.1002/14651858.CD013270.PUB2
18. Hong S, Park W, Eom Y, Kim HM, Song JS. Comparisons of outcomes and complications of immediate sequential bilateral cataract surgery and unilateral cataract surgery in a tertiary hospital in South Korea. Sci Rep. 2022;12(1). doi:10.1038/S41598-022-26851-2
19. Mazzini C. Visual and Refractive Outcomes after Cataract Surgery with Implantation of a New Toric Intraocular Lens. Case Rep Ophthalmol. 2013;4(2):48. doi:10.1159/000353389
20. Kretz FTA, Breyer D, Klabe K, et al. Clinical outcomes after implantation of a trifocal toric intraocular lens. J Refract Surg. 2015;31(8):504–510. doi:10.3928/1081597X-20150622-01
21. Hatch WV, Cernat G, Wong D, Devenyi R, Bell CM. Risk Factors for Acute Endophthalmitis after Cataract Surgery: a Population-based Study. Ophthalmology. 2009;116(3):425–430. doi:10.1016/J.OPHTHA.2008.09.039
22. Sun J, Guo Z, Li H, Yang B, Wu X. Acute Infectious Endophthalmitis After Cataract Surgery: epidemiological Characteristics, Risk Factors and Incidence Trends, 2008–2019. Infect Drug Resist. 2021;14:1231. doi:10.2147/IDR.S304675
23. Ferlini L, Perrone L, Caride GG, et al. Intracameral moxifloxacin for prophylaxis of endophthalmitis after cataract surgery: a case Series. Invest Ophthalmol Vis Sci. 2013;54(15):2985.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Visual and Refractive Efficacy of Panoptix Toric Intraocular Lens in a Clinical Setting
Ackerman M, Lawless M, Levitz L, Bhatt U, Reich JA, Sutton G, Roberts TV, Tenen A, Kaur A, Hodge C
Clinical Ophthalmology 2022, 16:4227-4237
Published Date: 19 December 2022
Clinical Outcomes and Management Strategies for Capitellum and Trochlea Fractures: A Systematic Review
Lari A, Alrumaidhi Y, Martinez D, Ahmad A, Aljuwaied H, Alherz M, Prada C
Orthopedic Research and Reviews 2024, 16:179-197
Published Date: 26 June 2024
Surgical Outcomes of Cataract Surgery Following Rapid Glycemic Control During Preoperative Period
Wang Y, Wu X, Liu X, Cheng C, Wang W, Dai Y
Clinical Ophthalmology 2026, 20:561071
Published Date: 8 January 2026
From Sinus to Fistula: The Hidden Cost of Repeated Incision and Drainage in Paediatric Branchial Cleft Anomalies, a Case Series
Buhwa G, Nakasagga E, Seguya A, Kabagenyi F
International Medical Case Reports Journal 2026, 19:569032
Published Date: 31 January 2026
Incremental Predictive Value of Preoperative Macular Optical Coherence Tomography for Postoperative Visual Acuity After Phacoemulsification Cataract Surgery: A Retrospective Cohort Study
AlJohani S, Alshehri A, Al Khathami A, Alshehri RS, AlJaafar NA, Albadran RA, Alismail MMA, Shaheen A
Clinical Ophthalmology 2026, 20:589672
Published Date: 17 April 2026